BEFORE&YOU& INTUBATE&...BEFORE&YOU& INTUBATE& Shikha Gupta Division of Pulmonary and Critical Care...
39
BEFORE YOU INTUBATE Shikha Gupta Division of Pulmonary and Critical Care 08/03/15 – 08/04/15
Transcript of BEFORE&YOU& INTUBATE&...BEFORE&YOU& INTUBATE& Shikha Gupta Division of Pulmonary and Critical Care...

BEFORE YOU INTUBATE Shikha Gupta Division of Pulmonary and Critical Care
08/03/15 – 08/04/15

OUTLINE
� Indica3ons of intuba3on � Airway examina3on and recognizing difficult airways � SeEng up for intuba3on � Pa3ent posi3oning � Confirma3on of endotracheal tube placement

INDICATIONS FOR INTUBATION
� Respiratory failure § Hypoxic: inability to oxygenate § Hypercapneic : inability to ven3late § Cardiopulmonary arrest § Can’t be managed with non invasive ven3la3on
� Airway protec3on § Gag reflex ? § Ability to handle secre3ons § Obstructed airway

� Surgical pa3ents requiring general anesthesia � An3cipated need for intuba3on
§ Sep3c shock § Burn vic3ms with smoke inhala3on § ARDS

CONTRAINDICATIONS
� Upper airway pathology which would preclude intuba3on § Laryngectomy § Laryngeal fracture § Penetra3ng trauma to upper airway § GloEc stenosis
� Difficult airway § Use cau3on and if not emergent wait for help

PREPARING FOR INTUBATION


PREPARING FOR INTUBATION
� Assess pa3ent’s airway � Pre-‐oxygenate � Suc3on � Bag valve mask � PEEP valve � Monitors: BP, pulse oximetry, con3nuous cardiac monitor, ?CO2 capnography
� IV access � Medica3ons: induc3on agents, neuromuscular blockade

Tools for laryngoscopy � Laryngoscope
§ Ensure ligh3ng, baZery, etc
� Endotracheal tube § 2 sizes, stylet, syringe and check for balloon, lubricate distal ETT
� Adjunct airway management device: bougie and other difficult airway devices
� Oral and nasal airways � Confirma3on of tube placement: End 3dal CO2 detector � Equipment to hold tube

Y BAG PEOPLE BAC � Yankauer � Bag valve mask with PEEP valve � Access � Get your team � Posi3on � Evaluate for difficult airway � Oxygen and oral airway � Pharmacy � Larynoscope � Endotracheal tube with syringe � Back up plan � Auscultate � Confirma3on

ALWAYS EVALUATE THE AIRWAY
� Difficult to intubate § LEMON approach
� Difficult to ven3late § MOANS evalua3on


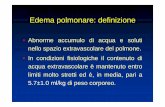
3: The pa3ent can open his/her mouth sufficiently to admit three of his/her own fingers. 3: The distance between the mentum and the neck/mandible junc3on (near the hyoid bone) is the length of three of the pa3ent's fingers. 2: The space between the superior notch of the thyroid car3lage and the neck/mandible junc3on, near the hyoid bone, is the length of two of the pa3ent's fingers.
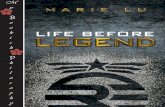
Class I: Visualiza3on of the soc palate, fauces, uvula, and both anterior and posterior pillars Class II: Visualiza3on of the soc palate, fauces and uvula
Class III : Visualiza3on of the soc palate and the base of the uvula Class IV : The soc palate is not visible at all

� Difficult to ven3late � MOANS evalua3on
§ M: mask seal • Normal anatomy, no facial hair, no bleeding/vomi3ng
§ O: obstruc3on/obesity § A: age > 55 years § N: no teeth
• If a pa3ent has dentures, they should be lec in situ during BMV, and then removed for laryngoscopy
§ S: s3ffness/snoring

AIRWAY MANEUVERS
� Improves airway patency � Head 3lt chin lic
§ two hands to extend the pa3ent's neck and open the airway. § While one hand applies downward pressure to the pa3ent's forehead,
the 3ps of the index and middle finger of the second hand lic the mandible at the mentum, which lics the tongue from the posterior pharynx

� Jaw thrust maneuver § Cervical spine injury is concerned § placing the heels of both hands on the parieto-‐occipital areas on
each side of the pa3ent's head, then grasping the angles of the mandible with the index and long fingers, and displacing the jaw anteriorly

BAG MASK VENTILATION � Mask placement:
§ Single hand • the web space between the thumb and index finger
res3ng against the mask connector
• other three fingers placed along the mandible and pull the mandible up
§ Two hand • Both thumbs and index fingers hold pressure along the
inferior and superior ridges of the mask. The other three fingers hold the mandible and perform chin-‐lic and jaw-‐thrust maneuver
• Thenar eminences along the long axis of mask, and four fingers provide chin-‐lic and jaw-‐thrust maneuvers

AIRWAY ADJUNCTS � prevent the tongue from occluding the airway and provide an open conduit for air to pass
� Oral airway § Size
• the flange at the pa3ent's mouth and the 3p directed toward the angle of the mandible. The 3p of an appropriately sized OPA should just reach the angle of the pa3ent's mandible

� Placement § star3ng with the curve inverted, and then rota3ng it 180 degrees as
its 3p reaches the posterior pharynx.

� Nasal airway § Size
• Length: distance between nostril and angle of mandible or ear lobe
§ Placement • Lubricate
• Bevel towards septum, advance akong floor of the nose • Rotate in the airway
§ Contraindica3ons • Epistaxis • known or suspected nasal fractures
• known or suspected basilar skull fractures

PRE-‐OXYGENATION � Goals:
§ Establish O2 reservoir § Maximize 3me for intuba3on
� Methods: § 3-‐5 minutes of 100% O2 via face mask § 4 (or 8) vital capacity breaths on 100% O2
§ Non invasive ven3lator: CPAP § Bag mask with PEEP valve § Non rebreather mask § High flow nasal canula

PRE-‐OXYGENATION
hZp://www.ncsrc.org/2_newsleZers_2008_2.shtml

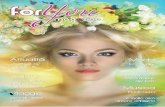
POSITIONING � Sniffing posi3on (RAMP)
§ atlanto-‐occipital extension with head eleva3on of 3 to 7 cm
§ adequate head eleva3on is the alignment of the pa3ent's ear (external auditory meatus) to the level of the sternal notch when seen from the side (sagiZal view)

� In poten3al cervical spine injury, head and neck manipula3on must NOT be performed. Manual in-‐line stabiliza3on should be used to minimize cervical spine mo3on.


RAPID SEQUENCE INTUBATION
� The induc3on of a state of unconsciousness with complete neuromuscular paralysis to achieve intuba3on without interposed mechanical ven3la3on in efforts to facilitate the procedure and minimize risks of gastric aspira3on

THE SIX P’S OF RAPID SEQUENCE INTUBATION � Prepara3on � Pre-‐oxygena3on � Pretreatment and induc3on � Paralysis � Placement of the tube � Post-‐intuba3on management

WHY WE DON’T DO RSI IN INTENSIVE CARE UNIT


� Hypotension � Hypoxia � Hyper-‐H+: Acidosis

� Hypotension § IV fluids § Pressors § Induc3on agents: Etomidate, Ketamine
� Hypoxia § Pre-‐oxygenate
� Hyper-‐H+: Acidosis § Bag mask and hyperven3late
� Seda3ve only intuba3on � Confirm that you can ven3late the pa3ent before you paralyze them

� Single center, prospec3ve observa3onal study � 664 intuba3ons in medical ICU � First aZempt success: OR 2.37


� No difference in rate of complica3ons

CONFIRMATION OF ENDOTRACHEAL TUBE � End 3dal CO2 detector � Clinical findings
§ Direct visualiza3on of the ET tube passing through the vocal cords
§ Bilateral breath sounds
§ absence of air movement during epigastric ausculta3on § Condensa3on (fogging) of water vapor in the tube on exhala3on
§ Maintenance of arterial oxygena3on
� Chest X-‐ray: the 3p of the ET tube should be between the carina and thoracic arc or approximately at the level of the aor3c arch § Doesn’t confirm endotracheal placement but used for posi3oning
� Ultrasound

END TIDAL CO2 DETECTOR
� EtCO2 detector § colorimetric § quan3ta3ve capnography
� Most accurate in non cardiac arrest � At least five exhala3ons with a consistent CO2 level § esophagus may yield small but detectable
amounts of CO2 during the first few posi3ve pressure ven3la3ons

DEPTH OF ENDOTRACHEAL TUBE
� Women: 20 to 21 cm from teeth � Men 22 to 23 cm from teeth
� 2 cms above carina