Scuola di Specializzazione in Medicina Interna - uniroma1.it · Scuola di Specializzazione in...
59
Direttore: Prof. Paolo Martelletti Scuola di Specializzazione in Medicina Interna Cronobiologia dell’emicrania Angela Koverech Esame V anno 28-06-2017
Transcript of Scuola di Specializzazione in Medicina Interna - uniroma1.it · Scuola di Specializzazione in...
Direttore: Prof. Paolo Martelletti
Scuola di Specializzazione in Medicina Interna
Cronobiologia dell’emicrania
Angela Koverech
Esame V anno28-06-2017
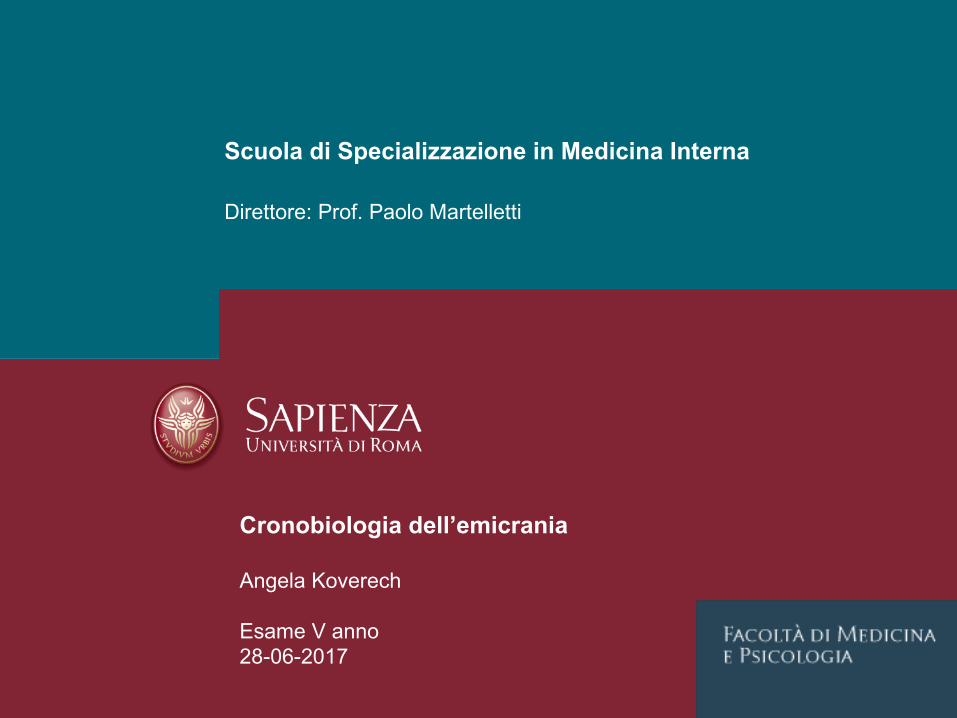
JensenR&StovnerLJ.Lancet2008
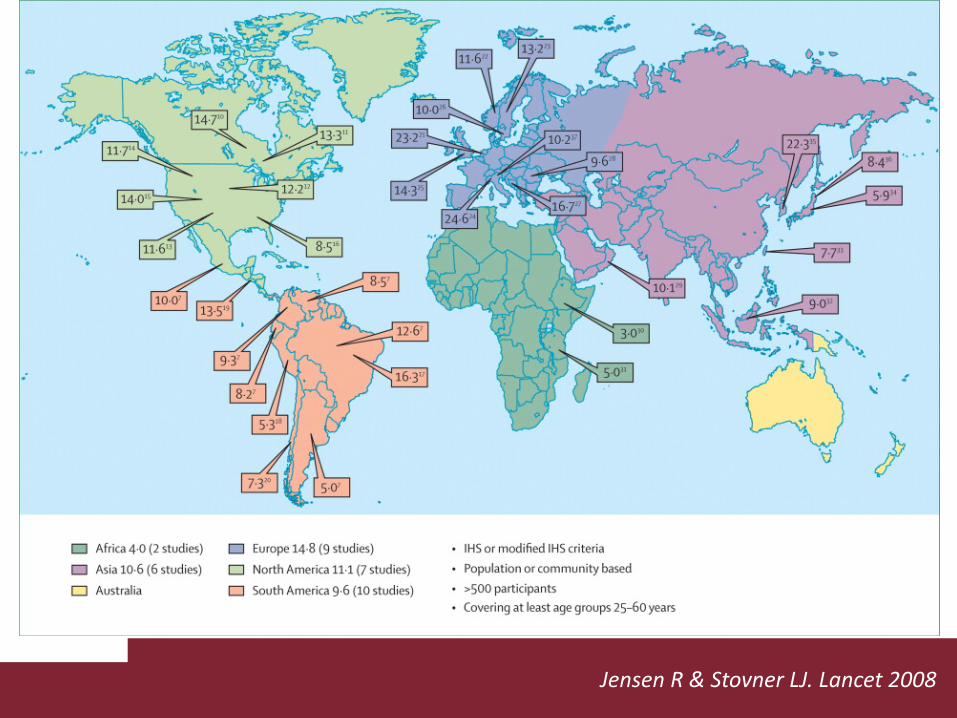
EpiCastReport:Migraine– EpidemiologyForecastto2023(2014)

JensenR&StovnerLJ.Lancet2008

BuseDCetal.Headache2012
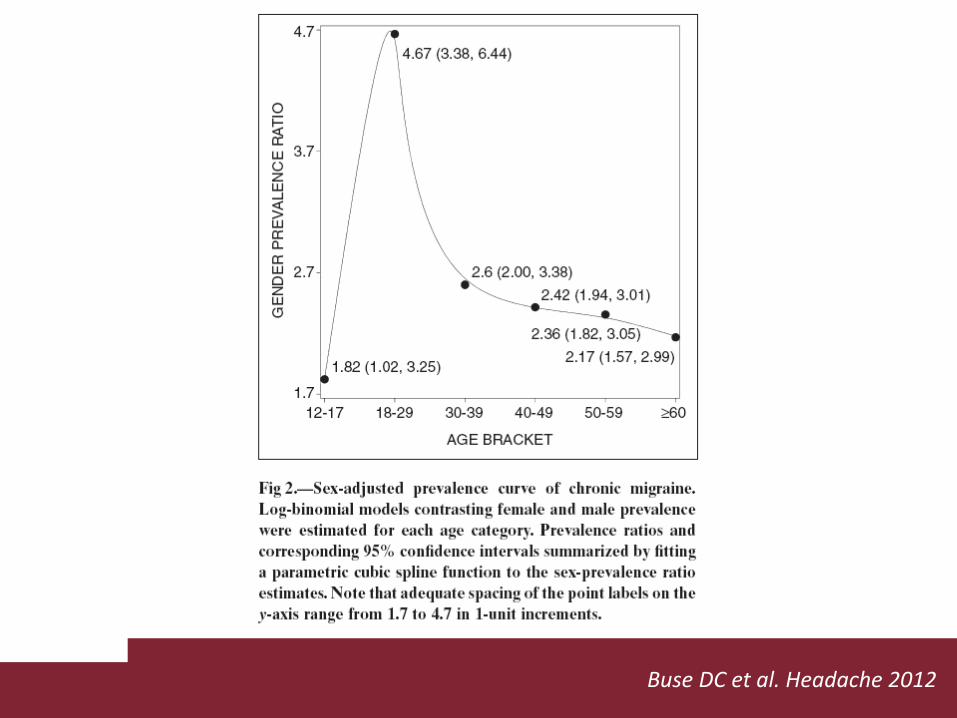
BuseDCetal.Headache2012


1.1 Migraine without auraPreviously used terms:Common migraine; hemicrania simplex.Description:Recurrent headache disorder manifesting in attacks lasting 4-72 hours. Typical characteristics of the headache are unilateral location, pulsating quality, moderate or severe intensity, aggravation by routine physical activity and association with nausea and/or photophobia and phonophobia.Diagnostic criteria:A. At least five attacks1 fulfilling criteria B-DB. Headache attacks lasting 4-72 hr (untreated or unsuccessfully treated)2;3
C. Headache has at least two of the following four characteristics:1. unilateral location2. pulsating quality3. moderate or severe pain intensity4. aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs)D. During headache at least one of the following:1. nausea and/or vomiting2. photophobia and phonophobiaE. Not better accounted for by another ICHD-3 diagnosis.

A1.1.1 Pure menstrual migraine without auraDiagnostic criteria:A. Attacks, in a menstruating woman1, fulfilling criteria for 1.1 Migraine without aura and criterion B belowB. Documented and prospectively-recorded evidence over at least three consecutive cycles has confirmed that attacks occur exclusively on day 1 ± 2 (ie, days −2 to +3)2 of menstruation1 in at least two out of three menstrual cycles and at no other times of the cycle.Notes:1. For the purposes of ICHD-3 (beta), menstruation is considered to be endometrial bleeding resulting from either the normal menstrual cycle or from the withdrawal of exogenous progestogens, as in the use of combined oral contraceptives or cyclical hormone replacement therapy.2. The first day of menstruation is day 1 and the preceding day is day −1; there is no day 0.

A1.1.2 Menstrually-related migraine without auraDiagnostic criteria:A. Attacks, in a menstruating woman1, fulfilling criteria for 1.1 Migraine without aura and criterion B belowB. Documented and prospectively-recorded evidence over at least three consecutive cycles has confirmed that attacks occur on day 1 ± 2 (ie, days −2 to +3)2 of menstruation1 in at least two out of three menstrual cycles, and additionally at other times of the cycle.Notes:1. For the purposes of ICHD-3 (beta), menstruation is considered to be endometrial bleeding resulting from either the normal menstrual cycle or from the withdrawal of exogenous progestogens, as in the use of combined oral contraceptives or cyclical hormone replacement therapy.2. The first day of menstruation is day 1 and the preceding day is day −1; there is no day 0.

CasoclinicoDonnadi48anni,BMI28,9DiagnosidiemicraniamenstruallyrelatedTerapiacon:Almogran12,5mg1cpincasodidolore
Nel2014 →perimenopausa→peggioramentodellasintomatologiaemicranica→comparsadiipertensionelieve140/90
Nel2015 →menopausa(12mesidiamenorrea)ecomparsadisintomi
Nel2016 →inizioHRT,aumentoponderale(BMI30,3)
Nel2017 →peggioramentoemicrania,chesipresentaciclicamente(ogni28±2gg),soprattuttoalrisveglio

Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinperi-menopausaemenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

RipaPetal.IntJWomenHealth2015
Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?Nonèinfrequentecheisintomidell’emicraniapeggiorinoconlamenopausa.
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

Gruber CJ et al. N Engl J Med 2002;346:340-352.
Ovarian Synthesis, Transport, and Metabolism of Estrogens.

Gruber CJ et al. N Engl J Med 2002;346:340-352.
Ligand-Dependent and Ligand-Independent Estrogen-Receptor Activation.

Gruber CJ et al. N Engl J Med 2002;346:340-352.
Classic Pathway of Estrogen Signal Transduction.

Gruber CJ et al. N Engl J Med 2002;346:340-352.
Effects of Estrogens in Different Organ Systems.

MacGregorEA.LancetNeurol2004
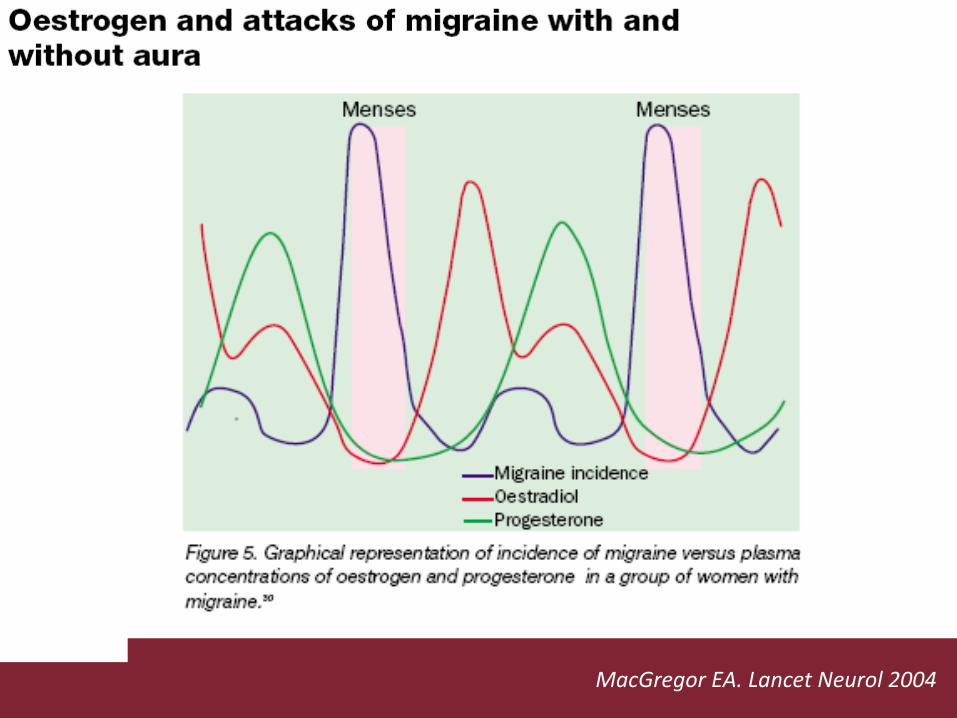
MacGregorEA.LancetNeurol2004

BorsookDetal.NeurobiolDis2014

BorsookDetal.NeurobiolDis2014

EbineTetal.NeurosciRes2016

GrassiSetal.Neuroscience2010

SantoroNetal.JClinEndocrinolMetab2017(epubaheadofprint)

SantoroNetal.JClinEndocrinolMetab2017(epubaheadofprint)
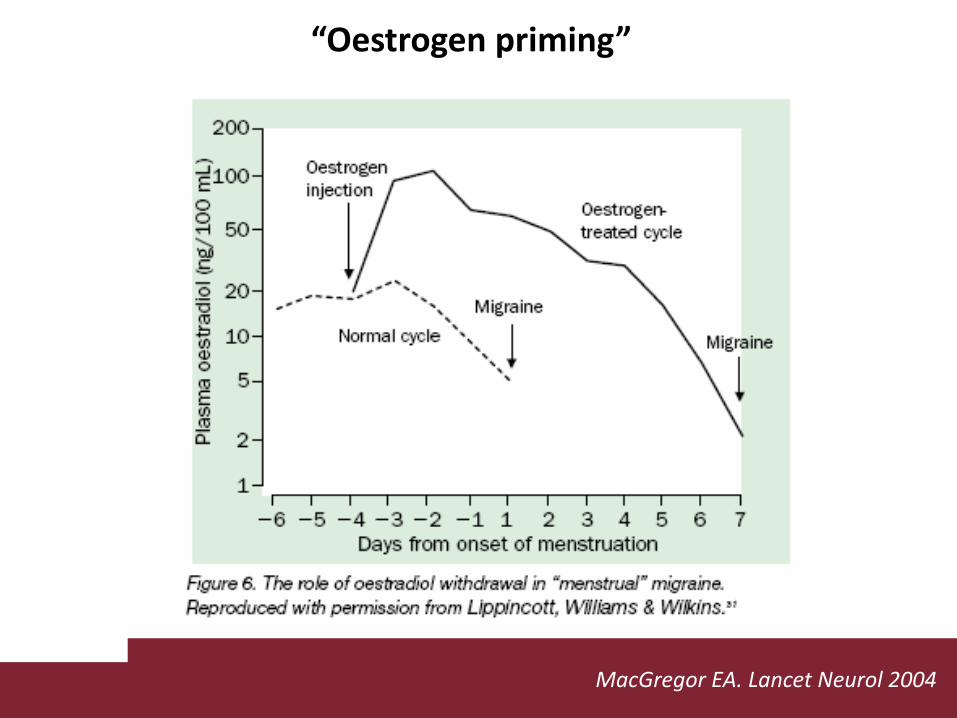
“Oestrogenpriming”
MacGregorEA.LancetNeurol2004

CasoclinicoQuesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?Ilcrolloelavariabilitàdelleconcentrazionicircolantidiestrogenidellafase,oraperimestruale,oraperimenopausale,contribuisconoall’aggravamentodegliattacchi.
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?
Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

LinYKetal.Medicine(Baltimore)2016
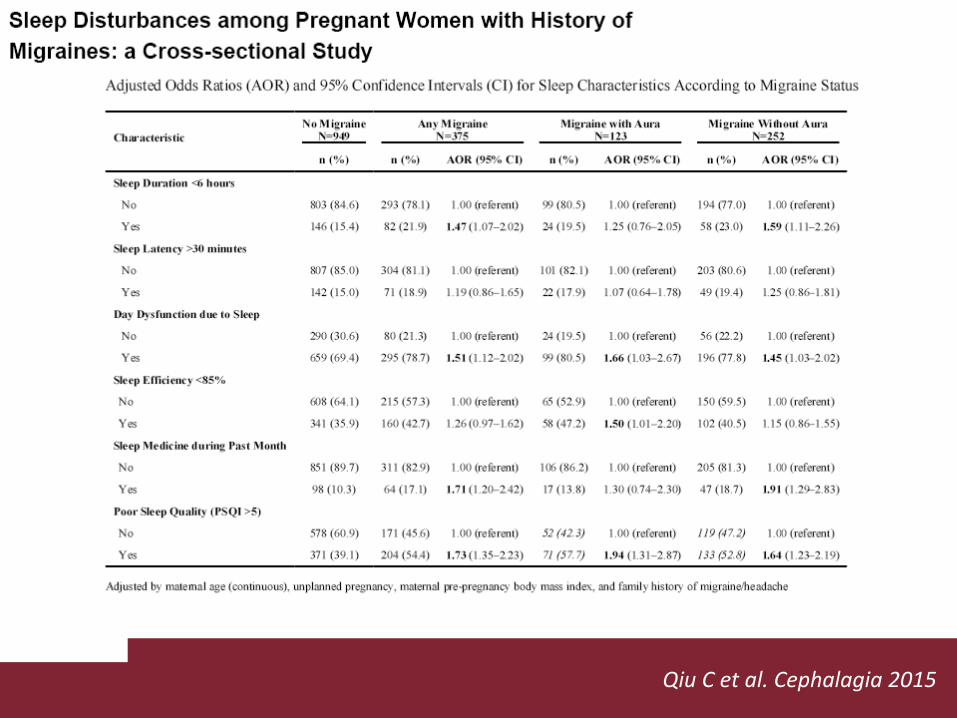
QiuCetal.Cephalagia2015
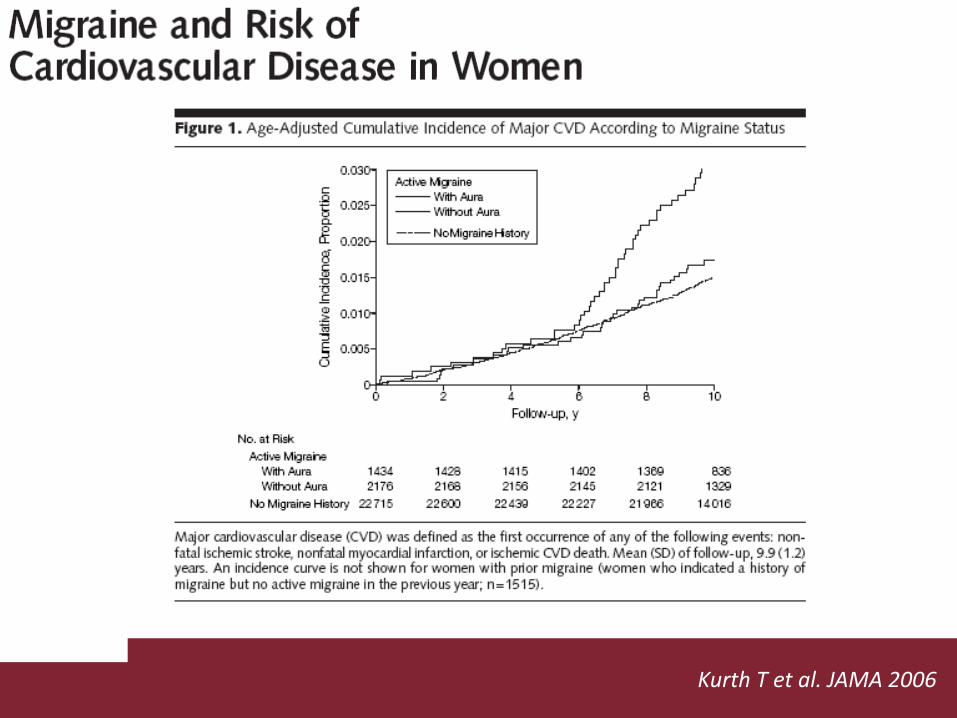
KurthTetal.JAMA2006

MateiDetal.EurRevMedPharmacolSci2015

Casoclinico
Quesiticlinici:1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?Conseguenzadell’aumentodellafrequenzadiattacchi,dell’usodellaHRTàsbilanciamentoautonomico→pressionearteriosa
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?
Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?


GradyD.NEnglJMed2006
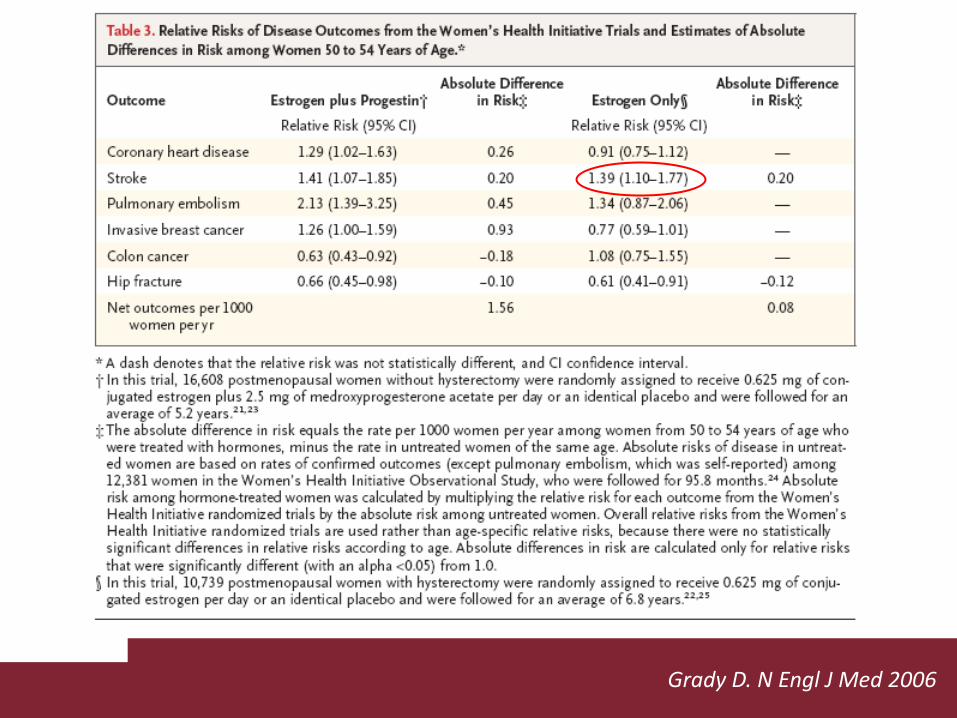
GradyD.NEnglJMed2006

LoboRA.NatRevEndocrinol2017

LoboRA.NatRevEndocrinol2017

LoboRA.NatRevEndocrinol2017

GradyD.NEnglJMed2006
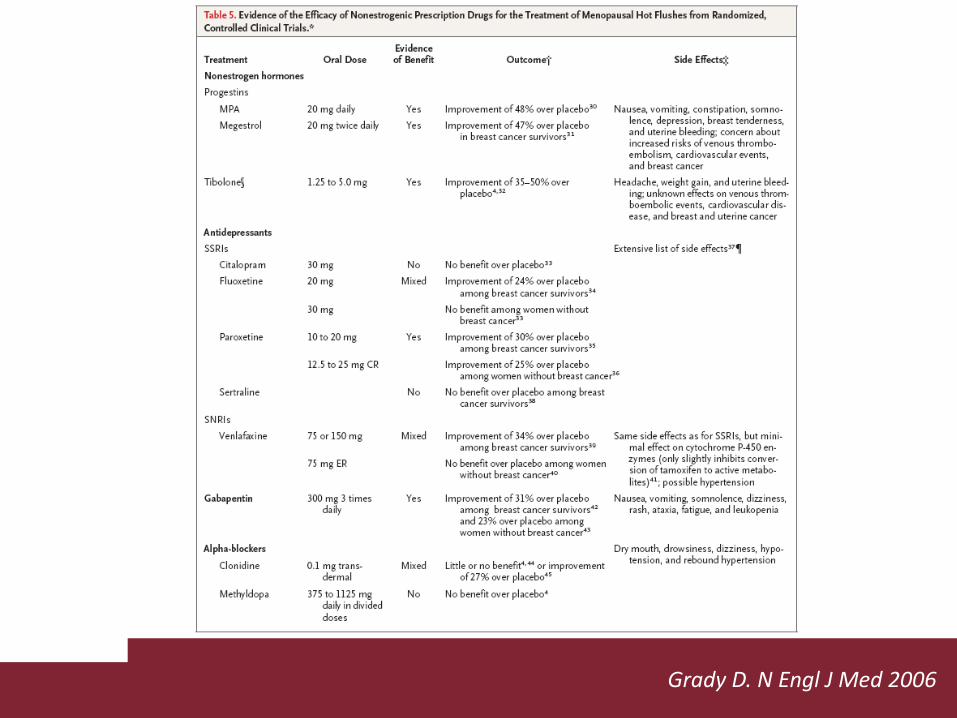
GradyD.NEnglJMed2006

ShusterLTetal.CurrNeurolNeurosciRep2011

ShusterLTetal.CurrNeurolNeurosciRep2011

ShusterLTetal.CurrNeurolNeurosciRep2011
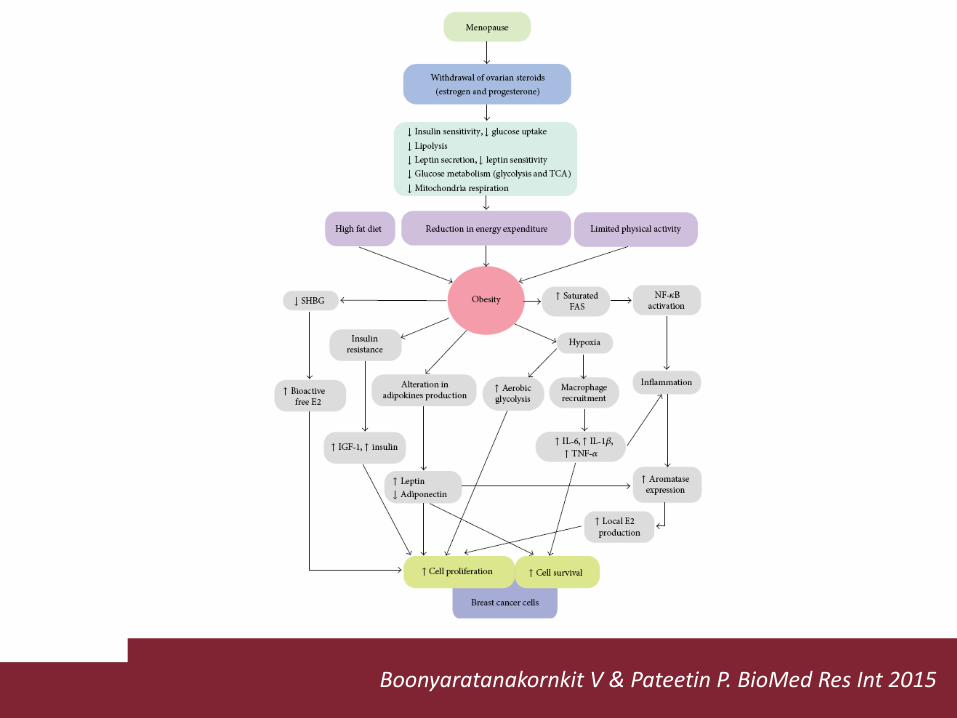
BoonyaratanakornkitV&PateetinP.BioMedResInt2015

Neurology. 2017Apr12.pii:10.1212/WNL.0000000000003919.doi:10.1212/WNL.0000000000003919.[Epubaheadofprint]Bodycompositionstatusandtheriskofmigraine:Ameta-analysis.GelayeB1, SaccoS1, BrownWJ1, NitchieHL1, OrnelloR1, PeterlinBL2.AuthorinformationAbstractOBJECTIVE:ToevaluatetheassociationbetweenmigraineandbodycompositionstatusasestimatedbasedonbodymassindexandWHOphysicalstatuscategories.METHODS:Systematicelectronicdatabasesearcheswereconductedforrelevantstudies.Twoindependentreviewersperformeddataextractionandqualityappraisal.Oddsratios(OR)andconfidenceintervals(CI)werepooledusingarandomeffectsmodel.Significantvalues,weightedeffectsizes,andtestsofhomogeneityofvariancewerecalculated.RESULTS:Atotalof12studies,encompassingdatafrom288,981uniqueparticipants,wereincluded.Theage- andsex-adjustedpooledriskofmigraineinthosewithobesitywasincreasedby27%comparedwiththoseofnormalweight(oddsratio[OR]1.27;95%confidenceinterval[CI]1.16-1.37, p <0.001)andremainedincreasedaftermultivariateadjustments.Althoughtheage- andsex-adjustedpooledmigraineriskwasincreasedinoverweightindividuals(OR1.08;95%CI1.04,1.12, p <0.001),significancewaslostaftermultivariateadjustments.Theage- andsex-adjustedpooledriskofmigraineinunderweightindividualswasmarginallyincreasedby13%comparedwiththoseofnormalweight(OR1.13;95%CI1.02,1.24, p <0.001)andremainedincreasedaftermultivariateadjustments.CONCLUSIONS:Thecurrentbodyofevidenceshowsthattheriskofmigraineisincreasedinobeseandunderweightindividuals.Studiesareneededtoconfirmwhetherinterventionsthatmodifyobesitystatusdecreasetheriskofmigraine.

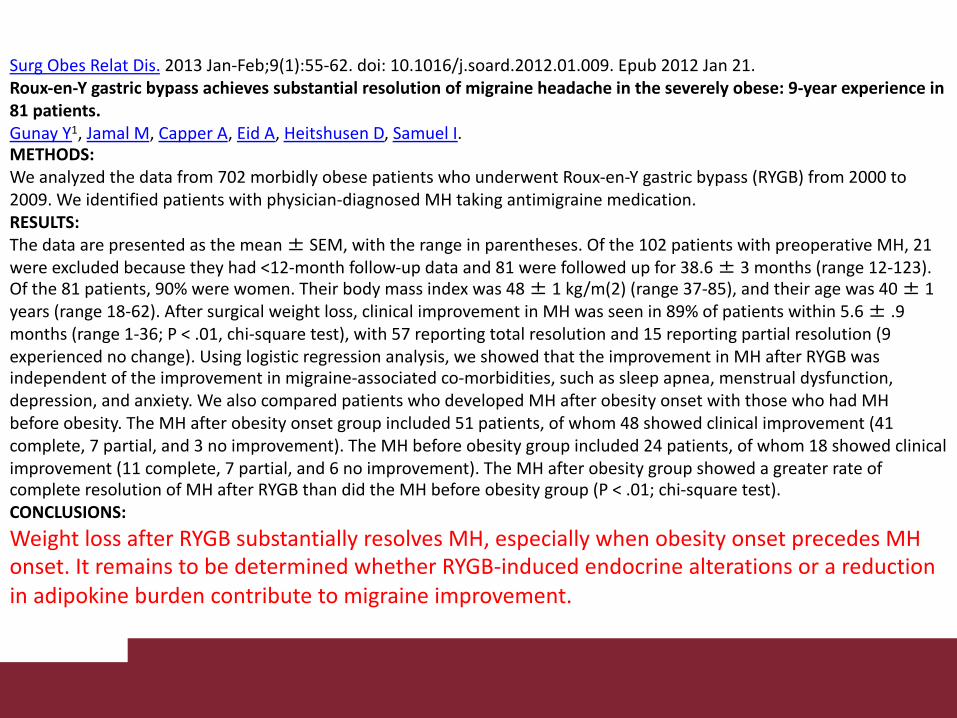
SurgObesRelatDis. 2013Jan-Feb;9(1):55-62.doi:10.1016/j.soard.2012.01.009.Epub2012Jan21.Roux-en-Ygastricbypassachievessubstantialresolutionof migraine headacheintheseverelyobese:9-yearexperiencein81patients.GunayY1, JamalM, CapperA, EidA, HeitshusenD, SamuelI.METHODS:Weanalyzedthedatafrom702morbidlyobesepatientswhounderwentRoux-en-Ygastricbypass(RYGB)from2000to2009.Weidentifiedpatientswithphysician-diagnosedMHtakingantimigrainemedication.RESULTS:Thedataarepresentedasthemean± SEM,withtherangeinparentheses.Ofthe102patientswithpreoperativeMH,21wereexcludedbecausetheyhad<12-monthfollow-updataand81werefollowedupfor38.6± 3months(range12-123).Ofthe81patients,90%werewomen.Theirbodymassindexwas48± 1kg/m(2)(range37-85),andtheiragewas40± 1years(range18-62).Aftersurgical weightloss,clinicalimprovementinMHwasseenin89%ofpatientswithin5.6± .9months(range1-36;P<.01,chi-squaretest),with57reportingtotalresolutionand15reportingpartialresolution(9experiencednochange).Usinglogisticregressionanalysis,weshowedthattheimprovementinMHafterRYGBwasindependentoftheimprovementin migraine-associatedco-morbidities,suchassleepapnea,menstrualdysfunction,depression,andanxiety.WealsocomparedpatientswhodevelopedMHafter obesity onsetwiththosewhohadMHbefore obesity.TheMHafter obesity onsetgroupincluded51patients,ofwhom48showedclinicalimprovement(41complete,7partial,and3noimprovement).TheMHbefore obesity groupincluded24patients,ofwhom18showedclinicalimprovement(11complete,7partial,and6noimprovement).TheMHafter obesity groupshowedagreaterrateofcompleteresolutionofMHafterRYGBthandidtheMHbefore obesity group(P<.01;chi-squaretest).CONCLUSIONS:Weightloss afterRYGBsubstantiallyresolvesMH,especiallywhen obesity onsetprecedesMHonset.ItremainstobedeterminedwhetherRYGB-inducedendocrinealterationsorareductioninadipokineburdencontributeto migraine improvement.

Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinrelatedmenopausa?
1.Qualisonoifattoricoinvolti?
2.Comeinterpretarelacomparsadiattacchinotturni?
3.QualeèilruolodellaHRT?AsecondadeltipodiHRT,possonopermanereinmenopausafluttuazioniormonalicheaggravanol’emicrania.Attenzioneallacomparsa/aggravamentodellaobesità.4.Qualistrategieterapeutichesipossonoadottare?

Casoclinico
Quesiticlinici:
1.E’riportatoilpeggioramentodellamenstruallyrelatedinmenopausa?
2.Qualisonoifattoricoinvolti?
3.Comeinterpretarelacomparsadiattacchinotturni?
4.QualeèilruolodellaHRT?
5.Qualistrategieterapeutichesipossonoadottare?

1. Mantenerelaattualeterapiaantiemicranica
2. PassareaHRTtransdermica
3. Altreterapieormonali(es.,tamoxifen,
danazolo,fitoestrogeni)emelatonina
4. Favorireilcaloponderale
5. Counsellingpsicologico
Loder E et al. Headache 2007Gelfand AA et al. Headache 2016



FrontiersinEndocrinology2015

SellixMT.FrontiersinEndocrinology2013