Innovazione Terapeutica - SIE · Obiettivi di riduzione del peso. Mantenimento della perdita di...
58
UNIVERSITÀ DI ROMA “TOR VERGATA” Dipartimento di Medicina dei Sistemi UOC di Medicina Interna Centro per la Cura dell’Obesità Policlinico Tor Vergata FONDAZIONE FONDAZIONE Innovazione Terapeutica nell’Obesità PAOLO SBRACCIA
Transcript of Innovazione Terapeutica - SIE · Obiettivi di riduzione del peso. Mantenimento della perdita di...

UNIVERSITÀ DI ROMA
“TOR VERGATA”Dipartimento di Medicina dei Sistemi
UOC di Medicina Interna
Centro per la Cura dell’Obesità
Policlinico Tor Vergata
FONDAZIONEFONDAZIONE
Innovazione Terapeutica
nell’Obesità
PAOLO SBRACCIA

Obiettivi di riduzione del peso. Mantenimento della perdita di peso. Contro-risposte fisiologiche al calo ponderale. Controllo ipotalamico del bilancio energetico,
regolazione omeostatica e ed edonicadell’appetito.
Determinanti dell’obesità. Nuovi farmaci disponibili sul mercato. Innovazione farmacologica futura. L’obesità è una malattia cronica che richiede un
trattamento cronico.
INDICE

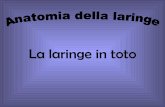
Natural historyof body weight
< 5 % weight lossMay reduce risk(Unsatisfactory)
Stable weight(Population Goal)
> 15 % weight losswith significnt riskreduction(Excellent)
Weightnormalization(Ideal but rare)
Bray G & Greenway F, Endo Rev, 1999
Years of Observation
20
Normal
>25
>30
Obese
BMI

Weight Loss Maintenance
Face-to-face
or web-basedIntervention
Diet
PhysicalActivity
Drugs
EducationalGroups
BariatricSurgery
WHAT MULTIDISCIPLINARY MEANS?
Cognitive Behavioural
Therapy

Mann et al. Am Psychol 2007
Weig
ht
chan
ge (
kg)
Anderson et al.
Fosteret al.
Graham et al.
Hensrudet al.
Jordanet al.
Krameret al.
Lantzet al.
Murphyet al.
Stalonaset al.
Waddenet al.
Walsh &Flynn
Wadden & Frey
Pekkarinen & Mustajoki
Stunkard & Penik
Mean change from baseline to end of diet (kg)
MAINTENANCE OF WEIGHT LOSS IS CHALLENGINGDiets Are Not the Answer?
Follow up range from 4 to 7 years
Mean change from baseline to follow-up (kg)
-30
-25
-20
-15
-10
-5
0
5

Knowler et al. Lancet 2009;374:1677–86
10-YEAR FOLLOW-UP OF DIABETES INCIDENCE AND WEIGHT LOSS IN THE DPP OUTCOMES STUDY
DietPhysicalActivity
EducationalGroups
Cognitive Behavioural
Therapy
CV EFFECTS OF INTENSIVE LIFESTYLE INTERVENTION IN T2DTHE LOOK AHEAD STUDY
The Look AHEAD Research Group, New Engl J Med, 2013
DietPhysicalActivity
EducationalGroups
Cognitive Behavioural
Therapy

WHAT IS THE DEFINITION OF WEIGHT LOSS MAINTENANCE?
Lifelong weight reduction!
Sjöström L, New Engl J Med 2004

Hunger Desire to
eat
Pancreas
Resting energy expenditure
Energy intake
Schwartz et al. Obes Rev 2010. Sumithran et al. N Engl J Med 2011
PHYSIOLOGICAL RESPONSES TO WEIGHT LOSS FAVOR WEIGHT REGAIN
GLP-1, CCK, PYY, GhrelinGut
Adipose tissue
Leptin
InsulinPancreas

Hypothalamic control of energy homeostasis
• AgRP, agouti-related peptide; CART, cocaine- and amphetamine-regulated transcript; LHA, lateral hypothalamic area; MC4R, melanocortin-4 receptor;α-MSH, α-melanocyte-stimulating hormone; NPY, neuropeptide Y; POMC, pro-opiomelanocortin; PVN, paraventricular nucleus
• Adapted from: Badman MK and Flier JS. Science 2005;307:1909–1914; Seo S et al. Endocr J 2008;55:867–874
Arcuate
POMC-MSHCART
PVN
Energy intake Energy expenditure
Adipose tissueMC4R
Peripheral signals
NPY/AgRP LHA
Energy intake Energy expenditure
Adipose tissue

Homeostatic regulation of appetite
• α-MSH, α-melanocyte stimulating hormone; AgRP, Agouti-related peptide; CART, cocaine- and amphetamine-regulated transcript; GLP-1, glucagon-like peptide-1; MC3/4R, melanocortin 3/4 receptor; NPY, neuropeptide Y; OXM, oxyntomodulin; POMC, pro-opiomelanocortin; PP, pancreatic polypeptide; PYY, peptide YY; Y1/Y5R, Y1/Y5 receptor
• Adapted from: Badman et al. Science 2005;307:1909–14; Seo et al. Endocr J 2008;55:867–74; Secher et al. J Clin Invest 2014;124:4473–88
Effectors
Hypothalamus
FeedingGastric emptyingMetabolic rate
Brainstem regions
Nucleus
tractus
solitarius
HungerSatietySecond-order neurons
MC3/4R Y1/Y5RAgRP
α-MSH
Arcuate nucleus First-order neurons
NPY/
AgRP
POMC/
CART
AppetiteAppetite
Area
postrema
Satiety peptides
Amylin GLP-1Vagal afferents
Satiety peptidesPYY GLP-1
PP OXM
Adiposity signalsLeptin Insulin
Hunger signalGhrelin

Homeostatic and hedonic
• Yu YH et al. Obes Rev 2015;16:234–247; Sorenson LB et al. Int J Obes Relat Metab Disord 2003;27:1152–1166
• Palatability
• Taste
• Texture
• Smell
• Genetics
• Epigenetics
Social factors Reward/pleasure
Food cuesEmotion
Homeostatic
signals

Obesity is a complex disease: Drivers of obesity
BMI, body mass index1. Sharma AM et al. Obes Rev 2010;11:362–370; 2. Chesi A et al. Trends Endocrinol Metab 2015;26:711–721
• Central nervous system pathways
– Hunger and reward
• Neuroendocrine signals– Long-term
– Short-term
• High heritability of body weight, especially at BMI extremes
• Genes in hypothalamus leptin-melanocortin pathway
• Single genetic mutations leading to obesity are rare, but variations in many genes may predispose to obesity
• Socio-cultural factors– Traditions, belief systems,
peer pressure
• Socio-economic factors– Education level
– Affordability of healthy food
• Food environment– Availability of inexpensive,
highly palatable food with high fat, sugar and salt content

MISMATCH EVOLUZIONISTICO
Daniel E. Lieberman, The story of the human body. Evolution, Health and Diseases, Pantheon Book, New York, 2013

2 yr re-randomisation trial shows need for continued drug use
Placebo Rim 20mg/Placebo Rim 20mg/20mg
Baseline mean (SD) 103.7 (21.1) Kg
- 7.9 kg
- 2.8 kg
0 8 16 24 32 40 48 56 64 72 80 88 96 104 LOCF
Weeks
-10
-8
-6
-4
-2
0
Wei
ght
chan
ge (
Kg)
(Mean ± SEM)
X. Pi-Sunyer, Circulation 2005:111(13);1727
- 2.8 kg

Wadden et al. N Engl J Med 2005
PHARMACOTHERAPY IN ADDITION TO DIET AND EXERCISE CAN HELP PATIENTS ACHIEVE CLINICALLY
RELEVANT WEIGHT LOSS
Lifestyle modification aloneSibutramine alone
Combined therapy
Sibutramine+ brief lifestyle modification
0
2
4
6
8
10
12
16
14
Weig
ht
loss (
kg)
Weeks0 3 6 10 18 40 52
+ Drugs

1. Obesity Drug Outcome Measures: A Consensus Report of Considerations Regarding Pharmacologic Intervention. Available at: http://sphhs.gwu.edu/pdf/releases/obesitydrugmeasures.pdf; 2. Jensen et al. Circulation 2014;129(25 Suppl 2):S102–38; 3. Courcoulas et al. JAMA 2013;310:2416–25; 4. LABS consortium. N Engl J Med 2009;361:445–54
Treatment options for people with obesity
Lifestyle modification
Gastric band
Gastric bypass
Pharmacotherapy plus lifestyle modification
0% 3% 8% 32%16%
Percent weight loss
“A treatment gap exists for those patients who do not respond sufficiently to behavioural and lifestyleinterventions and who are not viable candidates for, or do not wish to undergo, bariatric surgery. Such patientsneed additional options for treatment. Used appropriately, effective prescription drugs could potentially help fillthat gap”1.

FDA Drugs: http://www.fda.gov/Drugs/default.htm; EMA Medicines: http://www.ema.europa.eu/
Orlistat(Xenical®/Alli®)
PhenterminePhentermine/ Topiramate
(Qsymia®)
Lorcaserin(Belviq®)
Naltrexone / bupropion
(Mysimba®, Contrave®)
Liraglutide3.0 mg
(Saxenda®)
Status (EU)Approved
(Rx and OTC)Not approved Rejected Rejected Approved Approved
Status (US)Approved
(Rx and OTC)
Only approved for short term
useApproved Approved Approved Approved
Mechanismof action
Lipase inhibitor
Noradrenaline and dopamine/
serotoninreuptake inhibitor
Noradrenaline and dopamine/
serotoninreuptake inhibitor
Selective 5HT2c receptor
agonist
Noradrenaline and dopamine
reuptake inhibitor/µ-
opioid receptor antagonist
GLP-1 receptoragonist
Indications
Adjunct to diet for obesity, including weight loss and maintenance
Adjunct to diet and physical activity for chronic weight management in a) obese BMI≥30 and b) overweight BMI≥27 with comorbidity
A limited number of pharmacological treatment options are currently available

Naltrexone – Bupropione


EFFECT OF NALTREXONE PLUS BUPROPION ON WEIGHT LOSS IN OVERWEIGHT AND OBESE ADULTS
(COR-I TRIAL)
Greenway et al, Lancet 2010
%

Effect of Naltrexone-Bupropion on Major AdverseCardiovascular Events in Overweight and Obese Patients
With Cardiovascular Risk Factors
Nissen et al, JAMA 2016

Effect of Naltrexone-Bupropion on Major AdverseCardiovascular Events in Overweight and Obese Patients
With Cardiovascular Risk Factors
Nissen et al, JAMA 2016

COMMON ADVERSE REACTIONS REPORTED WITH NALTREXONE/BUPROPION
Adverse ReactionNB
N=2545PlaceboN=1515
Nausea 32.5 6.7
Constipation 19.2 7.2
Headache 17.6 10.4
Vomiting 10.7 2.9
Dizziness 9.9 3.4
Insomnia 9.2 5.9
Dry mouth 8.1 2.3
Diarrhea 7.1 5.2
*Adverse events occurring in greater than 5% of patients are shownData from Integrated Primary Data Set. Source: US Package Insert for CONTRAVE.

CONTROINDICAZIONI
• History of bipolar disorder.• Uncontrolled hypertension.• Seizure disorders.• Anorexia nervosa or bulimia.• Drug or alcohol withdrawal.• MAO inhibitors.• Current dependency on chronic opioids or opiate
agonists, or opiate withdrawal.

DOSAGGIO1 cp: Naltrexone SR/Bupropion SR, 8 mg/90 mg

Liraglutide

ArcuateNucleus
POMC/CART
NPY/AgRP
NPY/AgRPHunger
POMC/CARTSatiety
Liraglutide
Secher A, et al. J Clin Invest 2014;124:4473-88
AgRP, Agouti-related protein
CART, cocaine and amphetamine-regulated transcript
NPY, Neuropeptide Y
POMC, pro-opiomelanocortin
+ -
LIRAGLUTIDE EFFECTS ON HYPOTHALAMIC NEURONS INVOLVED IN APPETITE REGULATION

THE ARCUATE NUCLEUS MEDIATES GLP-1 RECEPTOR AGONIST LIRAGLUTIDE-DEPENDENT WEIGHT LOSS
Secher et al, J Clin Invest, 2014
Normal mice
GLP-1R -/- mice
Fluorescently labeledliraglutide in the mouse brain
GLP-1 caused membrane depolarization and increased firing rate of spontaneous action potentials in POMC/CART cells
• GLP-1R expression
– Absent on NPY/AgRP
– Present on POMC/CART

Liraglutide is not approved for weight management outside Canada, EU and US
*P<0.05 compared with saline treatment, same genotype unless otherwise indicated
Adapted from: Sisley et al. J Clin Invest 2014;124:2456–63
Body w
eig
ht
change (
%)
5
0
-5
-10
Saline Liraglutide
* *
Brain GLP-1 receptors mediate the body weight lowering effect of liraglutide
Peripheral nervous system GLP-1R-/-
Brain GLP-1R-/-
Control

Liraglutide is not approved for weight management outside Canada, EU and US
GLP-1 mediated regulation of GABAergic effects on POMC neurons
IPSC frequency (%) from voltage clamp recordings of POMC neurons showed an increased GABAergic IPSC frequency in the presence of GLP-1(7-36)amide. GLP-1, glucagon-like peptide-1; IPSC, inhibitory postsynaptic current; POMC, pro-opiomelanocortin; GABAergic, gamma-aminobutyric acid-ergic; GLP-1(7-36)amide, glucagon-like peptide-1(7-36)amide
10007505002500-250
100
200
300
400
Time (s)
Norm
alised I
PSC
frequency (
%)
Secher et al. J Clin Invest 2014;124:4473–88
GABA
Arcuate nucleus
GLP-1R
NPY POMC
+
?
GLP-1R ?
+
+
–

Liraglutide Modulates Appetite and Body Weight ThroughGlucagon-Like Peptide 1 Receptor–Expressing
Glutamatergic Neurons
Adams et al, Diabetes, 2018
Saline-Lira Saline-Lira Saline-Lira
(GABAERGIC) (GLUTAMATERGIC)

Hedonic Regulation of Appetite is Another Important Aspect of Food Intake
Billes SK, et al Pharmacol Res 2014;84:1–11
Prefrontal cortex
AmyAmigdala
V ralTVentral Tegmental Area
Hypothalamus (homeostatic regulation))
Substantia Nigra
Nucleus Accumbens
Striatum
Am gdala

The y-axis represents effect size of the activation (z scores). Blood oxygen level-dependent contrasts are superimposed on a T1 structural image inneurological orientation. The colour bar represents voxel T value
Farr et al. Diabetologia 2016;59:954-65
Liraglutide 1.8 mg decreased activation of the: Parietal cortex in response to highly desirable food images
Insula and putamen, areas involved in the reward system
0.5
0.3
0.1
-0.1
-0.3
-0.5
Left
insula
0.5
0.3
0.1
-0.1
-0.3
-0.7
Puta
men
-0.5
Liraglutide 1.8 mg
Placebo

Liraglutide 3.0 mgn=212
Placebon=210
SCALE Maintenance (1923) 3
Liraglutide 3.0 mgn=180
Placebon=179
SCALE Sleep Apnea (3970) 4
SCALE Obesity and Prediabetes (1839) 1
Liraglutide 3.0 mgn=423
Placebon=212
Liraglutide 1.8 mg n=211
SCALE Diabetes (1922) 2
Liraglutide 3.0 mg n=2487
Placebo n=1244
Weight management in type 2 diabetes
Weight management & delayed onset of diabetes
Prevention ofweight regain
Effect of liraglutide in subjects with obesity and moderate to severe OSA
SCALE Phase 3a Clinical Trial ProgramSCALE, Satiety and Clinical Adiposity Liraglutide Evidence in non-diabetic and diabetic individuals
OSA, Obstructive Sleep Apnea
1. Pi-Sunyer X, et al. NEJM 2015;373:11-22; 2. Davies MJ, et al. JAMA 2015;314:687-99; 3. Wadden TA, et al. Int J Obes 2013;37:1443-51, 4. Blackman A, et al. Int J Obes 2016;40:1310-9

Baseline Characteristics of the Patients
Pi-Sunyer et al. , New Engl J Med, 2015
SCALE Obesity and Prediabetes
61.2% had prediabetes

Inclusion criteria:• BMI: ≥30 kg/m2, or
≥27 kg/m2 + comorbidities*
• Stable body weight, and preceding failed dietary effort
0.6 mg
1.2 mg
1.8 mg
2.4 mg
Trial design
16040–2Week
Screening
Liraglutide 3.0 mg/day
Placebo
Randomisation2:1 (lira:pbo)
Dose escalation
56
EOS
68
Liraglutide 3.0 mg/day
Placebo
Liraglutide 3.0 mg/day
Placebo
Withoutprediabetes
With Prediabetes
0.6 mg
1.2 mg
1.8 mg
2.4 mgObservational
follow-up
172
Re-randomisation1:1 EOS**
*Treated or untreated hypertension or dyslipidaemia according to ATP-III; **Treatment ends at week 68 for the population without prediabetes and is followed by an off-treatment follow-up period of 2 weeks. EOS end of study; EOT, end of treatment. NN8022-1839 3yr data. ClinicalTrials.gov Identifier: NCT01272219. Pi-Sunyer et al. NEJM 2015;373:11–22
All arms included lifestyle intervention: −500 kcal/day hypocaloric diet + 150 min./week increased physical activity
Obs. follow-
up
70
EOT

Liraglutide is not approved for weight management outside Canada, EU and US
Mean weight loss (%) from baseline to week 56Change in w
eig
ht
(%)
Week
-12
-10
-8
-6
-4
-2
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
FAS, fasting visit data only. Line graphs are observed means (±SE). Circles are observed means LOCF. Statistical analysis is ANCOVA. FAS, full analysis set; LOCF, last observation carried forward; SE, standard error.
-8.0%
-2.6%
p<0.0001
Pi-Sunyer et al. , New Engl J Med, 2015
Liraglutide 3.0 mgObserved mean LOCF
PlaceboObserved mean LOCF
SCALE Obesity and Prediabetes

Liraglutide is not approved for weight management outside Canada, EU and US
Cumulative distribution of changes in body weight after 56 weeks of treatment
Weight change (%)
Liraglutide 3.0 mg Placebo
0
20
40
60
80
100
-45 -40 -35 -30 -25 -20 -15 -10 -5 0 5 10 15 20
63%
33%
14%
92%
100
80
60
40
20
0
65%
27%
11%
4%
Pro
po
rti
on
of
ind
ivid
uals
(%
)
Pi-Sunyer X, et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. NEJM 2015;373:11-22

Inclusion criteria:• BMI: ≥30 kg/m2, or
≥27 kg/m2 + comorbidities*
• Stable body weight, and preceding failed dietary effort
Trial design
16040–2Week
Screening
Placebo
Randomisation2:1 (lira:pbo)
Dose escalation
56
EOS
68
Liraglutide 3.0 mg/day
With Prediabetes
0.6 mg
1.2 mg
1.8 mg
2.4 mgObservational
follow-up
172
Re-randomisation1:1 EOS**
All arms included lifestyle intervention: −500 kcal/day hypocaloric diet + 150 min./week increased physical activity
70
EOT
le Roux CW et al. Lancet 2017 (Published Online 22 February 2017). DOI: http://dx.doi.org/10.1016/S0140-6736(17)30069–7.
Liraglutide 3.0 mg: WL and progression to T2DSCALE Obesity and Prediabetes: 3 years

-12
-10
-8
-6
-4
-2
0
0 16 28 40 56 68 80 92 104 116 128 140 152 160 172
Liraglutide 3.0 mg: WL and progression to T2DSCALE Obesity and Prediabetes: 3 years
le Roux CW et al. Lancet 2017 (Published Online 22 February 2017). DOI: http://dx.doi.org/10.1016/S0140-6736(17)30069–7.
Full analysis set, fasting-visit data only. Line graphs are observed means (±SE).
-2.1%
-5.2%
Change in w
eig
ht
(%)
Off-drug follow-up Off-drug follow-up
Liraglutide 3.0 mg Placebo
Week
-7.1%
-2.7%
0
2
4
6
8
10
12
0 16 32 48 64 80 96 112 128 144 160
Part
icip
ants
(%
)
80% risk reduction47
31
172
46
26
*Derived from the primary Weibull analysis. ETD, estimated treatment difference; LOCF, last observation carried forward; SCALE, Satiety and Clinical Adiposity –Liraglutide Evidence in individuals with and without diabetes; SE, standard error; T2D, type 2 diabetes; WL, weight loss.
Week
Full analysis set. Numbers in the figure correspond to the accumulated number of diagnosed participants.
-9.2%
-3.5%

Liraglutide is not approved for weight management outside Canada, EU and US
Adverse events reported in ≥5% of participants0–56 weeks
Liraglutide 3.0 mg%
Placebo%
20.0 8.7
9.5 3.1
Constipation
Dyspepsia
40.2 14.7Nausea
10.8 3.1Decreased appetite16.3 4.1Vomiting
20.9 9.3Diarrhoea
5.2 3.55.7 3.5
Abdominal painAbdominal pain upper
% of subjects
0 10 20 30 40 50
17.2 18.8Nasopharyngitis8.6 9.8Upper respiratory tract infection
5.2 5.95.8 5.3
SinusitisInfluenza
13.2 12.4Headache
6.7 4.87.5 5.2
DizzinessFatigue
11.9 3.3Hypoglycaemia
5.0 5.75.7 7.56.9 8.5
ArthralgiaInjection site haematomaBack pain
Liraglutide 3.0 mg Placebo
Safety analysis set
Pi-Sunyer et al. , New Engl J Med, 2015

Liraglutide is not approved for weight management outside Canada, EU and US
• Safety profile was generally consistent with that of previous clinical trials with liraglutide 3.0 mg1,2 and liraglutide 1.8 mg in individuals with T2D3
• Liraglutide 3.0 mg was generally well tolerated; nausea, diarrhoea and constipation were the most commonly reported adverse events
• Incidence of gallbladder disorders and acute pancreatitis was low, but more frequent with liraglutide 3.0 mg:
• Gallbladder disorders: 2.5 vs. 1.0 events/100 PYE (n=54 vs. 9)*
• Acute pancreatitis: 0.3 vs. 0.1 events/100 PYE (n=7 vs. 1)†
• Acute pancreatitis: no consistent mode of presentation or latency period, majority mild according to revised Atlanta criteria
Overall summary and conclusions (2/2)SCALE Obesity and Prediabetes
Pi-Sunyer et al. , New Engl J Med, 2015

Liraglutide is not approved for weight management outside Canada, EU and US
• Gallbladder-related adverse events and events of confirmed acute pancreatitis were low, but more frequent with liraglutide 3.0 mg vs. placebo
Gallbladder and pancreatic safety
PYO, patient years of observation
le Roux et al. Obesity Week 2015, 2–6 November 2015, Poster T-P-LB-3843
Liraglutide 3.0 mg Placebo
2.9
0.29
1.2
0.13
0
1
2
3
4
5
Gallbladder-related events Acute pancreatitis events
Events
per
100 P
YO

0,0
0,5
1,0
1,5
2,0
2,5
3,0
1. Novo Nordisk Briefing Document: Liraglutide 3.0 mg for weight management NDA 206-321; 2. FDA Endocrinologic and Metabolic Drugs Advisory Committee Meeting September 11, 2014
Data are from the NN8022-1839, -1922, -3970, -1923, -1807 and -1807-ext-1 trials. Full analysis set; last observation carried forward at end of trial; mean*Events of cholecystitis and cholecystitis acute, grouped as cholecystitis%, percentages based on total n; n, number of participants; WG, weight gain; WL, weight loss
• The incidence is higher in liraglutide 3.0 mg vs placebo at any given weight-loss category1,2
• Weight-loss independent factors in addition to weight loss per se with liraglutide involved1,2
Gallbladder-related events across weight-loss categories
Cholelithiasis
Liraglutide 3.0 mgPlacebo
n=
WG 0–4.9 5–9.9 ≥10
WL (%)
291 1020 958 1031 665 763 297 165
WG 0–4.9 5–9.9 ≥10
WL (%)
Pro
port
ion o
f part
icip
ants
(%
)

0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8 5 4 6 0
0 .0
0 .1
0 .2
0 .3
0 .4
0 .5
0 .6
Time to acute pancreatitis in the LEADER trial
Steinberg et al. Diabetes Care 2017;40:966–972
Full analysis set. Kaplan–Meier plot of time to first EAC-confirmed acute pancreatitis index event. Hazard ratio calculated using Cox analysisCI, confidence interval; EAC, event adjudication committee; HR, hazard ratio; NS, non-significant
Pati
en
ts w
ith
an
even
t (%
)
Subjects at risk
Liraglutide 4668 4641 4596 4554 4496 4434 4369 4309 1719 483 10
Placebo 4672 4644 4595 4537 4471 4394 4321 4250 1699 464 15
Placebo
Liraglutide 1.8 mg
HR: 0.78(95% CI: 0.42 ; 1.44); p=NS
Time since randomisation (months)
Liraglutide 1.8 mg is not approved for weight management

Liraglutide is not approved for weight management outside Canada, EU and US
Early responders, individuals who achieved ≥5% weight loss from baseline at 16 weeks; early non-responders, individuals who achieved <5% weight loss from baseline at 16 weeks.Week 56 completers, FAS, fasting visit data only. Line graphs are observed means (±95% CI). CI, confidence interval; FAS, full analysis set
Week
Change in w
eig
ht
(%)
-12
-10
-8
-6
-4
-2
0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
−11.5%
−3.8%
−3.6%
−9.3%
Early non-responders
SCALE Obesity and Prediabetes
Early responders
SCALE Diabetes
Blüher et al. IDF 2015. 30 November–4 December 2015, Vancouver, Canada. Poster 0208-P.
Change in body weight for early responders and non-respondersBaseline to week 56
5% stopping rule

47
31
0
2
4
6
8
10
12
0 16 32 48 64 80 96 112 128 144 160
le Roux et al. Lancet 2017;389:1399–1409
Full analysis set. Numbers in the figure correspond to the accumulated number of diagnosed participantsT2D, type 2 diabetes
Time course for incident T2DSCALE Obesity and Prediabetes – Kaplan–Meier plot: 0–160 weeks
504
205
Week160
1472 1313 1204 1135 1060 977 910 830 799863738 636 569 523 468 422 376 328 310350
n=
n=776
296
172
46
26
Liraglutide 3.0 mg Placebo
Part
icip
ants
(%
)
Placebo: 11%Liraglutide 3.0 mg: 3%
3-year data from SCALE Obesity and Prediabetes are only included in the labels in the EU, US and Canada
LEADER: MACE analysis – primary outcomeCV death, non-fatal myocardial infarction or non-fatal stroke
Marso et al. N Engl J Med 2016;375:311–322
The primary composite outcome in the time-to-event analysis was the first occurrence of death from CV causes, non-fatal myocardial infarction or non-fatal stroke. The cumulative incidences were estimated with the use of the Kaplan–Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MACE, major adverse cardiovascular events
0 6 18 24 30 36 42 48 540
5
10
15
20
12
HR: 0.87(95% CI: 0.78 ; 0.97)
p<0.001 for non-inferiorityp=0.01 for superiority
Time from randomisation (months)
Liraglutide 1.8 mgPlacebo
4668
4672
4593
4588
4496
4473
4400
4352
4280
4237
4172
4123
4072
4010
3982
3914
1562
1543
424
407
Patients at riskLiraglutide
Placebo
Patients
with a
n e
vent
(%)
Liraglutide 1.8 mg is not approved for weight management
Liraglutide is not approved for weight management outside Canada, EU and US
30
35
40
45
50
55
-2 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32
Change in AHI (events/h)0–32 weeks
AH
I (e
vents
/h)
Week
FAS. Line graphs are observed means (±SE). Circles are observed means LOCF. Statistical analysis is ANCOVA. AHI, apnoea–hypopnoea index, FAS, full analysis set; LOCF, last observation carried forward; SE, standard error
36.8
44.0
p=0.0150
Blackman et al., Int J Obes, 2016
LOCF week 32
Liraglutide 3.0 mg
Placebo
LOCF week 32
SCALE Sleep Apnoea
Liraglutide safety and efficacy in patients with NASH (LEAN):
a multicentre, double-blind, randomizedplacebo-controlled phase 2 study
Armstrong MJ et al., Lancet, 2015
ALT GT
Nine (39%) of 23 patients who received liraglutide and underwent end-of-treatment liver biopsy had resolution of defi nite non-alcoholicsteatohepatitis compared with two (9%) of 22 such patients in the placebogroup (relative risk 4∙3 [95% CI 1∙0–17∙7]; p=0∙019).

PIPELINES



Velneperit: Neuropeptide Y5 receptor inhibitor, appetite suppression, Phase II
Successful proof-of-concept study butdiscontinued from development after little weight loss.

Other drugs in development stages:
central hypothalamic pathways (e.g. RM-493, amelanocortin type 4 receptor agonist – Setmelanotide-, Tesofensine)
peripheral metabolism (e.g. Beloranib, increases fatoxidation), Phase III trial aborted in December 2015 after 2ndreported patient death in Prader-Willi trial.
inhibitors of intestinal fat absorbtion: Cetilistat

PEPTIDI MULTIFUNZIONALI

Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised,
placebo-controlled and active comparator-controlled phase 2 trial
Frias et al, Lancet, 2018

Efficacy and safety of semaglutide compared with liraglutide for weight loss in patients with obesity
O’Neil et al, Lancet, 2018


1. Obesity Drug Outcome Measures: A Consensus Report of Considerations Regarding Pharmacologic Intervention. Available at: http://sphhs.gwu.edu/pdf/releases/obesitydrugmeasures.pdf; 2. Jensen et al. Circulation 2014;129(25 Suppl 2):S102–38; 3. Courcoulas et al. JAMA 2013;310:2416–25; 4. LABS consortium. N Engl J Med 2009;361:445–54
Treatment options for people with obesity
Lifestyle modification
Gastric band
Gastric bypass
Pharmacotherapy plus lifestyle modification
0% 3% 8% 32%16%
Percent weight loss
“A treatment gap exists for those patients who do not respond sufficiently to behavioural and lifestyleinterventions and who are not viable candidates for, or do not wish to undergo, bariatric surgery. Such patientsneed additional options for treatment. Used appropriately, effective prescription drugs could potentially help fillthat gap”1.

Natural historyof body weight
< 5 % weight lossMay reduce risk(Unsatisfactory)
Stable weight(Population Goal)
> 15 % weight losswith significnt riskreduction(Excellent)
Weightnormalization(Ideal but rare)
Bray G & Greenway F, Endo Rev, 1999
Years of Observation
20
Normal
>25
>30
Obese
BMI
Weightnormalization