Convegno annuale fondazione Rosa Gallo Il CANCRO DEL...
30
D. Cenzi Imaging: indagini routinarie o personalizzate? Verona, 23 Novembre 2010 Azienda Integrata Ospedaliera-Universitaria Ospedale Civile Maggiore – U.O. di Radiologia Direttore: Dr.ssa Stefania Montemezzi Convegno annuale fondazione Rosa Gallo Il CANCRO DEL RETTO OGGI: ATTUALITA’ DIAGNOSTICHE E TERAPEUTICHE
Transcript of Convegno annuale fondazione Rosa Gallo Il CANCRO DEL...

D. Cenzi
Imaging: indagini routinarie
o personalizzate?
Verona, 23 Novembre 2010
Azienda Integrata Ospedaliera-Universitaria
Ospedale Civile Maggiore – U.O. di Radiologia
Direttore: Dr.ssa Stefania Montemezzi
Convegno annuale fondazione Rosa Gallo
Il CANCRO DEL RETTO OGGI:
ATTUALITA’ DIAGNOSTICHE E TERAPEUTICHE

Quesiti all’Imaging
• Bilancio loco-regionale di malattia
• Ristadiazione post-trattamento
neoadiuvante (“downstaging”)
• Stadiazione a distanza
• Follow up

Blomqvist L, Glimelius B, Acta Oncol 2008
Valutazione pre-operatoria

Retto superiore 20%
Retto inferiore 35%
Retto medio 45%
• Diffusione radiale della neoplasia (T)
• Rapporti con il mesoretto (CRM e fascia
mesorettale)
• Rapporti con il piano muscolare sfinteriale
• Invasione vascolare peritumorale
• Stato dei linfonodi loco-regionali
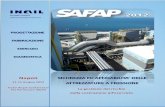
Bilancio loco-regionale

Diffusione radiale
Courtesy Minicozzi A.
• Accuratezza EUS: 69-97%
• Accuratezza TC multislice: 83%
• Accuratezza RM: 67-86%
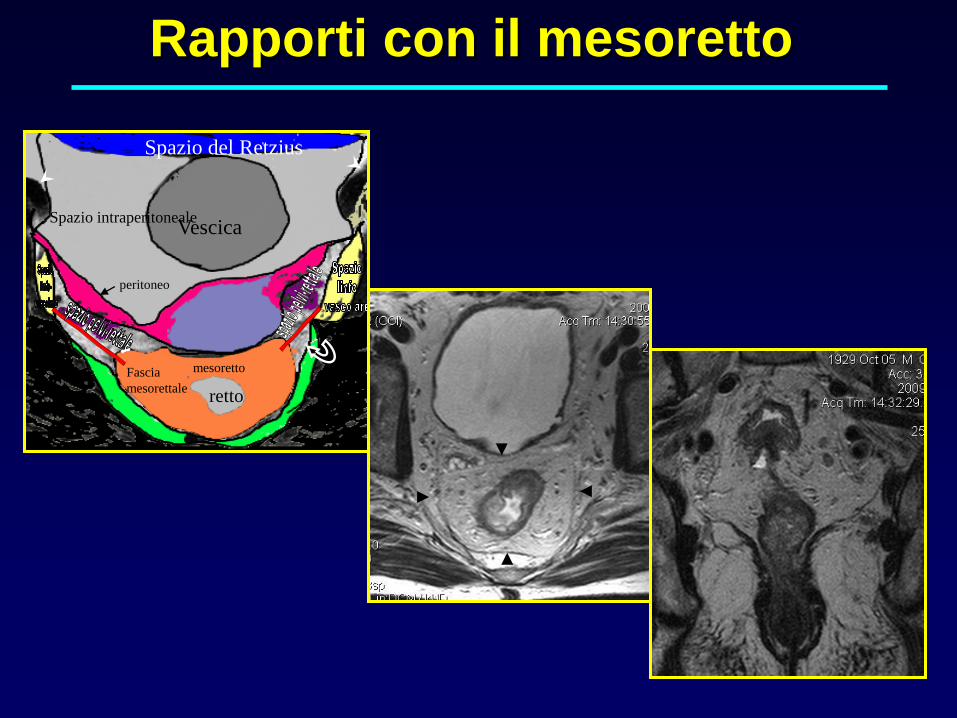
Spazio del Retzius
Vescica
mesoretto
retto
Spazio intraperitoneale
peritoneo
Fascia
mesorettale
Rapporti con il mesoretto
Il CRM
“ It is thought to be a cut-off distance of 6 mm
between a tumor and the mesorectal fascia. This
criterion was highly accurate in predicting CRM
involvement. A distance of at least 5 mm between a
tumor and the mesorectal fascia at MR imaging helped
predict an uninvolved CRM of 1 mm at histologic
analysis with 97% confidence. ”
Beet-Tan et al., Radiology 2004

Rapporti con il piano muscolare
“Phased array MRI is accurate in measuring the
distance between the anorectal junction and the distal
part of the tumour; it is also accurate for determining the
length of the tumour. Both endorectal MRI and phased
array MRI are reliable in assessing sphincter infiltration.
EUS is the preferred method but when it is
not available the external phased array technique is
recommended over an endoanal coil MR technique
because it is easier for the patient to tolerate.”EURECA-CC2, Radiotherapy and Oncology 2009
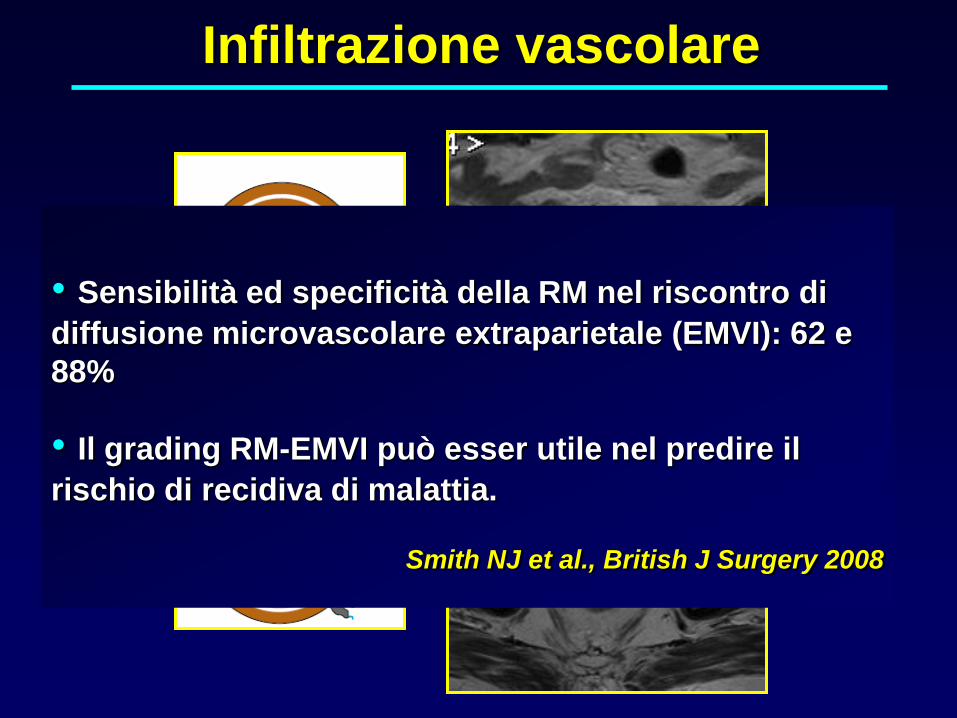
Infiltrazione vascolare
• Sensibilità ed specificità della RM nel riscontro di
diffusione microvascolare extraparietale (EMVI): 62 e
88%
• Il grading RM-EMVI può esser utile nel predire il
rischio di recidiva di malattia.
Smith NJ et al., British J Surgery 2008
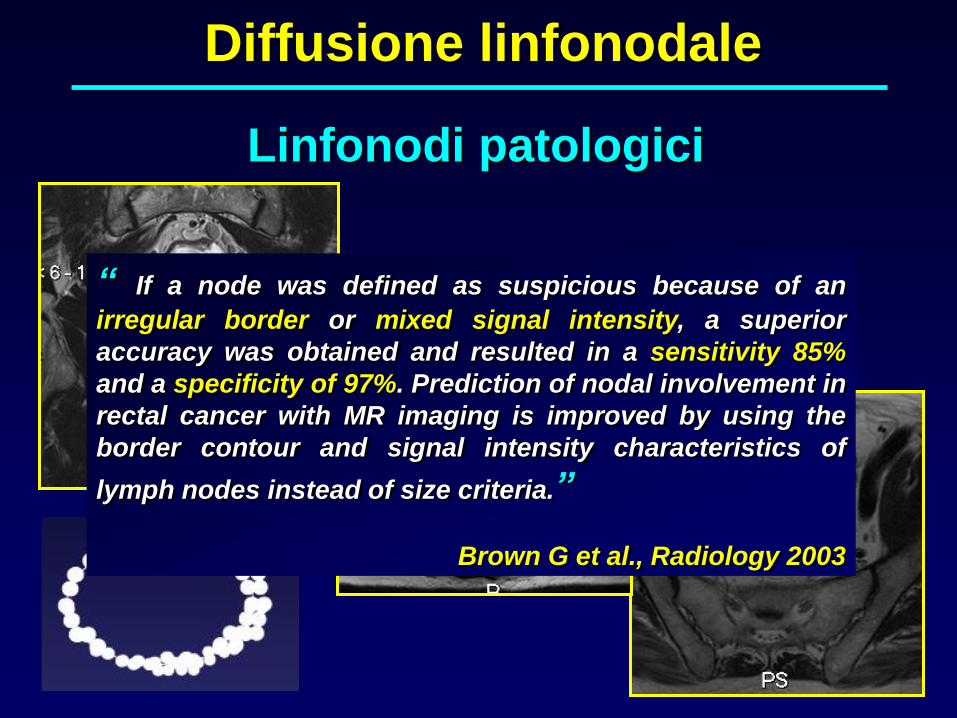
Linfonodi patologici
“ If a node was defined as suspicious because of an
irregular border or mixed signal intensity, a superior
accuracy was obtained and resulted in a sensitivity 85%
and a specificity of 97%. Prediction of nodal involvement in
rectal cancer with MR imaging is improved by using the
border contour and signal intensity characteristics of
lymph nodes instead of size criteria.”
Brown G et al., Radiology 2003
Diffusione linfonodale

Downstaging post-CRT
• Residuo di malattia
• Distinzione fibrosi post-trattamento
• Grado 1: completa regressione; non residuo tumorale; fibrosi.
• Grado 2: rare cellule neoplastiche residue o piccoli aggregati cellulari neoplastici.
• Grado 3: ampie aree di regressione con fibrosi e necrosi frammiste a grandi aggregati neoplastici residui.
• Grado 4: residuo tumorale con alcune aree di regrassione neoplastica.
• Grade 5: tumore residuo senza elementi di regressione.
Grading (TRG) secondo Dwork

Downstaging post-trattamento
neoadiuvante
Courtesy D. Rubello - G. Grassetto

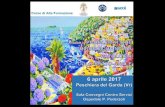
Down-staging post-CRT
T3d
T3c
Rivalutazione del CRM
• Buona accuratezza (83-89%) nella
ridefinizione dei rapporti con CRM
Kim DJ et al., Radiographics 2010
• FDG PET-CT:
- 55% dei residui tumorali sono sottostadiati come T0
• RM:
- 75-100% delle risposte complete sono sovrastadiate
Chen et al, Dis Colon Rectum 2005
Kuo et al, Dis Colon Rectum 2005
Maretto et al, Annal Surg Oncol 2007
Kulkarni et al, Colorectal Disease 2008
Capirci et al, Biomed Pharmacother 2004
Kristiansen et al, Dis Colon Rectum 2008
Guerra L et al., Abdom Imaging 2009
Downstaging post-trattamento
neoadiuvante

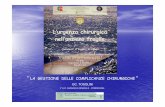
Down-staging post-CRT
Risposta al trattamento
T3
T1-T2pT0
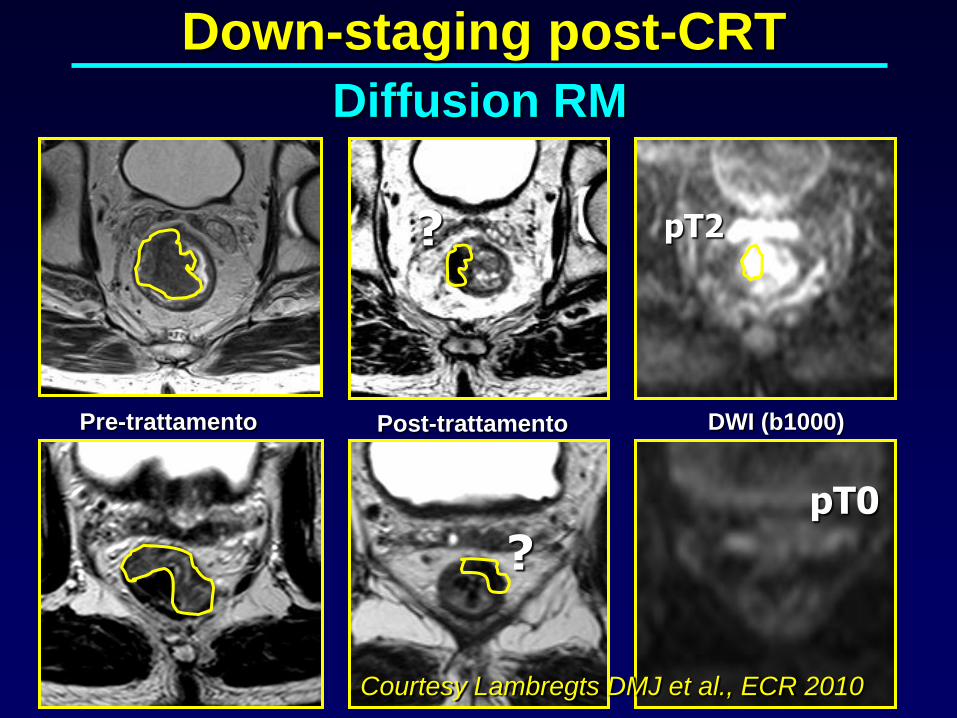
Pre-trattamento Post-trattamento DWI (b1000)
pT2?
?pT0
Courtesy Lambregts DMJ et al., ECR 2010
Down-staging post-CRT
Diffusion RM
Follow up
• Riscontro di metastasi a distanza
• Recidiva locale di malattia
TC
Accuratezza complessiva: 87%
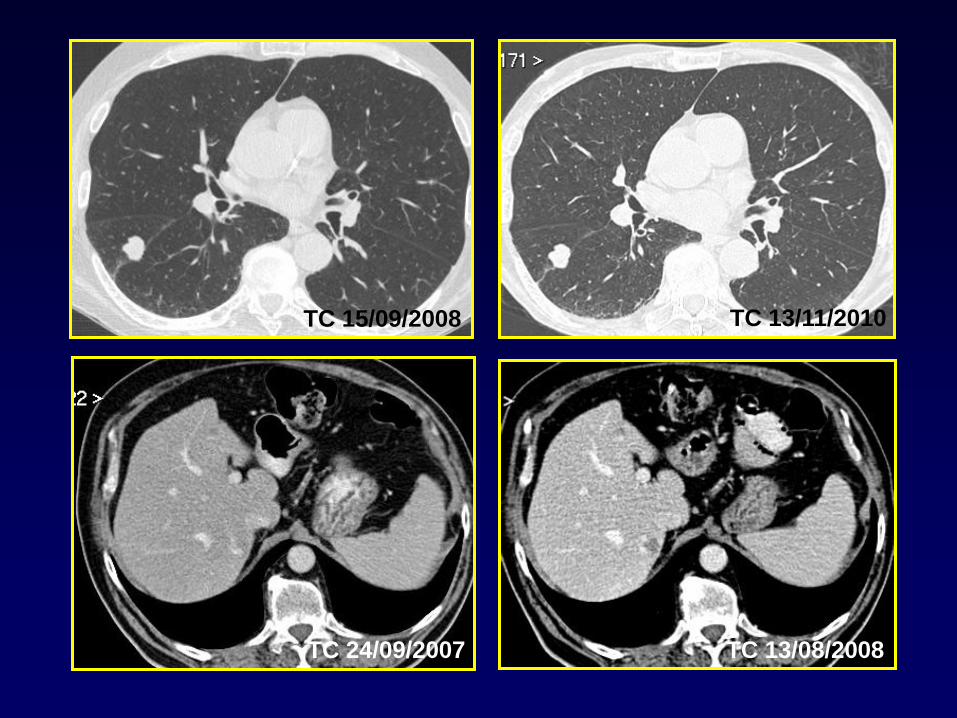
TC 13/08/2008
TC 15/09/2008 TC 13/11/2010
TC 24/09/2007

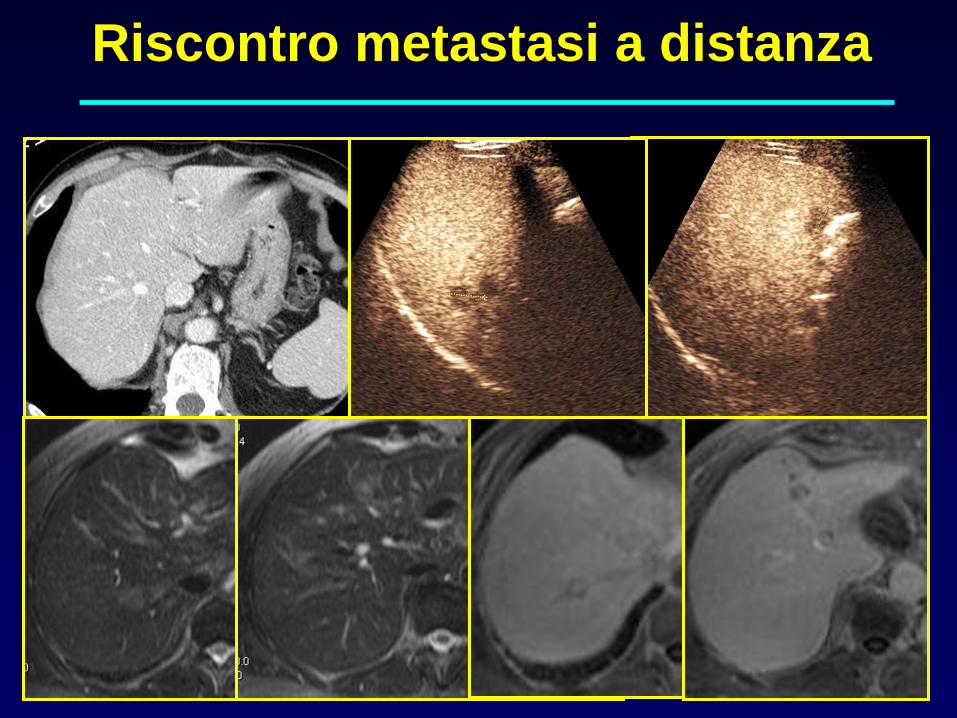
Riscontro metastasi a distanza
• TC
• RM e CEUS
• TC-PET e RM-PET
• Whole Body RM e Diffusion RM
Metodiche “a la carte”
“ CT, MRI and PET/CT have proven to be accurate in
the follow up rectal cancer. On the other hand, a debate
exists on which imaging procedure should be part of
an evidence-based surveillance program. ”
Schaefer O and Langer M., Eur Radiology 2007

Courtesy D. Rubello - G. Grassetto
Riscontro metastasi a distanza
Riscontro metastasi a distanza
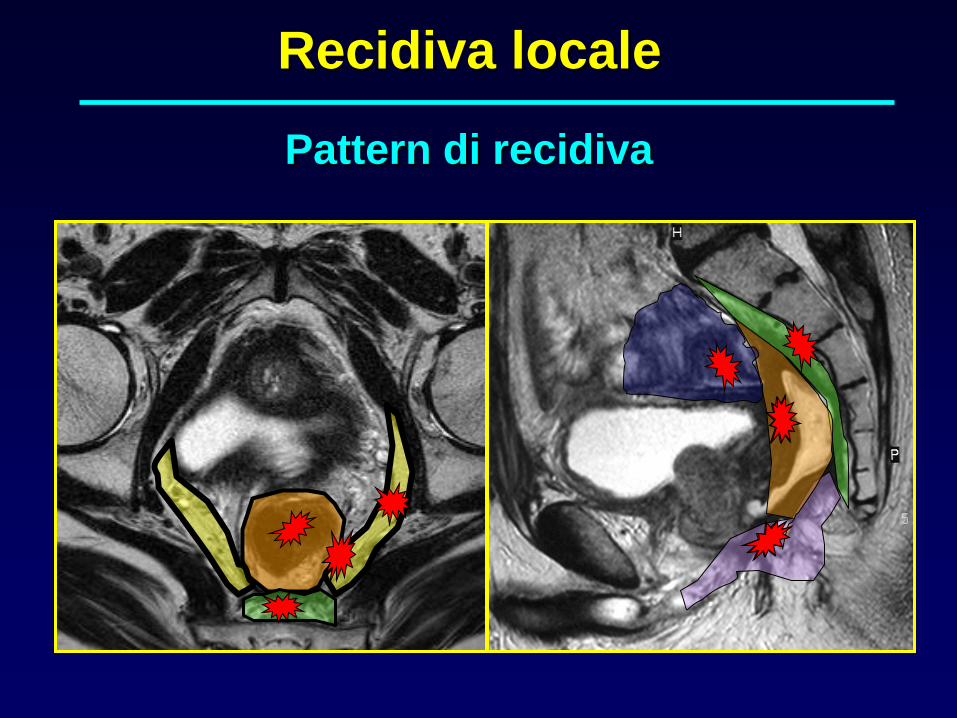
Recidiva locale
Pattern di recidiva

Operabile?
• Compartimento centrale
• Compartimento anteriore
inferiore alla riflessione
peritoneale
• Compartimento posteriore
inferiormente a S2
• Perineale
Pattern di recidiva
• Compartimento laterale
• Infiltrazione nervo
sciatico
• Infiltrazione sacrale di
S1-S2
• Perforazione peritoneale
TC 13/08/2008
TC 24/09/2007
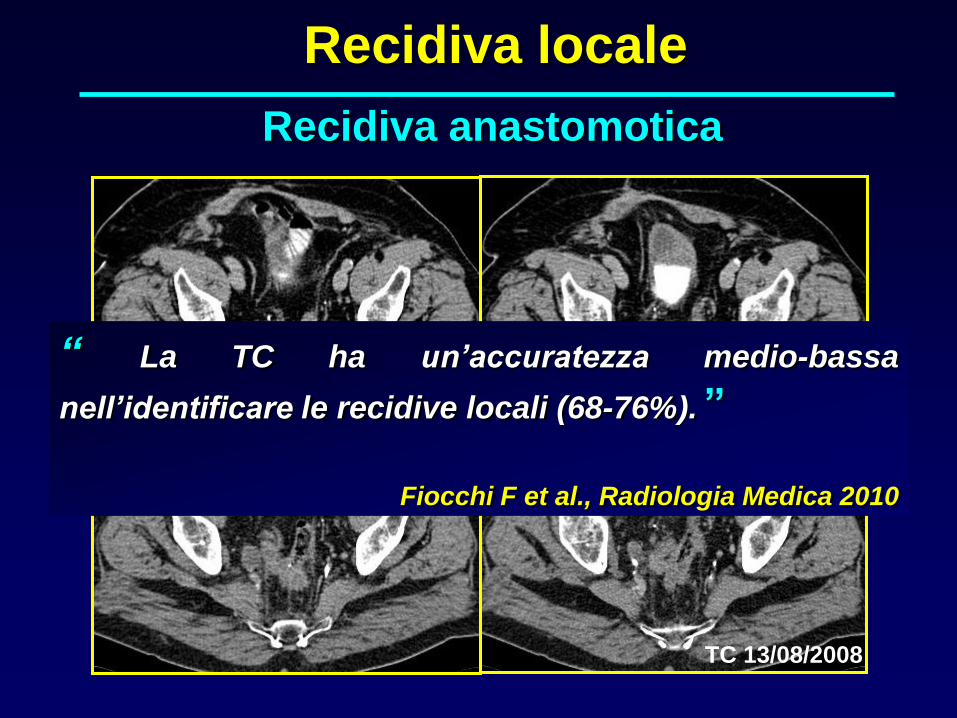
Recidiva locale
Recidiva anastomotica
“ La TC ha un’accuratezza medio-bassa
nell’identificare le recidive locali (68-76%). ”
Fiocchi F et al., Radiologia Medica 2010
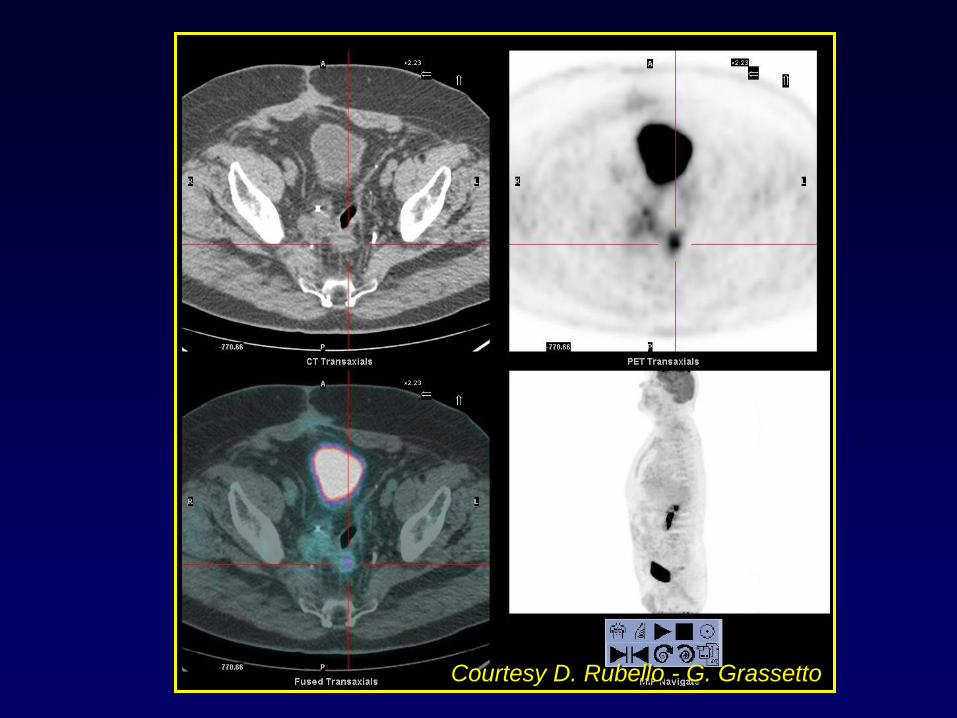
Courtesy D. Rubello - G. Grassetto
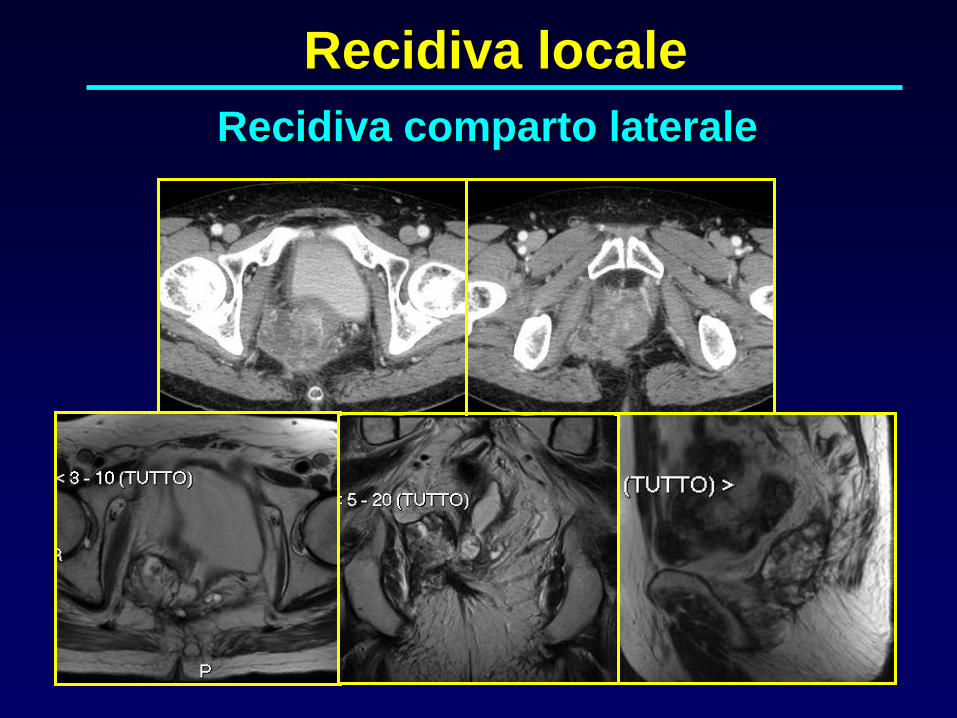
Recidiva locale
Recidiva comparto laterale
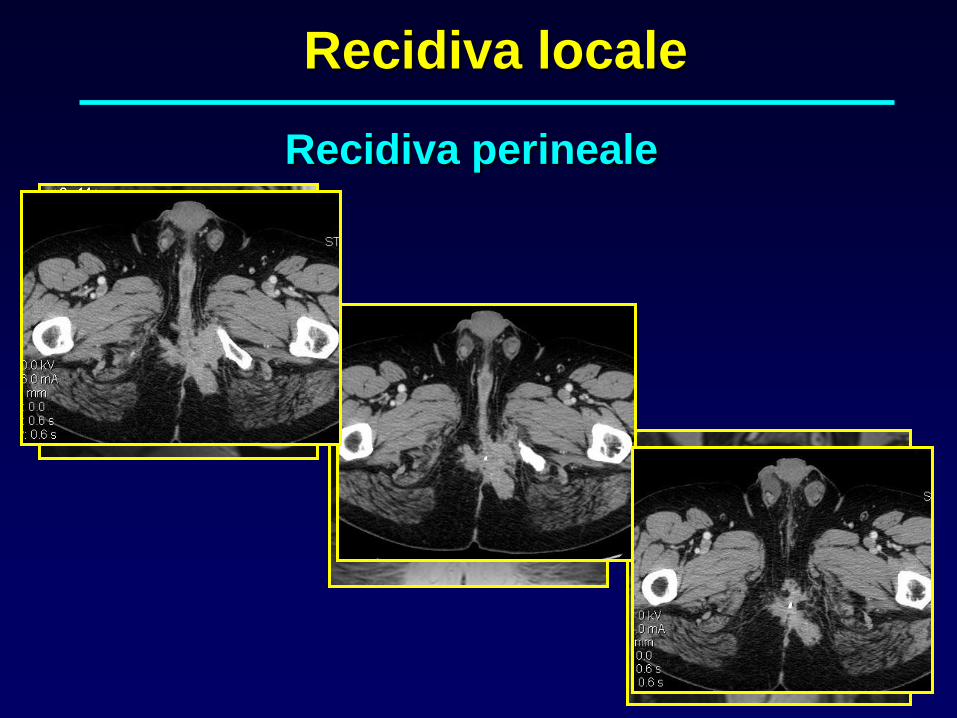
Recidiva locale
Recidiva perineale

Recidiva locale
Recidiva comparto postero-laterale

Confronto con TC precedenti
RM positiva - CEA elevato
Sospetto di
recidiva locale
RM pelvi per definire la recidiva
locale
RM positiva - CEA normale
Diagnosi di recidiva:
è resecabile?
FDG-PET TC
Follow up: che fare?
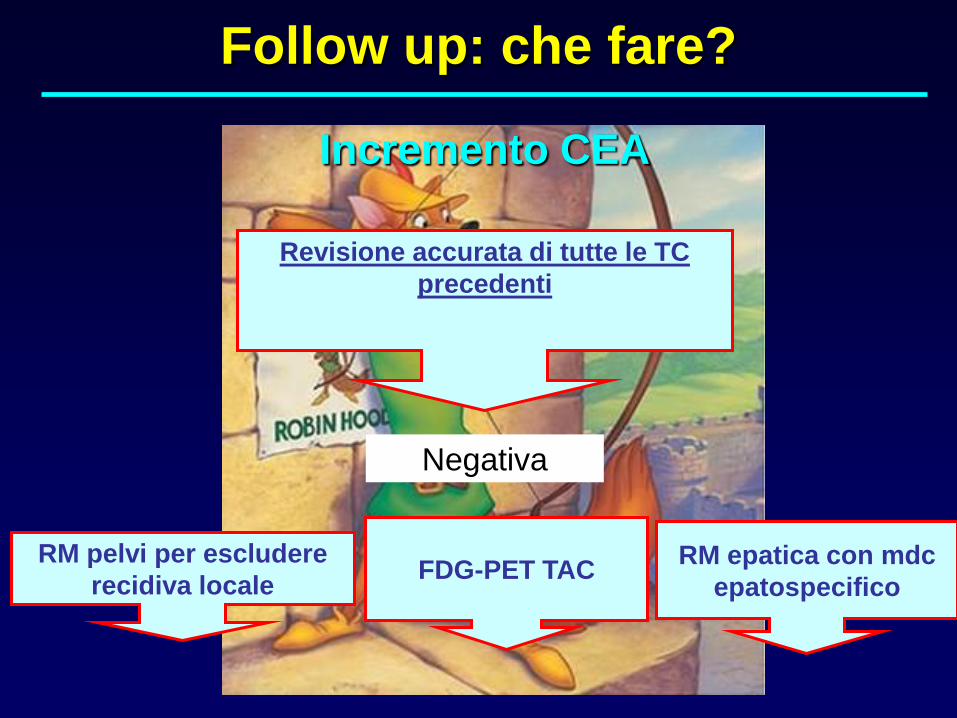
Incremento CEA
Revisione accurata di tutte le TC
precedenti
FDG-PET TAC
Negativa
RM pelvi per escludere
recidiva localeRM epatica con mdc
epatospecifico
Follow up: che fare?