Giuseppe Micieli Dip. Neurologia dUrgenza IRCCS Istituto Neurologico C Mondino Pavia Manifestazioni...
39
Giuseppe Micieli Dip. Neurologia d’Urgenza IRCCS Istituto Neurologico C Mondino Pavia Manifestazioni cliniche di sanguinamento: Manifestazioni cliniche di sanguinamento: Il sanguinamento Il sanguinamento cerebrovascolare cerebrovascolare
-
Upload
fiorella-manfredi -
Category
Documents
-
view
215 -
download
0
Transcript of Giuseppe Micieli Dip. Neurologia dUrgenza IRCCS Istituto Neurologico C Mondino Pavia Manifestazioni...

Giuseppe MicieliDip. Neurologia d’Urgenza
IRCCS Istituto Neurologico C MondinoPavia
Manifestazioni cliniche di sanguinamento:Manifestazioni cliniche di sanguinamento: Il sanguinamento Il sanguinamento cerebrovascolarecerebrovascolare

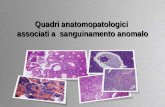
Cerebrovascular DiseaseCerebrovascular DiseaseStroke SubtypesStroke Subtypes
Albers GW et al. Chest. 1998;114:683S-698S.Rosamond WD et al. Stroke. 1999;30:736-743.
Ischemic stroke (83%)Hemorrhagic stroke (17%)
Atherothromboticdisease (20%)
Embolism (20%)
Lacunar small vessel disease (25%)
Cryptogenic (30%)
Intracerebralhemorrhage (59%)
SAH (41%)

Possible causes of spontaneous Possible causes of spontaneous nontraumatic ICHnontraumatic ICH
• Hypertension• Hematologic disorders
– Thrombocytopenia– Platelet dysfunction– Coagulopathies
• Blood vessel abnormalities– Arteriovenus malformation– Aneurism– Moyamoya disease– Amyloid angiopathy
• Tumors– Primary brain tumor (much
less common than metastatic tumor)
– Metastatic brain tumor (melanoma, choriocarcinoma, thyroid carcinoma, renal cell carcinoma, bronchogenic carcinoma, breast carcinoma)
• Drugs– Illicit drugs (cocaine,
amphetamine)– Over-the-counter
medications (phenylpropanolamine)
– Prescription medications (warfarin, aspirin, TPA, heparin)

Quality-of-care indicators and accepted reasons for nontreatment
Neurology 2005;65:360–365
Intervention Implementation Acceptable reason far nontreatmentThrombolysis within 3 hours IV-tPA, IA-tPA, tenecteplase Arrival > 3 hours after symptom onset,
unknown time of symptom onset, uncontrolled hypertension, rapid improvement, stroke too mild or too severe, seizure at onset, recent surgerv, refusal, history of intracranial bleeding or arteriovenous malformation, on-going bleeding, platelet count <100,000, abnormal aPPT or PT, glucose <50 mg\dL or >400 mg/dL, life expectancy I year, dementia
Antithrombotic medication within 48 hours
Antiplatelet agents, anticoagulants thrombolysis
Bleeding risk, terminal illness
D’VT prophylaxis by hospital day 2
Anticoagulants or vascular support hose with paeumatic compression devices
Patient ambulatory
Smoking cessation counseling
Counseling the stop smoking or smoking advice
Current nonsmoker, no history of smoking, death in hospital
Lipid-lowering medication at discharge
Lipid-lowering medications LDL < 100 mg/dL, death in hospital
Antithrombotic medication at discharge
With atrial fibrillation: anticoagulants; without atrial fibrillation: antiplatelet agents, anticoagulants
Bleeding risk (e.g., liver disease, active peptic ulcer disease, fall risk), refusal, terminaI ill, impaired mental status, planned surgery, death in hospital

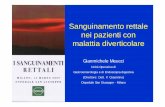
IH1: small petechiaeIH2: more confluent petechiaePH1: haematoma in <30% of the infarcted area; slight space-occupying effectPH2: dense haematoma >30% of the infarcted area; substantial space-occupying effect
IH1: small petechiaeIH2: more confluent petechiaePH1: haematoma in <30% of the infarcted area; slight space-occupying effectPH2: dense haematoma >30% of the infarcted area; substantial space-occupying effect
ICH after thrombolysisICH after thrombolysis

ICH: epidemiology and ICH: epidemiology and relationship with relationship with
antithrombotic treatmentantithrombotic treatment
Nicolini A et al. Haematologica 2002;87:948-956Nicolini A et al. Haematologica 2002;87:948-956

Volume of haemorrhage, AC Volume of haemorrhage, AC and AP useand AP use
Stead LG et al. Clin Neurol Neurosurg 2009Stead LG et al. Clin Neurol Neurosurg 2009

AP or OA therapy effect on AP or OA therapy effect on unfavorable outcome and in-unfavorable outcome and in-
hospital mortalityhospital mortality
Saloheimo P et al. Stroke 2006;37:129-133Saloheimo P et al. Stroke 2006;37:129-133Saloheimo P et al. Stroke 2006;37:129-133Saloheimo P et al. Stroke 2006;37:129-133

ICH: stima della frequenza ICH: stima della frequenza assolutaassoluta
Popolazione Popolazione generalegenerale
ASAASA ASA + ASA + ClopidogrelClopidogrel
WarfarinWarfarin Warfarin Warfarin + ASA+ ASA
0.15 %
FA: 0.2%CVD: 0.3%
FA: 0.3%CVD: 0.4%
FA: 0.3-0.6%CVD: 0.4-1.0% 0.5-1.0%
Hart RG et al. Stroke 2005;36:1588-1593Hart RG et al. Stroke 2005;36:1588-1593

Da soli o in associazione?Da soli o in associazione?

Rates of CNS bleeding during Rates of CNS bleeding during antiplatelet therapy with ASA and antiplatelet therapy with ASA and
ClopidogrelClopidogrel
Hart RG et al. Stroke 2005;36:1588-1593Hart RG et al. Stroke 2005;36:1588-1593

MATCH: life-threatening and major MATCH: life-threatening and major bleedingbleeding
Type of Bleeding Events (%)
Placebo + Clopidogrel (n=3,781)
ASA + Clopidogrel (n=3,759)
% AbsoluteDifference
(95% CI)
p value
Defined as Life-threatening Events (%)
49 (1.3) 96 (2.6)
1.26 (0.64, 1.88)
<0.001Gastrointestinal 21 (0.6) 51 (1.4)
Intracranial 25 (0.7) 40 (1.1)
Major Bleeding Events (%) 22 (0.6) 73 (1.9)1.36
(0.86, 1.86)<0.00
1Gastrointestinal 11 (0.3) 42 (1.1)
Life threatening: Life threatening: any fatal bleeding event, or a drop in haemoglobin of 5g/d, or significant hypotension with the need of any fatal bleeding event, or a drop in haemoglobin of 5g/d, or significant hypotension with the need of inotropes (hemorrhagic shock) or, symptomatic intracranial haemorrhage, or requiring transfusion of inotropes (hemorrhagic shock) or, symptomatic intracranial haemorrhage, or requiring transfusion of 4 4 units of RBC or equivalent amount of whole bloodunits of RBC or equivalent amount of whole blood
Major bleeding:Major bleeding: significantly disabling (with persistent sequelae), or intraocular bleeding leading to significant loss of vision significantly disabling (with persistent sequelae), or intraocular bleeding leading to significant loss of vision or, requiring transfusion of or, requiring transfusion of 3 units of RBC or equivalent amount of whole blood 3 units of RBC or equivalent amount of whole blood
Diener HC, et al. Lancet 2004;364:331-337

CHARISMA: Overall Population Safety Results
Endpoint* - N (%)
Clopidogrel+ ASA
(n=7802)
Placebo + ASA
(n=7801)
p value
GUSTO Severe Bleeding
130 (1.7) 104 (1.3) 0.09
Fatal Bleeding 26 (0.3) 17 (0.2) 0.17
Primary ICH 26 (0.3) 27 (0.3) 0.89
GUSTO Moderate Bleeding
164 (2.1) 101 (1.3)<0.00
1*Adjudicated outcomes by intention to treat analysisICH= Intracranial Hemorrhage
Bhatt DL, Fox KA, Hacke W, et al. NEJM 2006 – In press

ASA and ER-ASA and ER-Dipyridamole Dipyridamole versus versus Clopidogrel for Clopidogrel for recurrent recurrent stroke: primary stroke: primary and secondary and secondary outcomesoutcomes
Sacco R et al. NEJM 2008;359:1-14

Prasugrel vs Clopidogrel Prasugrel vs Clopidogrel in Acute Coronary Syndromes in Acute Coronary Syndromes
Wiviott SD et al. NEJM 2007;357:2001-2015

Platelet antiaggregants and anticoagulants within 48 Platelet antiaggregants and anticoagulants within 48 hours of acute ischemic strokehours of acute ischemic stroke
Coull BM et al, Stroke 2002

SPREAD: Terapia anticoagulante in SPREAD: Terapia anticoagulante in prevenzione secondariaprevenzione secondaria
Raccomandazione 10.12 Grado DIn pazienti con qualunque eziologia cardioembolica, escludendo i casi a rischio emboligeno molto elevato, qualora vi sia una lesione estesa alla TC a 48 ore, è indicato procrastinare di almeno 14 giorni l’inizio del trattamento anticoagulante, per il maggior rischio di trasformazione emorragica sintomatica.
Qualora una TC abbia documentato una lesione minore del 30% dell’emisfero colpito senza trasformazione emorragica in forma di ematoma, il trattamento può essere iniziato precocemente.
2003Raccomandazione 10.10 Grado D In pazienti con qualunque etiologia cardioembolica, in assenza delle controindicazioni elencate al Capitolo 5, è indicato iniziare il trattamento anticoagulante orale tra 48 opre e 14 giorni tenendo conto di:
•Gravità clinica•Estensione della lesione alle neuroimmagini•Comorbosità cardiologica (definita anche con ecocardiografia)
2007 (&2010)

ECASS study: ICH following ECASS study: ICH following thrombolysisthrombolysis
Derex L, Nighoghossian N. JNNP 2008;79:1093-1099

Thrombolysis-related ICHThrombolysis-related ICH
• Acute Myocardial Infarction: 0.6%• Pulmonary Embolism: 3%• Ischaemic Stroke*: 6-11%
– Intravenous thrombolytic therapy 6%– Intra-arterial thrombolytic therapy 11%
* ICH in brain areas outside the vascular distribution of the ischaemic stroke: 20%
Mac Carron MO & Nicol JAR, Lancet Neurology 2004;3(8):484

Tissue Plasminogen Activator – Tissue Plasminogen Activator – Possible Reasons for Temporal Possible Reasons for Temporal
RestrictionRestriction
rt-PA
Cleavage
Fibrin
Plasminogen
rt-PA
Plasmin
Sec
ond
Gen
erat
ion:
Rec
ombi
nant
Pro
tein
s
Multi-tasking: Additional physiological functions of tPA turn deleterious in the ischemic setting
tPA , a neurotoxic agent: Endogenous glutamate can cause neurotoxicity, e.g. under ischemic conditions; tPA is able to aggravate this toxicity.
Benchenane et al, Trends Neurosci 27: 155 (2004)

Caso clinico: maschio, 71 anni, Caso clinico: maschio, 71 anni, emiparesi sinistra, esordita da circa 45’ emiparesi sinistra, esordita da circa 45’
• Plavix 75 mg cp 1 cp dopo pranzoPlavix 75 mg cp 1 cp dopo pranzo• Cardioaspirin 100 mg cp 1 cp dopo cenaCardioaspirin 100 mg cp 1 cp dopo cena• Torvast 10 mg cp 1 cp alla sera• Triatec 5 mg cp 1 cp al mattino• Bisoprololo 2.5 mg cp 1 cp al mattino
Dopo circa 2 h Dopo circa 2 h dalla trombolisidalla trombolisiDopo circa 2 h Dopo circa 2 h dalla trombolisidalla trombolisi

AP treatment and thrombolysis:AP treatment and thrombolysis:distribution of the mRS scores at 3 distribution of the mRS scores at 3
monthsmonths
Diedler J et al. Stroke 2010;41:288-294Diedler J et al. Stroke 2010;41:288-294

AP treatment and thrombolysis:AP treatment and thrombolysis:causes of deathcauses of death
Diedler J et al. Stroke 2010;41:288-294Diedler J et al. Stroke 2010;41:288-294

Cerebral microbleedsCerebral microbleeds
• Prevalence:
• No CVD: 4.7%
• Ischemic CVD: 40%
• Ischemic CVD with cerebral
microangiopathy: 57%
• Hemorrhagic CVD: 68%
• Location:
• Cortical-subcortical areaKoennecke HC, Neurology 2006;66(2):165


Leukoaraiosi e ICH TAO-relataLeukoaraiosi e ICH TAO-relata
Valori espressi in n(%)
Smith EE et al, Neurology 2002
• Presenza:
OR: 12.9 (95%CI: 2.8-59.8)
• Grado 3-4:
OR: 24.9 (95% CI: 4.5-137.4)

Anticoagulant-related Anticoagulant-related ICHICH
Hart R, Stroke 1995;26:1471

Anticoagulant-related ICHAnticoagulant-related ICH
• Anticoagulation to conventional intensities increases the risk of intracranial hemorrhage 7- to 10-fold, to an absolute rate of nearly 1%/y for many stroke-prone patients.
• Most (70%) anticoagulant-related intracranial hemorrhages are intracerebral hematomas (approximately 60% are fatal); the bulk of the remainder are subdural hematomas.
• Predictors of anticoagulant-related intracerebral hematoma are advanced patient age (>75 yrs), race, prior ischemic stroke, hypertension (systolic BP >160 mmHg), intensity of anticoagulation, concomitant use of antiplatelet drug, and cerebral amyloid angiopathy.
• In approximately half of anticoagulated patients with intracerebral hematoma the bleeding evolves slowly over 12 to 24 hours, and emergency reversal of anticoagulation is crucial
Hart R mod, Stroke 1995;26:1471

Kaplan-Meier estimate of rate of Kaplan-Meier estimate of rate of
hemorrhage expansionhemorrhage expansion
Flibotte Neurology, 2004;63(6):1059

The increasing incidence of anticoagulant-The increasing incidence of anticoagulant-associated intracranial haemorrhageassociated intracranial haemorrhage
1988 1993-1994 1999
All ischemic stroke NA 140.0 (133.2-146.8) 142.6 (135.8-149.3)
Cardioembolic strokeNA 31.1 (27.9-34.3) 30.4 (27.3-33.5)
Cardioembolic ischemic strokedue to AF NA 22.0 (19.3-24.8) 20.6 (18.1-23.2)
All ICH 16.5 (14.1-18.9) 22.1 (19.4-24.8) 24.6 (21.8-27.4)
AAICH 0.8 (0.3-1.3) 1.9 (1.1-2.7) 4.4 (3.2-5.5)
Flaherty ML et al. Neurology 2007;68:116-121

Racial/ethnic differences in the Racial/ethnic differences in the risk of ICH among patients with risk of ICH among patients with
AFAF
Shen A Y-J et al. J Am Coll Med 2007;50:309-315

Predittori di ICH durante TAO Predittori di ICH durante TAO EtàEtà
Fang MC et al, Ann Intern Med 2004

Predittori di ICH durante TAO Ipertensione arteriosaIpertensione arteriosa
PROGRESS trial
• Il rischio assoluto passava da 0.6%/anno a 0.3%/anno e 0.2%/anno rispettivamente
-80
-70
-60
-50
-40
-30
-20
-10
0
-9 mmHg -12 mmHg
%
Pressione arteriosa sistolica
Chapman N et al, Stroke 2004

Rischio emorragico e valori di Rischio emorragico e valori di INRINR
• Aumento rischio ICH di 2-5 volte, direttamente correlato ai valori di INR. Buona parte delle ICH occorrono, tuttavia, con INR in range terapeutico
40%
Cantalapiedra A et al, J Thromb Thrombolysis 2006


Risk analysis of thrombo-embolic and Risk analysis of thrombo-embolic and recurrent bleeding events in AC-recurrent bleeding events in AC-
related ICHrelated ICH
De Vleeschouwe S et al, Acta Chir Bel 2005;105:268-274
TE risk: 0,66/1000 pts-day at risk (8/11590 pts-day)
Recurrent ICH: 8/108 pts (before restarting OAC)

Discontinued anticoagulation for Discontinued anticoagulation for intracranial haemorrhageintracranial haemorrhage
In a patient who is taking warfarin and experiences an intracranial haemorrhage, warfarin should be stopped and its effects reversed fully with vitamin K orally, subcutaneously or intravenously and clotting factor replacement.
The timing of recommencing anticoagulation will depend on the risk of embolisation and on the risk of rebleeding.
It is possible to resume warfarin therapy quite early, even within the first 7-14 days, without high risk of recurrent bleeding in patients with a high risk of re-embolisation and a small intracranial bleed.

Avoiding CNS bleeding during Avoiding CNS bleeding during antithrombotic therapyantithrombotic therapy
Hart RG et al. Stroke 2005;36:1588-1593Hart RG et al. Stroke 2005;36:1588-1593