Aspetti Clinici e di Laboratorio del Tromboembolismo...
53
Francesco Marongiu Università di Cagliari, Policlinico di Monserrato, Medicina Interna [email protected] Pavia, 21-22 giugno 2012 Pavia Spring Meeting on Thrombosis Aspetti Clinici e di Laboratorio del Tromboembolismo Venoso ed Arterioso alla luce delle Linee Guida ACCP 2012 Farmaci anticoagulanti vecchi e nuovi
Transcript of Aspetti Clinici e di Laboratorio del Tromboembolismo...

Francesco MarongiuUniversità di Cagliari, Policlinico di Monserrato, Medicina Interna
Pavia, 21-22 giugno 2012
Pavia Spring Meeting on ThrombosisAspetti Clinici e di Laboratorio del Tromboembolismo Venoso ed Arterioso
alla luce delle Linee Guida ACCP 2012
Farmaci anticoagulanti vecchi e nuovi
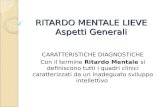
Professor Diakonov nel suo articolo del 1809,Changes ofhuman blood in the leechnel 1809, scrisse che “lack of bloodcoagulation and dissolution of red blood corpuscles in the leech’s intestinal duct testifies that some dissolving agent exists there”
IRUDINA
Historical Article: Hirudo medicinalis: ancient origins of, and trends in the use of medicinal leeches throughout history. Br J Oral and Maxillofacial Surg 2004;42: 133-7

McLean J. The thromboplastic action of cephalin. Am J Physiol 1916; 41: 250-7McLean J. The discovery of heparin. Circulation 1959; 19: 75-8.
Jay McLean

M W 15,000 (range: 3.000 to 30.000 d)Only one third of heparin molecules contain the high-affinity
pentasaccharide (AT) required for anticoagulant activity
UFH
Heparin doses Half-life min
25 U/Kg (1750 U) 30
100 U/Kg (7000 U) 45-60
400 U/Kg (28000 U) 46-150
Chest 2008;133;141-159
Highly sulphated mucopolysaccharide

Heparin binds to plasma proteins, endothelial cells, macrophages and AT.
Plasma proteins
Endothelial cells
Antithrombin
Macrophages
Chest 2008;133;141-159
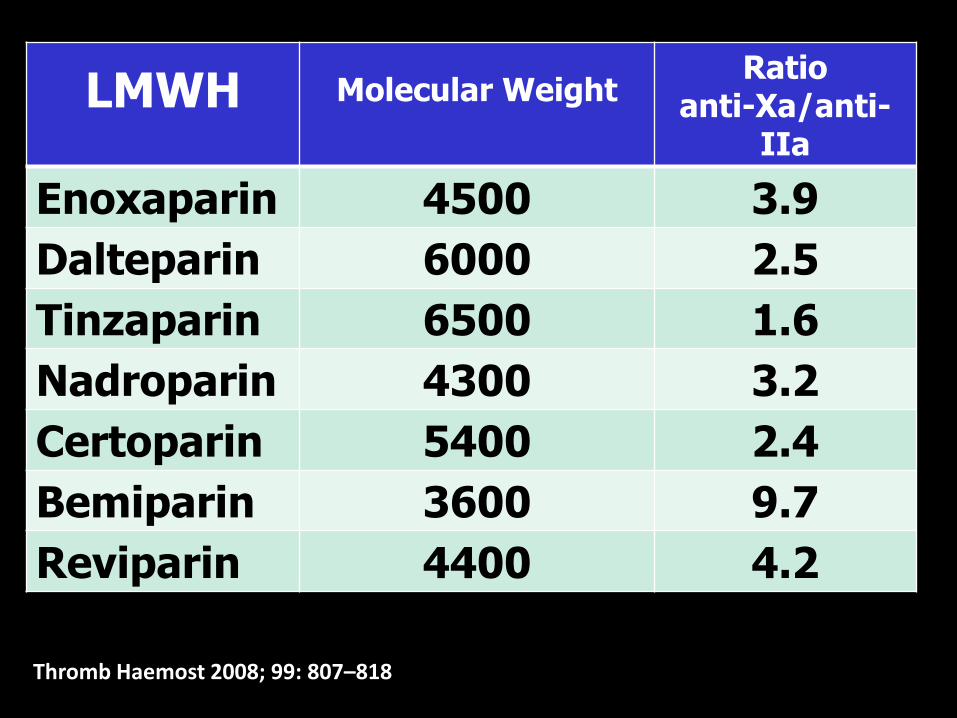
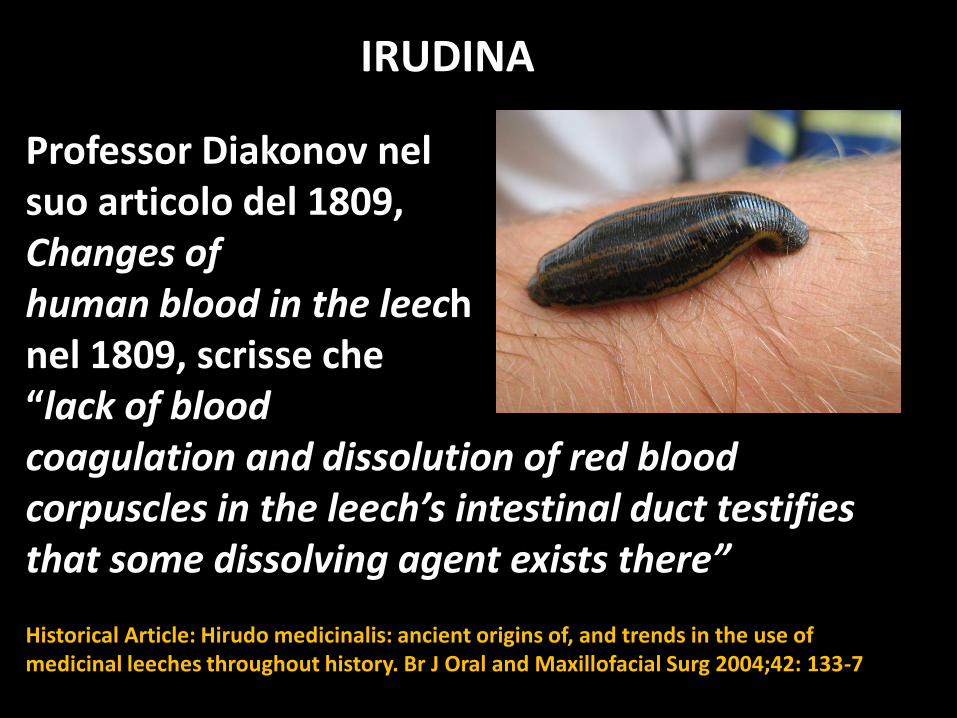
LMWH Molecular WeightRatio
anti-Xa/anti-IIa
Enoxaparin 4500 3.9
Dalteparin 6000 2.5
Tinzaparin 6500 1.6
Nadroparin 4300 3.2
Certoparin 5400 2.4
Bemiparin 3600 9.7
Reviparin 4400 4.2
Thromb Haemost 2008; 99: 807–818

Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism
Cochrane Database of Systematic Reviews 2010, Issue 9. Art. No.:
CD001100
Petra MG Erkens, Martin H Prins

.2 1 5 10
OR 0.71; 0.56 to 0.90
23 studies Follow-up3 months
Thrombosis
recurrence
LMWH:3382
NadroparinDalteparinCertoparinTinzaparinEnoxaparinReviparin
3.6 % (122)
5.2 % (164)
UH: 3169

OR 0.88 (0.48-1.63)
No significant difference
between:
LMWH (n=670) versus UFH (n=559)
in patients with pulmonary embolism

Pros and Cons versus UFH
1 bioavailability (they do not link to plasma proteins)
2 longer half-lifes (up to 4 times)
3 subcutaneoulsly administered (so at home)
4 they do not need lab monitor (in general)
Not recommended if GF<30 ml/min (may be accumulated)
Difficult reverse with protamine sulphate (about 40 %)

300 milioni di maiali
100 tonnellate di eparina
per anno
Eparine

Cina
Circa l’85 % del mercato mondialedelle eparine
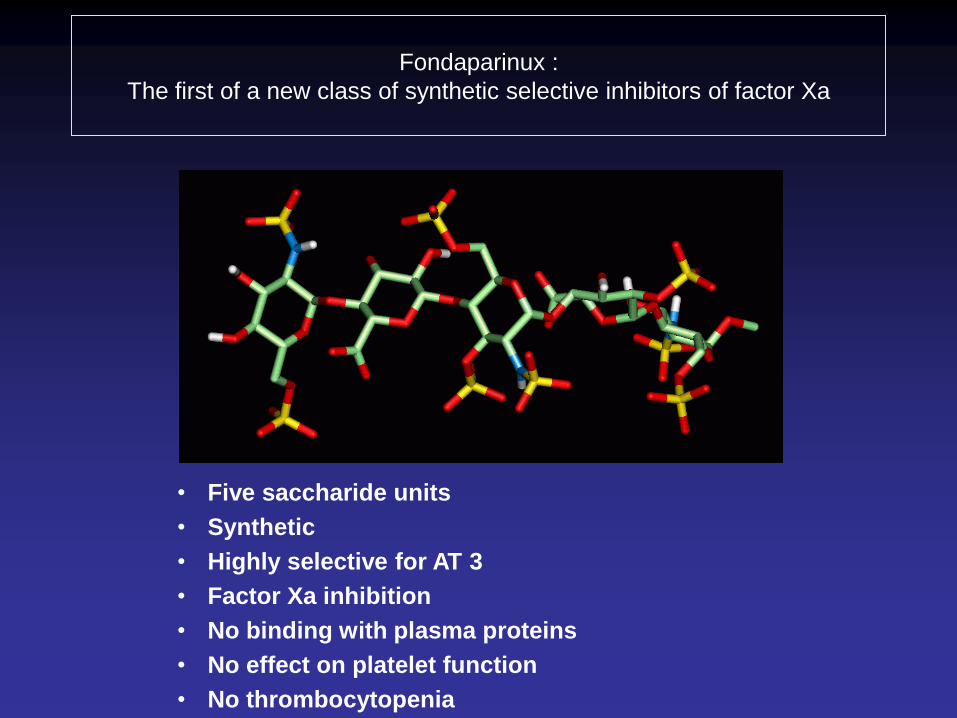
Fondaparinux :
The first of a new class of synthetic selective inhibitors of factor Xa
• Five saccharide units
• Synthetic
• Highly selective for AT 3
• Factor Xa inhibition
• No binding with plasma proteins
• No effect on platelet function
• No thrombocytopenia

Fondaparinux (N=1103) UFH (N=1110)
Fondaparinux - UFH (95 % CI )
Matisse PE
-1.2% = 3.5%0 0.5%-3.0%
Fatal PE 16 (1.5 %) 15 (1.4 %)
Non-fatal PE or DVT 26 (2.4 %) 41 (3.6 %)
Total symptomatic recurrent VTE 42 (3.8 %) 56 (5.0 %)
AT
I SS
E
M .
..
. ..
.
Primary Efficacy Outcome - 3 months -
(The Matisse Investigators; NEJM 2003;349:1695)
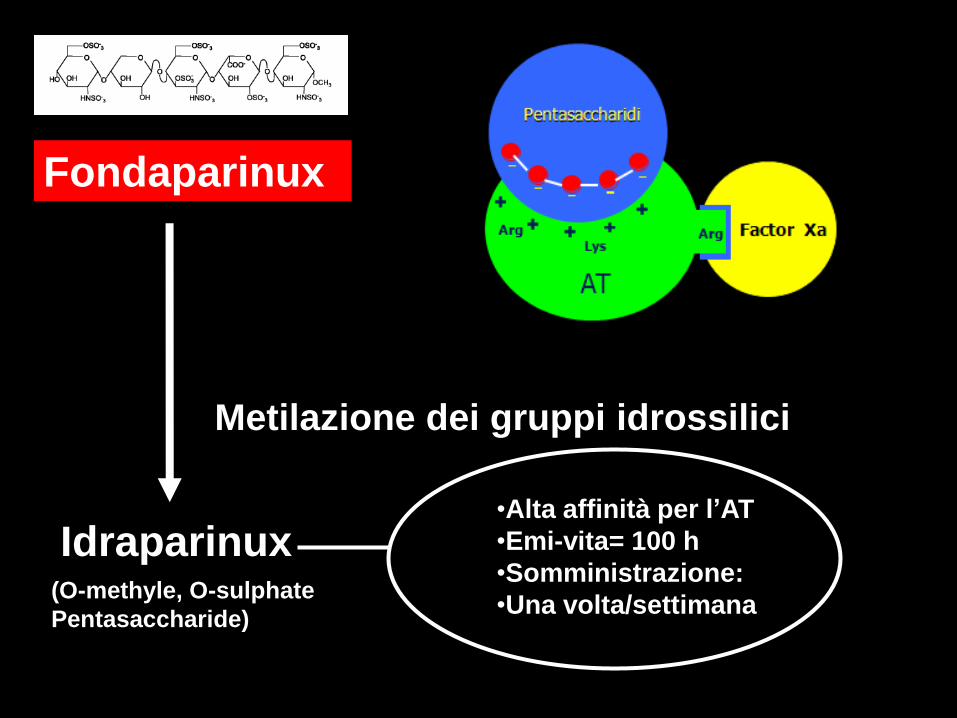
Fondaparinux
Metilazione dei gruppi idrossilici
Idraparinux(O-methyle, O-sulphate
Pentasaccharide)
•Alta affinità per l’AT
•Emi-vita= 100 h
•Somministrazione:
•Una volta/settimana

The Van Gogh Investigators. New Engl J Med 2007; 357: 1094-104
3 %
2.9 %
3.4 %
1.6 %
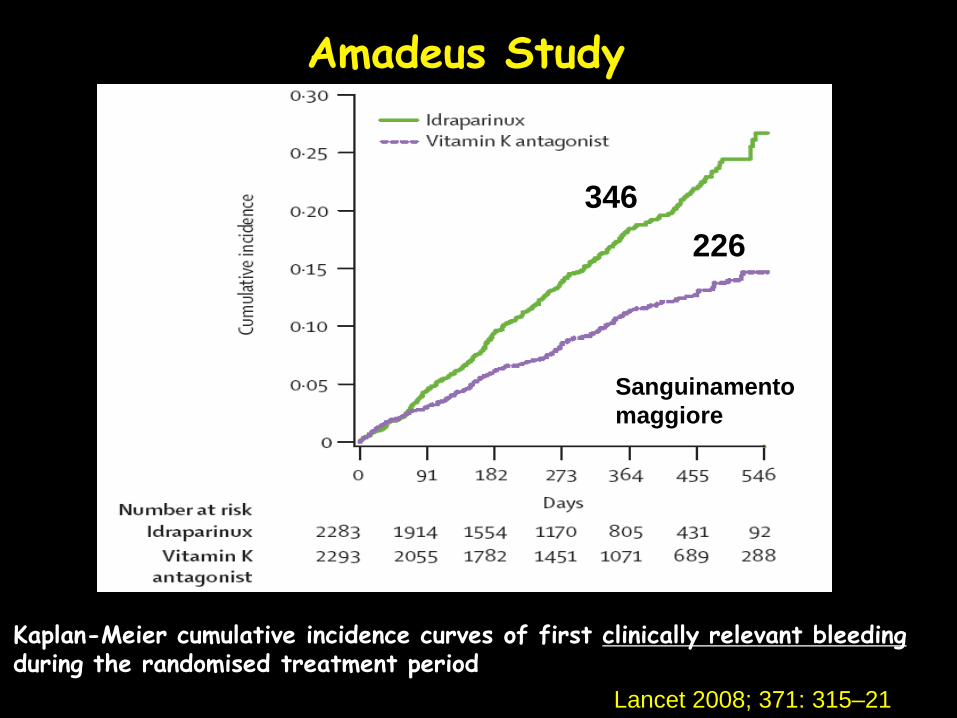
Kaplan-Meier cumulative incidence curves of first clinically relevant bleedingduring the randomised treatment period
Amadeus Study
Sanguinamento
maggiore
346
226
Lancet 2008; 371: 315–21

Idrobiotaparinux

In the BOREALIS trial, idrabiotaparinux was developed for the prevention of
thromboembolic events in patients with atrial fibrillation.
Considering recent therapeutic advances in this field, this compound does
not appear able to bring significant improvement in the care of these
patients. Therefore, the development in this indication is discontinued.
Sanofi-Aventis Press Release dec 21, 2009

Lancet 2012; 379:123-9
Idrabiotaparinux versus warfarin: 3202 randomized patientsEnoxaparin for all patients in the first 10 days
Recurrent venous thromboembolism:Idrabiotaparinux 2 % versus W 3 %

Idrabiotaparinux
A favore
SinteticoProtegge dopo molti mesiComoda somministrazione
Antidoto (avidina)
Contro
Emivita estremamente lungaPossibilità di accumulo
Possibili reazioni avverseall’avidina
R
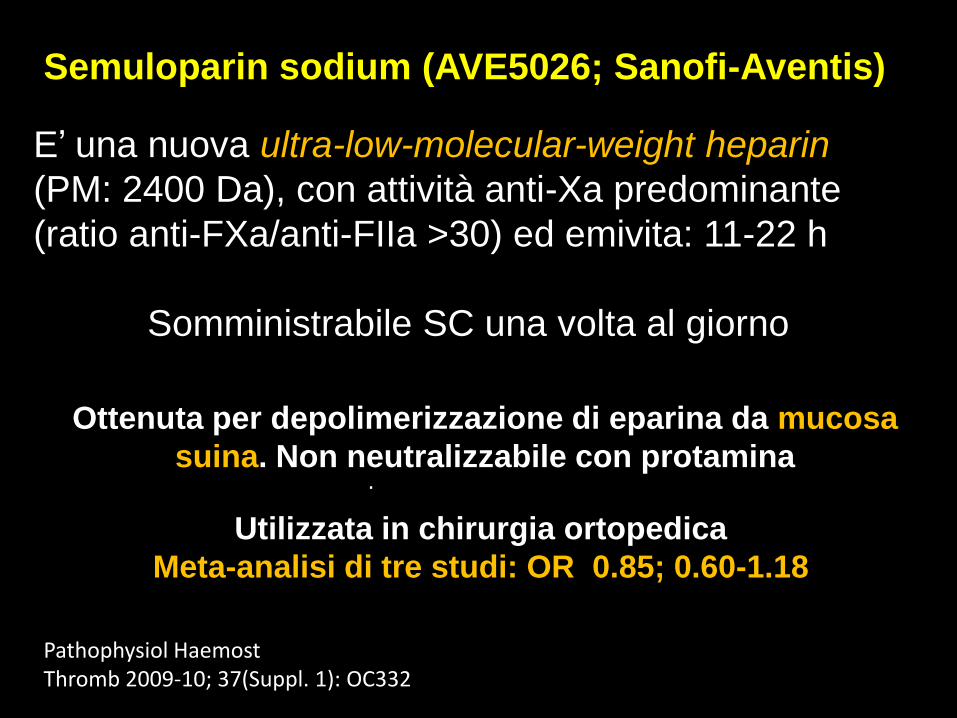
Semuloparin sodium (AVE5026; Sanofi-Aventis)
E’ una nuova ultra-low-molecular-weight heparin
(PM: 2400 Da), con attività anti-Xa predominante
(ratio anti-FXa/anti-FIIa >30) ed emivita: 11-22 h
Somministrabile SC una volta al giorno
.
Ottenuta per depolimerizzazione di eparina da mucosa
suina. Non neutralizzabile con protamina
Utilizzata in chirurgia ortopedica
Meta-analisi di tre studi: OR 0.85; 0.60-1.18
Pathophysiol HaemostThromb 2009-10; 37(Suppl. 1): OC332

Otamixaban (Sanofi-Aventis)
Potente ed altamente selettivo anti-Xa per IV
Rapida massima attività: 3 min
(Emivita: 30 minuti)
Escrezione biliare (soprattutto)
Antidoto: no
Sindromi Coronariche Acute

OTAMIXABAN Composite outcomes
0.035 mg/Kg/h 7.2 %
0.07 mg/Kg/h 4.6 %
0.105 mg/Kg/h 3.8 %
0.140 mg/Kg/h 3.6 %
0.175 mg/Kg/h 4.3 %
Control group: Heparin (60 IU/kg IV bolus followed by an infusion of 12 IU/kg/h) + eptifibatide (180 mg/kg IV bolus followed by an infusion of 1.0-2.0 mg/kg/min).
6.2 %
Otamixaban: alternativa all’eparina nelle ACS ?
Lancet 2009; 374: 787-795
SEPIA-ACS1 TIMI 42 trial; 3200 pazienti (dose-finding trial)

Pegmusirudin (PEG-hirudin; SPP200; LU87981)DTI con lunga emivita (fino a 36 h)
Antidoto: no
Emodialisi
Studio di fase II su 127 pazientiPEG-Hirudin: 0.052 o 0.065 mg/kg
Occlusione accesso vascolarePEG-hirudin 11 % versus Heparin 40 %
Sanguinamento maggiorePEG-Hirudin 8.4 % versus Heparin 5.4 %
Sanguinamento minore: 57.8 versus 32.4 %
J Am Soc Nephrol 17: F-PO769

Pentasaccaride + DTI +
biotina
Neutralizzato da avidina
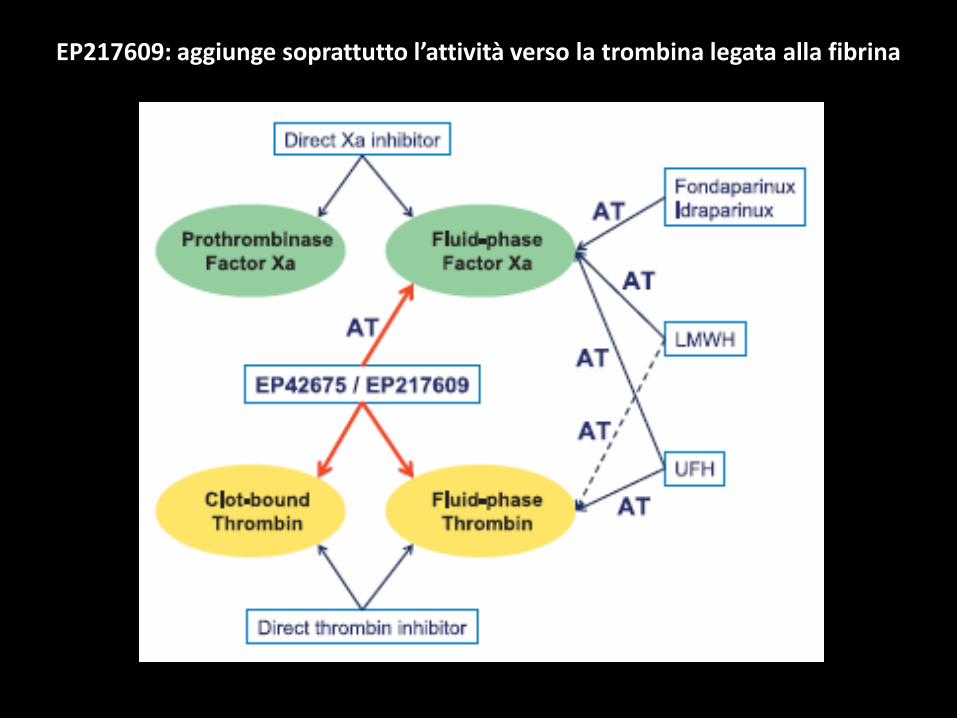
EP217609: aggiunge soprattutto l’attività verso la trombina legata alla fibrina

Antidote
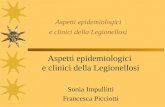
The REG1 anticoagulation system is composed of the drug RB006 and the oligonucleotide antidote to RB006 (RB007), which binds to RB006 via Watson-Crick base pairing and thereby neutralizes its pharmacological effect.
Anti-IX
Aptamer
Eur Heart J 2011;32:2412-9
Pegnivacogin results in near complete FIX inhibition in acute coronary syndrome patients: RADAR pharmacokinetic and
pharmacodynamic substudy.
The REG1 system (Regado Biosciences, Basking Ridge, NJ) consists of pegnivacogin (RB006), an RNA aptamer that directly inhibits factor IXa, and anivamersen (RB007), its complementary control agent.
RADAR is a Phase 2b study investigating the use of pegnivacogin in patients (n = 800) with ACS undergoing planned early cardiac catheterization.
Pegnivacogin 1 mg/kg rapidly achieved a high pegnivacogin plasmaconcentration (26.1 ± 4.6 µg/mL), prolonged the aPTT (mean aPTT 93.0 ±9.5 s), and approached near complete factor IX inhibition.

Anticoagulant Hours to
[C] maxHalf-life
hours
Renal
elimination
Dabigatran 2 12-14 80 %
Rivaroxaban 2-4 9-13 33 (66) %
Apixaban 1-3 8-15 25 %
Ericksson BI, Clin Phatmacokinet 2009
Ruff CR, Am Heart J 2010
General characteristics of NOA

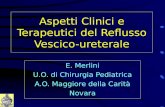
Study name Statistics for each study Risk ratio and 95% CI
Risk Lower Upper ratio limit limit Z-Value p-Value
Apixaban AF 0,797 0,667 0,952 -2,501 0,012
Re-ly 150 0,667 0,538 0,828 -3,668 0,000
Re-ly 110 0,916 0,751 1,116 -0,873 0,383
ROCKET AF 0,880 0,750 1,033 -1,559 0,119
0,822 0,749 0,901 -4,167 0,000
0,5 1 2
Favours NOA Favours Warfarin
NOA versus Warfarin
Meta Analysis
Stroke

Hazard ratios and 95% confidence intervals of the primary safety
outcome (major bleeding) in the 3 pivotal trials comparing new oral
anticoagulants with warfarin in nonvalvular atrial fibrillation.
JACC 2012; 59:1413–25
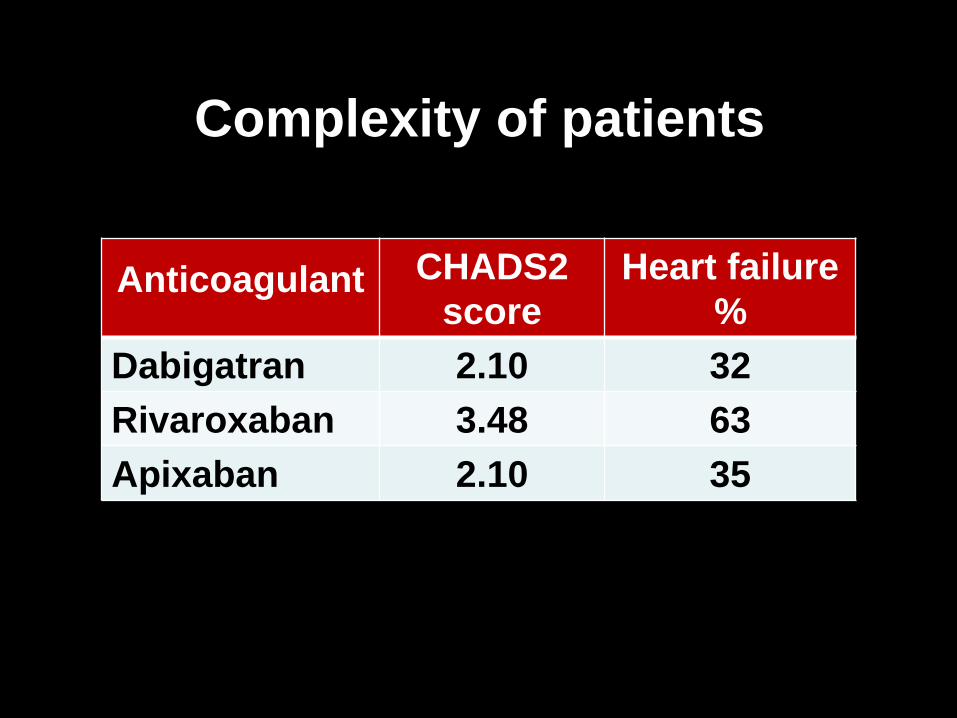
Anticoagulant CHADS2
score
Heart failure
%
Dabigatran 2.10 32
Rivaroxaban 3.48 63
Apixaban 2.10 35
Complexity of patients

Anticoagulant M. B. % y ICH % y
Dabigatran 150 mg
Dabigatran 110 mg
Warfarin 2.0-3.0 INR
3.11
2.71
3.36
0.10
0.12
0.38
Rivaroxaban 20 mg*
Warfarin 2.0-3.0 INR
3.60
3.40
0.50
0.70
Apixaban 5 mg
Warfarin 2.0-3.0 INR
2.13
3.09
0.24
0.47
* Once daily
NOA and Atrial Fibrillation:
Major bleeding with warfarin: 3.09-3.36 %y
an unrealistic result

Anticoagulant Gastrointestinal
bleeding
Rivaroxaban 20 mg 224 (3.15 %)
Warfarin 2.0-3.0 INR 154 (2.16 %)
p<0.001
More gastroenteric bleeding with
Rivaroxaban

Anticoagulant Gastrointestinal
bleeding
Dabigatran 150 mg 182 (1.51 % y)
Warfarin 2.0-3.0 INR 120 (1.02 % y)
RR: 1.50 (1.19-1.89) p<0.001
More gastroenteric bleeding with
Dabigatran 150 mg (t.d.))

Anticoagulant Dispepsia
Dabigatran 150 mg 688 (11.3 %) *
Dabigatran 110 mg 707 (11.8 %) *
Warfarin 2.0-3.0 348 (5.8 %)
More dyspepsia with Dabigatran)
* p<0.001
unreliable result
(never seen)

Questions and answers on the use of dabigatran and
perpectives on the use of other new oral anticoagulants
in patients with atrial fibrillation
A consensus document of the Italian Federation of
Thrombosis Centers (FCSA)
Vittorio Pengo; Luciano Crippa; Anna Falanga; Guido
Finazzi; Francesco Marongiu; Gualtiero Palareti; Daniela
Poli; Sophie Testa; Eros Tiraferri; Alberto Tosetto;
Armando Tripodi; Cesare Manotti
Thromb Haemost 2011;106:868-76

Which naive patient should be treated with NOA ?
All the patients with characteristics similar to those of
patients enrolled in the NOA studies.
Patients on VKAs with a TTR (time spent in the
therapeutic range) below 50-55 % (Grade A).
Patients at high risk of stroke (Grade A).
Patients willing to be prescribed the new drugs.
Patients with logistic problems or those confined to
home due to physical problems.

Which patients are definitely to remain on VKAs ?
Patients with both a stable INR and a low bleeding risk
(Grade A).
Patients with frequent dyspepsia (Grade A).
Patients who prefer to continue with VKAs after having
received complete information on the pros and cons of
NOA.
Patients with severe renal failure (Grade A).
Patients with previous myocardial infarction.

Should we expect significant drug interactions ?
What is recommended for the follow-up ?
Enter patient’s data into a registry
(indication, type of NOA, adverse events
etc.).
Follow-up after 3 and 6 months. Then,
every six months.

Conditions Dabigatran Rivaroxaban Apixaban
Heart valve disorders Excluded Excluded Excluded
Disabling stroke within the previous six months or any
stroke within the previous 14 d
Excluded Excluded NR
Increased risk of bleeding
a) previous surgery within the previous month Excluded Excluded NR
b) history of intracranial, intraocular, spinal
retroperitoneal or a traumatic intra-articular bleeding
Excluded Excluded Excluded
c) Gastrointestinal haemorrhage within the past year Excluded Excluded NR
e) Ulcer disease in the previous 30 days Excluded NR NR
f) Recent malignancy or radiation therapy Excluded NR NR
Severe renal impairment: creatinine clearance less than
30ml/min
Excluded Excluded Excluded
Anaemia (Hb<10g/dl) or thrombocytopenia (<100-90 x
109/L)
Excluded Excluded Excluded
Planned cardioversion NR Excluded NR
Indication for anticoagulation other than AF Excluded Excluded Excluded
Major surgery or invasive procedure planned NR Excluded NR
Simultaneous treatment with both aspirin and a
thienopyridine
NR Excluded Excluded
Fibrinolytic treatment within 2 to 10 days Excluded Excluded NR
Liver disease Excludded Excluded NR
NOA: Exclusion criteria

4.3 Contraindications
In general, patient populations not studied in the clinical trial
programme should be mentioned in section 4.4 (4.4 Special
warnings and precautions) for use and not in this section unless a
safety issue can be predicted (e.g. use of renally eliminated
substances with narrow therapeutic margin in renal failure
patients).
If, however, patients have been excluded from studies due to a
contraindication on grounds of safety, they should be mentioned
in this section. If applicable a cross-reference to section 4.4
should be made.

Advantages of NOA
1 No INR need
2 Predictable activity
3 Less strokes and major bleeding
events (Dabigatran and Apixaban)
4 Rapid anticoagulation activity

Circulation 2012;125:165-170
Disadvantages of New Oral Anticoagulants

ad alto rischio (CHADS2 >2): Rivaroxaban
a basso-medio rischio (CHADS2 1-2): dabigatran 150 o apixaban
con precedente emorragia gastroenterica: Apixaban
con dispepsia e basso e medio rischio (CHADS2 1-2): apixaban
con dispepsia ed alto rischio: rivaroxaban
Scelta dei nuovi anticoagulanti orali nei pazienti selezionati (1)

a basso rischio (CHADS2 1): dabigatran 150 o apixaban
con insufficienza renale moderata (Cr Cl: 30-50): apixaban se CHADS2 2 o Rivaroxaban se CHADS2 >2
con età >75 anni, indipendentemente dal rischio, apixaban o rivaroxaban (possibile rapido declino della funzione renale)
con molti farmaci (>5-6 al giorno per due volte): Rivaroxaban
Scelta dei nuovi anticoagulanti orali nei pazienti selezionati (2)
NOA:
What about
deep vein
thrombosis
and
pulmonary
embolism ?

Dabigatran versus Warfarin in VTE
Dabigatran 1274 patients Warfarin 1265 patients
after initial treatment with UHF, LMWH or fondaparinux
6-month incidence of recurrent symptomatic,
objectively confirmed VTE
D
2.4 %
W
2.1 %
P<0.001 for non-inferiority
New Engl J Med 2009; 361:2342–2352

Rivaroxaban versus Warfarin in VTE
Rivaroxaban 1731 patients VKAs 1718 patients
12-month incidence of recurrent symptomatic,
objectively confirmed VTE
R
2.1 %
VKA
3.0 %
after initial treatment
with UHF, LMWH or
fondaparinux
15 mg twice/day for 3 weeks
followed by 20 mg/day
N Engl J Med 2010; 363: 2499–2510
HR: 0.68, 0.44-1.04, p<0.001 for non-inferiority

Rivaroxaban versus Warfarin in PE
Rivaroxaban: 2419 patients VKAs: 2413 patients
9-month incidence of recurrent symptomatic,
objectively confirmed PE
R
2.1 %
VKA
1.8 %
after initial treatment
with UHF, LMWH or
fondaparinux
15 mg twice/day for 3 weeks
followed by 20 mg/day
N Engl J Med 2012; 366:1287–1297
HR: 1.12, 0.75–1.68, p= 0.003 for non-inferiority

Conclusioni1 Sapremo tra qualche anno se le vecchie eparine potranno essere sostituite da nuovi farmaci (efficacia, sicurezza e costi).
2 I nuovi anticoagulanti orali potranno essere somministrati a pazienti selezionati con l’impegno di un follow-up periodico documentato.
3 Sulla base degli studi può essere possibile scegliere tra i diversi NOA.
4 Sembra ottimale il loro utilizzo nel TEV.
5 Gli AVK possono però rappresentare ancora la prima scelta in determinate condizioni.