TCG immaturi: aspetti clinici e terapeutici - chped.itchped.it/gico/milano_2012/Tumori a cellule...
40
Dipartimento salute della donna, del bambino e del neonato U.O.C. Chirurgia Pediatrica Direttore: Dott. M. Torricelli TCG immaturi: aspetti clinici e terapeutici Aspetti clinici generali Dott.ssa Anna Maria Fagnani
Transcript of TCG immaturi: aspetti clinici e terapeutici - chped.itchped.it/gico/milano_2012/Tumori a cellule...

Dipartimento salute della donna, del bambino e del neonato U.O.C. Chirurgia Pediatrica
Direttore: Dott. M. Torricelli
TCG immaturi:
aspetti clinici e terapeutici
Aspetti clinici generali
Dott.ssa Anna Maria Fagnani
AM Fagnani Milano, 24 Ottobre 2012
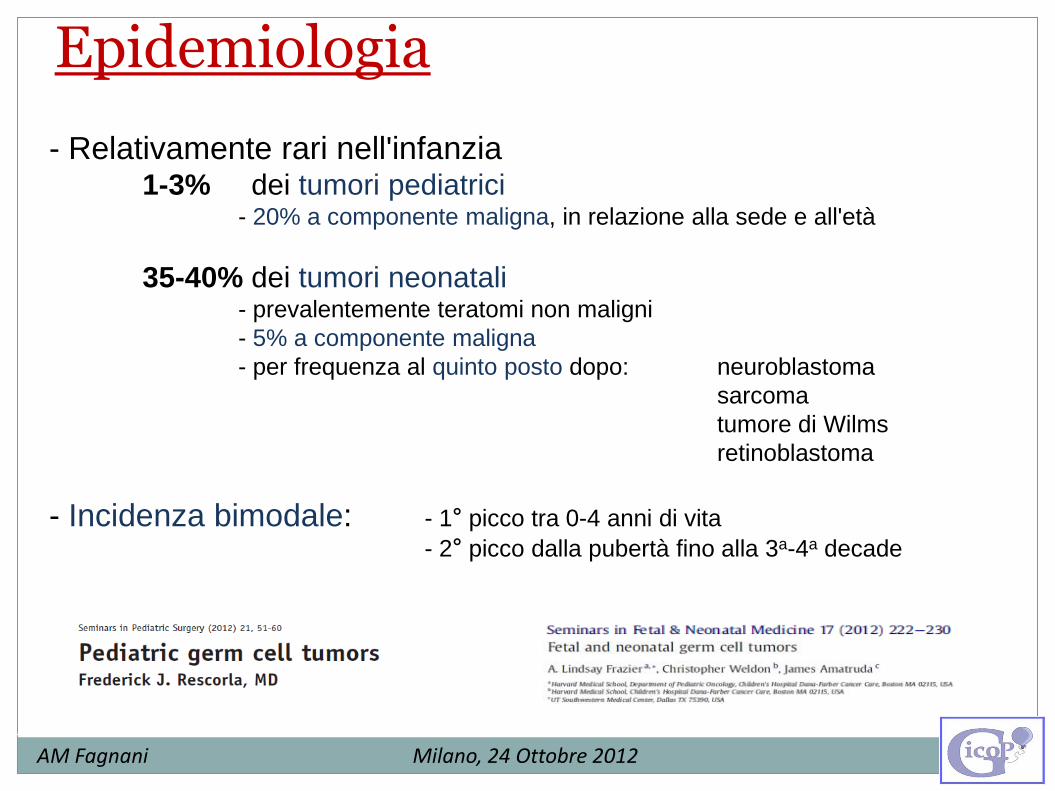
- Relativamente rari nell'infanzia 1-3% dei tumori pediatrici - 20% a componente maligna, in relazione alla sede e all'età
35-40% dei tumori neonatali - prevalentemente teratomi non maligni
- 5% a componente maligna
- per frequenza al quinto posto dopo: neuroblastoma
sarcoma
tumore di Wilms
retinoblastoma
- Incidenza bimodale: - 1° picco tra 0-4 anni di vita
- 2° picco dalla pubertà fino alla 3a-4a decade
Epidemiologia
AM Fagnani Milano, 24 Ottobre 2012
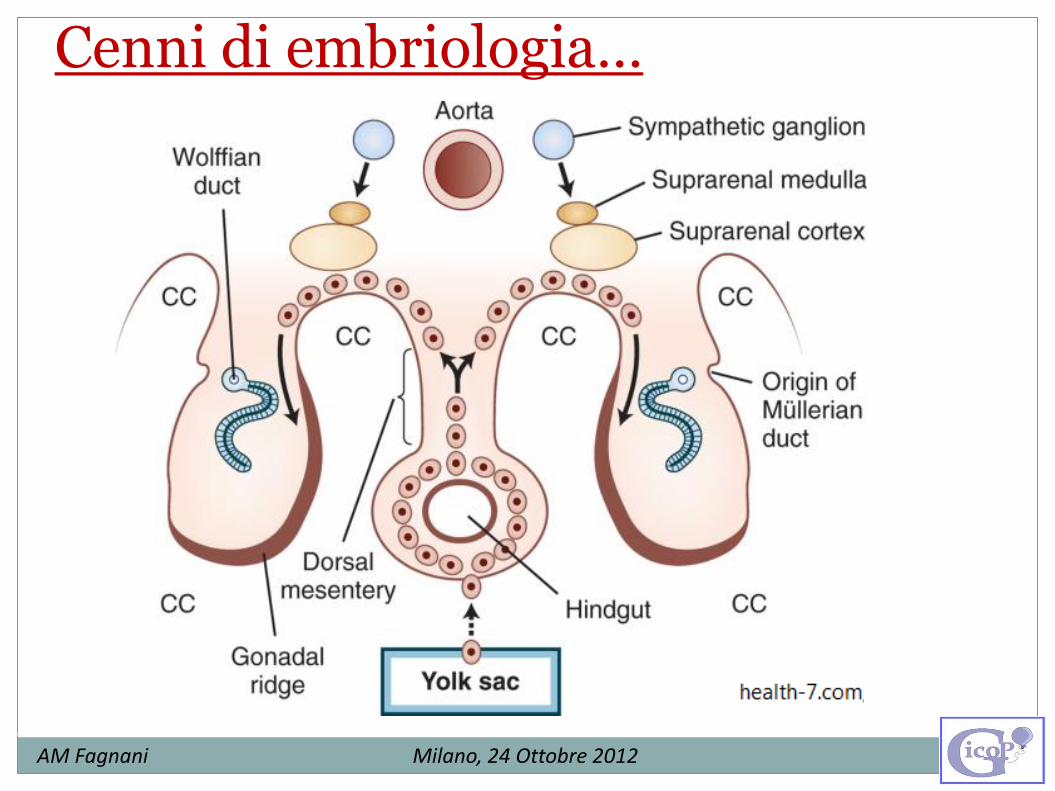
Cenni di embriologia…
AM Fagnani Milano, 24 Ottobre 2012
AM Fagnani Milano, 24 Ottobre 2012
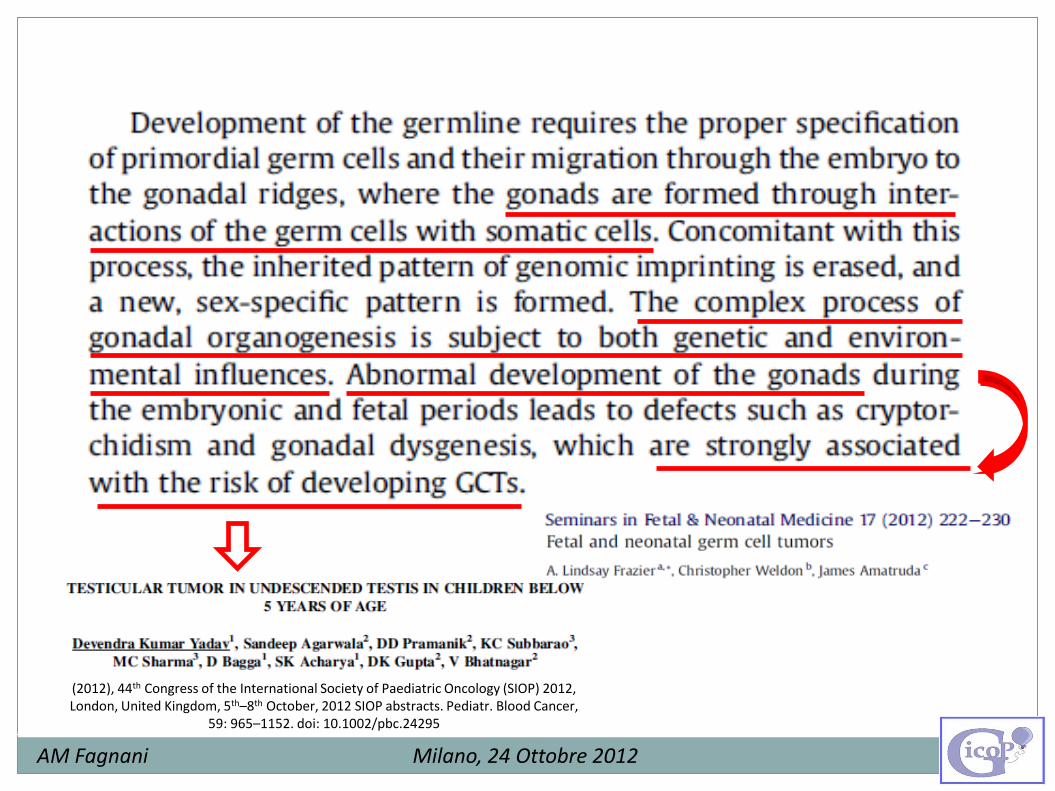
(2012), 44th Congress of the International Society of Paediatric Oncology (SIOP) 2012, London, United Kingdom, 5th–8th October, 2012 SIOP abstracts. Pediatr. Blood Cancer,
59: 965–1152. doi: 10.1002/pbc.24295
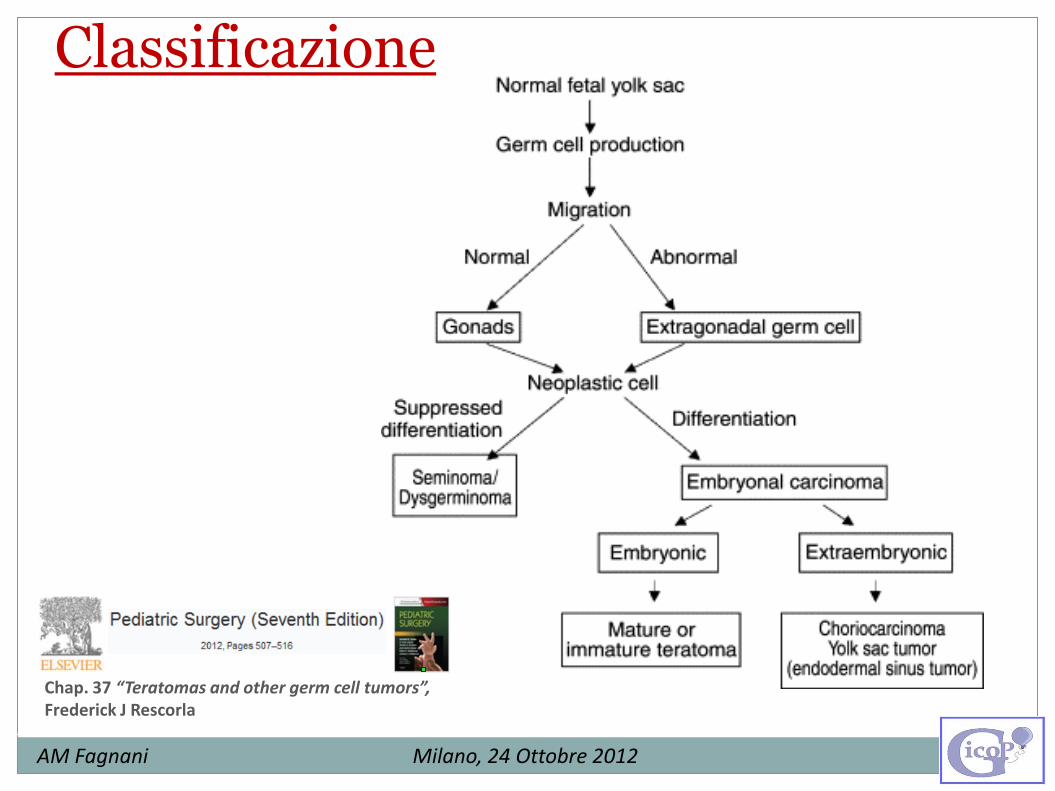
Classificazione
AM Fagnani Milano, 24 Ottobre 2012
Chap. 37 “Teratomas and other germ cell tumors”, Frederick J Rescorla
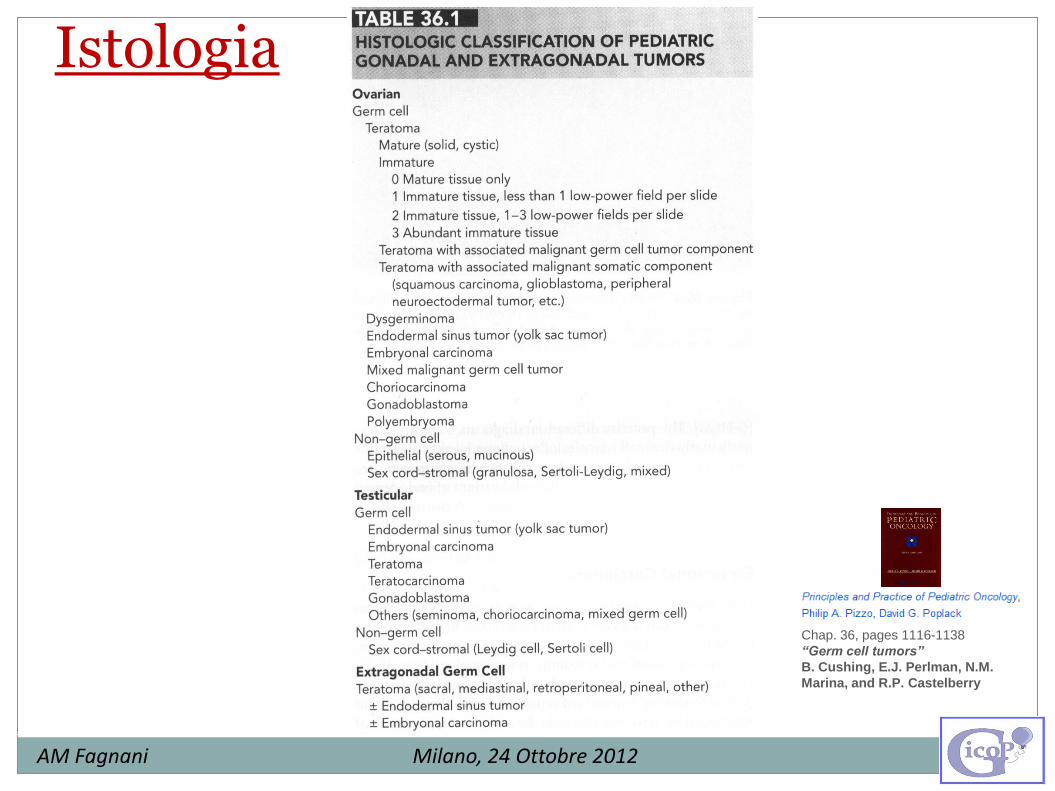
Istologia
AM Fagnani Milano, 24 Ottobre 2012
Chap. 36, pages 1116-1138
“Germ cell tumors”
B. Cushing, E.J. Perlman, N.M.
Marina, and R.P. Castelberry
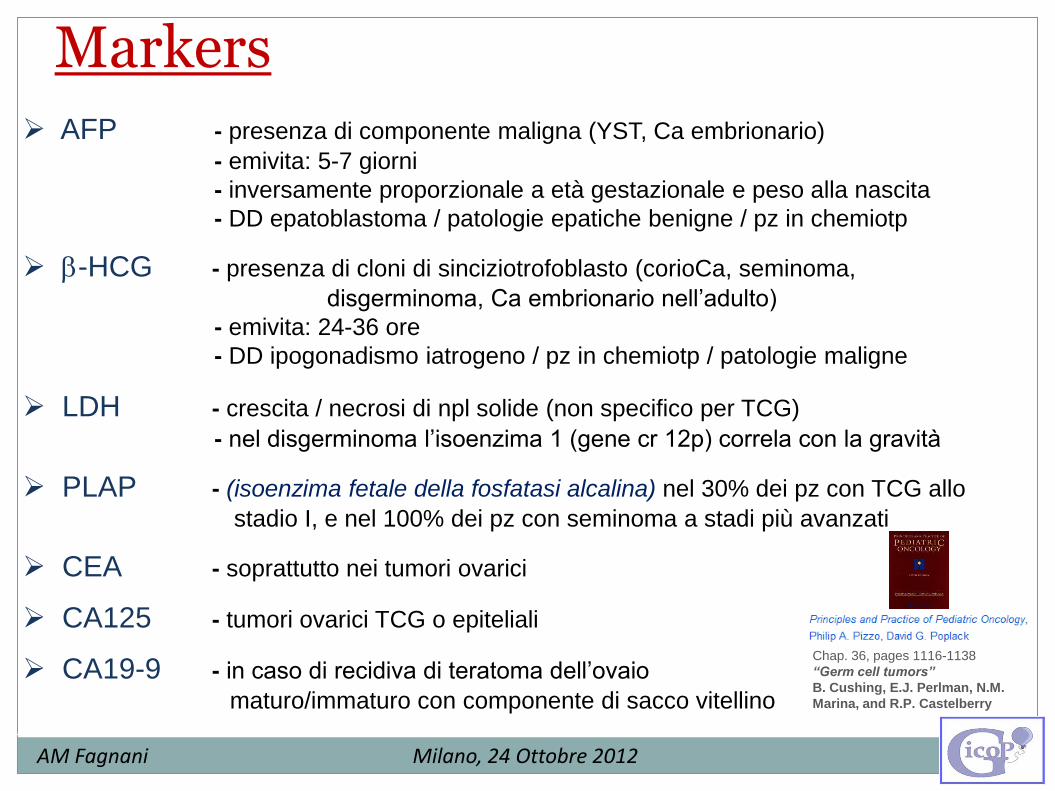
AFP - presenza di componente maligna (YST, Ca embrionario)
- emivita: 5-7 giorni
- inversamente proporzionale a età gestazionale e peso alla nascita
- DD epatoblastoma / patologie epatiche benigne / pz in chemiotp
-HCG - presenza di cloni di sinciziotrofoblasto (corioCa, seminoma,
disgerminoma, Ca embrionario nell’adulto)
- emivita: 24-36 ore
- DD ipogonadismo iatrogeno / pz in chemiotp / patologie maligne
LDH - crescita / necrosi di npl solide (non specifico per TCG)
- nel disgerminoma l’isoenzima 1 (gene cr 12p) correla con la gravità
PLAP - (isoenzima fetale della fosfatasi alcalina) nel 30% dei pz con TCG allo
stadio I, e nel 100% dei pz con seminoma a stadi più avanzati
CEA - soprattutto nei tumori ovarici
CA125 - tumori ovarici TCG o epiteliali
CA19-9 - in caso di recidiva di teratoma dell’ovaio
maturo/immaturo con componente di sacco vitellino
AM Fagnani Milano, 24 Ottobre 2012
Markers
Chap. 36, pages 1116-1138
“Germ cell tumors”
B. Cushing, E.J. Perlman, N.M.
Marina, and R.P. Castelberry
AM Fagnani Milano, 24 Ottobre 2012
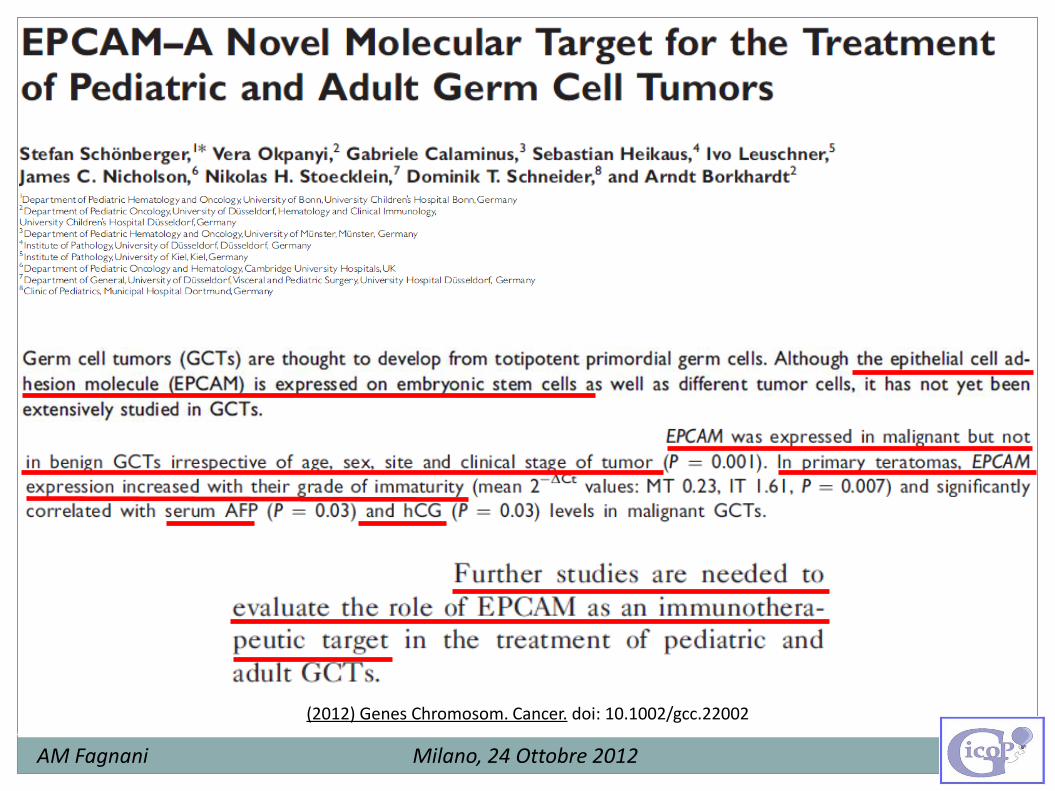
(2012) Genes Chromosom. Cancer. doi: 10.1002/gcc.22002

Fattori genetici Le aberrazioni genomiche dei TCG maligni in neonati e bambini sono in genere
diverse:
Adolescenti e adulti:
sovraespressione di 12p in tutti gli istotipi e sedi primarie (ovaie, testicoli,
extragonadiche)
Bambini < 4 anni:
- Tumori benigni: teratomi cellule diplodi con cariotipo normale
- Tumori maligni: prevalentemente tumori del sacco vitellino
cellule diploidi o tetraploidi
delezione di 1p e 6q (50%)
amplificazione di c-myc (piccola percentuale)
Le principali aberrazioni cromosomiche (1p-, 1q+, 6q- e 20q+) non sono altamente
specifiche per i TCG pediatrici.
AM Fagnani Milano, 24 Ottobre 2012
Chap. 37 “Teratomas and other germ cell tumors” Frederick J Rescorla
AM Fagnani Milano, 24 Ottobre 2012
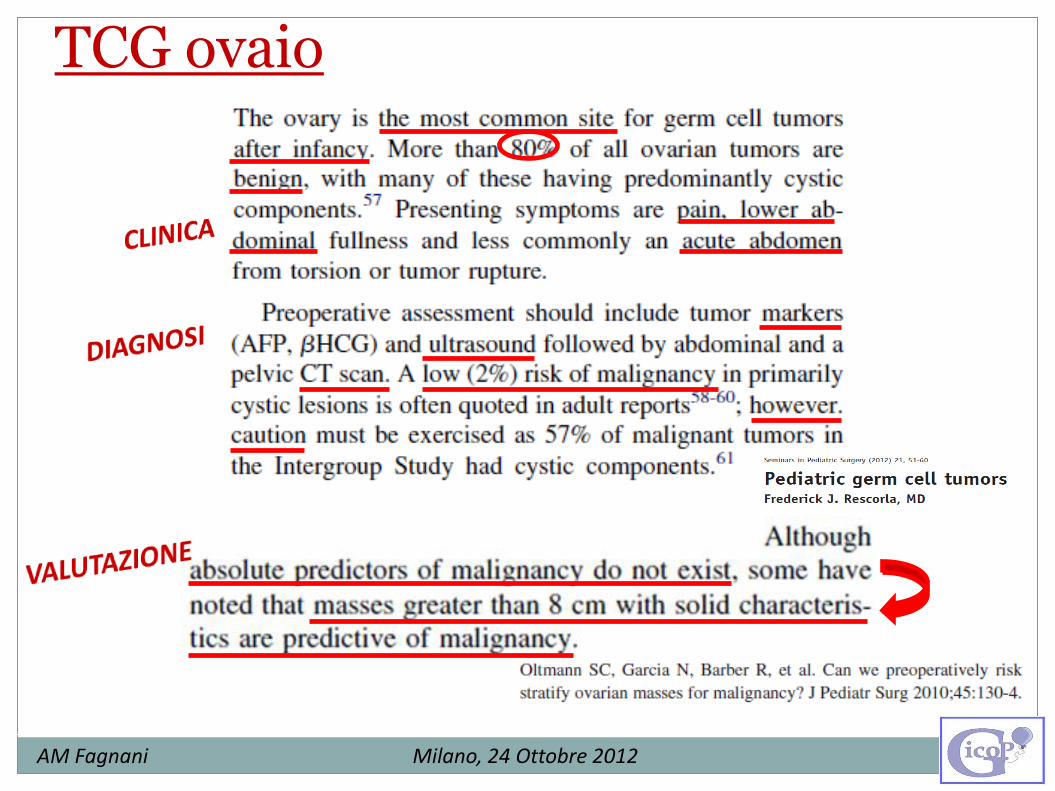
TCG ovaio
AM Fagnani Milano, 24 Ottobre 2012
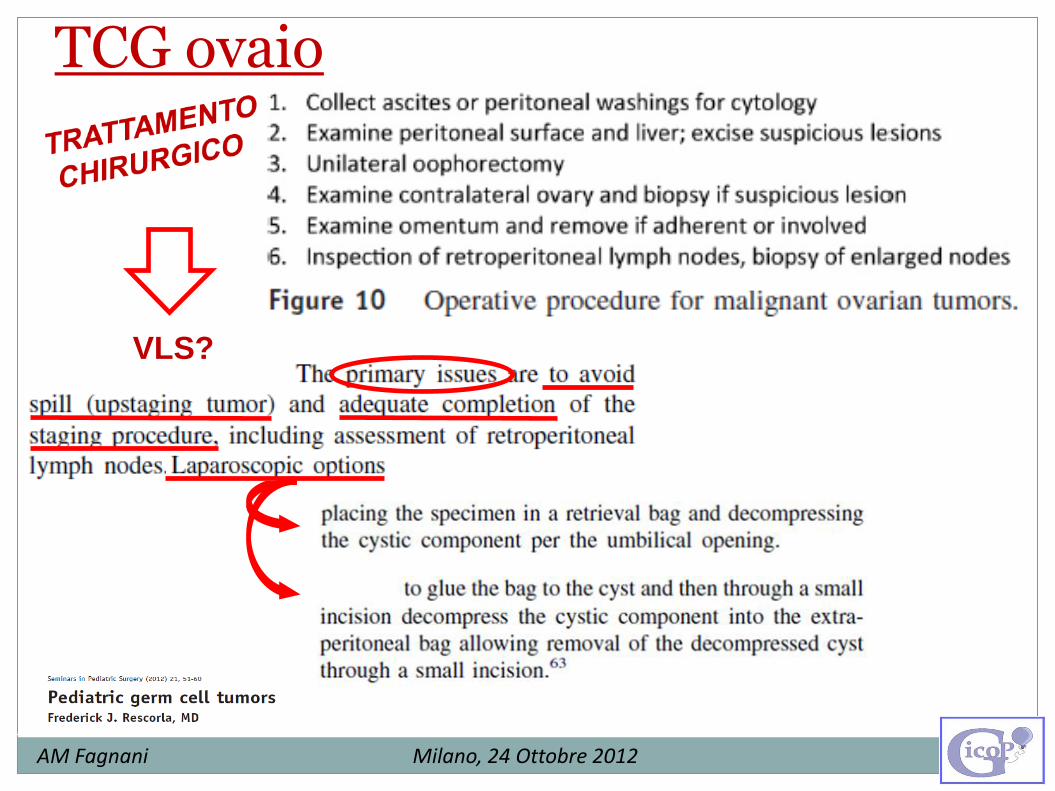
TCG ovaio
VLS?
AM Fagnani Milano, 24 Ottobre 2012
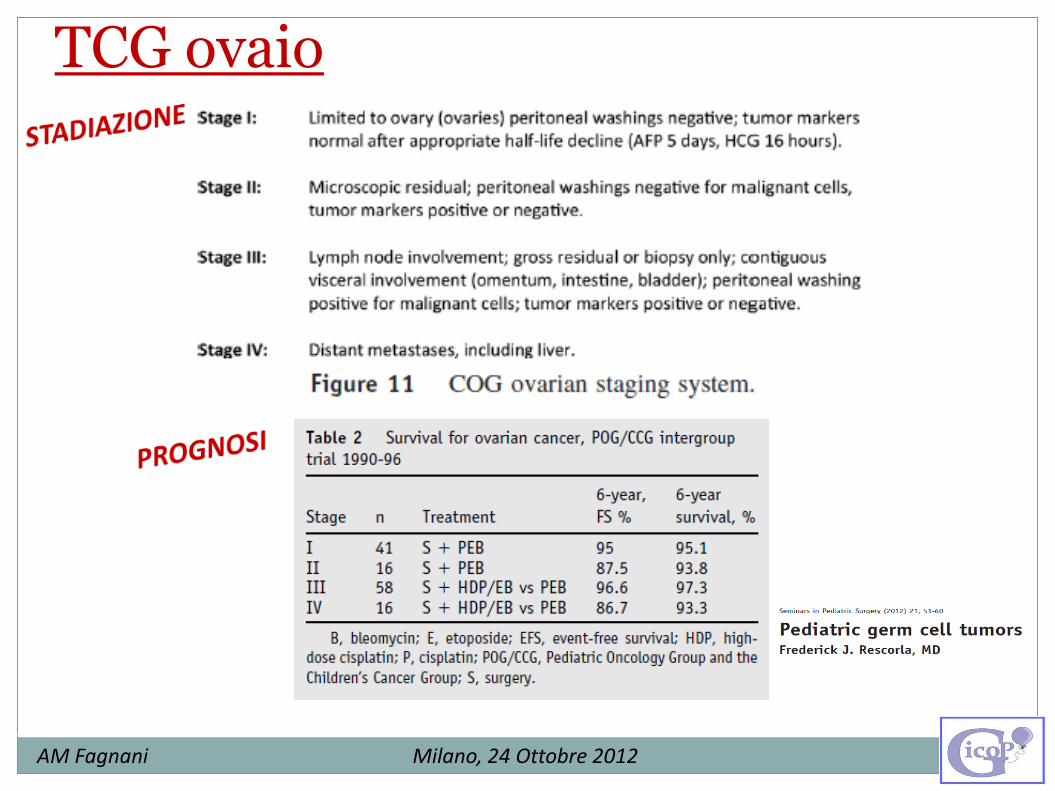
TCG ovaio
AM Fagnani Milano, 24 Ottobre 2012
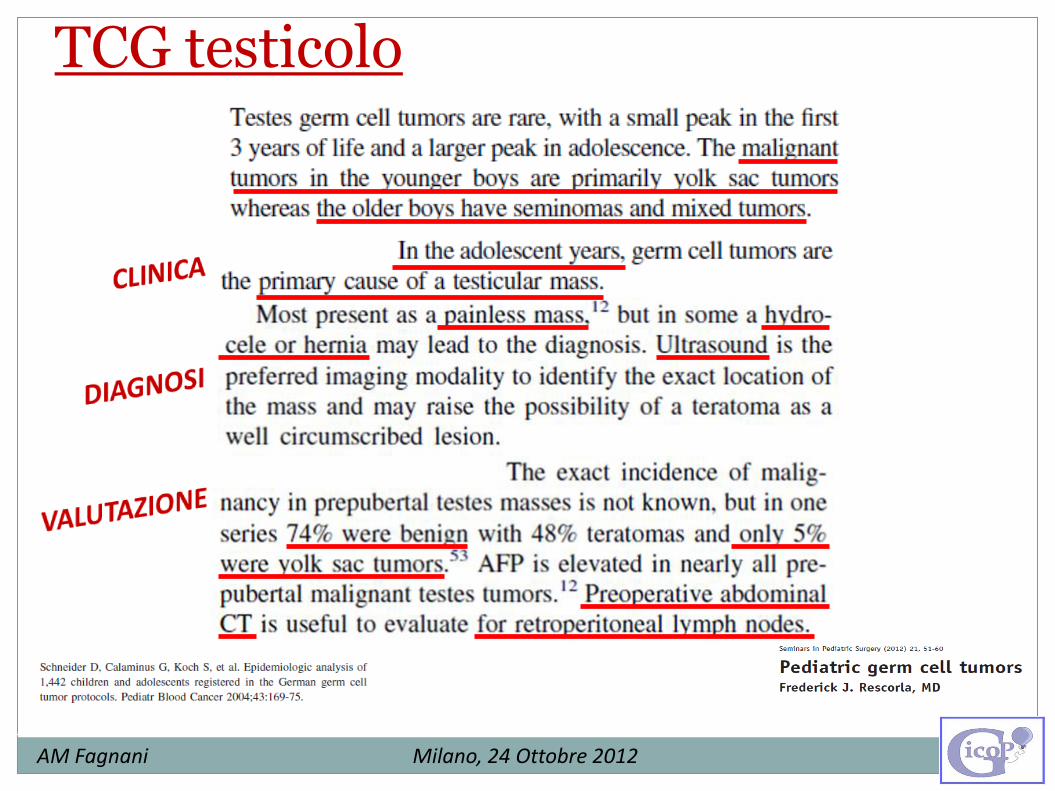
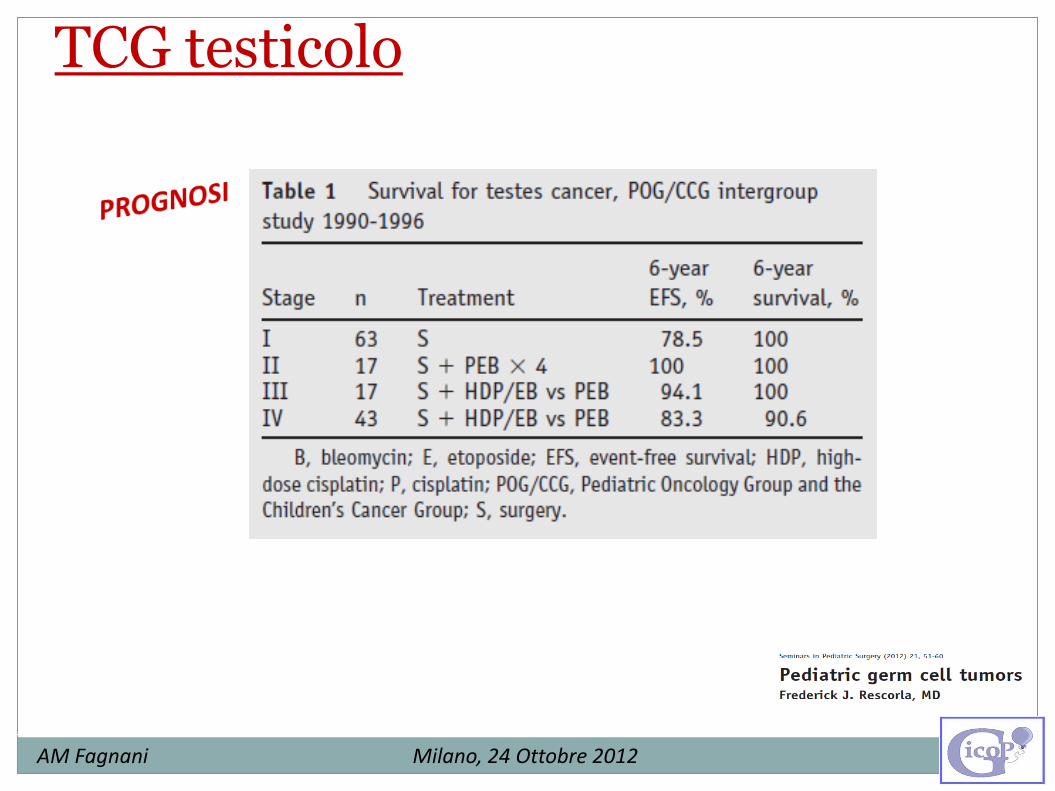
TCG testicolo
AM Fagnani Milano, 24 Ottobre 2012
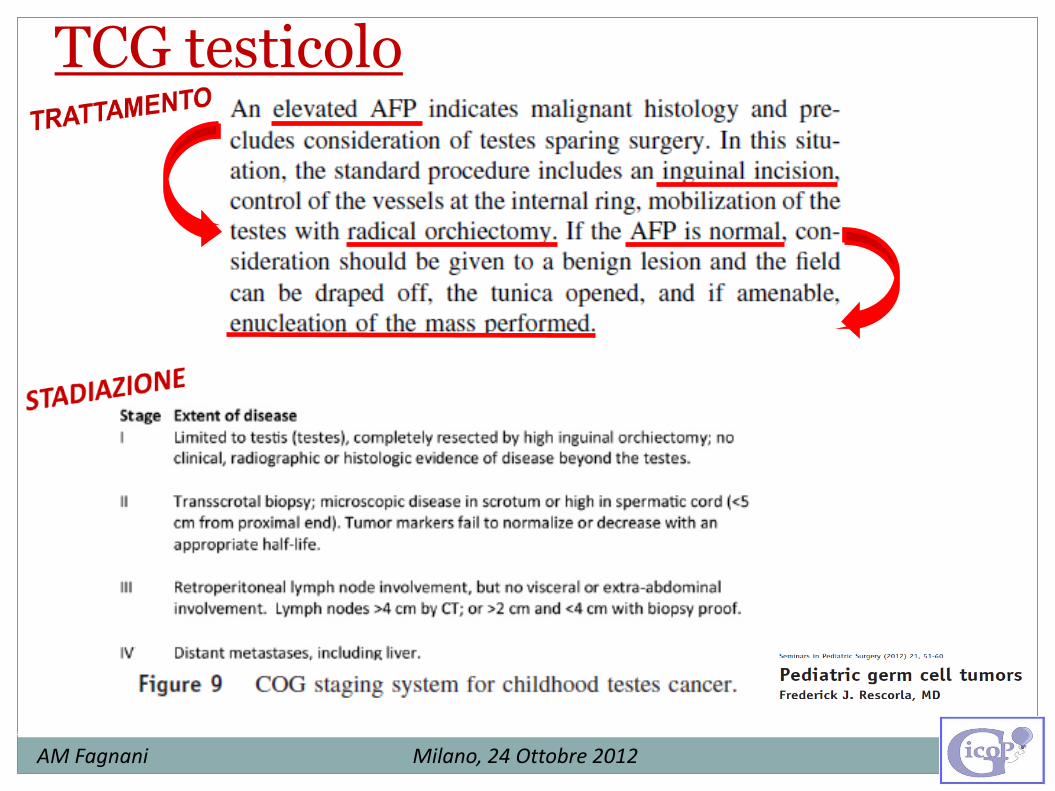
TCG testicolo
AM Fagnani Milano, 24 Ottobre 2012
TCG testicolo
AM Fagnani Milano, 24 Ottobre 2012
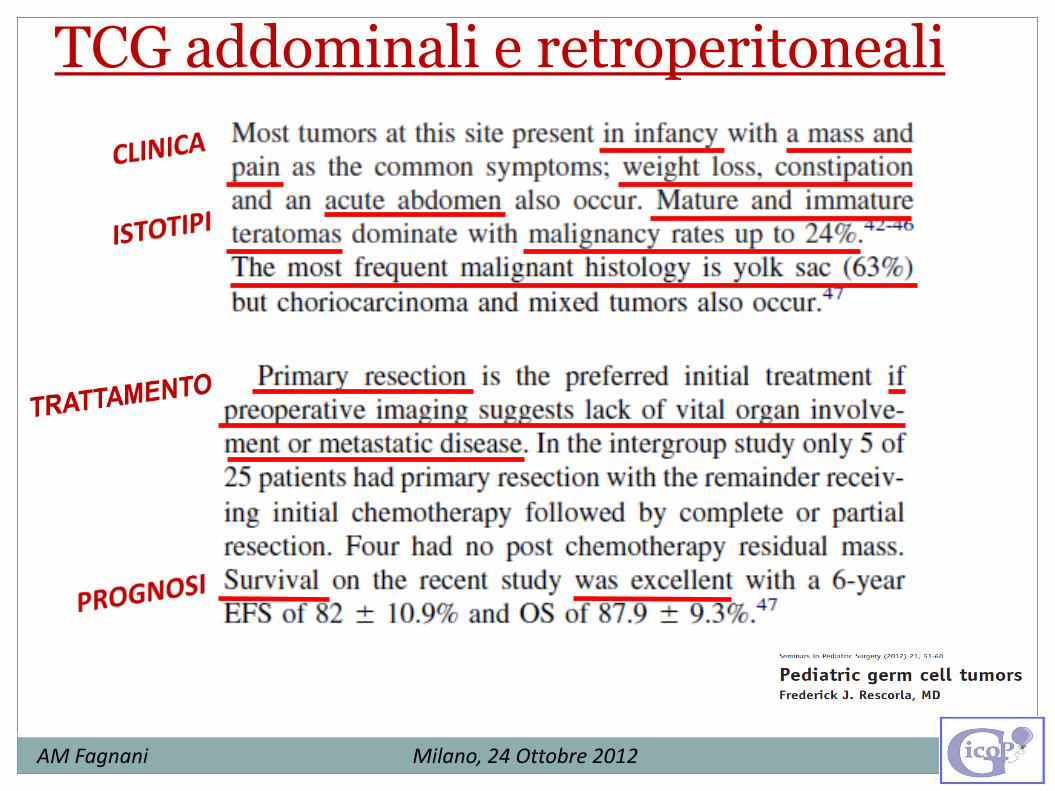
TCG addominali e retroperitoneali
AM Fagnani Milano, 24 Ottobre 2012
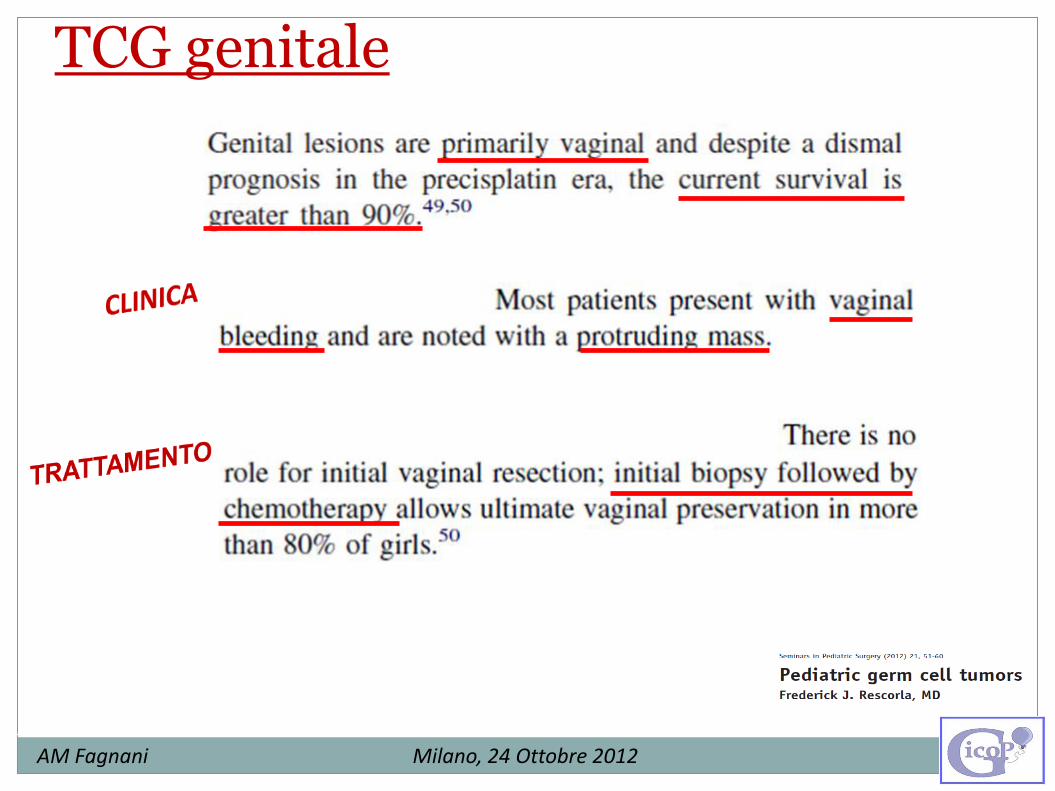
TCG genitale
AM Fagnani Milano, 24 Ottobre 2012
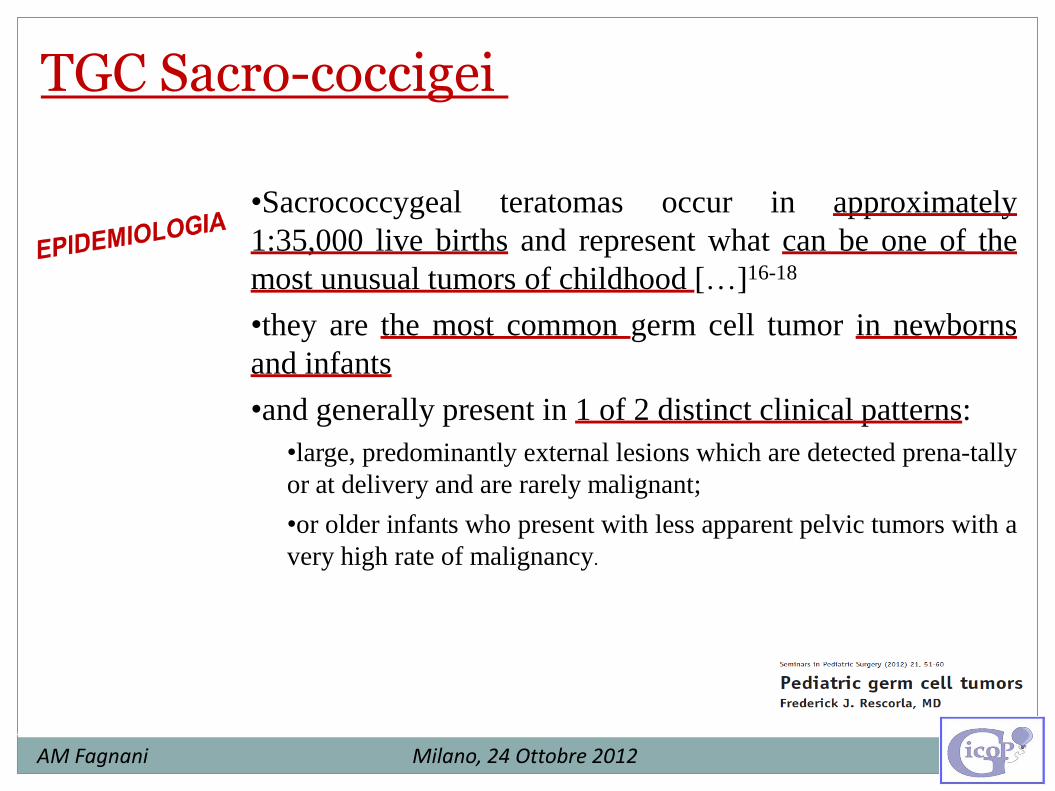
•Sacrococcygeal teratomas occur in approximately
1:35,000 live births and represent what can be one of the
most unusual tumors of childhood […]16-18
•they are the most common germ cell tumor in newborns
and infants
•and generally present in 1 of 2 distinct clinical patterns:
•large, predominantly external lesions which are detected prena-tally
or at delivery and are rarely malignant;
•or older infants who present with less apparent pelvic tumors with a
very high rate of malignancy.
TGC Sacro-coccigei

AM Fagnani Milano, 24 Ottobre 2012
•They can cause symptoms in utero secondary to the mass effect they
produce, polyhydramnios or shunting with high output cardiac failure,
and hydrops.
•Fetal resection or other fetal intervention (cyst drainage, laser ablation,
alcohol sclerosis)19,20 may be necessary.
•Adzick and colleagues21 performed the first successful fetal resection
and their recent recommendations include:
•fetal resection for high-output cardiac failure at less than 28 weeks’
gestation. 22
•Between 28 and 36 weeks, they recommend consideration of an ex utero
intrapartum therapy (EXIT) procedure in those with high-output cardiac
failure, tumor hemorrhage or impending labor attributable to
polyhydramnios as long as there is not maternal or placental compromise.
•If there is active labor, maternal mirror syndrome or placentomegaly after
28 weeks, emergency Cesarean delivery is recommended.
•Older infants usually present with symptoms related to bladder or
rectal displacement, often with very large pelvic masses.
•Association of presacral teratoma, anal stenosis, and sacral defects
as an autosomal-dominant condition: Currarino triad.24 (Ashcraft and
Holder23)
•The degree of pelvic and abdominal extension should be evaluated by:
− Ultrasound (US)
− Computed Tomography (CT)
− And/or Magnetic Resonance Imaging (MRI)
− In older infants evaluation of the chest for metastatic disease
(high rate of malignancy: 90%)
•AFP levels
AM Fagnani Milano, 24 Ottobre 2012

[…] based on Altman’s survey of the Surgical Section of the American
Academy of Pediatrics (Figure 4).27
•the malignancy rate was greater in the less-apparent lesions (types III
and IV).
•age was a significant factor on malignancy rate
Figure 4: Classification of sacrococcygeal
teratomas: type I (46.7%) predominantly
external; type II (34.7%); type III (8.8%)
visible externally put primarily pelvic and
abdominal; and, type IV (9.8%) entirely
presacral.
AM Fagnani Milano, 24 Ottobre 2012
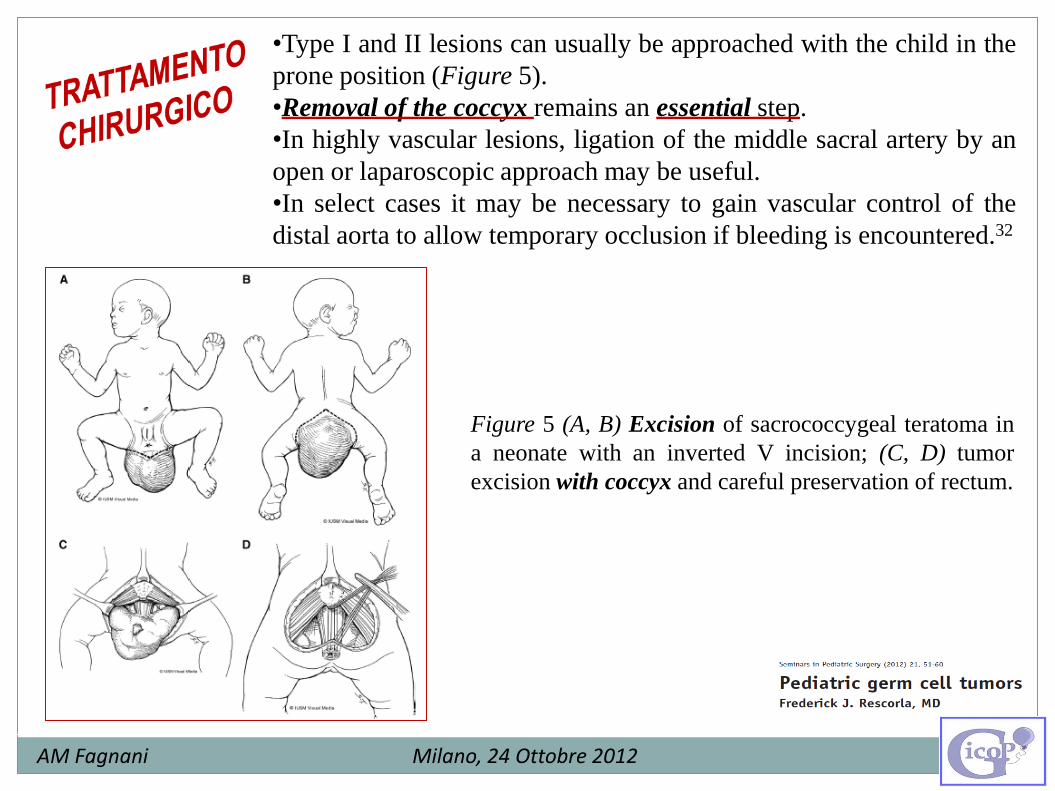
•Type I and II lesions can usually be approached with the child in the
prone position (Figure 5).
•Removal of the coccyx remains an essential step.
•In highly vascular lesions, ligation of the middle sacral artery by an
open or laparoscopic approach may be useful.
•In select cases it may be necessary to gain vascular control of the
distal aorta to allow temporary occlusion if bleeding is encountered.32
Figure 5 (A, B) Excision of sacrococcygeal teratoma in
a neonate with an inverted V incision; (C, D) tumor
excision with coccyx and careful preservation of rectum.
AM Fagnani Milano, 24 Ottobre 2012

AM Fagnani Milano, 24 Ottobre 2012
TCG sacro-coccigeo ulcerato

AM Fagnani Milano, 24 Ottobre 2012
AM Fagnani Milano, 24 Ottobre 2012

AM Fagnani Milano, 24 Ottobre 2012
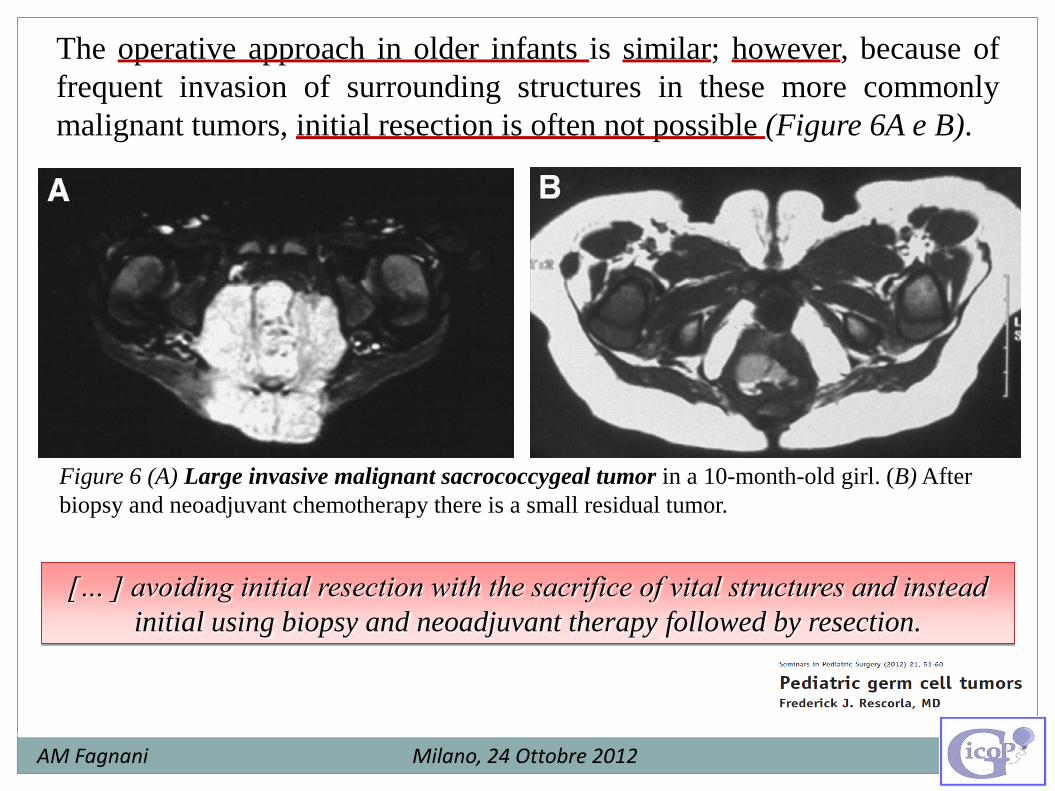
Figure 6 (A) Large invasive malignant sacrococcygeal tumor in a 10-month-old girl. (B) After
biopsy and neoadjuvant chemotherapy there is a small residual tumor.
The operative approach in older infants is similar; however, because of
frequent invasion of surrounding structures in these more commonly
malignant tumors, initial resection is often not possible (Figure 6A e B).
[… ] avoiding initial resection with the sacrifice of vital structures and instead
initial using biopsy and neoadjuvant therapy followed by resection.
AM Fagnani Milano, 24 Ottobre 2012
•Most neonatal tumors are mature or immature
teratomas that are treated with surgery and
observation.
•Follow-up should include:
• Serial AFP levels every 2-3 months to ensure
return to normal by 9 months
• Rectal examination every 3 months until age 3
years to evaluate for recurrence.
•Recurrent tumors are observed in 10%-20% of
initially benign tumors and 50% of these are
malignant.28,34
•Unfortunately, long-term sequelae, including
neuropathic bladder or bowel abnormalities, have
been observed in 11%-41% of survivors.35-37
AM Fagnani Milano, 24 Ottobre 2012
AM Fagnani Milano, 24 Ottobre 2012
TCG mediastinici
AM Fagnani Milano, 24 Ottobre 2012
TCG mediastinici

AM Fagnani Milano, 24 Ottobre 2012
TCG cervico-facciali
- Maggior prevalenza nel periodo perinatale diagnosi prenatale
- Generalmente teratomi maturi o immaturi
- Associati ad ostruzione delle vie aeree (1/3 dei casi)

AM Fagnani Milano, 24 Ottobre 2012
TCG cervico-facciali e mediastinici
Trattamenti Prenatali
- Lesioni isolate e non-comprimenti non compromettono il decorso
della gravidanza “wait and see” fino alla nascita
- Lesioni voluminose associate ad idrope possono portare a morte
fetale
Teratoma mediastinico complicato da idrope fetale, trattato con successo mediante aspirazione di liquido del tumore cistico Alla nascita: assenza di distress respiratorio In 3a giornata: asportazione del tumore Follow up chirurgico (6 m.): assenza di recidiva
AM Fagnani Milano, 24 Ottobre 2012
Teratoma pericardico fetale trattato con successo con shunt pericardio-amniotico
Pericardiocentesi a 32a, 33a e 34a settimana eg Exeresi in 3a giornata di vita: teratoma intrapericardico immaturo
Idrope fetale da esteso teratoma policistico mediastinico Associato ad ipoplasia polmonare e cardiaca Diagnosi istologica: teratoma immaturo (elementi epiteliali immaturi, mesenchimali, blastematosi)

TCG cervico-facciali Trattamenti Prenatali
Chirurgia fetale open
Criteri di eleggibilità: Età < 32a settimana Cariotipo normale Non malformazioni
anatomiche associate Non controindicazioni
materne
Lesioni voluminose + idrope: sopravvivenza 50%
AM Fagnani Milano, 24 Ottobre 2012

TCG cervico-facciali e mediastinici Trattamenti perinatali - EXIT
AM Fagnani Milano, 24 Ottobre 2012

Pervietà delle vie aeree garantita dall’intubazione naso/oro-
tracheale eseguita con successo
AM Fagnani Milano, 24 Ottobre 2012

EXIT pervietà vie aeree garantita tentativo di ventilazione se fallisce ECMO
Trattamenti perinatali EXIT + ECMO
AM Fagnani Milano, 24 Ottobre 2012

Trattamento postnatale
AM Fagnani Milano, 24 Ottobre 2012
AM Fagnani Milano, 24 Ottobre 2012
Grazie per l’attenzione