
Anticolinesterasici lavoro per ge
108
Fisiologia e farmacologia degli anticolinesterasici Claudio Melloni Anestesia e Rianimazione Ospedale di Faenza(RA)
-
Upload
claudio-melloni -
Category
Health & Medicine
-
view
253 -
download
2
description
anticholinesterases,muscle relaxant reversal,2004
Transcript of Anticolinesterasici lavoro per ge

Fisiologia e farmacologia degli anticolinesterasici
Claudio Melloni
Anestesia e Rianimazione
Ospedale di Faenza(RA)

Modello schematico del recettore Ach nicotinico(sec.Imoto,Alberts,Taylor)

Composizione delle subunità nel recettore Ach nicotinico

neostigmina

Condizioni accompagnate da up o down regolazione del recettore per Ach.
• Up regulation• Traumi midollari• Ictus• Ustioni
• Immobilità prolungata
• Prolungata esposizione a bloccanti nm.
• Sclerosi multipla• Sindr di Guillain Barrè
• Down regulation• Myastenia gravis• Avvelenamento da
anticolinesterasici • Avvelenamento da
organofosforici

Ach:
CH3-CO-O-(CH2)2-N+(CH3)3

H3C C O
O
CH2 CH2 N CH3
CH3
CH3+
Acetilcolina
Legame spezzato dall’Acetilcolinesterasi
Legame spezzato dall’Acetilcolinesterasi

Sito anionicoSito H donatore
Topologia dell’AchR visto dal lato sinaptico Lee C. Structure, conformation and action of neuromuscular blocking drugs. Br J Anaesth 2001; 87:755-69.

Canale ionico chiuso Canale ionico aperto da 2 molecole di Ach

Legame dell’ACH al substrato enzimatico,formazione dell’intermedio tetraedrale,perdita della colina e formazione dell’enzima acetilato ,idrolisi dell’enzima.

Il decametonio bloccaentrambi i siti anionici
Il vecuronium bloccasia il sito anionico che quello donante H di un unico recettore
Una grossa molecola Bisquaternaria blocca 2 siti anionici di 2 recettori

Modificazioni di forma;il decametonio preferisce una struttura lineare ,mentre Ach e SCC si piegano per le interazioni elettrostatiche fra i gruppi funzionali(methonium,gruppo carbonilico, O estereo).BJA 2001;87:755-69.


AChE
• Prevenzione dell’idrolisi dell’Ach a livello dei siti di trasmissione colinergica.
• Ne consegue che ACh rimane presente nella giunzione nm per un periodo di tempo + lungo e ciascuna molecola può legarsi ripetutamente con il recettore e quindi dare origine a maggiore corrente alla placca terminale …….

Legame dell’inibitore reversibile edrofonio e neostigmina,formazione dell’enzima carbamilato e idrolisi dell’enzima carbamilato

t/12 α(min)
T1/2 β(min)
V1(lt/kg) Vdss(Lt/kg) Cl (ml/kg/min)
3,4 77 0,2 0,7 9,1 prostigmina
6,7 113 0,3 1,1 8,6 piridostigmina
7,2 110 9,3 1,1 9,5 edrofonio
Variabili farmacocinetiche medie dei principali antichE. (da 99 a 102 ref)

Antagonismo dei miorilassanti

Presenza dei vapori….

Recovery parameters following neostigmine administration(Reid J, Breslin DS,Mirakhur R, Hayes A.Neostigmine antagonism of rocuronium block during anesthesia with sevoflurane,isoflurane or propofol.Can.Anesth.J. 2001:48 :351-55)
0
24
6
8
10
12
14
16
18
20
min
propcont
propstop
sevocont
sevostop
isocont
isostop
onset
Tof 0.80
RI
pts at 0.8 tof at 15 min
6 groups ,20 eachRocuronium,Force,neo at tof 25%!
*
***

TOF vs time after neostigmine 40 µgr/kg (from T1 25%);control(fent/N2O),isoflurane stopped,isoflurane continued (1.25%)Baurain MJ, d'Hollander AA,Melot C, Dernovoi BS,Barvais L.Effects of residual concentrations of isoflurane on the reversal of vecuronium induced neuromuscular blockade.Anesthesiology 1991:71:474- )

Valori del tetanic fade (stimolazione a 50 Hz sn,100 Hz dx)dopo 15 min dalla somministrazione di neostigmina 40 microgr/kg Baurain MJ, d'Hollander AA,Melot C, Dernovoi BS,Barvais L.Effects of residual concentrations of isoflurane on the reversal of vecuronium induced neuromuscular blockade.Anesthesiology 1991:71:474- )

• Insomma,continuare la soministraz del vapore ritarda la ripresa nm anche dopo rovesciamento……

Neostigmina vs edrofonio…..

Antagonism of atracurium or cisatracurium nm blockade(at T1 10%)with various dosages of neostigmine(fent,tps,N2O,isof anesth;Accel.) Naguib M,Riad W.Dose response relationship for edrophonijm and neostigmine antagonism of atracurium and cisatracurium induced neuromuscular block.Can.Anaesth.J 2000;47:1074-1081

Antagonism of atracurium or cisatracurium nm blockade(at T1 10%)with various dosages of edrophonium (fent,tps,N2O,isof anesth;Accel.) Naguib M,Riad W.Dose response relationship for edrophonijm and neostigmine antagonism of atracurium and cisatracurium induced neuromuscular block.Can.Anaesth.J 2000;47:1074-1081

Neostigmine vs edrophonium reversal of atracurium or cisatracuriun nm, blockade

Mean first twitch height vs time after administration of various doses of neostigmine and edrophonium starting from T 1 10% following atracurium and vecuronium Smith, CE, Donati F., Bevan DR.Dose Response Relationships for Edrophonium and Neostigmine as Antagonists of ‑Atracurium and Vecuronium neuromuscular Blockade.Anesthesiology 1989;71: 37-43.
Inspired enflurane concentration maintained at 0.5-1%

Dose response relationship of first twitch and TOF assisted recovery 5 and 10 min. following administration of the antagonist as a function of the dose of neostigmine and edrophonium following atracurium and vecuronium. Smith, CE, Donati F., Bevan DR.Dose Response Relationships for Edrophonium and Neostigmine as ‑Antagonists of Atracurium and Vecuronium Neuromuscular Blockade.Anesthesiology 1989;71: 37-43.
Inspired enflurane concentration maintained at 0.5-1%

Effect on T1 of 2 doses of neostigmine and edrophonium following atracurium and vecuronium Smith, CE, Donati F., Bevan DR.Dose Response Relationships for Edrophonium and Neostigmine ‑as Antagonists of Atracurium and Vecuronium Neuromuscular Blockade.Anesthesiology 1989;71: 37-43.
0
10
20
30
40
50
60
70
80
90
100
neo 0.02mg/kg
neo 0.04mg/kg
edroph 0.5mg/kg
edroph 1mg/kg
atrac at 5'
atrac at 10'
vecu at 5'
vecu at 10'
Inspired enflurane concentration maintained at 0.5-1%

Effect on Tof of 2 doses of neostigmine and edrophonium following atracurium and vecuronium Smith, CE, Donati F., Bevan DR.Dose Response Relationships for Edrophonium and Neostigmine as Antagonists of Atracurium and ‑Vecuronium Neuromuscular Blockade.Anesthesiology 1989;71: 37-43.
0
10
20
30
40
50
60
70
80
neo 0.02mg/kg
neo 0.04mg/kg
edroph 0.5 mg/kg
edroph 1mg/kg
atrac at 5'
atrac at 10'
vecu at 5'
vecu at 10'
Inspired enflurane concentration maintained at 0.5-1%

Neo vs edrofonio e profondità del blocco nm.

Ist twitch height vs dose 10 min. after neostigmine or edrophonium administered at 90
or 99% block.

Conclusione 1
• La dose giusta di neostigmina è…………
• Meditate gente meditate………………

Relationship between dose of neostigmine and percentage recovery during continuous infusion of vecuronium(filled circle) or pancuronium(empty circle)

Insomma,l’antagonismo dipende da:
• Profondità di blocco al momento della somministrazione dell’antagonista
• Presenza o meno di potenzianti nmb.
• Tipo di antagonista somministrato
• Tipo di miorilassante somministrato
• Dose dell’antagonista somministrato
• end point scelto;T1/Tc,Tof,ecc.

Conclusione 2
• E’ meglio somministrare gli antidoti quando la ripresa nm è iniziata
• È meglio cessare la somministrazione degli alogenati ( e monitorizzare la % et)…….

Effetti collaterali degli anti AchE

Effetti fisiologici della presenza di Ach
• Bradicardia
• Salivazione
• Iperperistalsi
• Secrezioni bronchiali

Pericoli degli AntiAchE: arresto cardiaco
• Bjerke, Richard J., MD; Mangione, Michael P.Asystole after intravenous neostigmine in a heart transplant recipinet.Can.Anaesth.J. 2001;48:305-07.
• Purpose: To describe a heart transplant recipient who developed asystole after administration of neostigmine which suggests that surgical dennervation of the heart may not permanently prevent significant responses to anticholinesterases.
• Clinical features: A 67-yr-old man, 11 yr post heart transplant underwent left upper lung lobectomy. He developed asystole after intravenous administration of 4 mg neostigmine with 0.8 mg glycopyrrolate for reversal of the muscle relaxant. He had no history of rate or rhythm abnormalities either prior to or subsequent to the event.
• Conclusion: When administering anticholinesterase medications to heart transplant patients, despite surgical dennervation, one must be prepared for a possible profound cardiac response.

Pericoli degli ACHE:FA con rapida risposta ventricolare…..
• Kadoya, TSA, Aoyama K, Takenaka I.Development of rapid atrial fibrillation with wide QRS complex after neostigmine in a patient with intermittent WPW stndrome.BJA 1999;83:815-818
•
• 1Department of Anaesthesia, Nippon Steel Yawata Memorial Hospital, 1-1-1 Harunomachi, Yahatahigashi-ku,
• ABSTRACT: We report the case of a 67-yr-old man with intermittent Wolff-Parkinson-White (WPW) syndrome in whom neostigmine produced life-threatening tachyarrhythmias. The patient was scheduled for microsurgery for a laryngeal tumour. When he arrived in the operating room, the electrocardiogram showed normal sinus rhythm with a rate of 82 beat min-1 and a narrow QRS complex which remained normal throughout the operative period. On emergence from anaesthesia, the sinus rhythm (87 beat min-1) changed to atrial fibrillation with a rate of 80–120 beat min-1 and a normal QRS complex. We did not treat the atrial fibrillation because the patient was haemodynamically stable. Neostigmine 1 mg without atropine was then administered to antagonize residual neuromuscular block produced by vecuronium. Two minutes later, the narrow QRS complexes changed to a wide QRS complex tachycardia with a rate of 110–180 beat min-1, which was diagnosed as rapid atrial fibrillation. As the patient was hypotensive, two synchronized DC cardioversions of 100 J and 200 J were given, which restored sinus rhythm. No electrophysiological studies of anticholinesterase drugs have been performed in patients with WPW syndrome. We discuss the use of these drugs in this condition.

Pericoli degli antiAchE:broncocostrizione
• Shibata O,Tsuda A,Makita T, Iwanaga S,Hara T,Shibata S,Sumikawa K. Contractile and phosphadytilinositol responses of rat trachea to anticholinesterase drugs.Can.Anaesth.J.1998;45:1190-95Purpose: Some anticholinesterases (anti-ChE) such as neostigmine and pyridostigmine but not edrophonium, stimulate phosphaticlylinositol (PI) response. Although a direct relationship was suggested between the increase in PI response and airway smooth muscle contraction, there are no data regarding the effects of anti-ChE drugs on airway smooth muscle. Thus, we examined the contractile properties and PI responses produced by anti-ChE drugs.
• Methods: Contractile response. Rat tracheal ring was suspended between two stainless hooks in Krebs-Henseleit (K-H) solution. (1) Carbachol (CCh), anti-ChE drugs (neostigmine, pyridostigmine, edrophonium) or DMPP (a selective ganglionic nicotinic agonist) were added to induce active contraction. (2) The effects of 4-diphenylacetoxy-N-methyl-piperidine methobromide (4-DAMP), an M3 muscarinic receptor antagonist, on neostigmine- or pyridostigmine-induced contraction of rat tracheal ring were examined. (3) Tetrodotoxin (TTX) was tested on the anti-ChE drugs-induced responses. PI response. The tracheal slices were incubated in K-H solution containing LiCl and 3[H]myo-inositol in the presence of neostigmine or pyridostigmine with or without 4-DAMP, an M3 muscarinic receptor antagonist. 3[H]inositol monophosphate (IP1) formed was counted with a liquid scintillation counter.
• Results: Carbachol (0.1 mM), neostigmine. (1 mM), pyridostigmine (10 mM) but not edrophonium or DMPP, caused tracheal ring contraction. 4-DAMP, but not tetrodotoxin, inhibited neostigmine and pyridostigmine-induced contraction. Neostigmine- or pyridostigmine-induced IP1 accumulation was inhibited by 4-DAMP.
• Conclusions: The data suggest that anti-ChE drugs activate the M3 receptors at the tracheal effector site.

Schema delle afferenze parasimpatiche a livello tracheale

Effetti contrattili di antiACHE,carbacolo e dimetilfenilpiperazinio sugli anelli tracheali di ratto.Shibata O,Tsuda A,Makita T, Iwanaga S,Hara T,Shibata S,Sumikawa K. Contractile and phosphadytilinositol responses of rat trachea to anticholinesterase drugs.Can.Anaesth.J.1998;45:1190-95

NEOSTIGMINE AND PONV

Tramèr, M. R. Fuchs-Buder, T..Omitting antagonism of nm block:effect on PONV and risk of residual paralysis.A systematic review.BJA 1999;82:379-386
• A systematic search (MEDLINE, EMBASE, Biological Abstracts, Cochrane library, reference lists and hand searching; no language restriction, up to March 1998) was performed for relevant randomized controlled trials. In eight studies (1134 patients), antagonism with neostigmine or edrophonium was compared with spontaneous recovery after general anaesthesia with pancuronium, vecuronium, mivacurium or tubocurarine. On combining neostigmine data, there was no evidence of an antiemetic effect when it was omitted. However, the highest incidence of emesis with neostigmine 1.5 mg was lower than the lowest incidence of emesis with 2.5 mg. These data suggested a clinically relevant emetogenic effect with the higher dose of neostigmine in the immediate postoperative period but not thereafter.
• Numbers-needed-to-treat to prevent emesis by omitting neostigmine compared with using it were consistently negative with 1.5 mg, and consistently positive (3–6) with 2.5 mg. There was a lack of evidence for edrophonium. In two studies, three patients with spontaneous recovery after mivacurium or vecuronium needed rescue anticholinesterase drugs because of clinically relevant muscle weakness (number-needed-to-harm, 30). Omitting neostigmine may have a clinically relevant antiemetic effect when high doses are used. Omitting antagonism, however, introduces a non-negligent risk of residual paralysis even with short-acting neuromuscular blocking agents.

Risk of omitting neostigmine….
• Residual paralysis!!!

Nelskylä, K.; Yli-Hankala, A.; Soikkeli, A.; Korttila, K.Noestigmine with glycopirrolate does not increase the incidence and severity of PONV in outpatients undergoing gynecological laparoscopy.BJA 1998;81:757.-760
• • ABSTRACT: • We studied 100 healthy women undergoing outpatient gynaecological laparoscopy in
a randomized, double-blind and placebo-controlled study to evaluate the effect of neostigmine on post-operative nausea and vomiting (PONV). After induction of anaesthesia with propofol, anaesthesia was maintained with sevoflurane and 66% nitrous oxide in oxygen. Mivacurium was used for neuromuscular block. At the end of anaesthesia, neostigmine 2.0 mg and glycopyrrolate 0.4 mg, or saline, was given i.v. The incidence of PONV was evaluated in the postanaesthesia care unit, on the ward and at home. The severity of nausea and vomiting, worst pain, antiemetic and analgesic use, times to urinary voiding and home readiness were recorded. During the first 24 h after operation, 44% of patients in the neostigmine group and 43% in the saline group did not have PONV. We conclude that neostigmine with glycopyrrolate did not increase the occurrence of PONV in this patient group.

Watcha MF, Safavi FZ, McCulloch DA, et al. Effect of antagonism of mivacurium-induced
neuromuscular block on postoperative emesis in children. Anesth Analg 1995; 80:713-7.
0
10
20
30
40
50
60
%
PONV antiemeticinecess
Vomito entro24 ore
Incidenza di PONV nella PACU
neostigmine 70micrograms/kg +glycopyrrolate 10micrograms/kg,
edrophonium 1 mg/kg +atropine 10micrograms/kg.
saline
**

Ding Y,Fredman B, White PF.Use of mivacurium during laparoscopic surgery:effect of reversal
drungs on postoperaive recovery.Anesth Analg 1994; 78:450–4
• outpatient laparoscopic tubal ligation • 60 healthy, nonpregnant women. • midazolam / fentanyl/tps• succ 1 mg/kg (Group I) vs mivacurium 0.2 mg/kg
(Groups II and III)• Anesthesia maintained with isoflurane (0.5%-2%
+67% N2O• Muscle relaxation maintained in all three groups with
intermittent bolus doses of mivacurium, 2–4 mg, IV.• In Group III, residual neuromuscular block reversed
with neostigmine 2.5 mg +glycopyrrolate, 0.5 mg,

Effetti collat dello studio di Ding et al.
0
10
20
30
40
50
60
70
80
%
nausea vomit antiemetici neck pain shoulder pain
succi/miva/no antag
miva/miva/ no antag
miva/miva/antag
*
*
*
*

Boeke AJ, de Lange JJ, van Druenen B, Langemeijer JJM. Effect of antagonizing residual neuromuscular block by neostigmine and atropine on postoperative vomiting. Br J Anaesth 1994; 72:654-6.
• 80 patients undergoing outpatient surgery
• allocated randomly to two groups: in group A residual neuromuscular block was antagonized with a mixture of neostigmine 1.5 mg and atropine 0.5 mg; in group B spontaneous recovery was allowed.
• patients assessed after operation in hospital and 24 h after discharge.

Boeke AJ, de Lange JJ, van Druenen B, Langemeijer JJM. Effect of antagonizing residual neuromuscular block by neostigmine and atropine on postoperative vomiting. Br J Anaesth 1994; 72:654-6.
• inguinal hernia repair & stripping of the major saphenous vein of one leg.
• no premed• atropine 0.5 mg i.v.• anaesthesia : tps 5–8 mg/kg + fent 2 µg/kg• vecu.0.1 mg kg-1. • 100% oxygen * 3 min• iot• IPPV 66% N2O/ haloth. 0.5%

Incid.di PONV nello studio di Boeke et al.
02468
101214161820
num.paz
PONV RR PONV II
antag
non antag
*

Boeke et al.;risultati e conclusioni.
• We found a significant difference (P < 0.05) in requirements for antiemetic therapy with a smaller need in the group which received neostigmine (in group A four of 40 patients received an antiemetic compared with 12 in group B).
• no significant difference in frequency of nausea or vomiting between the two groups.
• The incidence of postoperative nausea was 14 in group A and 18 in group B and the number of patients with postoperative vomiting was 10 in group A and 15 in group B.
• In conclusion, as there was an increase in the number of patients requiring antiemetics in group B compared with group A (P < 0.05), the results of this study may suggest an antiemetic effect of neostigmine.

Kao YJ, Mian T, McDaniel KE, et al. Neuromuscular blockade reversal agents induce postoperative nausea
and vomiting [abstract] Anesthesiology 1992; 77(Suppl):A1120.
0
510
1520
2530
35
%
PONV
Minilap per PPTL.Tps/succi/iot/fent/isof/N2O.Stomaco svuotato.Atrac 0.15 mg/kg.
no antag
A 0.15 micrG/kg + edroph 1mg/kg
A 0.15 micrg/kg+neo 0.05mg/kg
A 0.15 icrg/kg+pirido 0.25mg/KG
*

Antagonism of mivacurium block
• Savarese et al:neo accelerates recovery form mivac by 40%
• Kaoo:neo may delay complete recovery from deep mivac block
• Baurain,Naguib:neo accelerates recovery fron mivac block by 7-9 min vs 15-17 spont.
• Devcic:mean recovery accelerated by neo,but variability high:

Antagonism of deep mivacurium block.
0
5
10
15
20
nin
T125%
T150%
T175%
TOF25%
TOF50%
TOF75%
placebo
placebo
edrophonium
neostigmine
Dott. Melloni:
cDevcic et al.Anesthesia Analgesia,1995,81:1005-1009
Dott. Melloni:
cDevcic et al.Anesthesia Analgesia,1995,81:1005-1009

• Enzymatic Antagonism of Mivacurium-induced Neuromuscular Blockade by Human Plasma Cholinesterase. Anesthesiology. 83(4):694-701, October 1995.
Fisher, Dennis M. ,Szenohradszky, Janos , Hart, Paul S. .Antagonism of Residual Mivacurium Blockade: Setting the Record Straight. Anesthesiology. 84(6):1527-1528, June 1996.
• . Szenohradszky, Janos ,Fogarty, Declan Kirkegaard-Nielsen, Hans , Brown, Ronald, Sharma, Manohar L,Fisher, Dennis M. Effect of Edrophonium and Neostigmine on the Pharmacokinetics and Neuromuscular Effects of Mivacurium. Anesthesiology. 92(3):708-714, March 2000.

Effetti analgesici
• a muscarinic presynaptic inhibition of glutamatergic afferents, similar to how it has been described in the neostriatum. An important prerequisite for the effectiveness of neostigmine is a tonic cholinergic activity.

DTC PANC VECU ATRAC ROCU MIVA
Neostigmina
ED50 17±1 13±2 10±1 10±1 17±1 2±0.1
ED80 45±3 45±6 24±2 22±2 33±1 5±0.1
Edrofonio
ED50 270±27 170±24 180±50 110±30 161±10 3±0.1
ED80 880±93 680±102 460±13 440±110 690±10 9±0.1
Rapporti di potenza antagonistica per neostigmina e edrofonio (da Donati AA 1989,Smith
Anesthesiology 1989,Naguib Anesthesiology 1993,Naguib BJA 1993)

Comportamento suggerito per l’antagonismo dei miorilassanti a lunga e media durata di azione secondo le risposte al Tof
TOF esaurimento farmaco dose
Twitch visibili
nessuno Posponi antagonismo
Finchè almeno 1 o 2 contrazioni visibili!!
1-2 ++++ neostigmina 0.07 mg/kg
3-4 +++ neostigmina 0.04 mg/kg
4 ++ edrofonio 0.5 mg/kg
4 +/- edrofonio 0.25

FINE

• Szenohradszky, Janos, M.D.*; Fogarty, Declan, M.D.†; Kirkegaard-Nielsen, Hans, M.D.‡; Brown, Ronald, B.S.§; Sharma, Manohar L., Ph.D.ï÷; Fisher, Dennis M.,effect of edrophonium and neostigmine on the pharmacokinetics amnd neuromuscular effectsof mivacurium . Anesthesiology 2000;92:708-
• ABSTRACT: Background: Previous studies demonstrated that both edrophonium and neostigmine affect mivacurium's pharmacokinetics, thereby potentially affecting its recovery profile. However, those studies were not clinically relevant because mivacurium was still infused after the antagonists were given. In the present study, the authors gave antagonists (or placebo) after discontinuing a mivacurium infusion, thereby obtaining data that are more clinically relevant.
• Methods: In 18 patients, mivacurium was infused at 10 mg × kg-1 × min-1 for 40 min, the infusion was discontinued for 15 min and then restarted at the same rate for another 40 min. Patients were randomized to receive 500 mg/kg edrophonium, 50 mg/kg neostigmine, or saline at discontinuation of the second infusion; all subjects received 1 mg atropine. Plasma was sampled during the final 10 min of each infusion to determine steady state mivacurium concentrations and for 15 min after each infusion. Twitch tension was recorded. Mivacurium concentrations after each of the two infusions were compared.
• Results: After discontinuation of the second infusion, mivacurium concentrations were larger than those after the first infusion at 2 min with edrophonium and at 2, 4, and 7 min with neostigmine. With both neostigmine and edrophonium, twitch tension recovered after infusion #2 more rapidly than after infusion #1; however, the magnitude of this effect was small.
• Conclusion: Edrophonium transiently slows the rate at which mivacurium concentrations decrease; this is consistent with our previous findings. Neostigmine has a similar, although longer, effect. Despite altering mivacurium's elimination characteristics, both drugs facilitate neuromuscular recovery, although their benefit is small.

• Anticholinergic Drugs• Atropine and glycopyrrolate have muscarinic blocking (parasympatholytic)
effects, but no activity at nicotinic receptors. They are given to prevent the cardiovascular changes induced by the anticholinesterases. Atropine has a rapid onset of action (approximately 1 min) and a duration of 30–60 min, and it crosses the blood-brain barrier. Glycopyrrolate has a slower onset (2–3 min) and approximately the same duration of action, but does not cross the blood-brain barrier. Atropine has been associated with an increased incidence of memory deficit after anesthesia compared with glycopyrrolate. It is desirable to give an anticholinergic with a faster onset of action than the anticholinesterase, because it is easier to manage transient tachycardia than bradycardia. Thus, when edrophonium is given, atropine is preferred. Doses of 7 mg/kg atropine were recommended for edrophonium 0.5 mg/kg, but at least one study has shown that this dose of atropine might be too low. Bradycardia is more frequent with an opioid-nitrous oxide anesthetic, and a dose of 10–15 mg/kg may be more appropriate in certain circumstances. Because of the variability in atropine requirement, it is recommended that atropine be given either before edrophonium or at the same time but slowly.
• Neostigmine has a much slower onset of action, so that either atropine or glycopyrrolate may be given as an anticholinergic. The simultaneous administration of atropine and neostigmine leads to an initial tachycardia because of the more rapid action of atropine, followed 10–20 min later by a bradycardia. Atropine requirements are greater with neostigmine than with equipotent reversal doses of edrophonium. The dose of atropine required is approximately half that of neostigmine; i.e., 40 mg/kg neostigmine requires about 20 mg/kg atropine. Because the time course of action of glycopyrrolate matches that of neostigmine more closely, simultaneous administration of both drugs results in more stable heart rates over time. A dose equivalent to one fourth the dose of neostigmine gives the best results. With pyridostigmine 0.2 mg/kg, the required dose of anticholinergic agent is about the same as that for neostigmine. However, the onset of action of pyridostigmine is very slow, and an initial tachycardia may be expected with either atropine or glycopyrrolate.

• Factors Affecting Reversal
• Intensity of Block• The depth of neuromuscular blockade at the time of the administration of reversal agents has a profound influence on their effect. The
time to a specific endpoint, such as 95% T1 or 0.7 TOF, is inversely related to the T1 when the reversal agent is administered. The data obtained with pancuronium, dTC, atracurium, vecuronium, or doxacurium, showed a large increase in the recovery time if T1 was < 10–20% of control when neostigmine was given. Similarly, reversal of a profound atracurium or vecuronium blockade proceeded more slowly than reversal of less intense block. In other words, the dose response of reversal agents is shifted to the right in the presence of profound blockade. However, the magnitude of this shift is greater with either edrophonium or pyridostigmine than with neostigmine.
• An additional question is whether it is preferable to give the reversal agent when profound block is present or to wait for some spontaneous recovery before antagonizing the block. Those who have studied nostigmine, the agent of choice to reverse deep blockade, agree that administering the reversal agent accelerated recovery compared with spontaneous recovery. However, it appears that giving neostigmine early offers no advantage to waiting for 10–25% spontaneous recovery, and the results might be less predictable with the early administration of reversal agents.
• Dose of Reversal Agent• When given at 10% spontaneous T1 recovery (the twitch height most frequently tested), neostigmine, pyridostigmine, and edrophonium
produced larger effects when the dose was increased. The ceiling effect demonstrated during in vitro experiments does not appear to be present for the doses used clinically, i.e. neostigmine up to 0.04 mg/kg, pyridostigmine up to 0.2 mg/kg, and edrophonium 1 mg/kg. In the reversal of an intense vecuronium block, a second dose of neostigmine (0.07 mg/kg) did not result in further recovery, suggesting that the ceiling had been reached. Although the time required to reach a given effect is reduced if a large dose is given, this does not mean that a large dose of reversal agent is always indicated. When spontaneous recovery is almost complete, large doses might, at best, be unnecessary. For example, when used to reverse 50% T1 blockade produced by vecuronium, neostigmine 5 mg produced recovery to a TOF of 0.7 in 1.1 min compared with 1.2 min after neostigmine 2.5 mg. Clearly, the larger dose was unnecessary, and the smaller dose produced adequate and rapid recovery with the potential for fewer cardiovascular effects.

• Relaxant Administration
• Choice of Relaxant• The neuromuscular block produced by gallamine is reversed more slowly by neostigmine than is that of pancuronium or dTC. Similar
conclusions have been reached when the neostigmine was administered as repeated small doses (0.25 mg) every 3 min or by a single large bolus (0.05 mg/kg). Doses required to produce a desired level of recovery within a given time after the administration of reversal agents are less for atracurium and vecuronium than for dTC or pancuronium (). As discussed earlier, the differences in reversal between the long- and intermediate-acting relaxants are likely due to a faster rate of spontaneous recovery for the latter. Small differences in reversibility have been described among the long-acting and short-acting agents, but these differences appear to be clinically unimportant.
• Bolus versus Infusion• Differences in the recovery of neuromuscular function when reversal agents were administered either during the course of a relaxant
infusion or after bolus doses have been discussed. Kopman demonstrated that when reversal agents were given within 2 min of discontinuation of infusions of atracurium, vecuronium, or pancuronium, recovery was slower than after bolus injections. Under these conditions, neostigmine (0.05 mg/kg) produced more rapid and complete recovery than did edrophonium (0.75 mg/kg). In particular, Kopman found that edrophonium did not produce TOF > 0.7 at 20 min after its administration to patients receiving a pancuronium infusion even at a dose of 1 mg/kg. No differences in recovery were demonstrated between atracurium or vecuronium infusions after either neostigmine or edrophonium.
• Intense Block• Engbæk et al. demonstrated that when an infusion of atracurium was used to maintain a very intense block producing greater than
100% depression of T1, reversal after discontinuation of the infusion was slow. When neostigmine was administered at different levels of posttetanic count, the time to reach TOF > 0.7 depended on the degree of block. Total recovery time, spontaneous and after reversal, was not reduced by the earlier administration of neostigmine. Slower spontaneous recovery has been demonstrated previously after vecuronium infusions during surgery, presumably because of equilibration of drug concentrations in the circulation and peripheral tissues. After prolonged infusions, recovery becomes dependent on elimination and metabolism of the relaxant rather than redistribution. The differences between vecuronium and pancuronium then tend to disappear because they have similar terminal half-lives.
• Recently, prolonged neuromuscular blockade has been reported after long-term (2–6 days) administration of vecuronium to two critically ill patients. In this situation, the persistent paralysis was considered to be due to accumulation of the vecuronium metabolite 3-desacetylvecuronium. This metabolite, which is as potent as the parent compound, was not eliminated because the patients had developed renal failure. Such a situation is unlikely to occur during anesthesia.
• Thus, it appears that the duration of action and reversal of neuromuscular blocking drugs is influenced both by the choice of agent and by the method of administration.

• Age
• Infants and Children• The consequences of persistent neuromuscular paralysis are considered to be more serious in children, especially in infants, than in adults. In
general, spontaneous recovery from neuromuscular blocking drugs is more rapid in children aged 1–10 yr than in adults. Recovery in infants is slower than in children for pancuronium, atracurium, and vecuronium. In infants, vecuronium appears to behave like a longer-acting drug. The reason for the slower recovery probably is related to the larger volume of distribution of the drugs in infants. Consequently, some reduction in the rate of recovery might be expected after reversal.
• As in adults, recovery after reversal is dependent on the level of paralysis when the anticholinesterase is given. Recovery is more rapid after atracurium than after the longer-acting alcuronium. When the reversal agent is administered at a fixed point of recovery, reversal occurs more rapidly and the dose of reversal agent required to produce equivalent effects is less in infants and children than in adults. Dose-response curves for neostigmine, administered during continuous infusion of dTC to maintain 90% block, demonstrated that doses producing 50% reversal were 13.1 mg/kg in infants and 15.5 mg/kg in children compared with 22.9 mg/kg obtained in a similar study in adults. The difference in dose requirement could not be explained by different volumes of distribution for neostigmine. When fixed doses of neostigmine or edrophonium were administered at 90% T1 depression during recovery from a bolus dose of pancuronium, recovery was achieved more rapidly in infants and children than in adults; this has been confirmed after the administration of neostigmine to infants, children, and adults given bolus doses of vecuronium.
• Thus, reversal of neuromuscular blockade in infants and children should be expected to occur at least as rapidly as in adults. In one study examining neuromuscular activity of children on arrival in the recovery room, the authors were unable to demonstrate weakness in patients who had received pancuronium, atracurium, or vecuronium during anesthesia. This is in marked contrast to the numerous studies that show a high incidence of incomplete recovery in adults.
• Elderly Patients• The duration of action of most nondepolarizing relaxants is prolonged in the elderly person, probably as a result of age-related decreases in hepatic
metabolism and renal clearance. Consequently, the action of pancuronium, dTC, metocurine, and vecuronium is prolonged. As a result, the reversal of these nondepolarizing relaxants may be impaired. Atracurium, because of metabolism by Hofmann elimination and enzyme hydrolysis, is not affected. Such a delay was reported when neostigmine was administered in a dose of 0.04–0.05 mg/kg 30 min after the last dose of pancuronium but not after dTC. It was observed that the duration of antagonism of metocurine infusion block was prolonged in the elderly patient. Thus, it appears that although the elderly person may demonstrate impaired clearance of both relaxants and reversal agents, the speed and extent of recovery is no different between young and old if the reversal agent is given at the same level of neuromuscular blockade.
• Drug Interactions• Several drugs have been shown to potentiate neuromuscular blocking drugs. These include inhalational, intravenous, and

• Clinical Recommendations• Clinical strategies for the reversal of muscle relaxants should be based
on pharmacologic principles. In particular, the choice of agent and dose should be made according to the intensity of the block to be reversed. Reversal agents should always be given after the use of muscle relaxants unless full recovery of neuromuscular activity is confirmed. Because small degrees of block are difficult to assess clinically, reversal agents usually are given to all patients. Neostigmine is preferred for intense blocks, but the advantages of speed of onset and reduced cholinergic effects of edrophonium make it suitable, in the appropriate dose, when return of neuromuscular activity is well established. One suggested regimen using these principles is shown in . It should be recognized that these recommendations are based on response of the adductor pollicis to TOF ulnar nerve stimulation. No attempts have been made to differentiate between differences in the required doses of anticholinesterases necessary to reverse block produced by the intermediate- and longer-acting muscle relaxants. Using these doses, it is expected that recovery of neuromuscular activity will occur within 10 min. However, this must be confirmed by clinical testing when the patient has recovered from anesthesia.

• Salib, Y. M., FFARCSI; Donati, F., PhD FRCPC; Bevan, D. R., MRCP FFARCS• • From the Departments of Anaesthesia, Royal Victoria Hospital and McGill University, 687 Pine Avenue West,
Montreal, Quebec.• Address correspondence to: Dr. F. Donati, Department of Anaesthesia, Royal Victoria Hospital, 687 Pine
Avenue West, Suite S5.05, Montreal, Quebec, Canada H3A 1A1.• Accepted for publication June 1, 1993.• • ABSTRACT: The purpose of this study was to determine the optimal dose of edrophonium needed for successful
antagonism (train-of-four ratio, or T4/T1 > 0.7) of vecuronium-induced blockade when all four twitches were visible in response to indirect train-of-four (TOF) stimulation. Forty patients, scheduled for elective surgical procedures not exceeding 120 min, received vecuronium, 0.08 mg × kg-1, during thiopentone-N2O-isoflurane anaesthesia. Train-of-four stimulation was applied every 20 sec and the force of contraction of the adductor pollicis muscle was recorded. Increments of vecuronium, 0.015 mg × kg-1, were given as required. At the end of surgery, and provided that neuro-muscular activity had recovered to four visible twitches, edrophonium, 0.1 mg × kg-1, was given. Two minutes later, edrophonium, 0.1 mg × kg-1, was given if T4/T1 did not reach 0.7. After another two minutes, edrophonium, 0.2 mg × kg-1, was given if T4/T1 did not reach 0.7 or more. Finally, if T4/T1 was still < 0.7, a dose of 0.4 mg × kg-1 was given. Seventeen patients (42.5%) required 0.1 mg × kg-1 of edrophonium for successful reversal, sixteen patients (40%) needed a cumulative dose of 0.2 mg × kg-1 and six patients (15%) required 0.4 mg × kg-1. Only one patient received 0.8 mg × kg-1. There was a good correlation between T4/T1 two minutes after the first dose of edrophonium and pre-reversal T4/T1 (r = 0.6; P = 0.00014). All patients with pre-reversal T4/T1 > 0.23 required at most 0.2 mg × kg-1 of edrophonium for successful reversal. We conclude that when all four twitches are clearly visible following train-of-four stimulation, small doses of edrophonium (0.1–0.2 mg × kg-1) might be sufficient to antagonize vecuronium neuromuscular blockade.

Anticolinesterasici e dolore cronico…..
• Dougherty, Patrick M., Ph.D.*; Staats, Peter S., M.D.†• • * Associate Professor, Departments of Neuroscience and Neurosurgery.• † Associate Professor, Department of Anesthesiology and Critical Care Medicine.• Received from the Departments of Neuroscience and Neurosurgery and the Department of Anesthesiology and
Critical Care Medicine, The Johns Hopkins University School of Medicine, Baltimore, Maryland. Submitted for publication November 6, 1997. Accepted for publication April 30, 1999. Supported by the National Insitutes of Health (grant NS-32386; project 2), Bethesda, Maryland.
• Address reprint requests to Dr. Dougherty: Department of Neurosurgery, The Johns Hopkins University School of Medicine, 600 North Wolfe Street, Meyer 5-109, Baltimore, Maryland 21287-5354. Address electronic mail to: [email protected]
• • KEY WORDS: Dorsal horn; primary afferents; spinal cord• • SYSTEMIC analgesics and conservative therapies are effective in controlling chronic pain for the majority of
patients. However, many other patients, such as those with advanced head and neck carcinoma and those with neuropathic pain, require more aggressive therapy to directly modulate pain transmission in the central nervous system. Reversible methods of aggressive therapy in the spinal cord include electrical stimulation procedures and intrathecal delivery of analgesics by implanted pumps, both of which are finding ever-expanding roles in pain control. Of these, long-term intrathecal drug therapy is likely to show the largest near-term expansion because the numbers of agents approved for this route of administration are likely soon to increase substantially. Moreover, drug therapy itself will change as treatments using microsome drug encapsulation and novel suspension media are introduced. Further on the clinical horizon is intrathecal cell implantation for the relief of chronic pain. The goal of this review is to update the reader regarding each of these pending advances in intrathecal drug therapy for chronic pain.

• In ogni caso testa la ripresa clinica prima di inviare il paziente al reparto!!!

FINE

Domande per ECM
• La dose di neostigmina(somministrata al T1 10%) necessaria per antagonizzare completamente il blocco neuromuscolare da atracurium e cisatracurium è di:
• 0.2 mg/kg
• 0.02 mg/kg
• X 0.05 mg/kg

• Being mindful of the need for greater precision, I have updated the topology of the receptive sites and fitted molecules of Ach into the picture with what appears to be the correct dimensions and orientation, as follows:
• If 20 Å separates the receptive sites and each of the two Ach molecules that open the ionic channel occupies 6 Å with its methonium head, 8 Å remains in the lumen for the influx of the cations. This is just enough to prevent a bottleneck at the level of the receptive sites, considering that the trans-membrane tube portion of the channel also measures about 8 Å. Relative to the depolarizing cations and the channel, Ach is a large molecule.
• Each subunit has a positive and a negative face, arranged so that the positive face of each subunit faces the negative face of its neighbour (). It is the negative face of the g (or e) subunit that faces the a subunit and attracts the positively charged methonium head of Ach to their interface. For Ach to be bound to the a subunit, and if its methonium head fits the inferface, its acetyl portion has to point to the a subunit, not the other way around. Looking from the synaptic cleft down the receptor channel, this means that Ach sits clockwise from the carbonyl O to the quaternary N. This is because the subunits are clockwise from the a to the g (or e).
• Scientists may one day taylor the relaxant molecule to fit the specific receptive site; however, specific targeting of neuromuscular blocking agents to the adult or fetal type AchR seems a remote challenge.
• C. Lee • California • USA
• References:

• Fletcher GH, Steinbach JH. Ability of nondepolarizing neuromuscular blocking drugs to act as partial agonists at fetal and adult mouse muscle nicotinic receptors. Mol Pharmacol 1996; 49:938-47.<ldn>!
• 2: Lee C. Thoughts on the channel size of the motor endplate acetylcholine receptor. Br J Anaesth 2002; 88:309. <ldn>!
• 3: Prince RJ, Sine SM. The ligand binding domains of the nicotinic acetylcholine receptor. In: Barrantes FJ, ed. The Nicotinic Acetylcholine Receptor, Current Views and Future Trends. Berlin, Heidelberg, New York, Barcelona, Budapest, Hong Kong, London, Milan, Paris, Santa Clara, Singapore, Tokyo: Springer, 1998; 31-59

• Lee, C.• • Editor—Anaesthesia textbooks, chapters and monographs on neuromuscular pharmacology often present artistic diagrams of the acetylcholine receptor (AchR) of the
motor endplate. Accuracy of the diagram is of obvious importance to neuromuscular pharmacology. The size of the ionic channel determines the passage of the cations that generate the endplate potential. The topology of the channel at the receptive sites affects how muscle relaxants work.
• The endplate AchR channel is generally conceived as a funnel. The extracellular portion is a cone; the membrane-crossing portion is a tube. When the channel is closed, the tube is impermeable. When the channel is open, the tube passes Na+, K+ and other cations as large as tetraethylammonium (TEA) and Tris, but nothing much larger. Based on the permeability of TEA, Tris, and other cations, the cross-sectional diameter of the open tube is quoted as 7.4 Å. Decamethonium (C10) has two methonium heads. A methonium cation measures 5.2 Å in one direction and 6.0 Å in another. As a result, C10 can pass the channel to end up intracellularly.
• Of greater interest to neuromuscular pharmacology is the dimension of the cone at the level of the two receptive sites where the relaxant molecule binds to the receptor. The inner border of the receptive sites has been estimated to be 30 Å apart in the nicotinic AchR of the electric organ. Based on the optimal neuromuscular-blocking potency of muscle relaxants, Lee has proposed that, at one point of drug-receptor interaction, the space actually available to neuromuscular blocking agents measures about 20 Å. It seems reasonable to assume that the helical arrangement of the amino acid residues lining the channel, their variable side chains, and the possible existence of intervening water molecules may account for the unavailability of the 10 Å (5 Å on each side). Other explanations are possible.
• On further thought, if TEA will pass through the tube, it must first descend through the cone between the receptive sites. The passage happens when the channel is open; namely, when the two molecules of acetylcholine occupy 12 Å (6 Å for each methonium head) of the inter-site length. Subtracting from 20 Å, 8 Å remains, just enough room for passage of TEA through this portion of the cone.
• It is commonly said that the cone formation of the channel increases its cross-sectional area to facilitate convergent entrance of the cations down the tube. This notion needs be qualified at the level of the receptive sites. Unless the bound acetylcholine molecules sink into the wall, they will protrude into the lumen. From the above calculation, the cone formation adds just enough room to accommodate the acetylcholine molecules, so that the remaining free space between the receptive sites is not narrower than the diameter of the open channel below. In other words, the cone formation prevents formation of an inter-site bottleneck to TEA. Additionally, it permits passage of smaller cations (Na+, K+) on both sides of the inter-site line. Sinking of the bound acetylcholine molecules into the wall would require large conformational change of the receptor. It would not be an energy-efficient way to provide a stable anchor or hinge for the channel to swing open below, nor would it be conducive to easy return of the acetylcholine molecules to the extracellular fluid. Little is known whether the inter-site distance increases or whether the cone itself expands when the channel opens below. Neither appears essential or economical.
• This view of the AchR endplate sythesizes three key measurements: the lumen of the open tube, the inter-site distance as deduced from the optimal molecular length of C10 congeners, and some other muscle relaxants, and the size of the methonium head of acetylcholine, two molecules of which are required to open one nicotinic acetylcholine receptor channel.
• C. Lee • California • USA
• References:

• Villarroel A. Ion conduction through the acetylcholine receptor channel. In: Barrantes FJ, ed. The Nicotinic Acetylcholine Receptor, Current Views and Future Trends. Berlin, Heidelberg, New York, Barcelona, Budapest, Hong Kong, London, Milan, Paris, Santa Clara, Singapore, Tokyo: Springer; 1998; 109-44
• 2: Dilger JP. Structure and function of the nicotinic acetylcholine receptor. In: Yaksh TL, Lynch III C, Zapol WM, Maze M, Biebuyck JF, Saidman LJ, eds. Anesthesia Biologic Foundations. Philadelphia, New York: Lippincott-Raven Publishers, 1998; 221-37
• 3: <ldn>! • 4: Dwyer TM, Adams DJ, Hille B. The permeability of the endplate
channel to organic cations in frog muscule. J Gen Physiol 1980; 75:469-92.<ldn>!
• 5: Marshall CG, Ogden DC, Colquhoun D. The actions of suxamethonium (succinyldicholine) as an agonist and channel blocker at the nicotinic receptor of frog muscle. J Physiol (Lond) 1990; 428:155-74.<ldn>!





Lee C. Structure, conformation and action of neuromuscular blocking drugs. Br J Anaesth
2001; 87:755-69.• Ach, skeletal muscle endplate AchR, and cholinergic agonists
• Ach is a flexible molecule capable of adopting several conformations without significant energy penalty. This allows it to be physiologically multifunctional. Its symmetrical conformers can flip easily. The structure of Ach, CH3-CO-O-(CH2)2-N+(CH3)3, although simple, has several important functional features, namely the methonium head centred on the positively charged quaternary N atom, the alcohol O atom that forms the ester (-O-), and the acetyl group with the carbonyl O atom (-CO-).
• The skeletal muscle endplate Ach receptor (AchR) is generally modelled after the electric organ nicotinic AchR as a pentameric structure of a2bg (or e) d subunits arranged in a rosette around a sodium—potassium ionic channel (). Each receptor has two Ach receptive sites, one on each a subunit in a pocket near where the a subunit interfaces with its neighbour g or d subunit. Pedersen and Cohen proposed that it is unlikely for the b subunit to be between the a subunits, and accordingly, one likely arrangement of the rosette is agabd, or agadb viewed from the other direction. It takes two Ach molecules acting concomitantly, one on each receptive site, to open one AchR channel. The neighbouring subunits make the receptive sites different in affinity. The distance between the two receptive sites has been estimated to be about 50 Å between their outer limits and 30 Å between their inner limits (A). The space available for NMB agents could be smaller, but the cross-section of the entire receptor is larger and could exceed 80 Å. The pentameric arrangement in a circle indicates that the two Ach receptive sites are not symmetrical or mirror image to each other (B).
• Each receptive site, in turn, has two subsites, namely, an anionic subsite to attract the positively charged onium head and a hydrogen bond donor to attract the hydrogen bond acceptor of Ach (B). The asymmetrical arrangement makes it possible for subsites of like charges to completely avoid facing each other directly.
• Various cholinergic receptors and cholinesterases have different conformational requirements or preferences of their agonists (or substrates in the case of cholinesterase) and antagonists. Of the cholinergic compounds, a 1970 report, rarely quoted in literature on neuromuscular pharmacology, proposed that the distance from the centre of the cationic N to the van der Waals (vdw) extension of the respective O atom (or equivalent hydrogen bond acceptor) is important in determining whether a cholinergic agonist will be nicotinic or muscarinic (). A distance of 4.4 Å will impart muscarinic action, while a distance of 5.9 Å will impart nicotinic action. For convenience, these two rules will be referred to in this review as the Beers and Reich's rule of 4.4 Å for muscarinic action and rule of 5.9 Å for nicotinic action, respectively. The ester O and the carbonyl O of Ach can fulfil these respective rules readily.
• The receptive sites are chiral-sensitive or chiral-selective, if not chiral-specific. For example, cisatracurium is more potent than its stereoisomers supposedly because it fits the receptor at the receptive site better. A conformation of Ach bound to a Torpedo nicotinic receptor has been published. For medicinal chemistry and clinical anaesthesia, however, one must realize that species variation and status of desensitization may alter the conformation of Ach bound to the receptor and/or that of the receptor itself. Free Ach may prefer a bent configuration.


Farmacocinetica e dinamica • Pharmacokinetic Variables• • After a single bolus dose, the plasma concentrations of
neostigmine, pyridostigmine, and edrophonium reach a peak and decrease rapidly during the first 5–10 min. Then, a slower decline, corresponding to the elimination phase can be observed. In most studies, a two-compartment analysis was performed and the results are similar for all three drugs. The volume of distribution of these anticholinesterases is in the range of 0.7–1.4 L/kg and the elimination half lives are 60–120 min. Some authors have obtained shorter elimination half-lives (15–33 min) for neostigmine and edrophonium, but these probably resulted from too short a sampling time. The clearance of these drugs is in the range of 8–16 ml × kg-1 × min-1, which is much greater than the glomerular filtration rate. However, in patients with renal failure, clearance is reduced markedly and elimination half-life increases, and it is probable that these drugs are actively secreted by the renal tubules ().

• Duration of Action• The duration of action of these drugs corresponds to their pharmacokinetic
profiles. In clinical practice, anticholinesterases usually are given when the effect of the nondepolarizing muscle relaxant is wearing off. Thus, the net effect consists of two components: the diminishing effect of the relaxant and the antagonistic effect of the anticholinesterase agent. No recurarization would be expected in this setting as long as the duration of action of the latter exceeds that of the former. However, to remove the confounding effect of the neuromuscular relaxant, which is progressively eliminated, it is possible to study the action of anticholinesterases during a constant infusion of the nondepolarizing blocker. With the infusion rate of dTC adjusted to maintain 90% block, it has been shown that neostigmine (0.043 mg/kg), pyridostigmine (0.21 mg/kg), or edrophonium (0.5 mg/kg) has an anticurare effect of 1–2 h, with no clinically important differences among them.
• Onset of Action• The three agents have markedly different onset characteristics. During steady-
state infusion of muscle relaxant, the onset of action of edrophonium is 1–2 min and that of neostigmine is 7–11 min; pyridostigmine may take as long as 16 min to exert its full effect. Similar results have been obtained with neostigmine as an antagonist of pancuronium, vecuronium, and edrophonium when used to reverse metocurine blockade. The difference in times to peak effect can also be observed when these drugs are given during the spontaneous recovery phase of neuromuscular blockade (). The slow recovery from pyridostigmine is quite different from the rapid achievement of a pseudoplateau after edrophonium.
• Traditionally, the different onset times have been attributed to the different rates of binding to the enzyme. However, if acetylcholinesterase inhibition is not the only mechanism involved in the reversal of neuromuscular blockade, this might not be the only reason for these differences.

PK-PD of neostigmine• Heier, Tom, M.D., Ph.D.*; Clough, David, M.B.Ch.B.†; Wright, Peter M. C., M.D.‡; Sharma, Manohar L., Ph.D.§; Sessler, Daniel I.,
M.D.½½; Caldwell, James E., M.B.Ch.B.‡•
• * Assistant Professor of Anesthesia. Current position: Consultant Anaesthetist, Ullevaal University, Norway. † Assistant Professor of Anesthesia. Current position: Consultant, Monklands District General Hospital, United Kingdom. ‡ Professor of Anesthesia, § Research Chemist, University of California, San Francisco. ½½Associate Dean for Research, Director OUTCOMES RESEARCHä Institute, Weakley Distinguished University Professor, and Acting Chair in Anesthesiology, University of Louisville; Professor and Vice-Chair, Ludwig Boltzmann Institute, University of Vienna, Vienna, Austria.
• Received from the Department of Anesthesia and Perioperative Care, University of California, San Francisco, California.• Supported by the Department of Anesthesia and Perioperative Care, University of California, San Francisco, California.• The laboratory in which the work was performed and Dr. Caldwell have in the past (but not currently) received funding support from
Organon Incorporated, West Orange, New Jersey. Presented in part at the annual meeting of the American Society of Anesthesiologists, New Orleans, Louisiana, October 19-23,1996.
• • ABSTRACT: • Background: The pharmacokinetics, maximum effect, and time course of action of neostigmine were studied in seven human volunteers.• Methods: Each volunteer was studied twice, during both normothermia and hypothermia. Anesthesia was induced with 30 mg/kg alfentanil
and 3 mg/kg propofol, and was maintained with 60-70% nitrous oxide and 0.7-0.9% isoflurane. The mechanical response of the adductor pollicis to train-of-four stimulation of the ulnar nerve was recorded, and central body temperature maintained stable at either less than 34.5°C or greater than 36.5°C by surface cooling or warming. Before neostigmine administration, a stable 5% twitch height was obtained by an infusion of vecuronium, and the infusion rate remained unchanged thereafter. Neostigmine, 70 mg/kg, was then infused over 2 min, and blood samples for estimation of neostigmine concentrations were collected at intervals for 240 min.
• Results: With hypothermia, the central volume of distribution of neostigmine decreased by 38%, and onset time of maximum effect increased (4.6 vs. 5.6 min). Hypothermia did not change the clearance (696 ml/min), maximum effect, or duration of action of neostigmine.
• Conclusions: The efficacy of neostigmine as an antagonist of vecuronium-induced neuromuscular block is not altered by mild hypothermia.


• The duration of action of neostigmine as an antagonist of vecuronium-induced block is dependent on both the rate of decrease of the plasma concentration and the interaction with the enzyme acetylcholinestearase. During the interaction of neostigmine with acetylcholinesterase, a relatively stable carbamylated complex is formed. Decarbamylation of this complex is slow, and the process has a half-life of approximately 30 min. Termination of the effect of neostigmine may be rate limited by decarbamylation of the neostigmine/enzyme complex rather than simply the decrease in the plasma concentration of neostigmine. Hypothermia may slow the decarbamylation process, but this has been studied only in vitro and at temperatures of 30°C and below, and these results cannot be related directly to our study. The lack of effect of hypothermia on neostigmine Cl is consistent with its lack of effect on its duration of action.
• In the clinical situation, reversal of neuromuscular block is dependent on two processes, the interaction of neostigmine with acetylcholinesterase and the inherent duration of action of the neuromuscular blocking drug.

• 14: Barber HE, Calvey TN, Muir KT: The relationship between the pharmacokinetics, cholinesterase inhibition and facilitation of twitch tension of the quaternary ammonium anticholinesterase drugs, neostigmine, pyridostigmine, edrophonium and 3-hydroxyphenyltrimethylammonium. Br J Pharmacol 66:525–30, 1979<ldn>!
• 15: Wilson IB, Harrison MA, Ginsberg S: Carbamyl derivatives of acetylcholinesterase. J Biol Chem 238:1498–500, 1961
• 16: Verotta D, Kitts J, Rodriguez R, Coldwell J, Miller RD, Sheiner LB: Reversal of neuromuscular blockade in humans by neostigmine and edrophonium. J Pharmacokinet Biopharm 19:713–29, 1991<ldn>!



Reid J, Breslin DS,Mirakhur R, Hayes A.Neostigmine antagonism of rocuronium block during anesthesia with sevoflurane,isoflurane or propofol.Can.Anesth.J. 2001:48 :351-55
•
• Purpose: To examine the influence of continuing administration of sevoflurane or isoflurane during reversal of rocuronium induced neuromuscular block with neostigmine.
• Methods: One hundred and twenty patients, divided into three equal groups, were randomly allocated to maintenance of anesthesia with sevoflurane, isoflurane or propofol. Neuromuscular block was induced with rocuronium and monitored using train-of-four (TOF) stimulation of the ulnar nerve and recording the force of contraction of the adductor pollicis muscle. Neostigmine was administered when the first response in TOF had recovered to 25%. At this time the volatile agent administration was stopped or propofol dosage reduced in half the patients in each group (n = 20 in each group). The times to attain TOF ratio of 0.8, and the number of patients attaining this end point within 15 min were recorded.
• Results: The times (mean ± SD) to recovery of the TOF ratio to 0.8 were 12.0 ± 5.5 and 6.8 ± 2.3 min in the sevoflurane continued and sevoflurane stopped groups, 9.0 ± 8.3 and 5.5 ± 3.0 min in the isoflurane continued and isoflurane stopped groups, and 5.2 ± 2.8 and 4.7 ± 1.5 min in the propofol continued and propofol stopped groups (P < 0.5– 01). Only 9 and 15 patients in the sevoflurane and isoflurane continued groups respectively had attained a TOF ratio of 0.8 within 15 min (P < 0.001 for sevoflurane).
• Conclusions: The continued administration of sevoflurane, and to a smaller extent isoflurane, results in delay in attaining adequate antagonism of rocuronium induced neuromuscular block.

Baurain MJ, d'Hollander AA,Melot C, Dernovoi BS,Barvais L.Effects of residual concentrations of isoflurane on the reversal of vecuronium induced neuromuscular blockade.Anesthesiology 1991:71:474-
• • ABSTRACT: Thirty-six anesthetized patients (ASA physical status 1 or 2) undergoing elective surgery were monitored
(isometric adductor pollicis mechanical activity) to detect the effects of discontinuing isoflurane anesthesia upon the reversal of vecuronium-induced neuromuscular blockade. Neuromuscular blockade was produced by vecuronium 100 mg/kg and additional doses of 20mg/kg until completion of surgery. The patients were randomly divided into three groups: in the control group (n = 12), only fentanyl/N2O was given; in the “isostable” group (n = 12), isoflurane at an end-tidal concentration of 1.25% was maintained throughout anesthesia; in the “isostop” group (n = 12), isoflurane 1.25% was discontinued before neostigmine administration. In all groups, paralysis was antagonized with 15 mg/kg intravenous (iv) atropine and 40 mg/kg iv neostigmine when the twitch height (0.1 Hz) had regained 25% of its control value. The measured parameters were twitch height, train-of-four, and 50–100-Hz tetanic fade. No significant differences were found among the three groups with respect to the final twitch heights and tetanic fades at 50 Hz. In the isostable group, final mean train-of-four was significantly less (75%) than in the other patients (88%) (P < 0.01). Mean tetanic fade at 100 Hz was significantly less in the isostable group (31%) than in the isostop group (57%) (P < 0.01) and control group (84%) (P < 0.01). We conclude that discontinuing isoflurane anesthesia for 15 min improves the reversal of a vecuronium paralysis. In addition, after the antagonism of vecuronium-induced neuromuscular blockade, tetanic fade at 100 Hz appears useful to detect the slight impairment of the neuromuscular transmission that is induced by residual isoflurane concentrations and that is undetected by train-of-four measurements.
• • KEY WORDS: Anesthetics, volatile: isoflurane; Antagonists, neuromuscular relaxants: neostigmine; Neuromuscular
relaxants: vecuronium;

Neostigmine to be preferred to edrophonium….
• Driessen, J. J.; Robertson, E. N.; Booij, L.H.D. J.; Fisher, D. M.•
• Editor,—We read with interest the review article by Fisher on neuromuscular blocking agents in paediatric anaesthesia. It was a concise summary of the use of these agents in paediatric practice today. The author's preference for edrophonium over neostigmine, however, did not seem to be a true reflection of what is known about antagonism of neuromuscular block in children.
• There have been few comparative studies in children of the speed of action of edrophonium and neostigmine. In comparable mg per kg doses, recovery from an intense atracurium-induced neuromuscular block in children is faster after neostigmine than edrophonium. In adults, it has been shown that in the reversal of profound block produced by vecuronium or atracurium, neostigmine is more effective than edrophonium and its maximal effect is reached more quickly, even though edrophonium is faster in its initial onset. Monitoring of the depth of neuromuscular block in infants and children is technically more difficult and not perhaps as widespread as in Dr Fisher's department. This suggests that the chance of profound neuromuscular block at the end of surgery is greater in paediatric anaesthetic practice. Neostigmine would therefore be a better choice than edrophonium.
• In his article, Fisher stated that less neostigmine is needed in children than in adults, and quoted Fisher and colleagues. Quoting the same article, he then stated that the ED50 of neostigmine for antagonism was greater for children than for adults. It is possible that this is a typing error and that the author means to suggest that edrophonium has a higher ED50 in children than in adults. For this reason, the author suggests the use of higher doses of edrophonium for antagonism in infants and children. These studies, however, were carried out under steady-state infusion of tubocurarine and not during the recovery phase from the newer non-depolarizing agents. Moreover, there was no significant difference in the dose of edrophonium required to antagonize tubocurarine-induced neuromuscular block in children and adults. In contrast, several studies have shown that neostigmine antagonizes residual non-depolarizing neuromuscular block more effectively in children than in adults. Debaene, Meistelman and d'Hollander showed that, when twitch height recovered to 10% of control after vecuronium, neostigmine 30 mg kg-1 had a more rapid onset in children than in adults, and that a TOF of 0.7 was obtained in less than 10 min in all patients, including infants. The dose of neostigmine to effectively antagonize 90% block produced by rocuronium is indeed smaller in children (mean 7 mg kg-1) than in adults (56 mg kg-1). The effects of 2 x ED95 of rocuronium could effectively be antagonized in infants with neostigmine 20 mg kg-1.
• With mivacurium there may be an argument for the use of edrophonium as it slows the hydrolysis of mivacurium by plasma cholinesterase less than neostigmine. However, until this issue is resolved, we agree with the author's recommendation of not antagonizing profound mivacurium-induced block.
• In summary, we feel that there are little convincing scientific data to prefer edrophonium to neostigmine in paediatric patients. Indeed, with the new shorter acting neuromuscular blocking agents, there may be some advantage to the use of neostigmine over edrophonium.
•

• References • 1: Fisher DM. Neuromuscular blocking agents in paediatric anaesthesia. Br J Anaesth 1999;
83:58-64. <ldn>! • 2: Gwinnutt CL, Walker RWM, Meakin G. Antagonism of intense atracurium-induced
neuromuscular block in children. Br J Anaesth 1991; 67:13-6.<ldn>! • 3: Caldwell JE, Robertson EN, Baird WLM. Antagonism of profound neuromuscular blockade
induced by vecuronium or atracurium. Comparison of neostigmine with edrophonium. Br J Anaesth 1986; 58:1285-9.<ldn>!
• 4: Caldwell JE, Robertson EN, Baird WLM. Antagonism of vecuronium and atracurium: comparison of neostigmine and edrophonium administered at 5% twitch height recovery. Br J Anaesth 1987; 59:478-81.<ldn>!
• 5: Fisher DM, Cronelly R, Miller RD, Sharma M. The neuromuscular pharmacology of neostigmine in infants and children. Anesthesiology 1983; 59:220-5.
• 6: Fisher DM, Cronelly R, Sharma M, Miller RD. Clinical pharmacology of edrophonium in infants and children. Anesthesiology 1984; 61:428-33.<ldn>!
• 7: Debaene B, Meistelman C, d'Hollander A. Recovery from vecuronium neuromuscular blockade following neostigmine administration in infants, children and adults during halothane anaesthesia. Anesthesiology 1989; 71:840-4.<ldn>!
• 8: Abdulatif M, Mowafi H, Al-Ghamdi A, El-Sanabary M. Dose-response relationships for neostigmine antagonism of rocuronium-induced neuromuscular block in children and adults. Br J Anaesth 1996; 77:710-15.<ldn>!
• 9: Leuwer M, Motsch J, Schledt U, et al. Dose-response, time course of action and recovery of ORG 9426 (rocuronium) in infants during halothane anaesthesia. Br J Anaesth 1994; 73:716P.
• 7: Cronnelly R, Morris RB, Miller RD. Edrophonium: Duration of action and atropine requirement in humans during halothane anesthesia. Anesthesiology 1982; 57:261-6.<ldn>!
• 8: Miller RD, VanNyhuis LS, Eger EI II, et al. Comparative times to peak effect and durations of action of neostigmine and pyridostigmine. Anesthesiology 1974; 41:27-33.

• Editor,— • • D. M. Fisher • Department of Anesthesia • University of California • San Francisco, CA, USA

Smith, CE, Donati F., Bevan DR.Dose Response ‑Relationships for Edrophonium and Neostigmineas Antagonists of Atracurium and VecuroniumNeuromuscular BlockadeAnesthesiology 1989;71: 37-43.
• To determìne the potencies of edrophoniurn and neostigmine as gonists of nondepolarizing neuromuscular blockade produced
• atracuriunì and vecuronium, dose response curves were coned for hoth antagonists when given at 10% ‑spontaneous re
• of first twitch height. Ninety ASA physical status 1 and 2 ts were given either 0.4 mg/kg atracurium or 0.08 mg/kg venium during thiopental nitrous oxide enfiurane anesthesia. n of four stimulation was applied to ‑ ‑ ‑ ‑the uInar nerve every 12 the force of contraction of the adduetor pollicis muscle was rded. When spontaneous recovery of first twitch height reached of its initial control value, edrophonium (0. 1, 0.2, 0.4, or 1 mg/
• or neostigmine (0.005, 0.01, 0.02, or 0.05 tng/kg) was adminisby random allocation. Neuromuscular function in another ten was allowed to recover spontancously. Assísted recovery defined as actual recovery minus mean spontancous recovery in patients who were not given antagonists. First twitch was initiatty more rapid when vecuroniunì was antagonized red with atracurium, but no difference was detected after 10 At 10 min the neostigmine EDgO was 0.022 ± 0.003 (SEM) mg/
• dter atracurium and 0.024 0.003 mg/kg after vecuroniunì. edrophonium ED80 was 0.44 0.11 mg/kg with atracurium and ± 0.12 mg/kg with vecuronium, giving a neostigmine:edroi poteney ratio of 20. Atracurium train of four fade could‑ ‑
• antagonized more easily with edrophonium, whereas that of vewas more easily antagonized by neostigmine. It ìs conthat edrophoniunt and neostigmine are not equally effective
• atracurium and vecuronium. (Key words: Antagonists, neuar relaxants: edrophonium; neostigmine. Monitoring. trainr. Neuromuscular relaxants: atracurium; vecuronium.)

• WHEN neostigmine is used to reverse neuromuscular blockade, it
inhibits acetylcholine (ACh) metabolism at the muscarinic receptors of airway smooth muscle as well as at the nicotinic receptors of the neuromuscular junction. Thus, neostigmine may induce an increase in ACh in muscarinic receptors which results in bronchoconstriction. However, the mechanisms involved in anticholinesterase (anti-ChE) drug-induced bronchoconstriction have not been clarified.
• In a previous study we demonstrated that accumulation of inositol monophosphate (IP1), a degradation product of the phosphatidylinositol (PI) response, was stimulated by neostigmine and by pyridostigmine, not by edrophonium in rat tracheal slices, and that these increases were inhibited by atropine. The results suggest that neostigmine and pyridostigmine stimulate PI response in the airway smooth muscle, while edrophonium does not. Although a direct relationship was suggested between the increase in PI response and airway smooth muscle contraction,

• Muscarinic ACh receptors in the airway are divided into M2 and M3 receptors. The M3 muscarinic receptors exist on airway smooth muscle cell membrane, and M2 muscarinic receptors exist on postganglionic nerve terminals. Stimulation of M3 receptors induces bronchoconstriction, whereas stimulation of M2 receptors inhibits ACh release, resulting in attenuation of vagally-induced bronchoconstriction. In the present study, the contraction by neostigmine or pyridostigmine of rat tracheal rings was completely inhibited by 4-DAMP, a selective M3 antagonist at a dose of 10 nM. Ten Berge et al. tested the effects of 4-DAMP on the twitch response of electrical field-stimulated guinea pig tracheal ring preparations, and found that twitch contraction was nearly inhibited by 4-DAMP at a dose of 10 nM. Their result is consistent with our data. Thus, in the present study the contractile response to anti-ChE drugs is likely to be mediated via M3 muscarinic receptors.

Bevan DR, Donati F, Kopman AF: Reversal of neuromuscular
blockade. Anesthesiology 77:785–805, 1992

• Potency: Dose-Response Curves• Dose-response curves for edrophonium, neostigmine, and pyridostigmine can be constructed after their
administration during the constant infusion of nondepolarizing blockers. Peak effect is measured and plotted against dose. Experiments performed with dTC and with halothane as the background anesthetic indicated that edrophonium had approximately one twelfth and pyridostigmine one fifth the potency of neostigmine. Similar dose-response curves have been obtained during the spontaneous recovery phase of dTC or pancuronium block. In this situation, the apparent potency of the anticholinesterases increases with time because of spontaneous recovery of the block and because no recurarization takes place. Taking the measurements at 10 min leads to results similar to those obtained during constant infusion, with the advantage of greater clinical application (). The dose-response curve for edrophonium is flatter than that for neostigmine or pyridostigmine, which makes it difficult to establish potency ratios unless the part of the curve for which comparisons are made is specified. Furthermore, the potency ratio is not the same for single twitch and TOF. For example, if reversal is attempted at 10% T1 recovery during pancuronium blockade, 12 times as much edrophonium as neostigmine is required to achieve 80% T1, but 25 times as much is needed to reach a TOF ratio of 0.5. If vecuronium is used instead of pancuronium, 80% T1 recovery is achieved with 19 times as much edrophonium as neostigmine, and to obtain 50% T4/T1, the potency ratio is 26. Thus, the neostigmine-edrophonium potency ratio, previously estimated at 12, varies depending on the relaxant used, the depth of block, and the endpoint chosen.
• If the constant-infusion technique is used, there is no difference in the dose-response relationship for anticholinesterase agents if vecuronium is used instead of pancuronium (). However, there is a marked shift to the left for vecuronium if the data are obtained when the reversal agent is given while neuromuscular blockade is wearing off spontaneously (). This is related to the more rapid spontaneous recovery of vecuronium than of pancuronium. There are slight differences between atracurium and vecuronium. For example, the effect of neostigmine is greater 5 min after its administration in the reversal of vecuronium, but by 10 min there are no differences. Edrophonium appears to be less predictable if vecuronium is used as the relaxant.

• Reversal of Intense Block• The previous discussion pertained to reversing the block at 10% T1
height. When reversal is attempted at 1% T1, i.e., 99% block, the dose-response curves are shifted to the right. However, the shift is more important for edrophonium than for neostigmine (). The neostigmine-edrophonium potency ratio is 16.6 for 80% T1 recovery when given at 90% atracurium block, compared with 35.3 when administered at 99% block. Pyridostigmine also is comparatively less potent in reversing deep block. Thus, neostigmine appears preferable to either edrophonium or pyridostigmine when profound (> 90%) blockade is to be antagonized. The time taken to reach adequate recovery of neuromuscular function (TOF > 0.7) is dependent on the dose of anticholinesterase agent given. For example, neostigmine accelerates the rate of recovery from atracurium or vecuronium blockade, and this acceleration is dose-dependent.
• Potent anesthetic vapors potentiate neuromuscular block. Thus, their cessation at the end of surgery will assist the overall recovery of neuromuscular activity. (See also the section “Factors affecting reversal: drug interactions.”

• Complications of Reversal Agents
• Neuromuscular Block• Anticholinesterases may cause neuromuscular weakness in patients with myasthenia
gravis when the dose administered was too high. There are no convincing reports of this occurring in the postanesthetic period after the administration of a nondepolarizing muscle relaxant and neostigmine, pyridostigmine, or edrophonium. However, when relatively high doses of neostigmine are administered in the presence of little residual nondepolarizing blockade, tetanic fade is sometimes seen; this effect is reversed by the administration of small doses of a nondepolarizing blocker. TOF is usually not affected in this setting. The clinical importance of this brief (< 5 min) finding is uncertain. (See also the section “Anticholinesterase pharmacology: neostigmine block.”)
• Cardiovascular Effects• Anticholinesterases have pronounced vagal effects. Bradycardia and/or other
bradyarrhythmias such as nodal and ventricular escape beats and asystole may occur. These can be attenuated by the administration of an anticholinergic drug such as atropine or glycopyrrolate, both of which block muscarinic but not nicotinic receptors. Interestingly, some bradycardia occurs in the denervated heart, but the magnitude of this effect is not as great as in hearts with a normal vagus nerve. The time course of bradycardia parallels that of the reversal of block. Its onset is rapid for edrophonium, slower for neostigmine, and slowest for pyridostigmine.
• Alimentary Effects• Anticholinesterases are associated with increased salivation and increased bowel
motility. Atropine seems to block the former, but there is debate concerning its effectiveness in inhibiting peristalsis. Some studies claimed an increase of bowel anastomotic leakage when neostigmine was used to reverse neuromuscular blockade. However, the incidence of the complication may depend on surgical practice. The combination of atropine with neostigmine has been found to decrease cardiac sphincter pressure (lower esophageal pressure minus gastric pressure). In addition, a greater incidence of postoperative vomiting was observed after atropine and neostigmine than when these drugs were omitted.
• Respiratory Effects• Cholinergic stimulation of the bronchi produces bronchoconstriction, and
anticholinesterases have the potential to increase airway resistance. Anticholinergics tend to reduce this effect. The net effect on the lungs of administration of an anticholinesterase with an anticholinergic is unclear. Clinically, the drugs commonly are given at the end of an operation, when bronchospasm may be triggered by several other factors such as the presence of an endotracheal tube, pain, and light anesthesia.
• Reversal of Succinylcholine Phase II Block• Prolonged succinylcholine infusions now are used infrequently because of the
availability of intermediate-duration nondepolarizing muscle relaxants. With prolonged or repeated use, the characteristics of succinylcholine block change. The TOF ratio decreases progressively and, with doses greater than 5–7 mg/kg, the block appears to be nondepolarizing in nature. This type of block can be reversed with either neostigmine or edrophonium. However, in patients with abnormal plasma cholinesterase, who have prolonged apnea, TOF fade usually is present when the patient recovers, but the effect of anticholinesterases is unpredictable. It is probably safer to continue mechanical ventilation in these patients until full recovery of neuromuscular function can be demonstrated.

• Schäfer, Michael, M.D.• • (Accepted for publication November 30, 1999.)• • To the Editor:-In recent years, the journal ANESTHESIOLOGY has published several
reports on the analgesic effectiveness of the cholinesterase inhibitor neostigmine. Although there is good evidence for a spinal action of neostigmine, a rationale for a peripheral mechanism of action is lacking. Intrathecal injection of neostigmine produces analgesic effects in animals, including humans, accompanied by a high incidence of side effects. The inhibition of spinal cholinesterase results in an increase of endogenous acetylcholine, which is most likely released from intrinsic cholinergic neurons within the dorsal horn of the spinal cord. These cholinergic neurons terminate in the vicinity of primary afferents, which express muscarinic receptors. Consistently, analgesic effects of intrathecal neostigmine could be reversed by muscarinic receptor antagonists. The analgesic effect may be explained by a muscarinic presynaptic inhibition of glutamatergic afferents, similar to how it has been described in the neostriatum. An important prerequisite for the effectiveness of neostigmine is a tonic cholinergic activity.
• Although these mechanisms are clearly described for the spinal cord, evidence is lacking for the periphery. Therefore, the negative result of adding neostigmine to a mepivacaine axillary plexus block in the study by Bouaziz et al. is not surprising. How would neostigmine exert an effect within the nerve sheath of the axillary plexus? An endogenous release of acetylcholine does not exist. Interestingly, the authors hypothesized a peripheral action of neostigmine based on the demonstration of peripheral muscarinic receptors only; however, this is not enough. In their discussion, they refer to studies that investigated the effects of muscarinic agonists in spinal cord slice preparations in vitro or intrathecally in vivo. However, these effects are not described for peripheral nerve endings, and neostigmine should not be confused with muscarinic agonists. Therefore, a lack of neostigmine effectiveness within the nerve sheath of the axillary plexus should have been anticipated. For the same reasons, the results of experimental and clinical studies that showed analgesic effectiveness of intraarticular neostigmine are surprising. In rats, the intraarticular injection of neostigmine produces moderate analgesia to thermal stimuli, which is allegedly reversible by intraarticular atropine, although data were not shown in that study. In patients undergoing arthroscopic meniscus repair, intraarticular injection of 500 mg neostigmine resulted in a significant difference in pain intensity at 1 h postoperatively, in total consumption of intravenous rescue analgesics, and in time to first analgesic use. To support their hypothesis of a peripheral site of action, the authors refer to “preclinical data suggesting peripheral antinociceptive effects of acetylcholine.” However, acetylcholine is an agonist at muscarinic receptors. Again, the cholinesterase inhibitor neostigmine should not be confused with muscarinic agonists. In both cases, the question arises: Which cells in the periphery are responsible for a tonic cholinergic activity? This question has not been addressed in either of these studies; therefore, the mechanism of action of peripherally applied neostigmine is still lacking, and the identification of the presumed source of peripheral acetylcholine is urgently needed.



Potenza degli antiAche• Naguib M,Riad W.Dose response relationship for edrophonijm
and neostigmine antagonism of atracurium and cisatracurium induced neurmuscular block.Can.Anaesth.J 2000;47:1074-1081
• Purpose: To study the dose-response relationships for neostigmine and edrophonium during antagonism of neuromuscular block induced by atracurium and cisatracurium.
• Methods: One hundred and twenty eight, ASA group 1 or 2 adults were given either 0.5 mg×kg-1 atracurium or 0.1 mg×kg-1 cisatracurium during fentanyl-thiopental-nitrous oxide-isoflurane anesthesia. The neuromuscular block was measured by an acceleration-responsive transducer. Responses were defined in terms of percent depression in the first twitch (T1) and train-of-four (TOF) response. When spontaneous recovery of first twitch height reached 10% of its initial control value, edrophonium (0.1, 0.2, 0.4, or 1 mg×kg-1) or neostigmine (0.005, 0.01, 0.02, or 0.05 mg×kg-1) was administered by random allocation. Neuromuscular function in another sixteen subjects was allowed to recover spontaneously.
• Results: At five minutes, unlike edrophonium, neostigmine was equally effective against atracurium and cisatracurium with respect to T1 recovery. The neostigmine T1-ED50 was 10.3 ± 1.06 (SEM) mg×kg-1 after atracurium and 11.2 ± 1.06) mg×kg-1 after cisatracurium. The edrophonium ED50 was 157 ± 1.07 mg×kg-1 with atracurium and 47.4 ± 1.07 mg×kg-1 with cisatracurium, giving a neostigmine:edrophonium potency ratios of 15.2 ± 1.7 and 4.2 ± 0.41 (P < 0.001) for atracurium and cisatracurium, respectively. At 10 min neostigmine was 13 ± 1.4 times as potent as edrophonium for achieving 50% TOF recovery after atracurium paralysis. After cisatracurium the potency ratio was 11.8 ± 1.3 (NS).
• Conclusions: Although there were differences at five minutes, neostigmine:edrophonium potency ratios at 10 min, were similar in both relaxants studied.

Watcha MF, Safavi FZ, McCulloch DA, et al. Effect of antagonism of mivacurium-induced
neuromuscular block on postoperative emesis in children. Anesth Analg 1995; 80:713-7.
• The routine use of cholinesterase inhibitors to antagonize residual neuromuscular block may be associated with increased postoperative emesis.
• Rapid spontaneous recovery from mivacurium may obviate the need for these drugs.
• randomized, double-blind, placebo-controlled study • 113 healthy children • incidence of postoperative complications after spontaneous recovery and
after the use of neostigmine-glycopyrrolate or edrophonium-atropine. • anesthetic regimen :halothane, nitrous oxide, fentanyl, 2 micrograms/kg
mivacurium in an initial dose of 0.2 mg/kg, followed by an infusion, adjusted to maintain > or = 1 evoked contraction response to a supramaximum train-of-four stimulus.
• At the end of the procedure, patients received by random assignment one of three drug combinations: 1) neostigmine 70 micrograms/kg + glycopyrrolate 10 micrograms/kg, i.v., 2) edrophonium 1 mg/kg + atropine 10 micrograms/kg, i.v., and 3) saline.
• trachea extubated when evoked responses to peripheral nerve stimulation and clinical signs of adequate neuromuscular recovery were present.
• Postoperative pain was treated with morphine and emesis with metoclopramide.

![5 Modulo Ge[1].Spool](https://static.fdocumenti.com/doc/165x107/55759300d8b42ae7708b50b9/5-modulo-ge1spool.jpg)




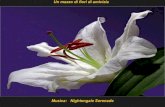









![6 Modulo Ge[1].Cnipa](https://static.fdocumenti.com/doc/165x107/557592fcd8b42ae7708b50b7/6-modulo-ge1cnipa.jpg)