VANTAGGI E LIMITI DELLA TERAPIA INSULINICA - Baroni Marco...VANTAGGI E LIMITI DELLA TERAPIA...
62
VANTAGGI E LIMITI DELLA TERAPIA INSULINICA Marco Giorgio Baroni Dipartimento di Medicina Sperimentale Università Sapienza di Roma Roma, 31 ottobre 2017 Diapositiva preparata da MARCO BARONI e ceduta alla Società Italiana di Diabetologia. Per ricevere la versione originale si prega di scrivere a [email protected]
Transcript of VANTAGGI E LIMITI DELLA TERAPIA INSULINICA - Baroni Marco...VANTAGGI E LIMITI DELLA TERAPIA...
-
VANTAGGI E LIMITI DELLA TERAPIA INSULINICAMarco Giorgio BaroniDipartimento di Medicina SperimentaleUniversità Sapienza di Roma
Roma, 31 ottobre 2017
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Dichiaro di aver ricevuto negli ultimi due anni compensi o finanziamenti dalle seguenti
Aziende Farmaceutiche e/o Diagnostiche:
SanofiNovo Nordisk
Abbott
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Diabetes is a progressive disease that requires reassessment to reach target
Canada(DICE)2
HbA1c
-
Controllo glicemico nei pazienti italianicon diabete tipo 2
Annali AMD 2012
Andamento per classi dell’HbA1c (normalizzata a 6,0)
Il 43.8% dei pazienti presenta valori 8%
Il 12% ha valori < 6%
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Diabete di tipo 2: durata dell’efficacia dei singoli farmaci
33
45
57
0 10 20 30 40 50 60
Glyburide
Metformin
Rosiglitazone
RosiglitazoneMetforminGlyburide
mesi
Kahn SE et al. NEJM 2006; 355: 2427–2443
Durata del ControlloGlicemico: tempo da intendersi Hba1c< 7% (ADOPT)
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
Diagramm1
Glyburide
Metformin
Rosiglitazone
mesi
Months
33
45
57
Tabelle1
Months
Glyburide33
Metformin45
Rosiglitazone57
Ziehen Sie zum Ändern der Größe des Diagrammdatenbereichs die untere rechte Ecke des Bereichs.
-
UKPDS1
(n=3867)ADVANCE2
(n=11,140)ACCORD3
(n=10,251)VADT4
(n=1791)
Duration of diabetes (years) 0* 8 10 11.5
Mean baseline HbA1c (%)
7.1 7.5 8.3 9.4
Mean baseline FPG (mmol/L) 8.0 8.5 9.7 11.4
Mean age (years) 53 66 62 60
MicrovascularMacrovascular
=±
==
1UKPDS Group. Lancet 1998; 352:837. 2ADVANCE Collaborative Group. N Engl J Med 2008; 358:25603ACCORD Study Group. N Engl J Med 2008; 358:2545. 4Duckworth et al N Engl J Med 2009; 360:129
*Newly diagnosed patients with no previous history of CVD; FPG: fasting plasma glucose
Disease progression
Early vs late glycemic intervention: UKPDS enrolled newly diagnosed patients
Intervento precoce ed individualizzazione della terapia
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The defect in insulin secretion is a
primary one. The primary defect in
insulin secretion is reverted by insulin
treatment
LIMITATIONS
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
UKPDS 16. Diabetes 1995;44:1249–58; Lebovitz 1999;7:139–53
Years from diagnosis
β-ce
ll fu
nctio
n (%
, HOM
A)
Diabetes diagnosis
β-cell function progressively declines
ADOPTUKPDS
0
20
40
60
80
100
Diet (n=110)Sulphonylurea (n=511)
Metformin (n=159)
–5 –4 –3 –2 –1 0 1 2 3 4 5 6
Extrapolation of β-cell function prior to diagnosis
0 1 2 3 4 50
60
70
80
90
100
Rosiglitazone, −2.0 (−2.6 to −1.3)Metformin, −3.1 (−3.8 to −2.5)Glyburide, −6.1 (−6.8 to −5.4)
Annualised slope (95% CI)
Treatment difference (95% CI)Rosiglitazone vs. metformin, 5.8 (1.9 to 9.8); p=0.003Rosiglitazone vs. glyburide, −0.8 (−4.7 to 3.1)); p=0.67
Time (y)
β-ce
ll fu
nctio
n (%
)
Kahn et al. N Engl J Med 2006;355:2427–43
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
-60 0 60 120 180 240
360
330300270240110
80
140130120110100
90
120906030
0
Glucose (mg/dl)
Insulin (μU/ml)
Glucagon (pg/ml)
Meal
(minutes)
Type 2 diabetes(n=12)
Normals (n=11)
Delayed/depressedinsulin response
Non-suppressed glucagon
Adapted from Muller WA et al. N Engl J Med. 1970;283:109
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Yoneda S et al. J Clin Endocrinol Metab 98: 2053–2061, 2013
Relative β-cell area to entire pancreatic section in NGT, IGT, newly diagnosed DM and longstanding T2DM
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Yoneda S et al. J Clin Endocrinol Metab 98: 2053–2061, 2013
T2DM had a significantly increased β-cell apoptosis compared with the NGT
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin prevents apoptosis induced by serum deprivation for 24 h in human pancreatic islets
Modified from Federici M al. FASEB J 15: 22-24, 2001
0
5
10
15
20
25
30
% a
popt
osis
Basal) Serum deprived Insulin(100 nm)
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
The insulin receptor is localized in insulin secretory vescicles in human pancreatic β-cells
Hribal et al. FASEB J 17: 1340-1342, 2003
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin stimulates its biosynthesis in human pancreatic islets
Modified from Andreozzi F et al. Endocrinology 145: 2845–2857, 2004
200
230
0
50
100
150
200
250
Insu
linbi
osyn
thes
is(%
ove
rbas
al)
Glucose(3 mm)
Glucose(16.7 mm)
Insulin(100 nm)
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Effetto della terapia insulinica intensiva sulla funzione -cellulare e sul controllo glicemico in diabetici tipo 2 di nuova diagnosi
Lancet 2008; 371: 1753-1760
51.1%
44.9%
26.7%
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
First-phase and second-phase insulin secretion in response to IVGTT in 14 patients with type 2 diabetes before and after 8 weeks of
insulin glargine treatment add-on to metformin
Pennartz C et al. Diabetes Care 34:2048–2053, 2011
The mean diabetes duration was 4.6±3.0 years
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
LIMITATIONS
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Key Pathogenetic Defects in T2DM:The Ominous Octet
IMPAIRED INSULIN SECRETION
INAPPROPRIATE GLUCAGON SECRETION
REDUCED GLUCOSE UPTAKE
REDUCED GLP-1Altered Adipòcyte Metabolism
Altered Brain Signalling
Increased RenalGlucose Reabsorption
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Islet β-cell
ImpairedInsulin Secretion
12.6%
HYPERGLYCEMIA
Groop L et al. Am J Med 87:183-190, 1989Mod. da Gerich JE, Diabetes,Obesity and Metabolism 2:345-350, 2000
Relative contributions of HGP and glucose disposal to secondary failure to oral agents in Finnish diabetic
patients
IncreasedHGP
26.1% Decreased GlucoseUptake17.3%
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Excessive hepatic glucose production
Glucagon secretion
Pancreatic cells: β-cell α-cell δ-cell
Hepatic glucose production
Insulin secretion
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Henquin JC et al. Diabetologia 54:1720–1725, 2011
Ratio of alpha cell/beta cell areas in 52 non-diabetic subjects (ND) and 50 type 2 diabetic (T2D) subjects
P < 0.0001
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Linn T et al. J Clin Endocrinol Metab 93: 3839–3846, 2008
* * *
20.0
0
21.0
0
22.0
0
23.0
0
0.0
0
1.0
0
2.0
0
3.0
0
4.0
0
5.0
0
6.0
0
7.0
0
8.0
0
9.0
0
10.0
0
** *
Nocturnal Hepatic Glucose Production after Bedtime Injection of Glargine or NPH Insulin in Patients with Type 2 Diabetes
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
LIMITATIONS
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
ORIGIN Trial Investigators, N Engl J Med 367: 319-28, 2012
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
ORIGINPrimary & Secondary Outcomes & their Components
HR (95% CI) P Insulin Standard/100 py /100 py
1st Coprimary 1.02 (0.94, 1.11) 0.63 2.94 2.852nd Coprimary 1.04 (0.97, 1.11) 0.27 5.52 5.28
Microvascular 0.97 (0.90, 1.05) 0.43 3.87 3.99Death 0.98 (0.90, 1.08) 0.70 2.57 2.60
MI 1.02 (0.88, 1.19) 0.75 0.93 0.90Stroke 1.03 (0.89, 1.21) 0.69 0.91 0.88CV Death 1.00 (0.89, 1.13) 0.98 1.57 1.55CHF Hospital 0.90 (0.77, 1.05) 0.16 0.85 0.95Revascularized 1.06 (0.96, 1.16) 0.24 2.69 2.52
0,5 1 2 Favors StandardFavors Insulin
HR
ORIGIN Trial Investigators, N Engl J Med 367: 319-28, 2012
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Marso SP et al. N Engl J Med. 377(8):723-732, 2017
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
DEVOTE Kaplan–Meier Analysis of the Composite Primary Outcome
Marso SP et al. N Engl J Med. 377(8):723-732, 2017
Rate:4.71/100 PYO
Rate:4.29/100 PYO
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Devote Primary Endpoints: 3-Point MACE, 4-Point MACE, and All-Cause Mortality
Marso SP et al. N Engl J Med. 377(8):723-732, 2017
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Titration algorithm: insulin degludec and insulin glargine
Meneghini L et al. Diabetes Care 36:858–864, 2013
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Treatment with insulin is associated with body
weight gain.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
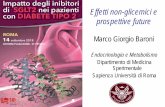
Type 2 diabetes –weight gain over time is associated with insulin and oral antidiabetic therapies
These major trials have shown weight gain over time:
– UKPDS, significant mean increase of 3.1 kg in weight in the intensive treatment (sulphonylurea or insulin) group compared with the conventional treatment (diet and exercise) group1
– Action to Control Cardiovascular Risk in Diabetes (ACCORD), where patients receiving intensive therapy (targeting an HbA1c 10 kg3
– In A Diabetes Outcome Progression Trial (ADOPT), patients receiving glibenclamidegained an average of 1.6 kg over a median treatment duration of3.3 years4
1. UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:837–53; 2. UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854–65;3. Members of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Study Group. N Engl J Med 2008;358:2545–59; 4. Kahn SE, Haffner SM, Heise MA, et al. for the ADOPT Study Group. N Engl J Med 2006;355:2427–43.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
In the UKPDS, insulin-treated patients with type 2 diabetes gained the most weight
UKPDS 34. Lancet 1998:352:854–865.
insulinconventional chlorpropamideglibenclamide
Chan
ge in
wei
ght (
kg)
Years from randomisation
10
0
2.5
5
7.5
0 3 6 9 12
metformin
While patients on all therapies gained weight, patients receiving insulin gained the most (up to 8 kg after 12 years of insulin therapy)
–2.5Diapos
itiva pre
parata d
a MARC
O BARO
NI e ced
uta alla
Società
Italiana
di Diabe
tologia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin and weight
• Reduced glycosuria
• Anabolic action of insulin
• Fluid retention
• Hypoglycaemia and increased calorie consumption
• Excess insulin administrationDiapositiv
a prepa
rata da
MARCO
BARONI
e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Network meta-analysis of pairwise comparisons of randomised controlled trials evaluating the use of anti-hyperglycaemic agents in addition to metformin vs.
placebo: Mean change from baseline in body weight
3,41
2,462,17
1,4 1,38
0,23
-1,01
-1,66-2
-3
-2
-1
0
1
2
3
4
Mea
n ch
ange
from
bas
elin
e in
bod
y w
eigh
t
Biphasic TZDs SU Glinides Basal DPP-4 Acarbose GLP-1R SGLT2*Insulin Insulin inhibitors agonists inhibitors
Liu S-C et al. Diabetes Obes and Metab 2012; 14: 810-820b Fujita Y et al. J Diabetes Investing 2014; 5: 265-275
*An estimate of body weight reduction; SGLT2 inhibitors were not included in the network analysis
DPP-4, dipeptidyl peptidase-4; SGLT2, sodium glucose cotransporter-2; TZDs, thiazolidinediones; GLP-1R, glucagon-like peptide 1 receptor; SU, sulphonylurea
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Treatment with insulin is associated with
body weight gain.
Treatment with insulin is associated with
increased risk for hypoglycemia.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Yki-Jarvinen et al. Ann Int Med 1999
Hypoglycaemia limits further reduction of FPG with basal insulin
Mea
n Hb
A 1c
[%]
Mean annual fasting blood glucose [mmol/l]
12
Freq
uenc
y of
Hyp
ogly
caem
ic
Episo
des [
%]
10
8
6
4
40
30
20
10
0
3 4 5 6 7 8 9 10 11
3 4 5 6 7 8 9 10 11
n = 13,072
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Thomas R. Pieber et al Diabetologia 2017
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Network meta-analysis of pairwise comparisons of randomised controlled trials evaluating the use of anti-hyperglycaemic agents in addition to metformin vs.
placebo: At least one event of overall hypoglycaemia (odds ratio)
17,78
10,51
8,86
4,77
1,13 0,92 0,45 0,41,1
0
2
4
6
8
10
12
14
16
18
20
Biphasic Glinides SU Basal DPP-4 GLP-1R TZDs Acarbose SGLT2*Insulin Insulin inhibitors agonists inhibitors
At le
ast o
ne e
vent
of o
vera
ll hy
pogl
ycae
mia
(odd
s ra
tio)
*An estimate of hypoglycaemia risk; SGLT2 inhibitors were not included in the network analysis b
Liu S-C et al. Diabetes Obes and Metab 2012; 14: 810-820b Fujita Y et al. J Diabetes Investing 2014; 5: 265-275
DPP-4, dipeptidyl peptidase-4; SGLT2, sodium glucose cotransporter-2; TZDs, thiazolidinediones; GLP-1R, glucagon-like peptide 1 receptor; SU, sulphonylurea
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
4T Study: Glycated Hemoglobin Level, Hypoglycemia, and Increase in Body Weight at 1 Year and 3 Years
N Engl J Med 361;18, 2009
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Black box denotes both treatment arms switching to NPH for 1 week then resuming IDeg or IGlar to allow for antibody measurement
Zinman et al. Diab Care 35:2464–71, 2012; Rodbard et al. Diabetic Med 30:1298–304, 2013
CoreCore0,0
0,2
0,4
0,6
0,8
1,0
52 65 78 91 104
Nocturnal confirm
ed hypoglycaemia
(cumulative events per patient)
0,0
0,2
0,4
0,6
0,8
1,0
0 13 26 39 52
Noc
turn
al c
onfir
med
hyp
ogly
caem
ia(c
umul
ativ
e ev
ents
per
pat
ient
)
0
1
2
3
4
5
52 65 78 91 104
Confirmed hypoglycaem
ia(cum
ulative events per patient)
0
1
2
3
4
5
0 13 26 39 52
Conf
irm
ed h
ypog
lyca
emia
(c
umul
ativ
e ev
ents
per
pat
ient
)
5,0
5,5
6,0
6,5
7,0
7,5
8,0
8,5
9,0
0 4 8 1216202428323640444852
HbA
1c(%
)
3
4
5
6
7
8
9
10
11
0 4 8 1216202428323640444852
FPG
(m
mol
/L)
HbA1c FPG
Confirmed hypoglycaemia Nocturnal confirmed hypoglycaemia
18% lower rate with IDeg (ns)
Extension
16% lower rate with IDeg (ns)
Extension
43% lower rate with IDeg, p=0.002
5,0
5,5
6,0
6,5
7,0
7,5
8,0
8,5
9,0
525660646872768084889296100104
HbA
1c (%)
0.0
Treatment difference:
non-inferior
26
Extension0.0
Treatment difference:
0.12%-points (ns)
65 79 91 104Time (weeks)
Core3
4
5
6
7
8
9
10
11
525660646872768084889296100104
FPG (m
mol/L)
0
Treatment difference:
–0.43 mmol/L, p=0.005
26
Core Extension0
Treatment difference:
–0.38 mmol/L, p=0.019
65 79 91 104Time (weeks)
Time (weeks) Time (weeks)
36% lower rate with IDeg, p=0.038
IDeg OD I Glar OD
Insulin-naïve T2D: study designBEGIN ONCE LONG – 2 years
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Marso SP et al. N Engl J Med. 377(8):723-732, 2017
Devote Secondary Endpoints: Rates of severe hypoglycaemia
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Marso SP et al. N Engl J Med. 377(8):723-732, 2017
Devote Secondary Endpoints: Rates of nocturnal severe hypoglycaemia
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Treatment with insulin is associated with
body weight gain.
Treatment with insulin is associated with
increased risk for hypoglycemia.
Insulin therapy needs to control both
FPG and post-prandial PG.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Comparison of 24-hour plasma glucose levels in healthy subjects vs patients with diabetes (p
-
Insulin therapy needs to control both FPG and post-prandial PG
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Glycaemic control (%) in patients with T2DM initiating basal insulin in Europe and the USA
Mauricio D et al. Diabetes Obes Metab 19:1155–1164, 2017
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Treatment with insulin is associated with
body weight gain.
Treatment with insulin is associated with
increased risk for hypoglycemia.
Insulin therapy needs to control both
FPG and post-prandial PG.
Insulin treatment may be refused by the
patient barriers.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
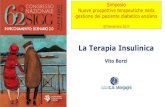
Reasons why health-care professionals and patients might refrain from starting insulin
treatment
Cahn A et al. Lancet 2015
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Patient-cited issues with insulin treatment
66,7%
59,8%
54,4%
81,4%
23,1%
27,6%
0% 20% 40% 60% 80% 100%
Insulin-treated diabetes controls their life
Insulin regimen can be restrictive
Hard to live normal life while managingdiabetes
Wish insulin regimen would fit daily lifechanges
Number of daily injections
Taking insulin at prescribed time/mealseveryday
Percentage
Peyrot et al. Diabetic Med 29:682–9, 2012
GAPP™• A global internet survey of patient
and physician beliefs regarding insulin therapy
• n=1530 insulin treated patients with diabetes
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Insulin therapy in T2DM
ADVANTAGES
The primary defect in insulin secretion is
reverted by insulin treatment
Insulin treatment reverted defects in
hepatic glucose production.
Insulin therapy is not associated with
atherogenesis and increased risk of CV
events.
Basal insulin is easy to use : one insulin,
once daily injection, one glucose target
(FPG), and easy dose titration (FPG).
LIMITATIONS
Treatment with insulin is associated with
body weight gain.
Treatment with insulin is associated with
increased risk for hypoglycemia.
Insulin therapy needs to control both
FPG and post-prandial PG.
Insulin treatment may be refused by the
patient barriers.
Insulin treatment is associated with
clinical inertia.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Median time to intensification and mean HbA1c at intensification in patients with T2DM currently treated with 1-2 OADs with intensification to 3 OADs or insulin
Khunti et al. Diabetes Care 36:3411-7, 2013
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Consequences of delayed intervention in patients with T2DM
Paul, SK et al. Cardiovasc. Diabetol. 14: 100, 2015
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
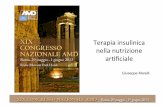
Modified from Raccah d et al. Diabetes Metab Res Rev 23: 257-264, 2007
??
Diet and exercise
Oral mono-or
combinationtherapy
Basal insulinOnce-daily
?
HbA1cuncontrolled
Time
HbA1c uncontrolled,FBG on target, PPBG >160 mg/dl
What next?
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Modified from Raccah d et al. Diabetes Metab Res Rev 23: 257-264, 2007
??
Diet and exercise
Oral mono-or
combinationtherapy
Basal insulinOnce-daily
Basal Bolus
3 prandial
HbA1cuncontrolled
Time
HbA1c uncontrolled,FBG on target, PPBG >160 mg/dl
Basal Plus
2 prandial for largest
glucoseexcurtions
Basal Plus
One prandial for largest
glucoseexcurtion
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Arguments in favor of timely insulin use in T2DM
• The defect in insulin secretion is a primary one.• Insulin treatment reverted defects in insulin secretion and
hepatic glucose production.
• Early insulin initiation is associated with reduced CVD risk• Treatment with insulin has high efficacy and is indicated in
certain clinical condition (pregnancy, hospitalized patients, critically ill patients).
• Increase in body weight and the risk for hypoglycemia may be minimized.
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
What are the real unmet needs in insulin therapy
• Early recognition of failure of oral therapy• Strong positive recommendation of benefits of
insulin treatment to patients• Reassurance concerning potential negative
consequences in therapy• Intense support to optimise insulin dosage• Regular expert clinic review to identify problems
with insulin therapyDiapos
itiva pre
parata d
a MARC
O BARO
NI e ced
uta alla
Società
Italiana
di Diabe
tologia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Need for personalized care
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Grazie
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
-
Diaposit
iva prep
arata da
MARCO
BARON
I e cedu
ta alla S
ocietà It
aliana d
i Diabeto
logia.
Per rice
vere la v
ersione
original
e si pre
ga di scr
ivere a
siditalia
@sidita
lia.it
Vantaggi e limiti della terapia insulinicaDichiaro di aver ricevuto negli ultimi due anni compensi o finanziamenti dalle seguenti Aziende Farmaceutiche e/o Diagnostiche:� �Sanofi�Novo Nordisk�Abbott�Diabetes is a progressive disease that requires reassessment to reach targetDiapositiva numero 4Diapositiva numero 5Early vs late glycemic intervention: �UKPDS enrolled newly diagnosed patientsDiapositiva numero 7Insulin therapy in T2DMDiapositiva numero 9Insulin and glucagon dynamics in response to meals are abnormal in type 2 diabetes�Diapositiva numero 12Diapositiva numero 13Diapositiva numero 14Diapositiva numero 15Diapositiva numero 16Effetto della terapia insulinica intensiva sulla funzione -cellulare e sul controllo glicemico in diabetici tipo 2 di nuova diagnosi�Diapositiva numero 18Insulin therapy in T2DMKey Pathogenetic Defects in T2DM:�The Ominous OctetDiapositiva numero 21Diapositiva numero 22Diapositiva numero 23Diapositiva numero 24Insulin therapy in T2DMDiapositiva numero 26ORIGIN�Primary & Secondary Outcomes & their ComponentsDiapositiva numero 28DEVOTE �Kaplan–Meier Analysis of the Composite Primary OutcomeDEVOTE Primary Endpoints:�3-Point MACE, 4-Point MACE, and All-Cause DeathInsulin therapy in T2DMTitration algorithm: insulin degludec and insulin glargineInsulin therapy in T2DMType 2 diabetes –weight gain over time is associated with insulin and oral antidiabetic therapiesIn the UKPDS, insulin-treated patients �with type 2 diabetes gained the most weightDiapositiva numero 36Diapositiva numero 37Insulin therapy in T2DMHypoglycaemia limits further reduction of FPG with basal insulinDiapositiva numero 41Diapositiva numero 424T Study: Glycated Hemoglobin Level, Hypoglycemia, and Increase in Body Weight at 1 Year and 3 YearsInsulin-naïve T2D: study design�BEGIN ONCE LONG – 2 yearsDEVOTE Secondary Endpoints:�Rates of Severe HypoglycemiaDEVOTE Secondary Endpoints:�Rates of Nocturnal Severe HypoglycemiaInsulin therapy in T2DM24-hour plasma glucose profile in T2DM and healthy subjectsThe Importance of Controlling PPGDiapositiva numero 50Insulin therapy in T2DMReasons why health-care professionals and patients might refrain from starting insulin treatmentPatient-cited issues with insulin treatmentInsulin therapy in T2DMClinical Inertia With Insulin TherapyDiapositiva numero 57Diapositiva numero 59Diapositiva numero 60Diapositiva numero 61Arguments in favor of timely insulin use in T2DMWhat are the real unmet needs in insulin therapyNeed for Personalized Care Diapositiva numero 65Diapositiva numero 66