Umberto Volta Resp. SSO Malattia Celiaca Dipartimento di ...doc/U-Volta.pdf · senza Glutine...
37
Celiachia a 360°: dalla Medicina alle Scienze Sociali e alla Tecnologia Alimentare Firenze, Palazzo dei Congressi 29-31 Marzo 2012 Sessione B, Sabato 31 Marzo 2012 Celiachia: oltre la Sicurezza Alimentare, Ristorazione fuori Casa e Qualità Aspetti Metabolici dell’Alimentazione senza Glutine Umberto Volta Resp. SSO Malattia Celiaca Dipartimento di Malattie dell’Apparato Digerente e Medicina Interna, Azienda Ospedaliero-Universitaria , Bologna
Transcript of Umberto Volta Resp. SSO Malattia Celiaca Dipartimento di ...doc/U-Volta.pdf · senza Glutine...

Celiachia a 360°: dalla Medicina alle Scienze Sociali
e alla Tecnologia Alimentare Firenze, Palazzo dei Congressi
29-31 Marzo 2012
Sessione B, Sabato 31 Marzo 2012
Celiachia: oltre la Sicurezza Alimentare, Ristorazione fuori Casa e Qualità
Aspetti Metabolici dell’Alimentazione senza Glutine
Umberto VoltaResp. SSO Malattia Celiaca
Dipartimento di Malattie dell’Apparato Digerente e Medicina Interna, Azienda Ospedaliero-Universitaria , Bologna
Gluten-free diet is the only effectivetreatment for coeliac disease
▲Disappearance of intestinal and extra-intestinal symptoms▲Normalization of duodenal histology ▲Antibody disappearance▲Prevention of auto-immune disorders ▲Protection against complication (refractory CD, intestinal lymphoma)
LIGHTS SHADES
▲Minerals and vitamins deficiency▲Psychological problems▲Metabolic Abnorm.▲Increased cardiovascular risk
Gluten-free Diet (GFD)
• Gluten proteins do not have a high biological value since they do not contain some essential amino acids. The exclusion of gluten-containing foods from the diet does not represent a problem from a nutritional point of view.
• However, GFD can be responsible of psychologycal and social problems considering the relevant role of cereals and gluten-containing foods in our alimentary life-style and culture
• A life-long strict GFD implies a positive awareness of a radical life-style change with a careful participation in the choices of the new alimentary regimen for a correct and balanced nutrition
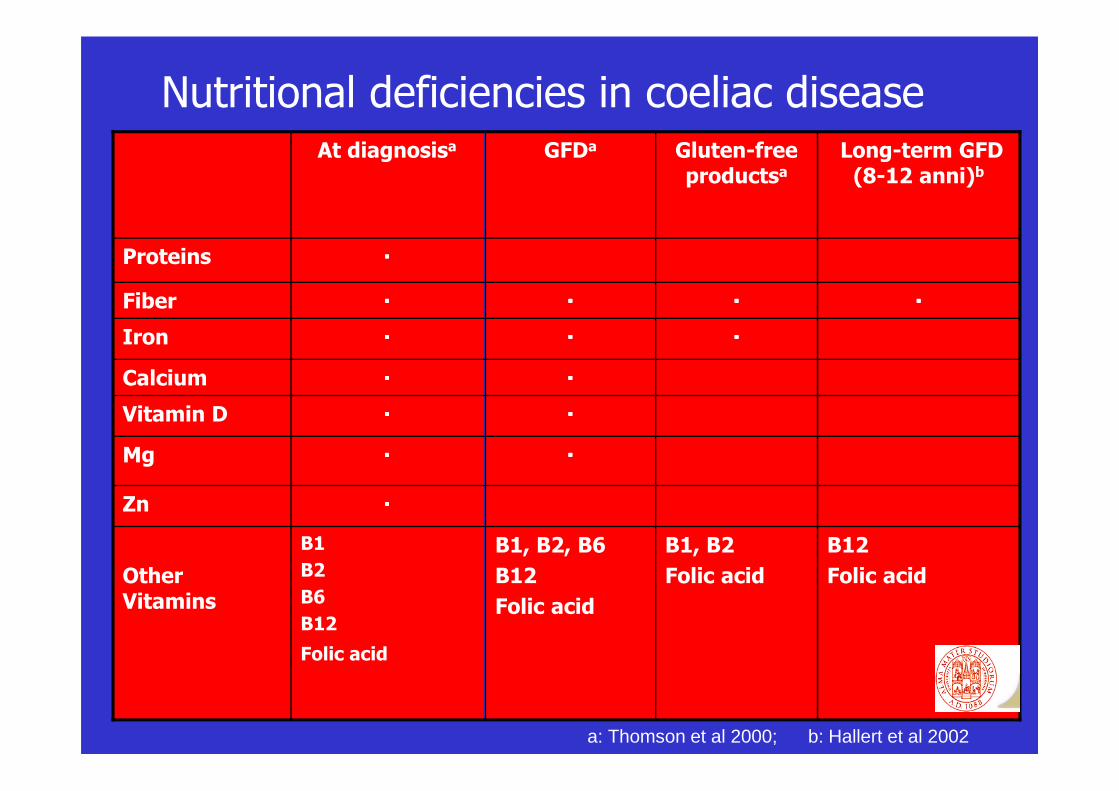
Nutritional deficiencies in coeliac disease
B1
B2
B6
B12
Folic acid
Other Vitamins
B12
Folic acid
B1, B2
Folic acid
B1, B2, B6
B12
Folic acid
Zn
Mg
Vitamin D
Calcium
Iron
Fiber
Proteins
Long-term GFD (8-12 anni)b
Gluten-free productsa
GFDaAt diagnosisa
a: Thomson et al 2000; b: Hallert et al 2002
Nutritional intake in young coeliac disease (CD) patients with a strict compliance with GFD
• Young CD patients with a strict compliance with GFDoften showed an inadequate nutritional intake
• Fiber and iron intakes were significantly lower and thesaturated fat intake was significantly higher thanrecommended but comparable with the general population
• Better medical and dietary support is necessary to preventlong-term complications and to achieve an ongoingsatisfying management in the group of young patients withCD
Hopman E et al, JPGN 2006
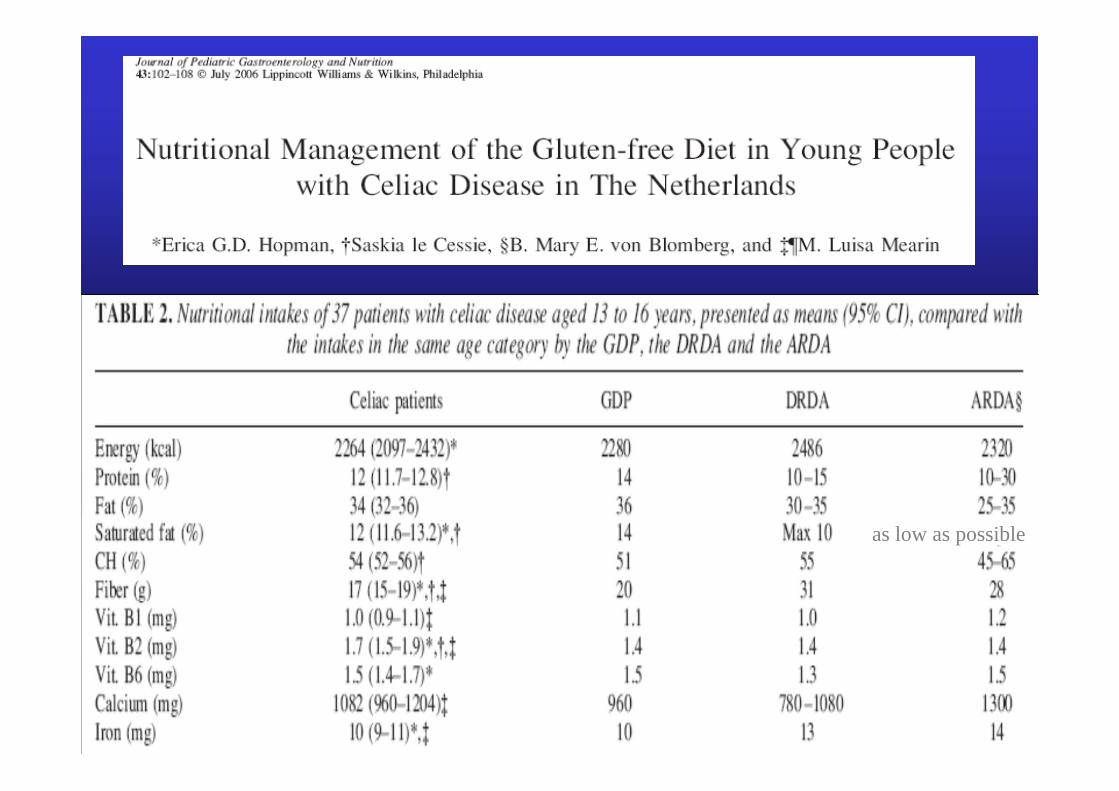
as low as possible
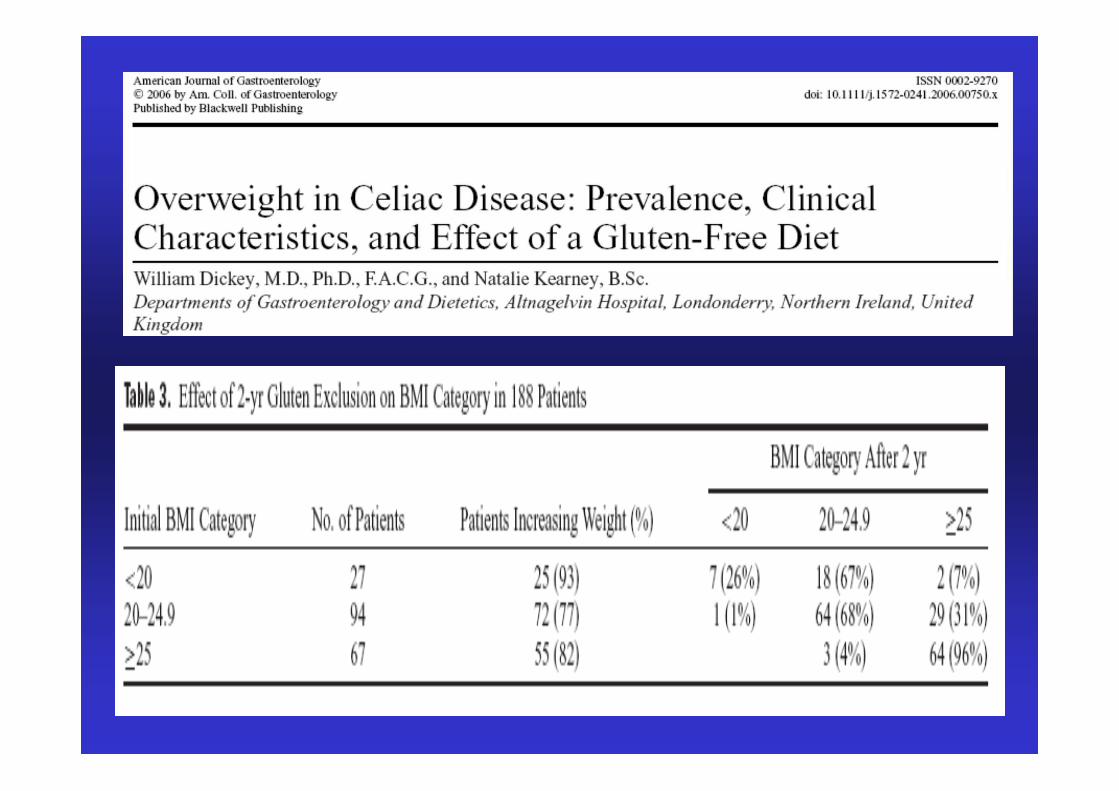
Gluten-free diet and metabolic abnormalities
� In coeliac disease on a GFDclinical experience andliterature data showthat a number of patients tend tooverweight up to obesity
� The development of overweight can be explained by thenormalization of intestinal absorption due to the regrowthof duodenal villi and to the high content of lipids of somedietary commercial products
Kupper C, Gastroenterology 2005
High fat content of gluten-free commercial products
• Bread substitutes (slice toasted, crackers, breadsticks)4 fat content from 1.5% a 20%4 caloric intake from 353 a 466 kcal per 100 grams4 rarely reported fat saturated content4 most of products contain “oils and/or
vegetable margarines”
• Sweets, biscuits/wafers and snacks4 fat content from 5% to 30%4 caloric intake from 300 to 550 kcal per 100 grams4 most of products contain “oils and/or vegetables
margarines (oils of palm/coconut palm)”

The Gluten -Free Diet (GFD): a Nutritional Risk Factor for
Adolescents with Celiac Disease?
Mariani P., J Pediatric Gastroenterol Nutr 1998
1. Adolescent celiacs in GFD usually had a highdietary intake in fat and proteins and a poor intake incarbohydrates.
2. The prevalence of overweight and obesity washigher in adolescents celiacs following a strict GFDthan in those with a partial compliance with GFD andcontrols on a gluten containing diet.
How does feeding change by following a GFD regimen?
• Both children and adults on GFDchange their dietcomposition by a lower intake of carbohydrates and ahigher amount of fat and proteins in comparison with thegeneral population:�The intake of gluten-free dietary bread substitutes such
as thin breadsticks and snacks with a high fat contentof poor quality is usually high in celiacs
�Gluten-free bread, pasta and pizza are less appetizingthan the same gluten-containing foods and for thisreason their intake is usually lower in celiacscontributing to the lowintake of carbohydrates
�Celiacs tend to eat more meat, eggs, milk and cheesewith a higher intake of proteins compared with the nonceliac general population
1. Mariani P, J Pediatr Gastroenterol Nutr; 2. Bardella MT, Am J Clin Nutr 2000
Why do celiacs increase their weight after starting GFD?
� Nutrient absorption improves following the normalizationof small intestinal mucosa.
� Coeliacs reach satiety sensation after a higher caloric intakedue to the reduced fiber content of GFD.
� Coeliacs do not increase their caloric consumption keepingunchanged their physical activity.
� A bad choice of gluten-free commercial foods can cause asignificant increase of fat and caloric intake, i.e. thereplacement of bread with thin breadsticks or salt snacksdo increase fat content from2 to 10-14 g and the caloriccontent of 90 kcal per 100 g of the product.
� Rarely celiacs are advised to make more frequent theirphysical activity taking in account of the newalimentaryregimen.
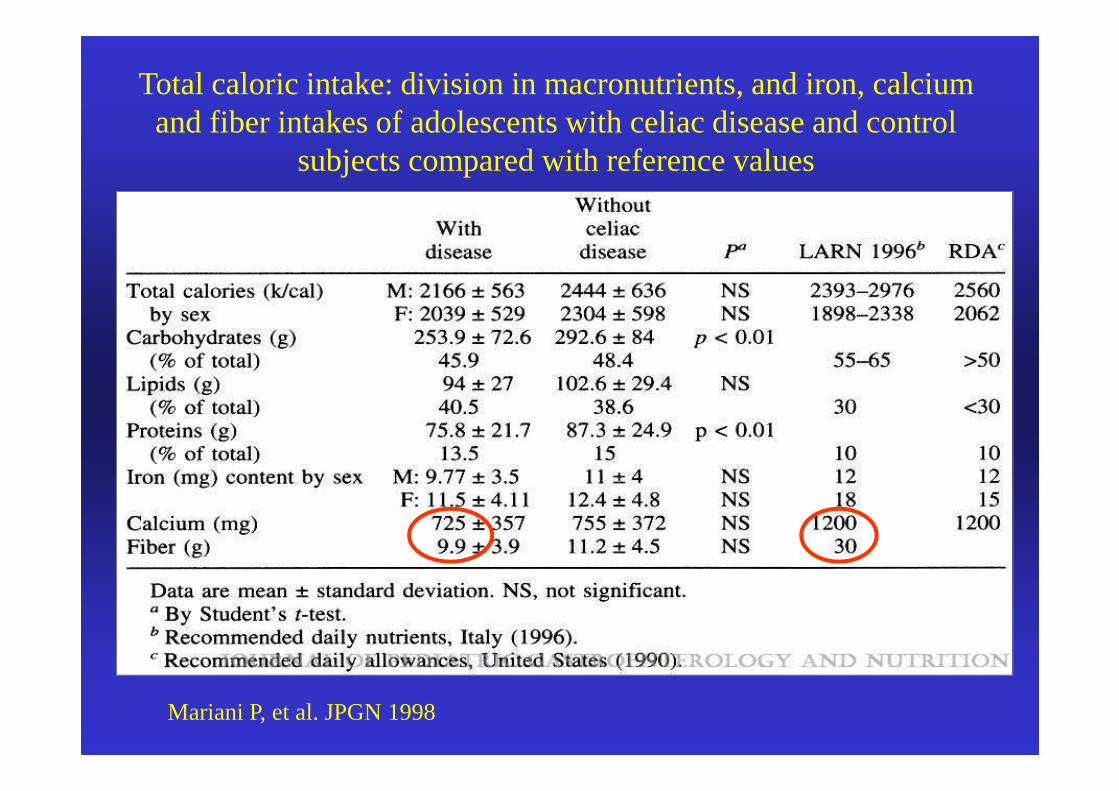
Total caloric intake: division in macronutrients, and iron, calciumand fiber intakes of adolescents with celiac disease and control
subjects compared with reference values
Mariani P, et al. JPGN 1998
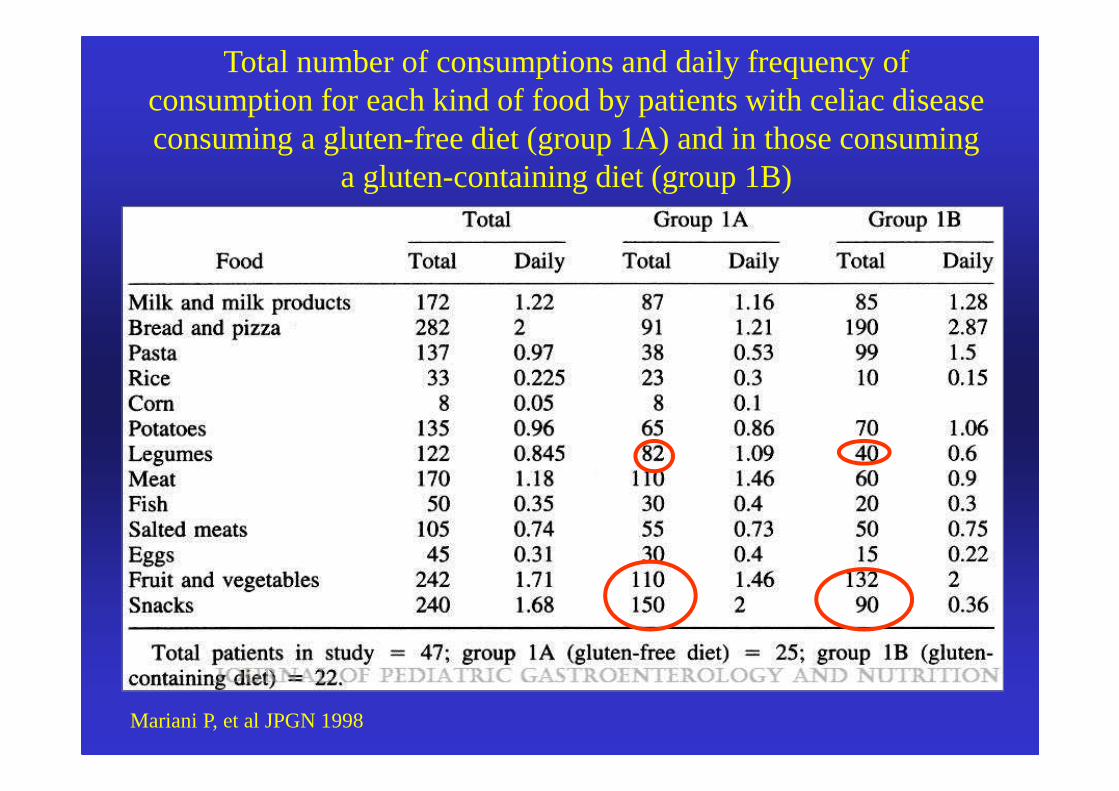
Total number of consumptions and daily frequency of consumption for each kind of food by patients with celiac disease consuming a gluten-free diet (group 1A) and in those consuming
a gluten-containing diet (group 1B)
Mariani P, et al JPGN 1998
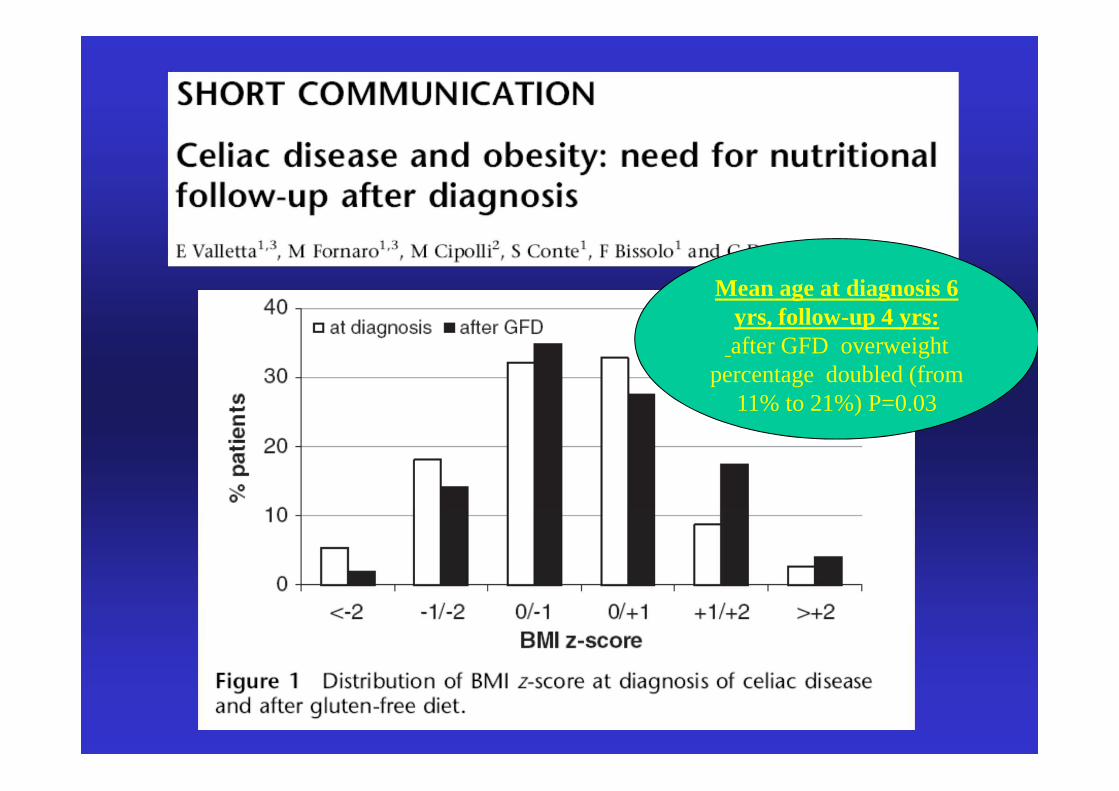
Mean age at diagnosis 6 yrs, follow-up 4 yrs:after GFD overweight
percentage doubled (from 11% to 21%) P=0.03
0
10
20
30
40
50
60
70
80
90
low weight normal overweight obesity
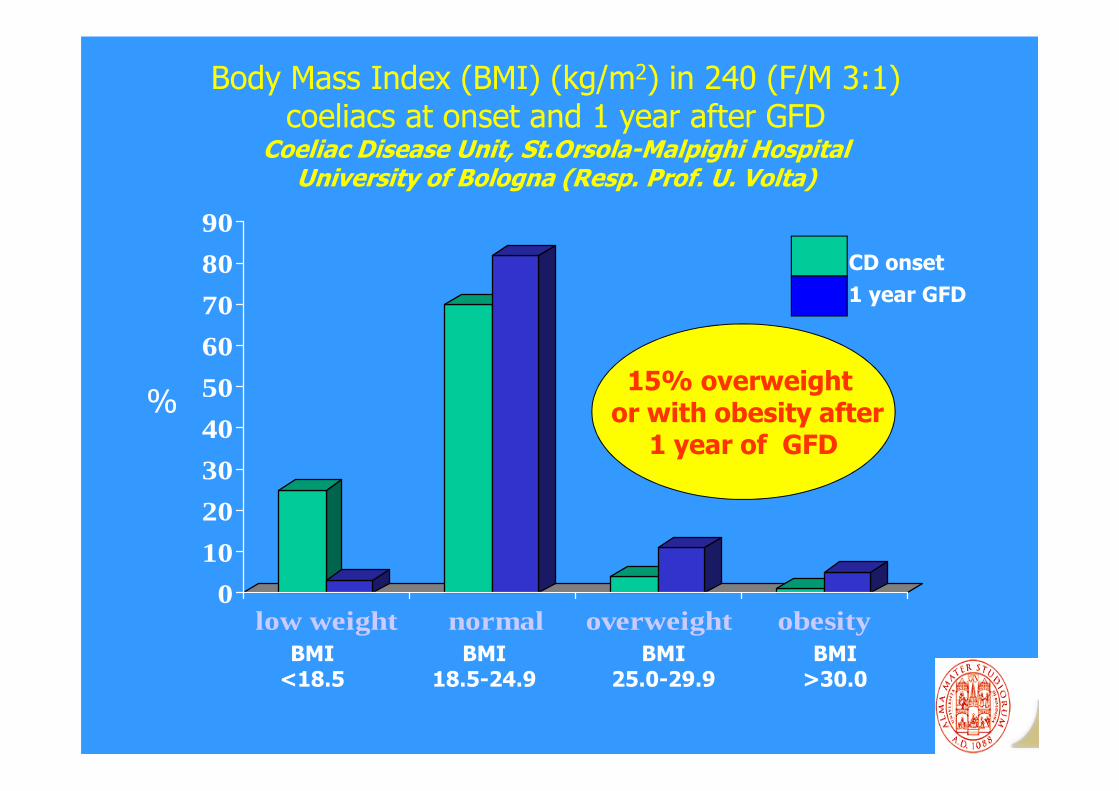
Body Mass Index (BMI) (kg/m2) in 240 (F/M 3:1) coeliacs at onset and 1 year after GFD
Coeliac Disease Unit, St.Orsola-Malpighi HospitalUniversity of Bologna (Resp. Prof. U. Volta)
BMI<18.5
%
BMI18.5-24.9
BMI25.0-29.9
BMI>30.0
CD onset
1 year GFD
15% overweight or with obesity after
1 year of GFD

05
101520253035404550
cholesterol tryglic. glucose
Metabolic abnormalities in 240 consecutive coeliacs at onset and 1 year after GFD
Coeliac Disease Unit St.Orsola-Malpighi HospitalUniversity of Bologna (Resp. Prof. U. Volta)
%
CD onset
GFD 1 year
↑↑↑↑ ↑↑↑↑ ↑↑↑↑
0
5
10
15
20
25
30
35
40
atdiagnosis
6 monthsof GFD
24 monthsof GFD
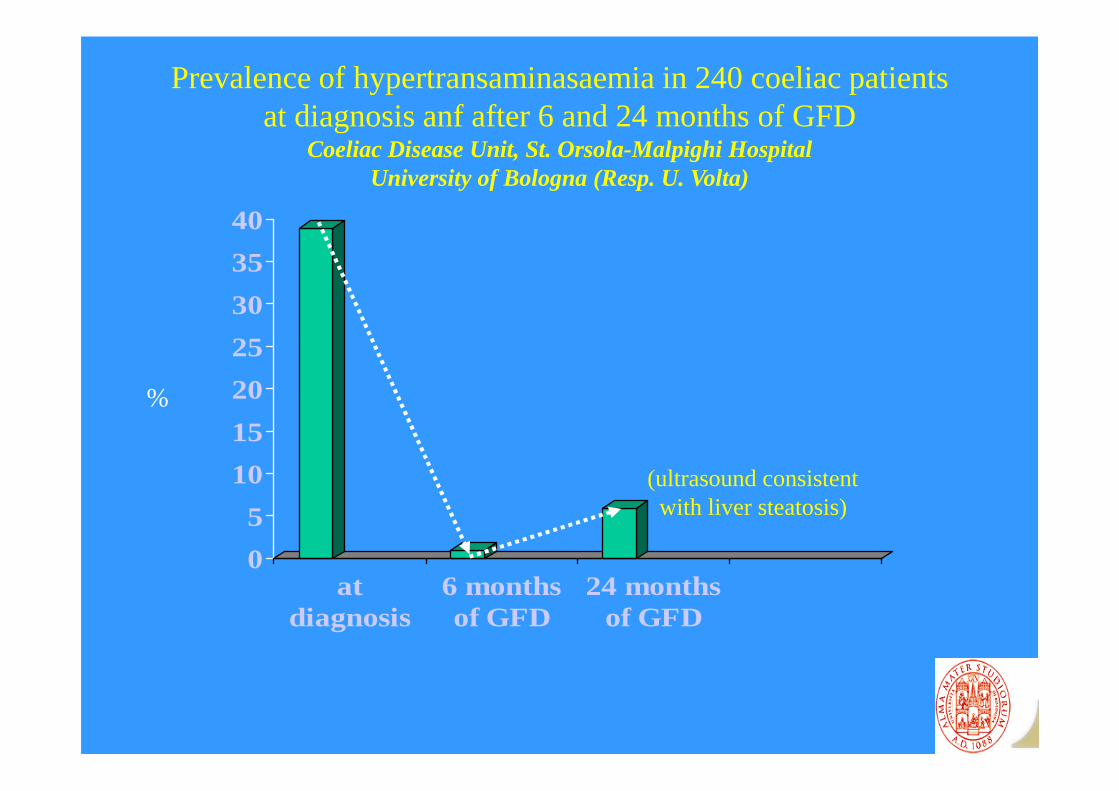
Prevalence of hypertransaminasaemia in 240 coeliac patients at diagnosis anf after 6 and 24 months of GFD
Coeliac Disease Unit, St. Orsola-Malpighi HospitalUniversity of Bologna (Resp. U. Volta)
%
(ultrasound consistent with liver steatosis)

GUIDELINES FOR THE DIAGNOSIS AND
FOLLOW -UP OF COELIAC DISEASEby
National Scientific Committee of the Italian Association of Coeliac Disease
(CSN A.I.C)U. Volta (coordinator), A. Calabrò, C. Catassi, I. De Vitis, P.
Lionetti, S. Martelossi, A. Picarelli, R. Troncone
in cooperation with the Italian Health Ministery
(published in the Official Gazette of the Italian Republic on February 7th 2008)
Follow-up GuidelinesIndications for monitoring
(Official Gazette of Italian Republic February 7th, 2008)
� Verification of the compliance with thediet
� Development of autoimmune disorders� Metabolic alterations� Neoplastic (lymphoma) and non-
neoplastic (refractory coeliac disease,ulcerative jejunum ileitis, collagenoussprue) complications
Follow-up of coeliac disease(Official Gazette of Italian Republic, February 7th 2008)
First evaluation 6 months after the diagnosis andthen yearly by means of:
• Medical examination and dietary interview• Blood absorption tests (ferritin, blood count
and other routine tests)• tTGA of IgA class (IgGclass if IgAdeficiency)TSH, anti-TPO, anti-TG
• Metabolic tests (cholesterol, HDL, tryglicerides,glucose, transaminases)

Metabolic abnormalities in coeliac disease (CD) after gluten-free diet (GFD)
CSN-AIC investigation in 109 CD Centers
109 CD Centers55 Pediatric
54 Adult
Overweight orobesity
5% childhood CD15% adult CD
↑Cholesterol5% childhood CD
15% adult CD
Availability of dieticians in 50%
of CD centers
Celiachia Notizie 2006
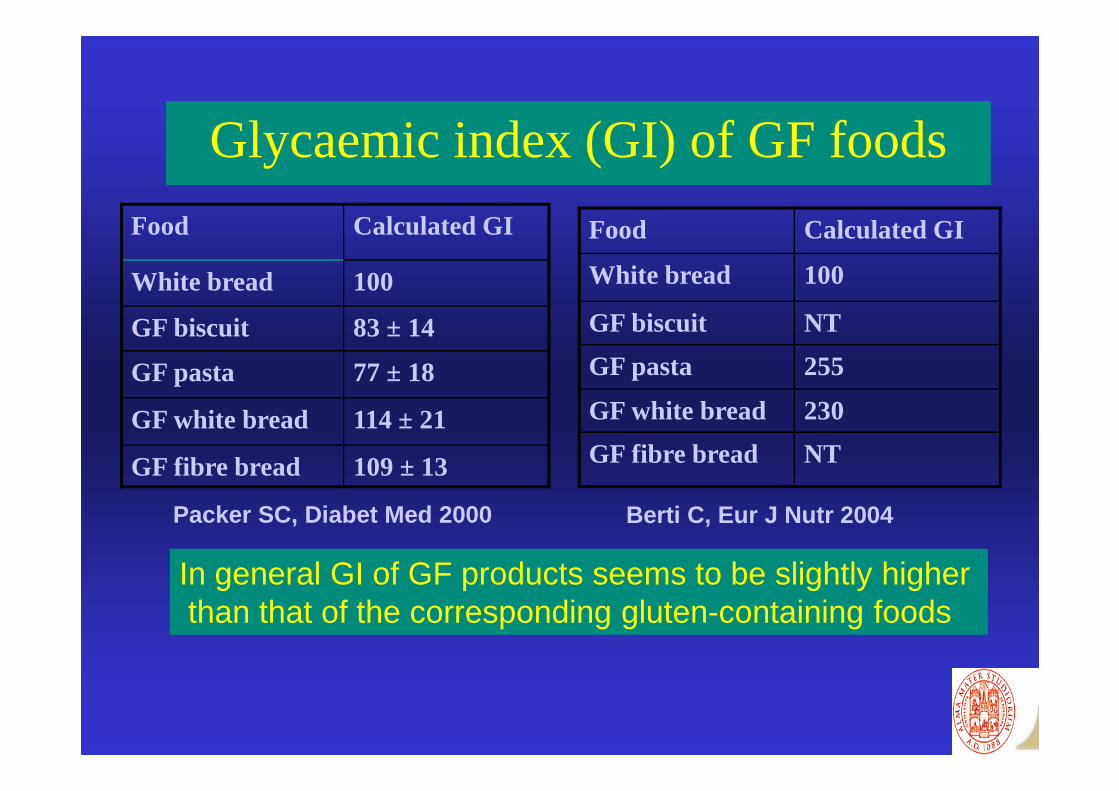
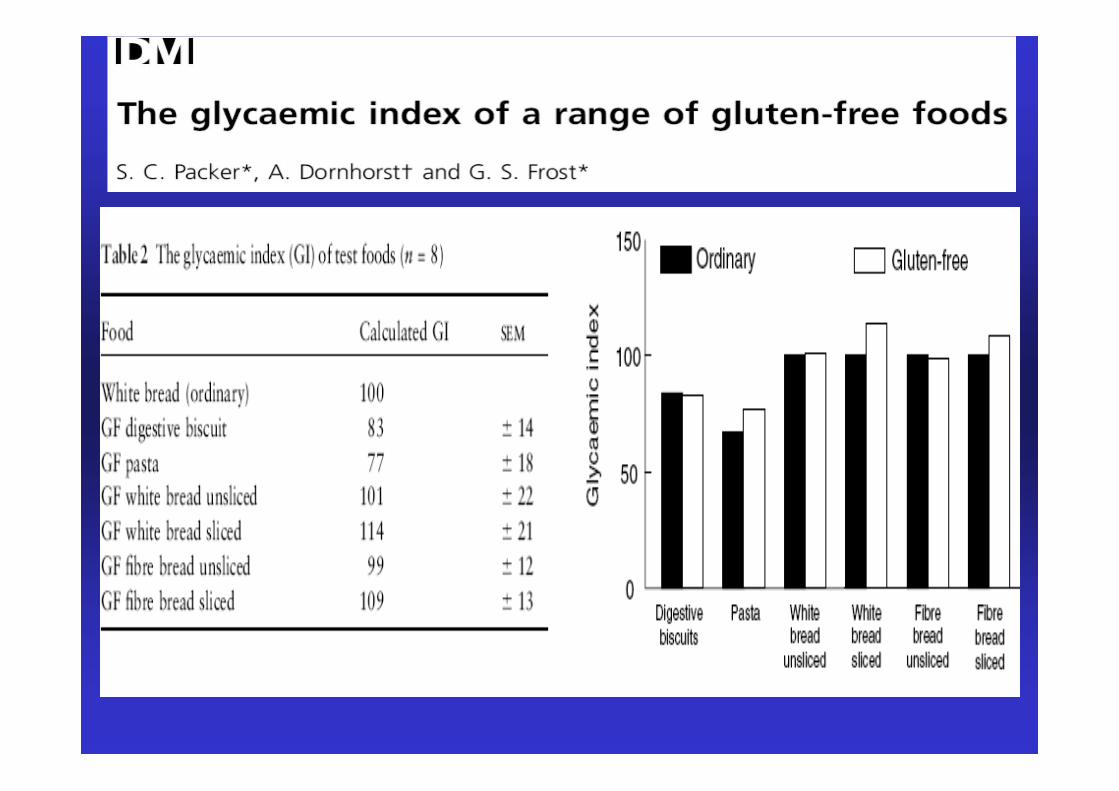
Glycaemic index (GI) of GF foods
Food Calculated GI
White bread 100
GF biscuit 83 ± 14
GF pasta 77 ± 18
GF white bread 114 ± 21
GF fibre bread 109 ± 13
Food Calculated GI
White bread 100
GF biscuit NT
GF pasta 255
GF white bread 230
GF fibre bread NT
Packer SC, Diabet Med 2000 Berti C, Eur J Nutr 2004
In general GI of GF products seems to be slightly higherthan that of the corresponding gluten-containing foods
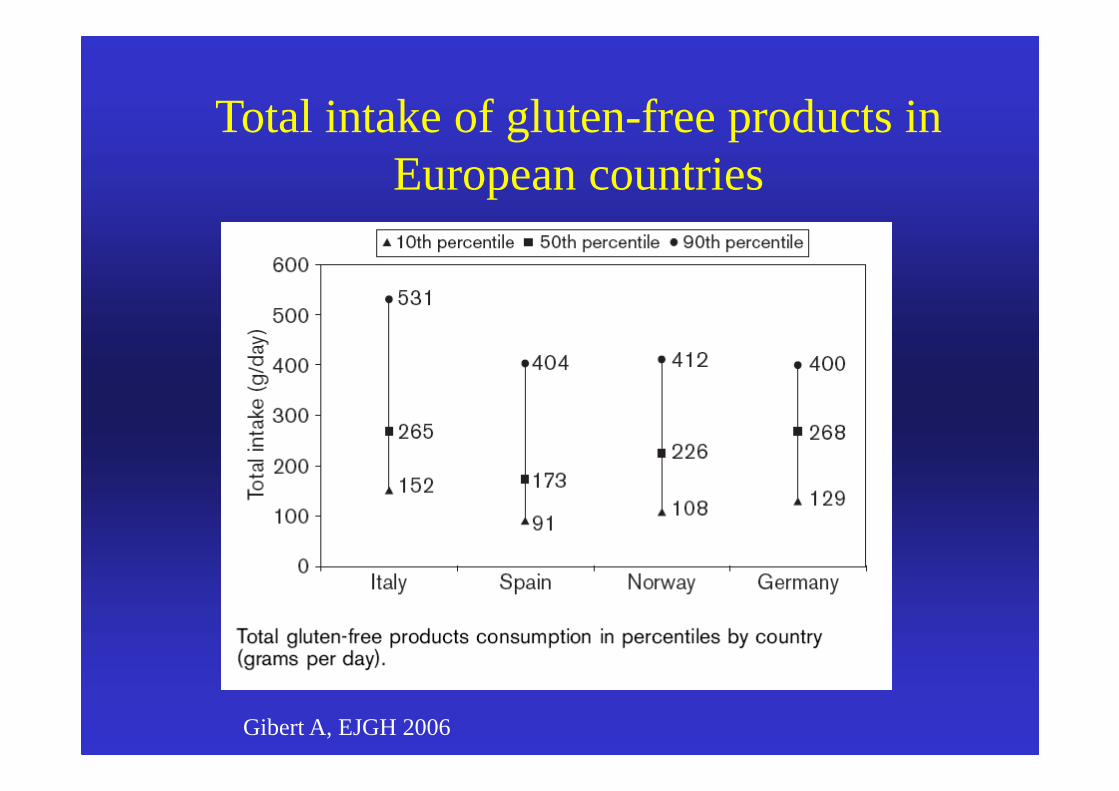
Total intake of gluten-free products in European countries
Gibert A, EJGH 2006
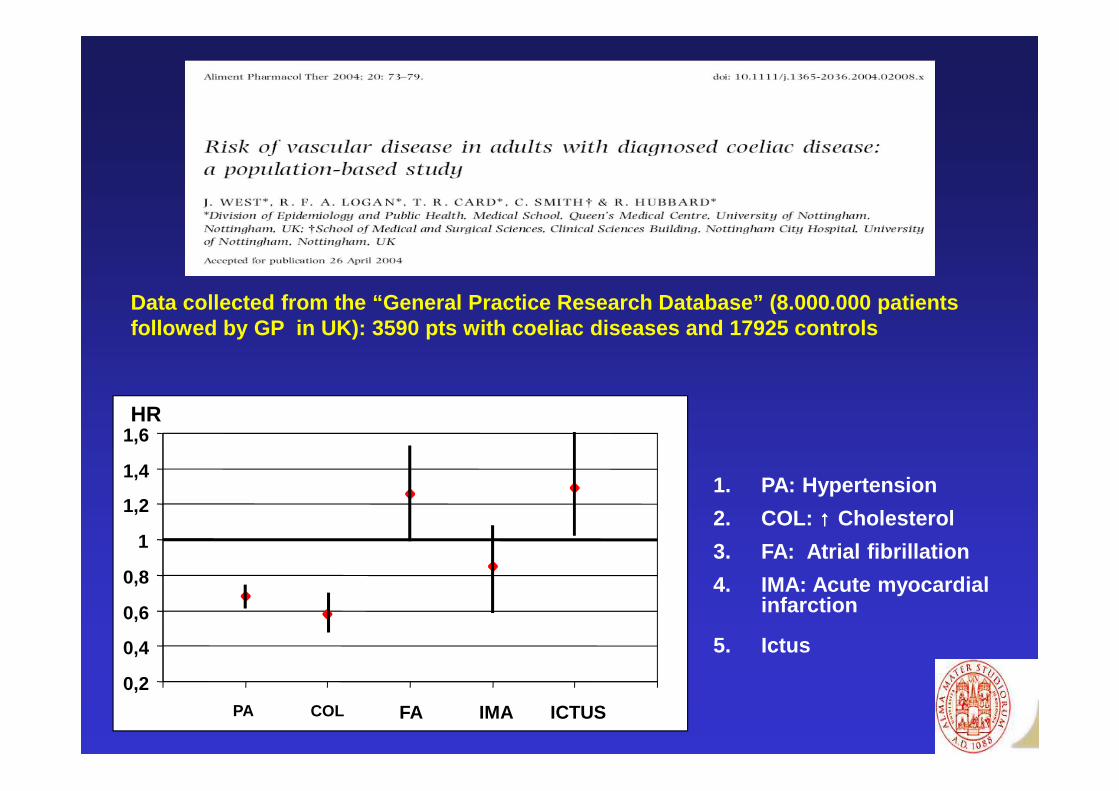
1. PA: Hypertension
2. COL: ↑↑↑↑ Cholesterol
3. FA: Atrial fibrillation
4. IMA: Acute myocardial infarction
5. Ictus
Data collected from the “General Practice Research Database” (8.000.000 patients followed by GP in UK): 3590 pts with coeliac disea ses and 17925 controls
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
PA COL FA IMA ICTUS
HR
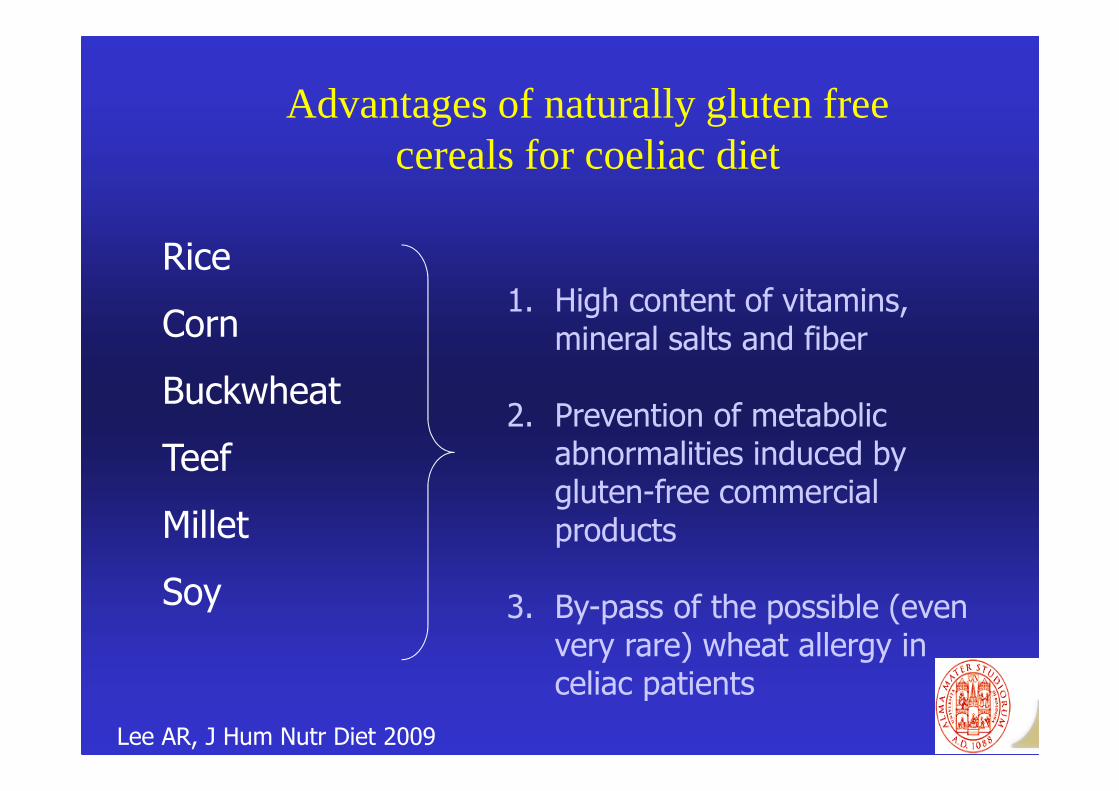
Advantages of naturally gluten free cereals for coeliac diet
Rice
Corn
Buckwheat
Teef
Millet
Soy
1. High content of vitamins, mineral salts and fiber
2. Prevention of metabolic abnormalities induced by gluten-free commercial products
3. By-pass of the possible (even very rare) wheat allergy in celiac patients
Lee AR, J Hum Nutr Diet 2009
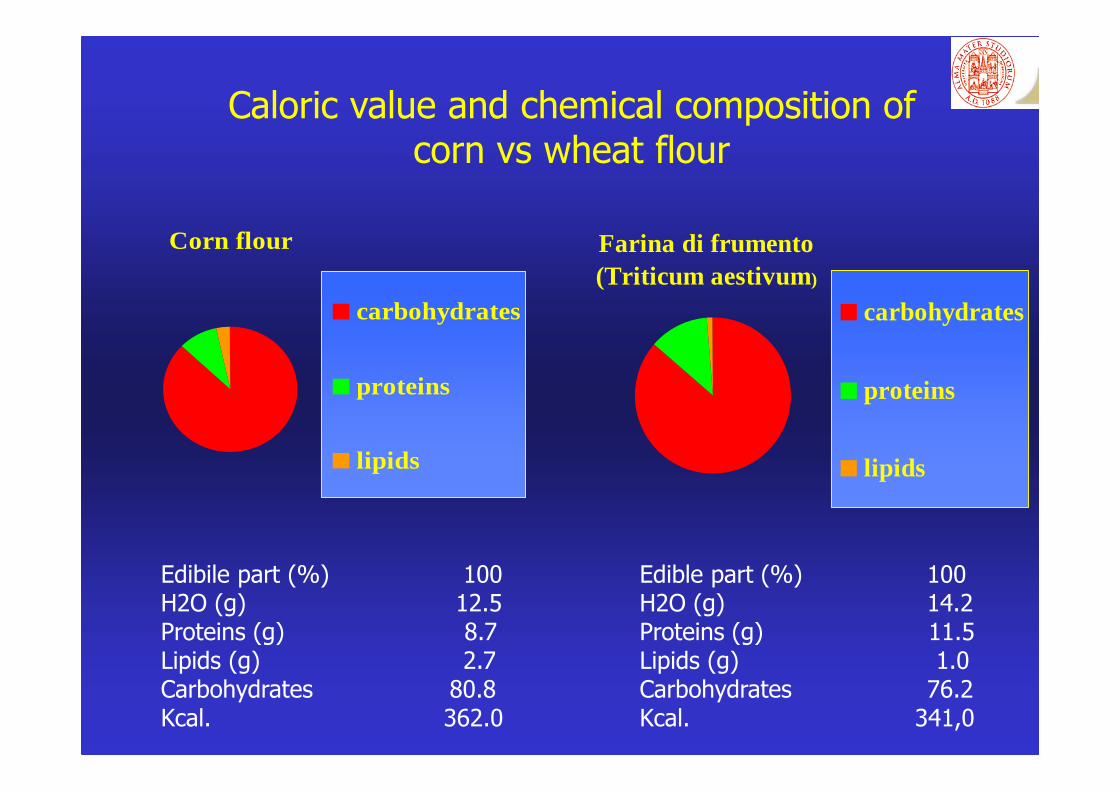
Corn flour
carbohydrates
proteins
lipids
Farina di frumento (Triticum aestivum)
carbohydrates
proteins
lipids
Edibile part (%) 100H2O (g) 12.5Proteins (g) 8.7Lipids (g) 2.7Carbohydrates 80.8Kcal. 362.0
Edible part (%) 100H2O (g) 14.2Proteins (g) 11.5Lipids (g) 1.0Carbohydrates 76.2Kcal. 341,0
Caloric value and chemical composition of corn vs wheat flour
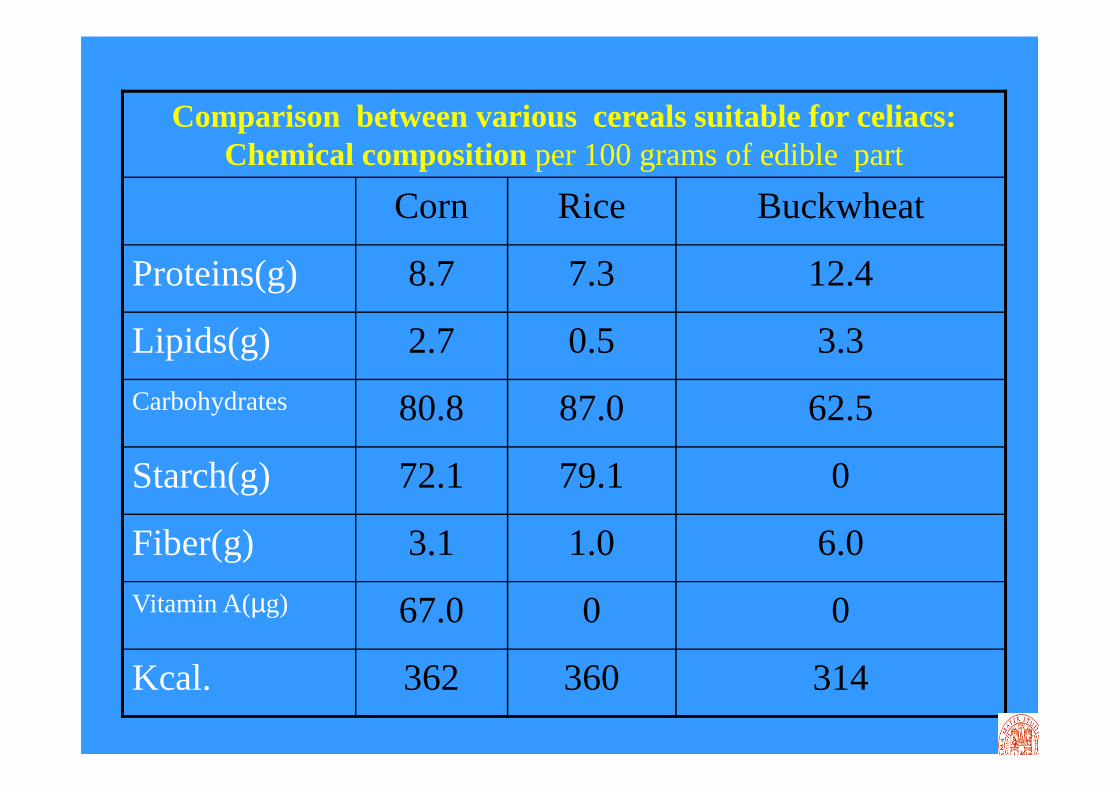
Comparison between various cereals suitable for celiacs: Chemical compositionper 100 grams of edible part
Corn Rice Buckwheat
Proteins(g) 8.7 7.3 12.4
Lipids(g) 2.7 0.5 3.3
Carbohydrates 80.8 87.0 62.5
Starch(g) 72.1 79.1 0
Fiber(g) 3.1 1.0 6.0
Vitamin A(µg) 67.0 0 0
Kcal. 362 360 314

Functional symptoms of gastro-enteric tract linked to ingestion of gluten-free commercial products
• Functional symptoms (vomiting, bloating, alterations ofbowel habits) are attributable to the presence ofpreservatives and additives in gluten-free commercialproducts.
• Patients complaining of these symptoms have benefitfrom the replacement of gluten-free commercial productswith naturally gluten-free cereals such as corn, rice,buckwheat, teef (decrease of symptoms from61% to17%)
Hopman E, Scand J Gastroenterol 2008

Alimentary Educational Course for Coeliac Disease Coeliac Disease Unit, St.Orsola-Malpighi Hospital University of Bologna
� Detailed information on GFD � Cereals and flours to be avoided and allowed� Guidelines on the correct alimentary approach � Nutritional aspects (intake of iron, calcium, vitamin D, vitamin B
group, fiber)� To read and understand food labels, cross-contamination of foods,
cuisine recipes� To eat gluten-free at restaurants and during travels � Commercially available gluten-free products
� General principles on the healthy food intake� Caloric balance – Weight monitoring – Nutritional principles� Food pyramid � Labels of food
� Physical activity and energetic balance� GFD and psycho-social aspects
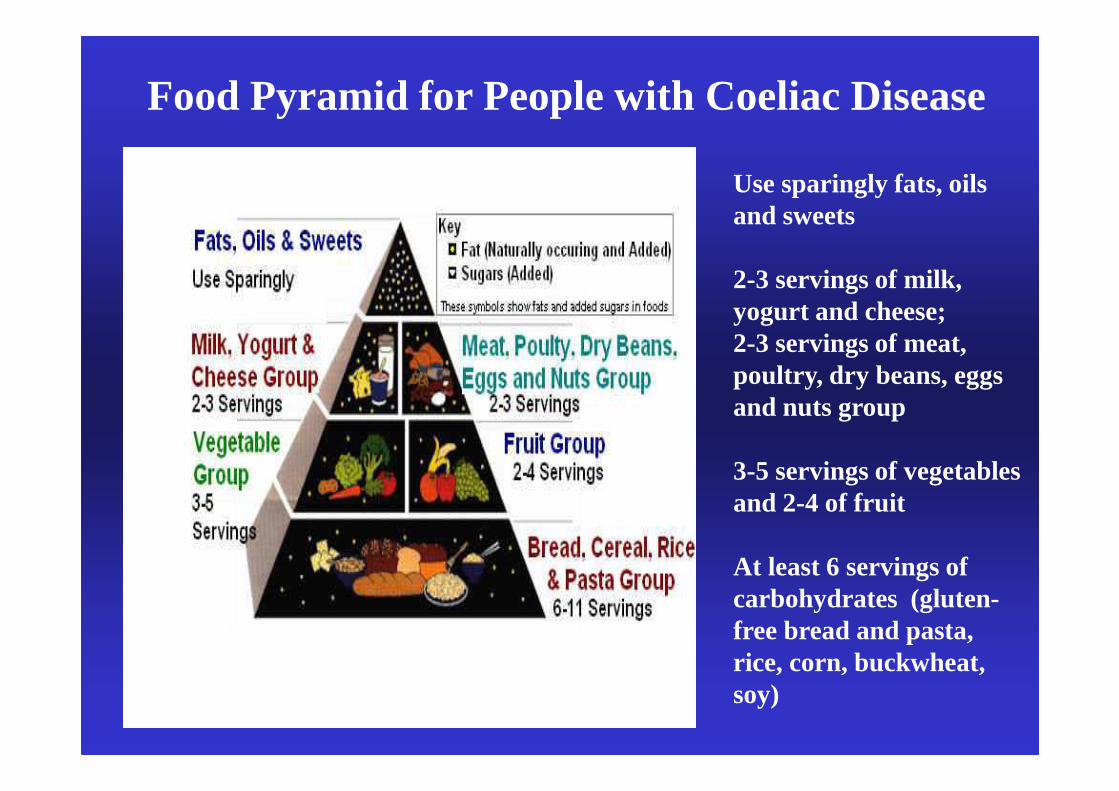
Use sparingly fats, oils and sweets
2-3 servings of milk, yogurt and cheese; 2-3 servings of meat, poultry, dry beans, eggs and nuts group
3-5 servings of vegetables and 2-4 of fruit
At least 6 servings of carbohydrates (gluten-free bread and pasta, rice, corn, buckwheat, soy)
Food Pyramid for People with Coeliac Disease

Nutritional plan for celiacs
� Diet does not take into account only the absence of gluten
� It must be highlighted the importance of caloric content, fiber intake, fat and characteristics of fat used
� Celiacs must be informed on nutritional content of gluten-free commercial foods and on the importance of checking the labels of gluten-free foods
� Celiacs must acquire the capacity to make appropriate alimentary choices.
� It must be stressed the important role of physical activity for maintaining a good state of health.
� Alimentary Educational Program is the best way for making the celiacs able of performing autonomously appropriate choices for their alimentation.

What must celiacs check on labels of gluten free commercial products?
� Caloric content
� Fat content
� Kind of fat � saturated/unsaturated
� absence of hydrogenate fat
� “fat/vegetable oils” (palm and coconut palm oils, which are vegetable oils of poor quality at high content of saturated fat)
� Vegetable margarines
� Fiber content
� Preservatives/additives

Regulations CE 41/2009 on commercial products for people with gluten intolerance
(in force from January 1st 2012)
Kind of products
Gluten <20ppm
Gluten 21-100 ppm
Gluten >100ppm
Dietetic
products
Very low
gluten content
Not allowed
for celiacs
Products for all people
Without
gluten It may contain traces of
gluten
EU Regulations on labelling of commercial products n.1169/2011, November 22, 2011
Nutritional labelling with detailed information (to be app liedwithin 5 years) : from the Big 4 (energy –Kcal-, proteins,carbohydrates, fat) to the Big 8 (energy –Kcal-, proteins,carbohydrates, sugars, fat, saturated fat, fiber, sodium)
The commitment of gluten free manufacturers
for celiacs’ information
• In order to help celiacs to make healthier choices in thefood they eat, gluten-free food manufacturers are applyingnutritional information (the “Big 8”) on the packaging oftheir food products included in list of gluten-freecommercial products
• Moreover, manufacturers are trying to increase the offerand the nutritional and palatable quality of gluten-freecommercial products, useful tools for increasing thecompliance with GFDand a lifelong good health of celiacsthrough a safe alimentation
Take home message• A number of coeliac patients on a strict GFD tend to develop
overweight and obesity due to an excessive intake of some gluten freeproducts at high lipid content.
• Metabolic abnormalities (↑ cholesterol,↑ triglycerides,↑ glucose,↑transaminases) are observed in this subgroup of coeliac patients. Acareful follow-up of these patients is mandatory.
• To prevent the development of metabolic syndrome in CD pts aneducational program with detailed information on the composition ofgluten-free commercial foods, general principles of the healthy foodintake, physical activity and energetic balance, and psycho-socialaspects (excessive fear of contamination resulting in exclusive intakeof gluten-free commercials products) is recommended.
• EU regulations on nutritional labelling of commercial products andthe increased commitment of gluten-free manufacturers will guaranteea better quality of commercial products for coeliac patients in nextyears.