TOPIC 10 CASI DIFFICILI IN REUMATOLOGIA · TOPIC 10 . CASI DIFFICILI IN REUMATOLOGIA . ... DIAGNOSI...
42
TOPIC 10 CASI DIFFICILI IN REUMATOLOGIA Caso 2 Impegno extra-articolare e comorbidità: difficile gestione di un caso di Artrite Reumatoide Discussant: Cristina Iannuccelli Presenter: Maria Paola Guzzo Sapienza - Università di Roma Reumatologia Early Arthritis Clinic
Transcript of TOPIC 10 CASI DIFFICILI IN REUMATOLOGIA · TOPIC 10 . CASI DIFFICILI IN REUMATOLOGIA . ... DIAGNOSI...
TOPIC 10 CASI DIFFICILI IN REUMATOLOGIA Caso 2 Impegno extra-articolare e comorbidità: difficile gestione di un caso di Artrite Reumatoide Discussant: Cristina Iannuccelli Presenter: Maria Paola Guzzo Sapienza - Università di Roma Reumatologia Early Arthritis Clinic
TOPIC 10 CASI DIFFICILI IN REUMATOLOGIA Caso 2 Impegno extra-articolare e comorbidità: difficile gestione di un caso di Artrite Reumatoide Cristina Iannuccelli Maria Paola Guzzo Sapienza Università di Roma Reumatologia Early Arthritis Clinic
65 ANNI
EX-METALMECCANICO
FUMATORE (60 sigarette/die )
FAMILIARITÀ CARDIOPATIA E NEOPLASIA
TBC POLMONARE
DIVERTICOLOSI DEL COLON
BPCO
Motivo: RETTORRAGIA Riferite artralgie mani e spalle VES 50 mm/h PCR 54 mg/L Waaler-Rose 13,7 UI/ml
Rx torace incremento della trama interstiziale con aspetto finemente reticolare a livello basale Dimissione: emorroidi esterne
RICOVERO MEDICINA INTERNA
CONSIGLIATA VISITA REUMATOLOGICA
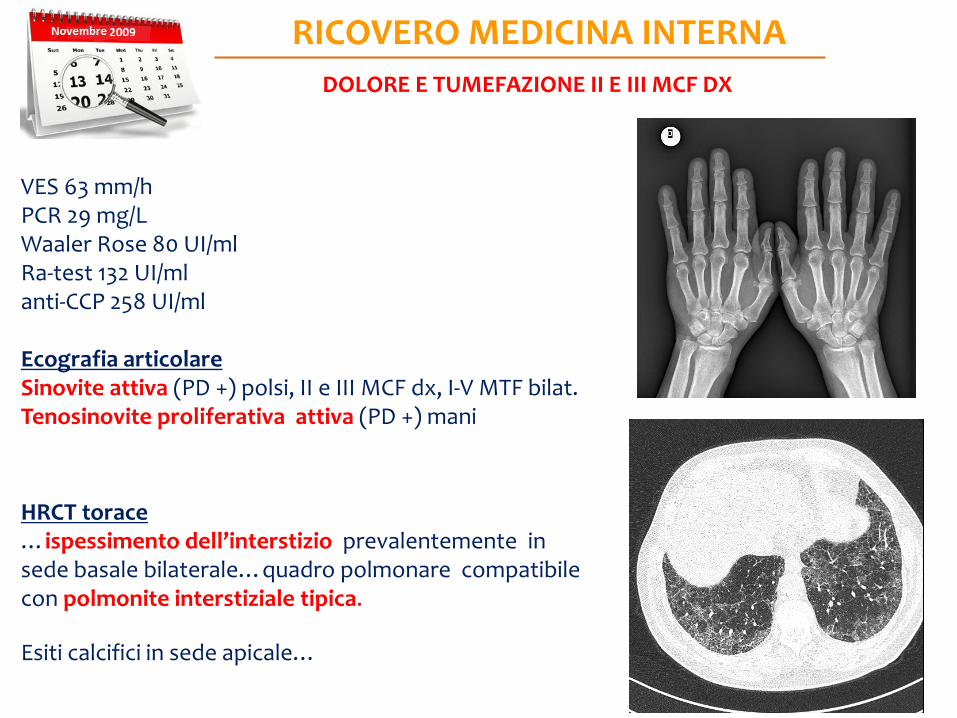
VES 63 mm/h PCR 29 mg/L Waaler Rose 80 UI/ml Ra-test 132 UI/ml anti-CCP 258 UI/ml Ecografia articolare Sinovite attiva (PD +) polsi, II e III MCF dx, I-V MTF bilat. Tenosinovite proliferativa attiva (PD +) mani HRCT torace …ispessimento dell’interstizio prevalentemente in sede basale bilaterale…quadro polmonare compatibile con polmonite interstiziale tipica. Esiti calcifici in sede apicale…
RICOVERO MEDICINA INTERNA DOLORE E TUMEFAZIONE II E III MCF DX
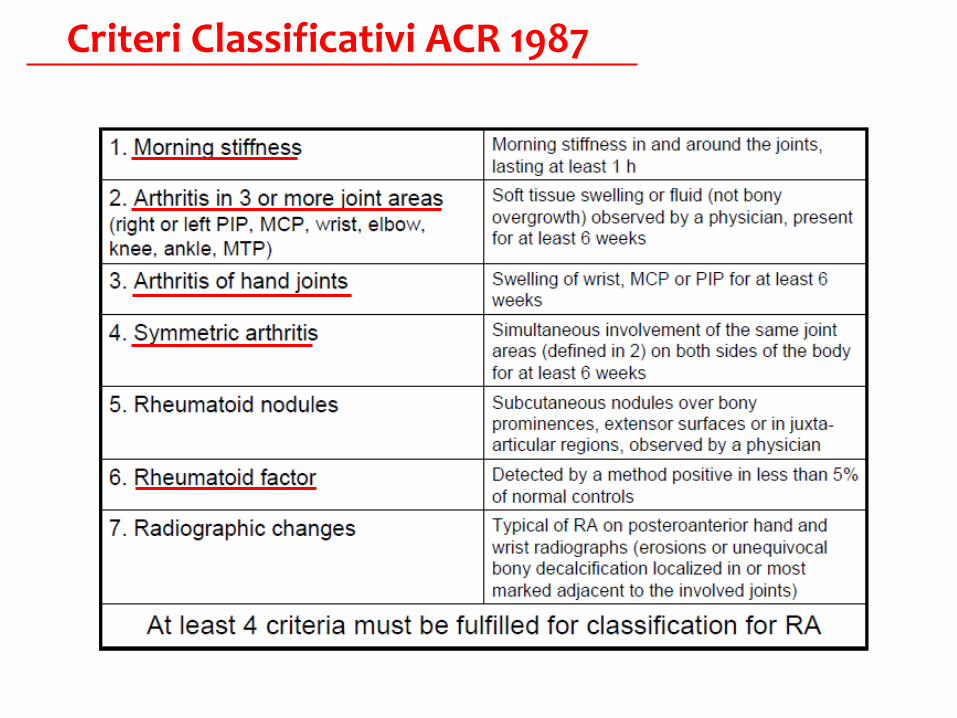
Criteri Classificativi ACR 1987
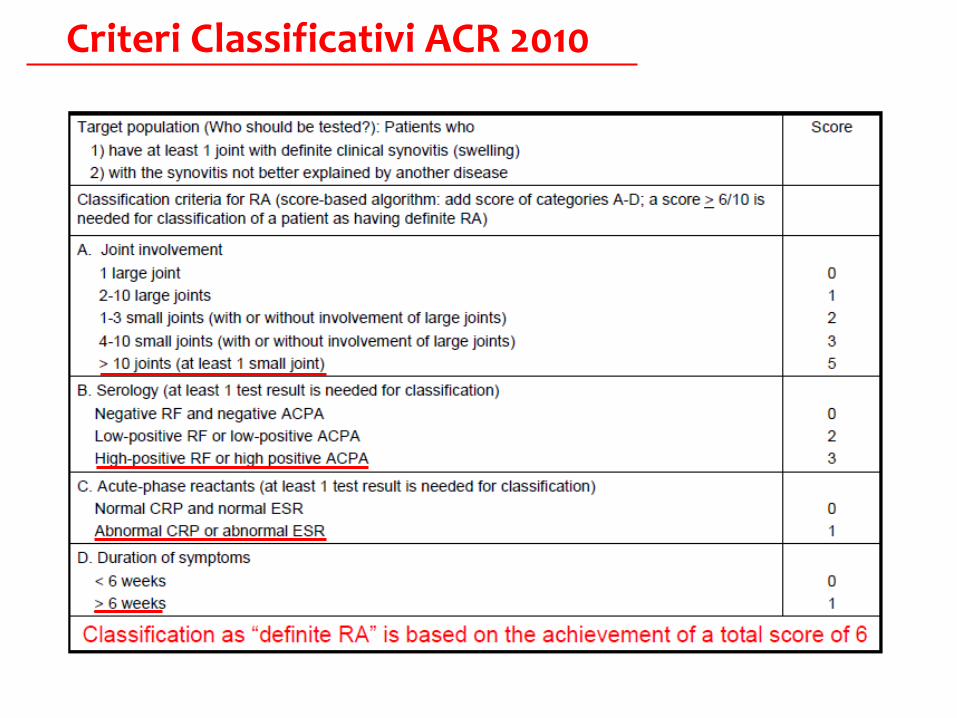
Criteri Classificativi ACR 2010
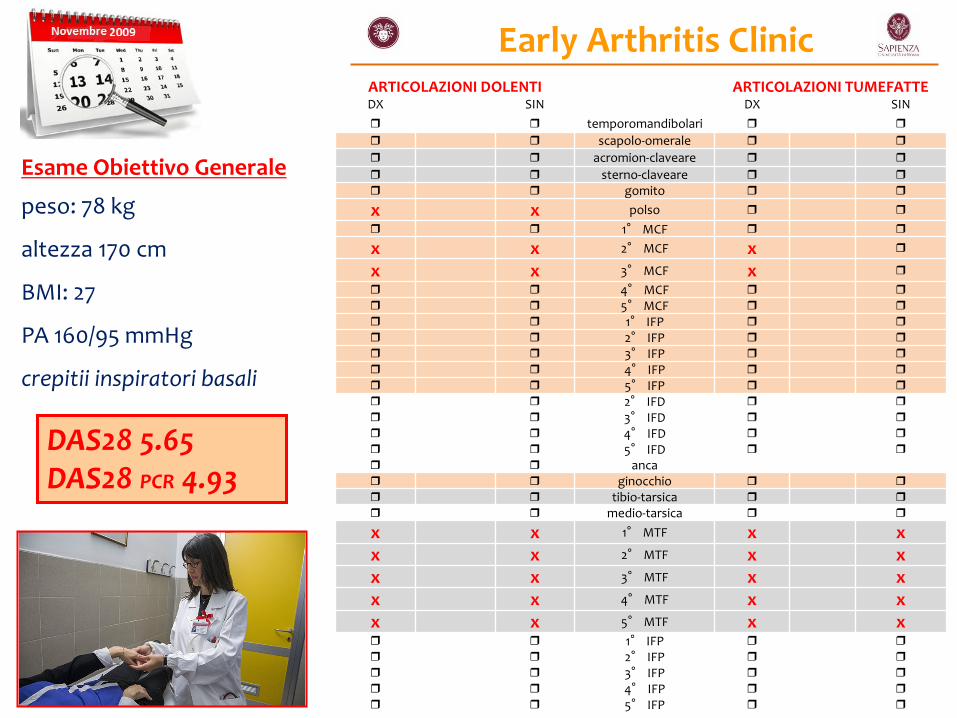
Early Arthritis Clinic ARTICOLAZIONI DOLENTI ARTICOLAZIONI TUMEFATTE DX SIN DX SIN temporomandibolari scapolo-omerale acromion-claveare sterno-claveare gomito
x x polso
1° MCF
x x 2° MCF x
x x 3° MCF x
4° MCF 5° MCF 1° IFP 2° IFP 3° IFP 4° IFP 5° IFP 2° IFD 3° IFD 4° IFD 5° IFD anca ginocchio tibio-tarsica medio-tarsica
x x 1° MTF x x x x 2° MTF x x x x 3° MTF x x x x 4° MTF x x x x 5° MTF x x 1° IFP 2° IFP 3° IFP 4° IFP 5° IFP
Esame Obiettivo Generale
peso: 78 kg
altezza 170 cm
BMI: 27
PA 160/95 mmHg
crepitii inspiratori basali
DAS28 5.65 DAS28 PCR 4.93
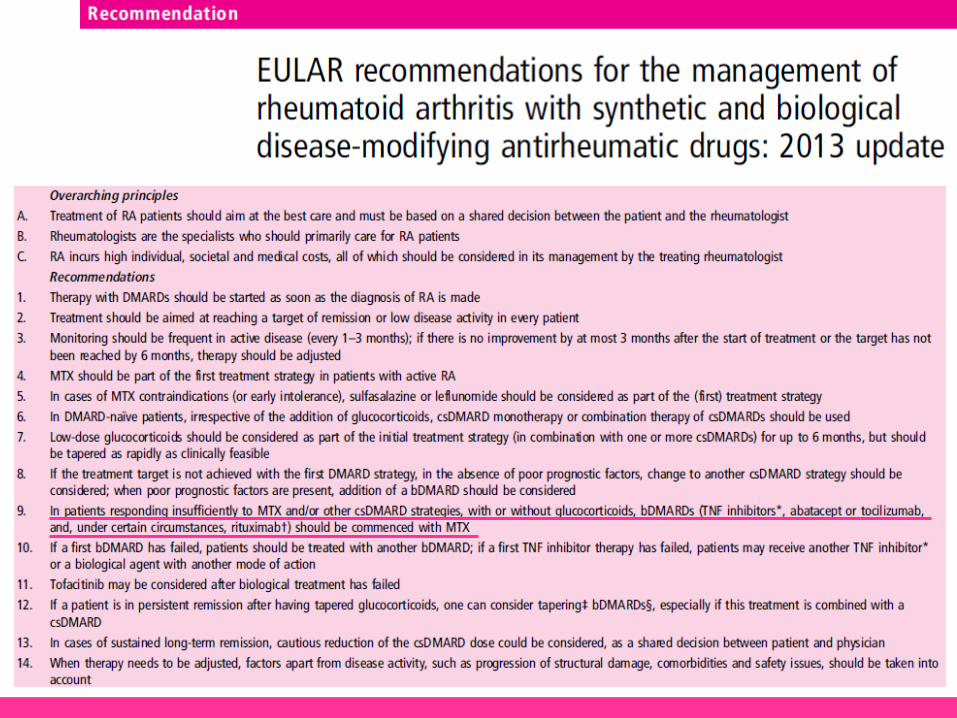
Recommendation 5 Patients at risk of developing persistent and/or erosive arthritis should be started with DMARDs as early as possible even if they do not yet fulfil established classification criteria for inflammatory rheumatological diseases. Recommendation 9 Among the DMARDs, methotrexate is considered the anchor drug and should be used first in patients at risk of developing persistent disease.
METHOTREXATE
D. Pre treatment Assessments: FBC, U&E & LFT, CXR. Pulmonary Function Tests (PFT) may be undertaken in some patients E. Safety Monitoring: to identify adverse effects such as myelosuppression, liver toxicity and pulmonary problems: FBC, LFT &U&E F. Actions to be taken: New or increasing dyspnoea or dry cough: Withhold and discuss urgently with Specialist team. G: Adverse Effects & Management 4. Pulmonary Symptoms: a small minority of patients develop symptoms of interstitial pneumonitis soon after starting treatment indicated by persistent dry coughs/shorteness of breath. Stop the MTX and refer to the specialist team or Casualty urgently.

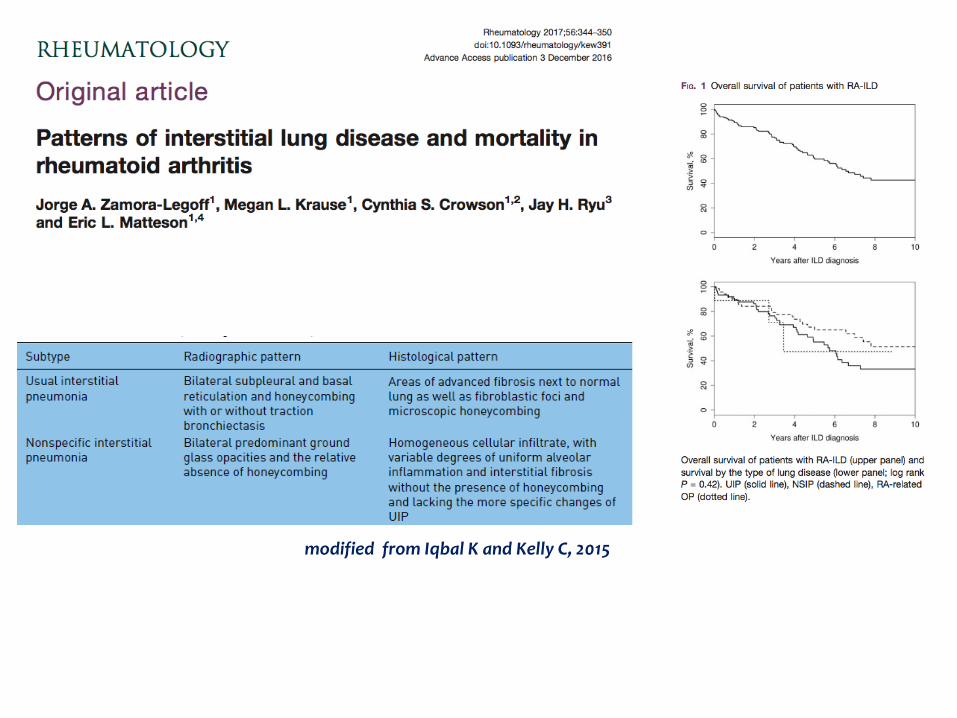
modified from Iqbal K and Kelly C, 2015
Terapia prescritta Sulfasalazina 500 mg 2 cp x 2/die Idrossiclorochina 200 mg x2/die Metilprednisolone 4mg 1 cp/die Si raccomanda:
sospensione abitudine tabagica
dieta
calo ponderale
monitoraggio PA
videat cardiologico
NOVEMBRE 2009 - Early Arthritis Clinic
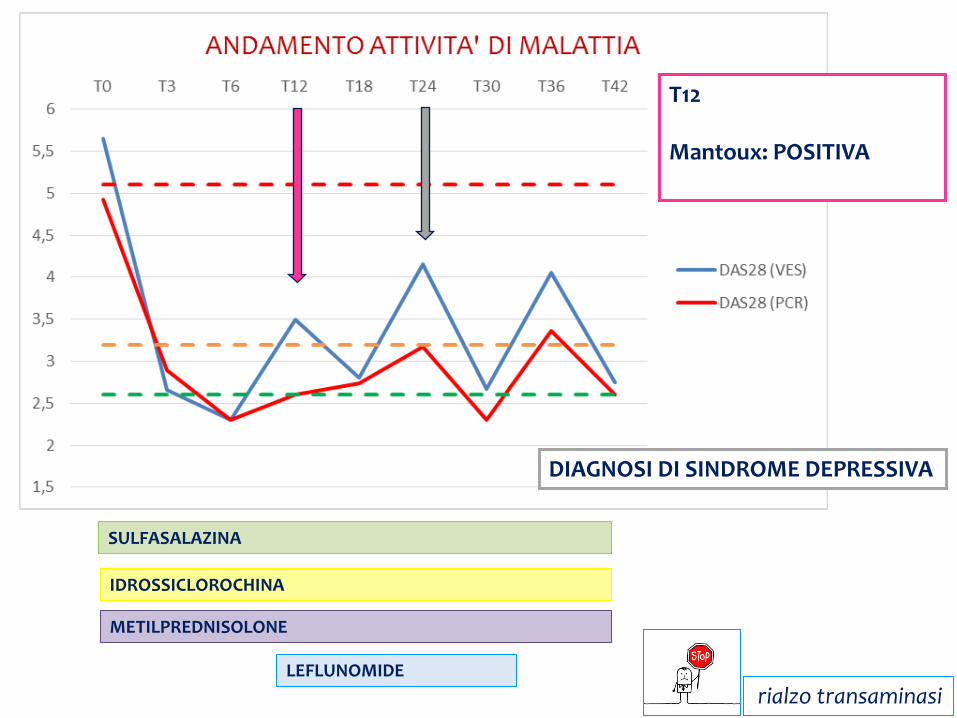
DIAGNOSI DI SINDROME DEPRESSIVA
SULFASALAZINA
METILPREDNISOLONE
LEFLUNOMIDE
IDROSSICLOROCHINA
T12 Mantoux: POSITIVA
rialzo transaminasi
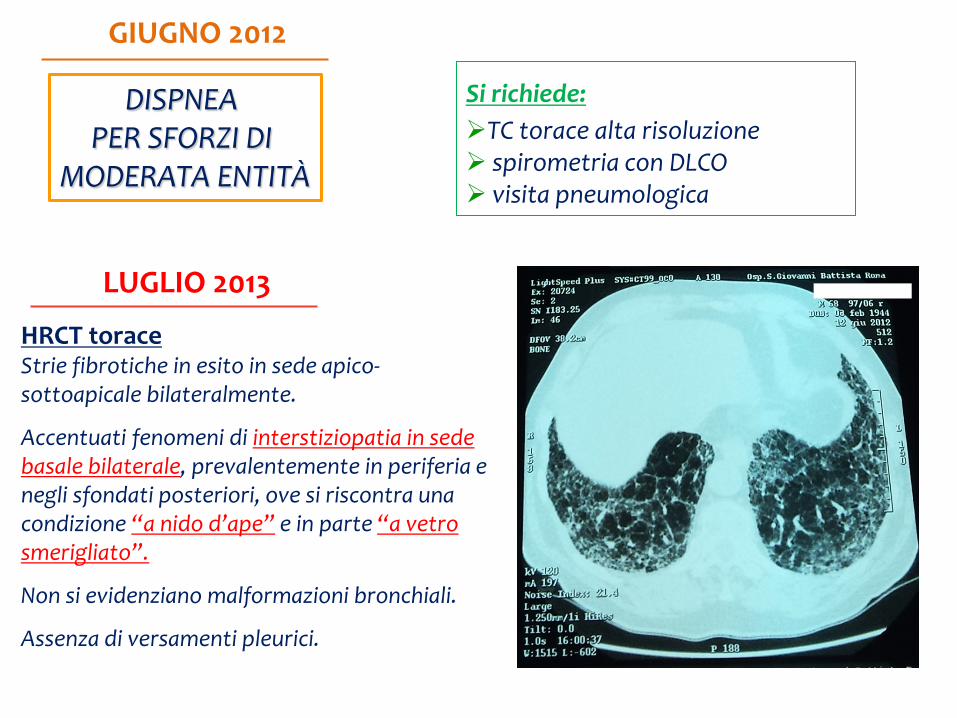
HRCT torace Strie fibrotiche in esito in sede apico-sottoapicale bilateralmente.
Accentuati fenomeni di interstiziopatia in sede basale bilaterale, prevalentemente in periferia e negli sfondati posteriori, ove si riscontra una condizione “a nido d’ape” e in parte “a vetro smerigliato”.
Non si evidenziano malformazioni bronchiali.
Assenza di versamenti pleurici.
GIUGNO 2012
DISPNEA PER SFORZI DI
MODERATA ENTITÀ
LUGLIO 2013
Si richiede: TC torace alta risoluzione spirometria con DLCO visita pneumologica
IMA STEMI in sede laterale
angioplastica primaria su ramo marginale con impianto di stent
introdotta terapia antipertensiva
introdotta terapia ipolipemizzante
interruzione dell’abitudine tabagica
SETTEMBRE 2013
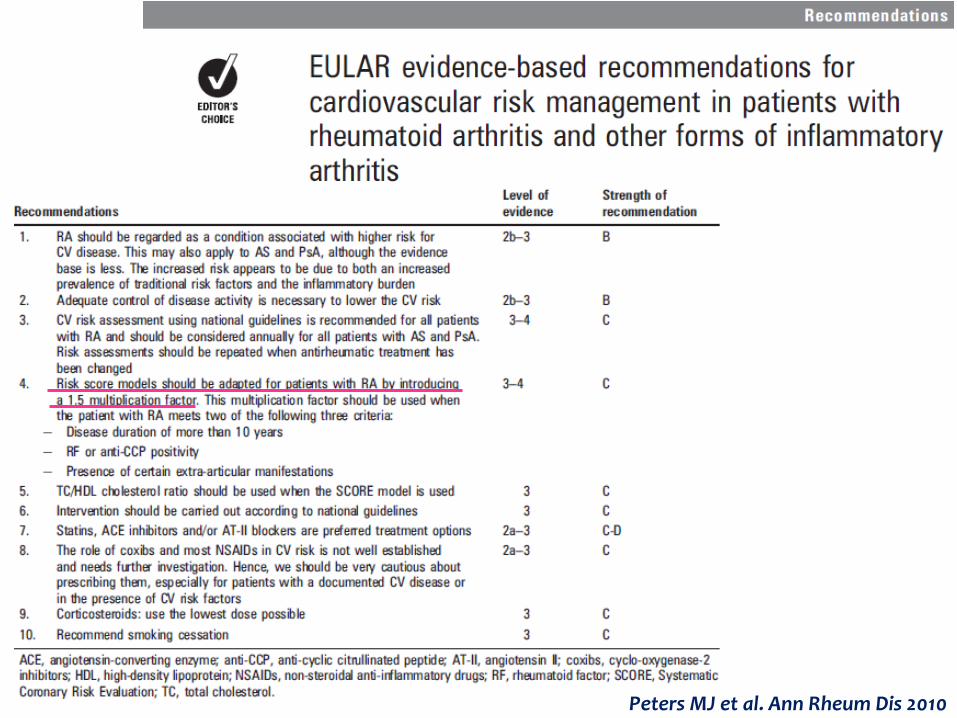
Peters MJ et al. Ann Rheum Dis 2010
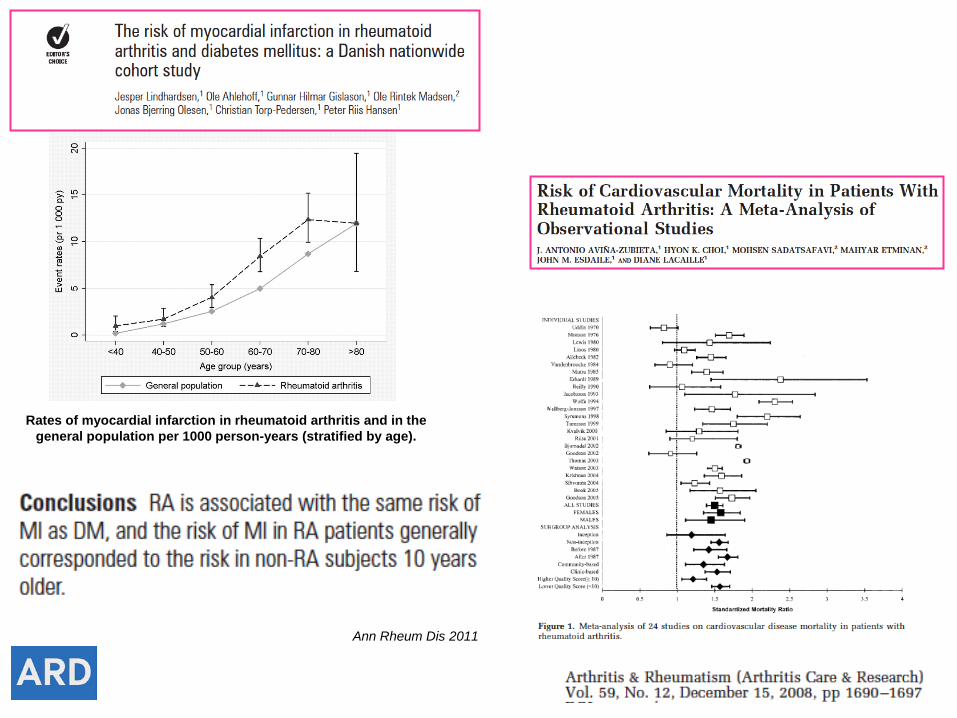
Ann Rheum Dis 2011
Rates of myocardial infarction in rheumatoid arthritis and in the general population per 1000 person-years (stratified by age).
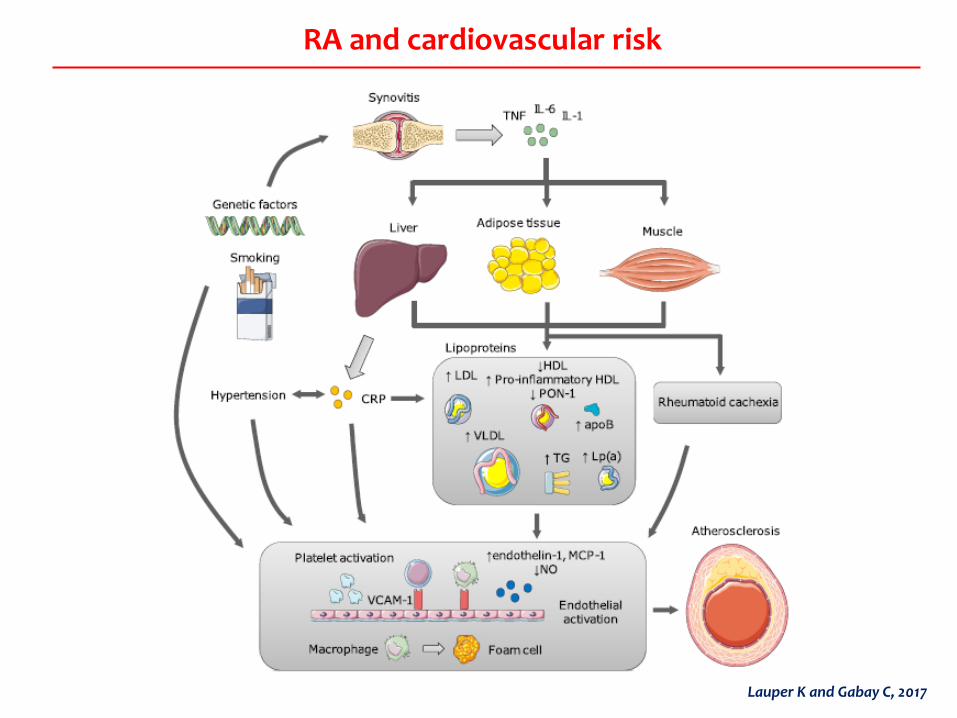
RA and cardiovascular risk
Lauper K and Gabay C, 2017
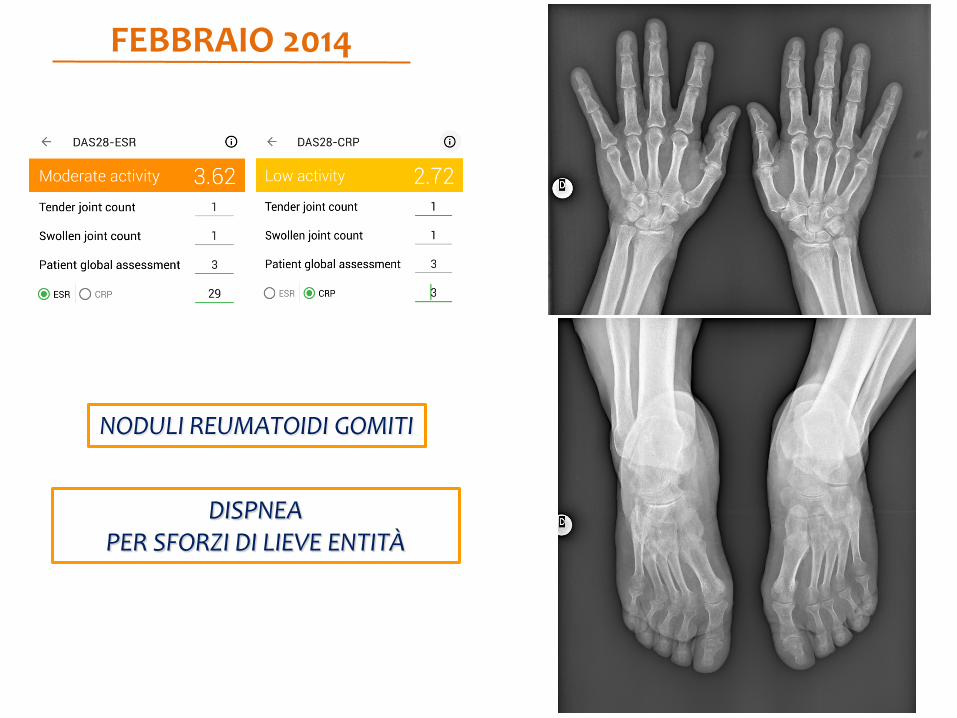
FEBBRAIO 2014
DISPNEA PER SFORZI DI LIEVE ENTITÀ
NODULI REUMATOIDI GOMITI
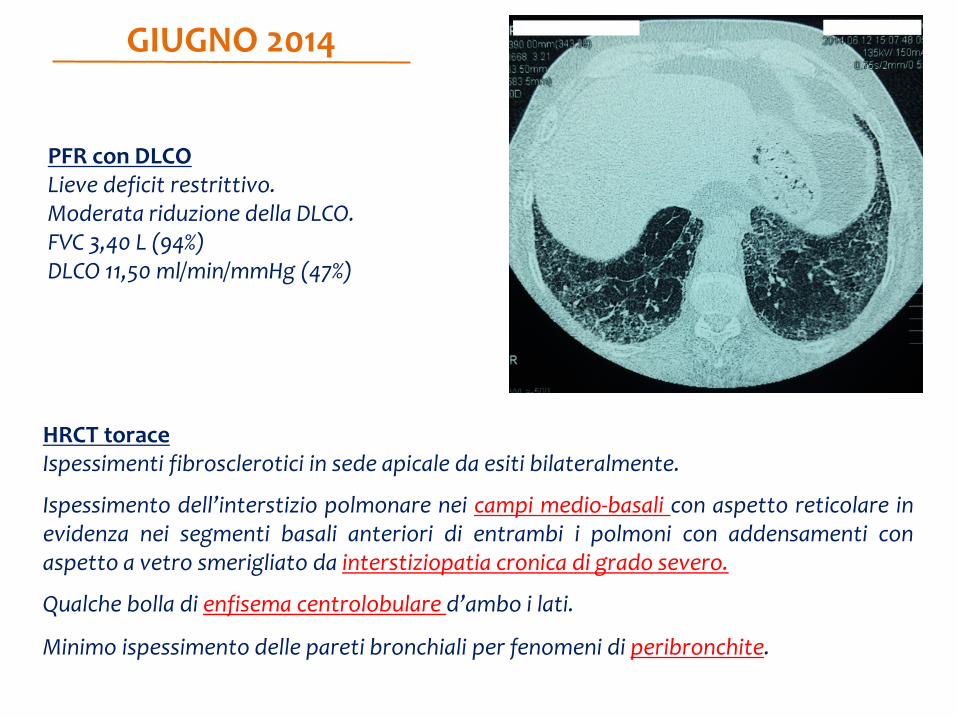
PFR con DLCO Lieve deficit restrittivo. Moderata riduzione della DLCO. FVC 3,40 L (94%) DLCO 11,50 ml/min/mmHg (47%)
HRCT torace Ispessimenti fibrosclerotici in sede apicale da esiti bilateralmente.
Ispessimento dell’interstizio polmonare nei campi medio-basali con aspetto reticolare in evidenza nei segmenti basali anteriori di entrambi i polmoni con addensamenti con aspetto a vetro smerigliato da interstiziopatia cronica di grado severo.
Qualche bolla di enfisema centrolobulare d’ambo i lati.
Minimo ispessimento delle pareti bronchiali per fenomeni di peribronchite.
GIUGNO 2014
PROBLEMI APERTI: Rivalutazione Interstiziopatia Rivalutazione funzionalità cardiaca Decisione terapeutica
RICOVERO REUMATOLOGIA VES 47 mm/h PCR 7 mg/L WR >160 UI/ml Ra-test 139 UI/ml anti-CCP >600 UI/ml Markers Epatite B e C negativi
PFR con DLCO Moderato deficit restrittivo. Marcata riduzione del transfer del CO. FVC 3,08 L (85%) DLCO 8,55 ml/min/mmHg (35%)
Ecocardiogramma Ventricolo sinistro con volume cavitario normale, ipertrofia parietale e cinesi globale normale. Lieve dilatazione delle cavità atriali. Minima insufficienza aortica. Lieve insufficienza tricuspidale. PAPs: 26 mmHg. F.E. 55%.
RICOVERO REUMATOLOGIA
Broncoscopia con BAL Lieve iperemia della mucosa bronchiale Esame citologico su BAL Abbondanti granulociti neutrofili, macrofagi, rari linfociti e cellule cilindriche dell’epitelio bronchiale esenti da alterazioni citologiche di rilievo. Assenza di particelle birifrangenti all’interno dei macrofagi. Negativa la ricerca di cellule neoplastiche. Esame colturale su BAL Negativo per germi comuni, miceti, BK
PROBLEMI APERTI: Rivalutazione Interstiziopatia Rivalutazione funzionalità cardiaca Decisione terapeutica
Clinical And Experimental Rheumatology, June 2011
Interstitial lung disease • When new-onset ILD occurs in patients treated with biologic agents,
withdrawal of the drug should be recommended and an exhaustive investigation should be performed to exclude infectious disease
• In these patients, reinitiation of biologic treatment (especially with the same agent) is not recommended
• In patients with pre-existing ILD, anti-TNF agents should be avoided
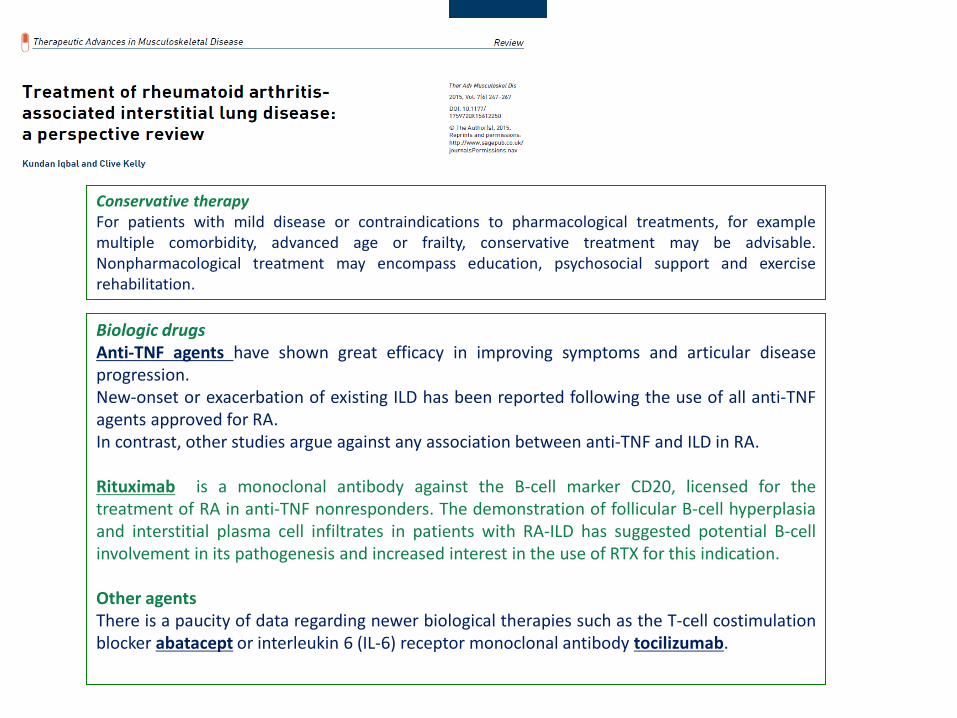
Conservative therapy For patients with mild disease or contraindications to pharmacological treatments, for example multiple comorbidity, advanced age or frailty, conservative treatment may be advisable. Nonpharmacological treatment may encompass education, psychosocial support and exercise rehabilitation.
Biologic drugs Anti-TNF agents have shown great efficacy in improving symptoms and articular disease progression. New-onset or exacerbation of existing ILD has been reported following the use of all anti-TNF agents approved for RA. In contrast, other studies argue against any association between anti-TNF and ILD in RA. Rituximab is a monoclonal antibody against the B-cell marker CD20, licensed for the treatment of RA in anti-TNF nonresponders. The demonstration of follicular B-cell hyperplasia and interstitial plasma cell infiltrates in patients with RA-ILD has suggested potential B-cell involvement in its pathogenesis and increased interest in the use of RTX for this indication. Other agents There is a paucity of data regarding newer biological therapies such as the T-cell costimulation blocker abatacept or interleukin 6 (IL-6) receptor monoclonal antibody tocilizumab.
Conservative therapy For patients with mild disease or contraindications to pharmacological treatments, for example multiple comorbidity, advanced age or frailty, conservative treatment may be advisable. Nonpharmacological treatment may encompass education, psychosocial support and exercise rehabilitation.
Biologic drugs Anti-TNF agents have shown great efficacy in improving symptoms and articular disease progression. New-onset or exacerbation of existing ILD has been reported following the use of all anti-TNF agents approved for RA. In contrast, other studies argue against any association between anti-TNF and ILD in RA. Rituximab is a monoclonal antibody against the B-cell marker CD20, licensed for the treatment of RA in anti-TNF nonresponders. The demonstration of follicular B-cell hyperplasia and interstitial plasma cell infiltrates in patients with RA-ILD has suggested potential B-cell involvement in its pathogenesis and increased interest in the use of RTX for this indication. Other agents There is a paucity of data regarding newer biological therapies such as the T-cell costimulation blocker abatacept or interleukin 6 (IL-6) receptor monoclonal antibody tocilizumab.
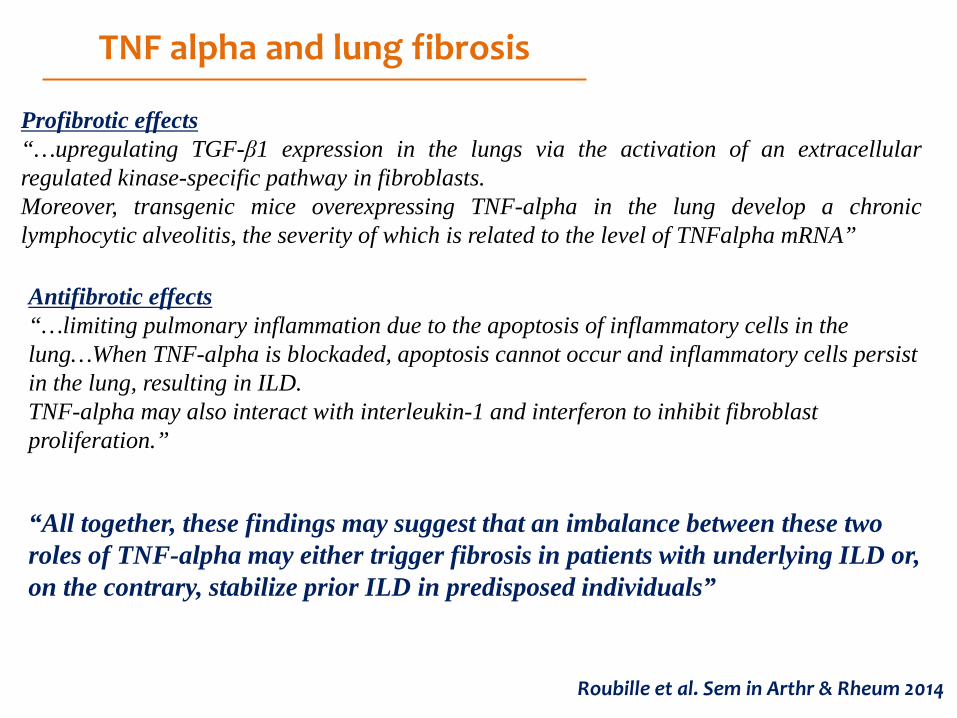
Roubille et al. Sem in Arthr & Rheum 2014
TNF alpha and lung fibrosis
Profibrotic effects “…upregulating TGF-β1 expression in the lungs via the activation of an extracellular regulated kinase-specific pathway in fibroblasts. Moreover, transgenic mice overexpressing TNF-alpha in the lung develop a chronic lymphocytic alveolitis, the severity of which is related to the level of TNFalpha mRNA” Antifibrotic effects “…limiting pulmonary inflammation due to the apoptosis of inflammatory cells in the lung…When TNF-alpha is blockaded, apoptosis cannot occur and inflammatory cells persist in the lung, resulting in ILD. TNF-alpha may also interact with interleukin-1 and interferon to inhibit fibroblast proliferation.”
“All together, these findings may suggest that an imbalance between these two roles of TNF-alpha may either trigger fibrosis in patients with underlying ILD or, on the contrary, stabilize prior ILD in predisposed individuals”
Conservative therapy For patients with mild disease or contraindications to pharmacological treatments, for example multiple comorbidity, advanced age or frailty, conservative treatment may be advisable. Nonpharmacological treatment may encompass education, psychosocial support and exercise rehabilitation.
Biologic drugs Anti-TNF agents have shown great efficacy in improving symptoms and articular disease progression. New-onset or exacerbation of existing ILD has been reported following the use of all anti-TNF agents approved for RA. In contrast, other studies argue against any association between anti-TNF and ILD in RA. Rituximab is a monoclonal antibody against the B-cell marker CD20, licensed for the treatment of RA in anti-TNF nonresponders. The demonstration of follicular B-cell hyperplasia and interstitial plasma cell infiltrates in patients with RA-ILD has suggested potential B-cell involvement in its pathogenesis and increased interest in the use of RTX for this indication. Other agents There is a paucity of data regarding newer biological therapies such as the T-cell costimulation blocker abatacept or interleukin 6 (IL-6) receptor monoclonal antibody tocilizumab.
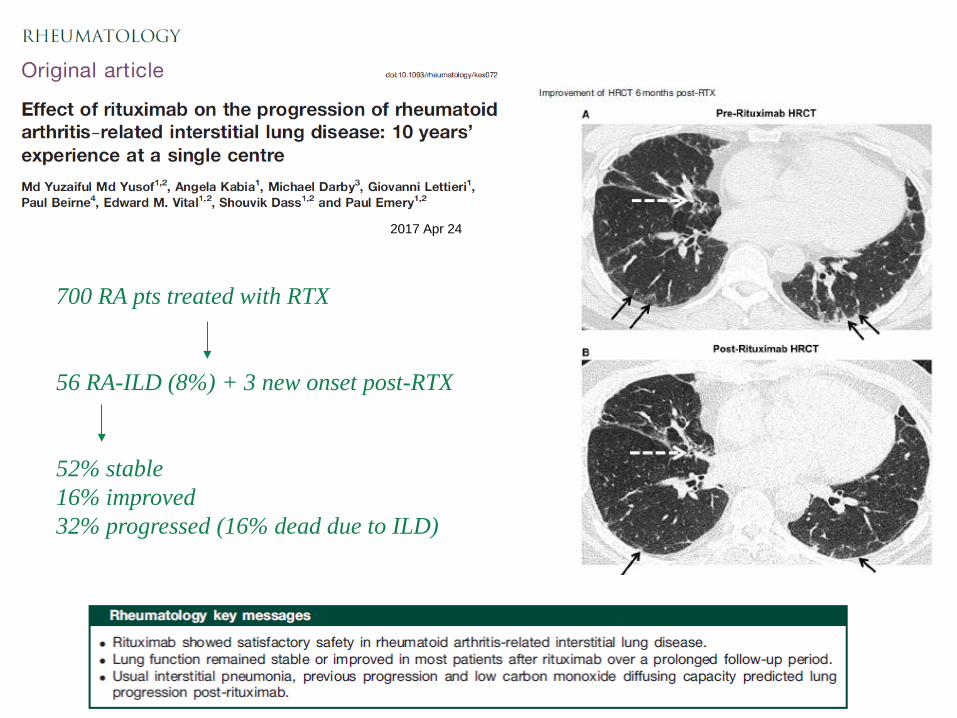
700 RA pts treated with RTX 56 RA-ILD (8%) + 3 new onset post-RTX 52% stable 16% improved 32% progressed (16% dead due to ILD)
2017 Apr 24
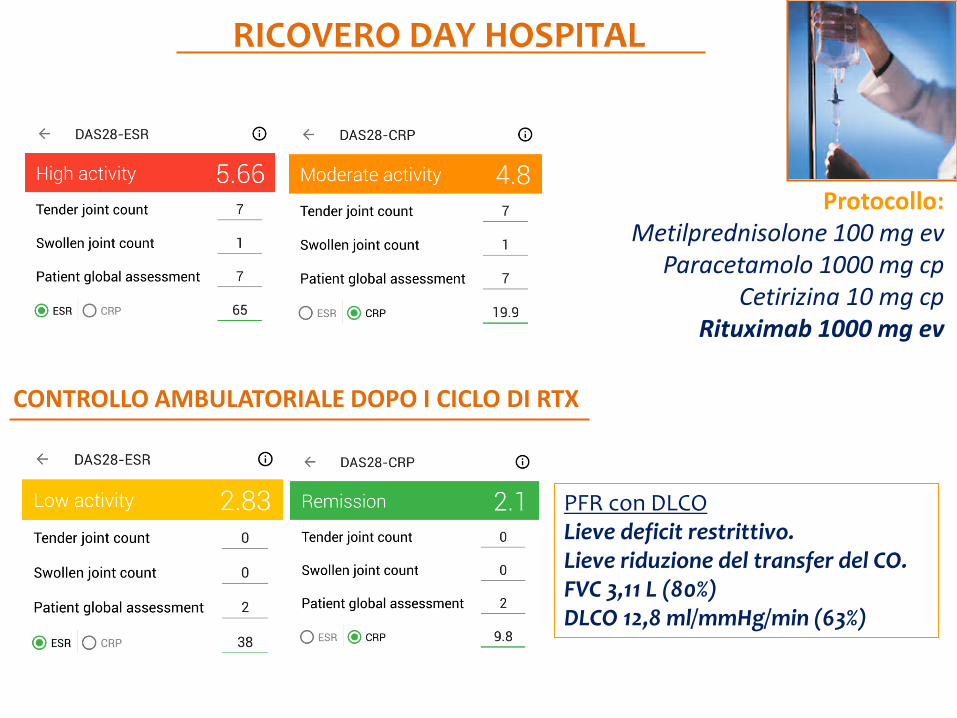
Protocollo: Metilprednisolone 100 mg ev
Paracetamolo 1000 mg cp Cetirizina 10 mg cp
Rituximab 1000 mg ev
CONTROLLO AMBULATORIALE DOPO I CICLO DI RTX
RICOVERO DAY HOSPITAL
PFR con DLCO Lieve deficit restrittivo. Lieve riduzione del transfer del CO. FVC 3,11 L (80%) DLCO 12,8 ml/mmHg/min (63%)
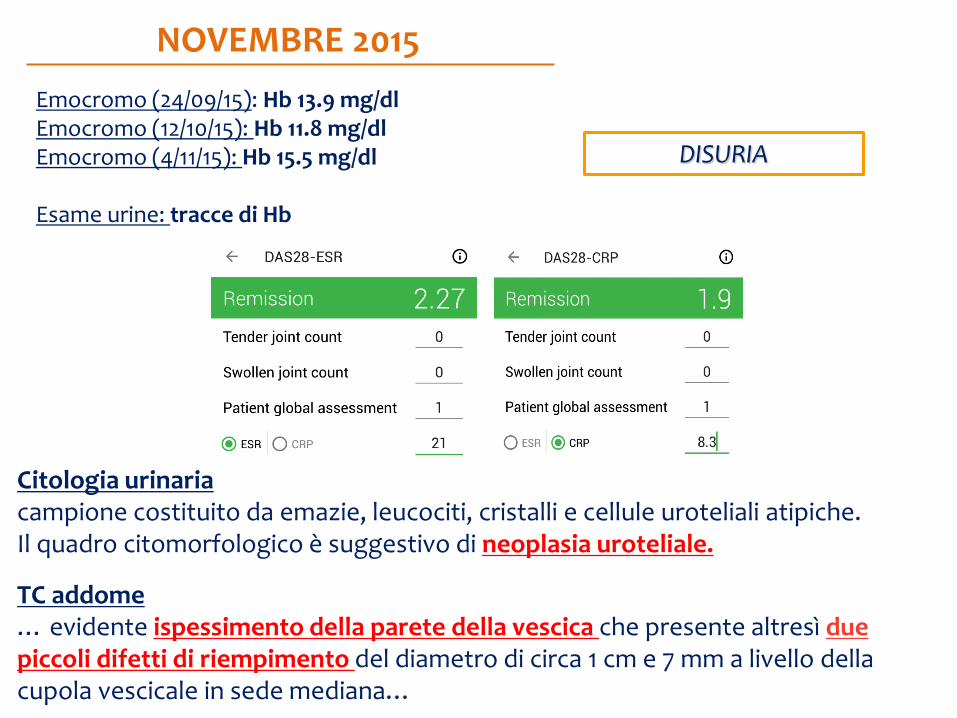
Emocromo (24/09/15): Hb 13.9 mg/dl Emocromo (12/10/15): Hb 11.8 mg/dl Emocromo (4/11/15): Hb 15.5 mg/dl Esame urine: tracce di Hb
NOVEMBRE 2015
Citologia urinaria campione costituito da emazie, leucociti, cristalli e cellule uroteliali atipiche. Il quadro citomorfologico è suggestivo di neoplasia uroteliale.
TC addome … evidente ispessimento della parete della vescica che presente altresì due piccoli difetti di riempimento del diametro di circa 1 cm e 7 mm a livello della cupola vescicale in sede mediana…
DISURIA

Esame istologico: 1)frammenti di parete vescicale sede di carcinoma uroteliale papillare di alto grado sec. WHO/ISUP 2005, infiltrante il tessuto connettivo subepiteliale. I frammenti di tonaca muscolare presenti sono esenti da infiltrazione neoplastica. (pT1) 2) frammenti di parete vescicale sede di cistite ghiandolare. In uno dei frammenti si osserva focolaio di carcinoma uroteliale infiltrante il tessuto connettivo subepiteliale.
GIUGNO-AGOSTO 2016 INSTILLAZIONI ENDOVESCICALI DI BCG (BACILLUS CALMETTE GUERIN ) Uretrocistoscopia …vescica normodistensibile, di normale capacità. Pareti vescicali iperemiche in verosimili esiti di BCG. Non evidenza di lesioni neoformate aggettanti nel lume dell’organo.
FEBBRAIO 2016
TURB
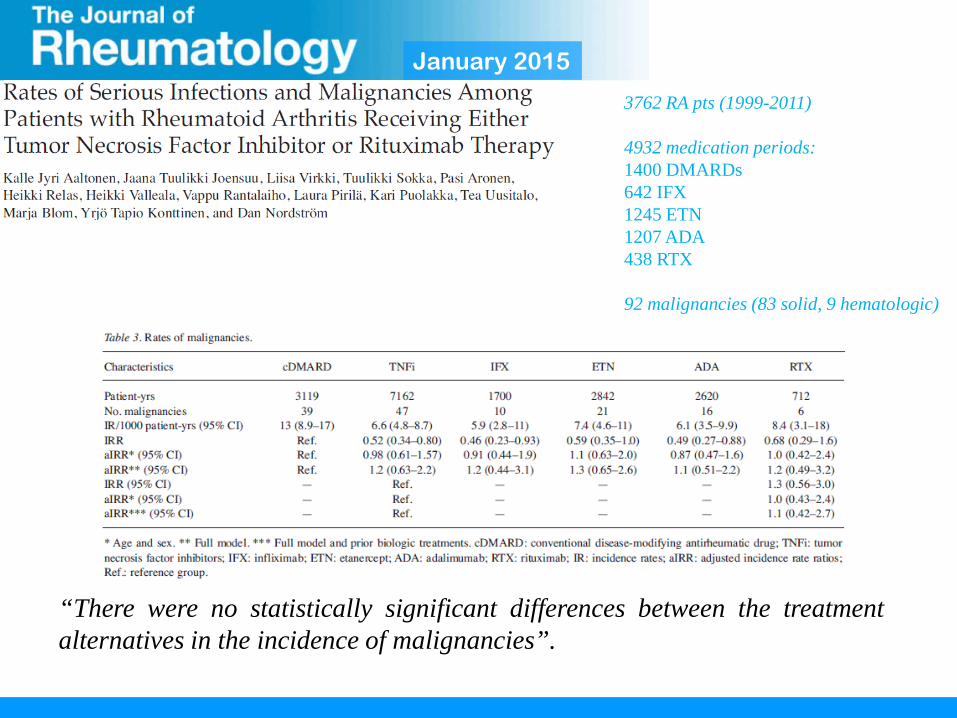
January 2015
“There were no statistically significant differences between the treatment alternatives in the incidence of malignancies”.
3762 RA pts (1999-2011) 4932 medication periods: 1400 DMARDs 642 IFX 1245 ETN 1207 ADA 438 RTX 92 malignancies (83 solid, 9 hematologic)
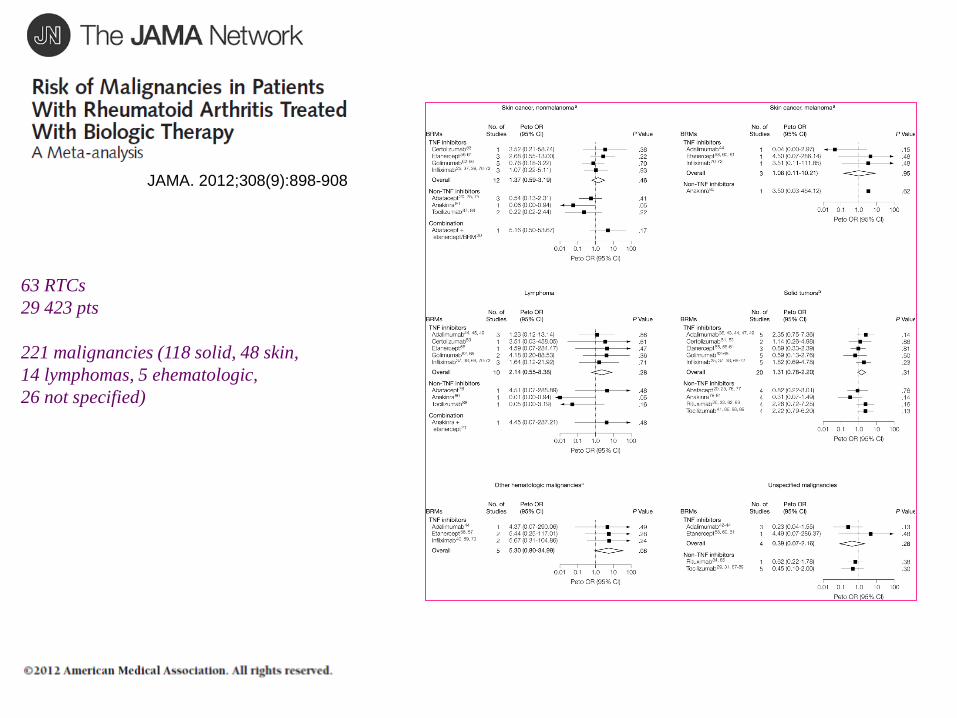
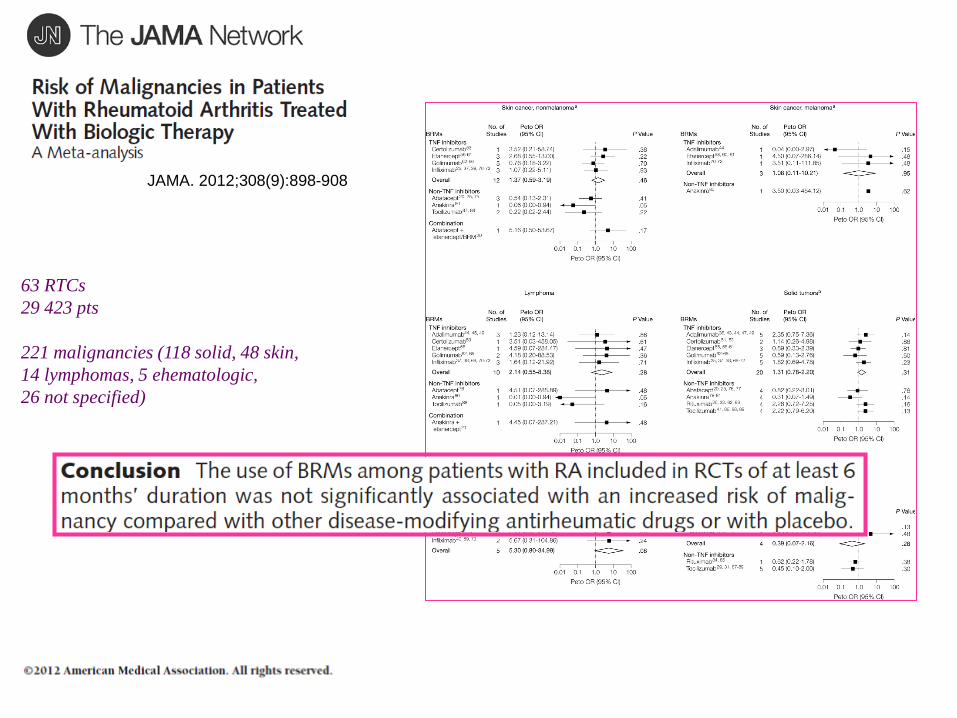
63 RTCs 29 423 pts 221 malignancies (118 solid, 48 skin, 14 lymphomas, 5 ehematologic, 26 not specified)
JAMA. 2012;308(9):898-908
63 RTCs 29 423 pts 221 malignancies (118 solid, 48 skin, 14 lymphomas, 5 ehematologic, 26 not specified)
JAMA. 2012;308(9):898-908
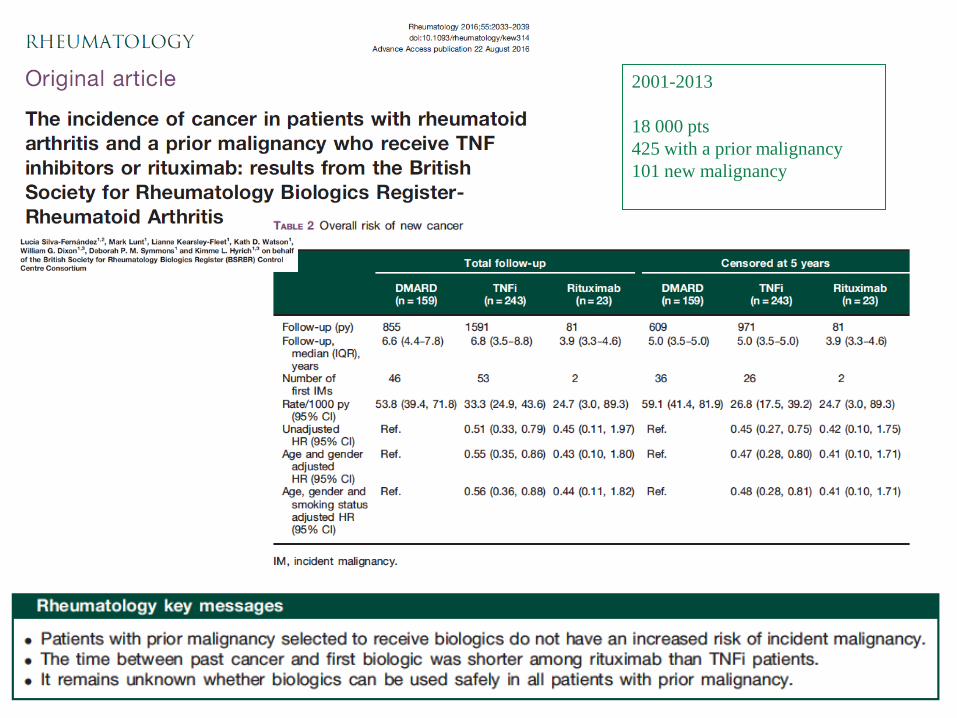
2001-2013 18 000 pts 425 with a prior malignancy 101 new malignancy
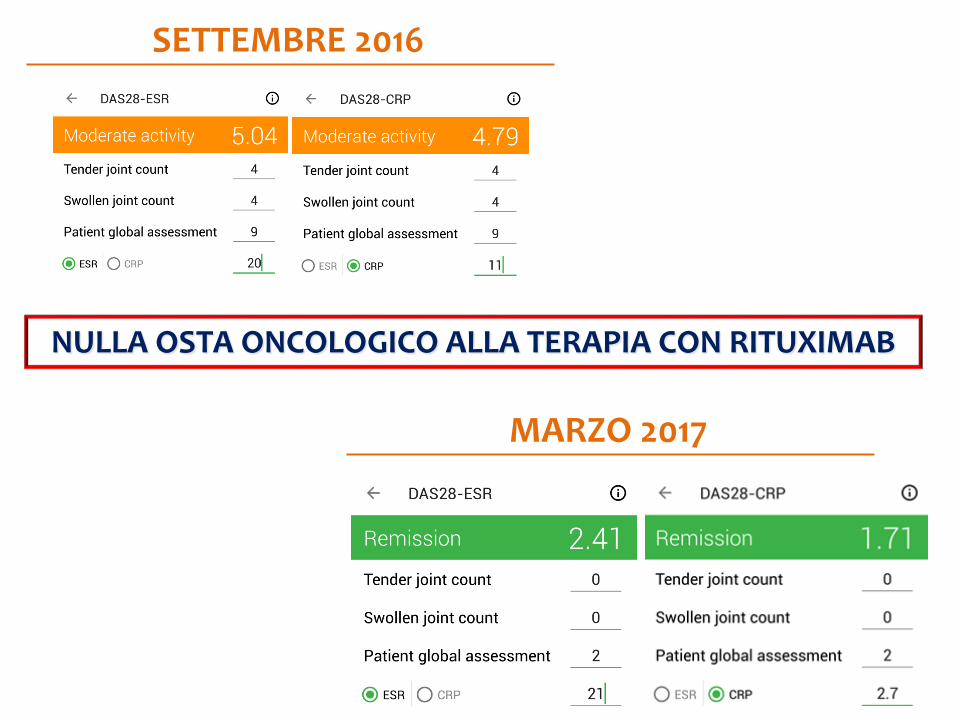
SETTEMBRE 2016
NULLA OSTA ONCOLOGICO ALLA TERAPIA CON RITUXIMAB
MARZO 2017
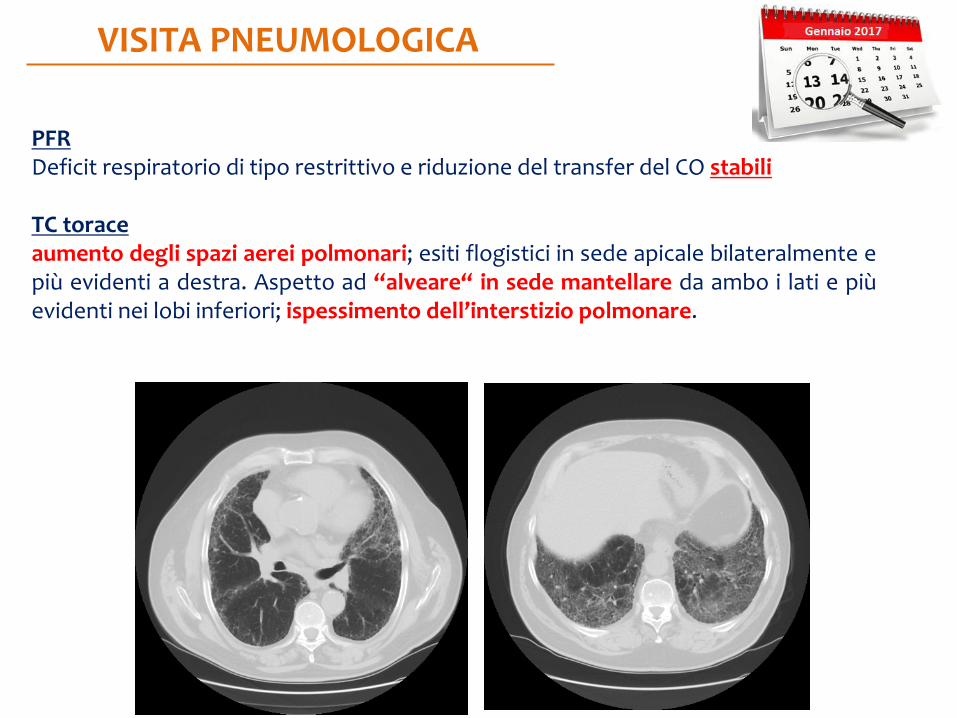
VISITA PNEUMOLOGICA
PFR Deficit respiratorio di tipo restrittivo e riduzione del transfer del CO stabili TC torace aumento degli spazi aerei polmonari; esiti flogistici in sede apicale bilateralmente e più evidenti a destra. Aspetto ad “alveare“ in sede mantellare da ambo i lati e più evidenti nei lobi inferiori; ispessimento dell’interstizio polmonare.
IMPEGNO EXTRA-ARTICOLARE COMORBIDITÀ
CONCLUSIONI SCELTE TERAPEUTICHE SCARSA COMPLIANCE E ADERENZA ALLA TERAPIA

Early Arthritis Clinic Manuela Di Franco Bruno Lucchino Chiara Gioia Francesca Romana Spinelli Guido Valesini Fabrizio Conti
Ringraziamenti