Studio del cuore con rm fetale Manganaro
50
STUDIO DEL CUORE CON RM FETALE Lucia Manganaro Dipartimento di Scienze Radiologiche Oncologiche e antamopatologiche
-
Upload
piccolo-grande-cuore-onlus -
Category
Health & Medicine
-
view
231 -
download
2
Transcript of Studio del cuore con rm fetale Manganaro

STUDIO DEL
CUORE CON RM
FETALE
Lucia Manganaro
Dipartimento di Scienze Radiologiche
Oncologiche e antamopatologiche

BACKGROUND
Congenital heart disease is one of the most frequent prenatal malformations (incidence of 5/1000 live births),it represents the primary cause of death in the first year of life
Considering the wide range of severity, a good prenatal examination acquires a great importance in order to formulate an early diagnosis and improve the pregnancy management
Nowadays investigation of CHD is performed with echocardiography considered the standard reference for diagnosis

Various studies demonstrated the potential role of fetal magnetic resonance imaging as an adjunctive imaging technique in the prenatal evaluation of CHD.
MRI may add other clinical information regarding associated extracardiac pathologies *
MRI could be advisable from the second trimester of pregnancy, when a preliminary ultrasound examination proves inadequate or diagnostically inconclusive *
MRI could offer a better imaging compared to US in an advanced gestational stage because of the progressive reduction of amniotic fluid and the ribs ossification
* Manganaro L; Savelli S; Di Maurizio M et al. Assessment of congenital heart disease (CHD): Is there a role for fetal magnetic resonance imaging
(MRI)?. European Journal of Radiology 72 (2009) 172-180.
Role of fetal MRI

KEY POINTS
Techniques
Anatomical considerations
Classification
Discussion
Conclusions

STANDARD PROTOCOL OF STUDY
Localization sequence : T2-weighted half-Fourier single-shot turbo spin-echo sequence (HASTE)(TR 1,000, TE 118/151, matrix 256×134, slice thickness 6 mm, FOV 27×20 cm) acquired in the coronal plane to evaluate fetal lie.
Anatomical study: T2 weighted HASTE sequences with a slice thickness of 3-4 mm, performed on a multiplanar orientation.
Static phase of study: ultrafast gradient-echo (GRE) sequences with SSFP, known as fast imaging with steady-state free precession (True-FISP)( TR/TE 3.5/1.5, matrix 256×144, slice thickness 3–4 mm, FOV 40×30 cm), oriented in the three planes of the space
Dynamic phase of study : real-time cine MRI True-FISP 2D sequences, known as TF2D on Magnetom Avanto (TR/TE 248.5/1.1, matrix 192×99, slice thickness 3–4 mm, FOV 38×26 cm, FA 77°, temporal resolution two slices/s), repeated dynamically (40 times)
MRI examination takes between 20 and 45 minutes depending on the movement of the fetus
1.5-T MR unit system, phased body coil (Siemens Magnetom Avanto, Erlangen,Germany).

suboptimal anatomical visualization of all the fetus body,
in particular of static fluid fast acquisition time
low ratio rumors-signal enables the avoidance of holding
mother’s breath highly sensitive to flow, heart and blood-filled vessels are
visualised as a lack of signal
T2 HASTE sequences

True-FISP (fast imaging with steady-state
free precession) sequences
Are not influenced by movement
highlight structures wirh fluid in motion showing high signal intensity
both static and motion fluid are visualised with elevated signal
The short echo time allows a good evaluation of the myocardial thickness and interventricular septum thanks to the higher contrast resolution blood-tissue on endocardium *
* Gorincour G, Bourliè Re-Najean B, Bonello B et al. Feasibility of fetal cardiac magnetic resonance imaging: preliminary
experience. Ultrasound Obstet Gynecol 2007; 29: 105–110

suboptimal visualization of the cardiac
movement
effective evidentation of the morphological
features
impossibility of fetal cardiac triggering
Real-time cine MRI True-FISP 2D
sequences

NEW PROSPECTIVES
Gradient Echo T1 w 3D
Angiography like
sequence:
Technical parameters:
TR: 25
TE: 8.4
Flip angle: 10
FOV: 17.7 cm x 29.9 cm
Matrice: 256 x 192
Slice thickness: 4.00
Distance factor: 50%
TA: 40s

TRANSVERSAL VIEWS: - Four chambers
- Five chambers
- Three vessels
SAGITTAL VIEWS: -
Short axis left ventricle
- Tricuspid-aortic cut
- Long axis of the ductus
arteriosus
- Long axis of the aortic arch
ANGULATED VIEWS: -
Long axis of the left ventricle
- Aortic arch and ductus
arteriosus
Projection

T2 HASTE sequences evaluate fetal lie (longitudinal, transverse,
oblique), presentation (cephalic, breech, shoulder), and anatomical
details
True-FISP sequences allow the highlighting of the cardial apex
orientation and the cardial situs
ANATOMICAL CONSIDERATIONS

ANATOMICAL CONSIDERATIONS

ANATOMICAL CONSIDERATIONS

Four chamber view
- heart size and orientation
- cardiac apex position
- ventricular septum angulation
- dimension of cardiac chambers
- integrity of ventricular and atrial
septum
Anatomy 1
RV
RA
LA
LV

Five chamber view
- aorta arising from the left ventricle in the center of the heart
Anatomy 2

Three vessels view:
- size and position of
pulmonary artery (PA),
aorta (Ao) and of
superior vena cava
(SVC)
Aortic arch view:
- aortic arch and SVC
Anatomy 2

Short axis of the left
ventricle:
- right ventricle shape
- left ventricle shape
- position of both ventricles
Tricuspid-Aortic view:
- right chambers position
- IVC and SVC outflow
- aortic outflow
Anatomy 4

Long axis of the ductus arteriosus :
- origin of pulmonary artery that connects to the Ao via the ductus, forming
a ductal arch
Anatomy 5

Long axis of the left ventricle:
- origin of the Aorta from left ventricle in the center of the heart
Anatomy 6

Anatomy 7
Aortic arch and ductus arteriosus view
- Simultaneous view of aortic arch and ducrus
- Same size of two vessels

CINE-MR videos

Fetal MRI study is based on the analisis of both direct and
indirect signs of pathology
DIRECT SIGNS INDIRECT SIGNS
cardial situs
cardiothoracic index
anomalies of the volume and
conformation of chambers and
myocardial
malrotation of the cardiac axis
septal defects
vessel’s pathologies
anomalies of the origin, size and
course of the great arteries
absence of anatomical structures
increased size of vessel before a
stenotic region
hypertrophy of the papillary
muscles
presence of cardiomegaly
pericardial effusion
Detection of CHD

To simplify the understanding of CHD we identify
7 categories:
1. cardial situs anomalies
2. right and left ventricular hypoplasia
3. cardiac masses
4. great vessel abnormalities
5. abnormalities of transposition and connection
6. defects of inflow and outflow
7. septal defects
Characterization of CHD

a
c
d
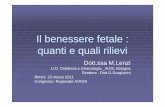
Situs inversus is easy to recognize after a first valuation of the position of the fetus compared to the mother in order to define the left and right sides. Moreover fetal MRI allows assessment of the visceroatrial situs in relation to the bronchi. The fluid-filled bronchial tree appears as high-signal-intensity structures on SSFP images *.
*Brugger PC, Stuhr F, Linder C, Prayer D. Methods of fetal MR: beyond T2-weighted imaging. Eur J Radiol2006
1.Cardial situs anomalies
b 27-week gestation fetus with complete situs inversus. Fetus position is transversal with head on the right side of
the mother as indicated by the position of the liver( white arrow) and stomach (red arrow)
Figure a) represent the posterior plan of the coronal view acquired on the mother, it shows the liver (arrow)
instead of the stomach, which is endeed shown on an anterior plane of the coronal view ( figure b).
c)Liver is located on the left side of the fetus. d) heart is located on the right side.

Right ventricular
hypoplasia:
reduction of the right
ventricular cavity with thick
walls (three vessels view)
Left ventricle
hypoplasia:
mitral and aortic atresia, both
left chambers appear reduced
with virtual cavity,the apex is
composed of the right
ventricle
2.Hypoplasia
32-week gestational age fetus with hypoplastic left heart syndrome. a) hypertrophic right
ventricle ,right ventricle occupies the aepex of the heart
a b
26-week gestational age fetus with hypoplastic lright heart syndrome. a)
hypertrophic left ventricle


Rhabdomyomas :
• most frequent prenatal tumors,
• usually associated with tuberous sclerosis
• frequently distributed in the left ventricle (move simultaneously with ventricles)
• appear hypointense in T2 weighted sequences and hyperintense in T1 weighted
sequences
• it’s required the study of the brain
3.Cardiac masses 1
33-week gestational age fetus affected by tuberous sclerosis,a) nodular hypointense lesion (arrow) located in the right
ventricle. b-c) subependymal rhabdomyoma located next to the lateral ventricle (arrows)

3. Cardiac masses
?

Teratomas:
• inhomogeneous in T2 weighted
sequences for the combination of
solid and fluid components
• differential diagnosis with thorax
pathologies (ex: CCAM , BPS)
3.Cardiac masses 2
25 week gestation fetus affected by perycardial teratoma.
Multilobulated lesion with inhomogeneous signal in T2w
sequences (arrow), located in the perycardium.

Aortic coartaction (CoA): reduction of the left ventricle; There is considerable overlap in the relative size of
the aortic arch, therefore a diagnosis of coartaction is generally a provisional diagnosis even in
echocardioghraphy. preliminary experiences demonstrated how measurement, on the three vessel view, of
the main mediastinal pulmonary artery to ascending Ao diameter ratio can be a helpful tool in distinguishing
true CoA[-]
Slodki M, Rychik J, Moszura et Al.Measurement of the great vessels in the mediastinum could help distinguish true from false-positive
coarctation of the aorta in the third trimester.J Ultrasound Med. 2009 Oct;28(10):1313-7.
.
4.Great vessels abnormalities
32 week gestation fetus affected by aortic coartaction (arrows). a-b) Gradient Echo T1 weighted 3D sequences
a b c

4.Great vessels abnormalities2
Aortic corctation 2:
28-week gestation
fetus.
a)vessel view (arrow)
b)hypoplastic left
ventricle (arrow)
c)aortic coartaction
(arrowhead)
Aortic corctation 3:
27-week gestation fetus
with DiGeorge
syndrome. Both axial
scans illustrate the
aortic coartaction (long
arrow) and the thymus
absence (short arrow) .
a b c

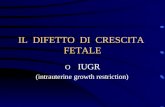
Transposition:
aorta arises form the right ventricle and the pulmonary artery from the left
ventricle, commonly associated to concordant atrio ventricular connection.
5.Abnormalities of great artery position and
connection 1
Ao Ao
RA
AP
LA
Ao
RV
RA
IVC
SVC
33-week gestational age fetus with complete transposition of the great vessels. Aorta (Ao) arising from the right
ventricle (RV), in a heart with concordant atrioventricular connections.

Double outlet right ventricle:
both great arteries arise mainly from the right ventricle. Signs of the
pathology are the disproportion of ventricles, the arteries position and
origins. Aorta and pulmonary artery show a parallel orientation
5.Abnormalities of great artery position and
connection 2
Both great arteries Ao (*) and PA (arrow) arise from right ventricle, and show parallel orentation

Fallot tetralogy:
aorta exiting the heart overriding ventricles, myocardial hyperthrophy,
interventricular septal defects caused by wrong alignment
5.Abnormalities of great artery position and
connection 3
38-week gestational age fetus with Fallot tetralogy. Aorta exiting the heart overriding
ventricles (arrows)

Common arterial trunk:
only one artery arising from the heart, which gives rise to aorta and
pulmonary artery; right position of the aorta, the possible interruption or
agenesis of the aorta, the absence or stenosis of the arterial duct
5.Abnormalities of great artery position and
connection 4
33-week gesttional fetus with common arterial trunk, unique artery (arrows) which gives rises to aorta and pulmonary artery
(arrow-head)

5.Abnormalities of great artery
position and connection 5
Azygos
continuation

Outflow defects:
obstructive left outflow:
disproportion of the left and right
chambers with the possibility of a
wider right ventricle
obstructive right outflow:
enlargement of the right ventricle,
associated to a right atrial
enlargement and myocardial
thickness.
Inflow defects:
mitral stenosis or valves
deficiency
6. Outflow and Inflow defects
30° week gestation fetus affected by obstructive right outflow (tricuspidal
atresia). Severe reduction of the right ventricle with virtual lumen (arrow) and
right atrium dilatation (*). B) absente visualization of pulmonary outflow

DIV
PULMONARY ATRESIA
DIV 27 Week
AP?
SVC
AO
AO
SVC
AO

PULMONARY ATRESIA
32° WEEK

Septal atrial defects:
secundum atrial septal defect,
difficult to diagnose because of
the physiological persistence of
the foramen ovale. In wide defects
indirect signs such as an
enlargement of the right atrium
can be associated.
Septal ventricular defects:
well studied in the four chamber
views, often associated with other
pathologies such as a Fallot
syndrome.
7.Septal defects 1
32-week gestational age fetus with septal ventricle defect. Lack of
continuity in the lower septal part (arrow)
27-weekgestational fetu swith wide septal artial defect, absence of the atrial
sepum (arrow) in a four chamber view.

Common atrioventricular
septal defect:
associated with a deficiency in
the central septal , a unique
central valve and a defect of the
ventricular septum which
appear to unevenly divide the
heart (unbalanced ventricles)
More difficult is the diagnosis
of partial atrioventricular septal
defect characterized by only the
atrial defect.
7.Septal defects 2
a) Wide septal atrial and ventricular defect . b) malrotation of the
cardiac axis

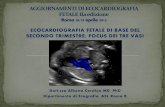
29-weeks fetus - VENTRICULAR SEPTAL DEFECT
(VSD) with possible association of coartaction of the aorta excluded by angio-MR sequences
T1 3D SPOILED
GE angio-MR
sequences to
assess the aorta
(MIP)

Lungs
Thymus
Other malformations (BRAIN)


Studies with heterogenus and small population
Absence of standardized measurement and protocols
Technical and Anatomical Limitations :
Severe heart malrotation
Small heart size
Low evaluation of motion fluid
Absence of real time resolution due to:
- Fast fetal heart rate
- Low time resolution
- Impossibility of cardiac triggering
LIMITS OF CARDIOVASCULAR MRI
Inability to study : - valvular disease (indirect signs)
- rhythm disorders


FETAL MRI ALLOWS:
Anatomical characterization of the fetal heart:
TrueFISP sequences
Suboptimal dynamic evaluation of cardiac function:
Real-time Cine-RM sequences
According to the preliminary experiences, other studies with
significantly large population may offer a standardization of the MRI
examination.
CONCLUSIONS 1

Nowadays few studies indicate that indications to fetal MRI
include inconclusive US examination* or coexistence of
extracardial associated pathologies
However in literature it is demonstrated that MRI may be used
as an adjunctive imaging technique associated to
echocardiography in order to confirm and better define the
diagnosis
CONCLUSIONS 2
* Saleem SN. Feasibility of MRI of the Fetal Heart with Balanced Steady-State Free Precession Sequence Along Fetal Body and
Cardiac Planes. AJR 2008; 191: 1208-1215

FETAL MRI
The development of new dynamic sequences may contribute to
expand the role of fetal MRI; moreover the development of
angiography-sequences may be helpful to visualize fetal
vascular in 2D or 3D * making it an indispensable tool in the
study of the fetal heart, in order to obtain a precise prenatal
diagnosis and a better delivery management.
*Baker E.. What’s new in magnetic resonance imaging? CardiolYoung 2001.11: 445–452
CONCLUSIONS 3

- Dott.ssa V. Vinci
- Dott.ssa A. Tomei
- Dott.ssa F. Fierro
- Dott. P. Sollazzo
- Dott.ssa D. Irimia
- Dott. ssa E. Sergi
--Dott.ssa S. Bernardo
Lucia Manganaro
Department of Radiological Sciences
Policlinico Umberto I Hospital, “Sapienza” University of Rome