PREVALENZA E DETERMINANTI DI ANEMIA DA DISORDINE … · ANEMIA DA DISORDINE CRONICO IN PAZIENTI...
15
PREVALENZA E DETERMINANTI DI ANEMIA DA DISORDINE CRONICO IN PAZIENTI ANZIANI OSPEDALIZZATI AFFETTI DA BPCO Piera Ranieri UO Medicina, Istituto Clinico S.Anna, Brescia, Gruppo di Ricerca Geriatrica, Brescia SEMINARI DEL VENERDI’ DEL GRUPPO DI RICERCA GERIATRICA Attualità nell’organizzazione dei servizi di geriatria Brescia, 23 gennaio 2009
Transcript of PREVALENZA E DETERMINANTI DI ANEMIA DA DISORDINE … · ANEMIA DA DISORDINE CRONICO IN PAZIENTI...

PREVALENZA E DETERMINANTI DI
ANEMIA DA DISORDINE CRONICO IN
PAZIENTI ANZIANI OSPEDALIZZATI
AFFETTI DA BPCO
Piera Ranieri
UO Medicina, Istituto Clinico S.Anna, Brescia,
Gruppo di Ricerca Geriatrica, Brescia
SEMINARI DEL VENERDI’ DEL GRUPPO DI RICERCA GERIATRICA
Attualità nell’organizzazione dei servizi di geriatria
Brescia, 23 gennaio 2009

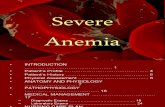
Selezione della popolazione di studio
Pazienti anziani ospedalizzati
(>65 anni)
n=811
Pazienti con diagnosi di BPCO
n=457 (56%)
Pazienti affetti da BPCO elegibili
per lo studio
n=386
Pazienti senza diagnosi di
BPCO
n=354
Pazienti affetti da malattie
severe o terminali
n=71
Pazienti affetti da
scompenso cardiaco
n=183
Popolazione di studio: pazienti
anziani affetti da BPCO
n=158
Pazienti con anemia micro e
macrocitica
n=45
ESCUSIONE
ESCUSIONE
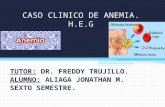
Prevalenza di anemia:
53,5%
45,5% 48,0%
51,9%
61,1 %

52,9 50,2 51,9
0
20
40
60
80
Total population NO COPD patients COPD patients
Pre
va
len
ce o
f A
ne
mia
(%
)
12,2
12,212,1
Figure 2. Prevalence of anemia in study population and mean Hb value (mg/dl) for each study group
Anemia e BPCO
La prevalenza di anemia nella popolazione generale aumenta
con l’età. La cosiddetta condizione “ anemia da disordine
cronico”, è una ben nota comorbilità di numerose patologie
croniche
E’ stato ampiamento dimostrato che in tali patologie, quali
l’insuffiienza renale cronica, lo scompenso cardiaco,
l’infezione da HIV, l’infezione epatitica cronica HCV correlata
e le neoplasie, la presenza di anemia si associa a ridotta
qualità della vita, aumentata morbilità ed aumentata mortalità
La prevalenza di anemia aumenta ulteriormente nei pazienti
anziani ospedalizzati , associandosi ad elevata mortalità,
disabilità, declino delle performance funzionali e bassa qualità
della vita.

Anemia e BPCO Tra le malattie croniche, la BroncoPneumopatia Cronica
Ostrutiva (BPCO) è un’altra condizione clinica che
sembra sia associata significativamente alla presenza di
anemia, soprattutto se considerata nell’ambito dei già noti
effetti sistemici di questa patologia, che attualmente viene
considerata una malattia infiammatoria multisistemica.
La policitemia, tradizionalmente associata alla BPCO, si
verifica sempe meno frequentemente in relazione alla più
ampia diffusione dell’ossigeno-terapia ed alla più
rigorosa correzione dell’ipossiemia
Recenti studi suggeriscono che l’anemia è altamente
prevalente nei pazienti affetti da BPCO ed è associata ad
outcome negativi

Erythropoietic response to hypoxaemia in diffuse
idiopathic pulmonary fibrosis, as opposed to chronic
obstructive pulmonary disease.Tassipoulos S, Kontos A, Konstantopoulos K et al.
Resp Med 2001; 95(6):471-475
The aim of this study was to assess the erythropoietic response to hypoxaemia in patients with
diffuse idiopathic pulmonary fibrosis (DIPF), and to speculate on the underlying mechanisms.
Patients on an established chronic respiratory failure due to DIPF or chronic obstructive
pulmonary disease (COPD) were studied. The erythropoietic response to hypoxaemia in both
conditions was assessed. We studied 18 patients with DIPF and 29 patients with COPD in
respiratory failure in a stable stage, free from acute infection and congestive heart failure.
Blood gases, erythrocytic parameters, as well the serum levels of iron, ferritin and
erythropoietin were determined. All the DIPF patients studied, apart from two, had normal or
subnormal haematocrit values. The patients with COPD had an inconsistant response to
hypoxaemia; 12 had normal or subnormal haematocrit values and the remaining 17 were
erythraemic. The mean value of erythropoietin (EPO) in both DIPF and COPD patients was
significantly higher than normal. In conclusion, patients with DIPF exhibit a lack of
erythropoietic response to hypoxaemia, despite the augmented erythropoietin levels. This may
reflect a defective bone marrow erythropoietic response in DIPF patients. It is suggested that
the pathophysiology of DIPF underlies this mechanism.

BACKGROUND: Anemia in patients with COPD and its pathophysiology is an
understudied issue.
METHODS: In a group of 101 COPD patients (FEV(1) percentage of predicted, 37 +/-
2% [mean +/- SEM]; mean age, 61 +/- 1 years; 35% female gender), the prevalence of
anemia and its relationship to body mass and weight loss, inflammatory parameters, and
erythropoietin levels was determined. Data were compared to a control group (healthy
persons with matched age) in order to identify potential factors that may influence the
development of anemia in patients with COPD.
RESULTS: Anemia was diagnosed in 13 patients (hemoglobin levels < 13.5 mg/dL in
male patients and < 12.0 mg/dL in female patients), which represents a prevalence of
13%. Anemic COPD patients showed elevated erythropoietin levels (41.8 +/- 25.4 U/L
vs 16.3 +/- 2.9 U/L) and an increased inflammatory response compared to nonanemic
patients. A significant inverse correlation of hemoglobin vs erythropoietin (r = - 0.84, p <
0.01) was observed in anemic COPD patients, but not in the nonanemic group.
CONCLUSION: Anemic COPD patients show high erythropoietin levels, which may
indicate presence of erythropoietin resistance. The latter may be mediated through
inflammatory mechanisms, which is typical for anemia of chronic illness.
Anemia and inflammation in COPDJohn M, Hoering S, Doehner W, at al.
Chest 2005;127:825-29

Anaemia of chronic disease (ACD), with chronically low levels of circulating haemoglobin, is
an immune driven abnormality that occurs in many inflammatory diseases, and also in
chronic heart failure. Although chronic obstructive pulmonary disease (COPD) is
"traditionally" associated with polycythaemia, the systemic inflammation that is now
recognised as a feature of COPD makes it a possible cause of ACD. If present in COPD,
anaemia could worsen dyspnoea and limit exercise tolerance. Preliminary evidence
suggests that anaemia in COPD patients may be more prevalent than expected, concerning
10-15% of patients suffering from severe forms of the disease. A database study conducted
in 2,524 COPD patients being prescribed long-term oxygen therapy has shown that a low
haematocrit is a strong predictor of survival in this population, before body mass index, and
is associated with more hospitalisations and a longer cumulative duration of hospitalisation.
COPD patients with low haemoglobin levels have a poorer prognosis than COPD patients
with normal haemoglobin levels in the event of acute gastrointestinal bleeding or after
elective aneurysm repair. Raising haemoglobinaemia through transfusion decreases minute
ventilation and work of breathing in COPD patients. These preliminary evidences point to the
need to study the prevalence of anaemia, and its physiological and clinical impact in chronic
obstructive pulmonary disease. When this body of knowledge is available, the question of
the putative benefits of raising haemoglobinaemia in chronic obstructive pulmonary disease
will have to be addressed.
The potential impact of anemia of chronic
disease in COPDSimilowski T, Agusti A, and Schonhofer B.
Eur Respir J. .2006;27:390-396

Haemoglobin level and its clinical impact in a cohort
of patients with COPDCote C, Zilberberg MD, Dordelly SH, and Celli B.
Eur Respir J. 2007;29:923-929.
Haemoglobin (Hb) abnormalities in chronic obstructive pulmonary disease (COPD) are
not well characterised. The present authors investigated the prevalence and association
of abnormal Hb with clinical outcomes. Analysis of a prospective cohort of stable COPD
outpatients (n = 683) in a USA Veterans Administration pulmonary clinic was
undertaken. Patients were classified as anaemic (Hb <13 g.dL(-1)), polycythemic (Hb >
or =17 g.dL(-1) and > or =15 g.dL(-1) for males and females, respectively) or normal.
Demographic characteristics and physiological/functional outcomes were compared
between groups. Regression models adjusting for confounders examined the
independent association of anaemia with clinical outcomes. Anaemia was present in 116
(17%) patients and polycythemia in 40 (6%). While the only values that differed between
polycythemic and nonpolycythemic patients were mean body mass index and Hb,
anaemic patients showed a significantly higher modified Medical Research Council
dyspnoea scale score (2.8 versus 2.6), lower 6-min walk distance (265 versus 325 m)
and shorter median survival (49 versus 74 months) than nonanaemic patients. In
regression models, anaemia independently predicted dyspnoea and reduced exercise
capacity. Anaemia in chronic obstructive pulmonary disease was an independent risk
factor for reduced functional capacity. Polycythemia prevalence was low and had no
association with worsened outcomes. Further work is required to evaluate the effect of
anaemia correction on outcomes in chronic obstructive pulmonary disease.

Pazienti e Metodi
811 pazienti ultra65enni (f = 61,7%; età media
80,1±7.5anni) consecutivamente ammessi in un reparto
di Medicina per acuti durante un periodo di 12 mesi.
Sono state valutate:
• funzioni cognitive (Mini Mental State Examination-MMSE)
• funzioni affettve (Geriatric Depression Scale-GDS 15 items))
• comorbilità (Charlson Index score)
• severità della pre-esistente ostruzione bronchiale (FEV1
%pred)
• gravità della patologia acuta (APACHE II score)
• indicatori nutrizionali e di fragilità (BMI, colesterolo ed
albumina serica)
• indicatori di infiammazione (VES e PCR)
• stato funzionale (IADL e Barthel Index pre-morboso,
all’ammissione ed alla dimissione)

Diagnosi di Anemia
L’ANEMIA è stata definita secondo I criteri
della World Health Organization (WHO):
Hb <12 d/dL nelle donne
Hb <13 g/dL negli uomini

Table 1. Characteristics of COPD study
population stratified for the presence of anemia
VARIABLES NO ANEMIA
(N=76)
ANEMIA
(N=82)
p
Age (years) 78.4±7.6 82.4±6.1 ,000
Age >80 years 37 71 ,000
Gender (Male) 29 59 ,000
Body Mass Index (Kg/m2) 24.3±4.4 24.2±4.6 n.s.
Smoking
Never 59 47 n.s.
Former 25 44 ,04
Current 16 9 n.s.
Mini Mental State Examination 22.6±5.4 20.7±6.5 ,056
Dementia (MMSE<18/30) 19 28 n.s.
Geriatric Depression Scale 4.7±3.2 4.7±3.0 n.s.
FEV1 (% of pred.) 82.5±8.3 58.6±7.8 ,05
FEV1 <60 % of pred. 37 75 ,05
Instrumental Activities of Daily Living (f. lost) 3.2±3.0 3.8±2.9 n.s.

Table 1. Characteristics of study population
stratified for the presence of anemia.
VARIABLES NO ANEMIA
(N=76)
ANEMIA
(N=82)
p
Barthel index (BI) pre-admission 83.4±26.5 73.5±28.5 ,026
Functional disability pre-admission (BI<60) 16 33 ,011
Barthel index at admission 67.3±33.8 51.6±35.4 ,005
Functional disability at admission (BI<60) 36 58 ,004
Barthel index at discharge 76.7±29.4 67.4±31.0 ,05
Functional disability at discharge (BI<60) 24 38 ,05
Apache II score 7.8±3.1 8.9±3.9 ,05
Charlson Index (CI) 3.4±1.5 4.1±1.8 ,009
High comorbidity (Charlson Index >3) 49 60 n.s.
Serum cholesterol (mg/dl) 188.2±46.3 171.8±42.1 ,021
Hypocholesterolemia (<140 mg/dl) 10 23 ,02
Serum albumin (mg/dl) 3.5±0.5 3.4±0.5 n.s.
Hypoalbuminemia (<3.4 mg/dl) 38 57 ,01
CRP (mg/dl) 45.4±52.0 49.6±46.0 n.s.
High CRP (>10 mg/dl) 56 77 ,005
Urea (mg/dl) 50.4±32.8 60.6±29.7 ,042
Creatinine(mg/dl) 1.15±0.9 1.29±0.6 n.s.
Renal Insufficiency (creatinine>1,3 mg/dl)

Table 3. Multiple Logistic Regression Analysis for
association between Anemia and clinical variable*
Variables B S.E. Exp (B) p
Age (>80 years) 1,77 0,43 5,9 ,000
Gender (male) -1,35 0,42 0,2 ,001
CRP (>10 mg/dl) 1,12 0,53 3,1 ,03
Renal insufficiency 1,07 ,503 2,9 ,03
*Adjusted for: severity of bronchial obstruction, pre-morbid functional disability, funcyional disability at hospital admission and at discharge, hypoalbuminemia, severity of acute ilness, ischemic heart disease and neoplastic disease.

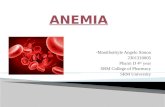
Kaplain-Meier curves stratified for anemia
INT MOR
2001000
Cu
m S
urv
iva
l
1,02
1,00
,98
,96
,94
,92
,90
,88
,86
,84
NON
ANEMIC
ANEMIC
P=0,02