Presentazione di PowerPoint -...
36
Transcript of Presentazione di PowerPoint -...


Le comorbidità: come valutarle nel’approccio
diagnostico e terapeutico
Guido Bonoldi
Direttore Dipartimento di Scienze Mediche
ASST Valle Olona


Comorbidità = medicina della complessità

COMORBIDITA’
presenza di 2 o più malattie concomitanti nello stesso soggetto
Classi di comorbidità
• Causale: malattie che hanno lo stesso meccanismo fisiopatologico
• Complicante: malattie che costituiscono complicazioni di altre patologie
• Concorrente: malattie croniche coesistenti che non hanno tra loro relazione di causa-effetto
• Intercorrente: malattie acute che si associano a patologie croniche.

Lancet, febbraio 2006:“Comorbidity end guidelines: conflicting interests”
Comorbidity is a regular feature of general practice.
However, evidence-based diagnostic and treatment strategies generally overlook comorbidity…performances indicators based on single-disease guidelines cannot accurately reflect the quality of care with multiple chronic diseases. Dealing with comorbidity needs a patient centered rather than a disease oriented approach.
Chris Van Weel e Francois Schellevis,
Università di Nijmegen
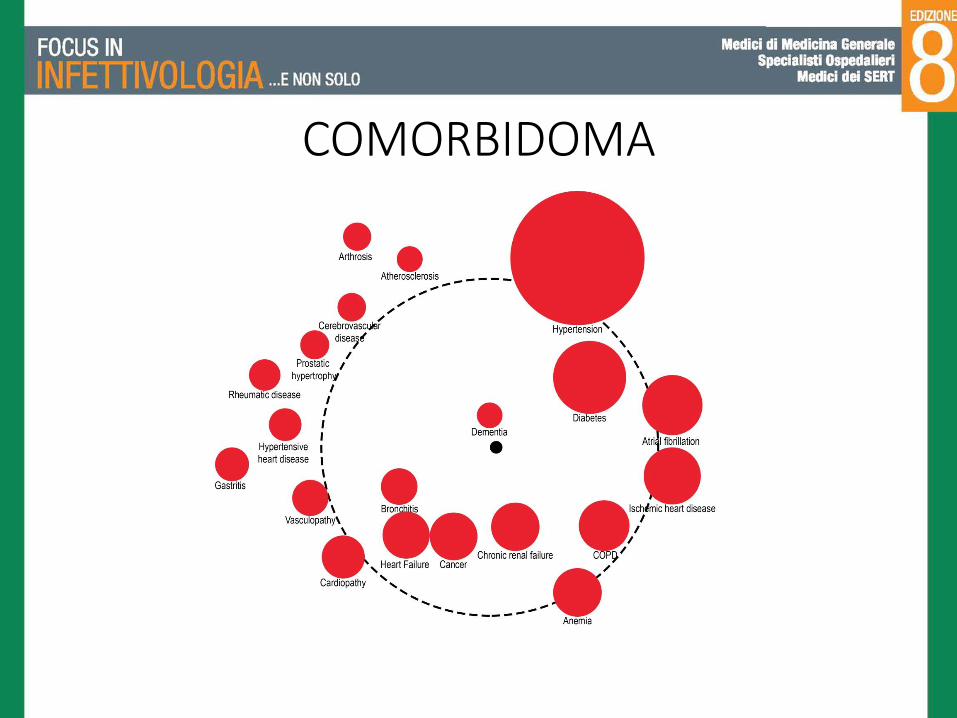
COMORBIDOMA

Presenza di 2 o più patologieconcomitanti
Compromissione fisica omentale che limita 1 o più
attività della vita quotidiana
Sindrome clinica caratterizzatada perdita di peso, fatica, bassaperformance motoria, anomaliedell’andatura e dell’equilibrio.
comorbidità
fragilità disabilità


Copyrights apply
Scompenso cardiaco, insufficienza renale ed anemia
• Correlazione lineare tra declino della funzione renale, anemia e ridotta produzione di eritropoietina, in particolare in pazienti con CrCl ≤ 30 ml/min.
(InCHIANTI study: Arch. Intern. Med. 2005; 165: 2222-7).
• Nello studio SOLVD (Studies of Left VentricularDysfunction) 22% dei pazienti presentava anemia, la gravità dell’anemia è risultata direttamente proporzionale all’aumento della mortalità

malattia cronicarenale
anemia
Insufficienza cardiaca
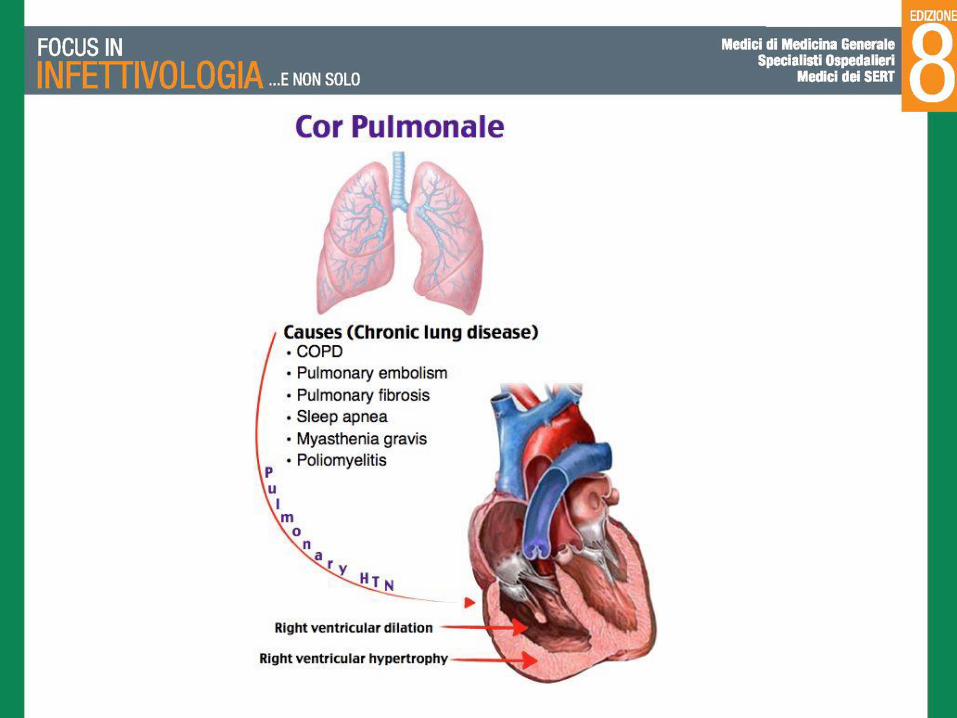

“Cor pulmonale parvus” in chronic obstructive pulmonary disease
(COPD) and emphysema. The Multi-Ethnic Study of Atherosclerosis
COPD Study
J Am Coll Cardiol. 2014 November 11; 64(19): 2000–2009. doi:10.1016/j.jacc.2014.07.991
Steven M. Kawut , Hooman D. Poor, Megha A. Parikh, Katja Hueper, Benjamin M. Smith, David A. Bluemke∫, Joao A. Lima‖ , Martin R. Prince , Eric A. Hoffman, John H. M. Austin , Jens Vogel-Claussen, and R. Graham Barr.

• Abstract
• Background: The classic cardiovascular complication of chronic obstructive pulmonary disease (COPD) is cor pulmonale, or enlargement of the right ventricle (RV). Most studies of cor pulmonale were conducted decades ago.
• Objective: We aimed to examine RV changes in contemporary COPD and emphysema using cardiac magnetic resonance imaging (MRI).
• Methods: We performed a case-control study nested predominantly in two general population studies of 310 participants with COPD and controls ages 50–79 years with ≥ 10 pack-years of smoking and who were free of clinical cardiovascular disease. RV volumes and mass were assessed using MRI. COPD and COPD severity were defined by standard spirometric criteria. Percent emphysema was defined as percent of lung regions <-950 Hounsfield units on full-lung computed tomography; emphysema subtypes were scored by radiologists. Results were adjusted for age, race/ethnicity, sex, height, weight, smoking status, pack-years, systemic hypertension and sleep apnea.
• Results: RV end-diastolic volume was reduced in COPD compared to controls (-7.8 mL, 95% CI: -15.0, -0.5 mL; p=0.04). Increasing severity of COPD was associated with smaller RV end-diastolic volume (p=0.004) and lower RV stroke volume (p<0.001). RV mass and ejection fraction were similar between the groups. Greater percent emphysema was also associated with smaller RV end-diastolic volume (p=0.005) and stroke volume (p<0.001), as was the presence of centrilobular and paraseptal emphysema.
• Conclusions: RV volumes are lower without significant alterations in RV mass and ejection fraction in contemporary COPD (“cor pulmonale parvus”) and this reduction is related to greater percent emphysema on computed tomography.

Impaired Left Ventricular Filling in COPD and Emphysema: Is It the Heart or the Lungs?
Benjamin M. Smith, MD, Martin R. Prince, MD, PhD, Eric A. Hoffman, PhD, David A. Bluemke, MD, PhD, Chia-Ying Liu, PhD, Dan Rabinowitz, PhD, Katja Hueper, MD, Megha A. Parikh, MS, Antoinette S. Gomes, MD, Erin D. Michos, MD, MHS, João A.C.
Lima, MD, R. Graham Barr, MD, DrPH
CHESTVolume 144, Issue 4, Pages 1143-1151 (October 2013)
DOI: 10.1378/chest.13-0183
• ABSTRACT
• BACKGROUND: COPD and heart failure with preserved ejection fraction overlap clinically, and impaired left ventricular (LV) filling is commonly reported in COPD. The mechanism underlying these observations is uncertain, but may include upstream pulmonary dysfunction causing low LV preload or intrinsic LV dysfunction causing high LV preload. The objective of this study is to determine if COPD and emphysema are associated with reduced pulmonary vein dimensions suggestive of low LV preload.
• METHODS: The population-based Multi-Ethnic Study of Atherosclerosis (MESA) COPD Study recruited smokers aged 50 to 79 years who were free of clinical cardiovascular disease. COPD was defined by spirometry. Percent emphysema was defined as regions <-910 Hounsfield units on full-lung CT scan. Ostial pulmonary vein cross-sectional area was measured by contrast-enhanced cardiac magnetic resonance and expressed as the sum of all pulmonary vein areas. Linear regression was used to adjust for age, sex, race/ethnicity, body size, and smoking.
• RESULTS: Among 165 participants, the mean (± SD) total pulmonary vein area was 558 ±159 mm2 in patients with COPD and 623 ± 145 mm2 in control subjects. Total pulmonary vein area was smaller in patients with COPD (-57 mm2; 95% CI, -106 to -7 mm2; P = .03) and inversely associated with percent emphysema (P < .001) in fully adjusted models. Significant decrements in total pulmonary vein area were observed among participants with COPD alone, COPD with emphysema on CT scan, and emphysema without spirometrically defined COPD.
• CONCLUSIONS: Pulmonary vein dimensions were reduced in COPD and emphysema. These findings support a mechanism of upstream pulmonary causes of underfilling of the LV in COPD and in patients with emphysema on CT scan.

Figure 2
CHEST 2013 144, 1143-1151DOI: (10.1378/chest.13-0183)
Presentazione spesso atipica della sepsi nell’anziano
• Ipertermia/ipotermia
• Delirium/letargia
• Disturbi del comportamento
• Perdita di autonomia
• Anoressia astenia vomito
• Incontinenza urinaria
• Cadute
• Tachipnea
• Ipotensione ortostatica

Risposta febbrile attenuata nel paziente anziano
• Alterata termoregolazione nell´anziano: vasocostrizione, perdita della normale regolazioneipotalamica e della capacità di termogenesi da parte del tessuto adiposo bruno.
• La temperatura basale è più bassa negli anziani.
• Considerare come „febbre“ un aumento della temperatura ≥ 1,1 °C rispetto alla temperaturabasale.

Indici di comorbidità
• Cumulative Illness Rating Scale - CIRS• Indice di severità
• Indice di comorbilità
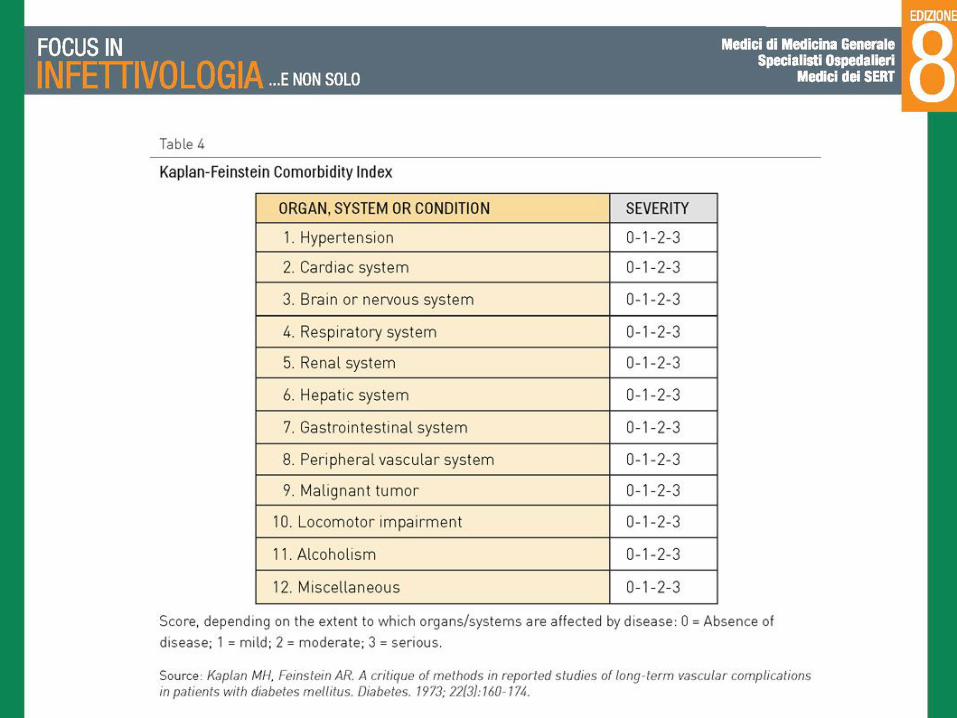
• Indice di Kaplan-Feinstein
• Indice di Charlson
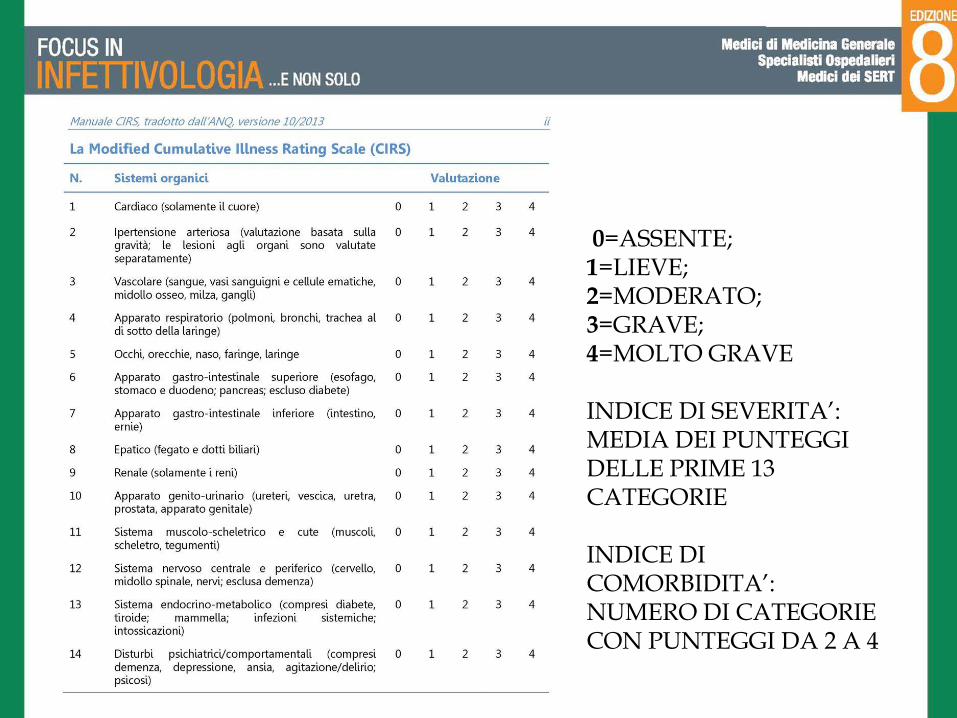
0=ASSENTE; 1=LIEVE; 2=MODERATO; 3=GRAVE;4=MOLTO GRAVE
INDICE DI SEVERITA’: MEDIA DEI PUNTEGGI DELLE PRIME 13 CATEGORIE
INDICE DICOMORBIDITA’: NUMERO DI CATEGORIE CON PUNTEGGI DA 2 A 4
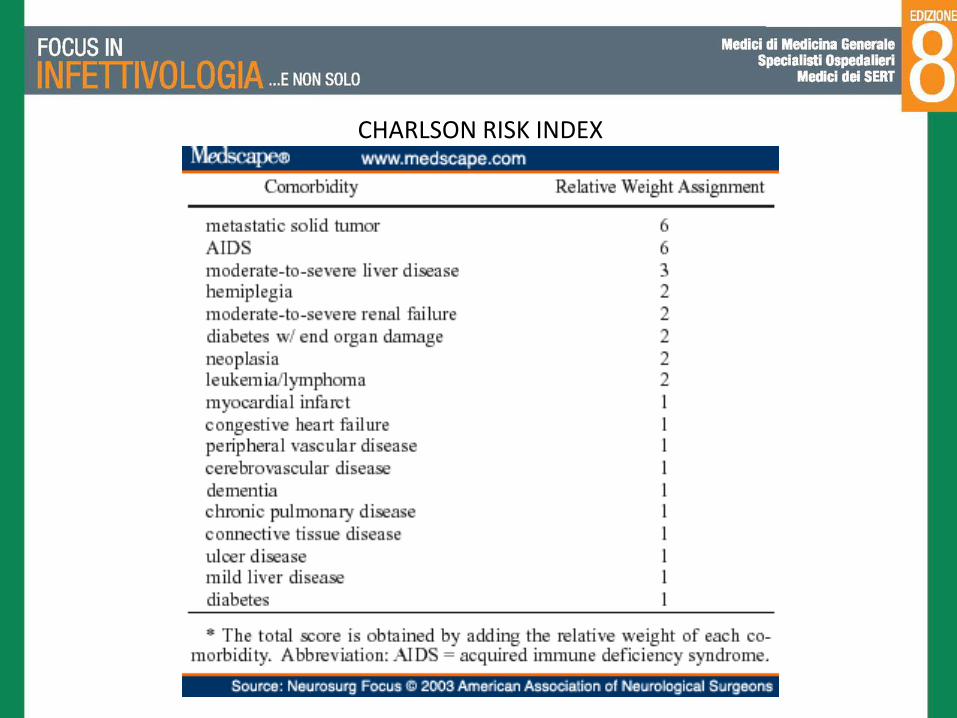
CHARLSON RISK INDEX

Copyrights apply