
Lopiano no video - Mondino · 14/12/2017 1 Leonardo Lopiano Università di Torino Nuove prospettive...
16
14/12/2017 1 Leonardo Lopiano Università di Torino Nuove prospettive terapeutiche per la malattia di Parkinson (farmaci e dispositivi)
Transcript of Lopiano no video - Mondino · 14/12/2017 1 Leonardo Lopiano Università di Torino Nuove prospettive...
14/12/2017
1
Leonardo LopianoUniversità di Torino
Nuove prospettive terapeutiche per la malattia di Parkinson (farmaci e dispositivi)

14/12/2017
2
Poewe et al. 2017
Terapia farmacologica
14/12/2017
3
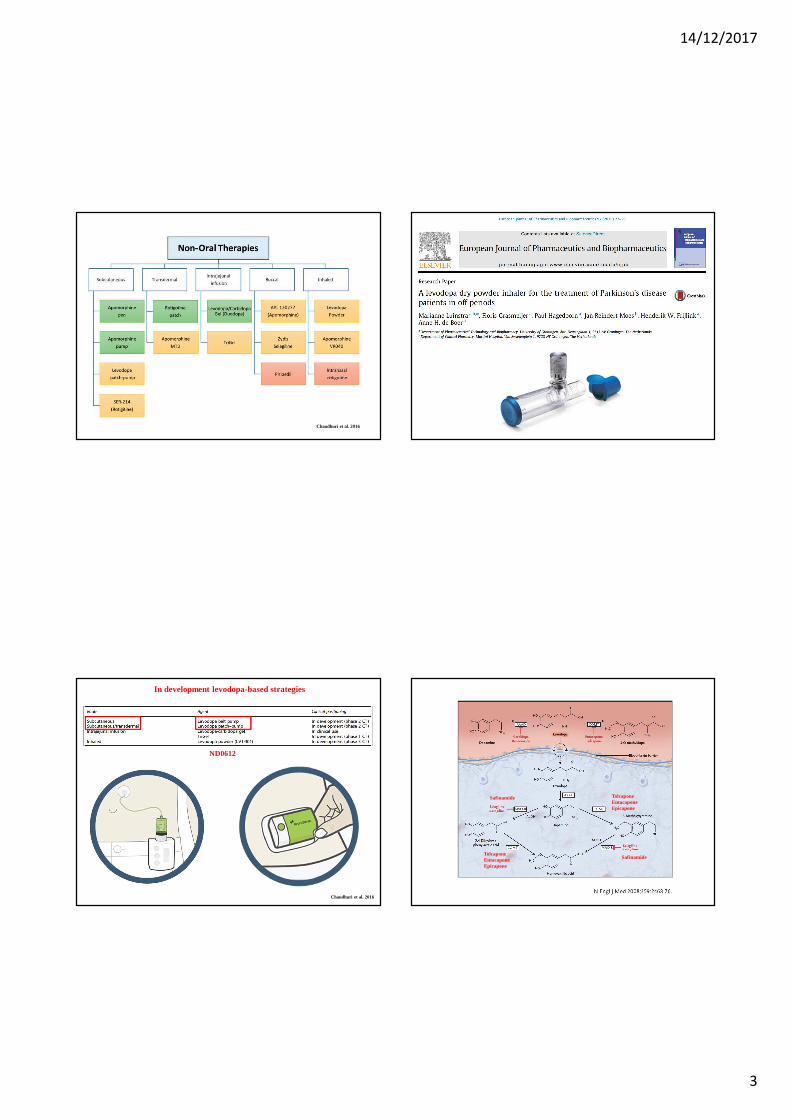
Chaudhuri et al. 2016
Chaudhuri et al. 2016
In development levodopa-based strategies
ND0612
Safinamide
Safinamide TolcaponeEntacaponeEpicapone
TolcaponeEntacaponeEpicapone

14/12/2017
4
Safinamide
• Phase III, multicentre,randomised, double-blind,placebo controlled, parallelgroup, 24 week duration trial.
• To evaluate the efficacy andsafety of safinamide versusplacebo as add-on therapy to astable dose of L-Dopa (alone orwith other antiparkinsoniandrugs) in pts with mid- to late-stage PD and motorfluctuations.
• The primary efficacy measurewas the change from baselineto 24 weeks in daily ON timewith no/non troublesomedyskinesia. The addiction of safinamide 50 mg/day or
100 mg/day to L-Dopa in PD patients andmotor fluctuations increased total ON timewith no or non-troublesome dyskinesia
At six months, safinamidesignificantly reduced dailyOFF time when used as add-on to levodopa.
SETTLE STUDY
At six months, safinamidesignificantly increaseed dailyON time when used as add-onto levodopa.

14/12/2017
5
• The primary endpoint was the mean change from baseline (study016 start) to study end (2 years) in the total Dyskinesia RatingScale (DRS) score evaluated during ON time.
14/12/2017
6
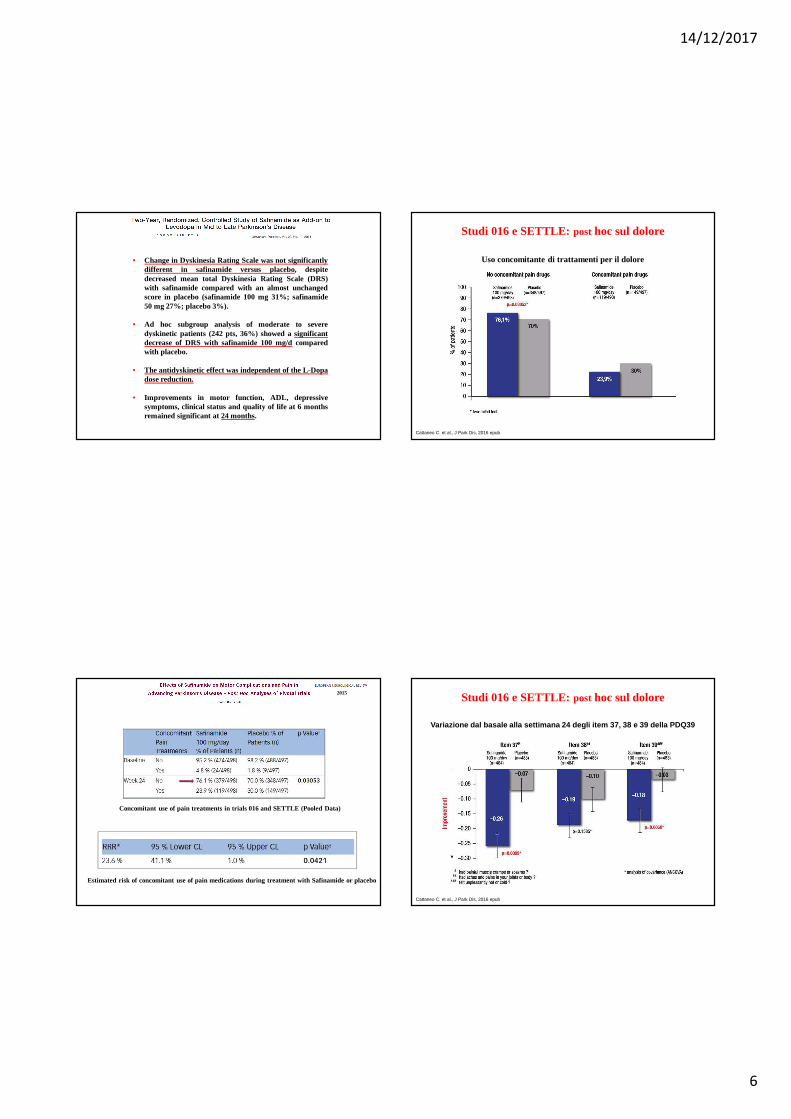
• Change in Dyskinesia Rating Scale was not significantlydifferent in safinamide versus placebo, despitedecreased mean total Dyskinesia Rating Scale (DRS)with safinamide compared with an almost unchangedscore in placebo (safinamide 100 mg 31%; safinamide50 mg 27%; placebo 3%).
• Ad hoc subgroup analysis of moderate to severedyskinetic patients (242 pts, 36%) showed a significantdecrease of DRS with safinamide 100 mg/d comparedwith placebo.
• The antidyskinetic effect was independent of the L-Dopadose reduction.
• Improvements in motor function, ADL, depressivesymptoms, clinical status and quality of life at 6 monthsremained significant at 24 months.
Concomitant use of pain treatments in trials 016 and SETTLE (PooledData)
Estimated risk of concomitant use of pain medications during treatment with Safinamide or placebo
2015
Uso concomitante di trattamenti per il dolore
Cattaneo C. et al., J Park Dis, 2016 epub
Studi 016 e SETTLE: post hoc sul dolore
Variazione dal basale alla settimana 24 degli item 37, 38 e 39 della PDQ39
Cattaneo C. et al., J Park Dis, 2016 epub
Studi 016 e SETTLE: post hoc sul dolore
14/12/2017
7
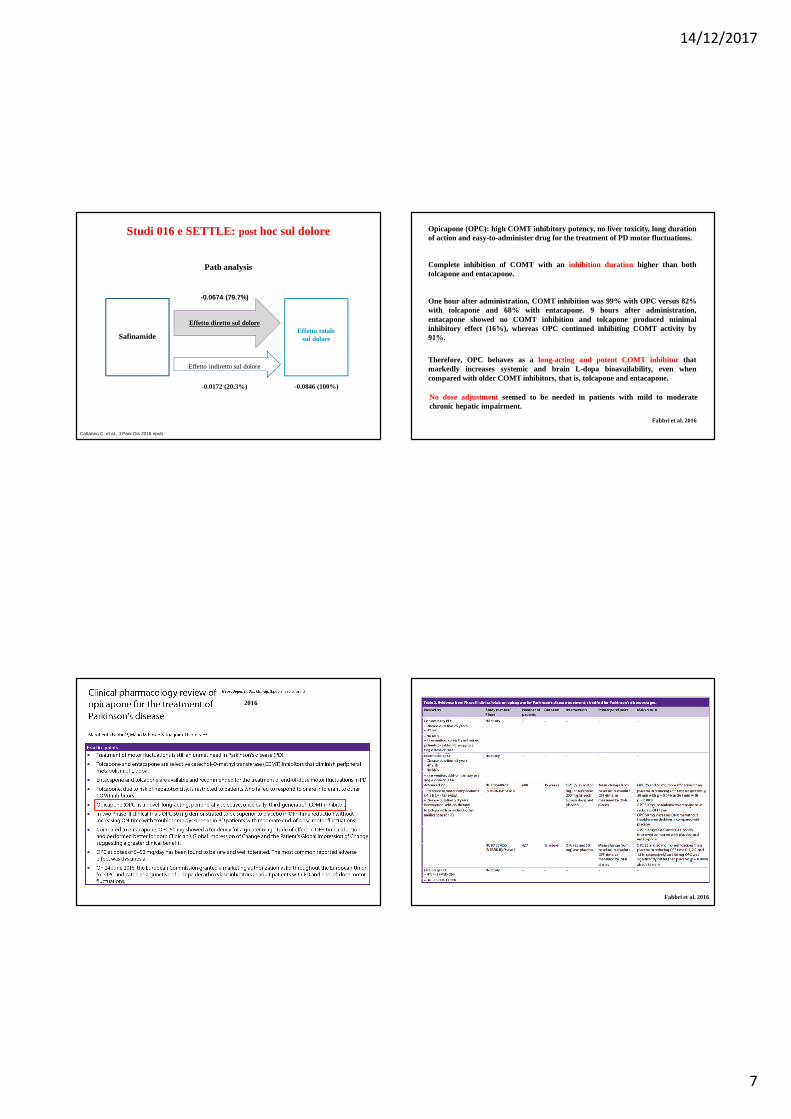
Cattaneo C. et al., J Park Dis 2016 epub
Path analysis
SafinamideEffetto totale
sul dolore
Effetto diretto sul dolore
Effetto indiretto sul dolore
-0.0172 (20.3%) -0.0846 (100%)
-0.0674 (79.7%)
Studi 016 e SETTLE: post hoc sul dolore
2016
Fabbri et al. 2016
Opicapone (OPC): high COMT inhibitory potency, no liver toxicity, l ong durationof action and easy-to-administer drug for the treatment of PD motor fluctuations.
Complete inhibition of COMT with an inhibition duration higher than bothtolcapone and entacapone.
One hour after administration, COMT inhibition was 99% with OPC versus 82%with tolcapone and 68% with entacapone. 9 hours after administration,entacapone showed no COMT inhibition and tolcapone produced minimalinhibitory effect (16%), whereas OPC continued inhibiting COMT activity by91%.
Therefore, OPC behaves as along-acting and potent COMT inhibitor thatmarkedly increases systemic and brain L-dopa bioavailability, even whencompared with older COMT inhibitors, that is, tolcapone and entacapone.
No dose adjustmentseemed to be needed in patients with mild to moderatechronic hepatic impairment.
Fabbri et al. 2016

14/12/2017
8
High COMT inhibitory potency, noliver toxicity, long duration of actionand easy-to-administer drug for thetreatment of PD motor fluctuations.
Complete inhibition of COMT with aninhibition duration higher than bothtolcapone and entacapone.
No dose adjustment seemed to beneeded in patients with mild tomoderate chronic hepatic impairment.
• OPC at doses of 5 mg/day to 50 mg/day has been found to besafeandwell tolerated.
• Two Phase III double–bind RCTs have investigated the efficacy ofOPC as adjunctive therapy to L-dopa for advanced PD patientswithmoderate end of-dose motor fluctuations showing thatOPC 50 mgwas superior to placebo and non inferior to entacapone in reducingOFF time.
• OPC 50 mg obtained a meanreduction time in the OFF state ofabout 60 min daily versus placebo without increasing the ON-time.
• OPC 50 mg presented a tendency for agreater effect magnitude forOFF-time reduction.
Fabbri et al. 2016
• Dyskinesiasare the most common AE, even when compared withentacapone and placebo. Interestingly, no issues of concern wereobserved for severe diarrhoea and report of urine discoloration.
Non-levodopa-based treatment strategies
Oertel 2017
Non-dopaminergic mode of action: new compounds or new formulation

14/12/2017
9
Oertel 2017
Non-dopaminergic mode of action: drug approved in another indication, nowtested in Parkinson’s disease
Subcutaneous apomorphine infusion
This is the first clinical trial performed with the levodopa-entacapone-carbidopaintestinal gel (LECIG). The results suggest that the required levodopa dose can besuccessfully reduced with LECIG without lowering the clinical effect.
TRIGEL infusion
DEEP BRAIN STIMULATION
130 Hz
• Amplitude (max 3,6 mA)• Frequency (130 Hz)• Pulse width (60 µsec)
Monopolarcathodic
Bipolarcathodic
Double monopolar
14/12/2017
10
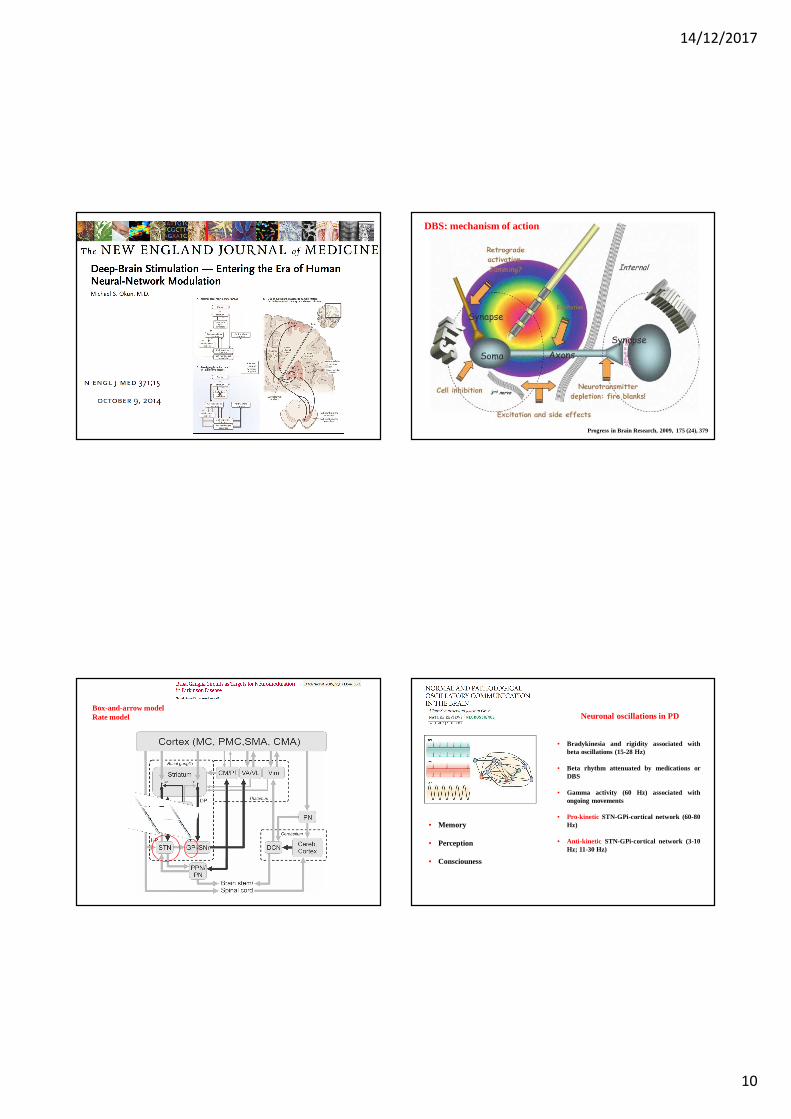
Box-and-arrow modelRate model
Progress in Brain Research, 2009, 175 (24), 379
DBS: mechanism of action
• Memory
• Perception
• Consciouness
Neuronal oscillations in PD
• Bradykinesia and rigidity associated withbeta oscillations (15-28 Hz)
• Beta rhythm attenuated by medications orDBS
• Gamma activity (60 Hz) associated withongoing movements
• Pro-kinetic STN-GPi-cortical network (60-80Hz)
• Anti-kinetic STN-GPi-cortical network (3-10Hz; 11-30 Hz)

14/12/2017
11
Suppression of beta activity before andduring movement
Relationship between systemperformance and neural synchrony
Best results have been reported in patients withadvanced PD and:
• excellent LD response• younger age• no or few axial non–LD-responsive motor symptoms• no or very mild cognitive impairment• absence of or well-controlled psychiatric disease
56,7
24,527,3
36,4
10,5
2,8 1,9 3,3
11,8
6,0 5,9 6,6
23,3
11,013,1
16,8
0,0
10,0
20,0
30,0
40,0
50,0
60,0
pre-op 1 y 5y 11y
UPDRS
score
UPDRS III tot
tremore
rigidità
bradicinesia
*
*
*
*
11,0
4,7
6,3
9,7
2,01,2
1,62,42,3
0,71,1
1,61,91,1 1,3
1,9
0,0
2,0
4,0
6,0
8,0
10,0
12,0
pre-op 1 y 5y 11y
UPDRS
score
assiali
linguaggio
deambulazione
stabilità posturale*
UPDRS III – Med OFF vs Med OFF/Stim On
p < 0.05 vs pre-op
• 26 patients• Mean Follow-up: 11 ys
14/12/2017
12
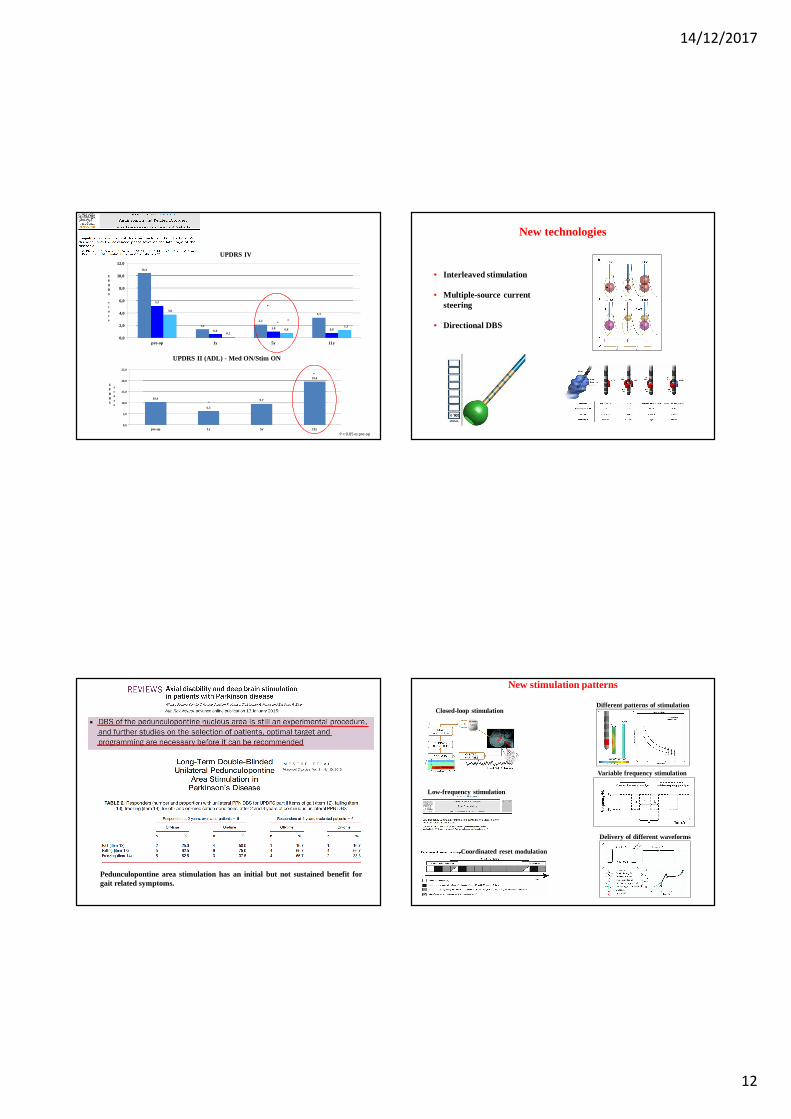
10,4
6,3
9,7
19,6
0,0
5,0
10,0
15,0
20,0
25,0
pre-op 1y 5y 11y
UPDRS
score
UPDRS II (ADL) - Med ON/Stim ON
*
10,4
1,4
2,2
3,3
5,2
0,61,0 0,8
3,8
0,20,8
1,3
0,0
2,0
4,0
6,0
8,0
10,0
12,0
pre-op 1y 5y 11y
UPDRS
score
UPDRS IV
*
**
*
P < 0.05 vs pre-op
Pedunculopontine area stimulation has an initial but not sustained benefit forgait related symptoms.
New technologies
• Interleaved stimulation
• Multiple-source currentsteering
• Directional DBS
New stimulation patterns
Closed-loop stimulationDifferent patterns of stimulation
Low-frequency stimulation
Variable frequency stimulation
Delivery of different waveforms
Coordinated reset modulation
14/12/2017
13
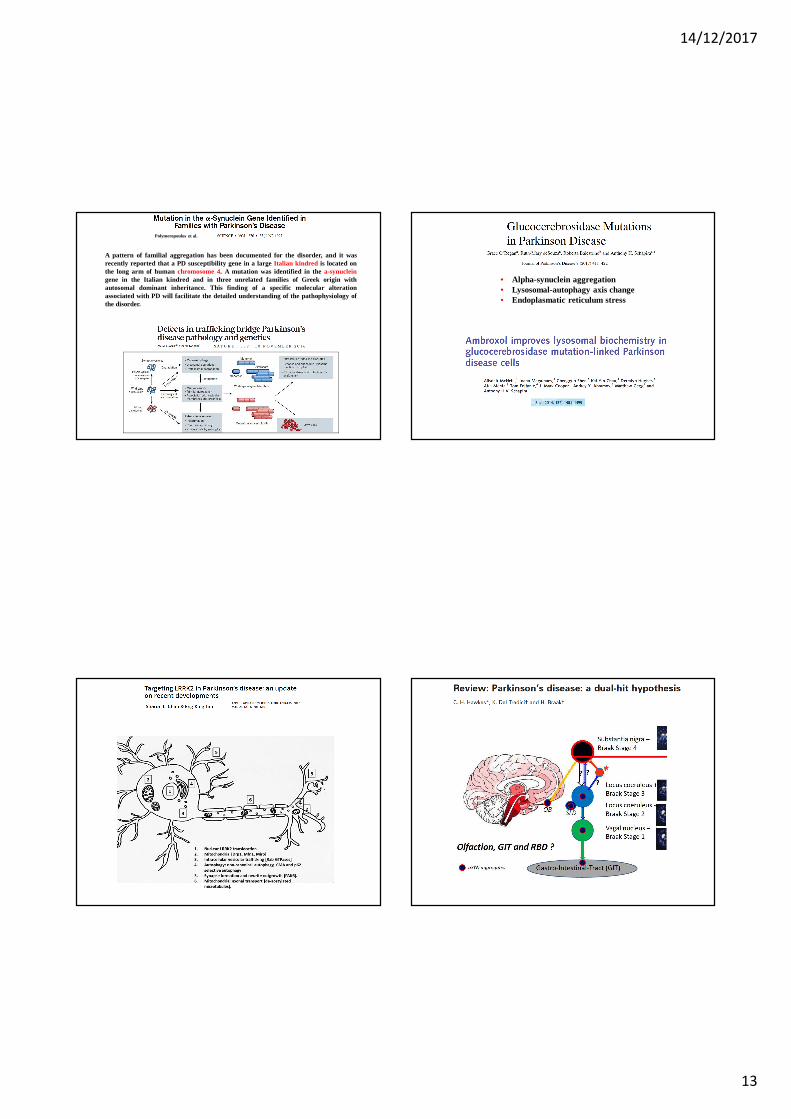
Polymeropoulos et al.
A pattern of familial aggregation has been documented for the disorder, and it wasrecently reported that a PD susceptibility gene in a largeItalian kindred is located onthe long arm of human chromosome 4. A mutation was identified in the a-synucleingene in the Italian kindred and in three unrelated families of Greek origin withautosomal dominant inheritance. This finding of a specific molecular alterationassociated with PD will facilitate the detailed understanding of thepathophysiology ofthe disorder.
• Alpha-synuclein aggregation• Lysosomal-autophagy axis change• Endoplasmatic reticulum stress
14/12/2017
14
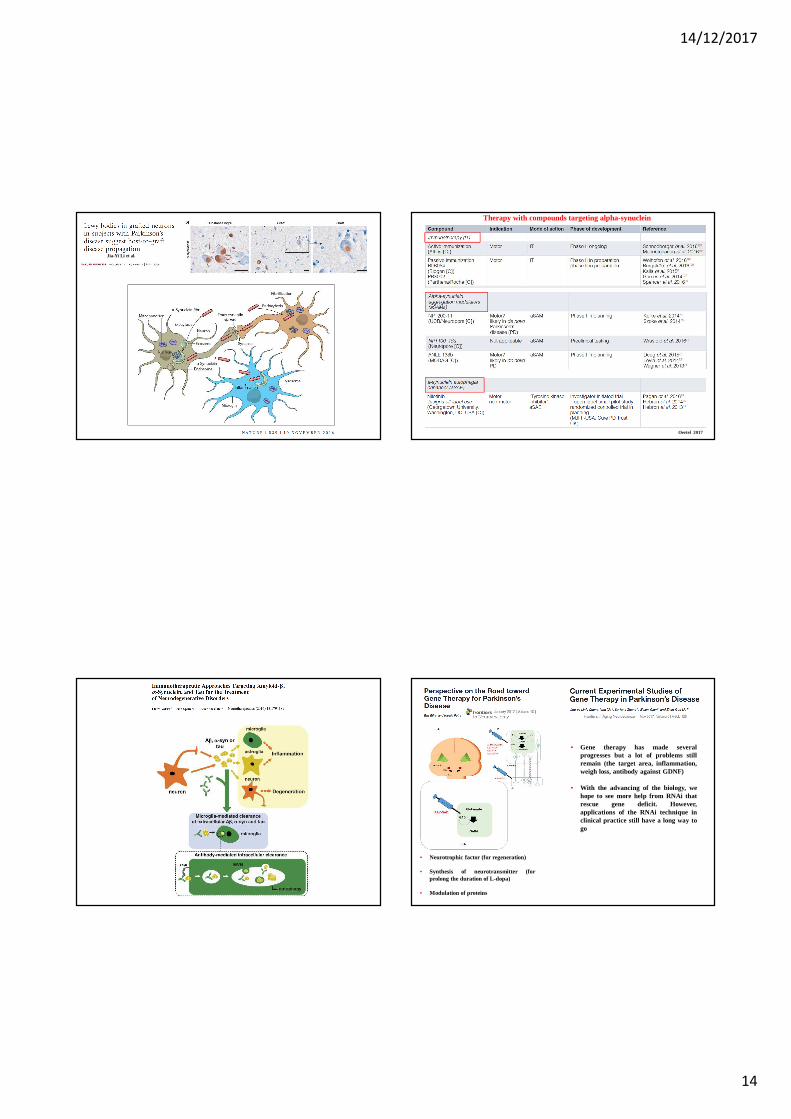
Jia-Yi Li et al.
Oertel 2017
Therapy with compounds targeting alpha-synuclein
• Gene therapy has made severalprogresses but a lot of problems stillremain (the target area, inflammation,weigh loss, antibody against GDNF)
• With the advancing of the biology, wehope to see more help from RNAi thatrescue gene deficit. However,applications of the RNAi technique inclinical practice still have a long way togo
• Neurotrophic factor (for regeneration)
• Synthesis of neurotransmitter (forprolong the duration of L-dopa)
• Modulation of proteins

14/12/2017
15
Comparison of the major approaches to cell-based therapies in Parkinson’s disease
2015
Trapianti di cellule mesencefaliche fetali
Studio europeo coordinato dall’Università di Cambridge chevaluterà 20 pazienti per almeno un anno e terminerà nel 2020(TRANSEURO Trial)
Cellule staminali adulte mesenchimali
Prelevate dal paziente o da un donatore, amplificate ereintrodotte nell’organismo per via intra-ventricolare ointra-arteriosa
14/12/2017
16
Centro Regionale Esperto per la malattia di Parkinson e i disturbi del movimento
Dipartimento di Neuroscienze “Rita-Levi Montalcini”Università di Torino
Dipartimento di Neuroscienze e Salute MentaleAOU Città della Salute e della Scienza di Torino
SC Neurologia 2U














![Malattia di Parkinson [slide ITA] -](https://static.fdocumenti.com/doc/165x107/55a332781a28ab86618b462c/malattia-di-parkinson-slide-ita-wwwluigibarattocom.jpg)


