Adenocarcinoma pancreatico: Prospettive degli studi di...
35
Adenocarcinoma pancreatico: Prospettive degli studi di fase I Stefano Cascinu Modena Cancer Center Modena, Italy
Transcript of Adenocarcinoma pancreatico: Prospettive degli studi di...

Adenocarcinoma pancreatico:
Prospettive degli studi di fase I
Stefano Cascinu
Modena Cancer Center Modena, Italy
Fasi I e adenocarcinoma pancreatico:
• Necessità di una terapia sistemica efficace
• La chemioterapia è la base della attuale terapia standard:
– Gem/abraxane
– FOLFIRINOX

Quale bersaglio?
• Cellule tumorali con relative mutazioni
• Stroma
• immunità
Fasi I e adenocarcinoma pancreatico:
Come disegnare uno studio di fase I nell’adenocarcinoma pancreatico?
Fasi I in corso
• BK-8040 (CXCR4 antagonist)
• Afatinib (irreversible EGFR Family Inhibitor)
• Gedatosilisib (Dual Inhibitor of PI3K and mTOR inhibitor)
• Defactinib (FAK focal adhesion kinase) inhibitor)
• Veliparib (PARP inhibitor)

High prevalence: KRAS, TP53, CDKN2A, & SMAD4
Other mutations: High variability and low prevalence
Pancreatic Cancer Is Genetically Diverse

Ras Mutations and Tumor Type
K ≈ 30-50 Lung (NSC) H, K <5 Breast N >50 Bile Duct H, N, K ≈ 25 Head & Neck H, N, K ≈ 50-80 Thyroid
≈ 20-86 Cervix K ≈ 40-50 Colon K ≈ 80 Pancreas
Predominant Ras Mutation % Ras Mutation Cancer

Phase II study of refametinib (BAY 86-9766), an allosteric dual MEK 1/2 inhibitor, and gemcitabine in patients with unresectable, locally advanced or metastatic pancreatic cancer Jean-Luc Van Laethem1, Jacek Jassem2, Volker Heinemann3, Collin Weekes4, John Bridgewater5, Stefano Cascinu6, Bohuslav Melichar7, Marc Peeters8, Paul Ross9, Piotr Saramak10, Marius Giurescu11, Vittorio L Garosi12, Katrin Roth11, Anke Schulz11, Michael Teufel11, Barrett H Childs13 Hanno Riess14
Ras Mutations as a therapeutic target
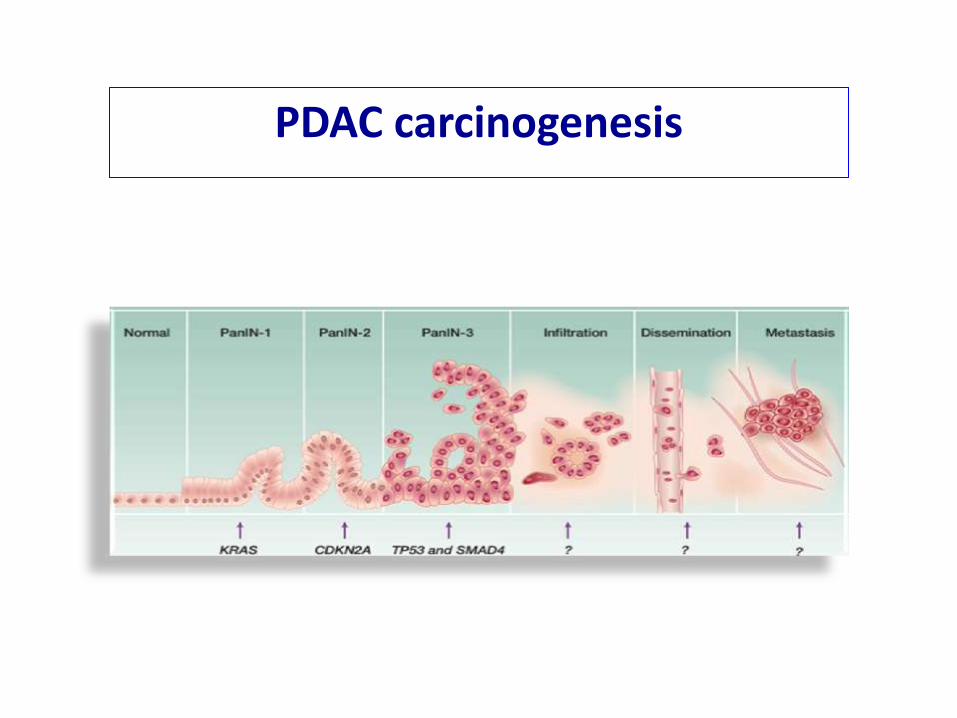
PDAC carcinogenesis
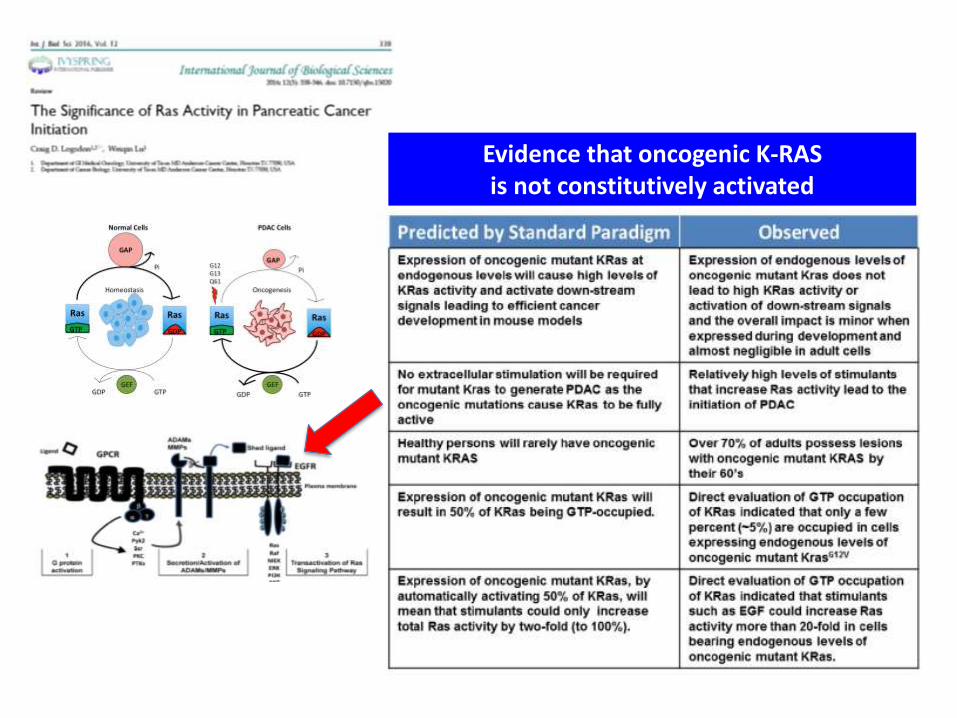
Evidence that oncogenic K-RAS is not constitutively activated
PDAC, pancreatic ductal adenocarcinoma
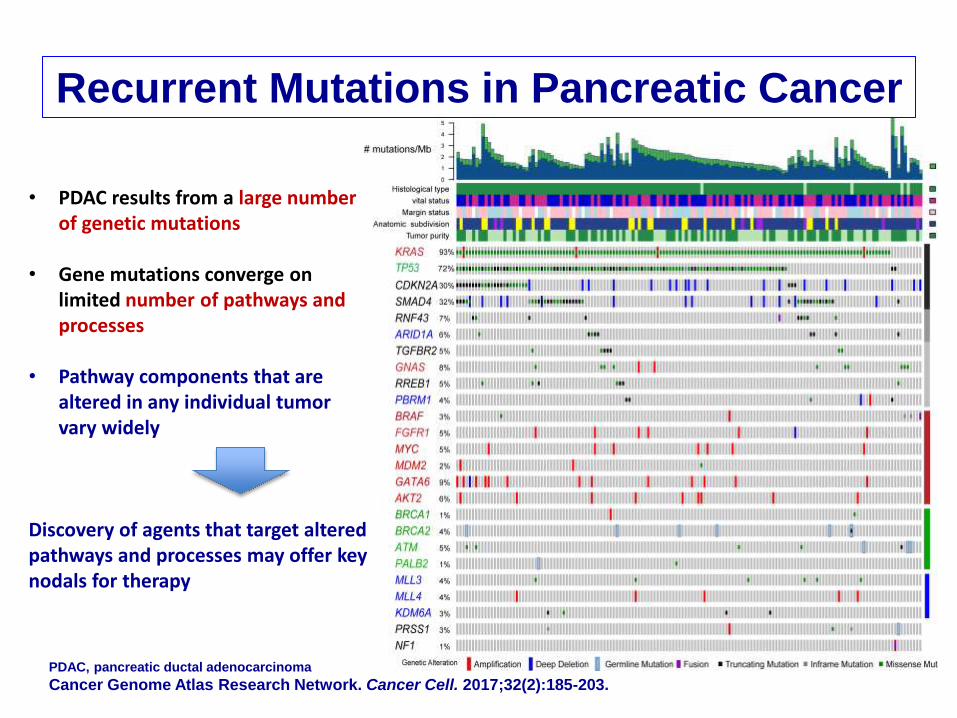
Cancer Genome Atlas Research Network. Cancer Cell. 2017;32(2):185-203.
Recurrent Mutations in Pancreatic Cancer
• PDAC results from a large number of genetic mutations
• Gene mutations converge on limited number of pathways and processes
• Pathway components that are altered in any individual tumor vary widely
Discovery of agents that target altered pathways and processes may offer key nodals for therapy

Integrated Genomic Analysis Revealed Potential Novel Vulnerabilities
N = 456 PDAC tissues 32 recurrently mutated genes 10 pathways & processes
Bailey P, et al. Nature. 2016;531(7592):47-52.
P. Bailey
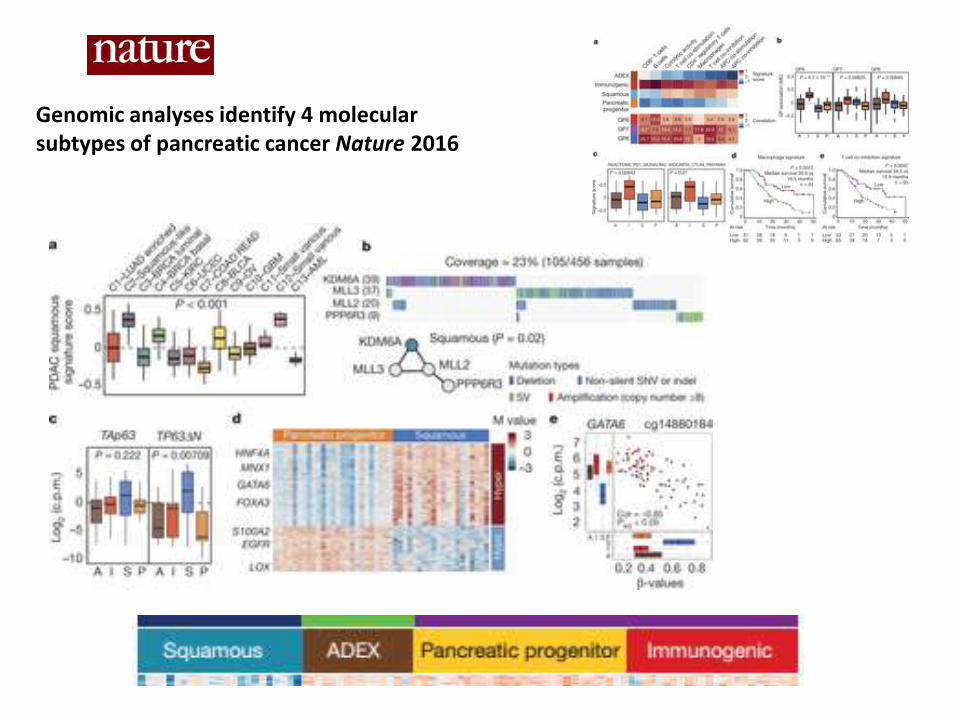
Genomic analyses identify 4 molecular subtypes of pancreatic cancer Nature 2016


protean, from Proteus with the meaning of "mutable", "capable of assuming many forms".
Pancreatic cancer: a “protean” disease
Proteus can foretell the future
but he will change his shape to
avoid having to. He answers only
to someone who is capable of
capturing him.

PDAC is characterized by low tumor
cellularity and a dense microenvironment
Neesse A, Ellenrieder V. Z Gastroenterol. 2015;53(4):337-338.

Rhim AD et al. Cell 2012
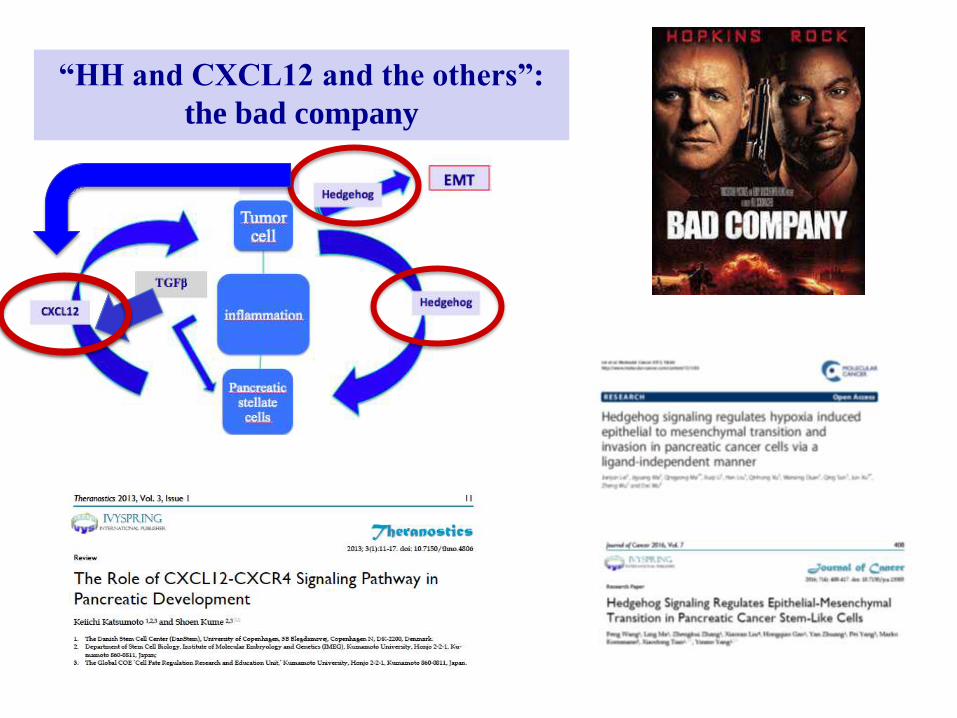
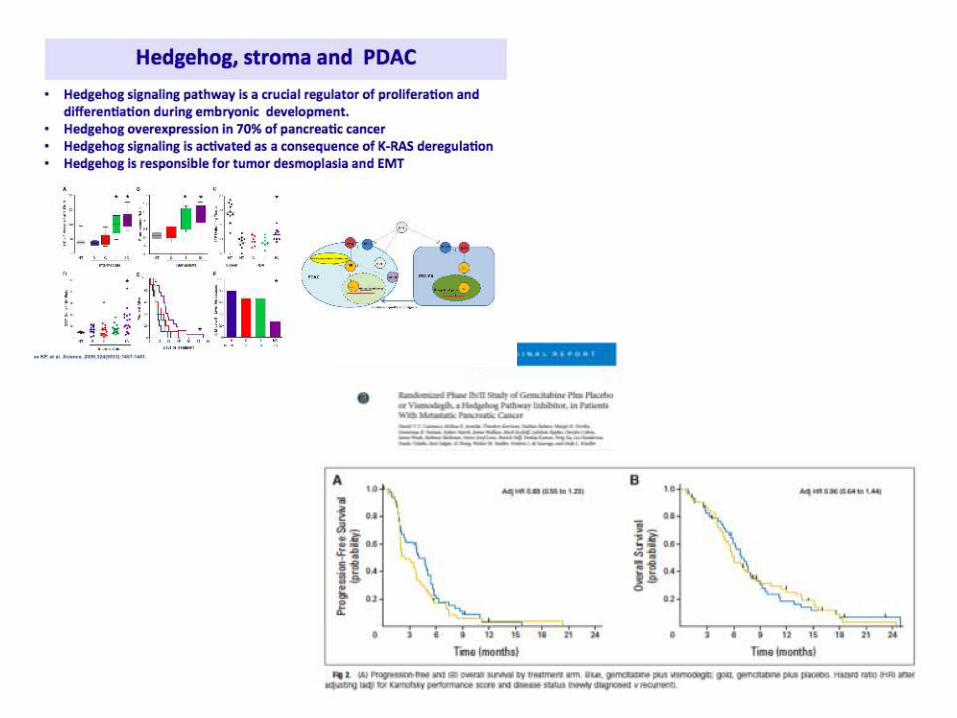
“HH and CXCL12 and the others”:
the bad company

Mesenchymal cancer cells
CD24+ cells
CD44+ cells
CD133+ cells
SHH
VEGF
IL-6
IGFB
SHH, PDGF, TGF-B, CXCL12
Epithelial cancer cells
Stellate
Cells
CAFs TGF-b CXCL12
CXCL12
IL-1β
IL-6 COX-2
K-Ras Mutation
Cellular necrosis, DAMPs
Andrikou, Cascinu, 2017

Targeting key signaling and transcription hubs: EMT
Napabucasin
Baumgart S, et al. Cancer Discov. 2014;4(6):688-701.
NFAT/STAT3 target genes: • PDL-1
• GM-CSF
• CXCL12
• CXCL5
• MMP11
• MMP1
• WNT1
• WNT10
• EGFR
• ...and stemness inhibition !

BBI608 (Napabucasin) = STAT3 Inhibitor
Phase Ib trial with napabucasin in combination with gemcitabine and nab-paclitaxel in patients with
metastatic pancreatic adenocarcinoma
N=41
Bekaii-Saab TS, et al. J Clin Oncol. 2017;35(suppl 4): Abstract 4106.
Promising activity in patients with refractory, heavily pretreated metastatic pancreatic cancer (N = 71); particularly, in patients who are taxane naïve. DCR was observed in 55 (77%), with 1 CR (1.4%) and 26 PR (37%) Treatment-related grade 3 adverse effects included diarrhea (4.9%), abdominal pain (4.9%), and nausea (2.4%), and were rapidly reversible
NCT02231723
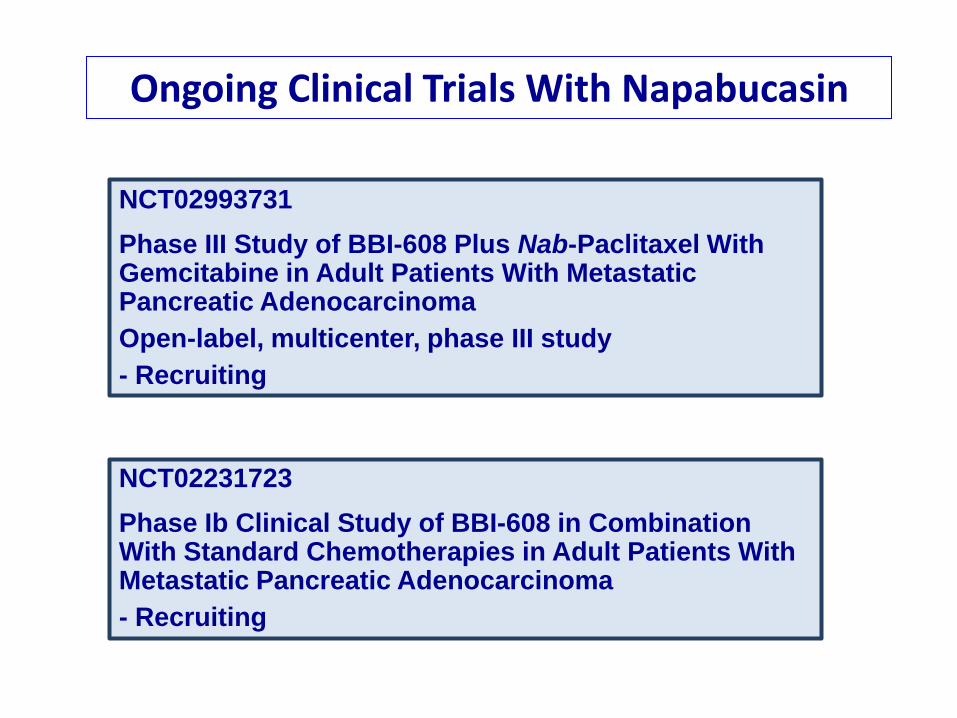
NCT02993731
Phase III Study of BBI-608 Plus Nab-Paclitaxel With Gemcitabine in Adult Patients With Metastatic Pancreatic Adenocarcinoma
Open-label, multicenter, phase III study
- Recruiting
NCT02231723
Phase Ib Clinical Study of BBI-608 in Combination With Standard Chemotherapies in Adult Patients With Metastatic Pancreatic Adenocarcinoma
- Recruiting
Ongoing Clinical Trials With Napabucasin

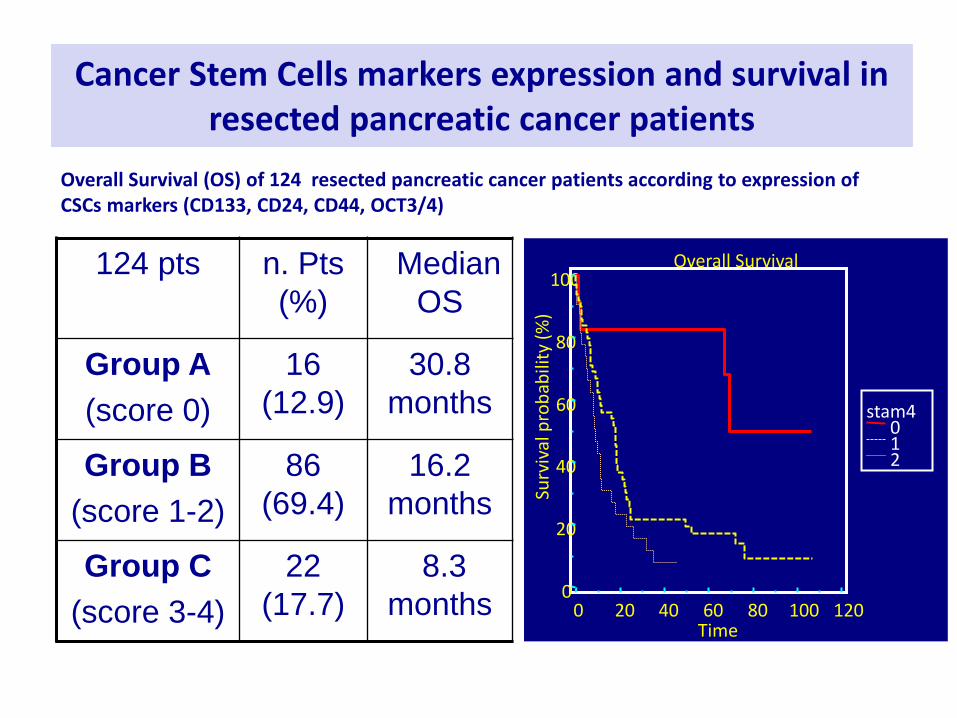
Cancer Stem Cells markers expression and survival in resected pancreatic cancer patients
124 pts n. Pts
(%)
Median
OS
Group A
(score 0)
16
(12.9)
30.8
months
Group B
(score 1-2)
86
(69.4)
16.2
months
Group C
(score 3-4)
22
(17.7)
8.3
months
stam4 0 1 2
Overall Survival
0 20 40 60 80 100 120
100
80
60
40
20
0
Time
Surv
ival
pro
bab
ility
(%
)
Overall Survival (OS) of 124 resected pancreatic cancer patients according to expression of CSCs markers (CD133, CD24, CD44, OCT3/4)

Targeting the Tumor Microenvironment
Stroma cells CAF Stellate cells
ECM Hyaluronic acid collagen I-IV laminin, fibronectin
Stromal Signaling Hedgehog TGFβ
CTGF
Immune regulation PD-1/PD-L1 CTLA4 Treg, MDSC
Tumor stroma

Multifaceted Biology of PDA
Hidalgo M, et al. Clin Cancer Res. 2012;18(16):4249-4256. PDA, pancreatic ductal adenocarcinoma
Multifaceted Biology of PDA
Hidalgo M, et al. Clin Cancer Res. 2012;18(16):4249-4256. PDA, pancreatic ductal adenocarcinoma
La somministrazione cronica di inibitori di HH riduce lo stroma ma
non determina alcun vantaggio terapeutico. Vi è anzi un aumento di
aggressività del tumore (attività proliferativa; angiogenesi).

Alcuni problemi in più: l’immunoterapia
Impatto significativo: Melanoma, Rene, Polmone, Vescica, LH, tumori con MSI


• Marked immune dysfunction driven by
immunosuppressive cell types, tumor
promoting immune cells and
inflammatory cells.
• A subset of immune cells has been
shown to support the growth of
pancreatic cancer cells.
• The ligand PD-L1 is upregulated
in pancreatic cancer and it may
explain the immunosuppression
present in this neoplasia.
• Tumors evade the immune
system by preventing the
presence of T cells and NK
cells (stroma, inflammatory
cytokines?)

TUMOURS CAN BE CATEGORISED INTO THREE TYPES ACCORDING
TO THE T CELL PATTERN ASSOCIATED WITH THE TUMOUR
IMMUNE DESERT CD8+ T cells absent from tumour and periphery Increase number of antigen-specific T cells or increase antigen presentation
IMMUNE EXCLUDED CD8+ T cells accumulated but not efficiently infiltrated Bring T cells in contact with cancer cells
INFLAMED CD8+ T cells infiltrated, but non-functional Accelerate or remove brakes on T cell response
MSS Majority of tumours don’t have T cells ► fail to respond to monotherapy with PD-L1/PD-1 inhibitors Kim and Chen. Ann Oncol 2016 Hegde et al. Clin Cancer Res 2016
MSI-high (5%) More likely to respond to monotherapy PD-L1/PD-1 pathway inhibitors
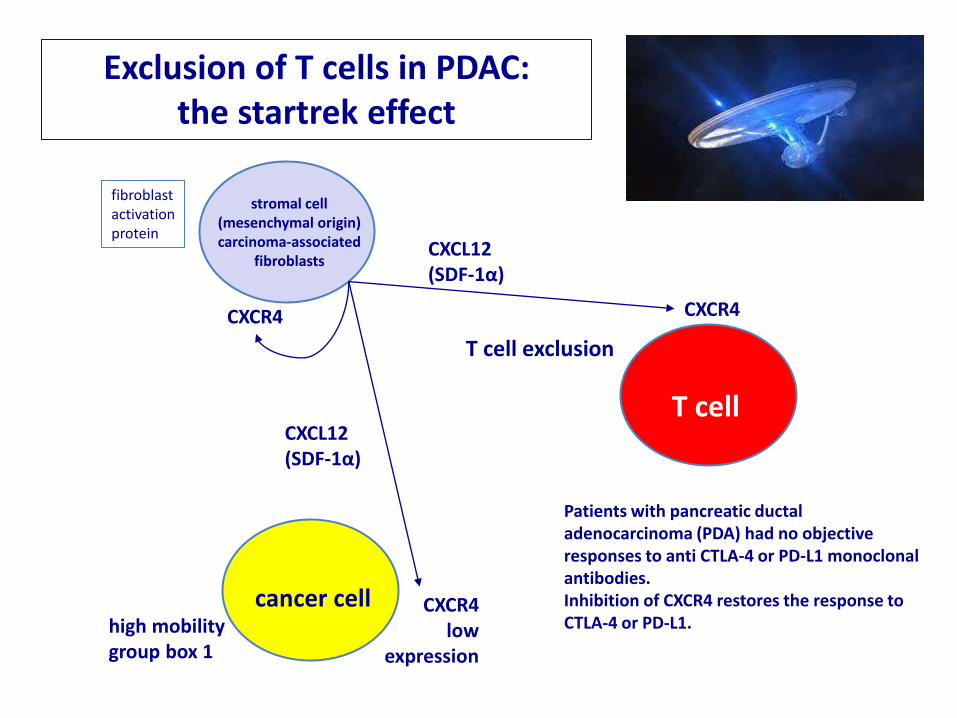
fibroblast activation protein
stromal cell (mesenchymal origin) carcinoma-associated
fibroblasts
cancer cell
T cell
CXCL12 (SDF-1α)
CXCR4
high mobility group box 1
Exclusion of T cells in PDAC: the startrek effect
T cell exclusion
CXCR4 low
expression
Patients with pancreatic ductal adenocarcinoma (PDA) had no objective responses to anti CTLA-4 or PD-L1 monoclonal antibodies. Inhibition of CXCR4 restores the response to CTLA-4 or PD-L1.
CXCL12 (SDF-1α)
CXCR4

Aspetti etici


Lo sviluppo delle tecnologie
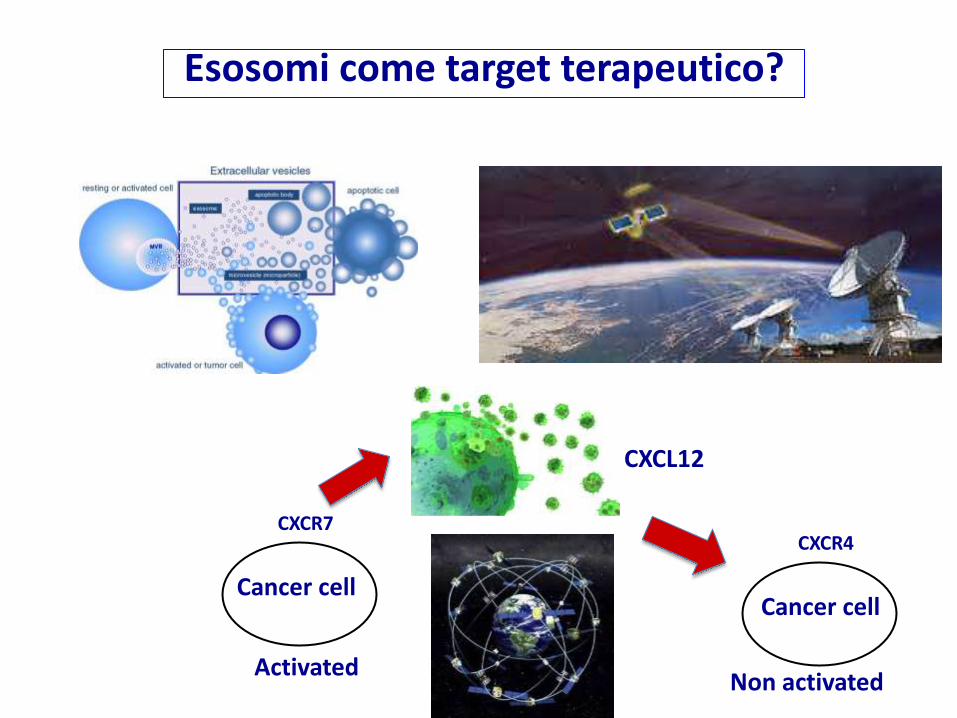
Cancer cell
CXCL12
CXCR4
Cancer cell
CXCR7
Esosomi come target terapeutico?
Activated Non activated