
2009 castel volturno, congresso sicoa regionale, l'ablazione della fibrillazione atriale
60
Responsabile: Stefano Nardi, MD, PhD L’ablazione transcatetere L’ablazione transcatetere della Fibrillazione della Fibrillazione Atriale: Atriale: Stato dell’arte Stato dell’arte “ “ AZIENDA OSPEDALIERA SANTA MARIA – TERNI” AZIENDA OSPEDALIERA SANTA MARIA – TERNI” DIPARTIMEN TO CARDIOTORACOVASCOLARE DIPARTIMEN TO CARDIOTORACOVASCOLARE STRUTTURA COMPLESSA DI CARDIOLOGIA STRUTTURA COMPLESSA DI CARDIOLOGIA CENTRO DI ARITMOLOGIA ED ELETTROFISIOLOGIA CARDIACA CENTRO DI ARITMOLOGIA ED ELETTROFISIOLOGIA CARDIACA
-
Upload
centro-diagnostico-nardi -
Category
Health & Medicine
-
view
40 -
download
5
Transcript of 2009 castel volturno, congresso sicoa regionale, l'ablazione della fibrillazione atriale
Responsabile: Stefano Nardi, MD, PhD
L’ablazione transcatetere L’ablazione transcatetere della Fibrillazione Atriale: della Fibrillazione Atriale:
Stato dell’arte Stato dell’arte
““AZIENDA OSPEDALIERA SANTA MARIA – TERNI”AZIENDA OSPEDALIERA SANTA MARIA – TERNI”DIPARTIMEN TO CARDIOTORACOVASCOLAREDIPARTIMEN TO CARDIOTORACOVASCOLARE
STRUTTURA COMPLESSA DI CARDIOLOGIASTRUTTURA COMPLESSA DI CARDIOLOGIACENTRO DI ARITMOLOGIA ED ELETTROFISIOLOGIA CARDIACA CENTRO DI ARITMOLOGIA ED ELETTROFISIOLOGIA CARDIACA
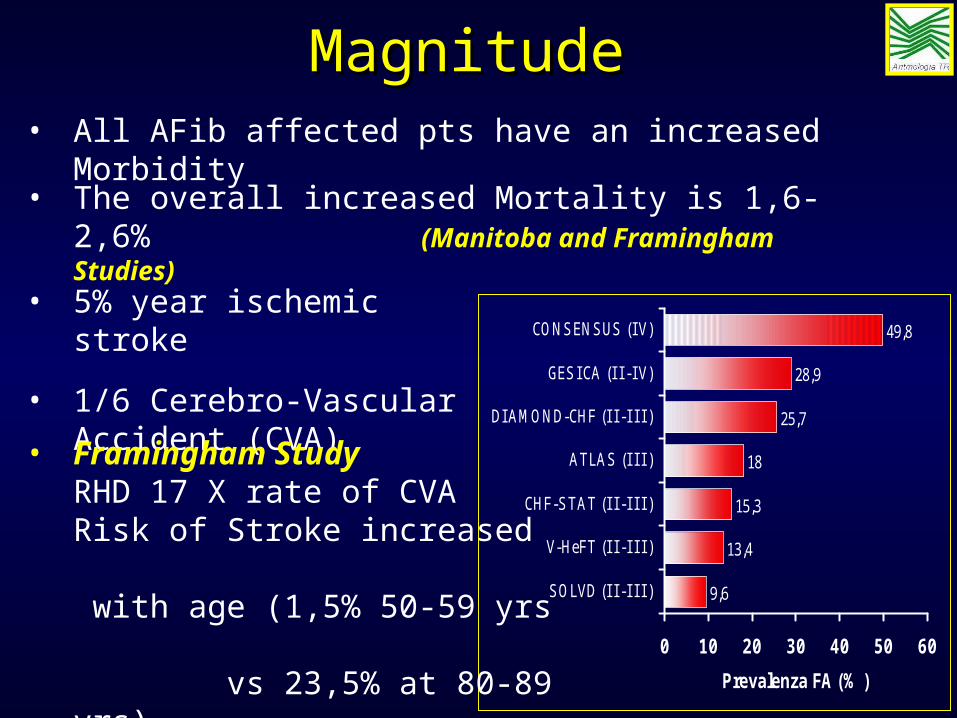
9,6
13,4
15,3
18
25,7
28,9
49,8
0 10 20 30 40 50 60
SOLVD (I I -I I I )
V-HeFT (I I -I I I )
CHF-STAT (I I -I I I )
ATLAS (I I I )
DI AMOND-CHF (I I -I I I )
GESI CA (I I -I V)
CONSENSUS (I V)
Prevalenza FA (% )
• All AFib affected pts have an increased Morbidity
• The overall increased Mortality is 1,6-2,6% (Manitoba and Framingham Studies)
• 5% year ischemic stroke
• 1/6 Cerebro-Vascular Accident (CVA)
• Framingham StudyRHD 17 X rate of CVA Risk of Stroke increased with age (1,5% 50-59 yrs vs 23,5% at 80-89 yrs)
MagnitudeMagnitude
AF and Congestive Heart AF and Congestive Heart FailureFailure
AF and Congestive Heart AF and Congestive Heart FailureFailure
• In the AMIOVIRT study AF resulted an In the AMIOVIRT study AF resulted an independent risk factor for mortality (RR 4) in pts independent risk factor for mortality (RR 4) in pts with CHF with CHF (Strickberger, J Am Coll Cardiol (Strickberger, J Am Coll Cardiol 2004)2004)
• In the AMIOVIRT study AF resulted an In the AMIOVIRT study AF resulted an independent risk factor for mortality (RR 4) in pts independent risk factor for mortality (RR 4) in pts with CHF with CHF (Strickberger, J Am Coll Cardiol (Strickberger, J Am Coll Cardiol 2004)2004)
• In the Analysis VEST study AF causes an increase In the Analysis VEST study AF causes an increase of 2.3 times the risk of death in patients with of 2.3 times the risk of death in patients with heart failure heart failure (Konety, AHA 1998)(Konety, AHA 1998)
• In the Analysis VEST study AF causes an increase In the Analysis VEST study AF causes an increase of 2.3 times the risk of death in patients with of 2.3 times the risk of death in patients with heart failure heart failure (Konety, AHA 1998)(Konety, AHA 1998)
• In the SOLVD study AF showed to be an In the SOLVD study AF showed to be an independent risk factor for mortality (RR 1.34) independent risk factor for mortality (RR 1.34) and progression of CHF (RR 1.42)and progression of CHF (RR 1.42)
(Vermes, Circulation 2003)(Vermes, Circulation 2003)
• In the SOLVD study AF showed to be an In the SOLVD study AF showed to be an independent risk factor for mortality (RR 1.34) independent risk factor for mortality (RR 1.34) and progression of CHF (RR 1.42)and progression of CHF (RR 1.42)
(Vermes, Circulation 2003)(Vermes, Circulation 2003)
• In the analysis AVID data, AF represents a risk In the analysis AVID data, AF represents a risk factor for the mortality in pts with VT/VF. factor for the mortality in pts with VT/VF. (D.G. (D.G. Wyse, AHA 1998)Wyse, AHA 1998)
• In the analysis AVID data, AF represents a risk In the analysis AVID data, AF represents a risk factor for the mortality in pts with VT/VF. factor for the mortality in pts with VT/VF. (D.G. (D.G. Wyse, AHA 1998)Wyse, AHA 1998)
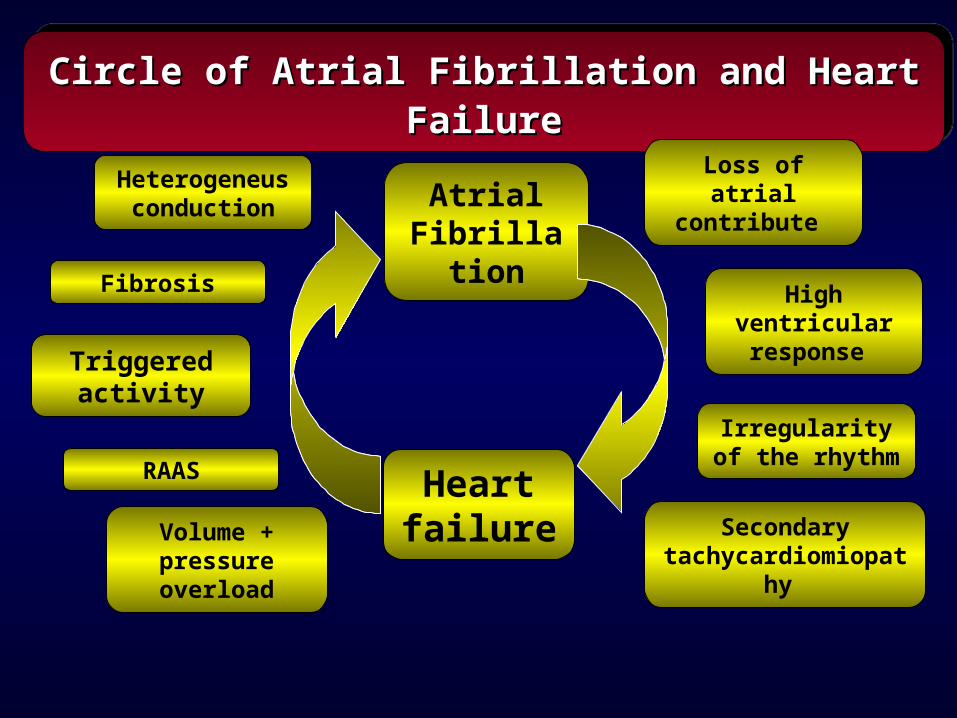
HeartfailureVolume +
pressure overload
RAAS
Triggeredactivity
AtrialFibrillati
on
Circle of Atrial Fibrillation and Heart Circle of Atrial Fibrillation and Heart FailureFailure
Circle of Atrial Fibrillation and Heart Circle of Atrial Fibrillation and Heart FailureFailure
Fibrosis
Heterogeneusconduction
Loss of atrial contribute
Irregularity of the rhythm
High ventricular response
Secondary tachycardiomiopa
thy
• AF reduces the cardiac performance because the loss of atrial contribute to the cardiac output
• The high ventricular response contributes to the cardiac output reduction
• The irregularity of the rhythm reduces itself by 15% the cardiac output.
• A secondary tachycardiomiopathy adds to a preexisting ventricular dysfuction.
• AF reduces the cardiac performance because the loss of atrial contribute to the cardiac output
• The high ventricular response contributes to the cardiac output reduction
• The irregularity of the rhythm reduces itself by 15% the cardiac output.
• A secondary tachycardiomiopathy adds to a preexisting ventricular dysfuction.
Atrial Fibrillation and Atrial Fibrillation and Congestive Heart FailureCongestive Heart Failure
Atrial Fibrillation and Atrial Fibrillation and Congestive Heart FailureCongestive Heart Failure
Preexisting LV
dysfunction
Preexisting LV
dysfunction
Further reduction of LV function
Further reduction of LV function
AAFFAAFF
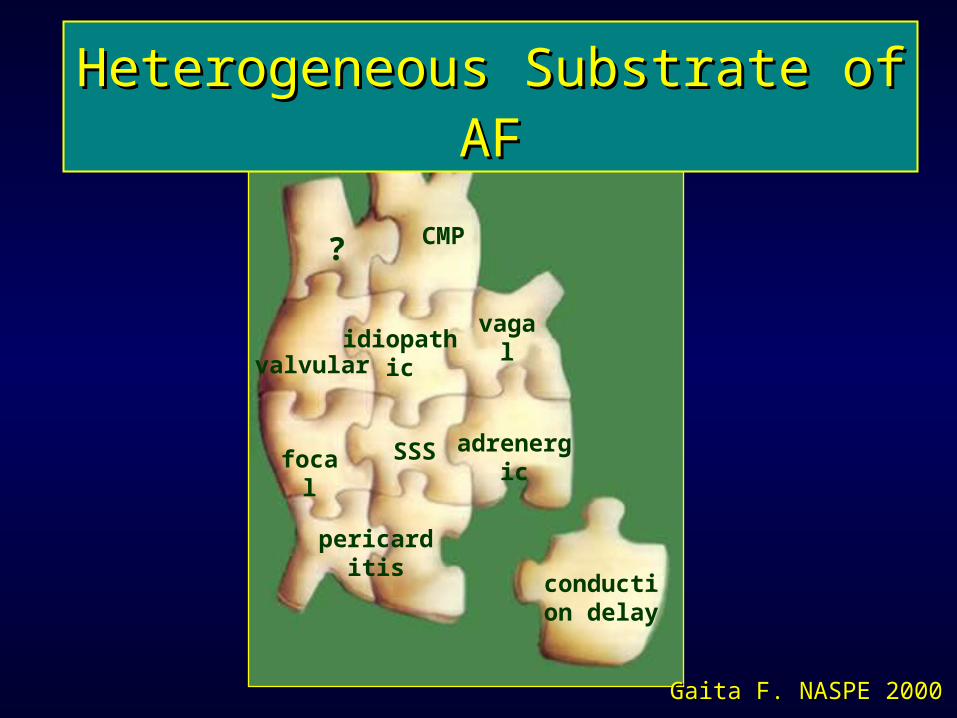
Heterogeneous Substrate of AFHeterogeneous Substrate of AF
CMP?
valvularidiopathic
vagal
focal SSS adrenergic
pericarditis
conduction delay
Gaita F. NASPE 2000Gaita F. NASPE 2000
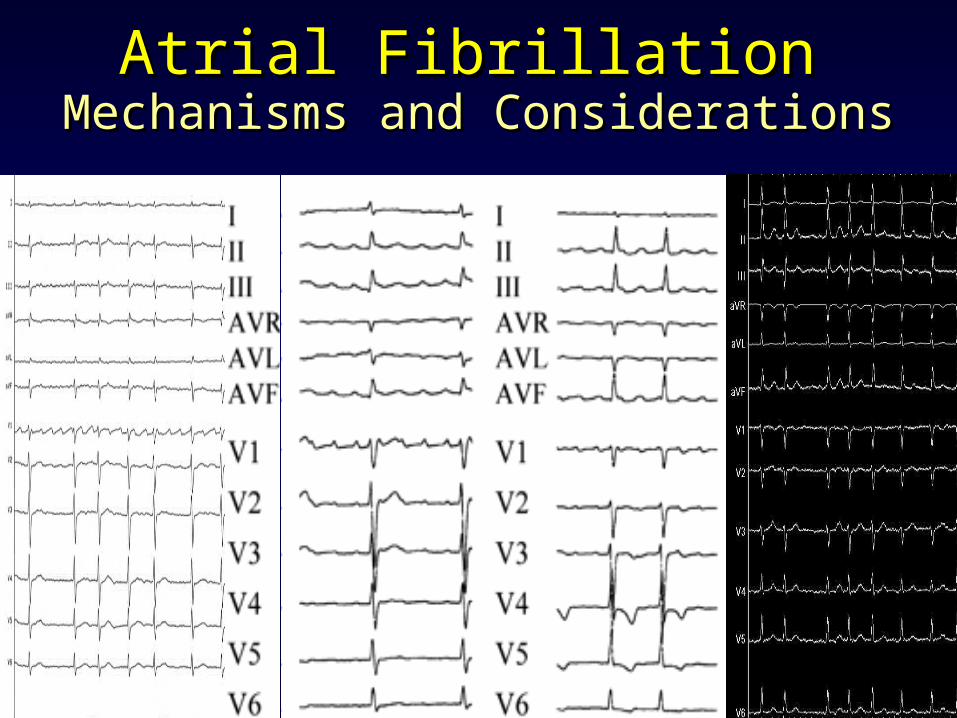
Atrial FibrillationAtrial FibrillationMechanisms and ConsiderationsMechanisms and Considerations
Atrial FibrillationAtrial FibrillationTherapeutic ApproachTherapeutic Approach
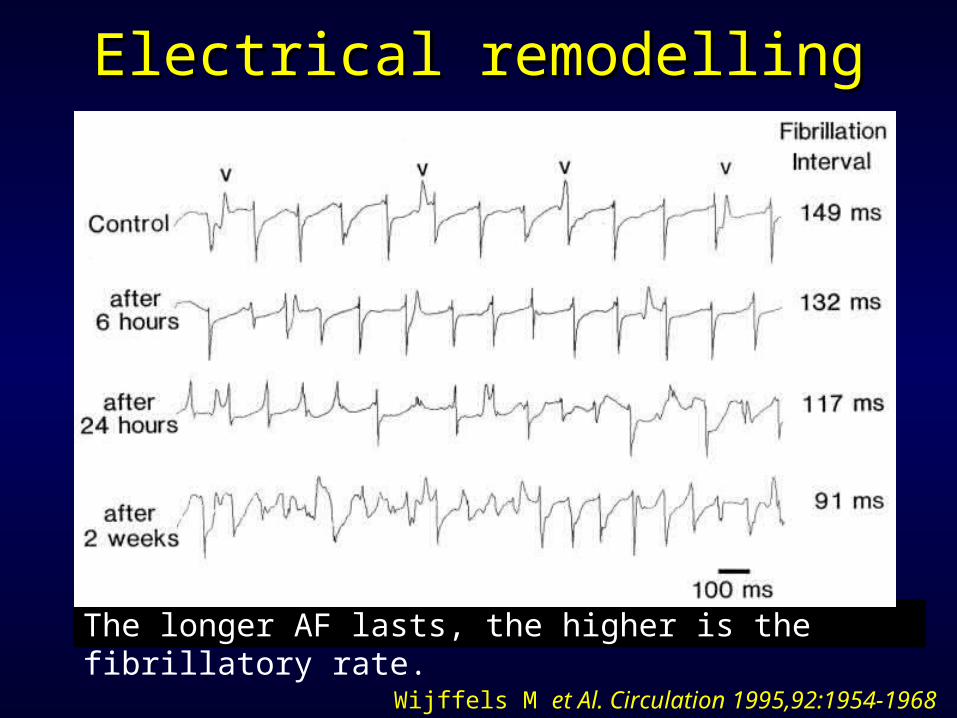
The longer AF lasts, the higher is the fibrillatory rate.
Wijffels M et Al. Circulation 1995,92:1954-1968
Electrical remodellingElectrical remodelling
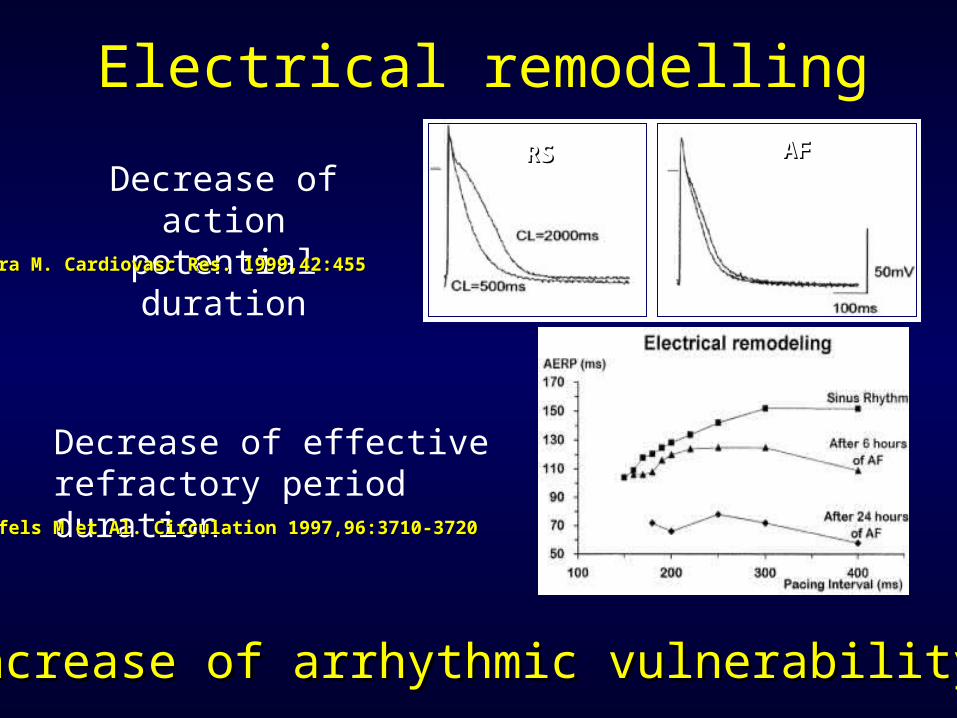
Electrical remodelling
Decrease of action potential duration
Increase of arrhythmic vulnerabilityIncrease of arrhythmic vulnerability
Decrease of effective refractory period duration
RSRS AFAF
Hara M. Cardiovasc Res. 1999,42:455Hara M. Cardiovasc Res. 1999,42:455
Wijffels M et Al. Circulation 1997,96:3710-3720Wijffels M et Al. Circulation 1997,96:3710-3720
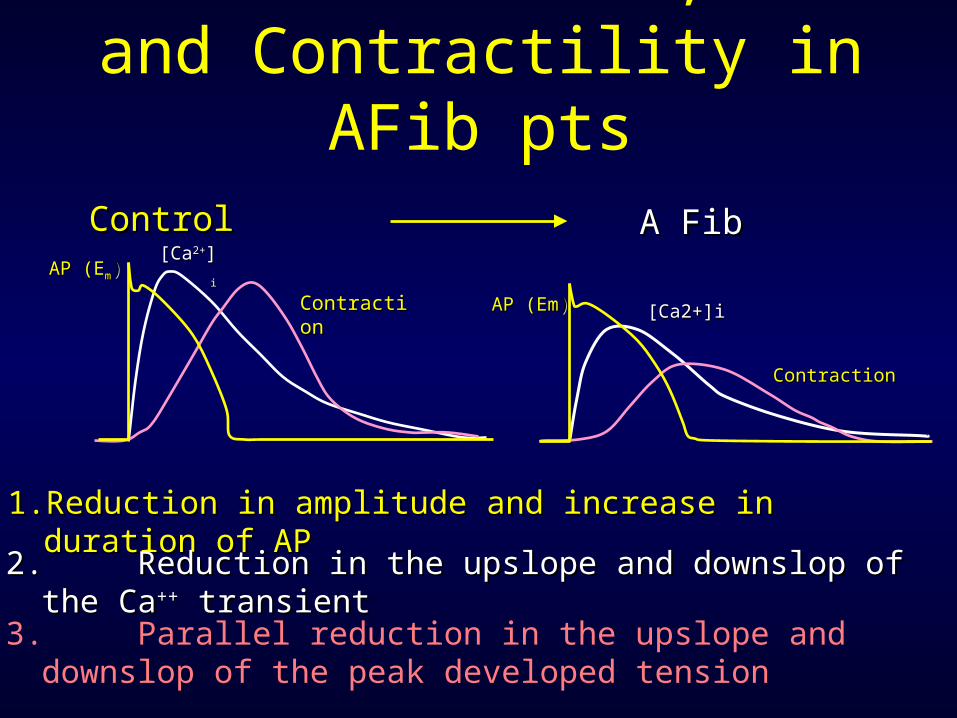
Action Potential, Ca++ and Contractility in AFib pts
1.1. Reduction in amplitude and increase in duration of Reduction in amplitude and increase in duration of APAP
Control Control A FibA FibAP (EAP (Emm))
[Ca[Ca2+2+]]ii
ContractioContractionn
2.2. Reduction in the upslope and downslop of the CaReduction in the upslope and downslop of the Ca++++ transienttransient
3. Parallel reduction in the upslope and downslop of the peak developed tension
ContractionContraction
[Ca2+]i[Ca2+]iAP (EmAP (Em))
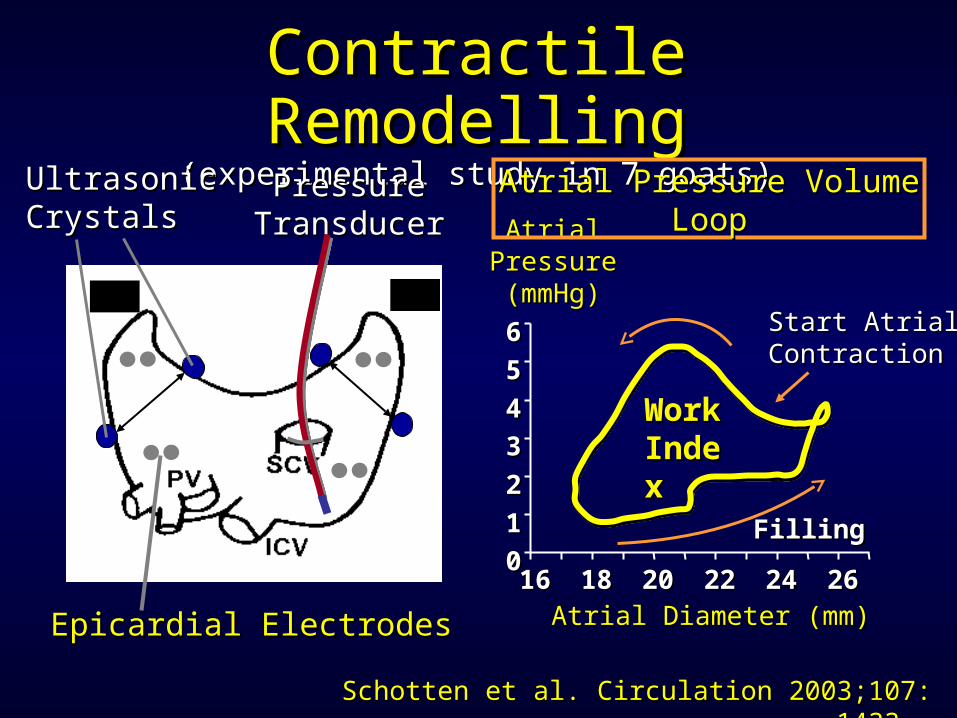
Contractile Contractile RemodellingRemodelling
(experimental study in 7 goats)(experimental study in 7 goats)Pressure Pressure TransducerTransducer
UltrasonicUltrasonicCrystalsCrystals
1616 1818 2020 2222 2424 262600
11
22
3344
55
66
AtrialAtrialPressurePressure(mmHg)(mmHg)
Atrial Atrial DDiameter (mm)iameter (mm)
Start AtrialStart AtrialContractionContraction
Atrial Pressure Volume Atrial Pressure Volume LoopLoop
FillingFilling
Epicardial ElectrodesEpicardial Electrodes
Schotten et al. Circulation 2003Schotten et al. Circulation 2003;107: 1433.;107: 1433.
WorkWorkIndexIndex
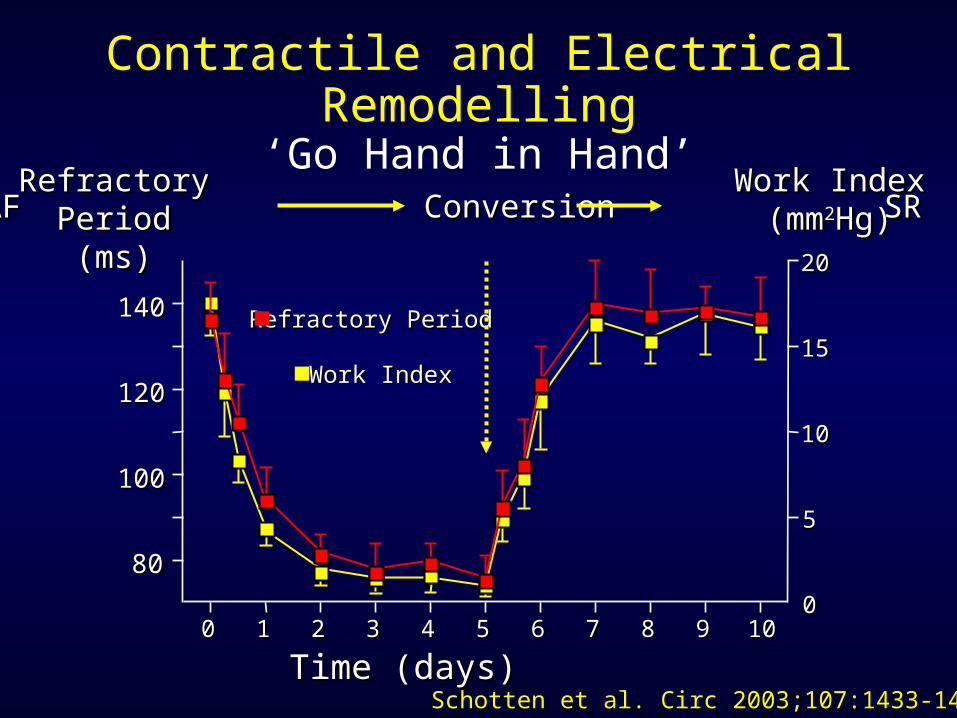
Contractile and Electrical Remodelling‘Go Hand in Hand’
00 11 22 33 44 55 66 77 88 99 1010
8080
100100
120120
140140 Refractory Refractory PPerioderiod
Work Work IIndexndex
00
55
1010
1515
2020
RefractoryRefractoryPeriodPeriod(ms)(ms)
Work Work IIndexndex(mm(mm22Hg)Hg)
Time (days)Time (days)
AF Conversion SR AF Conversion SR
Schotten et al. Circ 2003;Schotten et al. Circ 2003;107:1433-1439107:1433-1439
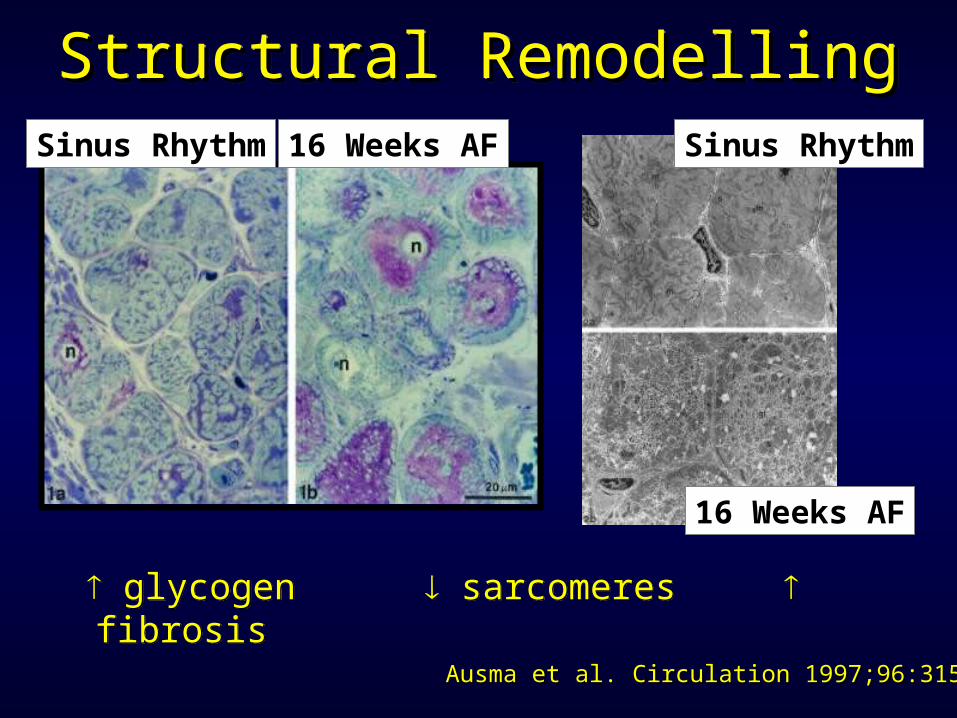
Structural RemodellingStructural RemodellingStructural RemodellingStructural RemodellingSinus Rhythm16 Weeks AF
Ausma et al. Circulation Ausma et al. Circulation 1997;96:3157 1997;96:3157
glycogen sarcomeres fibrosis glycogen sarcomeres fibrosis
Sinus Rhythm
16 Weeks AF
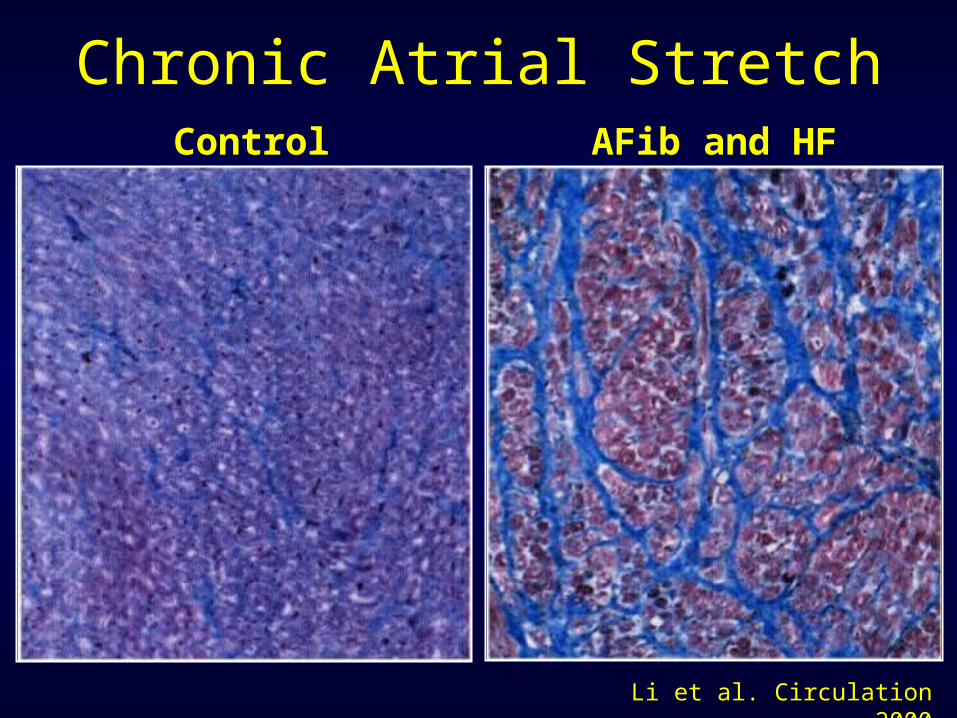
Li et al. Circulation 2000Li et al. Circulation 2000
Chronic Atrial StretchControl AFib and HF
“l’importanza di TROVARE il bandolo della matassa
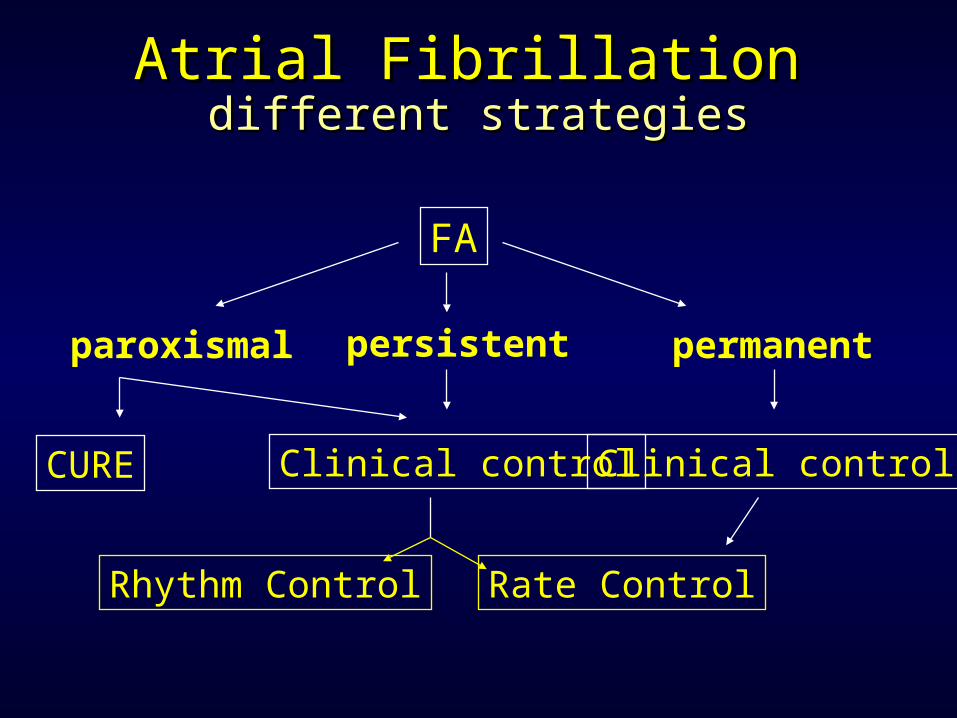
FA
CURE Clinical control
Rate ControlRhythm Control
Clinical control
paroxismal permanentpersistent
Atrial FibrillationAtrial Fibrillationdifferent strategiesdifferent strategies
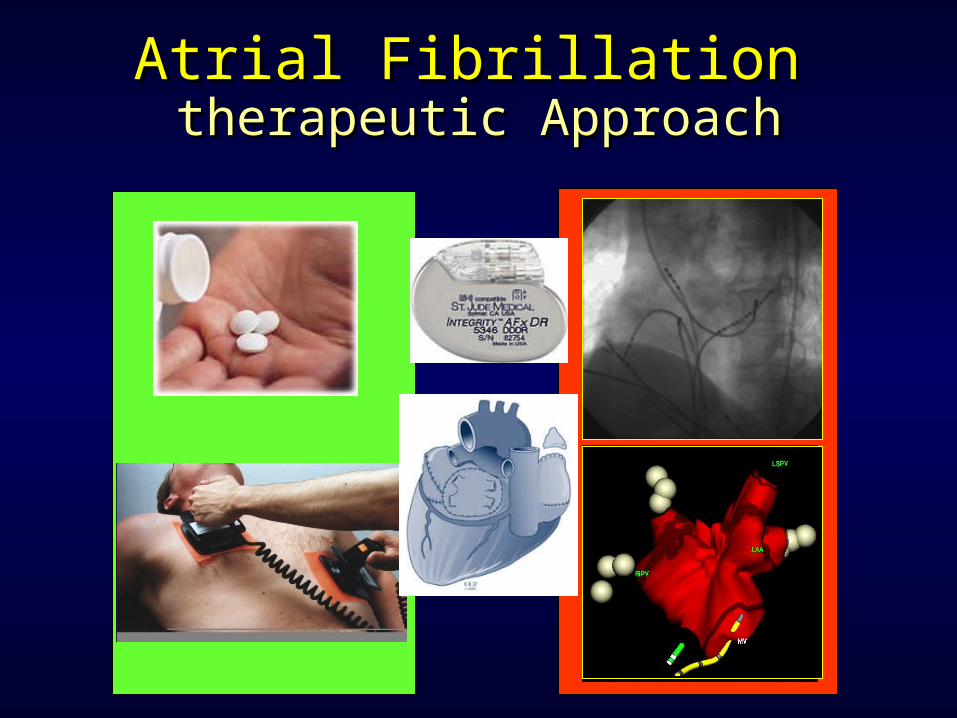
therapeutic Approachtherapeutic ApproachAtrial FibrillationAtrial Fibrillation
AFFIRM STAFSTAF
PIAPIAFF
HOT CAFÉHOT CAFÉ
PAF-PAF-22
RACRACEE
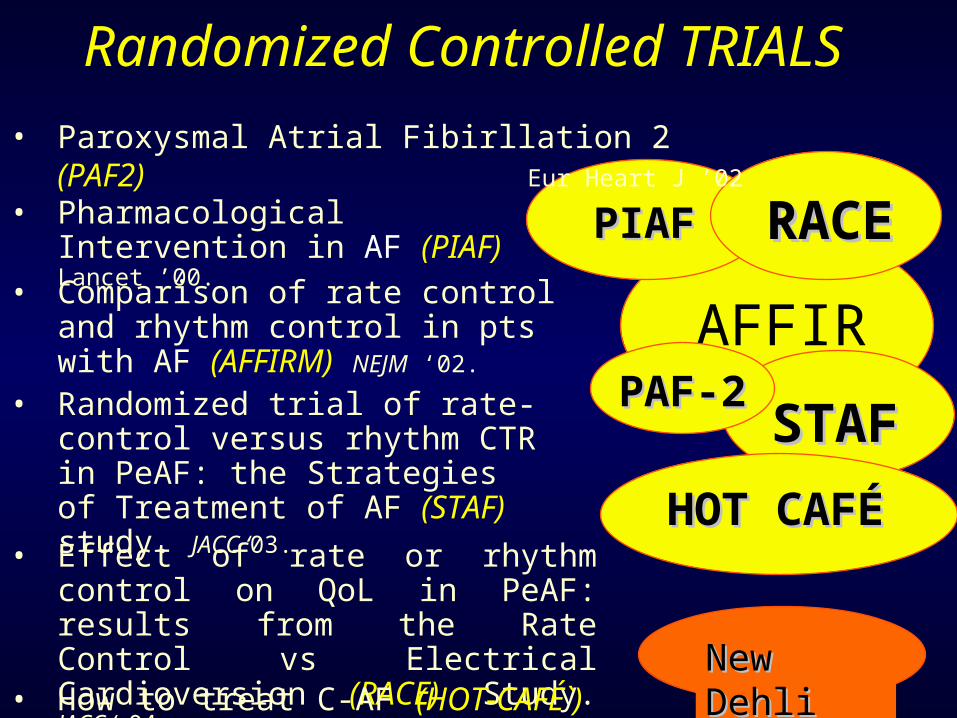
Randomized Controlled TRIALS• Paroxysmal Atrial Fibirllation 2 (PAF2)
Eur Heart J ’02
• Pharmacological Intervention in AF (PIAF) Lancet ’00.• Comparison of rate control and rhythm control in pts with AF (AFFIRM) NEJM ‘02.
• Randomized trial of rate-control versus rhythm CTR in PeAF: the Strategies of Treatment of AF (STAF) study. JACC ‘03.
• Effect of rate or rhythm control on QoL in PeAF: results from the Rate Control vs Electrical Cardioversion (RACE) Study. JACC ‘ 04.• How to treat C-AF (HOT-CAFÉ`)
New New DehliDehli
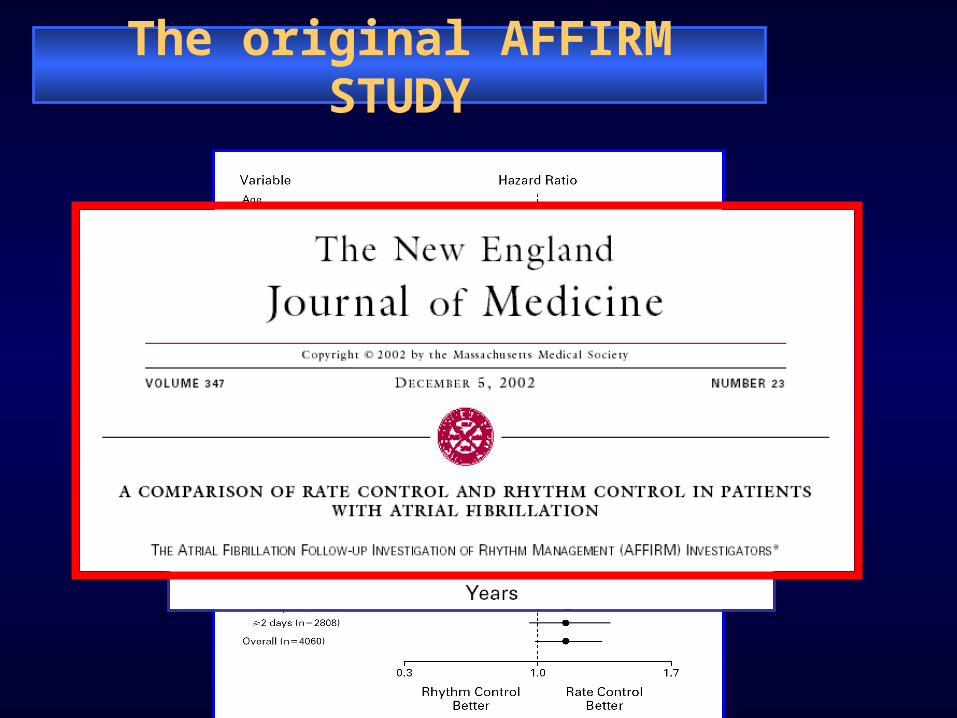
The original AFFIRM STUDY
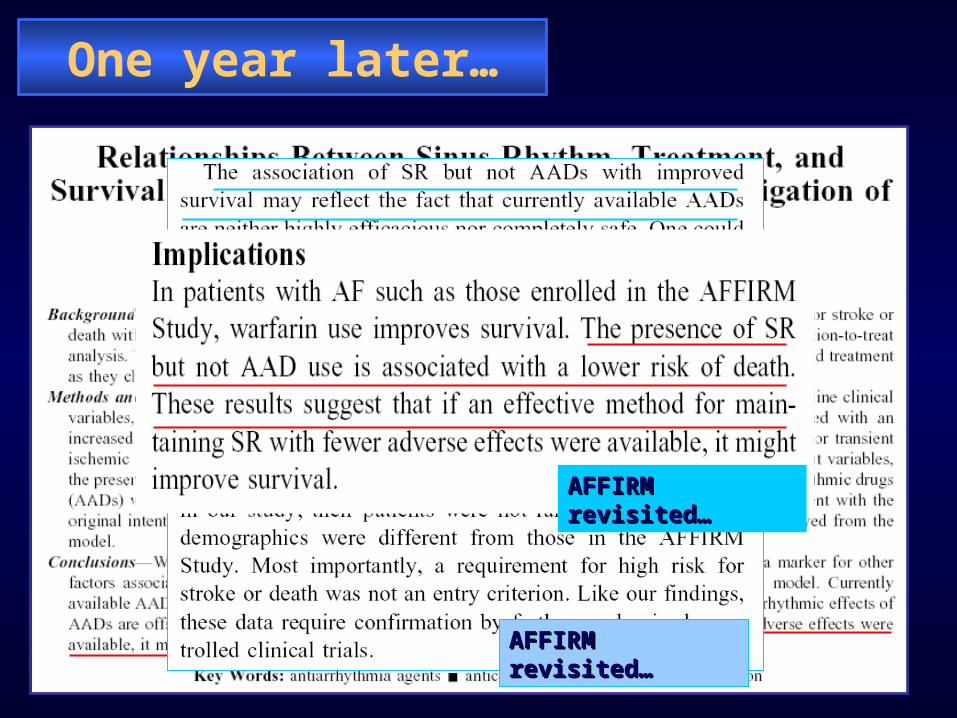
One year later…
AFFIRM revisited…AFFIRM revisited…
AFFIRM revisited…AFFIRM revisited…
AFFIRM revisited…AFFIRM revisited…
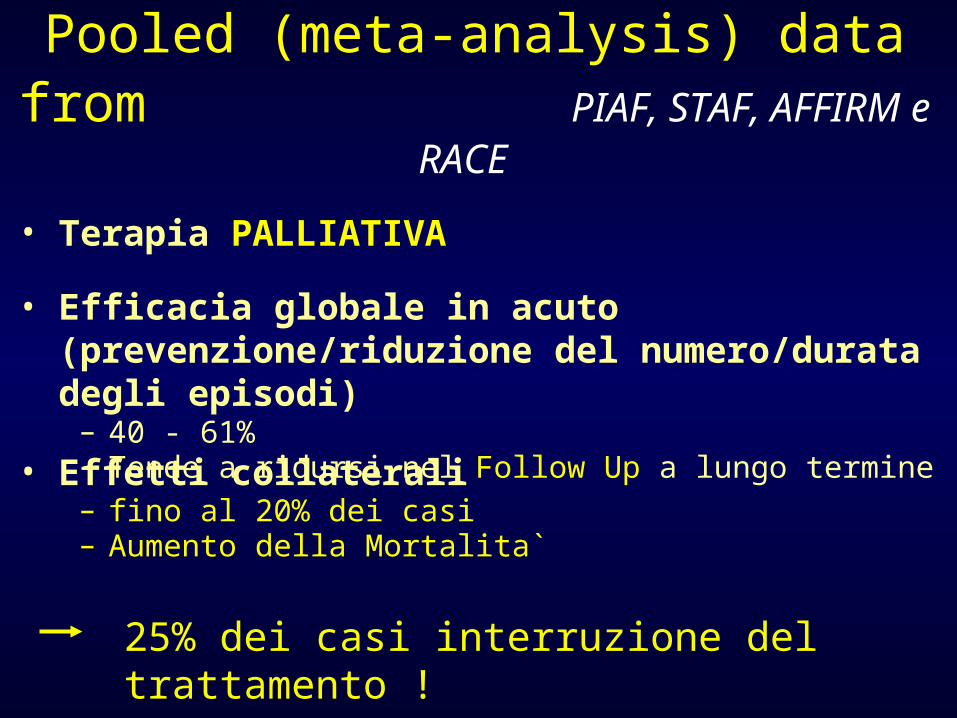
• Terapia PALLIATIVA
• Effetti collaterali– fino al 20% dei casi– Aumento della Mortalita`
25% dei casi interruzione del trattamento !
• Efficacia globale in acuto (prevenzione/riduzione del numero/durata degli episodi)
– 40 - 61%– Tende a ridursi nel Follow Up a lungo termine
Pooled (meta-analysis) data from PIAF, STAF,
AFFIRM e RACE
It’s really important to use the appropriate technique
for AF ablation
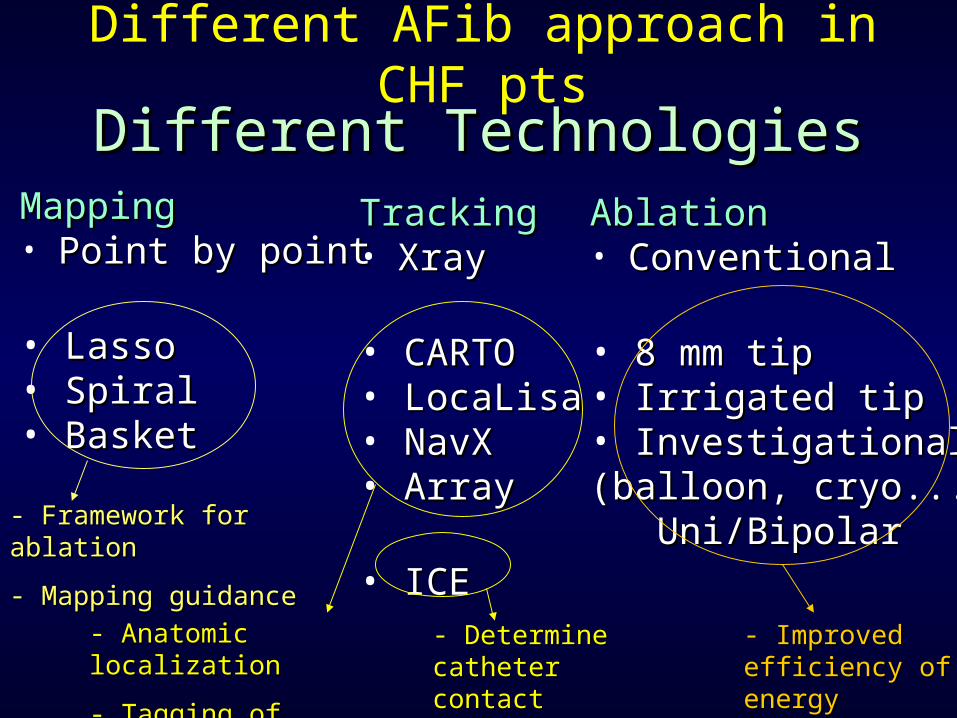
Different TechnologiesDifferent TechnologiesMappingMapping• Point by pointPoint by point
• LassoLasso• SpiralSpiral• BasketBasket
TrackingTracking• XrayXray
• CARTOCARTO• LocaLisaLocaLisa• NavXNavX• ArrayArray
• ICEICE
AblationAblation• ConventionalConventional
• 8 mm tip8 mm tip• Irrigated tipIrrigated tip• InvestigationalInvestigational(balloon, cryo...)(balloon, cryo...) Uni/BipolarUni/Bipolar- Framework for ablationFramework for ablation
- Mapping guidanceMapping guidance
- Anatomic localizationAnatomic localization
- Tagging of ablation - Tagging of ablation sitessites
- Determine Determine catheter contactcatheter contact
- Improved Improved efficiency of efficiency of energy deliveryenergy delivery
Different AFib approach in CHF pts
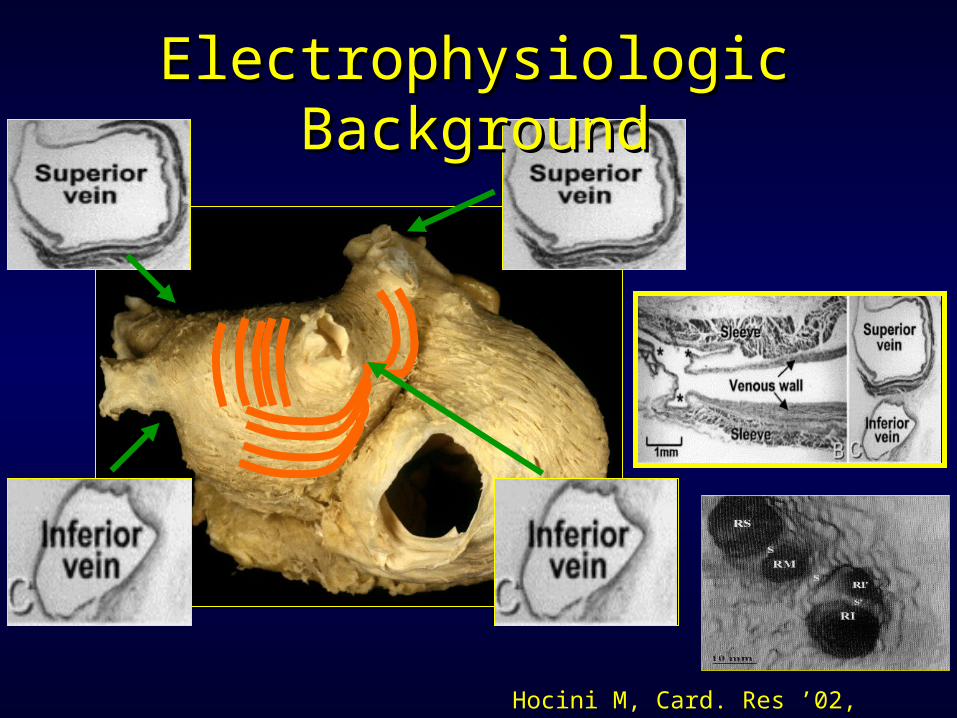
Hocini M, Card. Res ’02, Circulation ‘02
Electrophysiologic Electrophysiologic BackgroundBackground
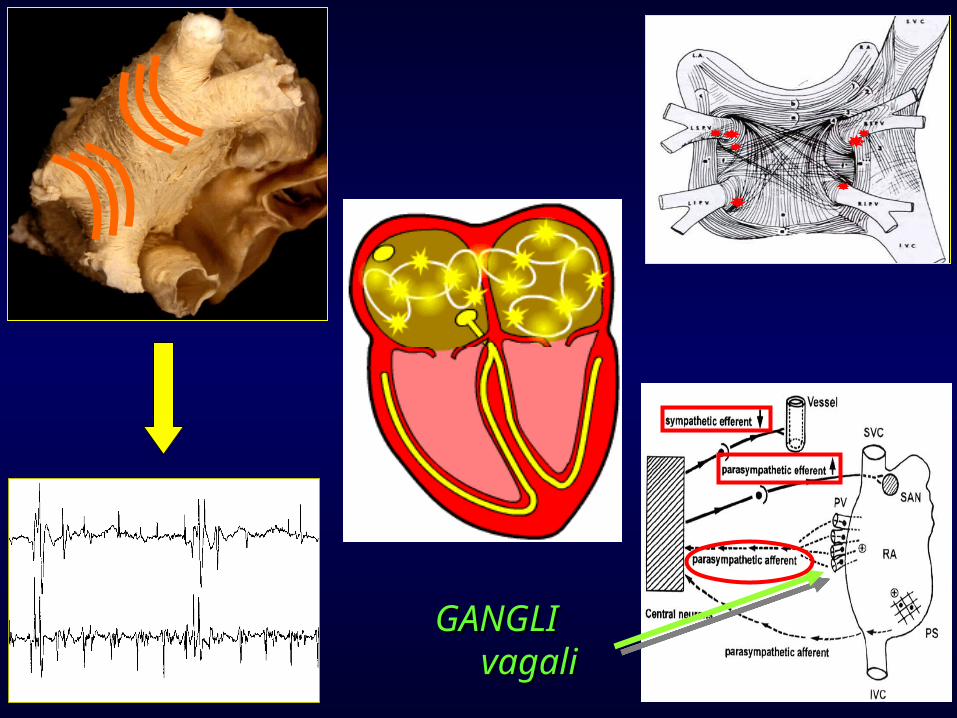
GANGLI GANGLI vagali vagali
RF
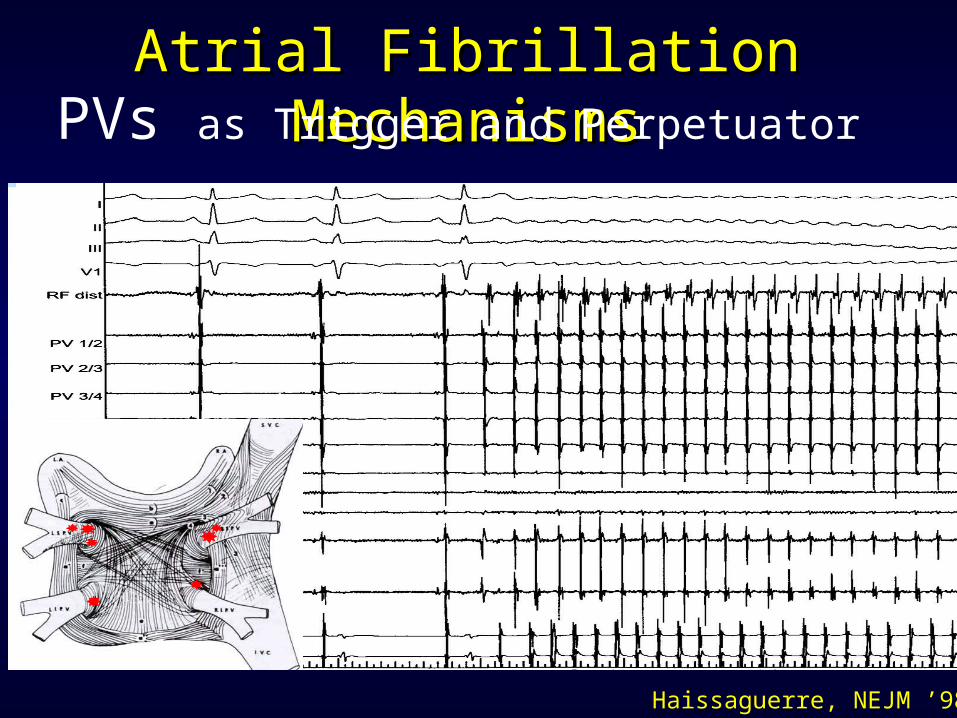
Haissaguerre, NEJM ’98
Atrial Fibrillation MechanismsAtrial Fibrillation MechanismsPVs as Trigger and Perpetuator
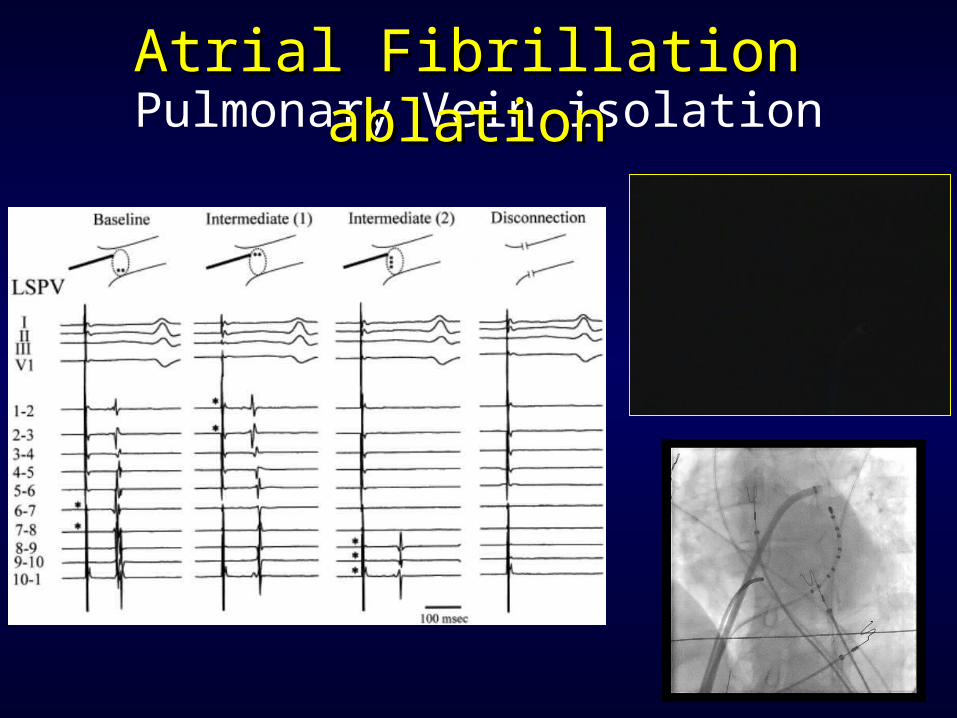
Pulmonary Vein isolationAtrial Fibrillation ablationAtrial Fibrillation ablation

Inferomediale
Infero-laterale
VPIL
VPSL
Fluoroscopic X ray
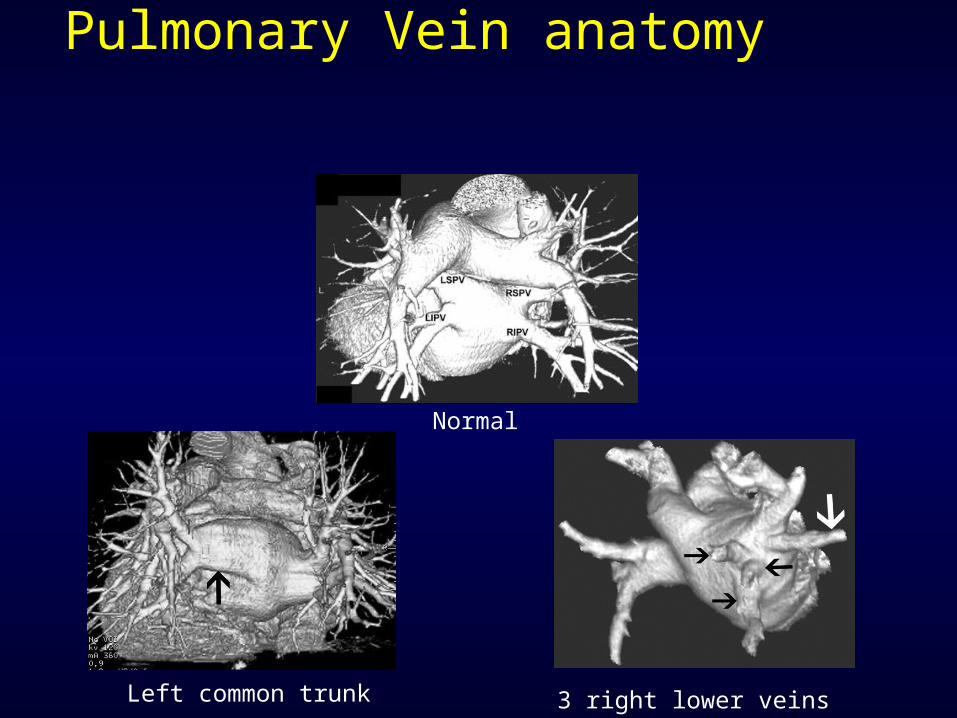
Left common trunk 3 right lower veins
Normal
Pulmonary Vein anatomy
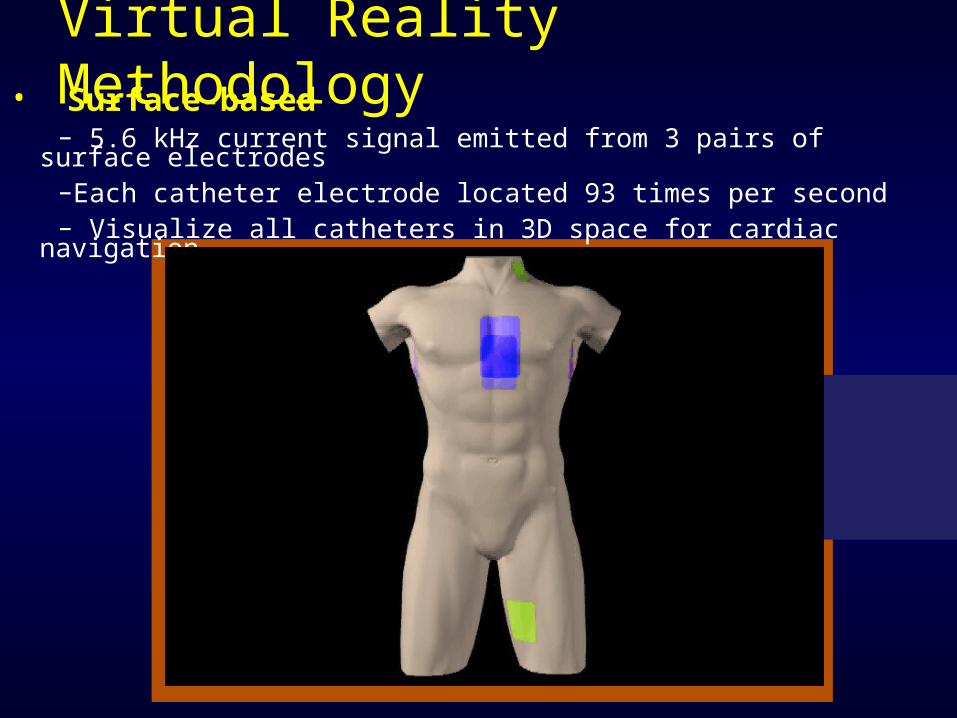
• Surface-based– 5.6 kHz current signal emitted from 3 pairs of surface
electrodes–Each catheter electrode located 93 times per second– Visualize all catheters in 3D space for cardiac navigation
Virtual Reality Methodology
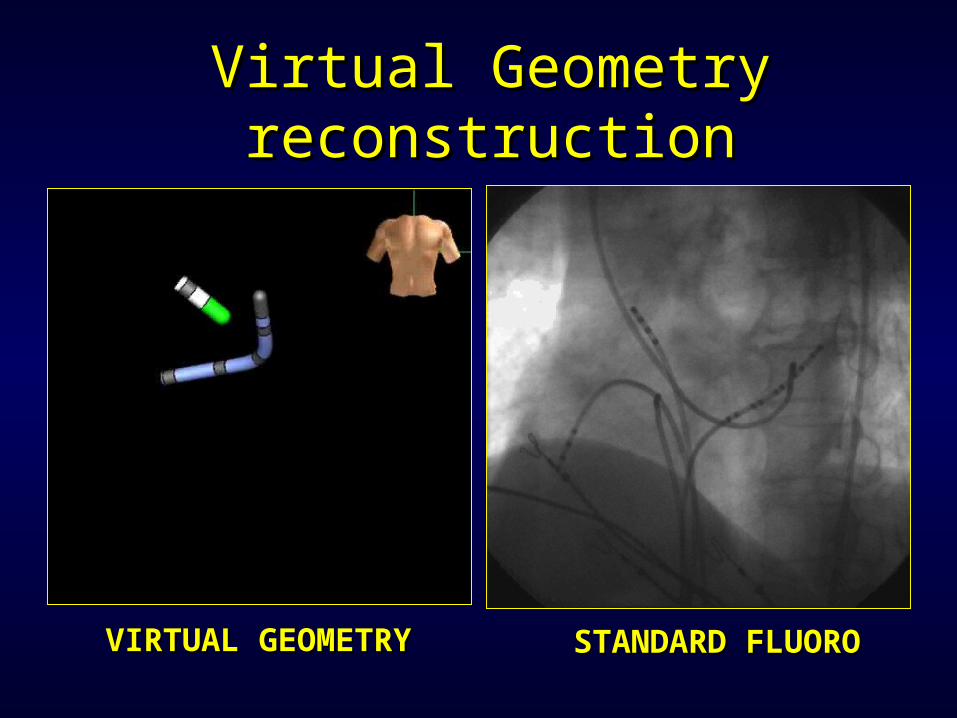
STANDARD FLUOROSTANDARD FLUOROVIRTUAL GEOMETRYVIRTUAL GEOMETRY
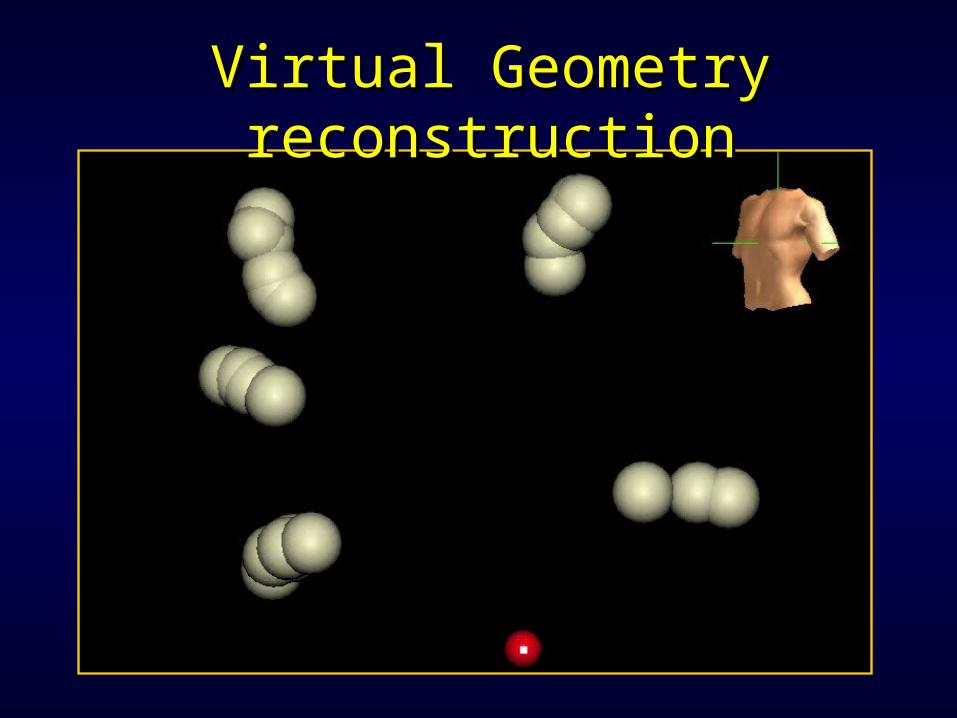
Virtual Geometry Virtual Geometry reconstructionreconstruction
Point-by-Point
Medium-Low
Virtual Geometry Virtual Geometry reconstructionreconstruction
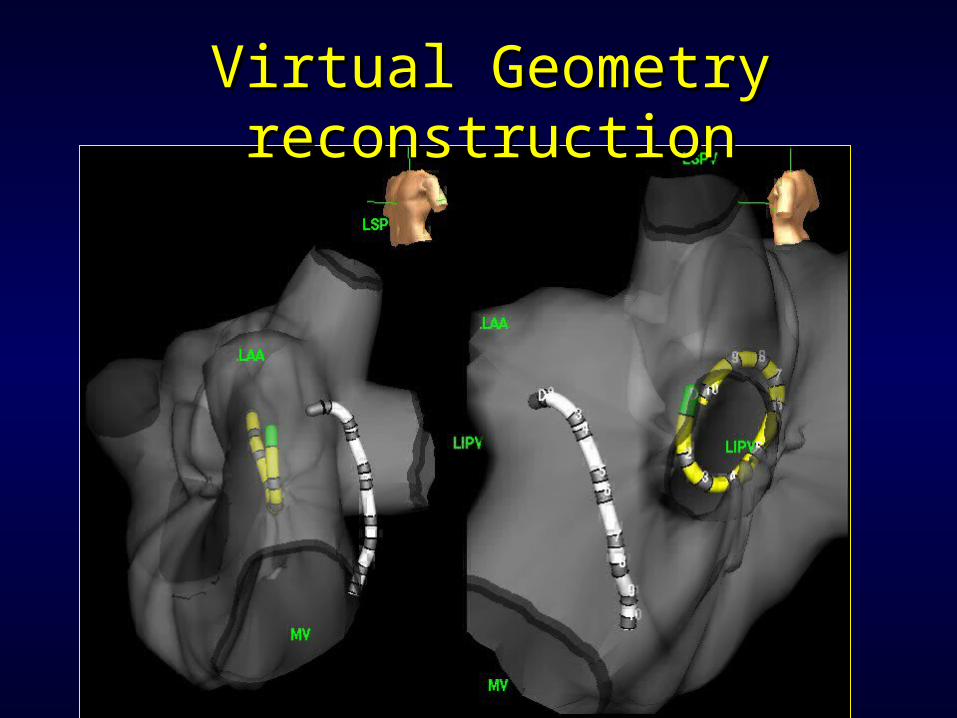
Virtual Geometry Virtual Geometry reconstructionreconstruction
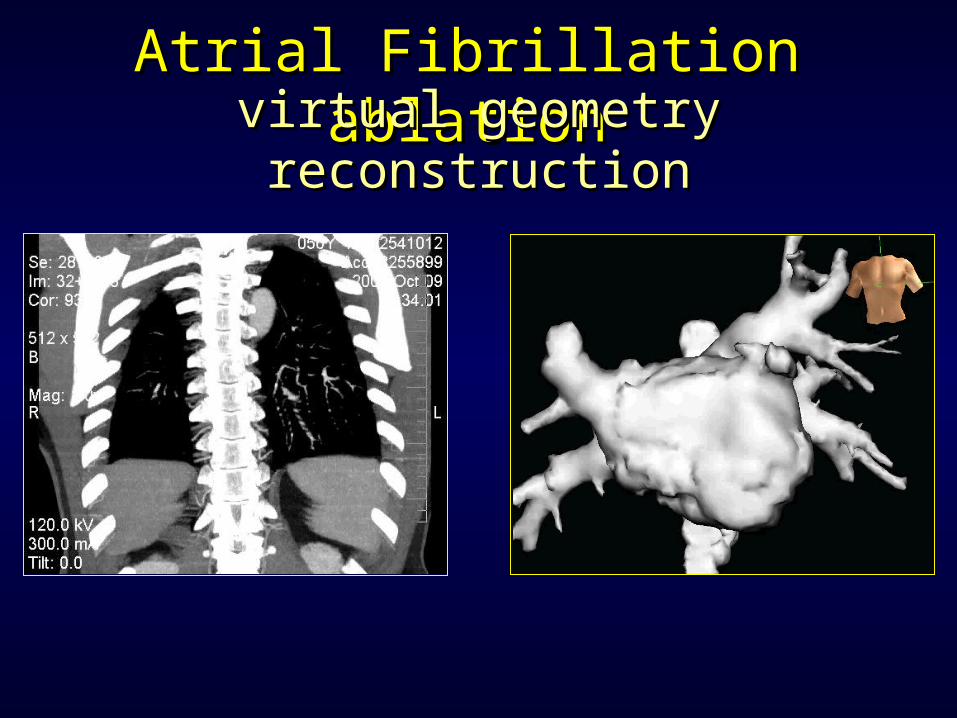
Atrial Fibrillation ablationAtrial Fibrillation ablationvirtual geometry reconstructionvirtual geometry reconstruction
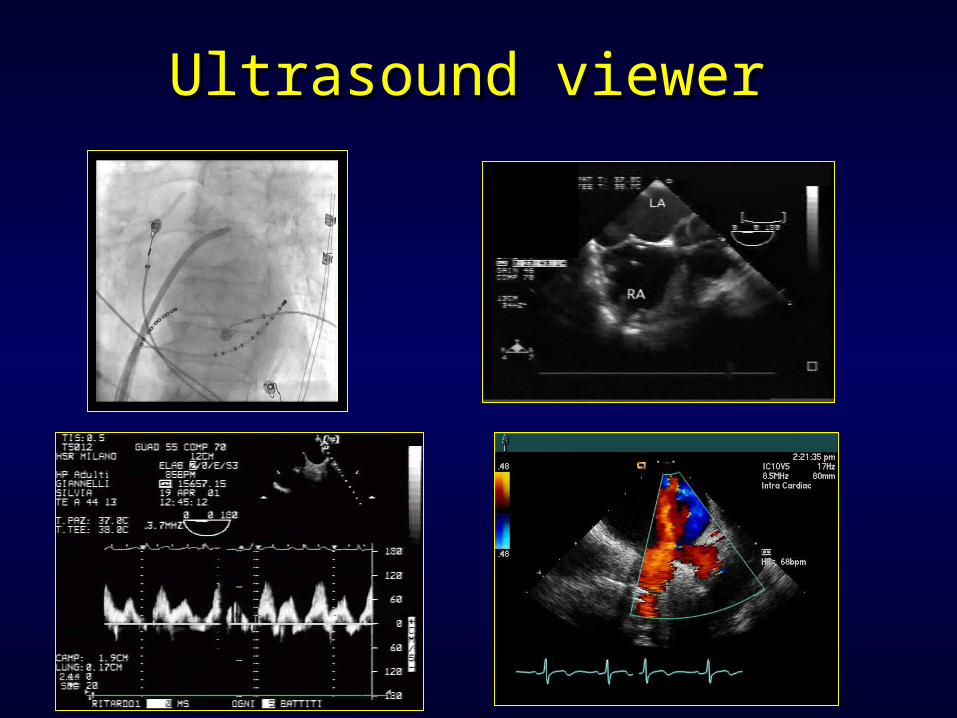
Ultrasound viewerUltrasound viewer
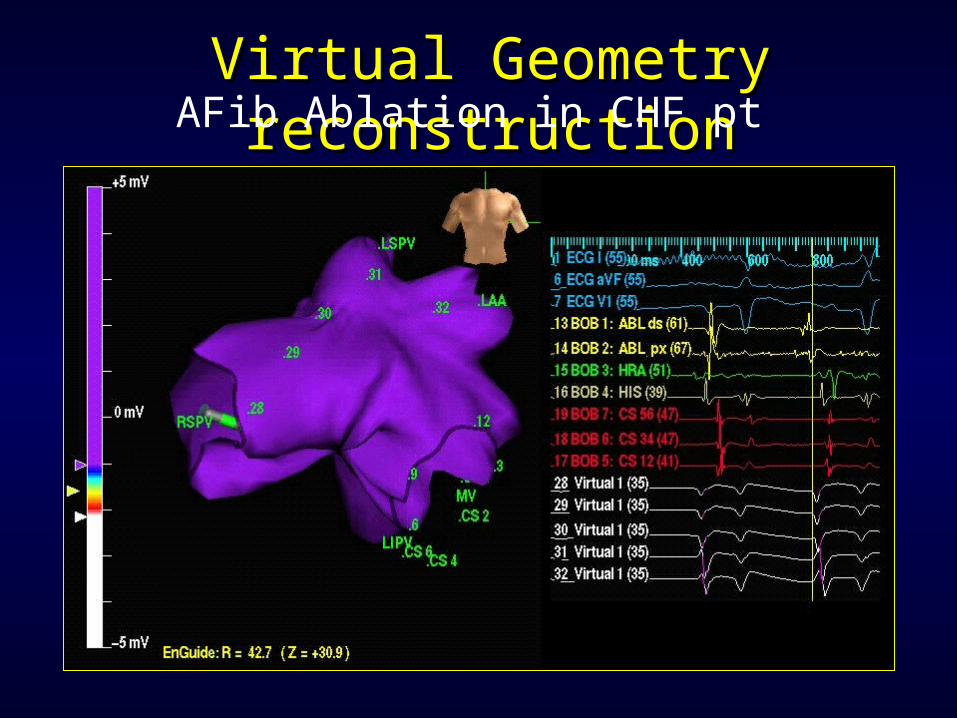
Virtual Geometry Virtual Geometry reconstructionreconstructionAFib Ablation in CHF pt
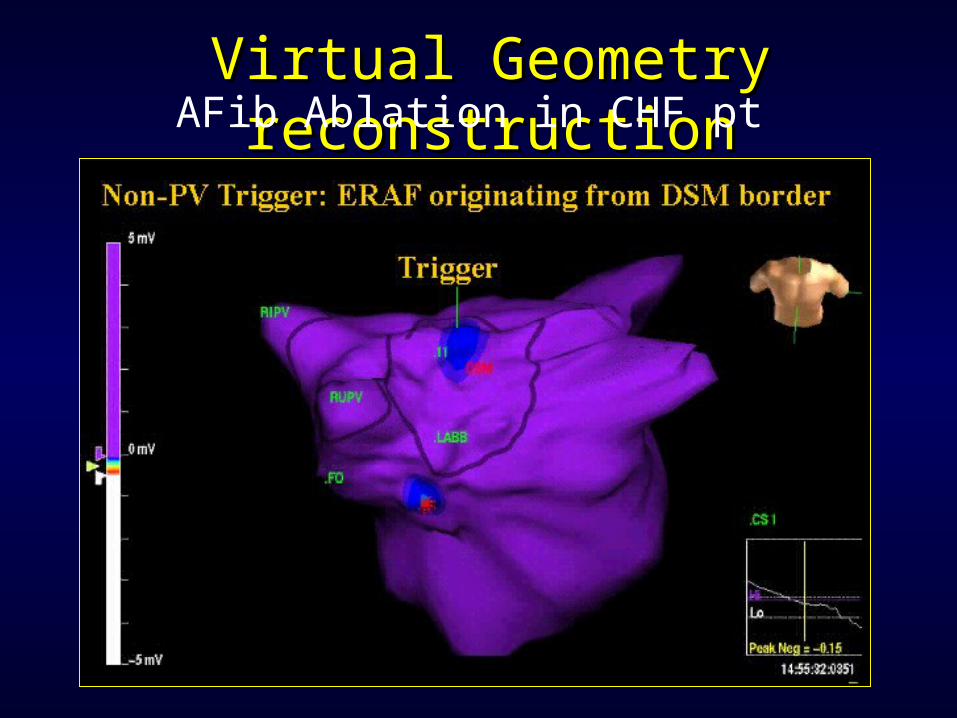
Virtual Geometry Virtual Geometry reconstructionreconstructionAFib Ablation in CHF pt
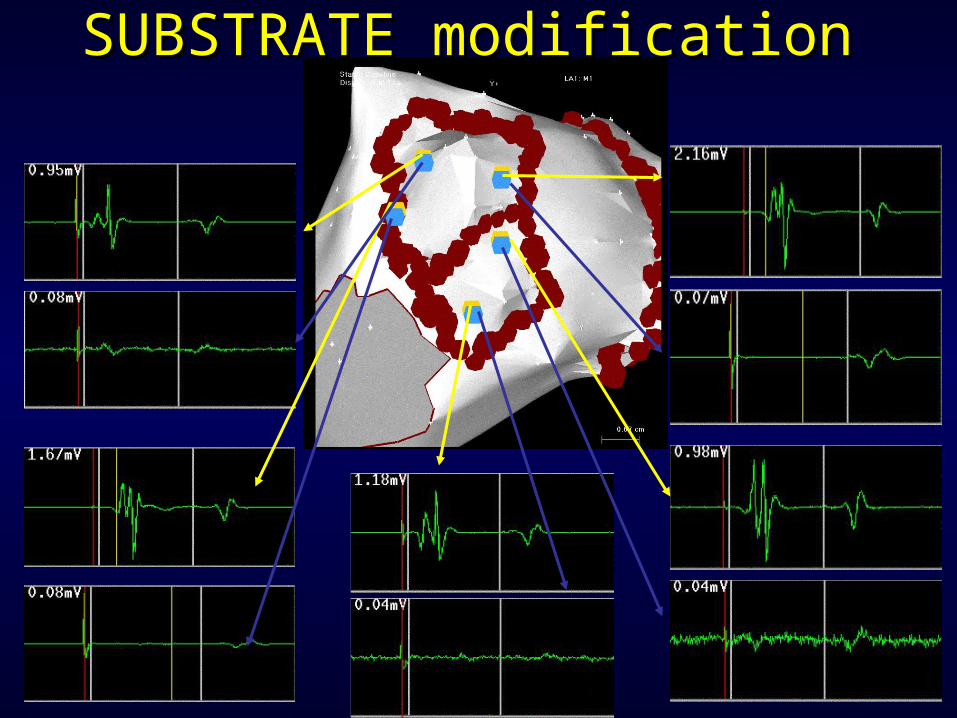
SUBSTRATE modificationSUBSTRATE modification
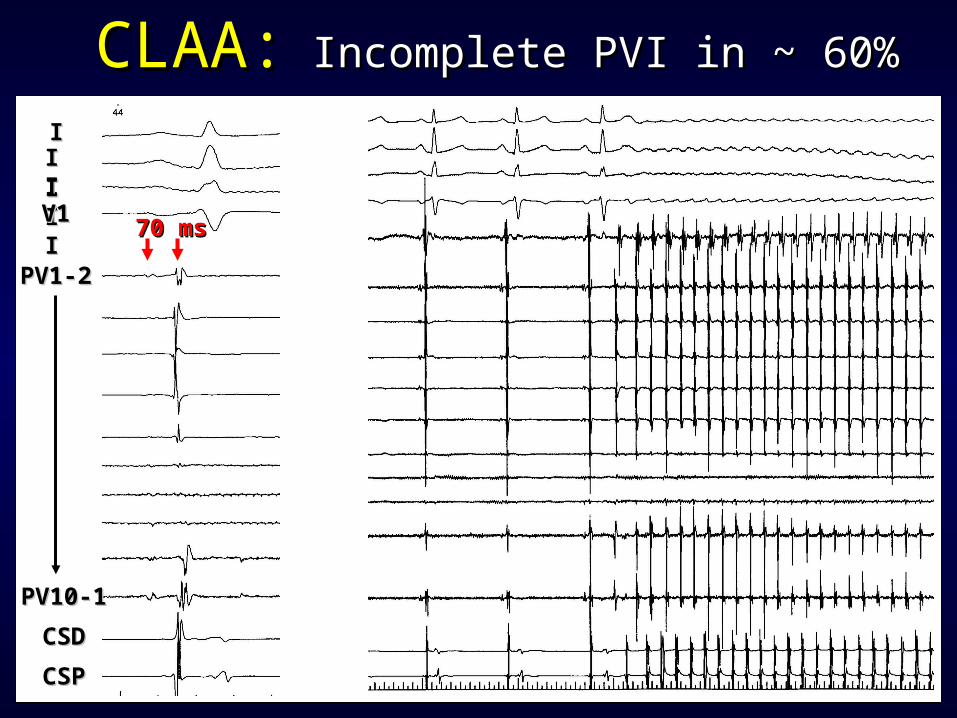
CLAA:CLAA: Incomplete PVI in ~ 60%Incomplete PVI in ~ 60%
70 ms70 ms
IIIIIIIIIIIIV1V1
PV1-2PV1-2
PV10-1PV10-1
CSDCSD
CSPCSP
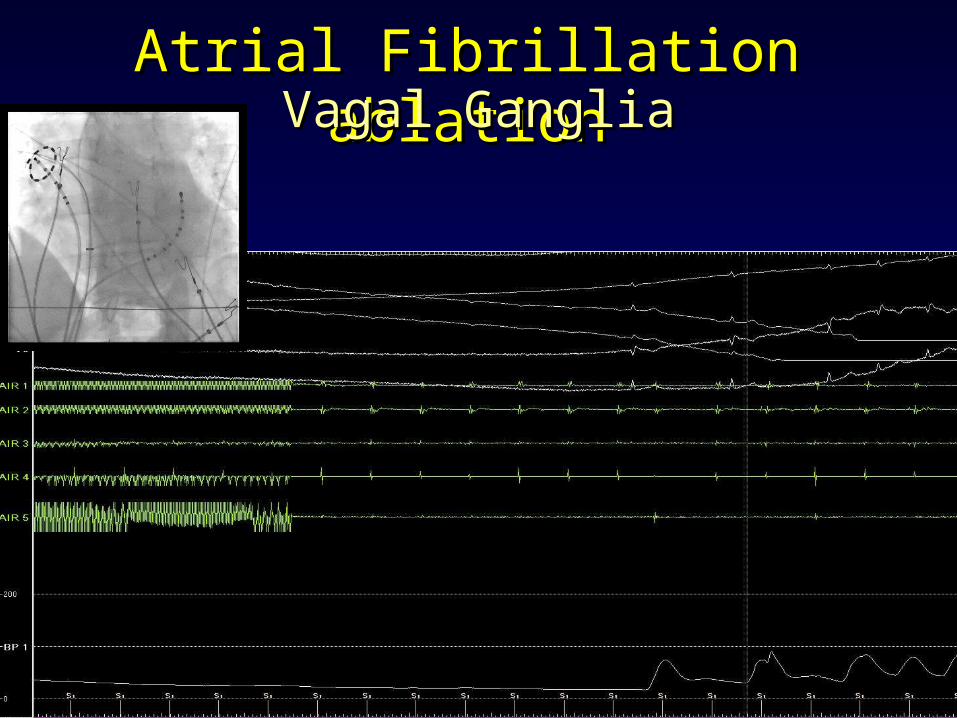
Atrial Fibrillation ablationAtrial Fibrillation ablationVagal GangliaVagal Ganglia
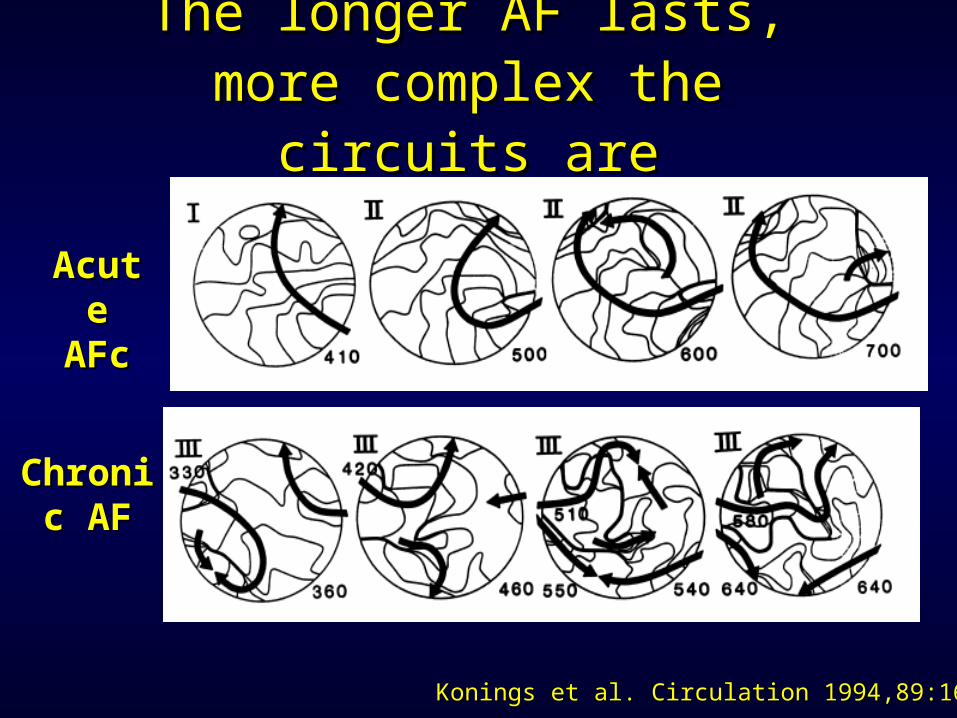
The longer AF lasts, more The longer AF lasts, more complex the circuits arecomplex the circuits are
AcutAcute e
AFcAFc
ChroniChronic AFc AF
Konings et al. Circulation 1994,89:1665Konings et al. Circulation 1994,89:1665
F. Gaita et al. JACC 2001;37:534F. Gaita et al. JACC 2001;37:534
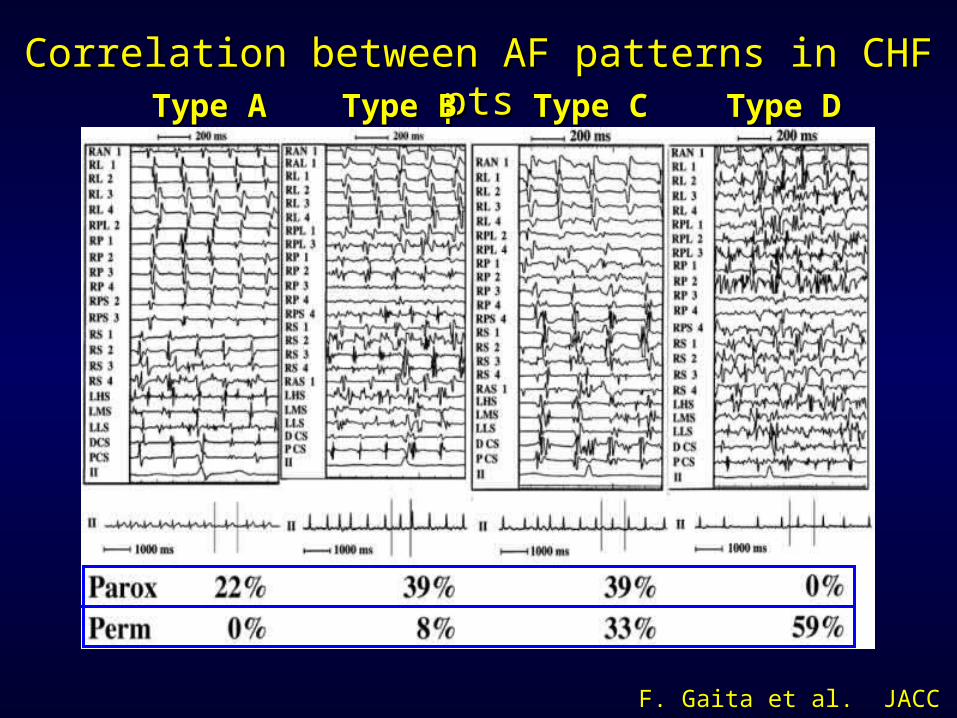
Correlation between AF patterns in CHF ptsCorrelation between AF patterns in CHF ptsType BType BType AType A Type DType DType CType C
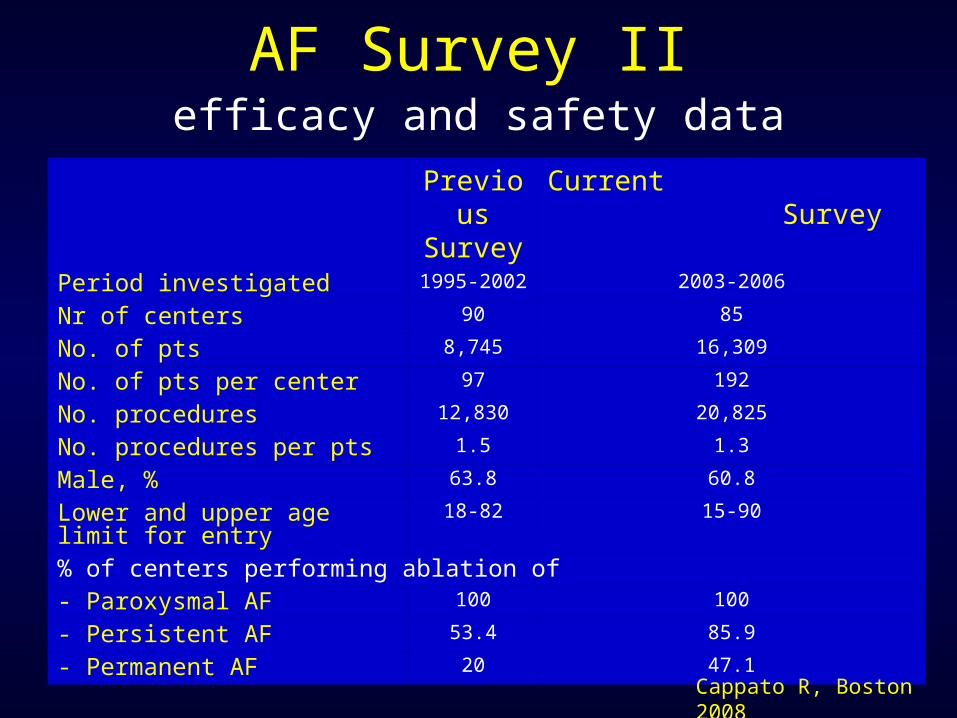
AF Survey II
Previous
Survey
Current Survey
Period investigated 1995-2002 2003-2006
Nr of centers 90 85
No. of pts 8,745 16,309
No. of pts per center 97 192
No. procedures 12,830 20,825
No. procedures per pts 1.5 1.3
Male, % 63.8 60.8
Lower and upper age limit for entry
18-82 15-90
% of centers performing ablation of- Paroxysmal AF 100 100
- Persistent AF 53.4 85.9
- Permanent AF 20 47.1Cappato R, Boston 2008
efficacy and safety data
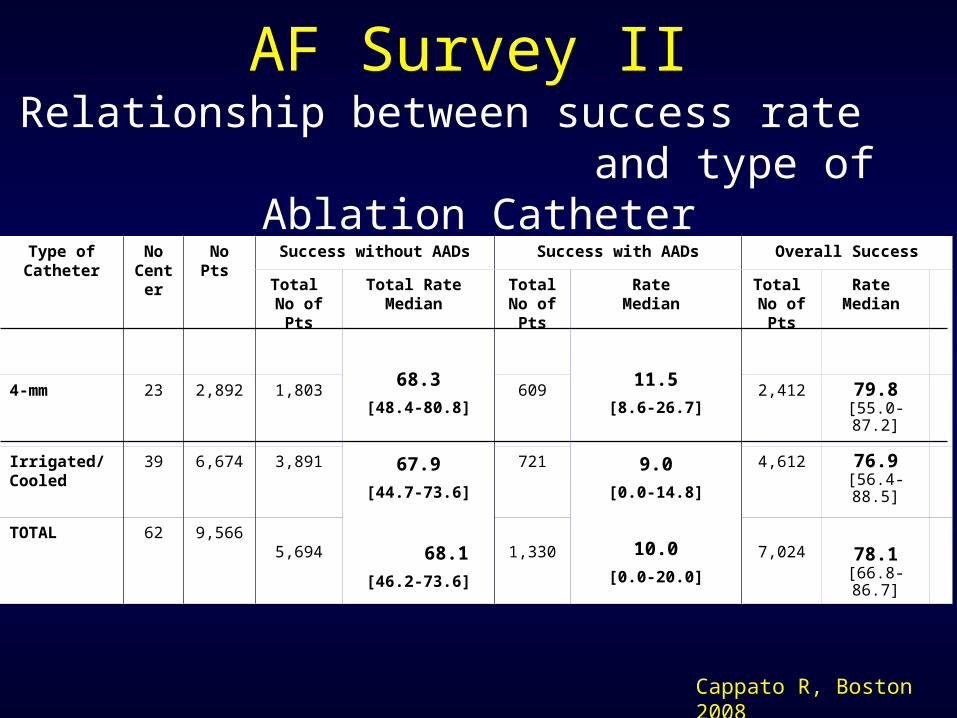
Relationship between success rate and type of Ablation Catheter
Type of Catheter
No Center
No Pts
Success without AADs Success with AADs Overall Success
Total No of Pts
Total Rate Median
68.3
[48.4-80.8]
67.9
[44.7-73.6]
68.1
[46.2-73.6]
Total No of Pts
Rate Median
11.5
[8.6-26.7]
9.0
[0.0-14.8]
10.0
[0.0-20.0]
Total No of Pts
Rate Median
4-mm 23 2,892 1,803 609 2,412 79.8[55.0-87.2]
Irrigated/ Cooled
39 6,674 3,891 721 4,612 76.9[56.4-88.5]
TOTAL 62 9,5665,694 1,330 7,024 78.1
[66.8-86.7]
AF Survey II
Cappato R, Boston 2008
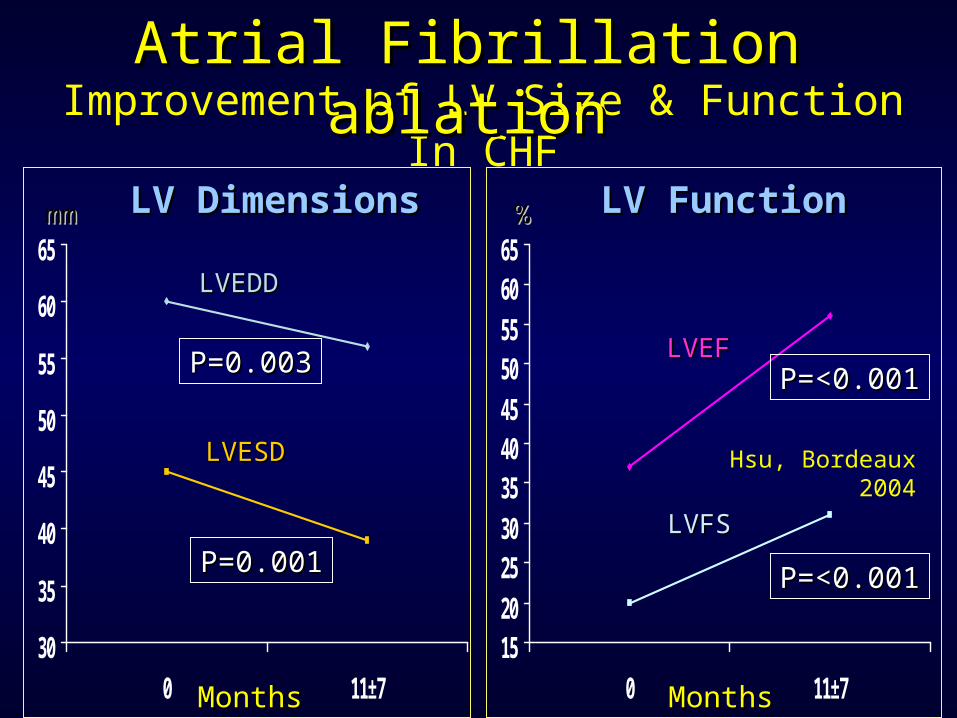
Improvement of LV Size & Function In CHF
30
35
40
45
50
55
60
65
0 11±7
LV DimensionsLV Dimensions
MonthsMonths
LVEDDLVEDD
P=0.003P=0.003
P=0.001P=0.001
LVESDLVESD
mmmm
1520253035404550556065
0 11±7
LV FunctionLV Function
MonthsMonths
LVEFLVEFP=<0.001P=<0.001
LVFSLVFS
%%
P=<0.001P=<0.001
Hsu, Bordeaux 2004
Atrial Fibrillation ablationAtrial Fibrillation ablation
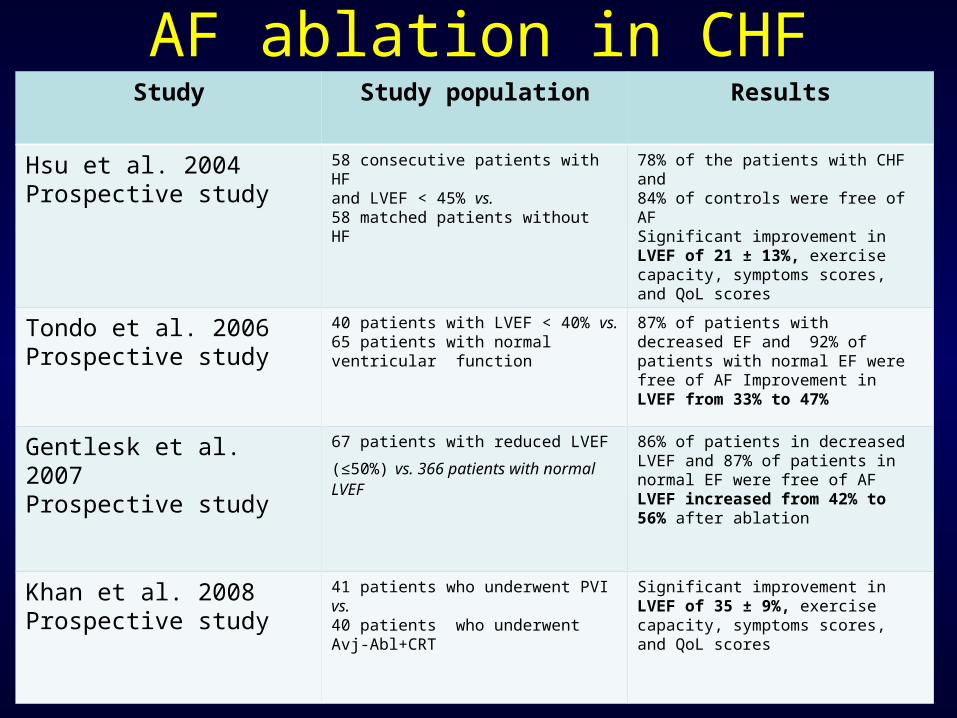
AF ablation in CHFStudy Study population Results
Hsu et al. 2004Prospective study
58 consecutive patients with HFand LVEF < 45% vs. 58 matched patients without HF
78% of the patients with CHF and84% of controls were free of AFSignificant improvement in LVEF of 21 ± 13%, exercise capacity, symptoms scores, and QoL scores
Tondo et al. 2006Prospective study
40 patients with LVEF < 40% vs. 65 patients with normal ventricular function
87% of patients with decreased EF and 92% of patients with normal EF were free of AF Improvement in LVEF from 33% to 47%
Gentlesk et al. 2007Prospective study
67 patients with reduced LVEF
(≤50%) vs. 366 patients with normal LVEF
86% of patients in decreased LVEF and 87% of patients in normal EF were free of AF LVEF increased from 42% to 56% after ablation
Khan et al. 2008Prospective study
41 patients who underwent PVI vs. 40 patients who underwent Avj-Abl+CRT
Significant improvement in LVEF of 35 ± 9%, exercise capacity, symptoms scores, and QoL scores
PVs isolation in CHF pts
1. No clinically relevant endpoints2. Inadequate sample sizes3. Younger patients (mean age range: 54-64 yrs)
4. Short term follow-up5. Long term effects remained
uninvestigated
considerations
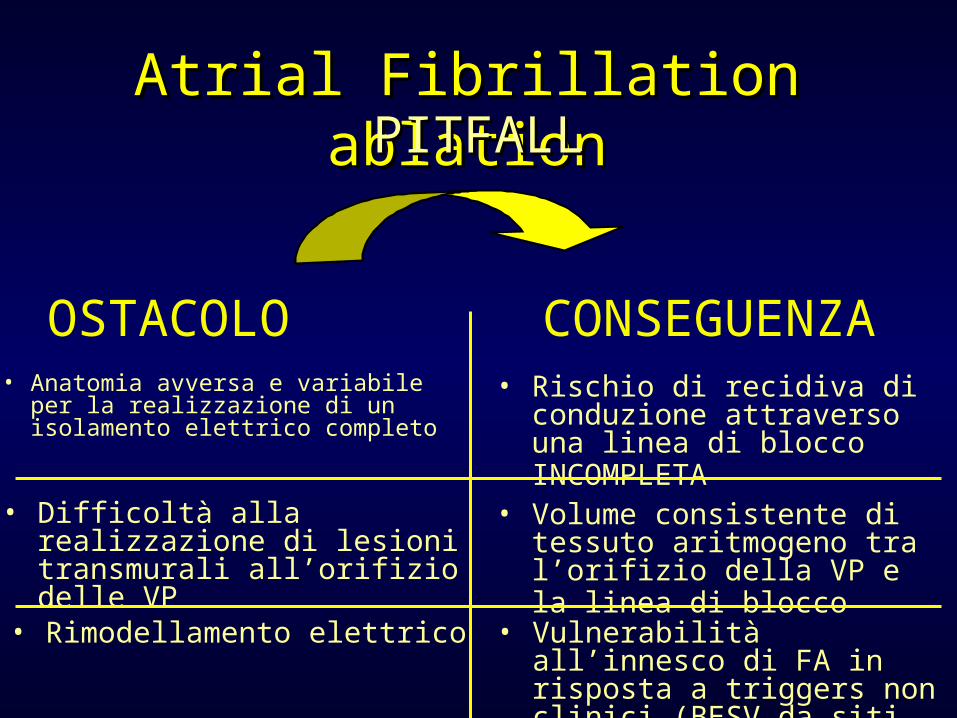
• Anatomia avversa e variabile per la realizzazione di un isolamento elettrico completo
• Rischio di recidiva di conduzione attraverso una linea di blocco INCOMPLETA
OSTACOLO CONSEGUENZA
• Difficoltà alla realizzazione di lesioni transmurali all’orifizio delle VP
• Rimodellamento elettrico
• Volume consistente di tessuto aritmogeno tra l’orifizio della VP e la linea di blocco
• Vulnerabilità all’innesco di FA in risposta a triggers non clinici (BESV da siti innocenti)
Atrial Fibrillation ablationAtrial Fibrillation ablationPITFALLPITFALL
tipo di FAtipo di FA cardiopatia sottostantecardiopatia sottostante
isolamento delle VP isolamento delle VP (ostiale, antrale, (ostiale, antrale, ecc)ecc)
ablazione ablazione circonferenzialecirconferenziale
lesioni lineari aggiuntivelesioni lineari aggiuntive ablazione in aree a ablazione in aree a
conduzione rallentataconduzione rallentata
effettivo isolamento VP
Riduzione/modifica del substrato
Δ tono autonomico
creazione di barriere elettriche complete e non
non inducibilità della FA
recidive aritmiche recidive aritmiche sintomatiche/asintomatichesintomatiche/asintomatiche
utilizzo terapia antiaritmicautilizzo terapia antiaritmica
Disomogeneità Disomogeneità delle popolazioni delle popolazioni
arruolatearruolate
Differenze della Differenze della tecnica ablativatecnica ablativa
End-point End-point procedurali non procedurali non
uniformiuniformi
Metodologia del Metodologia del follow-upfollow-up
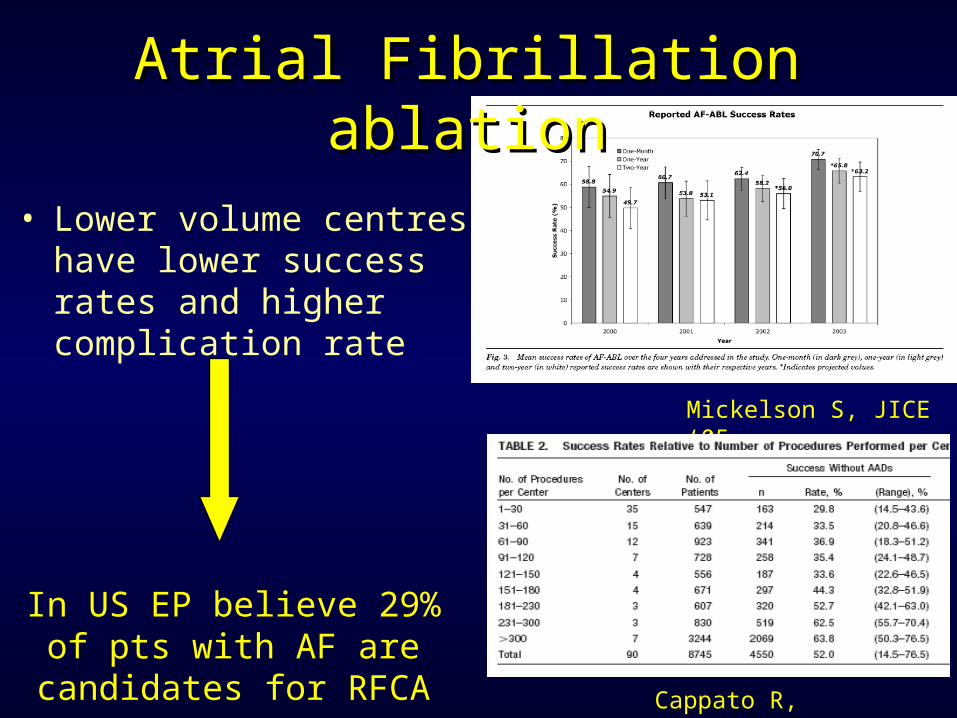
Mickelson S, JICE ‘05
Cappato R, Circulation ‘05
In US EP believe 29% of pts with AF are
candidates for RFCA
• Lower volume centres have lower success rates and higher complication rate
Atrial Fibrillation ablationAtrial Fibrillation ablation
Which is the impact of the new technologies ?
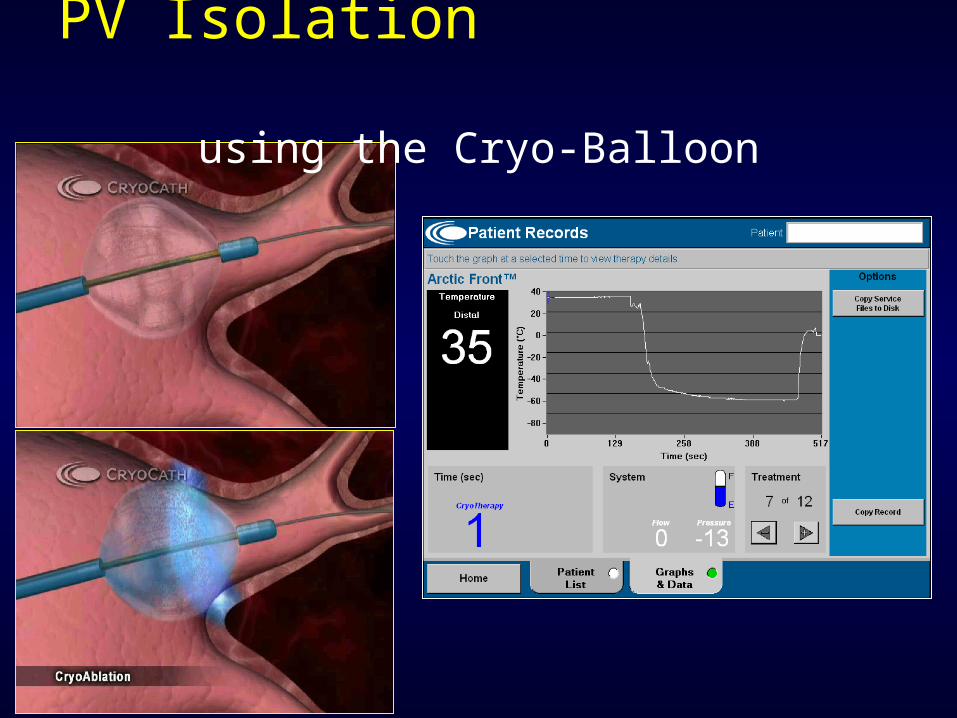
PV Isolation using the Cryo-Balloon
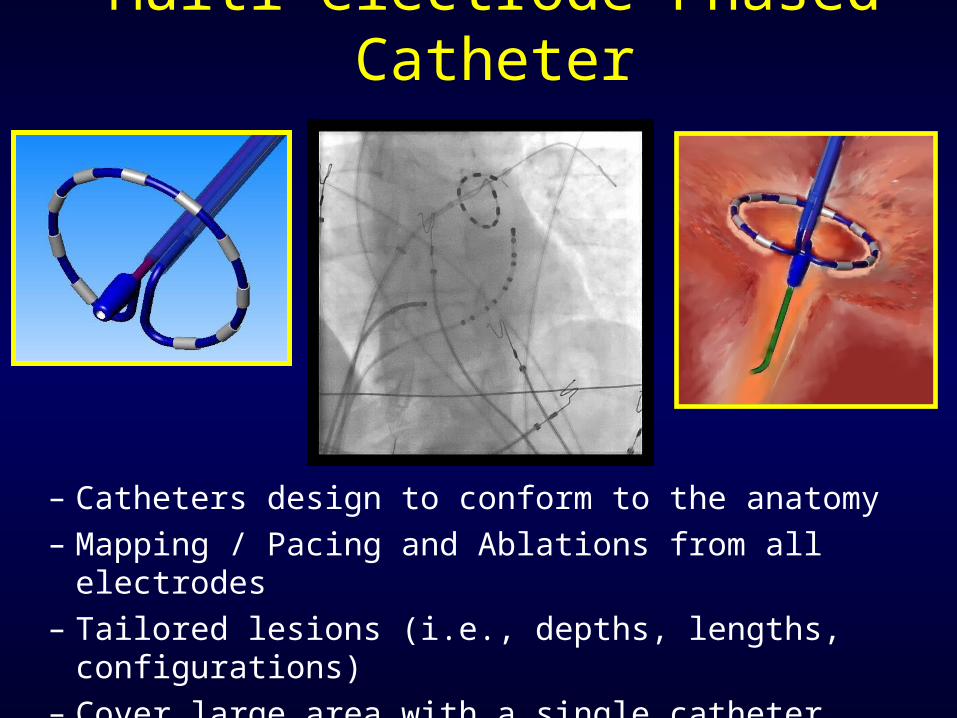
Multi-electrode Phased Catheter
– Catheters design to conform to the anatomy– Mapping / Pacing and Ablations from all electrodes – Tailored lesions (i.e., depths, lengths, configurations)– Cover large area with a single catheter placement– Do not require 3D mapping system
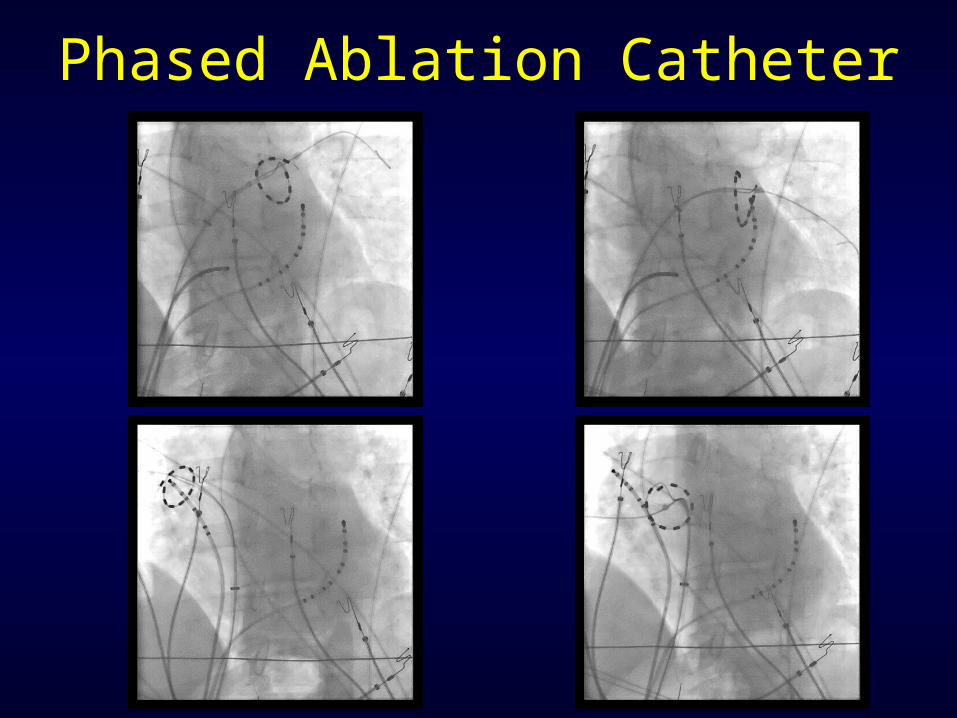
Phased Ablation Catheter
Does one AFib approach fit in all CHF pts?
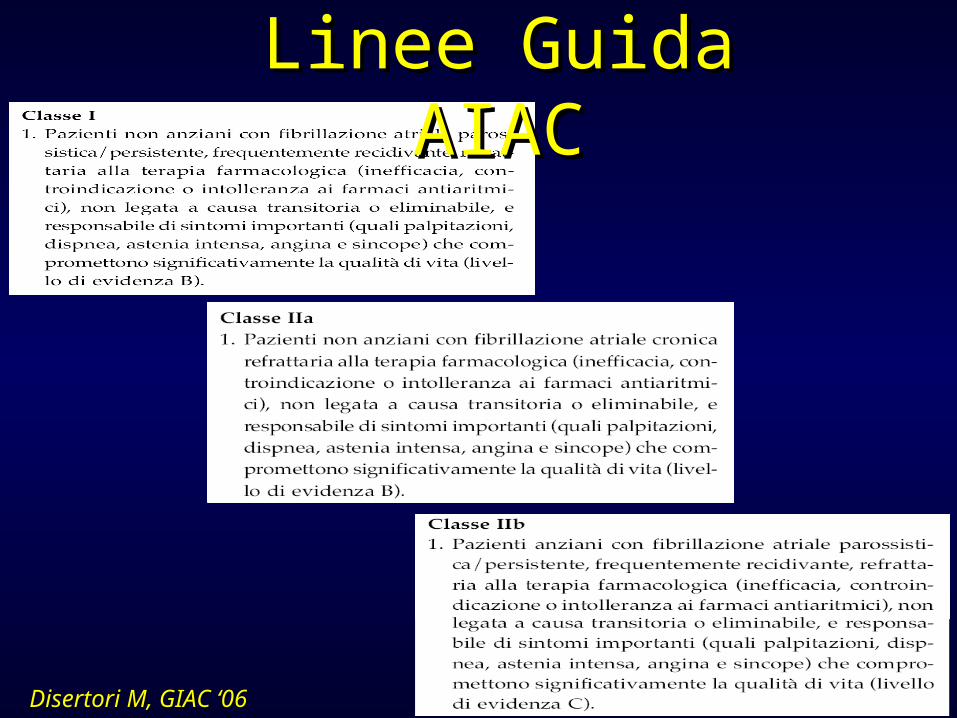
Disertori M, GIAC ‘06Disertori M, GIAC ‘06
Linee Guida AIACLinee Guida AIAC
Catheter Ablation Catheter Ablation of Atrial Fibrillation of Atrial Fibrillation
• An individually tailored approach is neededAn individually tailored approach is needed
• PVI renders 52-84% of PAF non-inducible and PVI renders 52-84% of PAF non-inducible and results in clinical success; substrate results in clinical success; substrate modification in such patients is not indicatedmodification in such patients is not indicated
• Substrate modification is likely to be required Substrate modification is likely to be required in 30% of PAF and most CAF, but needs in 30% of PAF and most CAF, but needs technological improvementstechnological improvements
What is success?
• Complete freedom of AF, off drug RX?• No symptoms, but drug Rx required?• Dramatic decrease in symptoms, but
drugs still required?• QoL• How do we detect asymptomatic
episodes?• Anticoagulation ………………...?


















