Vitamina D ed Asma - Prof. Boner Attilio Università di Verona
69
Vitamin D and Asthma Vitamin D deficiency- insufficiency Onset of Disease Morbidity & Exacerbations Protective Mechanisms University of Verona, Italy Attilio Boner [email protected]
-
Upload
roberto-conte -
Category
Health & Medicine
-
view
73 -
download
2
Transcript of Vitamina D ed Asma - Prof. Boner Attilio Università di Verona

Vitamin D and Asthma
Vitamin D deficiency-insufficiency Onset of Disease Morbidity & Exacerbations
Protective Mechanisms Summary & Conclusions
University of Verona,
Italy
Attilio Boner

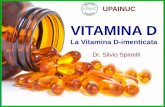
Synthesis and Metabolism of Vitamin D. Rosen CJ. NEJM 2011;364:248
Vitamin D is initially generated in the skin from the nonenzymaticconversion of provitamin D3 to previtamin D3.Dietary intake of vitamin D is usually relatively limited, since few foods, with the exception of certain kinds of fish, contain sizable amounts; supplements are commonly used. Vitamin D is either stored in adipose tissue or converted in the liver by the enzyme 25-hydroxylase to 25-hydroxyvitamin D3 (25[OH]D3), the form that circulates in the highest concentration and reflects solar and dietary exposure. It is converted to the active metabolite, 1,25-dihydroxyvitamin D (1,25[OH]2D), or calcitriol, in the kidney, although other tissues have 1α-hydroxylase enzymatic activity. The synthesis of calcitriol is enhanced (+) by increasing levels of parathyroid hormone (PTH), which rise in response to lower levels of serum calcium. Reduced levels of serum phosphate can also increase (+) the production of calcitriol.Its synthesis is suppressed (–) by the production of fibroblastgrowth factor 23 (FGF-23), which is secreted by osteocytes in the bone matrix. Calcitriol inhibits the activity of 1α-hydroxylase (CYP27B1) and stimulates the activity of 24-hydroxylase (CYP24R1), an enzyme that promotes production of 24,25(OH)2D3, a vitamin D productthat is not biologically active. In CYP2R1, CYP27B1, and CYP24R1, CYP denotes cytochrome P.

The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of
Medicine: what clinicians need to know.Ross AC, J Clin Endocrinol Metab. 2011;96:53-8.
RDA = Recommended Dietary Allowance; UL= tolerable upper intake level; c= not well defined

RDA = Recommended Dietary Allowance; UL= tolerable upper intake level; c= not well defined
The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of
Medicine: what clinicians need to know.Ross AC, J Clin Endocrinol Metab. 2011;96:53-8.
Dietary Reference Intake
shown in Table 1
are based on dietary
requirementsusing bone health
as an indicator.

There are several publications suggesting that vitamin D deficiency (25-hydroxyvitamin D level <20 ng/mL) and insufficiency (25-hydroxyvitamin D level >20 ng - <30 ng/mL) is a pandemic affecting all populations with serious health consequences.
Vitamin D deficiency-insufficiency
Wang TJ, Circulation 117, 503–511. Dobnig H, Arch Intern Med 168, 1340–1349. Melamed ML, Arch Intern Med 168, 1629–1637. Melamed ML, Arterioscler Thromb Vasc Biol 28, 1179–1185. Dong Y, J Clin Endocrinol Metab 95,4584–4591. Reis JP, Pediatrics 124, e371–e379. Kumar J, Pediatrics 124, e362–e370.Sabetta JR, PlosOne 5,e11088. Moan J, Proc Natl Acad Sci USA 105, 668–673.

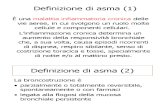
High Prevalence of Vitamin D Deficiency among Inner-City African American Youth with Asthma in
Washington Freishtat J Pediatr 2010;156:948-52
Urban African-American (AA) youth with asthma (=92)
control subjects without asthma (=21).
25-hydroxyvitamin D insufficiency (<30 ng/mL) and deficiency (<20 ng/mL).
86%
% children with <30 ng/mL Vit D
Asthmatics
Controls
19%
100 – 90 – 80 – 70 – 60 – 50 – 40 – 30 – 20 – 10 – 0

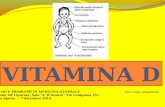
Asthma prevalence associated with geographical latitude and regional insolation in
the United States of America and Australia. Krstić G. PLoS One. 2011;6:e18492.
Asthma prevalence vs. latitude in metropolitan/micropolitan areas of
USA
Linear regression analyses on asthma prevalence in adult population vs. geographical latitude, insolation, air temperature, and air pollution (PM(2.5))
97 metropolitan/micropolitan statistical areas of the USA and in 8 metropolitan areas of Australia. 50°
25°

Asthma prevalence associated with geographical latitude and regional insolation in
the United States of America and Australia. Krstić G. PLoS One. 2011;6:e18492.Asthma prevalence vs. latitude in the
population of 8 major metropolitan areas of Australia.
Linear regression analyses on asthma prevalence in adult population vs. geographical latitude, insolation, air temperature, and air pollution (PM(2.5))
97 metropolitan/micropolitan statistical areas of the USA and in 8 metropolitan areas of Australia.
-50°
-10°

Vitamin D and Asthma
Vitamin D deficiency-insufficiency Onset of Disease Morbidity & Exacerbations
Protective Mechanisms Summary & Conclusions
University of Verona,
Italy
Attilio Boner

Vitamin D deficiency causes deficits in lung function and alters lung structure. Zosky GR,
AJRCCM. 2011;183:1336-43. mouse model of vitamin D deficiency
by dietary manipulation
thoracic gas volume
standard vitamin Dsufficient diet
airway resistance tissue elastance

Genetic analysis of lung function in inbred mice suggests vitamin D receptor as a candidate gene
Berndt A, Mol Genet Genomics 2011;286:237–246
Vitamin D receptor (Vdr) knockout mice
Vdr knockout mice showed significantly higher airway dynamic resistance than mice with one (i.e., heterozygous) orboth copies (i.e., wild-type) of the Vdr.
Increase in dynamic resistance (R slope) caused by consecutive doses of
methacholine exposure in mice deficient in Vdr (Vdr-KO) and mice carrying one (Vdr-HET) or two copies (Vdr-
WT ) of Vdr.
P<0.05
Vdr +Vdr +
Vdr +Vdr -
Vdr -Vdr -

1.194 mother-child pairs in Boston
Maternal intake of vitamin D during pregnancy with FFQ Recurrent wheeze
In 3 yrs-old children of mothers in the highest
quartile of vitamin D intake (724 IU) versus the lowest quartile (356 IU) OR for
1 –
0
0.39p<0.001
Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of
age.Camargo CA JrAm J Clin Nutr. 2007;85:788-95.

Random sample of 2000 healthy Scottish pregnant women at approximately 12 wk gestation
Maternal vitamin D intake ascertained at 32 wk of gestation with FFQ Ever
wheeze
In 5 year old children of mothers in the highest versus the lowest quintiles of vit D intake OR for1 –
0
0.48
Persistent wheeze
Wheeze in previous
year
0.35 0.33
Maternal vitamin D intake during pregnancy and early childhood wheezing. Devereux G, Am J Clin Nutr.
2007;85:853

596 pregnant women
Maternal 25 (OH) - vitamin D concentrations measured in late pregnancy
Atopy
In children whose mothers had a 25 (OH )-vitamin D
concentration >75 nmol/L compared to <30 nmol/L
3.26
Asthma
p=0.025
5.40p=0.038
1 –
0
Maternal vitamin D status during pregnancy and child outcomes. Gale CR, Eur J Clin Nutr.
2008;62:68-77.
at age 9 years
75 nmol/L = 30 ng/ml30 nmol/L = 12 ng/ml

Maternal and child’s vitamin D supplement use and
vitamin D level in relation to childhood lung function:
the KOALA Birth Cohort StudyCremers E, Thorax 2011;66:474-480
KOALA Birth Cohortlung function at age 6-7
years (n=436) Vitamin during
pregnancy and child’s vitamin D supplement use were collected through
questionnaires
no association was found between 25-hydroxyvitamin D levels, vitamin D supplementation inchildhood or recommended vitamin D dosage of≥ 10 µg/day during pregnancy and lung function in children aged 6-7 years.
1μg = 40 UI

VITAMIN D AND ASTHMA ONSET
observational studiesPaul G AJRCCM 2011
Review article
• insufficient evidence of a causal association between vitamin D
status and asthma per se.
•merits further assessment
The in utero effects of maternal vitamin D deficiency: how it
results in asthma and other chronic
diseases.Weiss ST, Am J Respir Crit
Care Med. 2011;183:1286-7.Editorial
• higher vitamin D intake in pregnant women has been linked to reduced rates of wheezing and
asthma in their offspring.

VITAMIN D AND ASTHMA ONSET
observational studiesPaul G AJRCCM 2011 in press
Review article
• insufficient evidence of a causal association between vitamin D
status and asthma per se.
•merits further assessment
The in utero effects of maternal vitamin D deficiency: how it
results in asthma and other chronic
diseases.Weiss ST, Am J Respir Crit
Care Med. 2011;183:1286-7.Editorial
• higher vitamin D intake in pregnant women has been linked to reduced rates of wheezing and
asthma in their offspring.
The knowledge that currently over 90% of African-American pregnant
women and over 60% of white pregnant women are vitamin D–deficient or insufficient and the knowledge of the multiple negative effects of vitamin D deficiency-insufficiency
early in lifesuggest the opportunity to evaluate vitamin D serum level during pregnancy and appropriate supplementation in deficient
or insufficient mothers> 20 ng/mL and < 50 ng/mL ideal level ?

Vitamin D and Asthma
Vitamin D deficiency-insufficiency Onset of Disease Morbidity & Exacerbations
Protective Mechanisms Summary & Conclusions
University of Verona,
Italy
Attilio Boner

25–hydroxyvitamin D levels
616 asthmatic children Vitamin D levels
deficient (<20 ng/ml), insufficient (≥20 and <30 ng/ml), and sufficient (≥30 ng/ml)
Vitamin D levels were significantly
and inversely associated with:
1) total IgE and eosinophil count
2) any hospitalization in the previous year (p=0.03),
3) any use of anti-inflammatory
medications in the previous year (p=0.01),
4) increased airway responsiveness (p = 0.05).
Serum Vitamin D Levels and Markers of Severity of Childhood Asthma in
Costa RicaBrehm Am J Respir Crit Care Med 2009;179:765

Distribution of serum vitamin D in children in Costa Rica
Serum Vitamin D Levels and Markers of Severity of Childhood Asthma in
Costa RicaBrehm Am J Respir Crit Care Med 2009;179:765
28% children with vit D
<30ng/mL (deficient-
insufficient)sufficient
levels

100 – 90 – 80 – 70 – 60 – 50 – 40 – 30 – 20 – 10 – 0
% asthmatic children with a desiderable level of
Vitamin D (at least 30 to 40 ng/mL)
9.3%
Verona = 45°
Vitamin D Serum Levels and Markers of Asthma Control in Italian Children Chinellato J Pediatr
2011;158:437
75 asthmatic children
25-hydroxyvitamin D
Spirometry
asthma control, according to GINA guidelines and with Childhood Asthma Control Test

75 asthmatic children
25-hydroxyvitamin D
Spirometry
asthma control, according to GINA guidelines and with Childhood Asthma Control Test
individual data of vitamin D serum levels in relationship with FVC %
predr= 0.29 p=0.0013
Vitamin D Serum Levels and Markers of Asthma Control in Italian Children Chinellato J Pediatr
2011;158:437

75 asthmatic children
25-hydroxyvitamin D
Spirometry
asthma control, according to GINA guidelines and with Childhood Asthma Control Test
Vitamin D Serum Levels and Markers of Asthma Control in Italian Children Chinellato J Pediatr
2011;158:437p=0.054
p=0.054

75 asthmatic children
25-hydroxyvitamin D
Spirometry
asthma control, according to GINA guidelines and with Childhood Asthma Control Test
r=0.29 p<0.01
Vitamin D Serum Levels and Markers of Asthma Control in Italian Children Chinellato J Pediatr
2011;158:437

45 children with intermittent asthma
25-hydroxyvitamin D baseline FVC, FEV1
∆FEV1 after a
standardized exercise challenge
mean 25-hydroxyvitamin D (ng/mL)
30 –
20 –
10 –
0∆FEV1≥10%
p=0.0002
∆FEV1<10%
23.516.2
Vitamin D Serum Levels and Lung Function and Exercise Induced Bronchoconstriction In
Children With Intermittent Asthma. Chinellato I, ERJ 2011;37:1366

Vitamin D Serum Levels and Lung Function and Exercise Induced Bronchoconstriction In
Children With Intermittent Asthma. Chinellato I, ERJ 2011;37:1366
Relationship between serum vitamin D levels and change FEV1 after
exercise challenge
Relationship between serum vitamin D serum level and
a) FVC and b) FEV1 % pred.
r=0.48; p=0.001
r=0.34; p=0.037
r=0.32; p=0.037

Relationship Between Serum Vitamin D, Disease Severity and Airway Remodeling in Children with
Asthma.Gupta A, Am J Respir Crit Care Med. 2011;184:1342
86 children (mean age 11.7 years),
36 with severe, therapy resistant asthma (STRA),
26 moderate asthmatics (MA) 24 non-asthmatic controls.
Serum 25-hydroxyvitamin D (25[OH]D3)
Median 25[OH]D3 levels nmol/L
28.0
STRA
p<0.00160 -
50
–
40
–
30
–
20
–
10
–
0
MA CONTROLS
42.5
56.5
11.2 ng/mL17.0 ng/mL
22.6 ng/mL
p<0.001
p=0.09

86 children (mean age 11.7 years),
36 with severe, therapy resistant asthma (STRA),
26 moderate asthmatics (MA) 24 non-asthmatic controls.
Serum 25-hydroxyvitamin D (25[OH]D3)
There was a significant negative correlation between serum 25[OH]D3 and volume
fraction of Airway Smooth Muscle (r= -0.6, p-0.008)
Vv (smooth muscle (SM)/SM + submucosa) = Volume fraction of smooth muscle indexed to volume of submucosa tissue
Relationship Between Serum Vitamin D, Disease Severity and Airway Remodeling in Children with
Asthma.Gupta A, Am J Respir Crit Care Med. 2011;184:1342

Serum vitamin D levels and severe asthma exacerbations in the Childhood Asthma
Management Program study Brehm JACI 2010;126:52 OR for any hospitalization or emergency department visit
1.52.0 –
1.5 –
1.0 –
0.5 –
0
p=0.01
In Vit D insufficiency (<30 ng/ml) at baseline
25-hydroxyvitamin D levels in sera in a retrospective longitudinal study.
Follow-up: 4 years
1024 children with mild-to-moderate persistent asthma at the time of enrollment in CAMP study.

Serum vitamin D levels and severe asthma exacerbations in the Childhood Asthma
Management Program study Brehm JACI 2010;126:52 OR for severe asthma
exacerbation (hospitalization or ED visit)
1
2.0 –
1.5 –
1.0 –
0.5 –
0ICS treatmentVit D sufficient
1.7
1.7
2
++
+-
-+
--

Vitamin D supplementation in children may prevent asthma exacerbation triggered by
acute respiratory infection. Majak P, J Allergy Clin Immunol 2011;127:1294-6.
48 children (5-18 yrs) with newly diagnosed asthma and sensitive only to house dust mites
budesonide 800 µg/d administered as a dry powder and vitamin D placebo (steroid group, n = 24), or budesonide 800 µg/d and vitamin D3-500 IU (steroid + vit D group n=24).
Follow-up: 6 months

Vitamin D and Asthma
Vitamin D deficiency-insufficiency Onset of Disease Morbidity & Exacerbations
Protective Mechanisms Summary & Conclusions
University of Verona,
Italy
Attilio Boner

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA MORBIDITY?Antiviral Properties•Airway epithelial cells can
hydroxylate 25(OH)D to its active form (1,25 (OH)2D3), leading to increased differentiation and recruitment of macrophages, enhanced production of cathelicidin and CD14, and potentiation of host defenses against M. tuberculosis and other bacteria, fungi, and viruses.
25(OH)D
1,25 (OH)2D3
CD14 has been shown to be expressed in monocytes, macrophages, polymorphonuclear neutrophils

Randomized trial of vitamin D supplementation to prevent seasonal influenza A in
schoolchildren. Urashima M, Am J Clin Nutr 2010;91:1255–1260.
Vitamin D(3) supplements (1200 IU/d) (n= 167) with placebo (n= 167) in schoolchildren
From December 2008 through March 2009
incidence of influenza A, diagnosed with influenza antigen testing with a nasopharyngeal swab specimen.
RR for asthma attacks1.0 –
0.5 –
0
0.17P=0.006
in asthmatic children who had been vitamin D
supplemented

Low serum 25-hydroxyvitamin D levels are associated with increased risk of viral coinfections
in wheezing children Jartti JACI 2010;126:1074
284 hospitalized wheezing children (median age 1.6 years).
Nasopharyngeal aspirate samples for 18 different viruses.
Serum 25(OH)D measurements.
0.91
For any 10 nmol/L (4 ng/mL) increase in vitamin D serum
levels OR for1.0 –
0.5 –
0
0.92
RSV
rhinovirus
0.91
multiple viral
cause Induced wheezingTo convert 25-OH vitamin D concentrations
from nanomoles per liter to ng/mL, divide by 2.496.

Associations of cord-blood 25(OH)D levels with probabilities of
cumulative wheeze or incident asthma by 5 years of age
Cord-Blood 25-Hydroxyvitamin D Levels and Risk of
Respiratory Infection, Wheezing, and Asthma Camargo Pediatrics 2011;127:180
25(OH)D in cord blood from 922 newborns.
History of respiratory infection at 3 mo of age or a history of wheezing at 15 mo and then annually thereafter.
Doctor-diagnosed asthma by age 5 years.To convert 25-OH vitamin D concentrations
from nanomoles per liter to ng/mL, divide by 2.496.

Associations of cord-blood 25(OH)D levels with probabilities of
cumulative wheeze or incident asthma by 5 years of age
Cord-Blood 25-Hydroxyvitamin D Levels and Risk of
Respiratory Infection, Wheezing, and Asthma Camargo Pediatrics 2011;127:180
25(OH)D in cord blood from 922 newborns.
History of respiratory infection at 3 mo of age or a history of wheezing at 15 mo and then annually thereafter.
Doctor-diagnosed asthma by age 5 years.To convert 25-OH vitamin D concentrations
from nanomoles per liter to ng/mL, divide by 2.496.
Cord blood25(OH)D levels were inverselyassociated with
wheeze throughout
early childhood but had no association
with incident asthma.

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA
MORBIDITY?Enhanced Steroid Responsiveness The overall mechanism of steroid hormone
action is the regulation of gene expression. The lipophilic steroid hormones are carried into the blood stream with the majority of hormone reversibly bound to carrier proteins and a small amount of free steroids. The free steroid diffuses throught the cell membrane and enters cells. The sensitive cells contain a high affinity steroid hormone receptor either in the cytosol or in the nucleus. The steroid receptor complex enters the nucleus and initiates a conformational change that involves dimerization to activate the complex to interact with specific regions on cellular DNA referred to as hormone responsive elements (HRE). This initiates the process of transcription to produce mRNA and translations to produce proteins. These proteins regulate cell function, growth differentiation, etc
TGF-β and IL-10

Reversing the defective induction of IL-10–secreting regulatory T cells in glucocorticoid-resistant asthma patients. Xystrakis E, J Clin Invest
2006;116:146–155.adding vitamin D to cell cultures increases glucocorticoid-induced
secretion of IL-10 by Tregs
Patients with severe asthma failling to demonstrate clinical improvement upon glucocorticoid therapy (steroid resistant = SR)
Dexamethasone does not enhance secretion of IL-10 by their CD4+ T cells

54 adult asthmatics serum 25(OH)D, lung function, AHRGC response as
measured by dexamethasone induced expression of MAP kinase phosphatase-1 (MKP-1) by PBMCs, a negative regulator of MAPK signal transduction pathways for pro-inflammatory genes
Serum vitamin D vs DEX-induced MKP-1 expression on
PBMC
r = 0.4 p = 0.04
Vitamin D Levels, Lung Function and Steroid Response in Adult Asthma. Sutherland ER, AJRCCM.
2010;181:669

54 adult asthmatics serum 25(OH)D, lung function, AHRGC response as
measured by dexamethasone induced expression of MAP kinase phosphatase-1 (MKP-1) by PBMCs.
Serum vitamin D vs baseline TNF-α
r = -0.3 p = 0.01
Vitamin D Levels, Lung Function and Steroid Response in Adult Asthma. Sutherland ER, AJRCCM.
2010;181:669
Higher serum vitamin D
concentrations were associated
withdecreased baseline
expression of TNF-a
by PBMCs

Decreased serum vitamin D levels in children with asthma are associated with increased corticosteroid use Searing JACI 2010;125:995
25-hydroxyvitamin D serum levels.
100 asthmatic children.
VitD's effects on dexamethasone (DEX) induction of mitogen-activated protein kinase phosphatase 1 and IL-10 in PBMCs.
29
40
–
30
–
20
–
10
–
0
Vitamin D serum levels ng/mL (median)
35
ICS (-)
ICS (+)
p=0.0475

Decreased serum vitamin D levels in children with asthma are associated with increased corticosteroid use Searing JACI 2010;125:995
25-hydroxyvitamin D serum levels.
100 asthmatic children.
VitD's effects on dexamethasone (DEX) induction of mitogen-activated protein kinase phosphatase 1 and IL-10 in PBMCs.
25
40
–
30
–
20
–
10
–
0
Vitamin D serum levels ng/mL (median)
32
(-) (+) Oral corticosteroids
p=0.02

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA MORBIDITY?
Down-regulation of atopy

ABPA (-)
Vitamin D3 attenuates Th2 responses to Aspergillus fumigatus mounted by CD4+ T cells
from cystic fibrosis patients with allergic bronchopulmonary aspergillosis. Kreindler JL, J Clin
Invest 2010;120:3242-54.
ABPA (+)patients
Vitamin D serum level (ng/mL)
36.56 p=0.0240
–
30
–
20
–
10
–
0
22.04
cohorts of A. fumigatus-colonized CF patients
with and without Allergic Bronchopulmonary Aspergillosis (ABPA)
AspergillussIgE

Vitamin D and atopy and asthma phenotypes in children: a longitudinal cohort study.
Hollams EM, Eur Respir J. 2011;38:1320-27
1. Serum vitamin D levels in children at both ages were negatively associated with concurrent allergic phenotypes;
2. Gender stratification revealed that this association was restricted mainly to boys.
3. Further, vitamin D levels at age 6 were significant predictors of subsequent atopy/asthma-associated phenotypes at age 14.
an unselected community birth cohort in Australia
6-year-olds (n=989) and 14-year-olds (n=1380);
associations between vitamin D status and biological signatures indicative of allergy and asthma development in children aged 6 and 14 years

Probability of atopic sensitisation decreases as vitamin D increases in
males only
Vitamin D and atopy and asthma phenotypes in children: a longitudinal cohort study.
Hollams EM, Eur Respir J. 2011;38:1320-27
an unselected community birth cohort in Australia
6-year-olds (n=989) and 14-year-olds (n=1380);
associations between vitamin D status and biological signatures indicative of allergy and asthma development in children aged 6 and 14 years

an unselected community birth cohort in Australia
6-year-olds (n=989) and 14-year-olds (n=1380);
associations between vitamin D status and biological signatures indicative of allergy and asthma development in children aged 6 and 14 years
Mean vitamin D levels and mean HDM-IgE titers combined over the
three year period
Vitamin D and atopy and asthma phenotypes in children: a longitudinal cohort study.
Hollams EM, Eur Respir J. 2011;38:1320-27

Variation in the average immunoglobulin E by
25-hydroxyvitamin D concentration in the 1958 British cohort at the age of 45
years.
Serum 25-hydroxyvitamin D and IgE a significant but nonlinear relationship Hyppönen
Allergy 2009;64:613
9377 participants in the 1958 British birth cohort.
Assessment at 45 years of age.
<10 ng/mL >50 ng/mL

Variation in the average immunoglobulin E by
25-hydroxyvitamin D concentration in the 1958 British cohort at the age of 45
years.
Serum 25-hydroxyvitamin D and IgE a significant but nonlinear relationship Hyppönen
Allergy 2009;64:613
9377 participants in the 1958 British birth cohort.
Assessment at 45 years of age.
There may be a threshold effect with
both low and high 25(OH)D
levels associated
with elevated IgE
concentrations.
>50 ng/mL<10 ng/mL

Cord blood 25-hydroxyvitamin D levels are associated with aeroallergen sensitization in
children from Tucson, Arizona. Rothers J, JACI 2011;128:1093-1099.
Cord blood 25(OH)D levels measured in 219 participants in the Tucson Infant Immune Study,
total IgE and specific IgE levels to 6 aeroallergens were measured at 1, 2, 3, and 5 years.
SPTs and physician-diagnosed active allergic rhinitis and asthma at age 5 years.
OR for detectable inhalant allergen-specific IgE
12
4
2.4P=0.03
P=0.01

It is possible that in the presence of vitamin D, Treg cells develop and function normally in suppressing inappropriate TH1 and TH2 responses to environmental exposure (ie, allergens, lack of infections, and so forth), leading to a more balanced immune response.
On the other hand, if vitamin D is lacking, Treg cells may not develop and function normally, and in the presence of the appropriate environmental influence, TH1 or TH2 responses are allowed to proceed unabated, leading to disease.
The paradox of vitamin D effects

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA
MORBIDITY?Other potential mechanisms: obesity

Season of birth and prevalence of overweight and obesity in Canada. Wattie N, Early Hum Dev
2008;84:539-47.
Canadian Community Health Survey,
birth data of
respondents 12 to 64 years old
among the 20-64 year olds, those in the obese III (BMI≥40
kg/m2) category OR for2 –
1 –
0
1.54
being born in the winter

Vitamin D deficiency and anthropometric indicators of adiposity in school-age children: a
prospective study. Gilbert-Diamond D, Am J Clin Nutr 2010;92:1446-51.
vitamin D serostatus and changes in body mass
index (BMI; in kg/m²), skinfold-thickness ratio (subscapular-to-triceps), waist circumference, and height
a longitudinal study in children from Bogota, Colombia.
Follow-up: 30 months
Vitamin D-deficient children vs vitamin D-sufficient children had:
1) an adjusted 0.1/y greater change in BMI (P for trend = 0.05).2) a 0.03/y greater change in subscapular-to-triceps skinfold-thickness ratio and 3) a 0.8 cm/y greater change in waist circumference

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA MORBIDITY?Other potential mechanisms: obesity
Given that overweight or obesity has been associated with asthma and increased asthma severity in children and adults, it is reasonable but highly speculative to postulate that vitamin D supplementation reduces asthma morbidity through beneficial effects on weight control.
An official American Thoracic Society Workshop report: obesity and asthma.
Dixon AE, Proc Am Thorac Soc 2010;7:325-35.

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA MORBIDITY?Other potential mechanisms: lung function

Relationship between serum 25-hydroxyvitamin D and pulmonary function in the Third National
Health and Nutrition Examination Survey. Black PN, Chest 2005;128:3792–3798.
a cross-sectional survey of 14,091 people > 20 years of age,
spirometry, and serum 25-hydroxy vitamin D levels
Mean increase for the highest quintile of serum 25-hydroxy vitamin D level
(>85.7 nmol/L – 34 ng/mL) compared with the lowest quintile (<40.4
nmol/L - 16 ng/mL).200 –
150 –
100 –
50 –
0
+ 172m
L
FVC FEV1
+ 126m
Lp<0.0001
p<0.0001

HOW COULD VITAMIN D PROTECT AGAINST ASTHMA MORBIDITY?
Other potential mechanisms: regulating expression of
disease-susceptibility genes.

Vitamin D may influence asthma by regulating expression of disease-susceptibility genes.
and some are in auto-immune pathways
in vitro binding of VDR in ~2,500 to 3,500 genes in Lymphoblastoid cell
lines; a fraction (~200-1,000) of these genes are
differentially expressed after calcitriol stimulation
• Ramagopalan SV, Genome Res 2010;20:1352-60. 97.
• Pike JW, J Steroid Biochem Mol Biol 2010;121:130-5.
• Hunninghake GM, BMC Pulm Med 2011;11:17.• Li X, J Allergy Clin Immunol 2011;127:1457-65.• Liu YJ. J Allergy Clin Immunol 2007;120:238-44;

Genome-wide association study reveals class I MCH-restricted T cell-associated molecule gene (CRTAM) variants interact with vitamin D levels to affect asthma exacerbations. Du JACI
2012;129:368
Background It has recently been shown that vitamin D deficiency can increase asthma development and severity and that variations in vitamin D receptor genes are associated with asthma susceptibility.
ObjectiveWe sought to find genetic factors that might interact with vitamin D levels to affect the risk of asthma exacerbation.

Genome-wide association study reveals class I MCH-restricted T cell-associated molecule gene (CRTAM) variants interact with vitamin D levels to affect asthma exacerbations. Du JACI
2012;129:368
• Genome-wide study of gene–vitamin D interaction on asthma exacerbations.• Population-based
and family-based approaches.• 23 polymorphisms.
We identified 3 common variants
class I MHC– restricted T cell–associated molecule gene
(CRTAM) that were associated with an increased rate of
asthma exacerbations
based on the presence of low circulating vitamin D level.

Genome-wide association study reveals class I MCH-restricted T cell-associated molecule gene (CRTAM) variants interact with vitamin D levels to affect asthma exacerbations. Du JACI
2012;129:368
• Genome-wide study of gene–vitamin D interaction on asthma exacerbations.• Population-based
and family-based approaches.• 23 polymorphisms.
We identified 3 common variants
class I MHC– restricted T cell–associated molecule gene
(CRTAM) that were associated with an increased rate of
asthma exacerbations
based on the presence of low circulating vitamin D level.
These results were replicated in a second
independent population.
CRTAM is highly expressed in activated
human CD81 and natural killer T cells, both implicated in asthmatic patients.

Vitamin D and Asthma
Vitamin D deficiency-insufficiency Onset of Disease Morbidity & Exacerbations
Protective Mechanisms Summary & Conclusions
University of Verona,
Italy
Attilio Boner

Vitamin D serum concentrationmodified from G Paul AJRCCM 2011
Lung maturity& development
Viralinfections
Steroidresposiveness Atopy
Asthma morbidity
Lung Function exacerbations Healthcare
utilization
?

Summary & Conclusions
Intervention trials are needed to assess the role of vitamin D supplementation during pregnancy and early in life to prevent asthma initiation.
Findings from several studies suggest beneficial effects of vitamin D on asthma morbidity in relation to prevention of viral infections, enhanced steroid responsiveness, improved lung function.
There is currently weak and inconsistent evidence for a link between vitamin D and atopic responses.

Preliminary intervention studies, suggest an effect of vitamin D on ameliorating ongoing disease but further studies are needed in different groups such as infants, children, adults, and ethnic minorities.
At this time, vitamin D supplementation is recommended for patients who have a serum vitamin D (25[OH]D) level <20 ng/ml, as this could potentially compromise asthma but for sure will impair their musculoskeletal health and may favor the onset of autoimmune diseases.
Summary & Conclusions

Vitamin D deficiency was the causeCourtesy of Holick MF

ACKNOWLEDGMENTS
• Iolanda Chinellato MD
•Michele Piazza PhD
•Giuseppe Gallo student