Tubercolosi, HIV e migrazione: una reale...
22
Miriam Lichtner Dipartimento di Malattie Infettive e Sanità Pubblica Sapienza Università di Roma Polo Pontino Componente dell’ Italian National Focal Point – Infectious Diseases and Migrant” Tubercolosi, HIV e migrazione: una reale emergenza? SESSIONE II -ˇ HIV e Tubercolosi nella persona immigrata
Transcript of Tubercolosi, HIV e migrazione: una reale...

Miriam LichtnerDipartimento di Malattie Infettive e Sanità Pubblica
Sapienza Università di Roma Polo PontinoComponente dell’ Italian National Focal Point –
Infectious Diseases and Migrant”
Tubercolosi, HIV e migrazione: una reale emergenza?
SESSIONE II -ˇ HIV e Tubercolosi nella persona immigrata

HIV, TB, migrazione: PUNTI in comuneHIV, TB, migrazione: PUNTI in comune
Migrazione
TBHIV
•STIGMA
STIGMA
•STIGMA

La lunga storia di Sergej

• Uomo ucraino di anni 36, diagnosi di psoriasi
all’età di 15 aa
• In Italia da 7 mesi
• Ha raggiunto la madre e la sorella a Terracina
• Non parla italiano
• E’ irregolare, non ha STP

È il 2006:
• Dic. 2006: ricovero in un piccolo reparto di mal inf del sud lazio per febbre di NDD:– HIV +, CD4+ Nadir: 72; HIV-RNA : 1.810.000
– HCV +, cachessia (47 Kg)
– (intradermo deb +, espettorato neg)
• Inizia Bactrim, Merrem, Amikacina (?)
• Inizia ART (Reyataz + Norvir+ truvada e poi Sustiva + Truvada per diabete?)

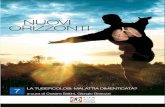
6 Source: Not Ist Super Sanità, 2010; 23(4 suppl. 1)
Proportion of AIDS cases who were unaware of their HIV infection at the time of AIDS diagnosis in Italy (1996-2009)
0% 20% 40% 60% 80% 100%
italians(23,092)
foreigners(3,411)
HI V unaware HI V aware
La diagnosi tardiva è comune tra i migranti sopratutto provenienti dall’Europa dell’est

Fattori associati a diagnosi di HIV tardiva
Variabile OR 95% ICEtà (anni)
<32 1.17* 1.04-1.31>32 - <39 1>39 1.32* 1.20-1.45
SessoFemminile 1Maschile 1.96* 1.76-2.19
Area di origineItalia
Nord 1Centro 1.22* 1.10-1.36Sud 1.29* 1.15-1.44Isole 1.52* 1.32-1.74
Estero 2.67* 2.31-3.09Categoria trasmissione
Tossicodipendente 1Omosessuale 6.24* 5.57-6.98Eterosessuale 9.43* 8.44-10.53Altro/nd 15.60* 13.56-17.95
Anno di diagnosi1996-97 11998-99 2.15* 1.95-2.362000-02 2.36* 2.12-2.61
Dati COA 2008



"We fear the police, and the police fear us": structural and individual barriers and facilitators to HIV medication adherenceamong injection drug users in Kiev, Ukraine.Mimiaga MJ, Safren SA, Dvoryak S, Reisner SL, Needle R, Woody G.SourceHarvard Medical School/Massachusetts General Hospital, Boston, MA, USA. [email protected] has one of the most severe HIV/AIDS epidemics in Europe, with an estimated 1.63% of the population living with HIV/AIDS in 2007. Injection drug use (IDU) remains the predominant mode of transmission in Kiev - the capital and largest city. Prior reports suggest that the HIV infection rate among IDUs in Kiev reaches 33%, and many have poor and inequitable access to highly active antiretroviral therapy (HAART). Among those with access to HAART, little is understood about barriers and facilitators to HAART medication adherence. In May 2009, two semi-structured focus groups were conducted with HIV-infected IDUs seeking treatment at the City AIDS Center, Kiev. The goal was to use this information to adapt and tailor, to Ukrainian culture, an evidence-based intervention for improving adherence to HAART. All 16 participants attributed HIV infection to IDU. Their average age was 31.6 (SD=7.0), average time with HIV 5.7 years (SD=4.0), average time on HAART 2.5 years (SD=1.7), average time as IDU 14.6 years (SD=6.8), and 88% were on opioid substitution therapy. The most salient themes related to adherence barriers included: (1) harassment and discrimination by police; (2) opioid dependence; (3) complexity of drug regimen; (4) side effects; (5) forgetting; (6) co-occurring mental health problems; and (7) HIV stigma. Facilitators of adherence included: (1) cues for pill taking; (2) support and reminders from family, significant other, and friends; (3) opioid substitution therapy; and (4) wanting improved health. Additional factors explored included: (1) knowledge about HAART; (2) storage of medications; and (3) IDU and sexual risk behaviors. Findings highlighted structural and individual barriers to adherence. At the structural level, police discrimination and harassment was reported to be a major barrier to adherence to opioid substitution therapy and HAART. Privacy and stigma were barriers at the individual level. Recommendations for adherence interventions included education, training, and identification cards to show police that medication was for treatment of HIV, not for abuse; and involving family members and other systems of support for HIV treatment.
AIDS Care. 2010 Nov;22(11):1305-13.

TERRITORIO E CLIMA �Situata in Europa orientale, l'Ucraina è circondata al sud dal Mar Nero, a sud-ovest dai Carpazi e al nord è aperta alle influenze polari. Le grandi pianure della parte nord-orientale hanno un inverno molto freddo; la regione di Kiev è coperta dalla neve per almeno 3 mesi. Nelle regioni orientali la nebbia è frequente. A Sud, le zone attorno al Mar Nero hanno temperature più miti. L'estate è lunga. Giugno-luglio sono i mesi in cui piove di più. Nel nord della Crimea ai bordi del mar d'Azov e nelle steppe ucraine sono frequenti tempeste di polvere.��CERTIFICAZIONI
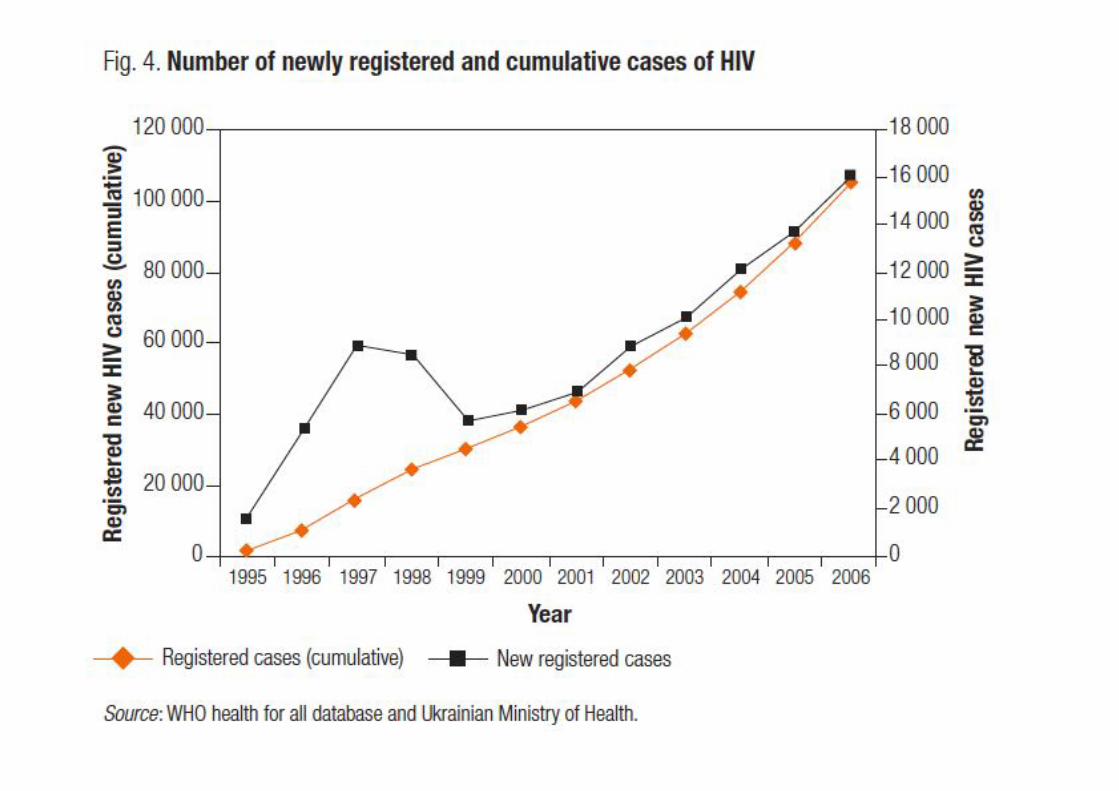
RICHIESTE �Nessun obbligo di vaccinazione per i viaggiatori internazionali. HIV - In Ucraina, i visitatori di età superiore ai 15 anni che intendano stare per più di tre mesi devono produrre un certificato contenente il risultato del test per l'HIV od eseguirlo in Ucraina . Coloro trovati positivi verranno espulsi.��RISCHI PER LA SALUTE �Malattie trasmesse da artropodi - Nei territori boscosi e nelle aree rurali è frequente incontrare l'encefalite da zecche (Tick Borne Encephalitis, TBE) ed il morbo di Lyme. Entrambe sono trasmesse attraverso il morso di zecche infette. Il rischio è maggiore nel periodo primaverile-estivo e primo autunnale durante i quali le zecche sono più diffuse.Contro l'encefalite da zecche esiste un vaccino inattivato (Ticovac-Baxter) sicuro ed efficace, che si assume in tre dosi. Contro la malattia di Lyme, non esiste al momento vaccino e la prevenzione - che vale naturalmente anche per l'encefalite da zecche- deve essere attuata vestendosi con pantaloni lunghi e scarpe chiuse in aree a rischio. Se si viene morsi, la zecca deve esser tolta il prima possibile. Possono verificarsi casi di febbre emorragica di Crimea-Congo. ��Altre malattie trasmesse da alimenti ed acqua - Sono segnalate la febbre tifoide, il colera, altre salmonellosi, la campilobatteriosi e l'epatite A. ��AIDS -L'epidemia continua a crescere. Le diagnosi di HIV sono quasi raddoppiate dal 2000 raggiungendo il numero di 12.400 nel 2004. Il numero non comprende naturalmente tutti coloro- e sono molti- che non si sottopongono al test. La prevalenza nazionale dell' HIV negli adulti è stimata essere del 1.4% (0.8%-4.3%) nel 2005, il che significa 410.000 persone (250.000-680.000). La tossicodipendenza ed il sesso non protetto rappresentano la benzina che fa progredire l'epidemia in Ucraina. In città come Odessa e Simferopol, il 58-59% dei tossicodipendenti èsieropositivo (Ukrainian AIDS Centre, 2005). In Odessa il 67% delle persone dedite alla prostituzione che fa anche uso di droghe è sieropositivo. La trasmissione sessuale dell' HIV sta diventando più comune ed è responsabile di almeno un terzo dei nuovi casi di AIDS. Una parte di essi aveva avuto rapporti con persone dedite all'uso di droghe, ma una percentuale molto ampia non ha all'anamnesi nulla di tutto questo, lasciando intendere che l'epidemia si stia diffondendo attraverso rapporti eterosessuali, coinvolgendo così l'intera popolazione. Il 42% delle nuove diagnosi di HIV è stato riscontrato in donne. In Odessa il 28% di soggetti omosessuali è risultato essere sieropositivo. L'epidemia in Ucraina ha raggiunto lo stadio in cui le morti per AIDS cominciano a crescere. Nei primi sette mesi del 2005, sono morte per AIDS 1138 persone. Il numero di persone che ha accesso agli antiretrovirali è passato dai 400 del 2004 ai 3000 del 2005. ��Altre malattie -Agli inizi degli anni novanta si registrò una vasta epidemia di difterite. Notificati casi di istoplasmosi. Tubercolosi endemica. Epatite B a media endemicità. scheda paese aggiornata il : 30.08.2008Torna indietro
PAESE: Ucraina CAPITALE: Kiev ALTITUDINE: 170 m

AIDS Res Hum Retroviruses. 2006 Aug;22(8):709-14.Molecular epidemiology of HIV Type 1 in Ukraine: birthplace of an epidemic.Saad MD, Shcherbinskaya AM, Nadai Y, Kruglov YV, Antonenko SV, Lyullchuk MG, Kravchenko ON, Earhart KC,
Sanchez JL, Birx DL, Carr JK.SourceU. S. Naval Medical Research Unit No. 3, Cairo, Egypt.AbstractDuring the 1990s, HIV-1 spread rapidly through drug networks in Ukraine and from therethroughout the former Soviet Union. To examine the origins of this epidemic, the genetics of HIV-1 in Ukraine were studied. Proviral DNA from PBMC was extracted and PCR amplified. Part of pol and nearly full genomes of HIV-1 were sequenced and characterized. The predominant genetic form in 163 strains was subtype A (66%), followed by subtypes B (30%), C (2%), D (1%), and a new AB recombinant form (1%). HIV strains from Kiev were diverse having subtypes A, B, C, and D. In Crimea, Donetsk, Poltava, and Odessa, however, the strains were overwhelmingly subtype A, while in Nikolaev subtype B predominated. After the near simultaneous introduction of subtypes A and B in Ukraine, subtype B remained where it was introduced while subtype A spread widely, creating the fastest growing epidemic in the world


Sergej
• Continua febbre…..
• TC suggestiva per miliare
• 15/02/2007: viene trasferito in un grande
ospedale romano riferimento per le malattie
infettive del lazio (hub)


E’ il 2007:
• Espettorato + per M. tuberculosis: diagnosi di
TB bacillifera
• Inizia terapia anti-TB ( 17/2/07): 4 farmaci
• Continua ATRIPLA
• Miglioramento clinico


cc

cc
In ItaliaMortality rate per TB: 0,7/ 100.000 ab