Trattamento con i nuovi farmaci nei pazienti sottoposti a ... · Trattamento con i nuovi farmaci...
39
Maria Rosaria Piras SSD Coordinamento Trapianto di Fegato Azienda Ospedaliera Brotzu Cagliari 19 dicembre 2015 Trattamento con i nuovi farmaci nei pazienti sottoposti a trapianto di fegato
Transcript of Trattamento con i nuovi farmaci nei pazienti sottoposti a ... · Trattamento con i nuovi farmaci...

Maria Rosaria Piras SSD Coordinamento Trapianto di Fegato Azienda Ospedaliera Brotzu Cagliari
19 dicembre 2015
Trattamento con i nuovi farmaci nei pazienti
sottoposti a trapianto di fegato
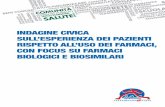
Treatment Pre-LT with the Goal of Preventing HCV Recurrence
Strategy 1: Treat to Cure Antiviral Therapy LT Strategy 2: Treat to Achieve HCV RNA Undectability
SVR No SVR
LT
Antiviral Therapy for 12-24 wks
100% HCV-free post-LT
Antiviral Therapy until HCV RNA negative for ≥ 4 wks
Follow up
100% HCV- infected post-LT
On-Treatment Response 95% HCV-free post-LT if HCV RNA negative at LT

Treatment Pre-LT with the Goal of Preventing HCV Recurrence
Strategy 1: Treat to Cure Antiviral Therapy LT Strategy 2: Treat to Achieve HCV RNA Undectability
SVR No SVR
LT
Antiviral Therapy for 12-24 wks
100% HCV-free post-LT
Antiviral Therapy until HCV RNA negative for ≥ 4 wks
Follow up
100% HCV- infected post-LT
On-Treatment Response 95% HCV-free post-LT if HCV RNA negative at LT
High % of patients achieve TND HCV RNA on DAAs
Shorter duration of therapy
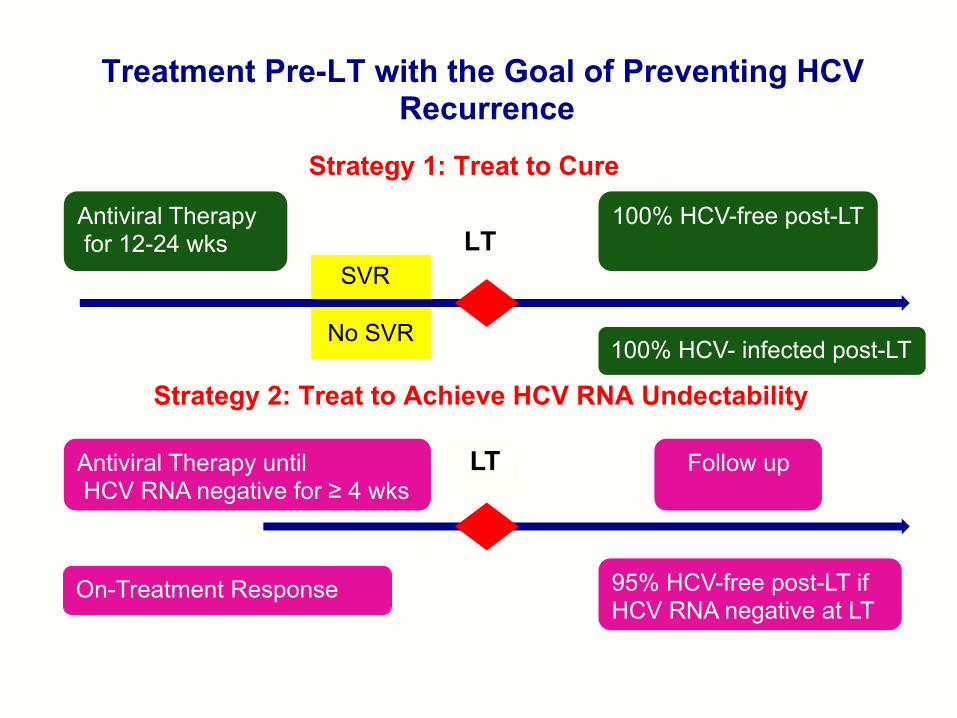
Post-Transplant HCV Recurrence in patients in whom HCV RNA was non detectable for 28 days prior to transplant
0 30 60 90 120 150 180 210 240 270 300 330 360 390
Days with HCV RNA Continuously TND Prior to Liver Transplant
No Recurrence (n=29) Recurrence (n=10)
No recurrence in 24/25 (96%) of patients who maintained HCV RNA TND >28 days
.
28 28
Curry MP et al, Gastroenterology 2015
Cirrhosis + HCC CTP ≤ 7 MELD exception for HCC 48 wks or LT No AEs due to SOF/RBV

47
N=227 HCC 47% GT 1/2/3/4 TE 55% HBsAg+ 5 HIV 10 MELD 13 (6-24) CTP 8 (5-12)
SOF/RBV safe and effective also in decompensated cirrhosis
227 PATIENTS
100 pts OLT
47 patients HCV RNA negative for > 4 wks at OLT
44 pts stop therapy
Positive:5 pts Negative:39 pts SVR12: 87%
Negative:3 pts SVR12:100%
3 pts bridge therapy
53 pts HCV RNA negative for < 4 wks or still positive at OLT
53 pts
19 pts stop therapy
3 deaths
Positive:6 pts Negative:10 pts SVR12:62.5%
34 pts bridge therapy
Positive:1 pts Negative:31 pts SVR12: 97%
10 30 pts 87 pts completed treatment
30 pts discontinued therapy
10 pts died for complications of cirrhosis
1 pt: medical decision 1 donor anti-HCV 1 donor HCV RNA
2 deaths (MOF)
National program for early access to SOF therapy in Italy for patients with chronic hepatitis C in liver LT waiting list
ITACOPS, AISF 2016 (227/243 pazienti, 93.5%)
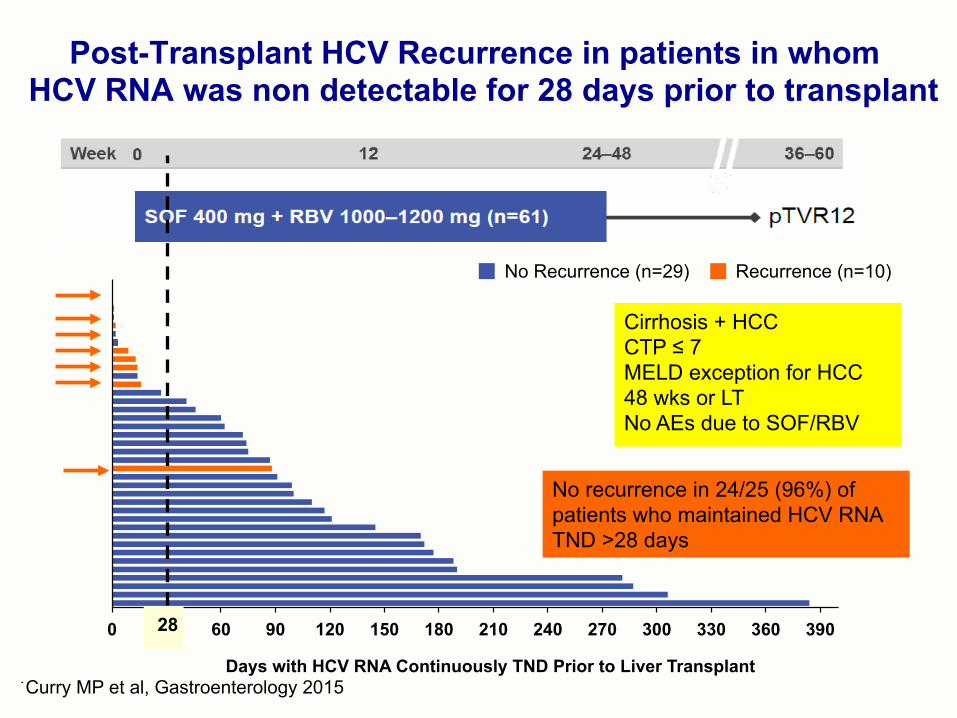
Advanced cirrhosis patients with treatment interrupted by LT could receive an additional 12 wks of treatment immediately post-LT
Advanced cirrhosis N=60
Post-LT N=53
DCV 60 mg QD
SOF 400 mg QD+RBV
Week 0 Week 12 Week 24 Week 36 SVR 12
§ HCV GT 1-75% (GT1a 57%) § IL28B non CC 78% § Naive or experienced patients § DAA failures allowed except NS5A § HCC allowed § CTP B-C 80%
Follow-up
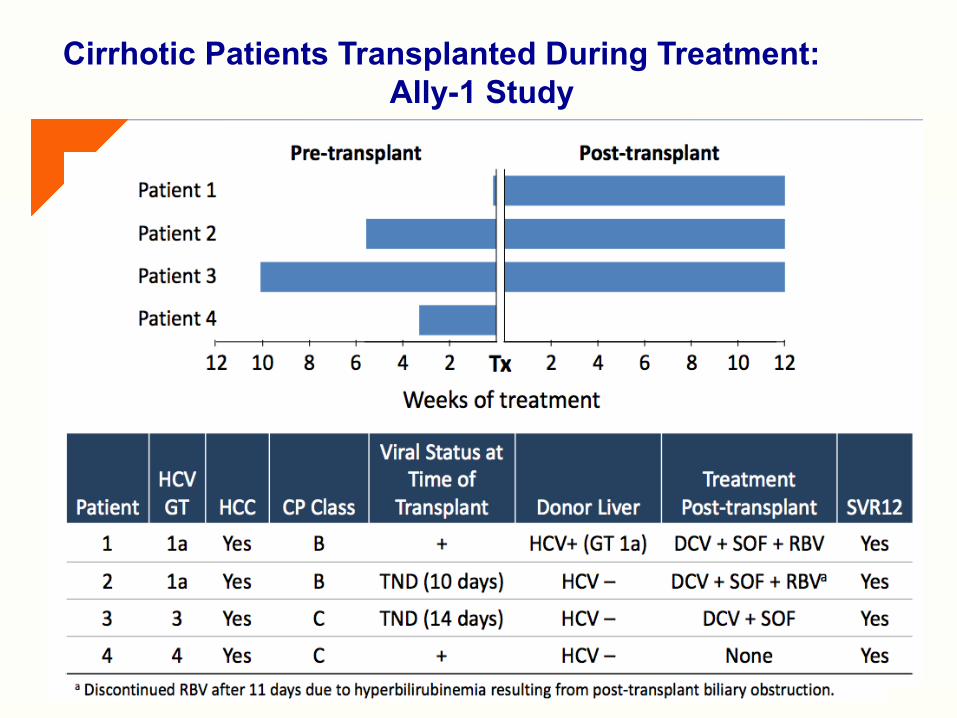
Cirrhotic Patients Transplanted During Treatment: Ally-1 Study
*Discontinued RBV after 11 days due to hyperbilirubinemia resulting from post-LT biliary obstruction
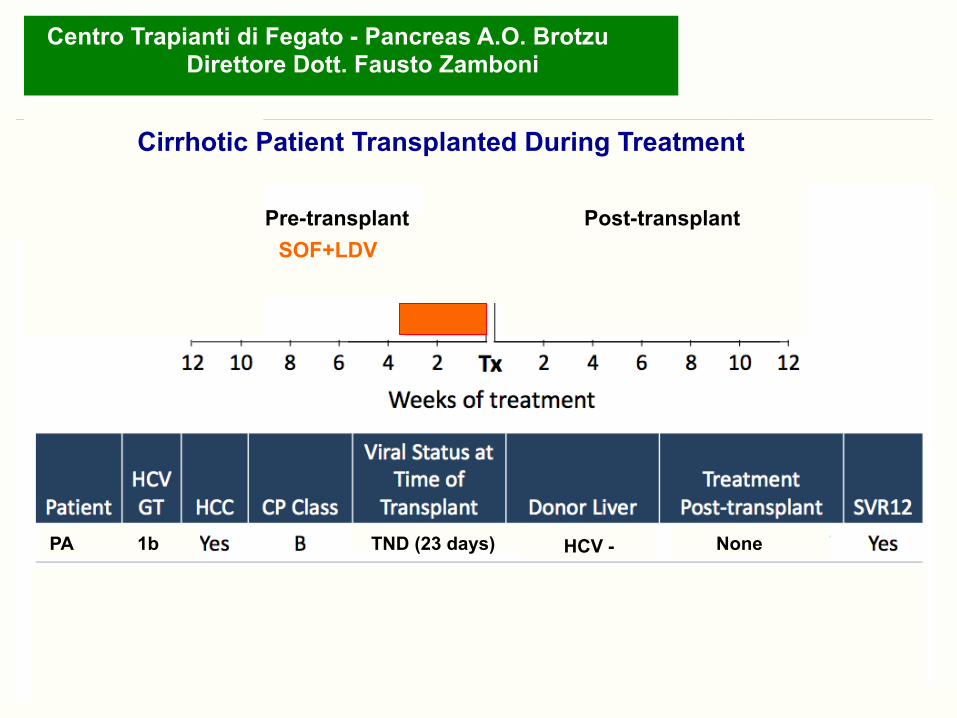
Cirrhotic Patient Transplanted During Treatment
Cirrhotic Patients Transplanted During Treatment:
*Discontinued RBV after 11 days due to hyperbilirubinemia resulting from post-LT biliary obstruction
PA 1b TND (23 days) HCV - None
Pre-transplant Post-transplant
Centro Trapianti di Fegato - Pancreas A.O. Brotzu Direttore Dott. Fausto Zamboni
Cirrhotic Patient Transplanted During Treatment
SOF+LDV
Post-Transplant Antiviral Therapy
Prevent graft loss
Prevent extra-hepatic complications
Reverse complications of decompensation
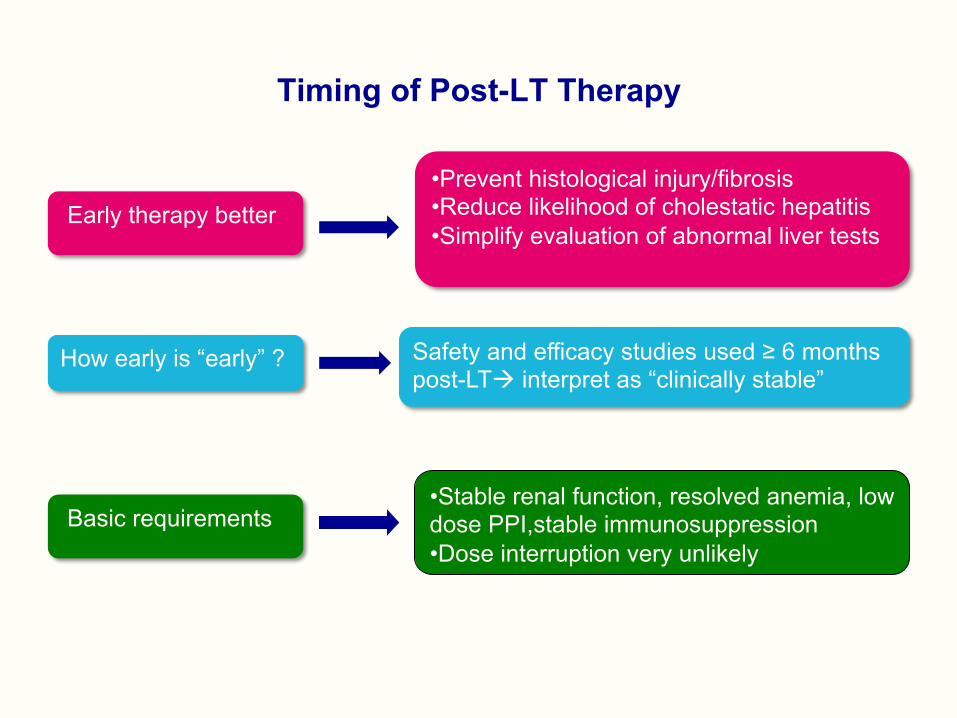
Timing of Post-LT Therapy
• Prevent histological injury/fibrosis • Reduce likelihood of cholestatic hepatitis • Simplify evaluation of abnormal liver tests
How early is “early” ? Safety and efficacy studies used ≥ 6 months post-LTà interpret as “clinically stable”
Basic requirements
Early therapy better
• Stable renal function, resolved anemia, low dose PPI,stable immunosuppression • Dose interruption very unlikely


• N=80 • Male 70% • White 93% • Median age 58 yr • TE 69% • HCV RNA 6.2 log IU/ml • GT1 87% (a=32%) • HBV coinfection 6% • ≥ post LT 3.3 yrs(0.3-21) • Cirrhosis 43% • CTP B/C 43% • MELD > 15 22% • FCH 11% • RBV 30% • TAC 74% • CsA 21% • Everolimus11% • Sirolimus 2% • MMF 51% • Steroids 16% Herzer K et al. AASLD 2015
European DCV Compassionate Use Program
Well tolerated No significant DDI No Rejection
24 wks
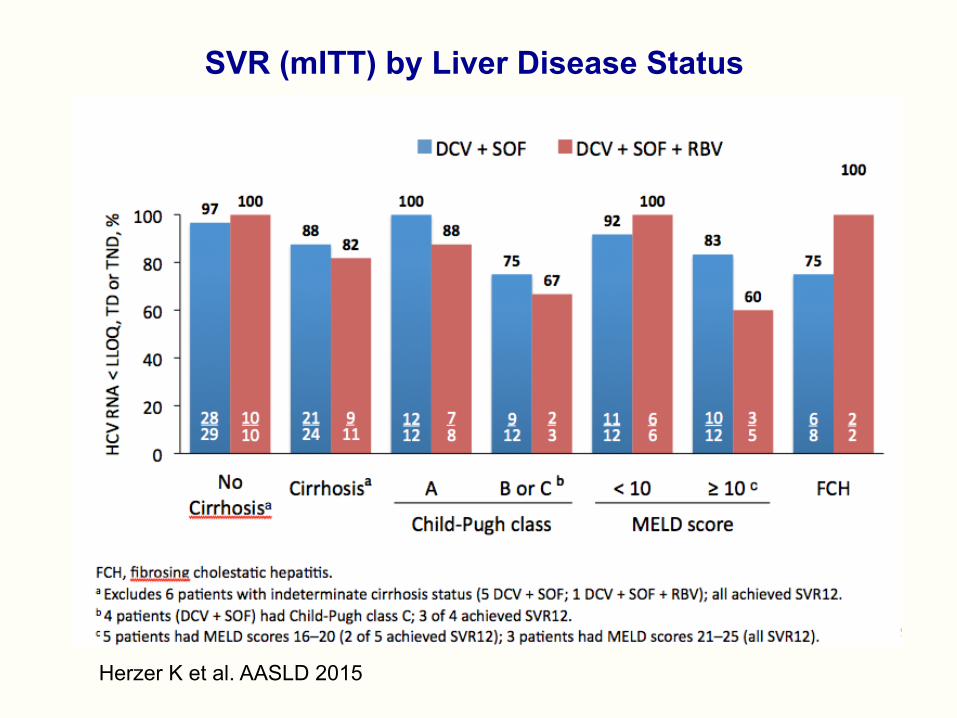
SVR (mITT) by Liver Disease Status
Herzer K et al. AASLD 2015
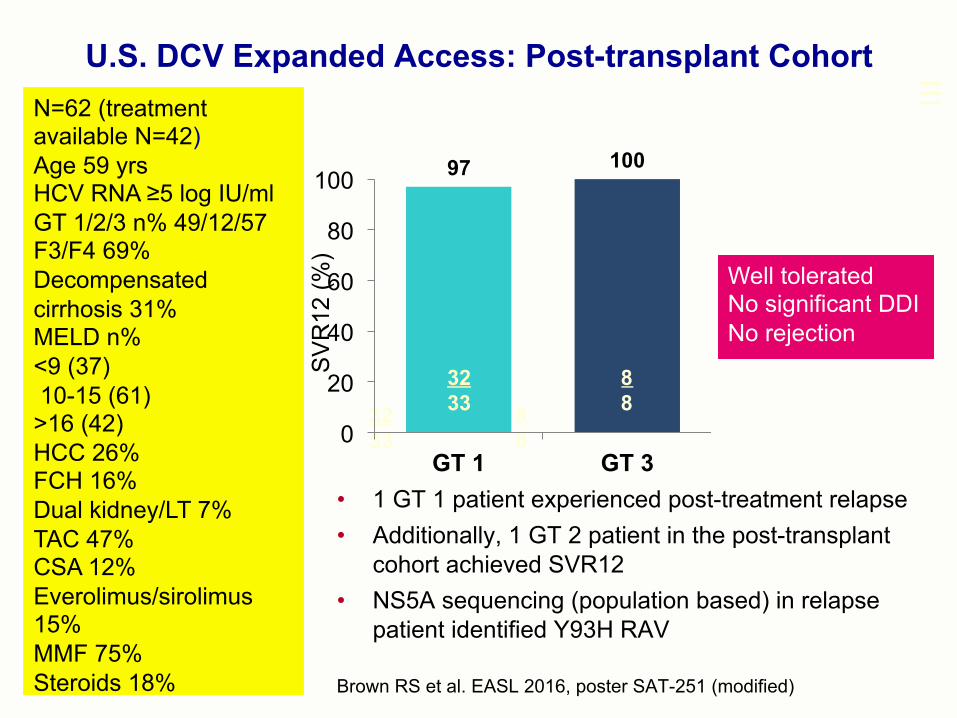
• 1 GT 1 patient experienced post-treatment relapse • Additionally, 1 GT 2 patient in the post-transplant
cohort achieved SVR12 • NS5A sequencing (population based) in relapse
patient identified Y93H RAV
U.S. DCV Expanded Access: Post-transplant Cohort
Brown RS et al. EASL 2016, poster SAT-251 (modified)
32 33
8 8
97 100
0
20
40
60
80
100
GT 1 GT 3
SV
R12
(%)
32 33
8 8
Well tolerated No significant DDI No rejection
N=62 (treatment available N=42) Age 59 yrs HCV RNA ≥5 log IU/ml GT 1/2/3 n% 49/12/57 F3/F4 69% Decompensated cirrhosis 31% MELD n% <9 (37) 10-15 (61) >16 (42) HCC 26% FCH 16% Dual kidney/LT 7% TAC 47% CSA 12% Everolimus/sirolimus 15% MMF 75% Steroids 18%
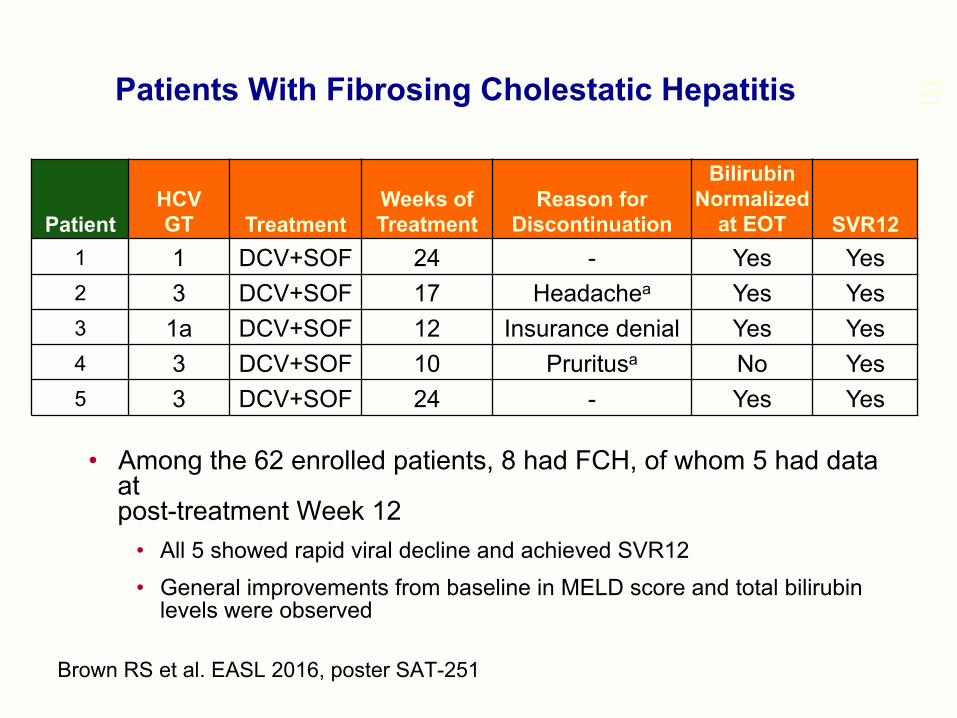
• Among the 62 enrolled patients, 8 had FCH, of whom 5 had data at post-treatment Week 12
• All 5 showed rapid viral decline and achieved SVR12 • General improvements from baseline in MELD score and total bilirubin
levels were observed
Patients With Fibrosing Cholestatic Hepatitis
Brown RS et al. EASL 2016, poster SAT-251
Patient HCV GT Treatment
Weeks of Treatment
Reason for Discontinuation
Bilirubin Normalized
at EOT SVR12 1 1 DCV+SOF 24 - Yes Yes 2 3 DCV+SOF 17 Headachea Yes Yes 3 1a DCV+SOF 12 Insurance denial Yes Yes 4 3 DCV+SOF 10 Pruritusa No Yes 5 3 DCV+SOF 24 - Yes Yes
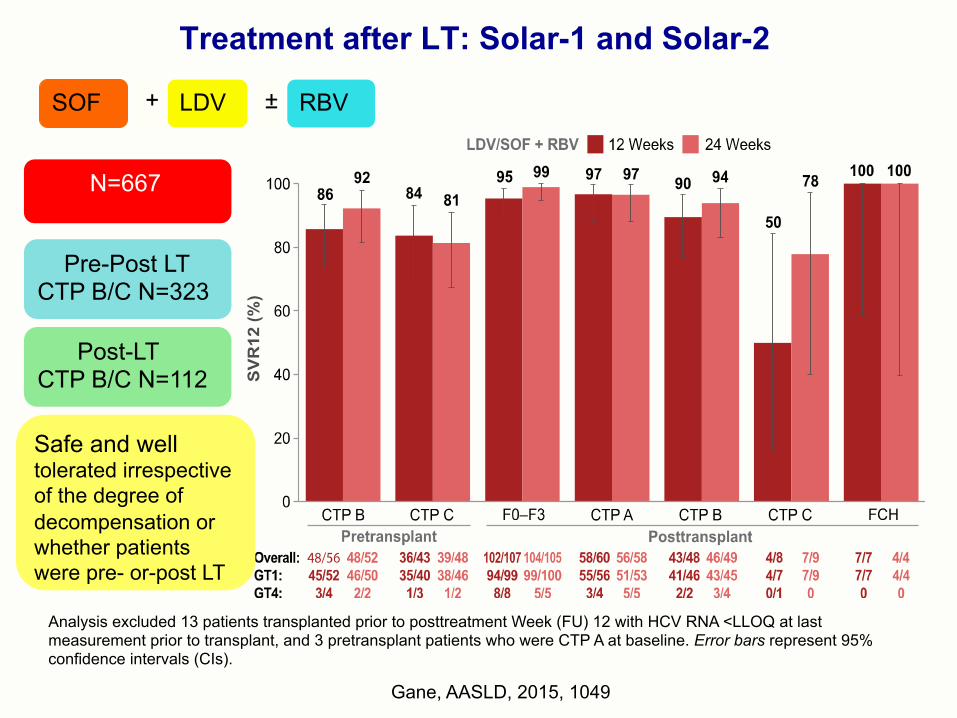
Treatment after LT: Solar-1 and Solar-2
Gane, AASLD, 2015, 1049
Analysis excluded 13 patients transplanted prior to posttreatment Week (FU) 12 with HCV RNA <LLOQ at last measurement prior to transplant, and 3 pretransplant patients who were CTP A at baseline. Error bars represent 95% confidence intervals (CIs).
SOF LDV +
N=667
Pre-Post LT CTP B/C N=323
Post-LT CTP B/C N=112
RBV ±
Safe and well tolerated irrespective of the degree of decompensation or whether patients were pre- or-post LT

Patient Disposition: Post-transplant
Cohort
Treatment outcome available N = 47
Ongoing treatment N =7
Completed treatment N = 48 (87%)
Discontinued prematurely N = 0
Adverse events anemia N =1 5 (27%)
Treatment outcome pending N = 1
Started treatment n=49 (+ 6 retreated) SOF+RBV (compassionate use) =20/ SOF+NS5A n=34/ SOF+RBV n=1
Started treatment n=49 (+ 6 retreated) SOF+RBV (compassionate use) =20/ SOF+NS5Ai n=34/ SOF+RBV n=1
Centro Trapianti di Fegato - Pancreas A.O. Brotzu Direttore Dott. Fausto Zamboni
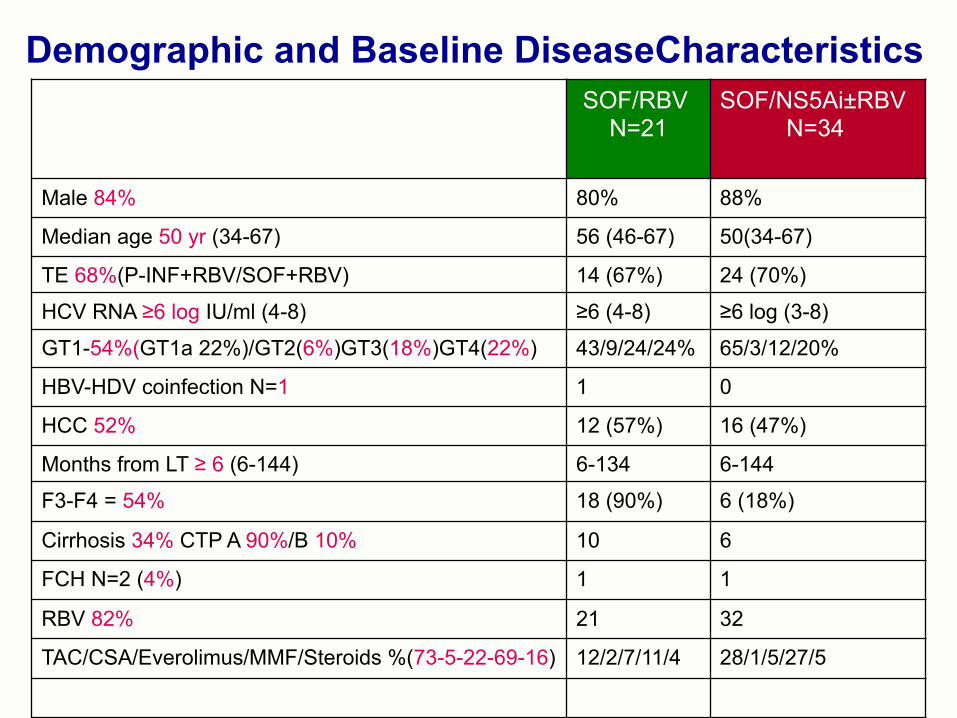
Demographic and Baseline DiseaseCharacteristics SOF/RBV N=21
SOF/NS5Ai±RBV N=34
Male 84% 80% 88%
Median age 50 yr (34-67) 56 (46-67) 50(34-67)
TE 68%(P-INF+RBV/SOF+RBV) 14 (67%) 24 (70%)
HCV RNA ≥6 log IU/ml (4-8) ≥6 (4-8) ≥6 log (3-8)
GT1-54%(GT1a 22%)/GT2(6%)GT3(18%)GT4(22%) 43/9/24/24% 65/3/12/20%
HBV-HDV coinfection N=1 1 0
HCC 52% 12 (57%) 16 (47%)
Months from LT ≥ 6 (6-144) 6-134 6-144
F3-F4 = 54% 18 (90%) 6 (18%)
Cirrhosis 34% CTP A 90%/B 10% 10 6
FCH N=2 (4%) 1 1
RBV 82% 21 32
TAC/CSA/Everolimus/MMF/Steroids %(73-5-22-69-16) 12/2/7/11/4 28/1/5/27/5
• Male 70% • White 93% • Median age 58 yr • TE 69% • HCV RNA 6.2 log IU/ml • GT1 87% (a=32%) • HBV coinfection 6% • ≥ post LT 3.3 yrs(0.3-21) • Cirrhosis 43% • CTP B/C 43% • MELD > 15 22% • FCH 11% • RBV 30% • TAC 74% • CsA 21% • Everolimus11% • Sirolimus 2% • MMF 51% • Steroids 16%
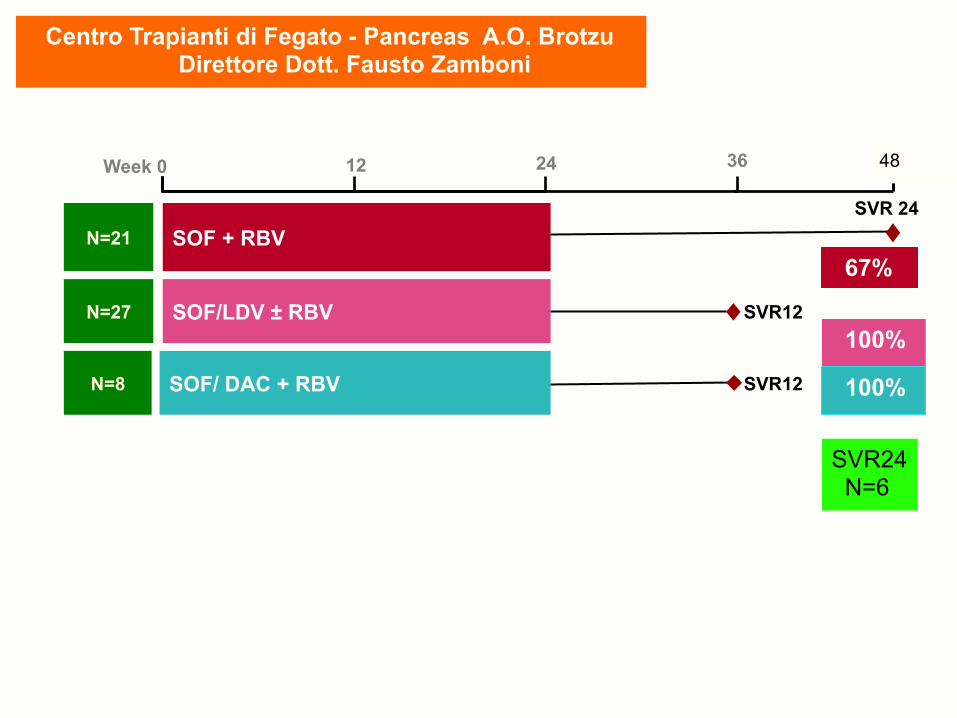
SOF + RBV
SOF/LDV ± RBV
Week 0 12 24 36
N=21
N=27
SVR 24
SVR12
SOF/ DAC + RBV N=8 SVR12
48
67%
100%
100%
SVR24 N=6
Centro Trapianti di Fegato - Pancreas A.O. Brotzu Direttore Dott. Fausto Zamboni

SOF + RBV
SOF/LDV + RBV
Week 0 12 24 36
N=21
N=27
SVR 24
SVR12 100% SVR SOF/ DAC + RBV N=8
67%
SVR12
48
SVR24 N=6
SOF + RBV NR= 7
FCH N=1 GT3
GT1b=3 (F3=1/cirrhosis=2) GT 3 =2 (F3=1/cirrhosis=1) GT4 =1 (cirrhosis=1)
100%
100%
Centro Trapianti di Fegato e Rene-Pancreas A.O. Brotzu Direttore Dott. Fausto Zamboni
Well tolerated No significant DDI No rejection
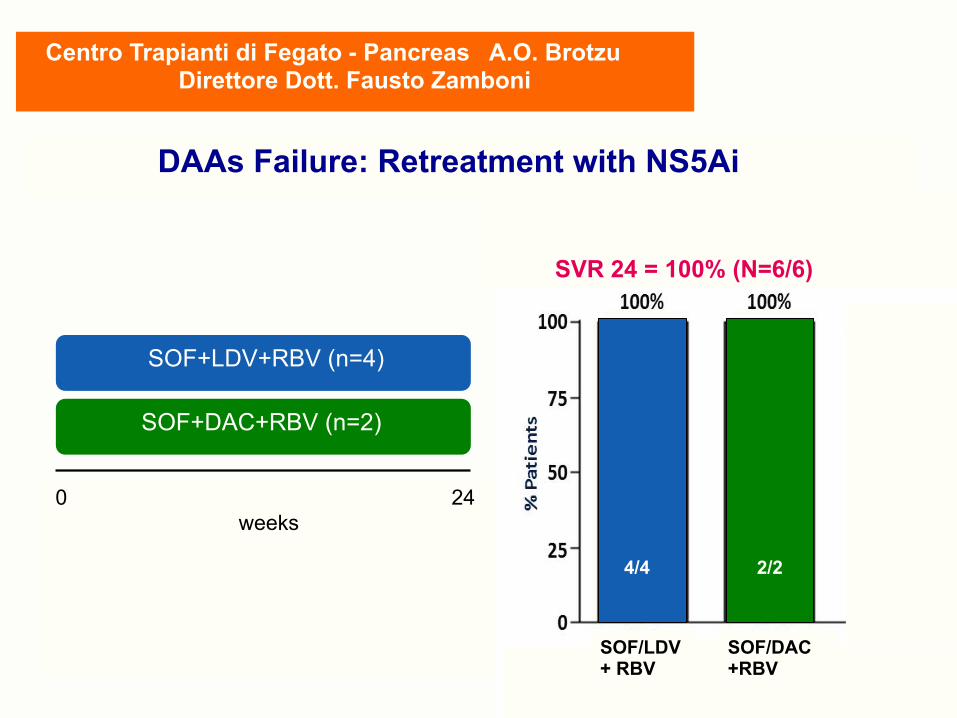
SOF+LDV+RBV (n=4)
SOF+DAC+RBV (n=2)
0 24 weeks
SOF/DAC +RBV
SOF/LDV + RBV
SVR 24 = 100% (N=6/6)
Centro Trapianti di Fegato - Pancreas A.O. Brotzu Direttore Dott. Fausto Zamboni
DAAs Failure: Retreatment with NS5Ai
4/4 2/2

1-Conclusions
• Treatment of HCV infection in patients awaiting LT is a good strategy to prevent HCV graft infection: it will increase survival an simplify post-LT follow-up
• Viral clearance may be associated with improvement in liver function, leading to delisting in some cases
• Treatment is not recommended in patients with very advanced liver disease
• All patients with HCV infection after LT are candidates for IFN-free antiviral therapy
• Treatment is recommended at an early stage of hepatitis C recurrence, preferably when patients are in stable condition
• In those cases of early recurrence (cholestatic forms) treatment shoud be administered as soon as the diagnosis is made

fpost-OLT à NAFLD Insufficienza renale acuta più frequente nel post operatorio Patogenesi multifatoriale e fattori in parte comuni a iperlipemia e diabete Stile di vita, modifiche immunosoppressione Osteopenia e fratture spontanee frequenti soprattutto I° semestre post-OLT Patogenesià m. colestatica, deficit e sintesi ed assorbimento vit.D, Malnutrizione, ipogonadismo, immobilità, diuretici, rapida perdita massa, recente Osteopenia e fratture spontanee frequenti ° semestre post-OLT Patogenesi multiffatoriale: m. colestatiche, deficit sintesi e metabolismo vit.D deficit assorbimanto calcio, malnutrizione, ipoginadismo, allettamento, diuretici rapida perdita massa ossea primo periodo post-OLT, terapia immunosop- pressiva, IRC jatrogena Calcio, vit. D e bifosfonati evidenza utilità Orlistat
Complicanze pre e post Trapianto di fegato
Cise
Centro Trapianti Fegato - Pancreas A.O.Brotzu - Cagliari Direttore: Dott. Fausto Zamboni
SSD Coordinamento Trapianto di Fegato A.O. Brotzu - Cagliari Dott.ssa Laura Mameli Dott.Francesco Sanna Direttore: Dott.ssa Maria Rosaria Piras

fpost-OLT à NAFLD Insufficienza renale acuta più frequente nel post operatorio Patogenesi multifatoriale e fattori in parte comuni a iperlipemia e diabete Stile di vita, modifiche immunosoppressione Osteopenia e fratture spontanee frequenti soprattutto I° semestre post-OLT Patogenesià m. colestatica, deficit e sintesi ed assorbimento vit.D, Malnutrizione, ipogonadismo, immobilità, diuretici, rapida perdita massa, recente Osteopenia e fratture spontanee frequenti ° semestre post-OLT Patogenesi multiffatoriale: m. colestatiche, deficit sintesi e metabolismo vit.D deficit assorbimanto calcio, malnutrizione, ipoginadismo, allettamento, diuretici rapida perdita massa ossea primo periodo post-OLT, terapia immunosop- pressiva, IRC jatrogena Calcio, vit. D e bifosfonati evidenza utilità Orlistat
Complicanze pre e post Trapianto di fegato
Cise
Centro Trapianti Fegato - Pancreas A.O.Brotzu - Cagliari Direttore: Dott. Fausto Zamboni
SSD Coordinamento Trapianto di Fegato A.O. Brotzu - Cagliari Dott.ssa Laura Mameli Dott.Francesco Sanna Direttore: Dott.ssa Maria Rosaria Piras
GRAZIE
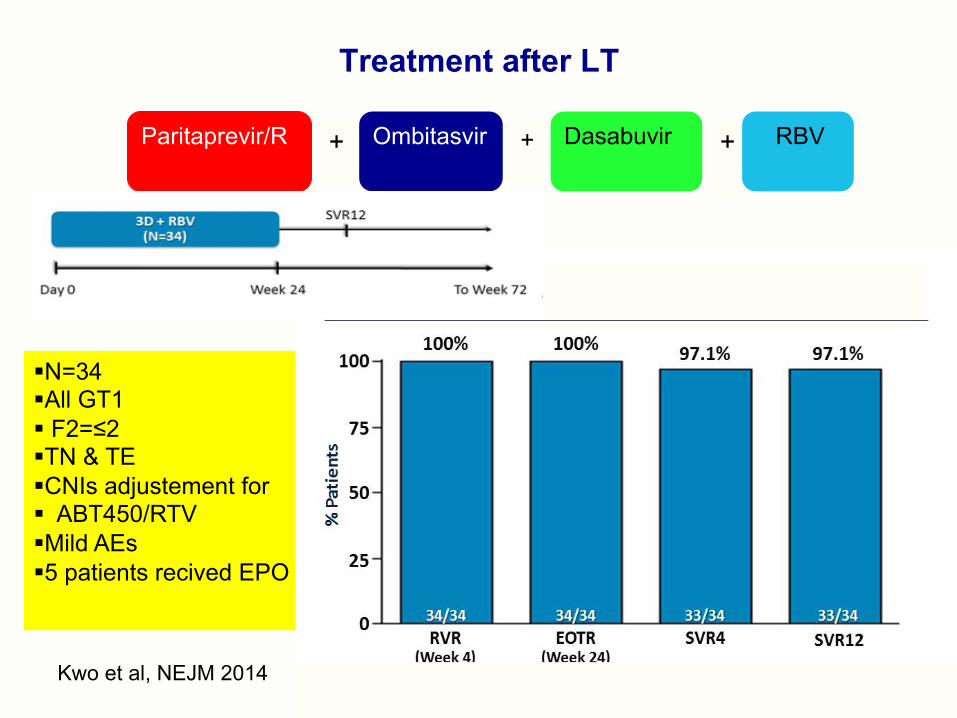
Treatment after LT
Kwo et al, NEJM 2014
§ N=34 § All GT1 § F2=≤2 § TN & TE § CNIs adjustement for § ABT450/RTV § Mild AEs § 5 patients recived EPO
Paritaprevir/R Ombitasvir Dasabuvir + + + RBV
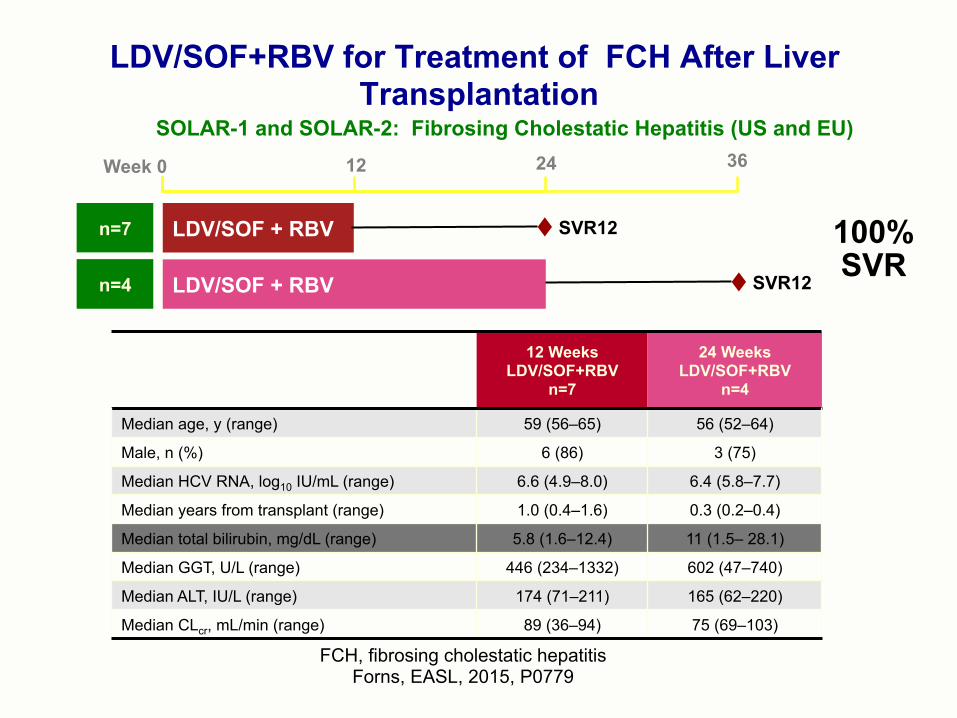
LDV/SOF+RBV for Treatment of FCH After Liver Transplantation
FCH, fibrosing cholestatic hepatitis Forns, EASL, 2015, P0779
LDV/SOF + RBV
LDV/SOF + RBV
Week 0 12 24 36
n=7
n=4
12 Weeks LDV/SOF+RBV
n=7
24 Weeks LDV/SOF+RBV
n=4
Median age, y (range) 59 (56–65) 56 (52–64)
Male, n (%) 6 (86) 3 (75)
Median HCV RNA, log10 IU/mL (range) 6.6 (4.9–8.0) 6.4 (5.8–7.7)
Median years from transplant (range) 1.0 (0.4–1.6) 0.3 (0.2–0.4)
Median total bilirubin, mg/dL (range) 5.8 (1.6–12.4) 11 (1.5– 28.1)
Median GGT, U/L (range) 446 (234–1332) 602 (47–740)
Median ALT, IU/L (range) 174 (71–211) 165 (62–220)
Median CLcr, mL/min (range) 89 (36–94) 75 (69–103)
SVR12
SVR12
SOLAR-1 and SOLAR-2: Fibrosing Cholestatic Hepatitis (US and EU)
100% SVR
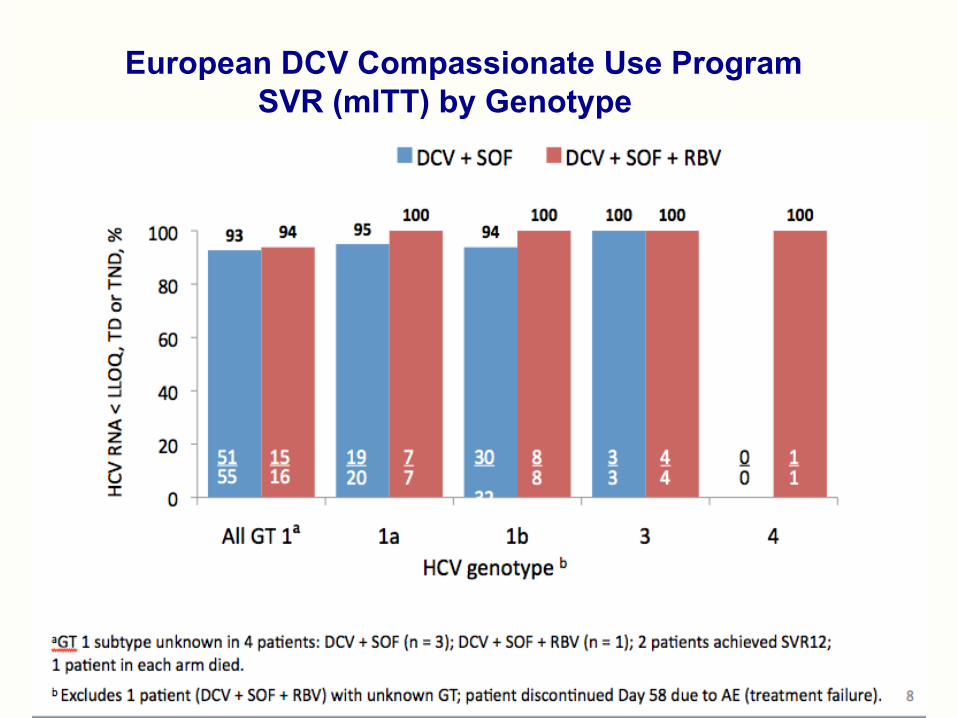
European DCV Compassionate Use Program SVR (mITT) by Genotype
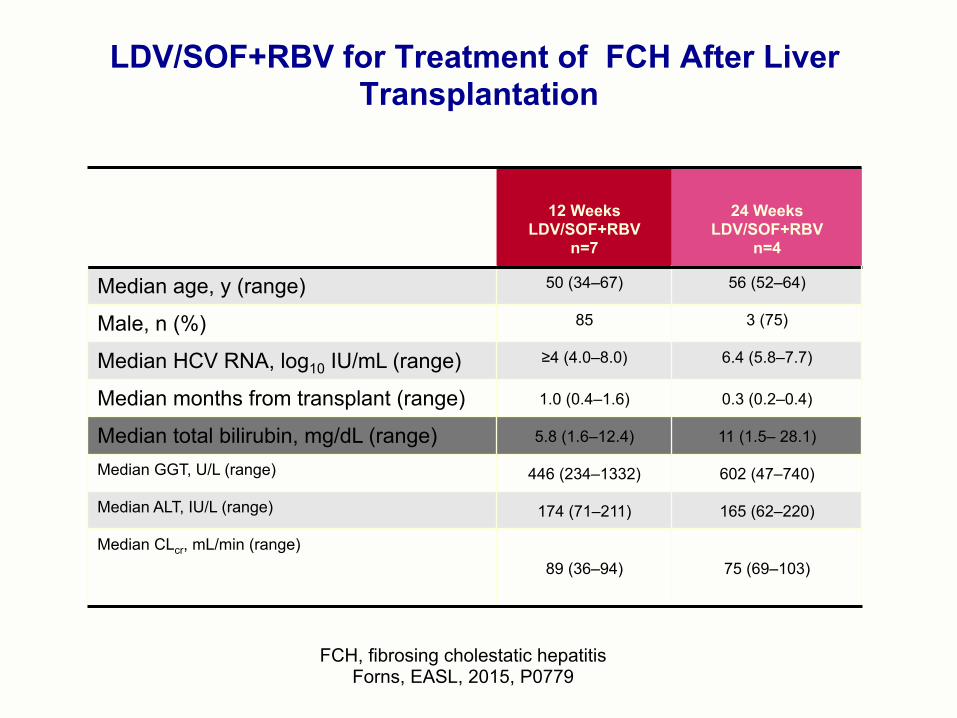
LDV/SOF+RBV for Treatment of FCH After Liver Transplantation
FCH, fibrosing cholestatic hepatitis Forns, EASL, 2015, P0779
12 Weeks LDV/SOF+RBV
n=7
24 Weeks LDV/SOF+RBV
n=4
Median age, y (range) 50 (34–67) 56 (52–64)
Male, n (%) 85 3 (75)
Median HCV RNA, log10 IU/mL (range) ≥4 (4.0–8.0) 6.4 (5.8–7.7)
Median months from transplant (range) 1.0 (0.4–1.6) 0.3 (0.2–0.4)
Median total bilirubin, mg/dL (range) 5.8 (1.6–12.4) 11 (1.5– 28.1)
Median GGT, U/L (range) 446 (234–1332) 602 (47–740)
Median ALT, IU/L (range) 174 (71–211) 165 (62–220)
Median CLcr, mL/min (range) 89 (36–94) 75 (69–103)
• Male 70% • White 93% • Median age 58 yr • TE 69% • HCV RNA 6.2 log IU/ml • GT1 87% (a=32%) • HBV coinfection 6% • ≥ post LT 3.3 yrs(0.3-21) • Cirrhosis 43% • CTP B/C 43% • MELD > 15 22% • FCH 11% • RBV 30% • TAC 74% • CsA 21% • Everolimus11% • Sirolimus 2% • MMF 51% • Steroids 16%

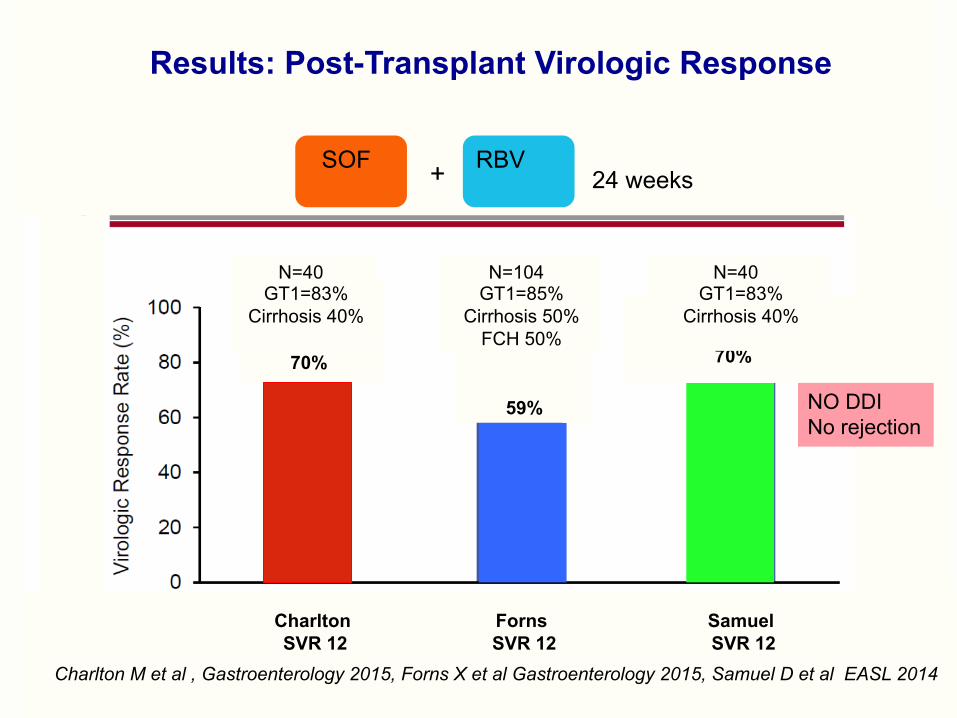
70%
59%
70%
Results: Post-Transplant Virologic Response
SOF RBV + 24 weeks
Charlton M et al , Gastroenterology 2015, Forns X et al Gastroenterology 2015, Samuel D et al EASL 2014
Charlton Forns Samuel SVR 12 SVR 12 SVR 12
NO DDI No rejection
N=40 GT1=83%
Cirrhosis 40%
N=104 GT1=85%
Cirrhosis 50% FCH 50%
N=40 GT1=83%
Cirrhosis 40%
HCV Infection and Liver Transplantation
• Universal reinfection after LT • Negative impact on long-term survival • Up to 1/3 of HCV transplanted patients will develop an accelerated course to cirrhosis within 5 yrs following LT
Berenguer M et al Hepatology 2000;32:852-858Neumann UP et al Transplantation 2004: 77:226-231, Belli L et al Liver Transpl 2007;13:733-740, Burra P et al J Hepatol 2013
HCV infection is the 1° cause of liver transplantation
in industrialized countries
BUT
Recurrence prevention
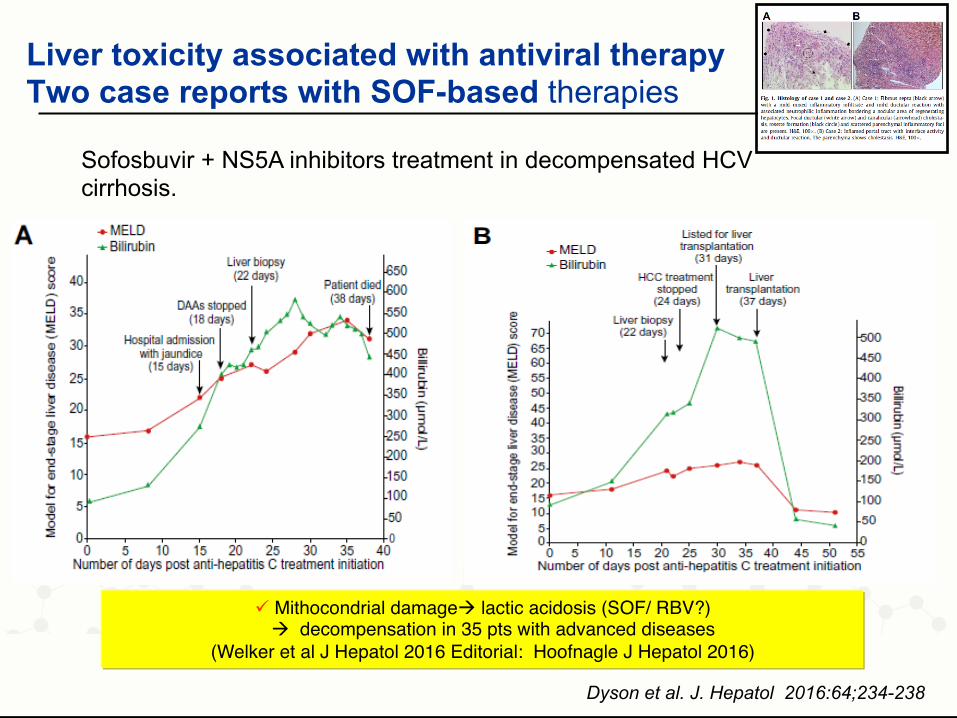
Liver toxicity associated with antiviral therapy Two case reports with SOF-based therapies
Dyson et al. J. Hepatol 2016:64;234-238
ü Mithocondrial damageà lactic acidosis (SOF/ RBV?) à decompensation in 35 pts with advanced diseases
(Welker et al J Hepatol 2016 Editorial: Hoofnagle J Hepatol 2016)
Sofosbuvir + NS5A inhibitors treatment in decompensated HCV cirrhosis.

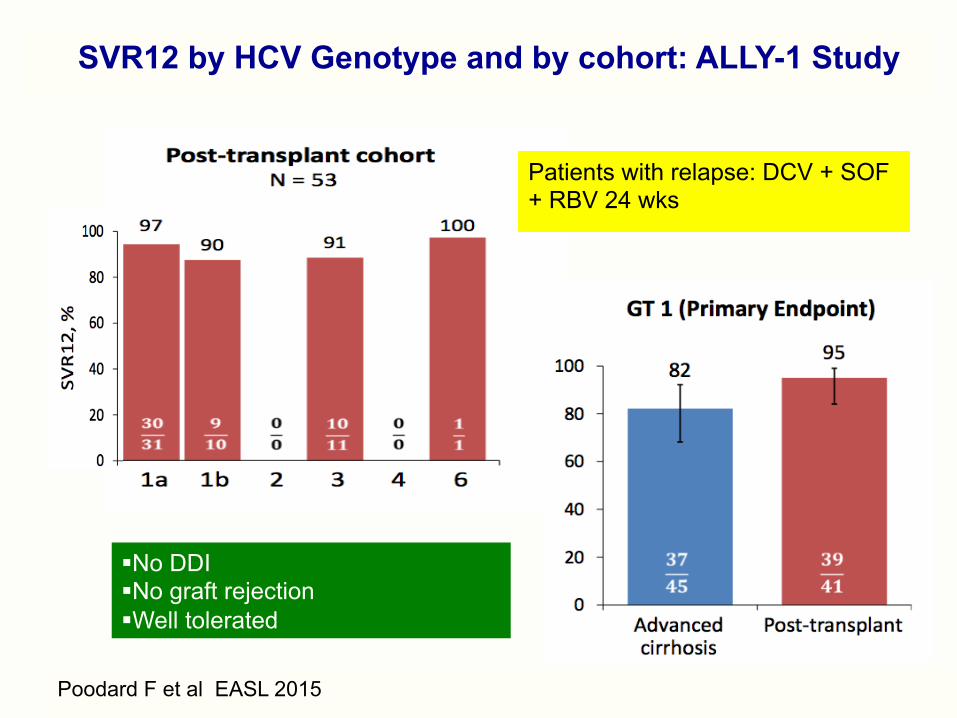
SVR12 by HCV Genotype and by cohort: ALLY-1 Study
§ No DDI § No graft rejection § Well tolerated
Poodard F et al EASL 2015
Patients with relapse: DCV + SOF + RBV 24 wks
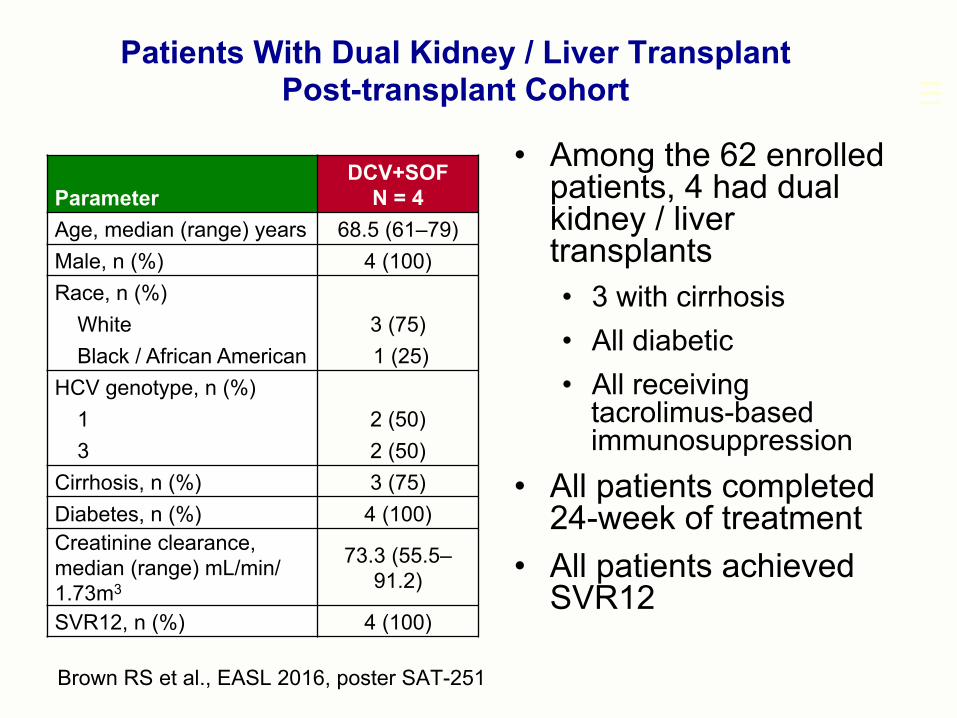
• Among the 62 enrolled patients, 4 had dual kidney / liver transplants • 3 with cirrhosis • All diabetic • All receiving
tacrolimus-based immunosuppression
• All patients completed 24-week of treatment
• All patients achieved SVR12
Patients With Dual Kidney / Liver Transplant Post-transplant Cohort
Brown RS et al., EASL 2016, poster SAT-251
Parameter DCV+SOF
N = 4 Age, median (range) years 68.5 (61–79) Male, n (%) 4 (100) Race, n (%)
White 3 (75) Black / African American 1 (25)
HCV genotype, n (%)
1 2 (50) 3 2 (50)
Cirrhosis, n (%) 3 (75) Diabetes, n (%) 4 (100) Creatinine clearance, median (range) mL/min/1.73m3
73.3 (55.5–91.2)
SVR12, n (%) 4 (100)
70%
59%
70%
Results: Post-Transplant Virologic Response
SOF RBV + 24 weeks
Charlton M et al , Gastroenterology 2015, Forns X et al Gastroenterology 2015, Samuel D et al EASL 2014
Charlton Forns Samuel SVR 12 SVR 12 SVR 12
NO DDI No rejection
N=40 GT1=83%
Cirrhosis 40%
N=104 GT1=85%
Cirrhosis 50% FCH 50%
N=40 GT1=83%
Cirrhosis 40%

Treatment after Liver Transplantation
SOF Simeprevir + 12-24 weeks RBV ±
Author N GT 1 Cirrhosis RBV SVR
Brown R 1 131 82% 60% 22% 91%
Pupapon S 2 109 100%
29% 22% 91%
Te H 3 40 100%
35% (F3-F4)
0% 71%
1-2 AASLD 2014, 3 EASL 2015
Treatment safe and well tolerated
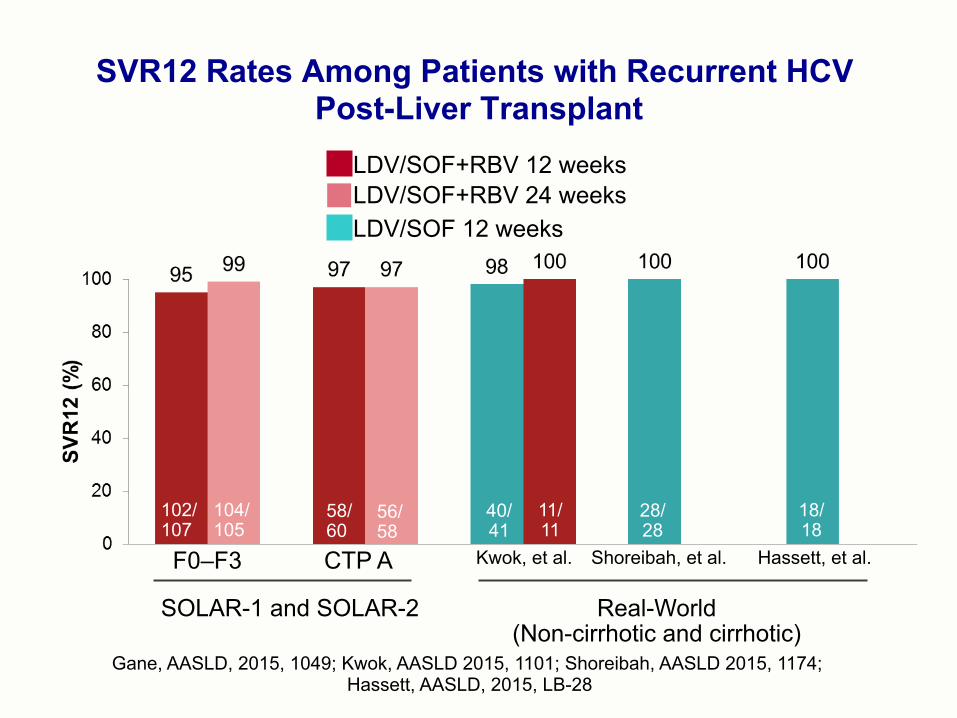
SVR12 Rates Among Patients with Recurrent HCV Post-Liver Transplant
F0–F3 CTP A Kwok, et al. Shoreibah, et al. Hassett, et al.
LDV/SOF+RBV 12 weeks LDV/SOF+RBV 24 weeks LDV/SOF 12 weeks
SOLAR-1 and SOLAR-2 Real-World (Non-cirrhotic and cirrhotic)
40/ 41
11/ 11
28/ 28
18/ 18
102/ 107
104/ 105
58/60
56/ 58
Gane, AASLD, 2015, 1049; Kwok, AASLD 2015, 1101; Shoreibah, AASLD 2015, 1174; Hassett, AASLD, 2015, LB-28