Tra innovazione e sostenibilità: nuovi algoritmi ... · Mieloma Multiplo Il mieloma multiplo è...
36
Tra innovazione e sostenibilità: nuovi algoritmi terapeutici nel mieloma multiplo Alessandro Corso Bolzano 26 ottobre 2017
Transcript of Tra innovazione e sostenibilità: nuovi algoritmi ... · Mieloma Multiplo Il mieloma multiplo è...
Tra innovazione e sostenibilità: nuovi algoritmi terapeutici nel mieloma
multiplo
Alessandro CorsoBolzano 26 ottobre 2017

Mieloma Multiplo
Il mieloma multiplo è una neoplasia ematologica incurabilecaratterizzata dalla presenza di cellule tumorali nel midollo osseo edi una componente monoclonale sierica e/o urinaria
Rappresenta l’1.3% di tutti i tumori e il 13% delle neoplasieematologiche con un’incidenza media ogni anno di 9,5 casi ogni100.000 uomini e 8,1 ogni 100.000 donne
L’età mediana alla diagnosi è di 70 anni
L’incidenza negli ultimi anni è stabile mentre la prevalenza è inaumento per l’allungamento della sopravvivenza dei pazienti con inuovi farmaci

Multiple myeloma


Continued improvement in survival in multiple myeloma:
changes in early mortality and outcomes in older patientsKumar et al. Leukemia 2013
PeriodMedian
OS
2001-2005 4,6 yrs
2006-20106,2 yrs
P=0,002
Period Median OS
2001-2005 3,2 yrs
2006-20105 yrs
P=0,01
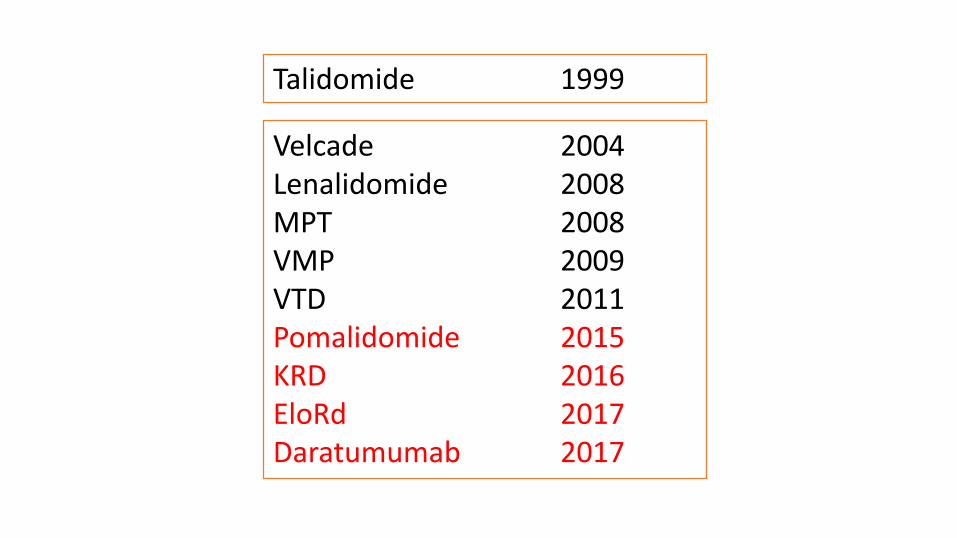
Talidomide 1999
Velcade 2004Lenalidomide 2008MPT 2008VMP 2009VTD 2011Pomalidomide 2015KRD 2016EloRd 2017Daratumumab 2017

Multiple Myeloma Treatment Transformed: A Population-Based Study of
changes in Initial Management Approaches in the United StatesWarren et al. J Clin Oncol 31:1984-1989; 2013
Patients (n. 1,976) with newly diagnosed myeloma in 1999, 2003, and 2007
were examined.
From 1999 to 2007, use of melphalan alone dropped from 32.0% to 4.1%,
and vincristine and doxorubicin use declined from 18.2% to 0.4%. The
percentage of patients receiving any novel agent rose from 3.9% in 1999 to
75.5% in 2007. HSCT increased from 11.1% in 1999 to 21.7% in 2007.
For white patients, use of novel agents was lower for those with Medicare
only (42.6%) than for those with private insurance (50.2%). For patients of
other races, those with Medicare only or Medicaid were less likely to receive
novel agents or transplantation compared with those with private insurance
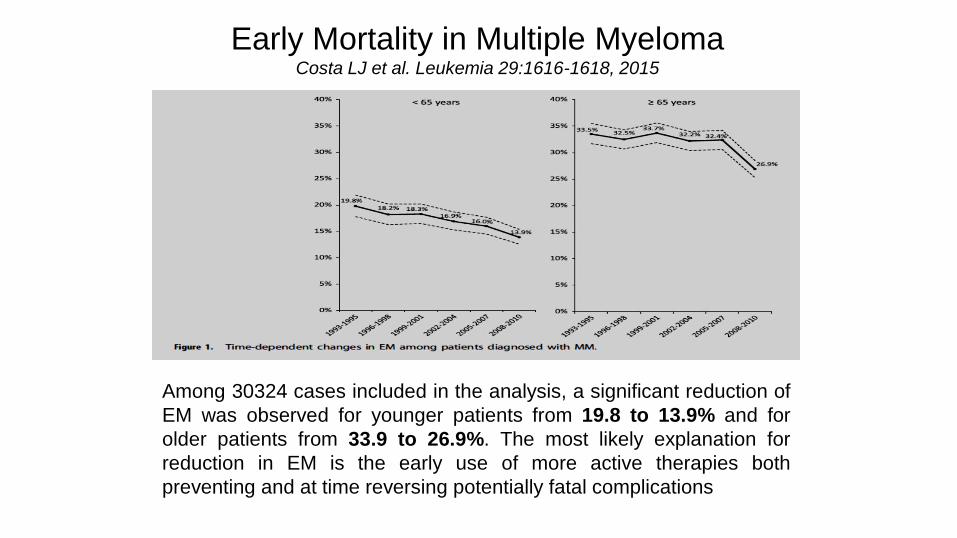
Early Mortality in Multiple MyelomaCosta LJ et al. Leukemia 29:1616-1618, 2015
Among 30324 cases included in the analysis, a significant reduction of
EM was observed for younger patients from 19.8 to 13.9% and for
older patients from 33.9 to 26.9%. The most likely explanation for
reduction in EM is the early use of more active therapies both
preventing and at time reversing potentially fatal complications

Natural History of MM
MGUS or
smoldering
myeloma
Asymptomatic Symptomatic
ACTIVE
MYELOMA
M P
rote
in (
g/L
)
20
50
100
1. RELAPSE
2. RELAPSE
REFRACTORY
RELAPSE
First-line therapy
Plateau
remission
Second-line Third-line

Diagnosis
10 months
1° Relapse
7 months
2° Relapse
6 months
≥3° Relapse
3-4 months
Therapeutic response in patients not transplant
candidates in pre-novel eraKumar et al, Mayo Clin Proc, 2004
Diagnosis
30 months
1° Relapse
15 months
2° Relapse
7 months
≥3° Relapse
4 months
Current therapeutic scenario in MM

MM: Epidemiologia
AIRTUM – 2014
31%
<65 anni
35%
> 75 anni
34%
65-74 anni
INCIDENZA (nord-centro-sud: 6.1-5-4.3/100.000
Regione Piemonte 2006
31%
<65 anni
33%
> 75 anni
36%
65-74 anni
INCIDENZA: 8.9/100.000
Registro Marchigiano MM 2010
32%
< 65 anni
30%
65-75 anni
38%
> 75 anni
INCIDENZA: 7.3/100.000

Trattamento del paziente con mieloma
Eleggibilità a un trattamento intensivo?
Età: fino a 70 e se FIT anche fino a 75 anni (circa il 30% dei pazienti oltre i
70aa)
Età > 70Circa il 50% dei pazienti
osservati
Sì No
Induzione con tripletta (VTD) per 4 cicliTrattamento intensivo con Melphalan
200 mg/m² ed autotrapiantoTrattamento di mantenimento
con lenalidomide
MVP, Rd

AGING HETEROGENEITY
•Older adult are underrepresented in cancer registration trials
•Only 30% of patients are over 65 yrs old
•Older adults included in clinical trials are not the mirror of
what we usually see in clinical practice

Improved survival in myeloma patients: starting to close in on the gapbetween elderly patients and a matched normal population.
Liwing et al. British Journal of Haematology, 2014, 164, 684–693
62%
39%
1638 pts observed between 2001 and 2011

Fig 4. Relationships betweenindividual response categories in thefirst and second lines of therapy
Fig 3. Response distribution nCR/VGPR/PR/NR in thefirst, second, third and fourth lines of therapy.Comparing the population treated with B, T or L to thepopulation treated with conventional drugs
Improved survival in myeloma patients: starting to close in on the gapbetween elderly patients and a matched normal population.
Liwing et al. British Journal of Haematology, 2014, 164, 684–693

Mieloma Multiplo scenario 2015-2019
2015 2016 2017 2018 2019
Revlimid 1L (Lenalidomide) (3Q 2016)
IMID
Celgene
Velcade MCL 1L
Imnovid (Pomalidomide)(3Q 2015)
IMID
Celgene
Farydak(Panobinostat)(2Q 2016)
HDAC
Novartis Kyprolis RR (Carfilzomib)(3Q 2016)
PI
Amgen
Ninlaro RR (Ixazomib)(4Q 2016)
PI
Takeda
Empliciti RR(Elotuzumab)(4Q 2016)
MAb SLAM F7
BMS
Darzalex BT(Daratumumab)2017
Darzalex +VD/RD(Daratumumab)(2017)
Empliciti 1L(Elotuzumab)(2Q 2018)
MAb SLAM F7
Takeda
Kyprolis 1L (Carfilzomib)(3Q 2018)
PI
Amgen
Isatuximab BT(2Q 2019)
MAb CD38
SanofiImnovid RR (Pomalidomide)(3Q 2019)
IMID
Celgene
Empliciti 1L (elotuzumab)(4Q 2019)
MAb SLAM F7
BMS
Ninlaro 1L(ixazomib)(4Q 2019)
PI
Takeda
HDAC
IMIDs
MAbPI

Innovazione nel trattamento
del mieloma multiplo
Incremento costi dei farmaciIncremento sopravvivenza
Miglioramento qualità della vita
Incremento reale dei costi?Diretti (sanitari, non sanitari) e indiretti

Direct Hospital resource utilization and costs of treating patients with multiple myeloma in southwest sweden: a 5-
year retrospective analysis.Ghatnekar O et al, Clinical Therapeutics/Volume 30, Number 9, 2008
The cost of treating Swedish patients with MM
varied greatly between individuals but, overall,
chemotherapy drugs constituted only a minor part
of the total monthly cost (2%), whereas costs for
inpatient stays and therapy-induced adverse
events or comorbidity-related events accounted
for 35% and 42%, respectively. There was no
significant difference in monthly cost between
treatment lines.

Direct Hospital resource utilization and costs of treating patients with multiple myeloma in southwest sweden: a 5-year
retrospective analysis.Ghatnekar O et al, Clinical Therapeutics/Volume 30, Number 9, 2008
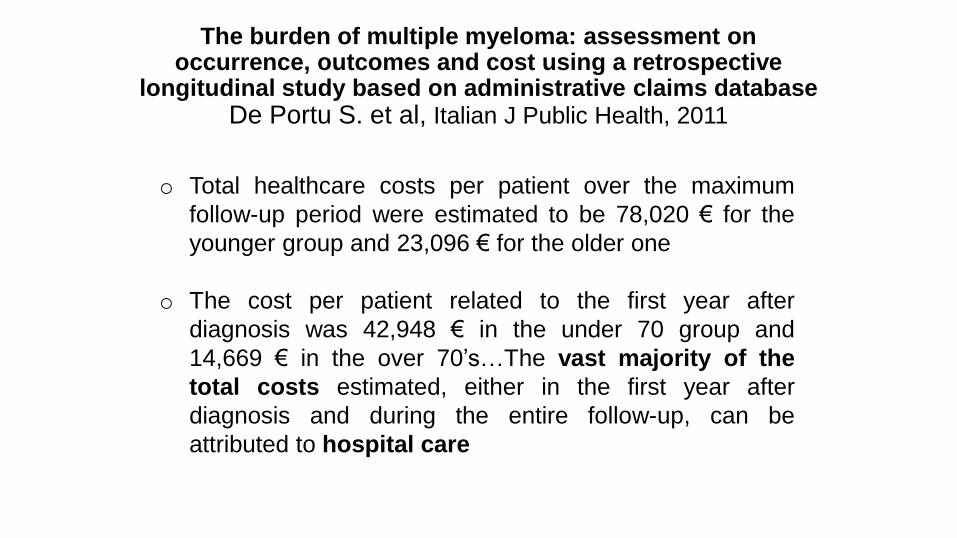
o Total healthcare costs per patient over the maximum
follow-up period were estimated to be 78,020 € for the
younger group and 23,096 € for the older one
o The cost per patient related to the first year after
diagnosis was 42,948 € in the under 70 group and
14,669 € in the over 70’s…The vast majority of the
total costs estimated, either in the first year after
diagnosis and during the entire follow-up, can be
attributed to hospital care
The burden of multiple myeloma: assessment on occurrence, outcomes and cost using a retrospective
longitudinal study based on administrative claims databaseDe Portu S. et al, Italian J Public Health, 2011

Patterns of total cost of economic consequences of progression for patientswith newly diagnosed multiple myeloma patients Arikian SR et al, CMRO 2015

Direct Healthcare Costs of Treated Multiple Myeloma: Results From a Population-Based StudyA. Corso et al. ASH meeting 2014
A retrospective study based on around 10 million people of theItalian Lombardy region performed through an administrativehealthcare databases. The study population was made up of allLombardy residents who, during the period 2003-2009, received adiagnosis of multiple myeloma. The study population was followedup until 31 December 2010.
Myeloma patients were grouped in those treated with CHT(chemotherapy) and SCT (stem cell transplant). Direct healthcarecosts were grouped into three categories: inpatient hospitalizations,outpatient visits, and drug prescriptions.

3,043 patients, observed for 8 years, were included in the analysis:• 925 (30%) treated with SCT, median survival 7.5 years,average cost 125,202• 2118 treated with CHT, median survival 2.8, average cost38,443• hospitalizations and drugs were the drivers of costs in bothgroups• no increase of average costs per patient groups was observedover time, even considering the availability of new and moreexpensive MM specific drugs.
Direct Healthcare Costs of Treated Multiple Myeloma: Results From a Population-Based StudyA. Corso et al. ASH meeting 2014

SCT vs CHT patients: mean cost (€) per patient
during the study period

1,9232,801
66,068
17,042
24,462
10,93414,624
10,336
14,898
10,034
15,597
9,31712,624
8,556
15,939
7,72611,050
6,381
Mean cost (euro) for SCT and CHT patients
by type of cost and year of observation

Baseline FU1 FU2 FU3 FU4 FU5 FU6 FU7 FU8
N. patients 3,043 3,043 2,513 1,840 1,305 881 609 331 146
€/patient 2,534 31,945 15,790 12,061 12,137 12,212 10,492 11,671 8,939
The average cost for SCT patients during the 8 years of study period was 125,202,
72% of which spent during the first 2 years after the index date.

Baseline FU1 FU2 FU3 FU4 FU5 FU6 FU7 FU8
N. patients 2,118 2,118 1,611 1,100 741 475 319 172 66
€/patient 2,800 17,042 10,935 10,336 10,035 9,318 8,555 7,726 6,381
The average cost for CHT patients during the 8 years of study period was 38,443,
73% of which spent during the first 2 years after the index date.
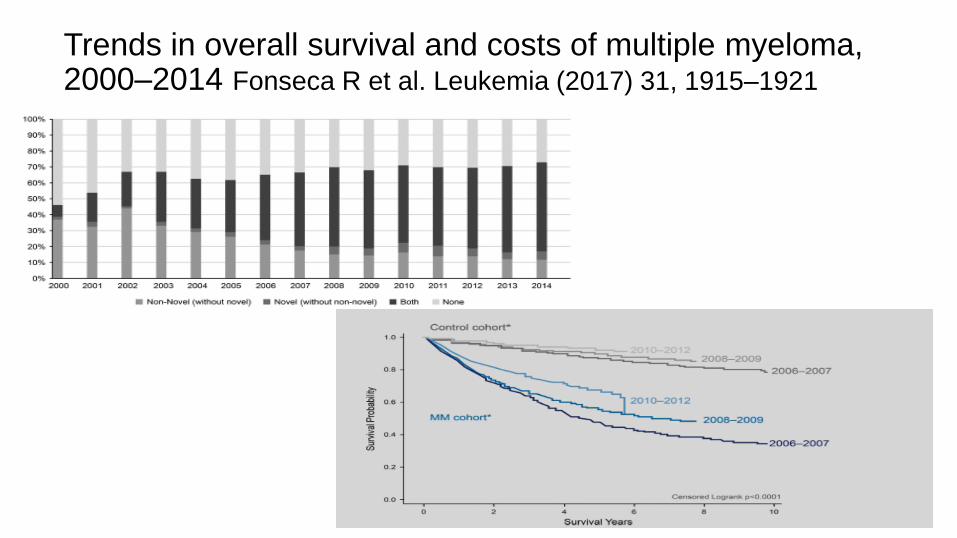
Trends in overall survival and costs of multiple myeloma, 2000–2014 Fonseca R et al. Leukemia (2017) 31, 1915–1921

Trends in overall survival and costs of multiple myeloma, 2000–2014 Fonseca R et al. Leukemia (2017) 31, 1915–1921

The Role of Bortezomib, Thalidomide and Lenalidomide in the Management of Multiple Myeloma
An Overview of Clinical and Economic Information Messori A et al. Pharmacoeconomics 2011; 29 (4): 269-285
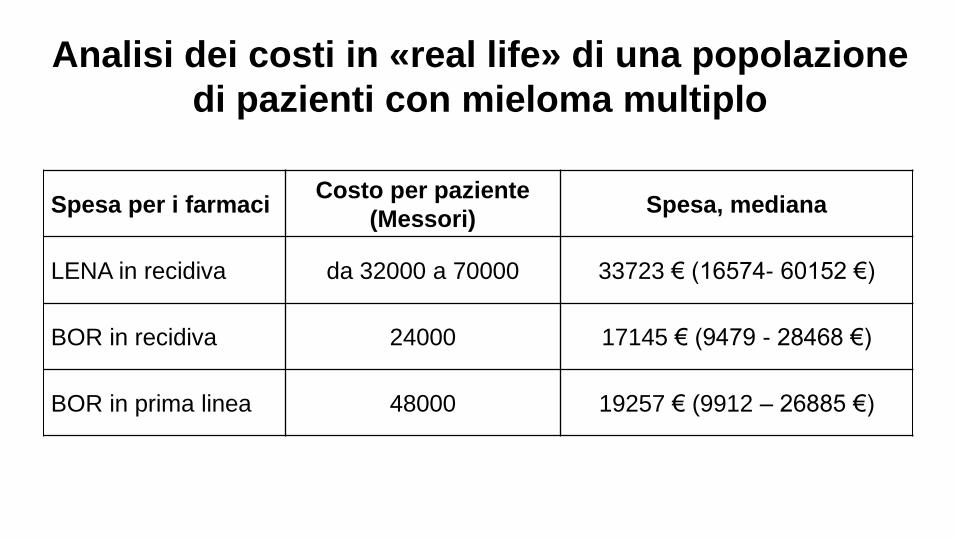
Spesa per i farmaciCosto per paziente
(Messori)Spesa, mediana
LENA in recidiva da 32000 a 70000 33723 € (16574- 60152 €)
BOR in recidiva 24000 17145 € (9479 - 28468 €)
BOR in prima linea 48000 19257 € (9912 – 26885 €)
Analisi dei costi in «real life» di una popolazione
di pazienti con mieloma multiplo

TMO (2008-15) No TMO (2008-15)
Spesa totale della I
linea di terapia60546 (51909-68451) 19257 (9912-26885)
Spese farmaci 623 (23-12220) 8304 (1137-18385)
Spese ambulatoriali 2833 (1674-4059) 1658 (680-3193)
Spese ricoveri 50627 (48371-53192) 3941 (0-8218)
Analisi dei costi in «real life» di una popolazione
di pazienti con mieloma multiplo
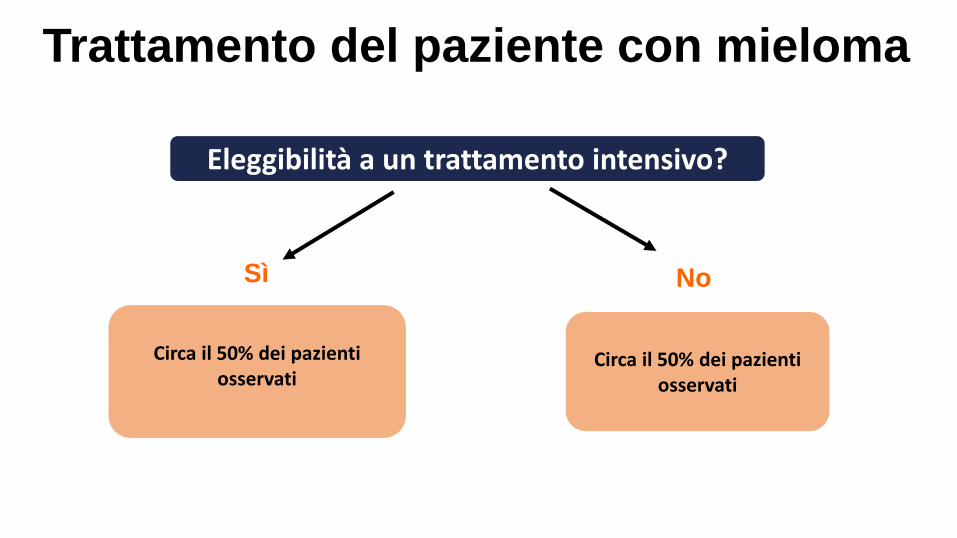
Trattamento del paziente con mieloma
Eleggibilità a un trattamento intensivo?
Circa il 50% dei pazientiosservati
Circa il 50% dei pazientiosservati
Sì No
Debating the Oncologist’s role in defining the value in cancer care: we have duty to society
Jagsi R, J Clin Oncol 2008, vol 32, N 36: 4035-38
“Physicians have a societal responsibility to provide care that minimizes waste. They should develop a culture of financial
stewardship developing explicit standard and norms for professional behavior in order to ensure an appropriate
delivery of high value cancer care to all patients”
Debating the Oncologist’s role in defining the value in cancer care: our duty is to our patients
Sulmasy D, J Clin Oncol 2008, vol 32, N 36: 4039-41
“Physicians should still be free to fulfil their primary duty to act in the best interest of their individual patients within the
practical limits established by society”

Nell’ultima decade la storia del mieloma è cambiata completamente. Le possibilitàterapeutiche sono aumentate in modo esponenziale raddoppiando la sopravvivenzanon solo dei più giovani ma anche di quelli non candidati a terapie ad alte dosi
La disponibilità di nuovi farmaci e la prospettiva di averne molti altri nel giro di pochianni, non solo in ambito ematologico, sollevano problemi di sostenibilità eappropriatezza
Questi per essere affrontati nel modo più corretto dovranno tener conto:
• Diritto alla tutela della salute
• Complessità del paziente e della malattia
• Costi in real life e non su modelli basati sugli studi
• Costo del paziente in toto e mai solo costo dei farmaci
• Ruolo centrale dell’ematologo
Conclusioni