Sindrome dell’Ovaio Policistico: UpDate dei CRITERI ...€¦ · 4 Polycystic Ovary (O) 1 3 2 4....
174
Sindrome dell’Ovaio Policistico: UpDate dei CRITERI DIAGNOSTICI Roberto Mioni MD, PhD Dipartimento di Medicina Clinica Medica 3 – Azienda Ospedaliera di Padova Università di Padova - Padova La Sindrome dell’Ovaio Policistico: Martedì 12 Maggio 2020 PADOVA
Transcript of Sindrome dell’Ovaio Policistico: UpDate dei CRITERI ...€¦ · 4 Polycystic Ovary (O) 1 3 2 4....

Sindrome dell’Ovaio Policistico:
UpDate dei CRITERI DIAGNOSTICI
Roberto Mioni MD, PhD
Dipartimento di Medicina
Clinica Medica 3 – Azienda Ospedaliera di Padova
Università di Padova - Padova
La Sindrome dell’Ovaio Policistico: Martedì 12 Maggio 2020 PADOVA

ANTONIO VALLISNERI, ALLIEVO DEL MALPIGHI,
nel 1721 descrisse:
“giovane rustica e maritata, moderatamente pingue ed infeconda, con due ovaie più grandi del normale, bernoccolute, lucenti e biancastre”
§
Stein I.F. & Leventhal M.L. (1935)Am. J. Obst. Gyn., 29:181-191
“descrissero 7 soggetti di sesso femminile con amenorrea, ovaie ipertrofiche di colorito
bianco madreperlato e con capsula spessa, non conteneti corpi lutei. Avevano inoltre
barba, baffi e peluria terminale diffusa, obese e alcune con ipertrofia della muscolatura
pettorale”
Sindrome dell’Ovaio Policistico dalle sue Origini....
Clinica Medica 3-University of Padua, Italy

(1900)…
Clinica Medica 3-University of Padua, Italy

(1900)…
(2000)…
Clinica Medica 3-University of Padua, Italy

Criteria for Polycystic Ovary Syndromeand Related Disorders
Clinica Medica 3-University of Padua, Italy
1990 – U.S.A.
2003 – Europe
2005 – U.S.A.

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
[Type 2 (H+A)]
[Type 3 (H+O)]
[Type 4 (A+O)]
[Type 1 (H+A+O) – Classical]

Final Report – Executive SummaryDiagnosis of Polycystic ovary syndrome
( Pannel Raccomendations – December 3-5, 2012)
Clinica Medica 3-University of Padua, Italy
Polycystic ovaries
Androgen
ExcessAnovulation
1
3
2
Frank S. J.C.E.M. 2006; 91 (3), 786
4
Polycystic Ovary (O)
1
3
2
4

Androgeni
Carmina E.,Lobo A 2013

PCOS-Criteria of Exclusion
• Hypothyroidism
• Hyperthyroidism
• Enzymatic defect of adrenal steroidogenesis (21-OH-Lyase deficit)
• Hyperprolactinemia (adenoma, drugs, functional)
• Neoplastic androgen secretion
• Drugs with androgenic activity, neuromodulating effects (GABA, EOP, Serotonin, etc.),
• OtherS. Franks J FPl RH 2012, A.Dunaif et a. JCEM 2013

Incidence of Polycystic ovary syndrome( Panidis et al. 2017)
Clinica Medica 3-University of Padua, Italy
• Most common endocrinopathy among women of reproductive age
• Affects approximately 5 million women, approx 10% of US population
• In Europe –Study PCOS reached about 10- 13 % of population
Italian-Study PCOS reached about 10-18% of population (SIE - Club Endocrinologia della Donna 2013-2020)

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOS
Alopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
Dati Anamnestici

Clinica Medica 3-University of Padua, Italy
STORIA FAMILIARE
- Infertilità
- Disturbi menstruali
- Irsutismo, acne, alopecia androgenica nel sesso feminile
- Calvizia precoce nel sesso maschile
- Quadri di sindrome metabolica (obesità, IGT, DM tipo 2, dislipidemia, iperPAO)
- Rischi cardio vascolare o ictus cerebri.
STORIA FISIOLOGICA/PERSONALE
- Peso alla nascita
- Inizio: - dell’adrenarca - dell’ircarca - del pubarca - del menarca
- Irregolarità del ciclo mestruale
- Comparsa obesità
- Stile di vita (anam. alimentare - bilancio dei macronutrienti - attività fisica – fumo)
STORIA PATOLOGICA
- Irsutismo, acne, alopecia androgenica
- Disturbi del ciclo mestruale (oligomenorrea, amenorrea)
- Obesità
- Alterazioni del tono dell’umore (depressione, ansia..)
- Infertilità

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOS
Alopecia
Androgenica
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
Irsutismo

Irsutismo ed ipertricosi
Irsutismo : presenza di un’eccessiva quantità di peli terminali (peli scuri, spessi e lunghi) in zone androgeno-dipendenti (viso, mento, collo , petto, area ombelicale, fondo schiena, regione perianale, braccio, cosce) nelle quali il sistema pilifero, per caratteristiche di sesso, è usualmente assente.
Ipertricosi: aumento della pelosità delle zone non androgeno-dipendenti (dorso, avambraccio, gambe) con peli più corti , sottili e meno scuri, nelle quali il sistema pilifero è usualmente presente.
Clinica Medica 3-University of Padua, Italy

Prevalence of Specific Diagnosis in Patients Presenting with Hirsutism
Clinica Medica 3-University of Padua, Italy
56.8 ± 12.4 %

Prevalence of Specific Diagnosis in Patients Presenting with Hirsutism
Clinica Medica 3-University of Padua, Italy
Prevalence of Hirsutism in PCOS patients( 2003-2012 )
• Orio F. et al. 2003 100 % (n.pz 100)
• Azziz R.et al. 2004 72.2 % (n.pz 873)
• Legro et al. 2006 80.6 % (n.pz 626)
• Diamanti-Kandarakis E. et al 2007 69.5% (n.pz 634)
• Azziz E AE-PCOS Society 2009 74.69% (n.pz 6281)
• Guastella E et al. 2010 91.6% (n.pz 382)
• Huang A et al 2010 72.2 % (n.pz 716)
• Zuliani L. et al 2012 (unpublished) 82.4% (n.pz 578)80.4 ± 11.9

Clinica Medica 3-University of Padua, Italy

A. Rebora et al. Dermatology 2002;205:108-110
Clinica Medica 3-University of Padua, Italy

CRESCITA PILIFERA DIFFERENZIATA per AREE
Zona del % Peli in % Peli in Durata Durata Numero Tasso di Numero Profondità
corpo Telogen ANAGEN Telogen ANAGEN follicoli crescita totale follicolo
per cm2 giornaliera follicoli in Anagen
terminale
(mm)
Cuoio
capelluto 13 85 3-4 mesi 2-6 anni 350 0.35 mm 1 milione 3-5
Guance 30-50 50-70 880 0.32 mm /testa e 2-4
Mento 30 70 10 settim. 1 anno 500 0.38 mm capillizio 2-4
Baffi/
labbro sup 35 65 6 settim. 16 settim. 500 1-2.5
Torace 50 - 60 70 0.30 mm 425000 2-4.5
Zona
pubica 70 30 12 settim. 4 settim 70 3.5-4.75
Braccia 80 20 18 settim. 13 settim. 80 0.30 mm 220000
Gambe
cosce 80 20 23 settim. 16 settim. 60 0.21 mm 370000 2.5-4
Seno 70 30 65 0.35 mm 3-4.5

DURATA della fase ANAGENA
//0 1 2 3 4 12 24 mesi
Cuoio capelluto
Baffi/labbro sup
Pube
Braccia
Gambe/cosce
Mento
Clinica Medica 3-University of Padua, Italy

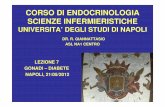
FERRIMAN – GALLWEY Scale
Scala di Ferriman-Gallwey per stabilire il grado di irsutismo. Le nove zone del
corpo androgeno-dipendenti sono valutate da 0 (vello) a 4 (peli terminali con
distribuzione maschile) per calcolare il punteggio totale. Il grado d’irsutismo
normale ha un punteggio inferiore a 8. (Reproduced from Ehrmann et al., 2000.) Clinica Medica 3-University of Padua, Italy

FERRIMAN – GALLWEY Scale
Scala di Ferriman-Gallwey per stabilire il grado di irsutismo. Le nove zone del
corpo androgeno-dipendenti sono valutate da 0 (vello) a 4 (peli terminali con
distribuzione maschile) per calcolare il punteggio totale. Il grado d’irsutismo
normale ha un punteggio inferiore a 8. (Reproduced from Ehrmann et al., 2000.) Clinica Medica 3-University of Padua, Italy
Punteggio totale : 0 – 36
- Irsutismo leggero : 8 – 15- Irsutismo moderato : 16 – 25- Irsutismo grave : > 25
(CUT-OFF > 8)

Clinica Medica 3-University of Padua, Italy

DeUgarte CM et al 2006
mFG hs > 8 California U.S.A.
Gudmundsson JA et al. 2007
mFG hs > 6 Reykjavı´k, Iceland
Welt CK et al 2006
mFG hs > 9 Boston U.S.A.
Diamanti-Kandarakis E. et al. 2016
mFG hs > 9 Atene - GR
Karrer-Voegeli S. et al. 2009
mFG hs > 8 Losanna - CH
Tsan-Hon Liou et al.2016
mFG hs > 6 Taiwan
HY Zhang et al. 2017
mFG hs > 4 Cina
Naiwa S. et al. 2008
mFG hs > 8 Ohio U.S.A.Ibanez L. et al. 2006
mFG hs > 8 Barcellona - E
Merino P et al. 2009
mFG hs > 9 Santiago - Cile
Escobar-Morreale HF et al 2007
mFG hs > 8 Madrid - E
Franks S. et al 2004
mFG hs > 8 Londra - UK
Norman RJ et al. 2004
mFG hs > 8 Adelaide - Australia
Clinica Medica 3-University of Padua, Italy

Moghetti P. et al 2000
mFG hs > 8 Verona.
Bruni V. et al. 2010
mFG hs > 8 Firenze
Gambineri A. et al. 2004
mFG hs > 8 Bologna
De Leo V. al. 2004
mFG hs > 8 Siena
Fruzzetti F. et al. 2009
mFG hs > 8 Pisa
Toscano V. et al 1999
mFG hs > 8 Roma
Mioni R. et al 2002
mFG hs > 8 Padova
Lanzone et al. 2000
mFG hs > 8 Roma
Fulghesu AM et al.2006
mFG hs > 8 Cagliari
Palomba S. et al. 2006
mFG hs > 8 Catanzaro
Orio F. Jr et al. 2003
mFG hs > 8 Napoli- Salerno
Carmina R. et al. 2006
mFG hs > 8 Palermo
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
Ferriman – Gallwey Scale(modified by SOMANI N. et al. 2008)

Visually Scoring Hirsutism (I)( Bulent OY et al Hum Reprod Up 2010 )
Clinica Medica 3-University of Padua, Italy

Visually Scoring Hirsutism (II)( Bulent OY et al Hum Reprod Up 2010 )
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
Ferriman – Gallwey Scale(modified by SOMANI N. et al. 2008)

Ferriman – Gallwey ScoreConfronto Ambulatoriale - Studio Regionale Finalizzato 2001
0
20
40
60
80
100
120
0 2 4 6 8 10 12 14 > 16
MR NX LZ BA
Hormonal Score
n.pa
zient
i (tot
ali 4
82)
(Mioni R. et al 2002)
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, ItalyClinica Medica 3-University of Padua, Italy
Comparison of Ferriman – Gallwey Scale (hs) in PCOS subgroups
H + A + O H + A H + O A + O Control( Type 1 ) ( Type 2 ) ( Type 3 ) ( Type 4 )
11.2 ± 6.7 8.4 ± 4.1 8.2 ± 1.8 4.9 ± 2.2 3.6 ± 1.5Zhang HY et al. 2009n (%) 193 (26.8) 55 (7.6) 96 (13.4) 375 (52.2) 85
16.4 ± 5.7 14.7 ± 9.1 9.6 ± 6.1 4.2 ± 2.4 3.9 ± 2.0Welt CK et al. 2006n (%) 298 (71.0) 7 (2.0) 77 (18) 36 (9.0) 64
11.4 ± 4.0 11.5 ± 5..0 9.4 ± 3.6 3.0 ± 1.0 2.0 ± 1.0Guastella E et al.2010n (%) 206 (53.9) 34 (8.9) 110 (28.8) 32 (8.4) 85
PCOS
13.4 ± 5.8 9.6 ± 3.9 9.6 ± 4.8 4.2 ± 1.8 3.8 ± 1.0Franks S. et al. 2008n (%) 175 (58.2) 34 (11.3) 72 (24.4) 21 (6.1) 62
O
H A
13
2
4

Club SIE (2013-2020)
“Endocrinologia della Donna”
Il Club SIE di Endocrinologia della Donna si propone di riunire i cultori dei variegati aspetti che rendono peculiare il sistema endocrino della donna, al fine
di facilitarne l’interazione multidisciplinare e di realizzare una integrazione dell’attività di ricerca clinica e di base.
In primis, considerando la molteplicità delle problematiche e delle discipline coinvolte e le potenziali prospettive immediate, il Club si propone di realizzare
studi epidemiologici multicentrici su campioni di popolazione ampi, su cui poi organizzare trial randomizzati controllati di intervento e, in campioni
rappresentativi, studi di biologia molecolare, con potenziali prospettive di ricaduta in termini di algoritmi diagnostici e di gestione clinica condivisi. Fra le tematiche che potranno essere inizialmente affrontate nell’ambito del Club vi
sono la PCOS e la sindrome da eccesso di androgeni, le relazioni fra ormoni sessuali, sindrome metabolica e obesità viscerale, le disfunzioni endocrine della
gravidanza, le relazioni fra esercizio fisico e patologia riproduttiva, l’insufficienza ovarica primaria.
I Coordinatori
Luca PERSANI (MI) - Linda VIGNOZZI (FI) – Alessandra GAMBINERI (BO) invitano tutti i Soci interessati a questa tematica a iscriversi e a partecipare all’attività di questo nuovo Club SIE.
S I E

Videodermascopia Computerizzata
( x 20 ) Clinica Medica 3-University of Padua, Italy

Dispositivo Moritex -iScope
Valutazione Videodermoscopica
x 10
Progetto SIE - Club “Endocrinologia della Donna”
Coordinatori: Prof.ri P. Moghetti e C. Moretti
Researcher: Prof. C Moretti - Osp. FateBeneFratelli - Isola Tiberina – Roma
UOC Endocrinologia Diabetologia e Malattie Metaboliche Sezione di Endocrinologia della Riproduzione ed Andrologia Università TorVergata
S I E

Valutazione Videodermoscopica
(Gentilmente fornito dal Prof. C. Moretti – Roma)

Indice Videodermoscopico (IV)
IV 1 ( 1-3 u.p.s/4cm2)
IV 2 ( 4-8 u.p.s/4cm2)
IV 3 ( 9-15 u.p.s/4cm2)
IV 4 (16-37 u.p.s/4cm2)
IV 5 ( > 38 u.p.s/4cm2)
(Gentilmente fornito dal Prof. C. Moretti – Roma)

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
AcneSeborrea

Definition of Acne Vulgaris
• Acne is a multifactorial disease in the sebaceous follicles of the face, chest, and back. which, although not life threatening, has profound effects on patients
• The pathogenesis of acne is thought to be due to a complex interaction between:
- abnormal follicular differentiation
- androgens excess
- sebum production
- anaerobic microorganism Propionibacterium acnes
(P.acnes)
G.F. Weber BMJ 2002;325:475–9
Clinica Medica 3-University of Padua, Italy

The Assessment of Acne
• Grade 1:Simple noninflammatory acne – comedones
and a few papules (B)
• Grade 2:Comedones, papules, and a few pustules (C)
• Grade 3:Larger inflammatory papules, pustules, and a
few cysts; a more severe form involving the
face,neck and upper portions of the trunk (D)
• Grade 4:More severe,with cysts becoming confluent (E)
Witkowski J.A. et al. ,Clinics in Dermatology; 2004;22:394–397
Clinica Medica 3-University of Padua, Italy

The Assessment of Acne
Clinica Medica 3-University of Padua, Italy
I gradoII grado
III grado IV grado

Clinica Medica 3-University of Padua, Italy
Prevalence of Acne vulgaris in PCOS
• Franks S. et al 2001 27.2 % (n pz 300)
• Azziz R.et al. 2004 18.4 % (n.pz 873)
• Rosenfield R.L. et al.2005 10-12 % (n.pz 386)
• Legro R.S.et al. 2006 14.8 % (n.pz 626)
• Welt C.K et al. 2006 10.2 % (n.pz 382)
• Diamanti-Kandarakis E. et al 2009 24.3% (n.pz 634)
• Zuliani L. et al. 2012 22.4% (n.pz 578)
• Zouboulis C.C. et al 2013 24,2 % (n.pz 482)
16.8 ± 6.4

Hormones and the pilosebaceous unit
WC Chen1 and Zouboulis C C Dermato-Endocrinology 1:2, 81-86 2009

Hormones and the pilosebaceous unit
WC Chen1 and Zouboulis C C Dermato-Endocrinology 1:2, 81-86 2009

Hormones and the pilosebaceous unit
WC Chen1 and Zouboulis C C Dermato-Endocrinology 1:2, 81-86 2009

Acne Vulgaris: Pathogenesis
• Acne does not come from bad behaviour.(1)
• Acne is it not a disease of poor hygiene.(2)
• diet has never been shown to have much effect on acne.(3)
• Although most patients exhibit hyper-responsiveness to endogenous androgens rather than frank androgen excess, patients with androgen excess frequently develop acne.(4,5)
1) Hamilton F et al. 2009; 2) Davidovici BB et al.Clin Dermatol 2010;3)Youn SW Clin Dermat 2012;4) Ganceviciene R et al. Dermatoendocrinol 2012; 5) Zouboulis CC J Dtsch Dermatol Ges. 2013
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
Global Acne Grading System (GAGS)
(Doshi et al. 1997

Clinica Medica 3-University of Padua, Italy
VALUTAZIONE CLINICO-TOPOGRAFICA DELL ACNE
Paziente: Cognome_________________Nome:______________; ID:__- Esame obiettivo
H = _______cm; Peso = ______kg ; BMI:_______; W=______; H=______; WHR:_____
- Tipo lesioni: _ comedoni _ papule _ pustole _ noduli _ cisti _ cicatrici _ altro: ………
Sede:_ viso _ _ fronte _ zigomi _ mento _ regione periorale
_ dorso
_ regione sternale
_ arti superiori _ _ spalle _ braccia
Grado:n° comedoni __ <5 __ 5-15 __ 16-25 __ 26-35 __ >35
n° papule __ <5 __ 5-15 __ 16-25 __ 26-35 __ >35
n° noduli __ <5 __ 5-15 __ 16-25 __ 26-35 __ >35
- Global Acne Grading System (Doshi A. et al., Int. J Dermatol 1997 modificato)
• Score regionale:Grade:
0 __ no lesioni
1 __ 1 comedone
2 __ 1 papula
3 __ 1 pustola
4 __ 1 nodulo
• Fronte ………x 2 =………+
• Guancia dx ………x 2 =………+
• Guancia sin ………x 2 =………+
• Naso ………x 1 =………+
• Mento ………x 1 =………+
• Torace/dorso ………x 3 =………=
- GS= ______ (GS = 1-18 acne lieve; 19-30 acne moderata; 31-38 acne severa; >39 acne molto severa)
Global score modificato = somma scores regionali/n° delle regioni coinvolte =....../…….=……
- Segni clinici associati: _ irsutismo/ipertricosi _ obesità _ alopecia androgenetica _ seborrea

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOS
Alopecia
Androgenica
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
AlopeciaAndrogenica
Irsutismo

Clinica Medica 3-University of Padua, Italy
Female AndroGenic Alopecia (FAGA)(Ludwing’ Scale)
- FAGA Degree I (Minimal) It is considered as the beginning of FAGA there is a
perceptible thinning of hair from the anterior part of
the crown with minimal widening of the part width.
-FAGA Degree II (Moderate): The “crown” area of thinning will be more evident
because of an increase in the number of thin and short
hairs.
-FAGA Degree III (Intense):The “crown” becomes practically total alopecia or
denuded,” with significantwidening of the part width,
but the frontal hairline is maintained.

Female AndroGenic Alopecia of Male Pattern (FAGA - M)
(Olsen’ Scale)
- FAGA - M Degree I (Minimal)
- FAGA - M Degree II (Moderate)
- FAGA – M Degree III (Intense)
Clinica Medica 3-University of Padua, Italy

Female AndroGenic Alopecia of Male Pattern (FAGA - M)
(Olsen’ Scale)
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
• Futterweit et al. 1988 36.5 % (n.pz 40)
• Franks S. et al 2000 3.2 % (n pz 300)
• Vexiou P. et al.2000 10.8 % (n.pz 110)
• Balen A.H.et al. 2002 6.8 % (n.pz 174)
• Cela E. et al. 2003 12.3% (n.pz 87)
• Welt C.K et al. 2006 14.2 % (n.pz 382)
• Karrer-Voegelis S. et al 2012 24,2 % (n.pz 179)
Prevalence of Androgenic Alopecia (FAGA)in PCOS
15.4 ± 9.6

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
Esami di Laboratorio

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy


Ovarian Regulatory System in PCOS
Clinica Medica 3-University of Padua, Italy
HYPERINSULINEMIA HYPERANDROGENISM
SHBG
AROMATASE ACTIVITY(fat, muscle, skin)
T
A
LH
(Nestler et al 2000 modified)
Chronic ANOVUATION
LEPTIN

Clinica Medica 3-University of Padua, Italy
Iperandrogenismo Biochimico
Definizione : presenza di elevati valori plasmatici di
ormoni steroidei ad attività androgenica a prescindere
dalla loro origine (surrenalica, ovarica, periferica,
iatrogena/factitia)
• Testosterone: > 1.67 nmol/L (> 0.57 ng/dL) *
• Androstenedione: > 9.4 nmol/L (>2.4 ng/mL) *
• DHEA-s: > 8.5 μmol/L (>2.8 ng/mL) *
• 17-OH-Progesterone: > 2.5 nmol/L e < 6.0 nmol/L(< 3.0 ng/mL) *
• FAI > 4.0
* prelievi avvenuti entri i primi 7 gg del ciclo spontaneo o dopo somministrazione di MAP(10 mg x 7 gg) su nostri pazienti (oltre 400 soggetti di età compresa tra 13 e 38 aa)(Mioni R 2002-2006 dati personali – aggiornati al 2017)

Clinica Medica 3-University of Padua, Italy
Percorso Diagnostico della Sindrome dell’Ovaio Policistico

Clinica Medica 3-University of Padua, Italy
Indagini di Laboratorio(entro i primi 7 gg del ciclo mestruale (se presente)
β-hCG * (amenorrea)
TSH (fT4)
Prolattina (dopo 20’ di riposo)
LH, FSH (LH/FSH > 2.0) *
Testosterone totale, (Tfree)
SHBG
DHEA-S
Androstenedione
17-OH Progesterone

Clinica Medica 3-University of Padua, Italy
Basal Hormonal Parameters of PCOS
LH / FSH (> di 2) 62-68 %
Prolactin (dopo 20’ di riposo) 38-46 %
Testosterone (Total) 56-68 %
Testosterone (Free) 68-76 %
SHBG 46-62 %
FAI (Tt(nmol/L) x SHBG(nmol/L) : 100) 64-74 %
DHEA-S 48-54 %
Androstenedione 64-78 %
17-OH Progesterone 46-56 %
17-β- Estradiol 12-18 %

The Endocrine Society
College of American Pathologists (CAP)
Nelle donne e nei bambini la determinazione del Te sierico è
inaccurata, imprecisa, poco sensibile e selettiva limitandone
l’utilizzo nella diagnosi clinica
Il Concilio della “Endocrine Society” ha formato una “task
force” di cinque esperti per esaminare il problema e produrre
soluzioni adeguate(Rsner et al. - J Clin Endocrinol Metab, February 2007)

Quale metodo analitico utilizzare per la diagnosi di PCOS?
o
ECLIA Elecsys
Modular E-170 RocheLC-MS/MS

LA NOSTRA ESPERIENZA
Novembre 2011
Dott. Carlo Artusi
Dipartimento Medicina Laboratorio - Azienda Ospedaliera
Direttore: Prof. M. Plebani
Richiesta clinica di valutare un test più accurato e sensibile per la
determinazione del testosterone sierico per la diagnosi di PCOS

n Min 1st Quartile Median 95% CI 3rd Quartile Max IQRIMM 123 0,10 0,402 0,970 0,850 to 1,150 1,470 5,63 1,068
MASSA 123 0,08 0,732 1,150 1,010 to 1,320 1,580 6,70 0,848
Confronto metodi LC-MS vs ECLIA

Confronto metodi LC-MS vs ECLIADeming regression
inferiori a 1.20 nmol/L con ECLIA
LOQ=0.165 nmol/L
LOQ=0.416 nmol/L

LC-MS ECLIA
1,80 1,40
1,87 0,71
1,88 2,03
1,93 0,35
1,93 1,42
2,00 1,06
2,00 1,80
2,03 1,66
2,05 1,37
2,06 1,56
2,13 2,00
2,25 1,80
2,30 1,40
2,30 2,20
2,45 2,58
2,55 1,68
2,70 1,94
3,00 3,44
3,10 3,52
3,15 3,27
3,30 2,02
3,60 3,12
4,90 4,82
6,70 5,63
ECLIA LC-MS
1,80 2,25
1,80 2,00
1,90 0,95
1,94 2,70
1,95 1,60
2,00 2,13
2,02 3,30
2,03 1,88
2,17 1,05
2,20 2,30
2,58 2,45
3,12 3,60
3,27 3,15
3,44 3,00
3,52 3,10
4,82 4,90
5,63 6,70
Confronto metodi LC-MS vs ECLIA
Cut-off Te nella PCOS 1.8 nmol/L*
Pazienti con Te < 1.8 nmol/L in ECLIA = 17
Concordanza con LC-MS = 15 su 17 (88.2%)
Pazienti con Te < 1.8 nmol/L LC-MS = 24
Concordanza con ECLIA = 13 su 24 (54.16%)
( * Bart H.J.,Eur J Endocrinol 162, 2010)
Determinazione del Te sierico in
123 pazienti donne

Confronto metodi LC-MS vs ECLIA
Cut-off Te nella PCOS 3.0 nmol/L
Pazienti con Te > 3.0 nmol/L in LC-MS = 7
Concordanza con ECLIA = 6 su 7 (86%)
Pazienti con Te > 3.0 nmol/L in ECLIA = 6
Concordanza con LC-MS = 6 su 6 (100%)
ECLIA LC-MS
3,12 3,60
3,27 3,15
3,44 3,00
3,52 3,10
4,82 4,90
5,63 6,70
LC-MS ECLIA
3,00 3,44
3,10 3,52
3,15 3,27
3,30 2,02
3,60 3,12
4,90 4,82
6,70 5,63
Determinazione del Te sierico in
123 pazienti donne

Clinica Medica 3-University of Padua, Italy
Indagini di Laboratorio(entro i primi 7 gg del ciclo mestruale (se presente)
β-hCG * (amenorrea)
TSH (fT4)
Prolattina (dopo 20’ di riposo)
LH, FSH (LH/FSH > 2.0) *
Testosterone totale (Tfree)
SHBG (FAI > 4.0)
DHEAS
Androstenedione
17-HOProgesterone
Free Androgen Index (FAI) :
Testosterone (nmol/L) x 100 : SHBG (nmo/L)

TRYPTARELIN- TEST
• GnRH agonist test:Blood samples (LH, FSH and steroid hormones) were obtained before (i.e. at baseline) and 2, 4,12, 20, 24 h after the administration of 100 ug of Tryptarelin (Decapeptyl –Ipsen- Italy).
• The serum samples were stored at -20° C until they were assayed.
• Before the Test:A pre-treatement with 2 mg/day of dexamethasone ( Dex 0.5 mg/os 1 cpr at 08.00 and 14.00 and 2 cpr at 22.00) 2 days before the tryptorelin test and continuing throughout the day of the test.


Ovarian Response to GnRHa (Buserelin)in PCOS and Control Subjects
0
40
80
120
160
200
Controls nINS hINS
AU
C-
An
dro
sten
edio
ne
( nm
ol/
L/2
4h)
Lean Obesep < 0.01
p < 0.001p < 0.01
0
2
4
6
8
10
12
0 12h 16h 20h 24h
An
dro
sten
edio
ne
(nm
ol/
L)
Baseline
time
Gn
RH
a 0
.10
0 m
g s
c Controls nINS hINS
Clinica Medica 3-University of Padua, Italy(Mioni R. et al. 2001)
AU
C –
Tes
tost
eron
e(
nm
ol/
L/2
4h)
0
40
80
120
160
200
Controls nINS hINS
Lean Obese p < 0.01
p < 0.001p < 0.01
0
2
4
6
8
10
12
0 12h 16h 20h 24h
Tes
tost
eron
e(n
mol/
L)
Baseline
time
Gn
RH
a 0
.10
0 m
g s
c Controls nINS hINS

0
500
1000
1500
2000
0 12h 16h 20h 24h time
17
-Est
rad
iol
(pm
ol/
L)
Baseline
Gn
RH
a 0
.10
0 m
g s
c
0
500
1000
1500
2000
0 12h 16h 20h 24h time
17
-Est
rad
iol
(pm
ol/
L)
BaselineControls nINS hINSControls nINS hINS
Gn
RH
a 0
.10
0 m
g s
c
0
5000
10000
15000
20000
25000
30000
35000
Controls nINS hINS
E2 (
pm
ol/
L/2
4h) p< 0.02
AUCpost
0
5000
10000
15000
20000
25000
30000
35000
Controls nINS hINS
AU
C -
E2 (
pm
ol/
L/2
4h)
p< 0.02
Lean Obesep< 0.001
P < 0.01
p< 0.02
Ovarian Response to (E2 ) GnRHa (Buserelin)
in PCOS Patients and Control Subjects
Clinica Medica 3-University of Padua, Italy

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
Esami Strumentali

Clinica Medica 3-University of Padua, Italy
Indagini Strumentali
Ecografia pelvica Transaddominale (TA)
Ecografia Pelvica Transvaginale (TV)
Ecografia Pelvica Transrettale (TR)
TAC (addome inferiore -/+ mdc)
RMN (addome inferiore)

Clinica Medica 3-University of Padua, Italy

Ovaio PolicisticoOvaio Policistico

Amenorrea ipotalamica

S / T > 0.32 = PCO
S / T < 0.32 = Multi

Studio Morfologico Ovarico in PCOS
246.1mm2
TFA
151TNF
Clinica Medica 3-University of Padua, Italy

Ultrasound Criteria forPolycystic Ovary Syndrome
Ovary 1991 2003 2009 2011 2013
FollicularDistrib
Periph + Stromal
++
++
--
Stroma Echogen
Hyperech + + + +
TNFn°/ovary
> 8 10 12 19 26
TNAmm2/ov
180 + + + -
Ovolcm3/ov
10 + + + +
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
( 2011 - 2013)

Studio Morfologico Ovarico in PCOS
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
( 2011 - 2013)
( 2014 – 201…)

Parametri di morfologia ovarica
*p<0.01 vs Con
13.6±2.0*14.2±2.4*14.8±2.1*15.3±3-1*8.3±2.48.6±2.3Ovolcm3/ov
*p<0.01 vs Con
278±42^246±54*284±48*268±62*152.2±40146.8±32TNAmm2/ov
*p<0.01 vs Con
21.3±4.*23.6±7.*22.6±3.*24.3±6.*9,4±2.69.8±2.3TNFn°/ovary
LeftrightleftrightleftrightOvary
PPCOS
Lean hINS
PCOS
Obese hINSControls
(R. Mioni et al. JEI 2016)
Clinica Medica 3-University of Padua, Italy

Studio Morfologico Ovarico in PCOS
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
Disturbi del Ciclo Mestruale

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
HYPERINSULINEMIA HYPERANDROGENISM
SHBG
AROMATASE ACTIVITY(fat, muscle, skin)
T
A
LH
(Nestler et al 2000 modified)
Chronic ANOVULATION
LEPTIN
Ovarian Regulatory System in PCOS

Definition of Irregular Menses in Adolescent Girls
Clinica Medica 3-University of Padua, Italy
• Normal during the first year postmenarche
• From 1 to 3 y postmenarche < 21 d or > 45 d
• From 3 y postmenarche < 21 d or >35 d or < 8 cycles yr
• From 1 y postmenarche > 90 d for any one cycle
• Primary amenorrhea by age 15 y or > 3 y after thelarche
S F Witchel et al. J Endocrinol Soc. 2019

Alterazioni del ciclo Mestruale
• Eumenorrea: ciclo mestruale ogni 24-32 gg- (a) n. cicli anno tra 10 e 12 – (b) n. cicli anno > 8
• Oligomenorrea: ciclo mestruale oltre 35 -38 gg- (a) n. cicli anno tra 4 e 8 - (b) n.cicli anno < a 8
• Amenorrea: ciclo mestruale assente da oltre 6 mesiciclo mestruale assente da oltre 3 mesi nelle normomestruanti
----------
• Ciclo Ovulatorio: picco Progesterone>16 nmol/L (20-23gg)
• Ciclo Anovulatorio: picco Progesterone < 6 nmol/L
Clinica Medica 3-University of Padua, Italy


FSH secretion
ANDROGENS
OVULATION

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy

AMH in ovarian physiology: possible actions
AMH
FSH
1
2
AMH serum levels show a reduction throughout reproductive life
Undetectable AMH levels in post-menopausal period
AMH as a marker for ovarian ageing
In women:
1) Inhibition of follicular activation
and recruitmen
2) Inhibition of FSH stimulated
growth
(Visser, 2005; Themmen, 2005)

AMH Concentration and Production in Human and Normal Ovary
(Mason H. et al Clin Endocrinol 2010)

AMH in human menstrual cycle:

AMH in human menstrual cycle:
Anti-Müllerian Hormone levels do not show substantial fluctuation
during the spontaneous menstrual cycle
(Streuli et al., 2007; Hehenkamp et al., 2006; La Marca et al., 2007)
correlationsFSH
LH T
(early follicular ph.)


AMH in human menstrual cycle:
Anti-Müllerian Hormone levels do not show substantial fluctuation
during the spontaneous menstrual cycle
(Streuli et al., 2007; Hehenkamp et al., 2006; La Marca et al., 2007)
La Marca et al 2014
correlationsFSH
LH T
(early follicular ph.)
Dewailly D et al. Human Rep 2014

(Pigny et al., 2003 and Jonard et al., 2003, modified)
NORMAL OVARY POLYCYSTIC OVARY
FSH
AMH
AMHFSH
AndrogensAndrogens
Estradiol
LH ?
? Estradiol
??

&AMH PCOS
Autore AnnoPazienti
(n)
Livelli AMH (ng/ml)
Contr PCOS ∆%
Cook et al. 2002 47 2.4±0.2 5.3±0.7 +120
Pigny et al. 2003 104 2.9±0.3 6.6±0.4 +127
La Marca et al. 2004 29 1.3±0.5 5±1.8 +284
Laven et al. 2004 109 2.1±0.6 7.6±1.8 +261
Piltonen et al. 2005 170 2.4±0.2 8.1±0.8 +237
Eldar-Geva et 2005 52 1.6±0.8 5.1±1.3 +218
La Marca et al. 2006 34 3.5±1.5 7.4±1.7 +111
Wachs et al. 2007 27 2.1±0.4 7.2±0.5 +242
Ritunnano et al. 2010 49 3.02±1.3 6.1±2.6 +202


Percorso Diagnostico della Sindrome dell’Ovaio Policistico
PCOSAlopecia
Androgenica
Irsutismo
Acne
SeborreaDisturbi del Ciclo
Esami di
Laboratorio
ALTRO?
Clinica Medica 3-University of Padua, Italy
ALTRO ?

Clinica Medica 3-University of Padua, Italy
Common Clinical Manifestations Associated With the Syndrome Across the Life Course and Types of Research Recommended

Clinica Medica 3-University of Padua, Italy
Common Clinical Manifestations Associated With the Syndrome Across the Life Course and Types of Research Recommended

Clinica Medica 3-University of Padua, Italy
Common Clinical Manifestations Associated With the Syndrome Across the Life Course and Types of Research Recommended


( Dunaif A et al., JCEM 1996 )
250
200
150
100
50
0
Time in Minutes
InsulinmU/ml
0 30 60 90 120 180
Obese Obese PCOSControl
250
200
150
100
50
00
Time in Minutes
Glucosemg/100 ml
30 60 90 120 180
Plasma glucose concentrations during oral glucose testing (OGTT 75 g)
Clinica Medica 3-University of Padua, Italy

800
900
1000
1100
1200
Controls nINS - PCOS hINS - PCOS
Glu
cose
(mm
ol/
L/2
4h
)
0
3000
6000
9000
12000
15000
Insu
lin
(m
UI/
L/2
4h
)
p < 0.01
p< 0.002
Lean Obese ( Mioni R. et al. 2000)
Effect of OGTT on Insulin and Glucose (AUC)
in PCOS and Control Subjects
Clinica Medica 3-University of Padua, Italy

Hormonal
activaction
GLUT
(Exercise, Stress, etc )
Insulin
Insulin Signaling Pathways Regulating Glucose Metabolism in the Cells
Clinica Medica 3-University of Padua, Italy

Hormonal
activaction
GLUT
Mechanisms Involved in Insulin Resistance in Polycystic Ovary Syndrome at Tissutal Level
(Exercise, Stress, etc )
Insulin
GLUT 4
Clinica Medica 3-University of Padua, Italy

GLUT4 mRNA expression in endometrial samples of lean or obese nINS or hINS PCOS and Control subjects.
mR
NA
GL
UT
4
( arb
itra
ry u
nit
s)
0
20
40
60
80
100
120
Control Lean Obese Lean Obese
H-INS n-INS
p<0.01
p<0.01
p<0.01
p=0.003
mR
NA
GL
UT
4
( arb
itra
ry u
nit
s)
0
20
40
60
80
100
120
Control Lean Obese Lean Obese
H-INS n-INS
p<0.01
p<0.01
p<0.01
p=0.003
Mw
GLUT4 (447bp)
RT-PCR products
Clinica Medica 3-University of Padua, ItalyClinica Medica 3-University of Padua, Italy
( Mioni R. et al. 2004)

INSULIN Excess onHypothalamic- Pituitary – Ovarian axis
HYPERINSULINEMIA HYPERANDROGENISM
SHBG
AROMATASE ACTIVITY(fat, muscle, skin)
T
A
LH
Chronic ANOVULATION
LEPTIN
In Human: LH Basal and GnRH-induced
Androstenedione17-OH-ProgesteroneTestosterone
17β-Estradiol (-/+)SHBG
( Mioni et al. 2001; Viani et al. 2008; Mioni et al.2008; Tosi et al. 2012; Rosenfield et al. 2013 )


Effects of LGD on the Frequency of Menstration in Lean PCOS and Control Subjects
Clinica Medica 3-University of Padua, Italy
p< 0.05
p< 0.05
0
0,4
0,8
1.2
Control nINS hINS
cycle
/ m
onth
Baseline After Diet
a b,c
a: p< 0.05 vc Con
b: p< 0.03 vs nINS
c: p< 0.01 vs Base
(Mioni et al. 2007)


Trend of Weight Prevalence among PCOSObese Women Aged 18 - 44 yrs
Clinica Medica 3-University of Padua, Italy
0
10
20
30
40
50
60
USA Europe Italy
1980
1998
2014
19
80
1980
1998
19
98
2014
2014
Pre
vale
nce
(%
)
BMI > 30
(Metanalysis of 28 papers from 1988 to 2016)

Weight Prevalence between Obese and
PCOS Obese Women
Clinica Medica 3-University of Padua, Italy
0
10
20
30
40
50
60
USA Europe Italy
2010
2010
2010
2014 -
PC
OS
2014 -
PC
OS
2014 -
PC
OS
BMI > 30
Pre
vale
nce
(%
)
(Metanalysis of 28 papers from 1988 to 2016)
(Flegal KM et al, 2002; Bray GA, 2004; Koletzko B et al, 2004; Carmina E. et al., 2015)

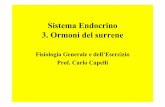
Outline of three obese women with approximately thesame BMI, but differing in pattern of fat distribution
Visceral•Central
•Android
•“apple distribution”
Subcutaneous•Peripheral
•Gynoid
•“pear distribution”
Intermediate type
distribution
Clinica Medica 3-University of Padua, Italy

0
10
20
30
40
50
60
70
80
90
lean Con lean PCOS Obese Con Obese PCOS
Total nINS hINS
% o
f pat
ients
wit
h v
scer
al f
at d
istr
ibuti
on
Clinica Medica 3-University of Padua, Italy
Visceral Fat Distribution in Young Patients
affected by PCOS
(Modified from Kirchengast S. et al. Hum Reprod 2001 ; Gambineri A et al. Diabetes 2014)


Genetic Predisposition
Aging
Pregnancy
Drugs
Lifestyle
Insulin
Resistance
Hyperinsulinemia
Altered Fat Metabolism
Altered Steroid Hormone Metabolism
PCOS: Acne, hirsutism,
hyperandrogenism infertility
Cristello F et al, Gynecological Endocrinology, 2005.
Android
Obesity
↑ Lipid Storage

Cardiometabolic disturbances in PCOS.
Randeva H S et al. Endocrine Reviews 2012;33:812-841

Clinica dell’Ovaio Policistico
PCOSHyperandrogenism
Disturbi del ciclomestruale
Irsutismo
AcneSeborrea
Obesità
AlopeciaAndrogenica
Aspetti Glico-Metabolici
?
Clinica Medica 3-University of Padua, Italy
AspettiCardio-Circolatori

PCOS e disfunzione endoteliale
• Perdita del dipping notturno della PAO
• Aumento dei markers di disfunzione endoteliale
• Ispessimento intima-media delle carotidi
Bibliografia• Arslanian S.A et al JCEM 2001; 86: 66-71• Diamanti Kandarakis E et al JCEM 2016; 86: 4666-4673• Orio jr. F. et al JCEM 2004; 89: 4588-4593• Vryonidou A. et al JCEM 2015; 90: 2740-2746
Clinica Medica 3-University of Padua, Italy

• L’ipertensione arteriosa risulta non frequente nei soggetti giovani con PCOS. (Wild RA et al. 2002)
• La prevalenza di ipertesione arteriosa sembra essere maggiore nei soggetti PCOS obesi. (obesità centrale come “organo adiposo endocrino”) (Conway GS et al-1992)
• La prevalenza dell’ipertensione arteriosa aumenta in prossimità del periodo perimenopausale (40%) in donne con precedente diagnosi di PCOS. (Cibula D. et al. 2000)
• L’obesità rappresenta il principale determinante delle anomalie pressorie in pazienti con PCOS. (Escobar M. et al. 2007)
PCOS E PRESSIONE ARTERIOSA
Clinica Medica 3-University of Padua, Italy

Clinica Medica 3-University of Padua, Italy
SUDDIVISIONE
BMI INSULINA
22 pazienti
OBESE
32 pazienti
NORMOPESO
54 soggetti affetti
da PCOS
32 pazienti(h-INS)
22pazienti(n-INS)
54 soggetti affetti
da PCOS

BMI INSULINA
DIFFERENZE nella CADUTA NOTTURNA
PASPAS
PAD10,1
12,814,3
16,4
12,1
14,6
0
5
10
15
20
25
30
obese normopeso
(%
)
Differenza diurna/notturna
MEDIAMEDIA
PAD
PASPAS
PAD10,1
12,814,3
16,4
12,1
14,6
0
5
10
15
20
25
30
obese normopeso
(%
)
Differenza diurna/notturna
MEDIAMEDIA
PAD
PASPAS
PAD10,1
12,814,3
16,4
12,1
14,6
0
5
10
15
20
25
30
obese normopeso
(%
)
Differenza diurna/notturna
MEDIAMEDIA
PAD
PAS
PAS
PAD
PAD
9,6
15,3
12,8
20
11,2
17,6
0
5
10
15
20
25
30
h-INS n-INS
Dif
fere
nza d
iurn
a/n
ottu
rn
a (
%)
MEDIA
MEDIA
p < 0,04 vs n-INS
*
*
p < 0,03 vs n-INS
* *
p < 0,02 vs n-INS
*
*
PAS
PAS
PAD
PAD
9,6
15,3
12,8
20
11,2
17,6
0
5
10
15
20
25
30
h-INS n-INS
Dif
fere
nza d
iurn
a/n
ottu
rn
a (
%)
MEDIA
MEDIA
p < 0,04 vs n-INS
*
*
p < 0,03 vs n-INS
* *
p < 0,02 vs n-INS
*
*
( Bleve L. et al. Atti Congresso SIDR Abano Terme 2010 )
Clinica Medica 3-University of Padua, Italy

BMI + INSULINADIFFERENZE nella CADUTA NOTTURNA
0
5
10
15
20
25
30
h-INS
obese
h-INS
normopeso
n-INS
obese
n-INS
normopeso
10,5311,77
16,7117,92
Media della differenza diurna/notturna della PA sisto-diastolica
* p < 0,05 vs n-INS
%
0
5
10
15
20
25
30
h-INS
obese
h-INS
normopeso
n-INS
obese
n-INS
normopeso
10,5311,77
16,7117,92
Media della differenza diurna/notturna della PA sisto-diastolica
* p < 0,05 vs n-INS
%
Differenza diurna/notturna della PA sistolica
0
5
10
15
20
25
%
* p < 0,05 vs n-INS
7,94
10,99
16,3815,03
30
12,49 13,25
17,47
20,93
0
5
10
15
20
25
h-INS
obese
h-INS
normopeso
n-INS
obese
n-INS
normopeso
%
* p < 0,05 vs n-INS
Differenza diurna/notturna della PA diastolica
Differenza diurna/notturna della PA sistolica
0
5
10
15
20
25
%
* p < 0,05 vs n-INS
7,94
10,99
16,3815,03
30
12,49 13,25
17,47
20,93
0
5
10
15
20
25
h-INS
obese
h-INS
normopeso
n-INS
obese
n-INS
normopeso
%
* p < 0,05 vs n-INS
Differenza diurna/notturna della PA diastolica
( Bleve L. et al. Atti Congresso SIDR Abano Terme 2010 )

Clinica dell’Ovaio Policistico
PCOSHyperandrogenism
Disturbi del ciclomestruale
Irsutismo
AcneSeborrea
Obesità
AlopeciaAndrogenica
Aspetti Glico-Metabolici
AspettiCardio-Circolatori
Clinica Medica 3-University of Padua, Italy
?

Clinica Medica 3-University of Padua, Italy
• Laura Zuliani, MD - U.O.C. di Medicina – Este (PD)• Sara Azzolini, MD - U.O.S. Endocrinologia Pediatrica–Az Osp Padova• Letizia Glinski, MD – Medicina di Urgenza – Università di Padova
• Eugenio De Carlo, MD• Pietro Maffei, MD, PhD
• Chiara Martini, MD
(Direttore Prof. Roberto Vettor)
Un Grazie di Cuore a:
• Marnie Granzotto, BD• Clinica Medica 3 – Università di Padova
• Jenni Turra, MD
• Medicina di Laboratorio – Università di Padova ( Dir. Prof. Mario Plebani)
• Diego Faggian, BD• Carlo Artusi, MD
• Nadia Xamin, MD - U.O.C. di Medicina – Bassano del G. (VI)
• Bruno Mozzanega, MD• Dip. della Salute della Donna e del Bambino – Università di Padova
• Anna Dalla Cà, MD
• Laura Cervino, MD
• Pietro Litta, MD

Clinica dell’Ovaio Policistico
PCOSHyperandrogenism
Disturbi del ciclomestruale
Irsutismo
AcneSeborrea
Aspetti Glico-Metabolici
AlopeciaAndrogenica
Aspetti Cardio-Circolatori
?
Clinica Medica 3-University of Padua, Italy
Obesità

Energy Balance Equation (food intake ?)
Adipose Tissue
Normalweight Overweight Obesity
Clinica Medica 3-University of Padua, Italy

Body Fat distribution in Obese Subjects
affected by PCOS
Clinica Medica 3-University of Padua, Italy

Estimates of FFM, FM, and percentage body fat in
European-American boys (closed symbols) and girls (open
symbols) from infancy through early adulthood (age 20 yr)
Clinica Medica 3-University of Padua, Italy
( Veldhuis, J. D. et al. Endocr Rev 2005; 26:114-146 )

FFM, FM, and percentage body fat in American-European
obese PCOS-girls from menarche through early adulthood
Clinica Medica 3-University of Padua, Italy
(U.S.A.):Palmert et al. 2002; Cruz M.L et al 2004;Coviello A.D.et al 2007
(Europe):Franks et al. 2000; Ibanez.L et al 2002;Ibanez L..et al 2004-2007

Adipose Tissue
Energy Balance Equation in PCOS (food intake ?)
Clinica Medica 3-University of Padua, Italy

ENERGY FUELS
LeptinInsulin
HYPOTHALAMUS
Endogenous Exogenous
Clinica Medica 3-University of Padua, Italy
How Much?

Obesity and Dietary Intake* in American
Women with PCOS
PCOS (n 68) Control (n 37) P
BMI (kg/m2) 38.37 ± 7.28 35.67 ± 4.88 ns
Energy (from food)(Kcal) 1981.34 ± 793 1742.56 ± 655 ns
Protein (g) 78.97 ± 30 (15.9%) 61.79 ± 22.7 (14.9%) ns
Carbohydrates (g) 227.50 ± 84 205.2 ± 75 ns
Total fat (g) 87.98 ± 43 75.36 ± 35 ns
SFA (g) 26.41 ± 14 22.88 ± 11 ns
MUFA 32.87 ± 16 28.02 ± 12 ns
PUFA 21.99 ± 11.26 18.85 ± 10 ns
Cholesterol (mg) 234.20 ± 141 190.64 ± 98 ns
(Wright CE et al., Int J Obesity, 28, 1026-1032, 2004)
* ( Dietary information by a self-administered diet history questionnaire )
Clinica Medica 3-University of Padua, Italy

PCOS (n 68) Control (n 37) P
BMI (kg/m2) 38.37 ± 7.28 35.67 ± 4.88 ns
Energy (from food)(Kcal) 1981.34 ± 793 1742.56 ± 655 ns
Protein (g) 78.97 ± 30 (15.9%) 61.79 ± 22.7 (14.9%) ns
Carbohydrates (g) 227.50 ± 84 205.2 ± 75 ns
Total fat (g) 87.98 ± 43 75.36 ± 35 ns
SFA (g) 26.41 ± 14 22.88 ± 11 ns
MUFA 32.87 ± 16 28.02 ± 12 ns
PUFA 21.99 ± 11.26 18.85 ± 10 ns
Cholesterol (mg) 234.20 ± 141 190.64 ± 98 ns
Obesity and Dietary Intake* in American
Women with PCOS
(Wright CE et al., Int J Obesity, 28, 1026-1032, 2014)
* ( Dietary information by a self-administered diet history questionnaire )
Clinica Medica 3-University of Padua, Italy

PCOS (n 68) Control (n 37) P
BMI (kg/m2) 38.37 ± 7.28 35.67 ± 4.88 ns
Energy (from food)(Kcal) 1981.34 ± 793 1742.56 ± 655 ns
Protein (g) 78.97 ± 30 (15.9%) 61.79 ± 22.7 (14.9%) ns
Carbohydrates (g) 227.50 ± 84 205.2 ± 75 ns
Total fat (g) 87.98 ± 43 75.36 ± 35 ns
SFA (g) 26.41 ± 14 22.88 ± 11 ns
MUFA 32.87 ± 16 28.02 ± 12 ns
PUFA 21.99 ± 11.26 18.85 ± 10 ns
Cholesterol (mg) 234.20 ± 141 190.64 ± 98 ns
Obesity and Dietary Intake* in American
Women with PCOS
(Wright CE et al., Int J Obesity, 28, 1026-1032, 2014)
* ( Dietary information by a self-administered diet history questionnaire )
Clinica Medica 3-University of Padua, Italy

Italian PCOS (n 20) American PCOS (n 20) P
BMI (kg/m2) 29.7 ± 1.0 40.3 ± 1.0 <0.01
Energy (from food)(Kcal) 2325 ± 68 2277 ± 109 ns
Protein (g) 80.5 ± 38 86.9 ± 34 ns
Carbohydrates (g) 318.5 ± 54 294 ± 69 ns
Total fat (g) 84.9 ± 48 89.5 ± 45 ns
SFA (g) 18.2 ± 2 31.9 ± 3 <0.01
Obesity and Dietary Intake* in American and
Italian Women with PCOS
* ( food, drink and other supplements consumed over 3 days )
(Carmina E. et al., Hum Reprod, 18, 11 2289-2293, 2013)
Clinica Medica 3-University of Padua, Italy

Italian PCOS (n 20) American PCOS (n 20) P
BMI (kg/m2) 29.7 ± 1.0 40.3 ± 1.0 <0.01
Energy (from food)(Kcal) 2325 ± 68 2277 ± 109 ns
Protein (g) 80.5 ± 38 86.9 ± 34 ns
Carbohydrates (g) 318.5 ± 54 294 ± 69 ns
Total fat (g) 84.9 ± 48 89.5 ± 45 ns
SFA (g) 18.2 ± 2 31.9 ± 3 <0.01
Obesity and Dietary Intake* in American and
Italian Women with PCOS
* ( food, drink and other supplements consumed over 3 days )
(Carmina E. et al., Hum Reprod, 18, 11 2289-2293, 2013)
Clinica Medica 3-University of Padua, Italy

Italian PCOS (n 20) American PCOS (n 20) P
BMI (kg/m2) 29.7 ± 1.0 40.3 ± 1.0 <0.01
Energy (from food)(Kcal) 2325 ± 68 2277 ± 109 ns
Protein (g) 80.5 ± 38 86.9 ± 34 ns
Carbohydrates (g) 318.5 ± 54 294 ± 69 ns
Total fat (g) 84.9 ± 48 89.5 ± 45 ns
SFA (g) 18.2 ± 2 31.9 ± 3 <0.01
Obesity and Dietary Intake* in American and
Italian Women with PCOS
* ( food, drink and other supplements consumed over 3 days )
(Carmina E. et al., Hum Reprod, 18, 11 2289-2293, 2013)
Clinica Medica 3-University of Padua, Italy

Italian PCOS (n 20) American PCOS (n 20) P
BMI (kg/m2) 29.7 ± 1.0 40.3 ± 1.0 <0.01
Insulin (mU/L) 18.1 ± 2 29.5 ± 2 <0.01
Glucose/insulin ratio 5.3 ± 1 3.6 ± 0.5 <0.01
Total cholesterol (mg/dl) 183 ± 12 187 ± 8 ns
Triglycerides (mg/dl) 91 ± 8 156 ± 18 <0.01
Testosterone (ng/dl) 79 ± 10 76 ± 7 ns
Testosterone free (pg/dl) 18 ± 3 21 ± 2 ns
DHEA-s (ug/ml) 2.3 ± 0.4 2.2 ± 0.3 ns
Obesity and Dietary Intake in American and
Italian Women with PCOS
Hormonal and metabolic parameters
Carmina E. et al., Hum Reprod, 18, 11 2289-2293, 2013)
Clinica Medica 3-University of Padua, Italy

Obese PCOS (n 80) Lean PCOS (n 19) P
Age (years) 23.5 ± 5.8 23.6 ± 5.2 ns
BMI (kg/m2) 33.7 ± 4.1 22.3 ± 1.7 <0.001
Waist circumf (cm) 95.7 ± 13.4 71.4 ± 5.5 <0.001
Energy (from food)(Kcal) 1947 ± 424 1735 ± 275 ns
Protein (%) 17.1 ± 11.2 16.5 ± 4.8 ns
Carbohydrates (%) 54.2 ± 33.5 50.1 ± 11.3 ns
Total fat (%) 35.1 ± 7.3 33.3 ± 7.8 ns
Obesity and Dietary Intake* in Italian
Women with PCOS (Obese and Lean)
* ( Dietary information by the dietitian attending in the Endocrinological Unit )
Modified from (Gambineri A. et al, Diabetes, 53, 2353-2358, 2014)
Clinica Medica 3-University of Padua, Italy

Obese PCOS (n 80) Lean PCOS (n 19) P
Age (years) 23.5 ± 5.8 23.6 ± 5.2 ns
BMI (kg/m2) 33.7 ± 4.1 22.3 ± 1.7 <0.001
Waist circumf (cm) 95.7 ± 13.4 71.4 ± 5.5 <0.001
Energy (from food)(Kcal) 1947 ± 424 1735 ± 275 ns
Protein (%) 17.1 ± 11.2 16.5 ± 4.8 ns
Carbohydrates (%) 54.2 ± 33.5 50.1 ± 11.3 ns
Total fat (%) 35.1 ± 7.3 33.3 ± 7.8 ns
* ( Dietary information by the dietitian attending in the Endocrinological Unit )
Obesity and Dietary Intake* in Italian
Women with PCOS (Obese and Lean)
Clinica Medica 3-University of Padua, Italy
Modified from (Gambineri A. et al, Diabetes, 53, 2353-2358, 2014)

Obese PCOS (n 80) Lean PCOS (n 19) P
Age (years) 23.5 ± 5.8 23.6 ± 5.2 ns
BMI (kg/m2) 33.7 ± 4.1 22.3 ± 1.7 <0.001
Waist circumf (cm) 95.7 ± 13.4 71.4 ± 5.5 <0.001
Energy (from food)(Kcal) 1947 ± 424 1735 ± 275 ns
Protein (%) 17.1 ± 11.2 16.5 ± 4.8 ns
Carbohydrates (%) 54.2 ± 33.5 50.1 ± 11.3 ns
Total fat (%) 35.1 ± 7.3 33.3 ± 7.8 ns
* ( Dietary information by the dietitian attending in the Endocrinological Unit )
Obesity and Dietary Intake* in Italian
Women with PCOS (Obese and Lean)
Clinica Medica 3-University of Padua, Italy
Modified from (Gambineri A. et al, Diabetes, 53, 2353-2358, 2014)

0
10
20
30
40
50
60
Carbohydrates Proteins Lipids
Controls (18)
PCOS (34)
ns ns ns
Dietary Intake^ in Italian Obese
Women with PCOS
^ ( Dietary information by a self-administered diet history questionnaire)
Clinica Medica 3-University of Padua, Italy
( Mioni R et al. 2010)

Energy Balance Equation in PCOS
Clinica Medica 3-University of Padua, Italy
Adipose Tissue

ENERGY FUELS
LeptinInsulin
HYPOTHALAMUS
Endogenous Exogenous
Clinica Medica 3-University of Padua, Italy
How?

Clinica dell’Ovaio Policistico
PCOSHyperandrogenism
Disturbi del ciclomestruale
Irsutismo
AcneSeborrea
Obesità
AlopeciaAndrogenica
Aspetti Cardio-Circolatori
?
Clinica Medica 3-University of Padua, Italy
AspettiGlico-Metabolici

Factors regulating abdominal fat distribution
Clinica Medica 3-University of Padua, Italy
( Wajchemberg B.L - Endcrin Rev 2000)

Factors regulating abdominal fat distribution
Clinica Medica 3-University of Padua, Italy
( Wajchemberg B.L - Endcrin Rev 2000)

Clinica Medica 3-University of Padua, Italy

Factors regulating abdominal fat distribution
Clinica Medica 3-University of Padua, Italy
( Wajchemberg B.L - Endcrin Rev 2000)

Factors regulating abdominal fat distribution
Clinica Medica 3-University of Padua, Italy
( Wajchemberg B.L - Endcrin Rev 2000)

Factors regulating abdominal fat distribution
Clinica Medica 3-University of Padua, Italy
( Wajchemberg B.L - Endcrin Rev 2000)
PCOS - Ring

Effect of Diet in Obese PCOS Patients
< 1000 kcal: - Kopelman PG et al(Clin Endocrinol 1981;15:113)
- Bates GW et al (Fertil Steril 1982;38:406)
- Harlass FE et al (Fertil Steril 1984;42:649)
- Kiddy DS et al (Clin Endocrinol 1992;36:105)
LH Androgens
> 1000 kcal: - Pasquali R et al (J Clin Endocrinol Met 1989;68:173)
- Guzick DS et al (Fertil Steril 1994;61:598)
- Holte J et al (J Clin Endocrinol Met 1995;80:2586)
- Crave JC et al (J Clin Endocrinol Met 1995; 80:2057)
- Clark AM et al (Hum Reprod 1995;10:2705)
- Jakubowicz DJ et al(J Clin Endocrinol Met 1997;82:556)
Clinica Medica 3-University of Padua, Italy
Ovulation

Effects of weight loss on Clinical and biochimical of Obese PCOS

Effects of Diet on the frequency of menstration
in Obese PCOS and Control Subjects
0
0,2
0,4
0,6
0,8
1
1,2
Control nINS hINS
cycl
e /
mon
th
baseline afterDiet
p< 0.05
p< 0.05
Clinica Medica 3-University of Padua, Italy
( Azzolini S. et al. 2010 )

PCOS e Diabete tipo 2
• Maggiore probabilità (5-10 volte) di sviluppare DM2 sia nelle PCOS obese che magre (30% IGT- 3.7% Diabete).
• Riduzione della first-phase insulin secretion.
• Complicanza tempo-dipendente(> 5 anni)
• Iperandrogenismo per se causa principale.
Bibliografia• Lewy VD et al. J Pediatr. 2011; 136;38-44• Palmert MR et al. JCEM 2012; 87:1017-1023• Silfen ME et al. JCEM 2013,; 88:4682-4688• Saad R et al Pediatr.Diabetes 2015; 6:95-99
Clinica Medica 3-University of Padua, Italy

PCOS e Dislipidemia
• LDL colesterolo
• HDL colesterolo
• LDL/HDL
• Trigliceridi
• Adiponectina
• Bibliografia
• Ibanez L. et al. J.of Pediatrics 2014; 144: 23-29
• Weiss R. et al. NEJM 2016; 350:2362-2374
Clinica Medica 3-University of Padua, Italy