Presentazione standard di PowerPoint - Aristea · Sezione di Oftalmologia Responsabile: ... a color...
70
Retinopatia diabetica : quando e come trattarla Università degli Studi di Palermo Scuola di Medicina e Chirurgia Dipartimento di Biomedicina Sperimentale e Neuroscienze Cliniche Sezione di Oftalmologia Responsabile: Prof. Salvatore Cillino Salvatore Cillino Simona Di Naro Valentina Sunseri Anna Mangione
-
Upload
vuongtuyen -
Category
Documents
-
view
213 -
download
0
Transcript of Presentazione standard di PowerPoint - Aristea · Sezione di Oftalmologia Responsabile: ... a color...

Retinopatia diabetica : quando e come trattarla
Università degli Studi di Palermo
Scuola di Medicina e Chirurgia Dipartimento di Biomedicina Sperimentale
e Neuroscienze Cliniche
Sezione di Oftalmologia
Responsabile: Prof. Salvatore Cillino
Salvatore Cillino
Simona Di Naro
Valentina Sunseri
Anna Mangione

Diabetic Retinopathy
Epidemiology
• The total number of people with diabetes is projected
to rise from 285 million in 2010 to 439 million in 2030.
• Diabetic retinopathy is responsible for 1.8 million of
the 37 million cases of blindness throughout the
world.
• Diabetic retinopathy (DR) is the leading cause of
blindness in people of working age in industrialized
countries.

• The best predictor of diabetic retinopathy is the duration
of the disease
• After 20 years of diabetes, nearly 99% of patients with
type 1 diabetes and 60% with type 2 have some degree
on diabetic retinopathy
• 33% of patients with diabetes have signs of diabetic
retinopathy
• People with diabetes are 25 times more likely to become
blind than the general population.
Diabetic Retinopathy
Epidemiology
Ophthalmology Myron Yanoff MD and Jay S. Duker
Basic and Clinical Science Course, Section 12: Retina and
Vitreous AAO
http://www.aao.org/eyecare/news/upload/Eye-Health-Fact-Sheet.pdf -

• DR was a cause of 4,8% of global blindness in 2002,
3,9% in 2004 and 1% in 2010
• The percentage of adults with diagnosed diabetes, who
reported visual impairment, declined significantly,
from 23.7% in 1997 to 16.7% in 2010
Diabetic Retinopathy
Epidemiology

Relationship between oxidative stress and DR
Polyol pathway AGE RAGE PKC
DR
Suk-Yee Li,Zhong Jie Fu, and Amy C. Y. Lo. Hypoxia-Induced Oxidative Stress in Ischemic Retinopathy.
Oxidative Medicine and Cellular Longevity Volume 2012, doi:10.1155/2012/426769
Hexosamine
I/R
ROS/RNS
Lipid
peroxidation PARP JNK p38 MAPK NFkB Mitochondrial
dysfunction

Inflammatory Biomarkers in Diabetic Retinopathy
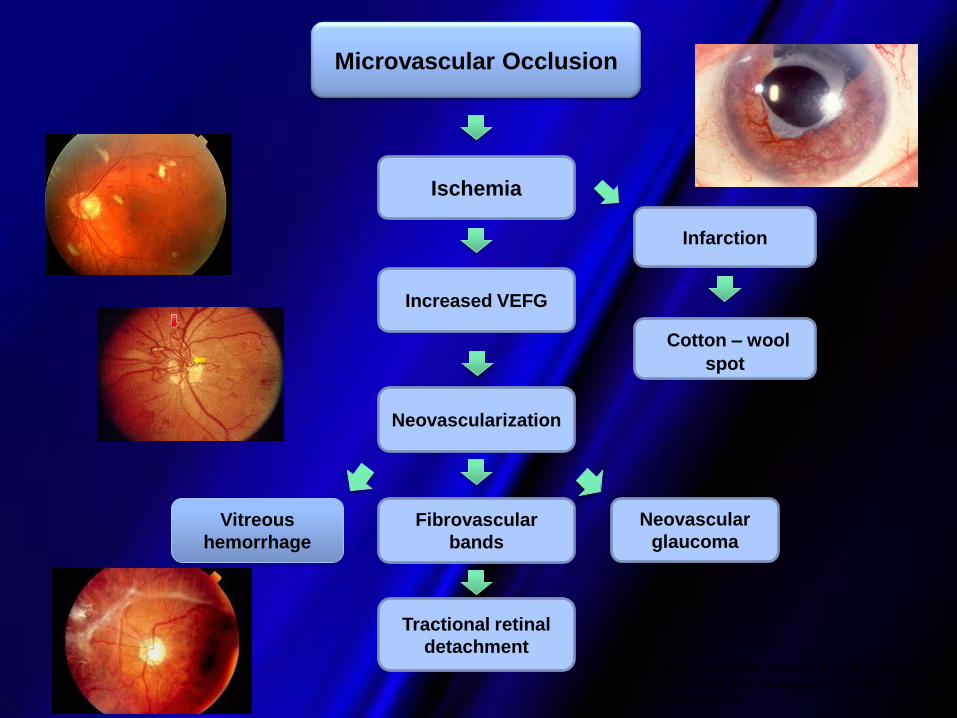
Cotton – wool
spot
Neovascularization
Ischemia
Neovascular
glaucoma
Microvascular Occlusion
Fibrovascular
bands
Vitreous
hemorrhage
Increased VEFG
Tractional retinal
detachment Retina in systemic disease : a color manual of
ophthalmoscopy / Homayoun Tabandeh, Morton F.
Goldberg 2009
Infarction

Edema Retinal
hemorrhage Hard exudates
Microvascular
Leakage

Edema Maculare Diabetico
Diabetic Macular Edema (DME):
Consiste nell’accumulo di fluido
nello spessore della retina a
livello della macula per una
eccessiva essudazione,
leakage, di fluidi e di
macromolecole lipidiche dai
vasi capillari retinici
DME
Microaneurysm Retinal capillary
Fovea
Edema
Retina
RPE layer
Choroid
Hard exudate

Patogenesi del DME
Bhagat N et al. Surv Ophthalmol 2009;54:1–32
AII, angiotensina II; AGE, prodotti finali glicazione avanzata; BRB, barriera
emato-retinica; DAG, diacilglicerolo; ET, endotelina; LPO, lipossigenasi;
MMP, matrice metallo-proteinasi; NO, ossido nitrico; PKC, proteina chinasi
C; PPVP, posterior precortical vitreous pocket; RAS, sistema renina
angiotensina
Ruolo di fattori genetici? Iperglicemia
Edema
maculare
AGEs
ET
VEGF Ipossia IL-6 Destabilizzazione del vitreo
Anomalie nel collagen cross-linking
MMP attività
PPVP
DAG
PKC
Vasocostrizione
Istamine
Recettori ET sui
periciti Danno ossidativo
LPO, NO, NADH/NAD+
Enzimi antiossidanti
RAS
attivazione
Tensione del vitro maculare
Accumulo di
citocheratina e glial
fibrillary acidic
protein
Fosforilazione delle
giunzione proteiche
strette
Disorganizzazione della
BRB
AII

Diabetic macular edema
• Diabetic macular edema can be present at any
stage of the disease, but is more common in
patients with proliferative diabetic retinopathy
• Diabetic macular edema is the leading cause of
legal blindness in diabetics.

DR diagnosis
• ETDRS acuity
• Midriatic examination (retinography)
• OCT – Quantification and qualification of the edema
– Evaluation of the vitreous - retinal interface
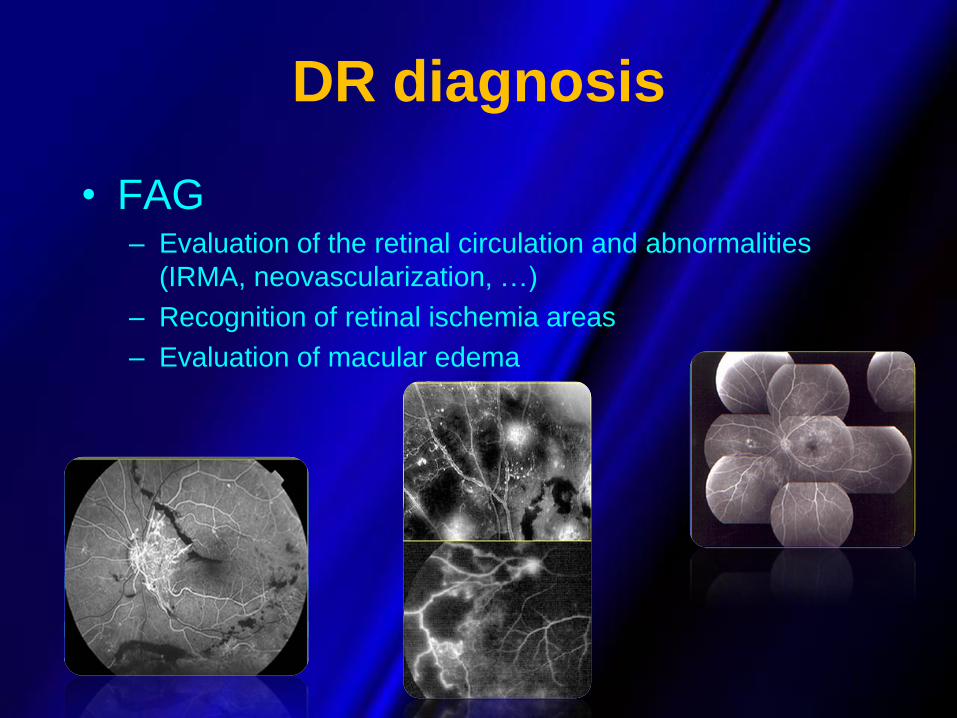
DR diagnosis
• FAG – Evaluation of the retinal circulation and abnormalities
(IRMA, neovascularization, …)
– Recognition of retinal ischemia areas
– Evaluation of macular edema

DR diagnosis
• Microperimetry (SLO)
• Multifocal ERG

DR diagnosis
• Ecography
Risk factors
Changeables Low metabolic
control
Hyperlipemia
Obesity
Smoking
High blood
pressure
Not changeables Age
Familiarity
Race
Duration of
diabetes

Mild nonproliferative diabetic
retinopathy
Microaneurysms

Moderate Nonproliferative
Diabetic Retinopathy (NPDR)
Hard exudates
Flamed shaped
hemorrhage
Microaneurysm

DCCT (Diabetic Control and Complication Trial)

DCCT (Diabetic Control and Complication Trial)
EDIC Study Epidemiology of Diabetes
Interventions and Complications Study


When to treat?
• Loss of vision
• Clinically significant macular edema
• Retinal ischemia
• Neovascularization
• Vitreous hemorrhage
• Consistent vitreous – macular traction

Severe Nonproliferative Diabetic
Retinopathy (NPDR)
Venous
beading
High-Risk Proliferative diabetic
retinopathy
At risk for serious vision loss
Any combination of three of the following four findings
• Presence of vitreous or preretinal hemorrhage.
• Presence of new vessels (neovascularization, NV)
• Location of NV on or near the optic disc.
• Moderate to severe extent of new vessels.

Proliferative diabetic retinopathy
Neovascularization
Hard exudate
Cotton-wool
spotspot
Blot hemorrhage

Proliferative papillary retinopathy

Haemovitreous

Options for the treatment
• Laser photocoagulation: current
standard of care for proliferative
retinopathy or vasogenic CSME
• Anti-VEGFcompounds [RBZ, Aflibercept (VEGF
Trap)]
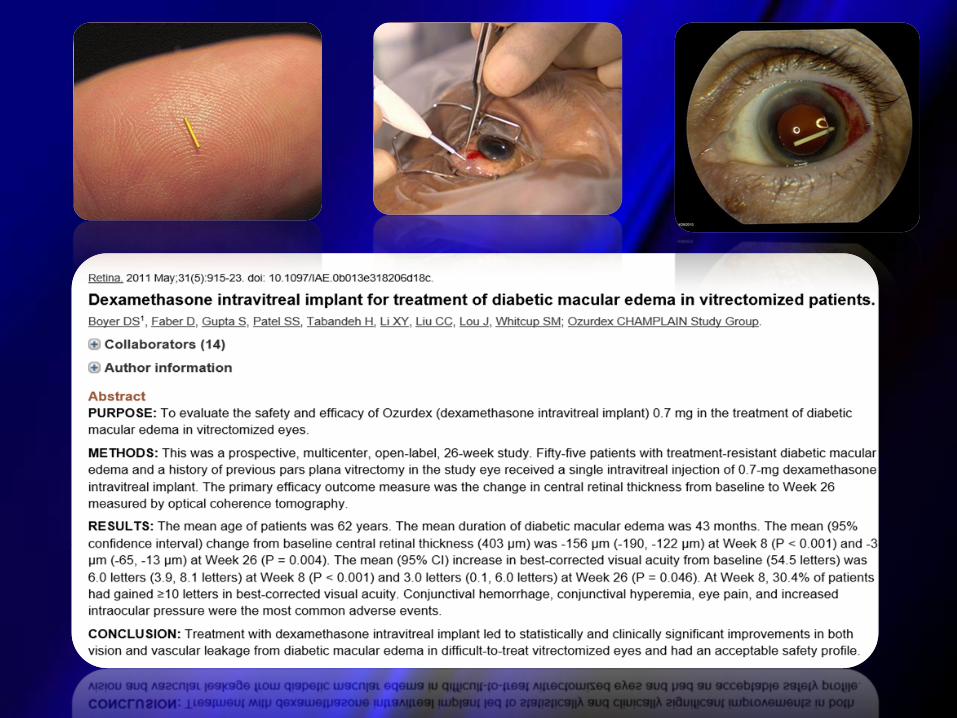
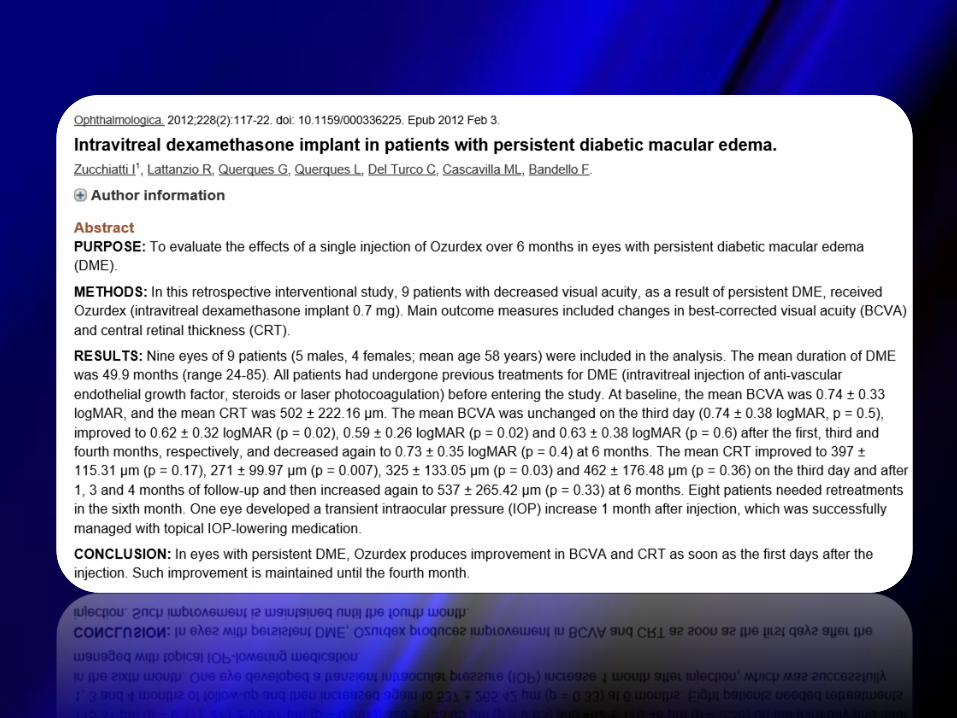
• Steroid implants (dexamethasone, fluocinolone
acetonide)
• Vitrectomy

Panretinal photocoagulation reduced
the incidence of severe vision loss
from proliferative retinopathy by 50%




Laser photocoagulation for DME
Limitations of treatment
o does not eliminate possibility of further vision loss
o improvement in visual acuity is uncommon
o complications including permanent damage to the retinal
pigment epithelium and secondary choroidal neovascularization
36
National Eye Institute, National Institutes of Health. Diabetic Retinopathy. http://www.nei.nih.gov/health/diabetic/retinopathy.asp#4a
Accessed February 2009
AAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009
Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005.
http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf.


PASCAL =
pattern scanning laser

Micropulse mode
Dorin G. Semin Ophthalmol 2003; 18:147-153


Laser in DME
• Il trattamento Laser per lo piu’ non migliora la visione
Trial Cambiamento medio
VA con laser
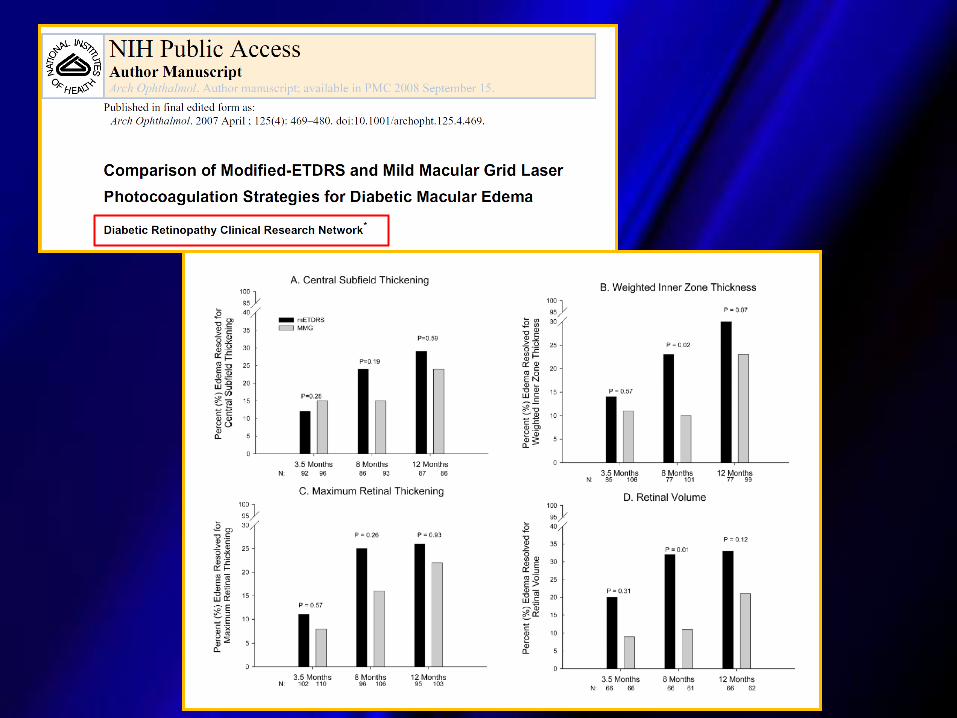
DRCR.net Grid laser vs. IVTA 1 letter
DRCR.net Mod Macular Grid 0 letters
DRCR.net Ranibizumab vs.
prompt/ deferred laser/ IVTA
3 letters
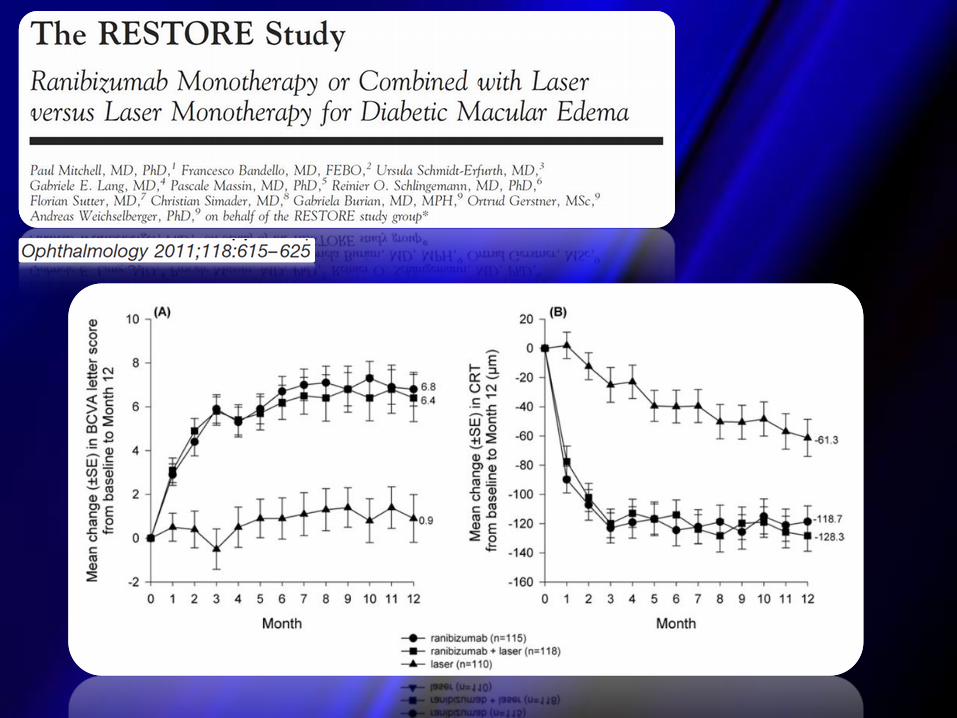
RESTORE 1 letter
BOLT -4.6 letters
Diabetic Retinopathy Clinical Network. Ophthalmology 2008;115:1447-59e10; Diabetic Retinopathy Clinical Network. Ophthalmology
2010;117:1064-77; Mitchell et al. Ophthalmology 2011 118:615-25; Michaelides et al. Ophthalmology 2010;117:1078-86

Ranibizumab
Ranibizumab è un frammento di un anticorpo monoclonale umanizzato che si lega specificatamente e inibisce tutte le isoforme biologicamente attive del VEGF-A
Recettori
VEGF-A
VEGF-A Ranibizumab
Krzystolik et al. Arch Ophthalmol 2002; 120: 338-346 VEGF, fattore di crescita vascolare endoteliale
Inibisce il legame del VEGF-A con
i recettori VEGF, prevenendo la
cascata degli eventi che conduce
all’angiogenesi:
Inibisce la permeabilità
vascolare
Inibisce la proliferazione
endoteliale
Inibisce la migrazione delle
cellule endoteliali

Fase II: RESOLVE (Safety and Efficacy of Ranibizumab in Diabetic Macular Edema)
Massin P,. Diabetes Care 2010 *Tutti i pazienti, gruppi A+B
Set completo di analisi, LOCF
La prima misurazione post-basale di VA era stata effettuata al giorno 8

Fase II: RESOLVE (Safety and Efficacy of Ranibizumab in Diabetic Macular Edema)
Massin P,. Diabetes Care 2010
*Tutti i pazienti, gruppi A+B
Set completo di analisi, LOCF
La prima valutazione post-basale di CRT è stata effettuata il giorno 8
CRT, central retinal thickness

Fase II: Read-2 study
Ranibizumab 0.5 mg PRN Laser Laser PRN
Months 0 1 2 3 4 5 6 7-24 24-36
Group 1: Ranibizumab 0.5 mg
Group 2: Laser
Group 3: Ranibizumab 0.5 mg + laser
Treatment Initiation Phase* Retreatment phase† Retreatment phase‡
Ranibizumab 0.5 mg
*Treatment criteria: Ranibizumab 0.5 mg at baseline, Months 1, 3, and 5 (fixed regimen) for the ranibizumab 0.5 mg group; laser at baseline and again at Month 3 if CSFT ≥250 μm for the laser treatment group; ranibizumab 0.5 mg + laser treatment (always administered 1 week after ranibizumab) at baseline and Month 3 for ranibizumab 0.5 mg + laser treatment group †Retreatment criteria: Ranibizumab 0.5 mg no more than every 2 months or laser no more than every 3 months if the CSFT ≥250 μm; after the primary endpoint (Month 6), if retreatment criteria were met, patients in the RBZ group were treated with 0.5 mg RBZ, patients in the laser group could be treated with laser or RBZ, and patients in the combination group could receive laser plus RBZ or RBZ alone ‡Retreatment criteria: Ranibizumab 0.5 mg given as frequently as monthly if CSFT ≥250 μm
CSFT: center subfield thickness; PRN: pro re nata; RBZ: ranibizumab
Nguyen QG et al. Ophthalmology 2009;116(11):2175-81.e1 Nguyen QG et al. Ophthalmology 2010;117(11):2146-51 Do D et al. Arch Ophthalmol 2013; 131(2):139-145

9
-1
7
5
3
1
11 Ranibizumab 0.5 mg (n = 28) Laser (n = 22) Ranibizumab 0.5 mg + laser (n = 24)
Baseline Month 6 Month 12 Month 24 Month 36
Me
an c
han
ge in
B
CV
A, E
TDR
S le
tte
rs
p = 0.1
p = 0.009
p = 0.3
10.3
1.4
8.9
Patients included in the analysis were those who completed 36 months and the patients who completed 33 months or above; LOCF method was used to impute missing values; statistical comparisons made between Month 24 and Month 36 values for the same group of patients were calculated using the Wilcoxon signed rank test; BCVA: best-corrected visual acuity; ETDRS: Early Treatment Diabetic Retinopathy Study; LOCF: last observation carried forward
There was a significant BCVA improvement of 3.1 ETDRS letters at Month 36 for the patients in ranibizumab group when compared with the Month 24
There was an improvement of 2.0 letters in the ranibizumab + laser group and decline of 1.6 letters in the laser group at Month 36 when compared with Month 24
Ranibizumab allowed as of Month 6
READ-2
49 Do D et al. Arch Ophthalmol 2013; 131(2):139-145
Fase II: Read-2 study

200
250
300
350
400
450
500
Ranibizumab 0.5 mg (n = 28) Laser (n = 22) Ranibizumab 0.5 mg + laser (n = 24)
Baseline Month 6 Month 12 Month 24 Month 36
LOCF method was used to impute missing values; statistical comparisons made between Month 24 and Month 36 values for the same group of patients using the Wilcoxon signed rank test CSFT: center subfield thickness; LOCF: Last observation carried forward
p = 0.12
p = 0.006
p = 0.14
Mea
n f
ove
al t
hic
knes
s, µ
m
282
265
226
Patients in the ranibizumab monotherapy group showed a significant reduction of mean CSFT by 70 µm from Month 24 to Month 36
READ-2
50 Do D et al. Arch Ophthalmol 2013; 131(2):139-145
Fase II: Read-2 study
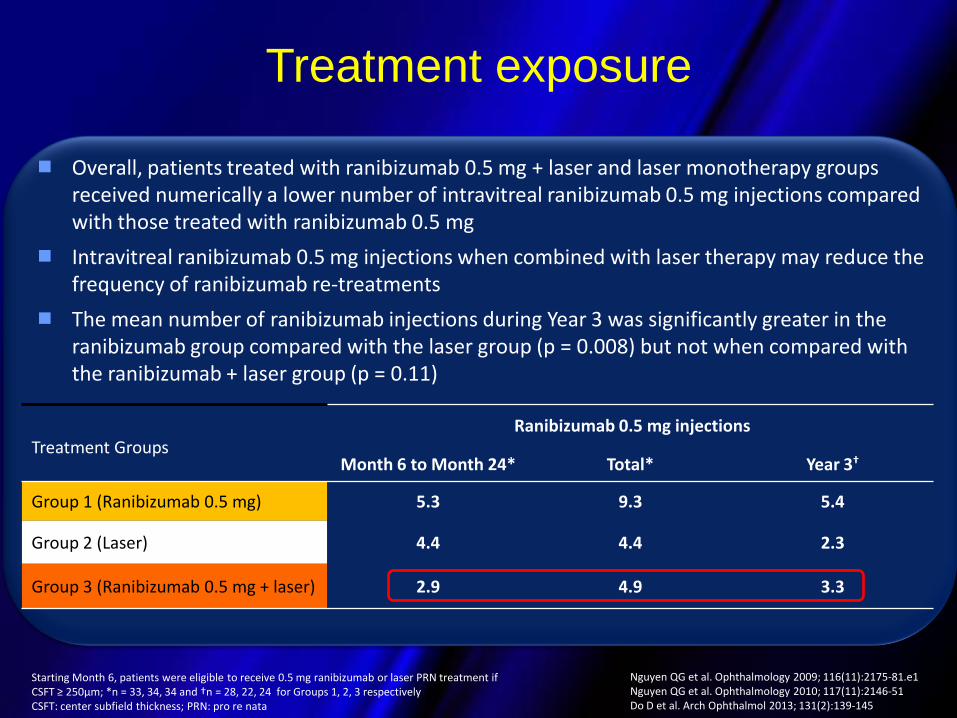
Treatment exposure
Overall, patients treated with ranibizumab 0.5 mg + laser and laser monotherapy groups received numerically a lower number of intravitreal ranibizumab 0.5 mg injections compared with those treated with ranibizumab 0.5 mg
Intravitreal ranibizumab 0.5 mg injections when combined with laser therapy may reduce the frequency of ranibizumab re-treatments
The mean number of ranibizumab injections during Year 3 was significantly greater in the ranibizumab group compared with the laser group (p = 0.008) but not when compared with the ranibizumab + laser group (p = 0.11)
Starting Month 6, patients were eligible to receive 0.5 mg ranibizumab or laser PRN treatment if CSFT ≥ 250µm; *n = 33, 34, 34 and †n = 28, 22, 24 for Groups 1, 2, 3 respectively CSFT: center subfield thickness; PRN: pro re nata
Treatment Groups Ranibizumab 0.5 mg injections
Month 6 to Month 24* Total* Year 3†
Group 1 (Ranibizumab 0.5 mg) 5.3 9.3 5.4
Group 2 (Laser) 4.4 4.4 2.3
Group 3 (Ranibizumab 0.5 mg + laser) 2.9 4.9 3.3
Nguyen QG et al. Ophthalmology 2009; 116(11):2175-81.e1 Nguyen QG et al. Ophthalmology 2010; 117(11):2146-51 Do D et al. Arch Ophthalmol 2013; 131(2):139-145
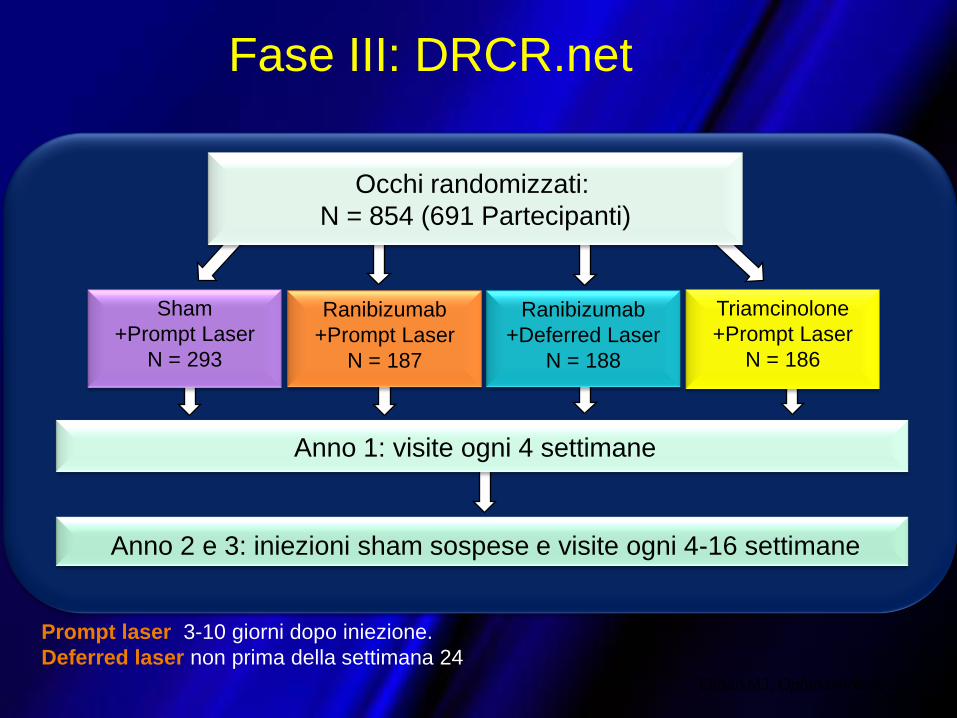
Ranibizumab
+Prompt Laser
N = 187
Ranibizumab
+Deferred Laser
N = 188
Sham
+Prompt Laser
N = 293
Triamcinolone
+Prompt Laser
N = 186
Occhi randomizzati:
N = 854 (691 Partecipanti)
Anno 1: visite ogni 4 settimane
Anno 2 e 3: iniezioni sham sospese e visite ogni 4-16 settimane
Prompt laser 3-10 giorni dopo iniezione.
Deferred laser non prima della settimana 24
Elman MJ, Ophthalmology 2010
Fase III: DRCR.net

53
0
1
2
3
4
5
6
7
8
9
10
11
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80 84 88 92 96 100 104
Sham+prompt laser
Ranibizumab+prompt laser
Ranibizumab+deferred laser
Triamcinolone+prompt laser
Primary outcome time point
* Values that were ±30 letters were assigned a value of 30
P-values for difference in mean change in visual acuity from sham+prompt laser at the 52-week visit:
ranibizumab+prompt laser <0.001; ranibizumab+deferred laser <0.001; and triamcinolone+prompt laser=0.31.
Fase III: DRCR.net

Elman MJ, Ophthalmology 2012
Fase III: DRCR.net
RBZ+deferred laser
RBZ+prompt laser
+9,7
+6,8

Elman MJ, Ophthalmology 2012
Fase III: DRCR.net
RBZ+deffered laser
RBZ+prompt laser
- 152 µm
- 174 µm

Sham
+Prompt
Laser
Ranibizumab
+Prompt
Laser
Ranibizumab
+Deferred
Laser
Triamcinolone
+Prompt
Laser
No. iniezioni 1° anno n/a 8 9 3
No. iniezioni 2° anno
n/a 2 3 1
No. iniezioni 3° anno n/a 1 2 n/a
Fase III: DRCR.net

Fase III: RESTORE
Fase III, doppio cieco
N=315
Valutazione dell’efficacia e della
sicurezza con iniezioni mensili di
ranibizumab (0.5 mg) come terapia
aggiuntiva alla fotocoagulazione laser
e/o monoterapia in pazienti con visual
impairment dovuto a DME
12 mesi con estensione in aperto a 36
mesi
Obiettivo primario: dimostrare la superiorità di Ranibizumab (0.5mg) in monoterapia e/o in
terapia aggiuntiva al trattamento laser vs terapia laser basandosi sui cambiamenti medi di AV
rispetto al basale in un periodo di trattamento di 12 mesi
Iniziezione
sham
Diminuzione visiva
causata da DME
Randomizzati 1:1:1
N=315
Sham laser Active laser
111
Ranibizumab
0.5 mg
86
Ranibizumab
0.5 mg
118
Active laser

+7.9 +7.9
+7.1 +6.7
+2.3
+5.4
-2
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36
Var
iazi
on
e m
ed
ia in
BC
VA
dal
bas
ale
(l
ette
re E
DR
S)
Mesi
Ranibizumab 0.5 mg (n = 83) Ranibizumab 0.5 mg + laser (n = 83) Laser (n = 74)
Core study assessment Interim Analysis Full analysis/Study
completion
Core study Extension study (Ranibizumab 0.5 mg PRN)
+8.0
+6.7 +6.0
59
I pazienti trattati dal primo anno con ranibizumab mantengono il miglioramento
medio della BCVA a 36 mesi
I pazienti trattati con laser il primo anno e poi passati a un trattamento con
ranibizumab hanno un miglioramento medio progressivo della BCVA dal mese
12 al mese 36
Mitchell P et al. AAO Nov 2012 PO532
Fase III: RESTORE



VEGF TRAP EYE/
AFLIBERCEPT
• Similar to ranibizumab and bevacizumab,
aflibercept binds to all isomers of the VEGF-A
family.
• Additionally, aflibercept binds to VEGF-B and
placental growth factor; it is hypothesized that
by blocking these factors, aflibercept may
prove to be more efficacious




Randomised controlled trials
of vitrectomy surgery for PDR

Randomised controlled trials
of vitrectomy surgery for DME



Algoritmo di trattamento per DME
Bandello et all:Treatment Recommendations for DME, Eye 2012,1-9

76
Management Paradigms for Diabetic Macular Edema
Paul Mitchell, Tien Yin Wong

Linee guida per lo screening, la diagnostica e il
trattamento della RD in Italia: aggiornamento 2013