Presentazione standard di PowerPoint - Aristea Calabro Genova.pdf · doppia cecità Maggior...
51
PCSK9 inibitori: Basi fisiopatologiche ed impiego clinico Alirocumab Paolo Calabrò Cattedra Cardiologia Seconda Università Napoli
Transcript of Presentazione standard di PowerPoint - Aristea Calabro Genova.pdf · doppia cecità Maggior...

PCSK9 inibitori: Basi fisiopatologiche ed
impiego clinico
Alirocumab
Paolo Calabrò Cattedra Cardiologia
Seconda Università Napoli
Lith
uan
ia
Ger
man
y
Ro
man
ia
Po
lan
d
Fin
lan
d
Swed
en
Bel
giu
m
Ital
y
Fran
ce
Net
her
lan
ds
Spai
n
UK
Irel
and
6000
5000
4000
3000
2000
1000
0
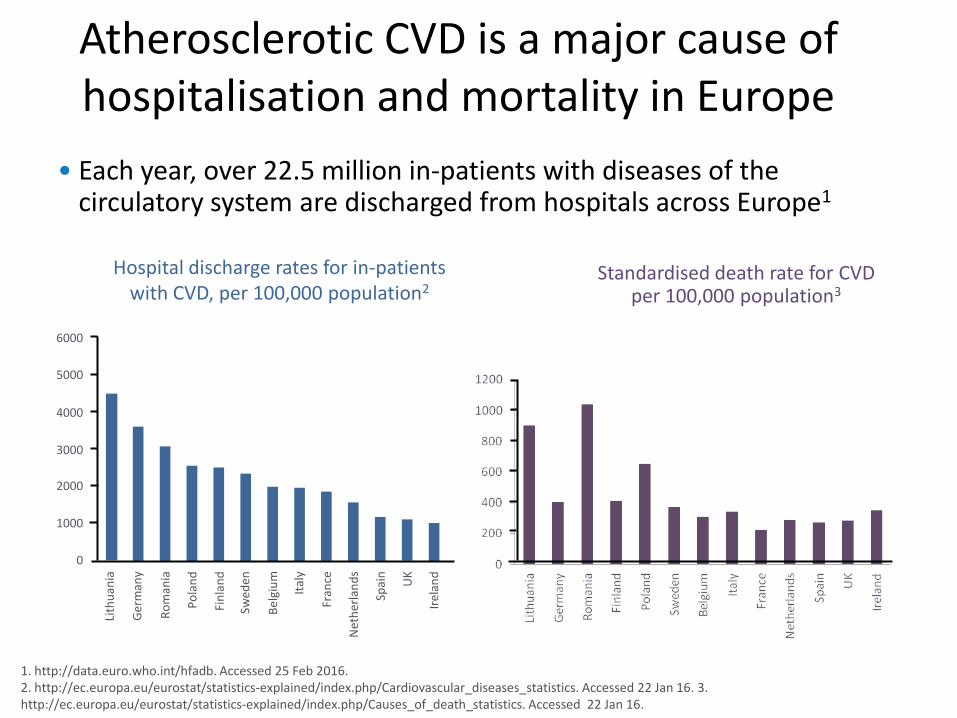
Atherosclerotic CVD is a major cause of hospitalisation and mortality in Europe
• Each year, over 22.5 million in-patients with diseases of the circulatory system are discharged from hospitals across Europe1
1. http://data.euro.who.int/hfadb. Accessed 25 Feb 2016. 2. http://ec.europa.eu/eurostat/statistics-explained/index.php/Cardiovascular_diseases_statistics. Accessed 22 Jan 16. 3. http://ec.europa.eu/eurostat/statistics-explained/index.php/Causes_of_death_statistics. Accessed 22 Jan 16.
Hospital discharge rates for in-patients with CVD, per 100,000 population2
Standardised death rate for CVD per 100,000 population3
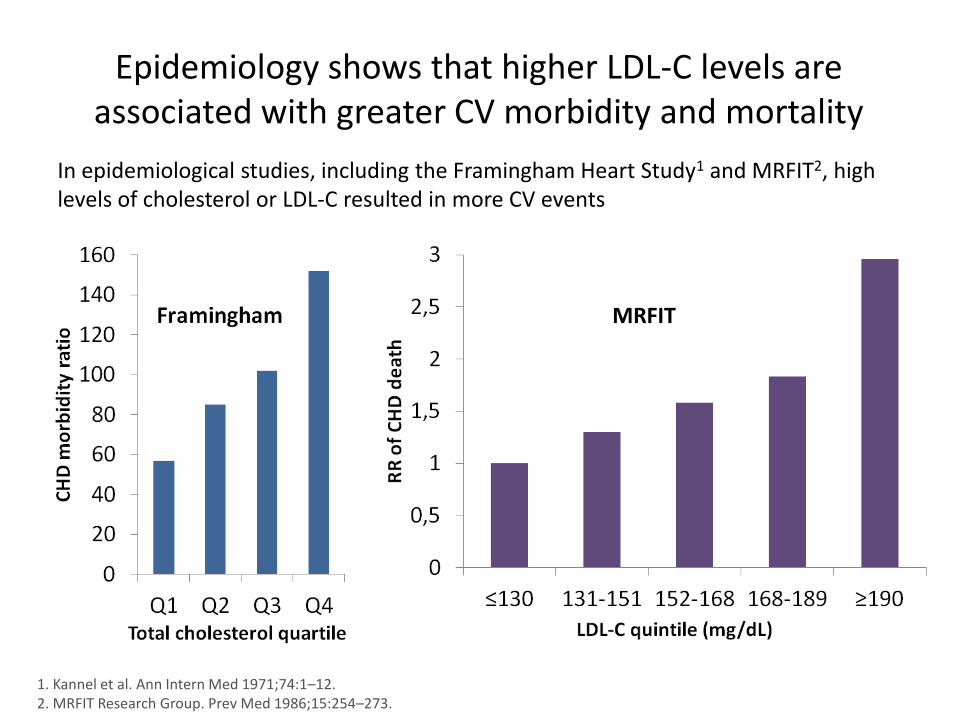
Epidemiology shows that higher LDL-C levels are associated with greater CV morbidity and mortality
In epidemiological studies, including the Framingham Heart Study1 and MRFIT2, high levels of cholesterol or LDL-C resulted in more CV events
1. Kannel et al. Ann Intern Med 1971;74:1–12. 2. MRFIT Research Group. Prev Med 1986;15:254–273.
MRFIT
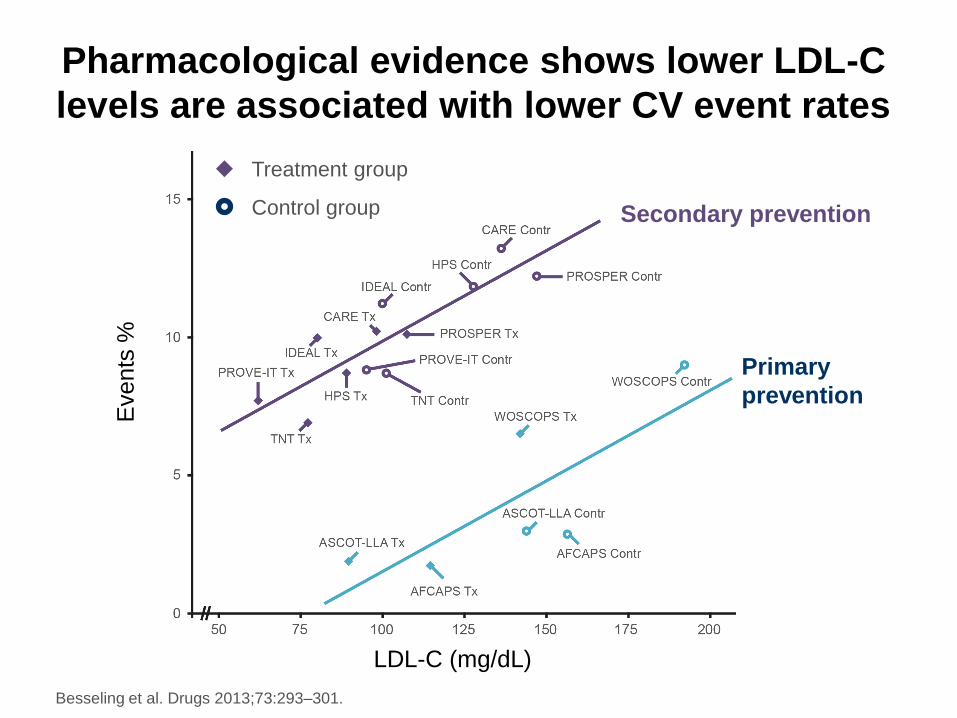
Pharmacological evidence shows lower LDL-C
levels are associated with lower CV event rates
Besseling et al. Drugs 2013;73:293–301.
Even
ts %
LDL-C (mg/dL)
Treatment group
Control group Secondary prevention
Primary
prevention
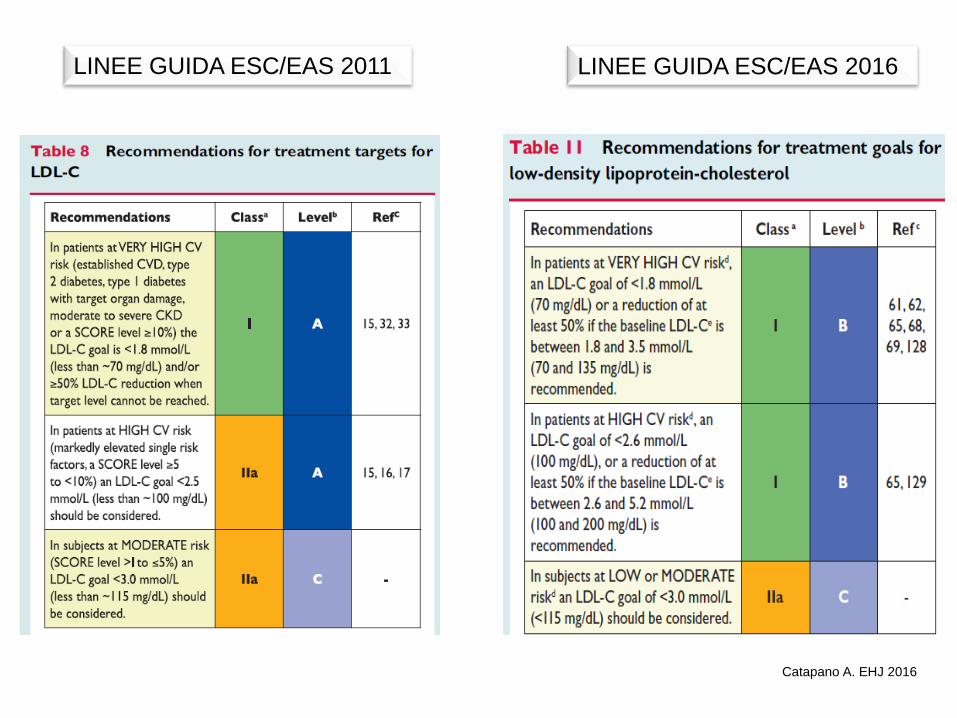
LINEE GUIDA ESC/EAS 2011 LINEE GUIDA ESC/EAS 2016
Catapano A. EHJ 2016
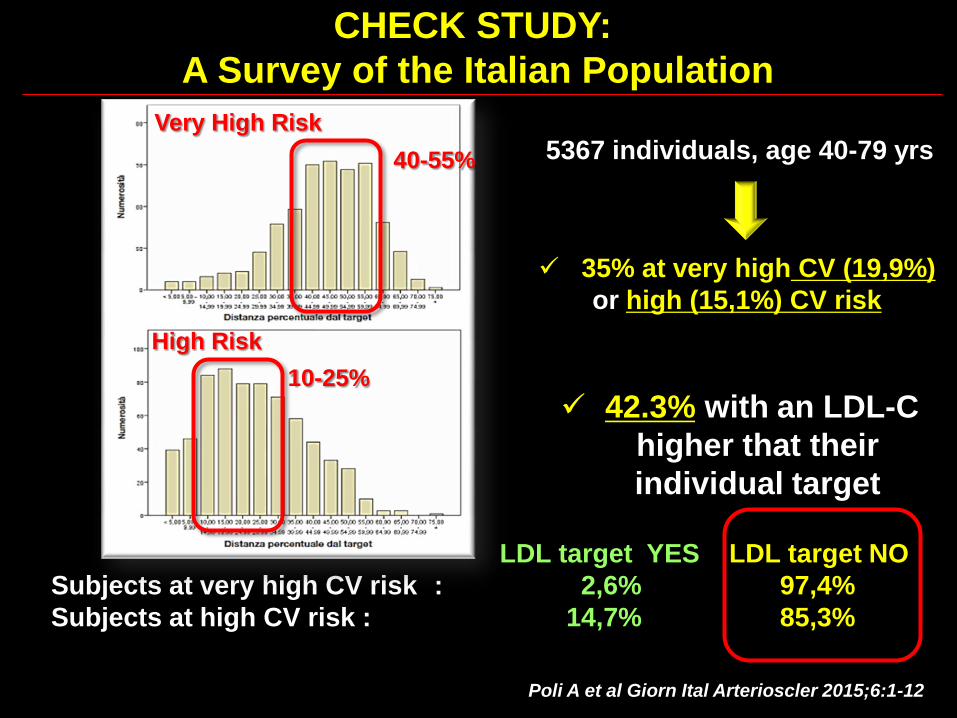
CHECK STUDY:
A Survey of the Italian Population
area dei soggetti “non a target”
Poli A et al Giorn Ital Arterioscler 2015;6:1-12
5367 individuals, age 40-79 yrs
42.3% with an LDL-C
higher that their
individual target
35% at very high CV (19,9%)
or high (15,1%) CV risk
LDL target YES LDL target NO
Subjects at very high CV risk : 2,6% 97,4%
Subjects at high CV risk : 14,7% 85,3%
Very High Risk
40-55%
High Risk
10-25%
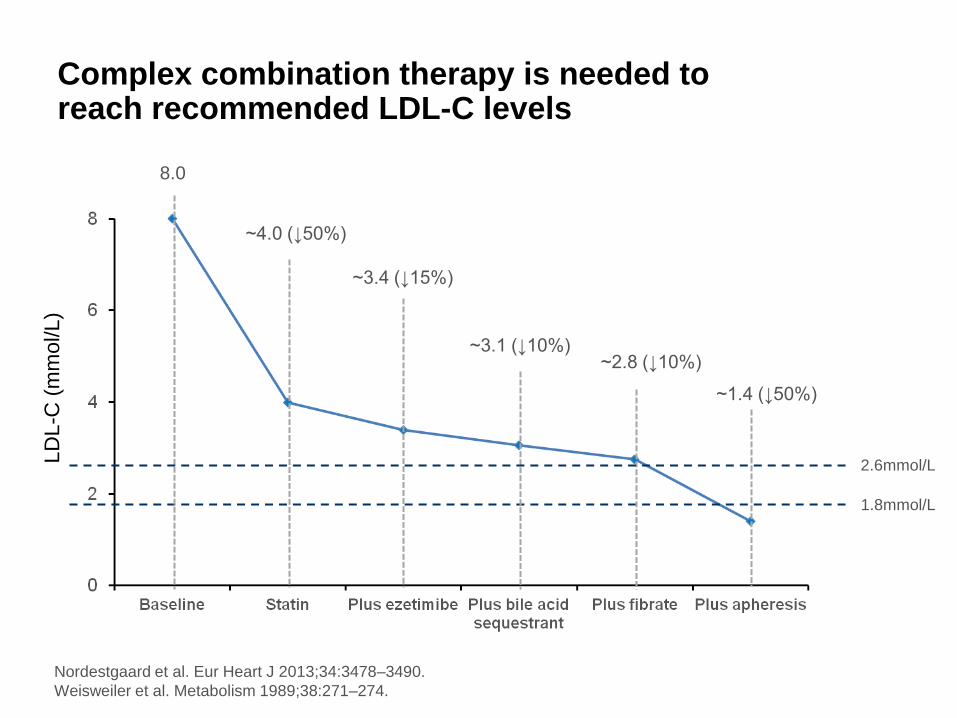
Complex combination therapy is needed to reach recommended LDL-C levels
Nordestgaard et al. Eur Heart J 2013;34:3478–3490.
Weisweiler et al. Metabolism 1989;38:271–274.
LD
L-C
(m
mol/L)
8.0
~4.0 (↓50%)
~3.4 (↓15%)
~3.1 (↓10%) ~2.8 (↓10%)
2.6mmol/L
1.8mmol/L
~1.4 (↓50%)
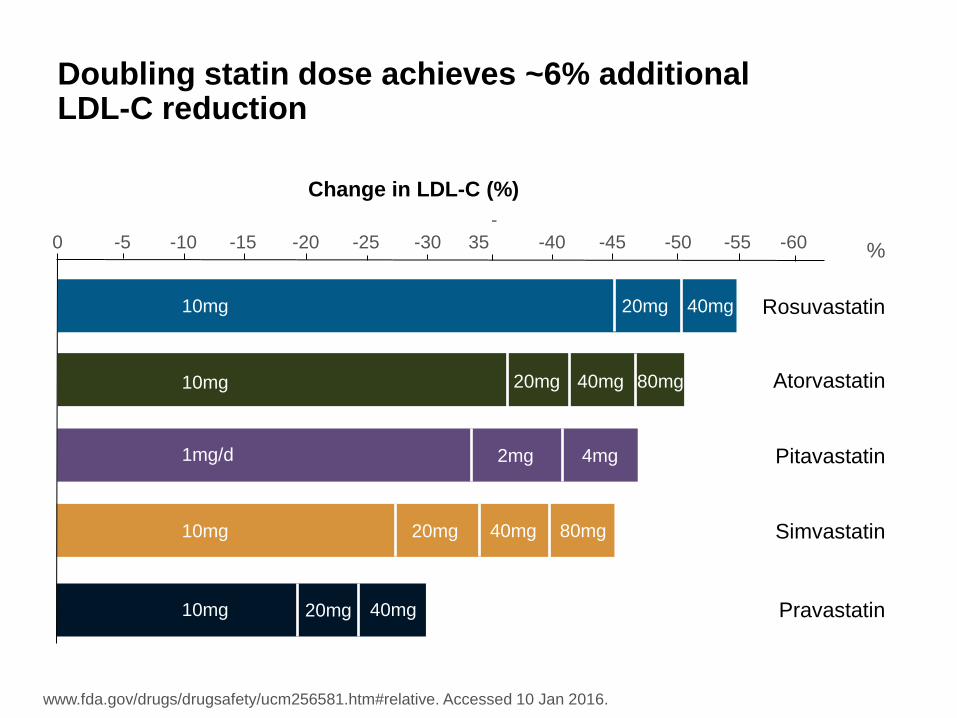
% -60 -55 -50 -45 -40
-
35 -30 -25 -20 -15 -10 -5 0
Rosuvastatin
10mg
40mg 20mg
20mg Atorvastatin 80mg 40mg
Simvastatin 10mg 20mg 40mg 80mg
Pravastatin 10mg 20mg 40mg
Pitavastatin 1mg/d 2mg 4mg
10mg
Doubling statin dose achieves ~6% additional LDL-C reduction
www.fda.gov/drugs/drugsafety/ucm256581.htm#relative. Accessed 10 Jan 2016.
Change in LDL-C (%)
ALIROCUMAB
• Alirocumab: cosa è e come agisce
• Efficacia su LDL-C (in associazione a statine)
• Quando impiegarlo (popolazioni Target)
• Potenziali benefici su eventi CV
*Proprotein Convertase Subtilisin/kexin Type 9 (PCSK9)
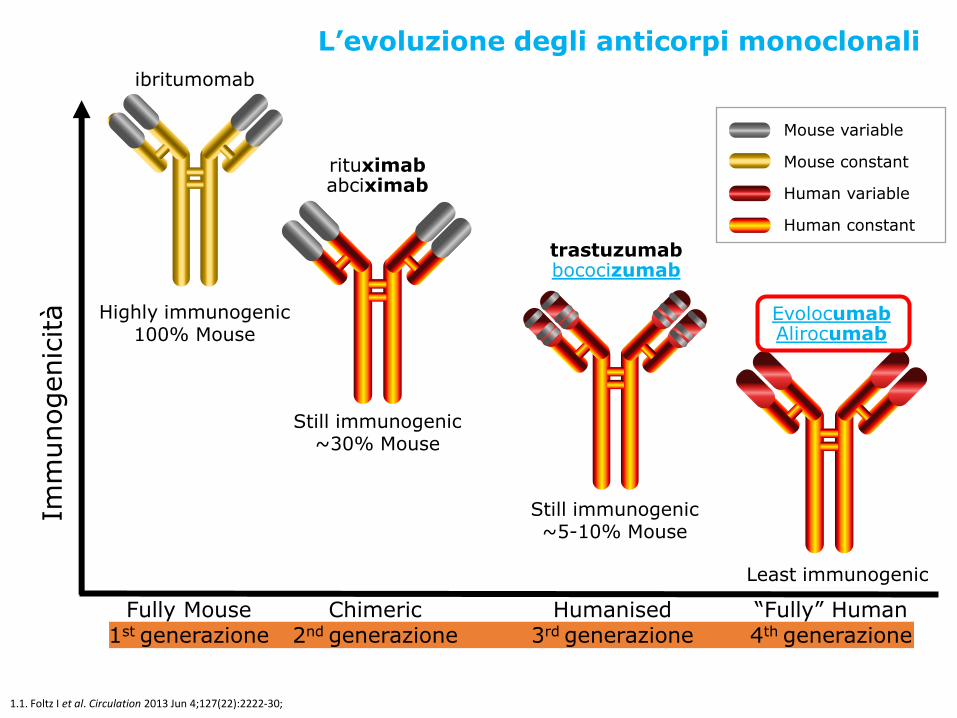
Imm
unogenic
ità
Fully Mouse 1st generazione
Chimeric 2nd generazione
Humanised 3rd generazione
“Fully” Human 4th generazione
Highly immunogenic 100% Mouse
Still immunogenic ~30% Mouse
rituximab abciximab
Still immunogenic ~5-10% Mouse
trastuzumab bococizumab
Least immunogenic
Evolocumab Alirocumab
ibritumomab
Mouse variable
Mouse constant
Human variable
Human constant
1.1. Foltz I et al. Circulation 2013 Jun 4;127(22):2222-30;
L’evoluzione degli anticorpi monoclonali
BLA 125559 Animal Toxicology Summary – C. Lee Elmore, PhD
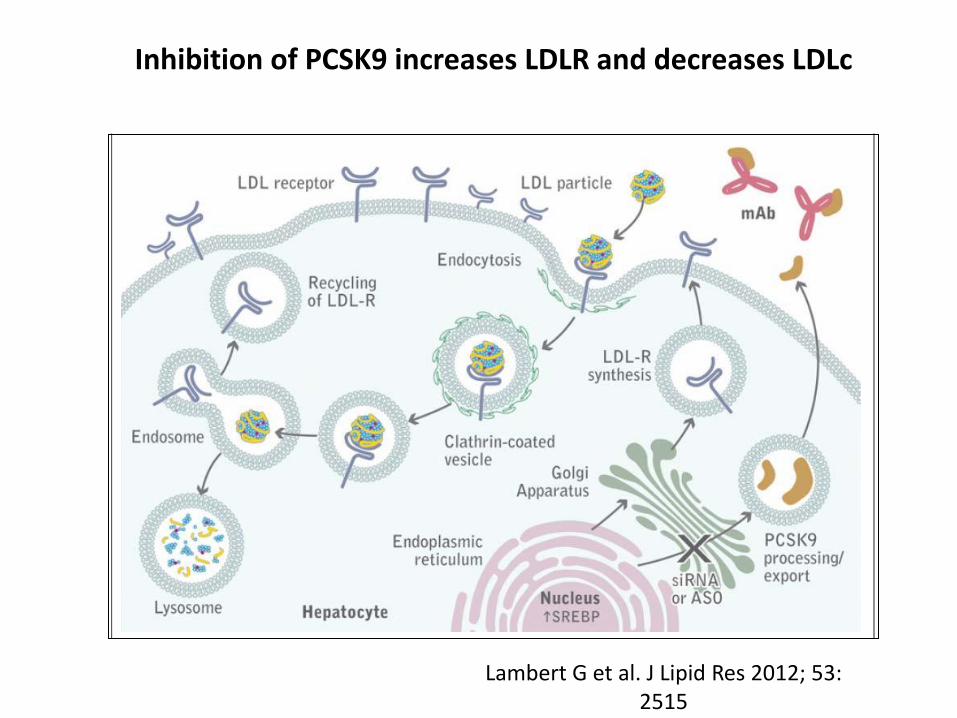
Figure 3: Alirocumab inhibits PCSK9, increases LDLR, and decreases LDL-C
Alirocumab bound to PCSK9 (represented here by mAb, monoclonal antibody) prevents the association
between PCSK9 and the LDLR. The LDLR binds the LDL particle and is internalized. The LDL particle is
degraded in the lysosome, but the LDLR is recycled back to the plasma membrane. SREBP, sterol
regulatory element binding protein. ASO, antisense oligonucleotides and siRNA, small interfering RNAs
are alternate mechanisms for targeting PCSK9 at the transcriptional level.
(Adapted from Lambert G, et al.3)
PCSK9 and LDLR pharmacology:
Transcription of PCSK9 and LDLR genes share a common regulatory mechanism mediated by
sterol regulatory element-binding protein 2 (SREBP2). SREBP2 interacts with another
membrane protein, SREBP cleavage-activating protein (SCAP), which functions as a sterol
sensor. Intracellular sterols inhibit LDLR and PCSK9 gene transcription by suppressing the
processing and release of SREBP2. In the presence of sterols, inactive SREBP2 remains bound
to the endoplasmic reticulum after synthesis.4
In the sterol-depleted state, SCAP escorts the SREBP2 to the Golgi where it is proteolytically
cleaved, which releases the mature SREBP2 capable of transcriptional activation. Mature
SREBP2 enters the nucleus and binds to the sterol regulatory element 1 (SRE-1) site of LDLR and PCSK9 promoters, leading to increased transcription and translation of both proteins.
3 Lambert G, et al. “The PCSK9 decade” J Lipid Res 2012; 53:2515-2524.
4 Dong B, et al. “CETP inhibitors downregulate hepatic LDL receptor and PCSK9 expression in vitro and in vivo
through a SREBP2 dependent mechanism” Atherosclerosis 2014; 235:449-462.
3
Inhibition of PCSK9 increases LDLR and decreases LDLc
Lambert G et al. J Lipid Res 2012; 53: 2515
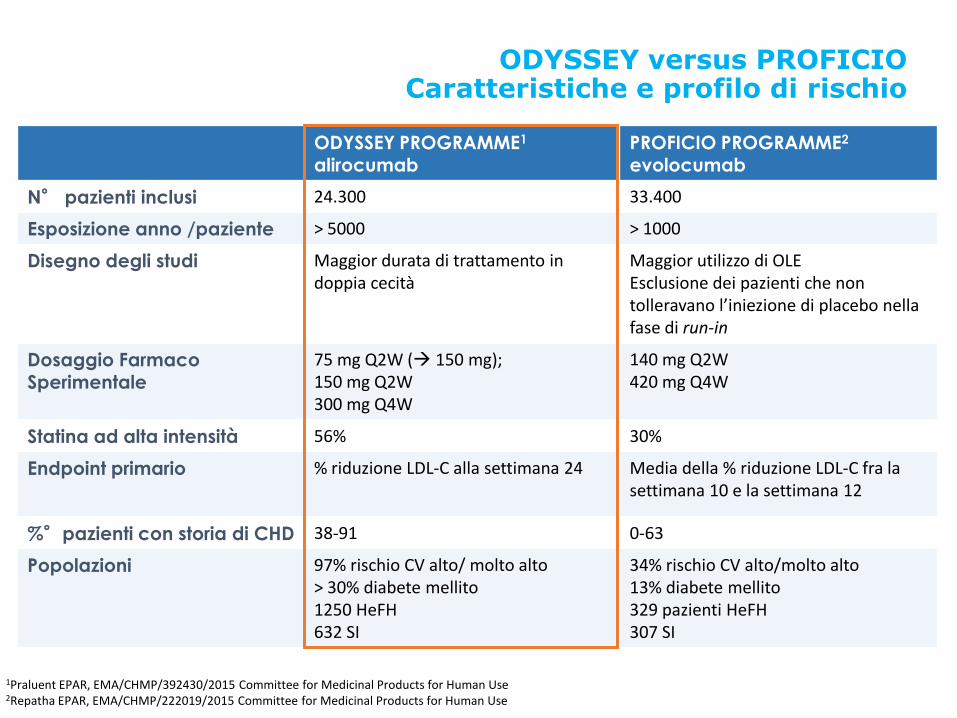
ODYSSEY versus PROFICIO Caratteristiche e profilo di rischio
1Praluent EPAR, EMA/CHMP/392430/2015 Committee for Medicinal Products for Human Use 2Repatha EPAR, EMA/CHMP/222019/2015 Committee for Medicinal Products for Human Use
ODYSSEY PROGRAMME1
alirocumab PROFICIO PROGRAMME2
evolocumab
N° pazienti inclusi 24.300 33.400
Esposizione anno /paziente > 5000 > 1000
Disegno degli studi Maggior durata di trattamento in doppia cecità
Maggior utilizzo di OLE Esclusione dei pazienti che non tolleravano l’iniezione di placebo nella fase di run-in
Dosaggio Farmaco
Sperimentale
75 mg Q2W ( 150 mg); 150 mg Q2W 300 mg Q4W
140 mg Q2W 420 mg Q4W
Statina ad alta intensità 56% 30%
Endpoint primario % riduzione LDL-C alla settimana 24 Media della % riduzione LDL-C fra la settimana 10 e la settimana 12
%°pazienti con storia di CHD 38-91 0-63
Popolazioni 97% rischio CV alto/ molto alto > 30% diabete mellito 1250 HeFH 632 SI
34% rischio CV alto/molto alto 13% diabete mellito 329 pazienti HeFH 307 SI
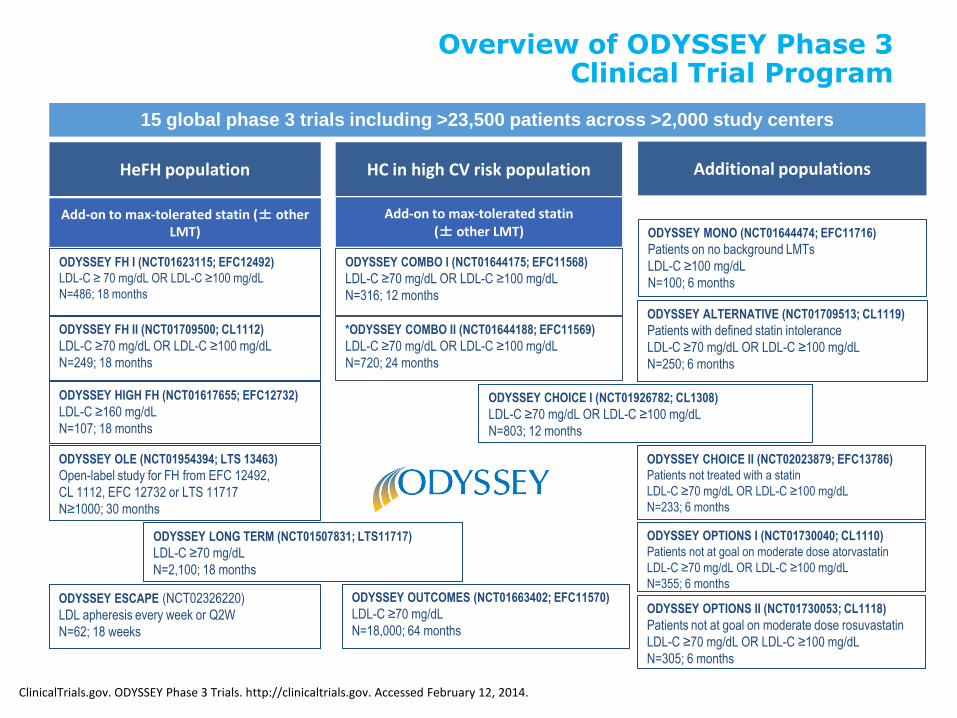
Overview of ODYSSEY Phase 3 Clinical Trial Program
15 global phase 3 trials including >23,500 patients across >2,000 study centers
ODYSSEY OUTCOMES (NCT01663402; EFC11570)
LDL-C ≥70 mg/dL
N=18,000; 64 months
HC in high CV risk population
ODYSSEY COMBO I (NCT01644175; EFC11568)
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=316; 12 months
Add-on to max-tolerated statin (± other LMT)
*ODYSSEY COMBO II (NCT01644188; EFC11569)
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=720; 24 months
Additional populations
ODYSSEY ALTERNATIVE (NCT01709513; CL1119)
Patients with defined statin intolerance
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=250; 6 months
ODYSSEY OPTIONS II (NCT01730053; CL1118)
Patients not at goal on moderate dose rosuvastatin
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=305; 6 months
ODYSSEY MONO (NCT01644474; EFC11716)
Patients on no background LMTs
LDL-C ≥100 mg/dL
N=100; 6 months
ODYSSEY OPTIONS I (NCT01730040; CL1110)
Patients not at goal on moderate dose atorvastatin
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=355; 6 months
ODYSSEY CHOICE I (NCT01926782; CL1308)
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=803; 12 months
ODYSSEY CHOICE II (NCT02023879; EFC13786)
Patients not treated with a statin
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=233; 6 months
ODYSSEY FH II (NCT01709500; CL1112)
LDL-C ≥70 mg/dL OR LDL-C ≥100 mg/dL
N=249; 18 months
HeFH population
ODYSSEY HIGH FH (NCT01617655; EFC12732)
LDL-C ≥160 mg/dL
N=107; 18 months
ODYSSEY FH I (NCT01623115; EFC12492)
LDL-C ≥ 70 mg/dL OR LDL-C ≥100 mg/dL
N=486; 18 months
ODYSSEY LONG TERM (NCT01507831; LTS11717)
LDL-C ≥70 mg/dL
N=2,100; 18 months
Add-on to max-tolerated statin (± other LMT)
ODYSSEY OLE (NCT01954394; LTS 13463)
Open-label study for FH from EFC 12492,
CL 1112, EFC 12732 or LTS 11717
N≥1000; 30 months
ClinicalTrials.gov. ODYSSEY Phase 3 Trials. http://clinicaltrials.gov. Accessed February 12, 2014.
ODYSSEY ESCAPE (NCT02326220)
LDL apheresis every week or Q2W
N=62; 18 weeks
Anticorpo monoclonale Anti PCSK9*: ALIROCUMAB
• Alirocumab: cos è e come agisce
• Efficacia su LDL-C (in associazione a statine e/o altre LLT)
• Quando impiegarlo (popolazioni Target)
• Potenziali benefici su eventi CV
*Proprotein Convertase Subtilisin/kexin Type 9 (PCSK9)
ClinicalTrials.gov. ODYSSEY Phase 3 Trials. http://clinicaltrials.gov. Accessed February 12, 2014.
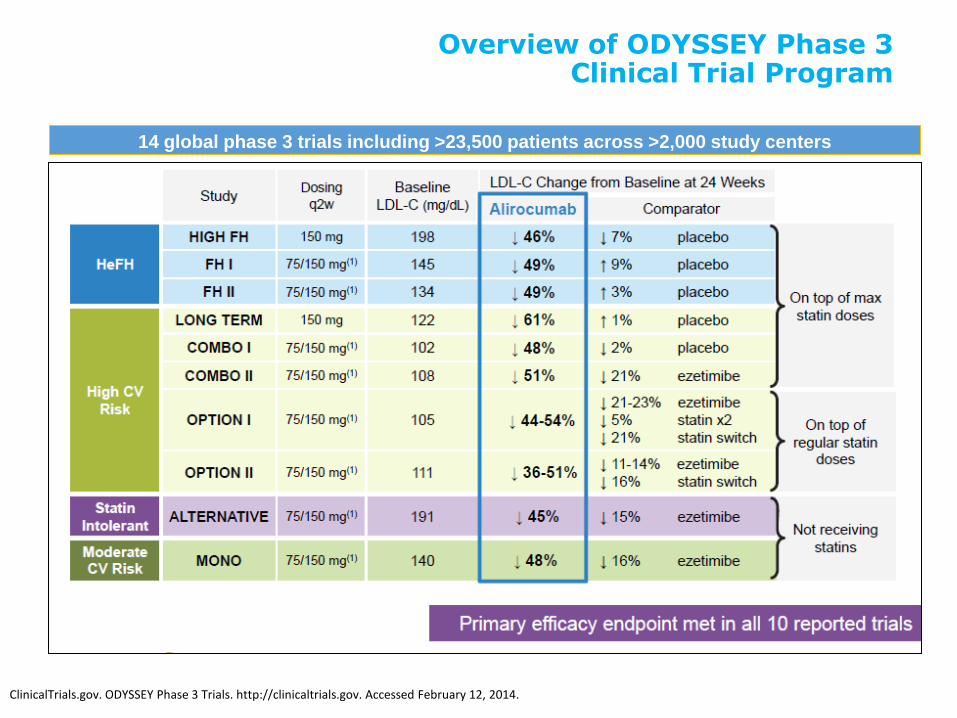
14 global phase 3 trials including >23,500 patients across >2,000 study centers
Overview of ODYSSEY Phase 3 Clinical Trial Program
Anticorpo monoclonale Anti PCSK9*: ALIROCUMAB
• Alirocumab: cos è e come agisce
• Efficacia su LDL-C (in associazione a statine)
• Quando impiegarlo (popolazioni Target)
• Potenziali benefici su eventi CV
*Proprotein Convertase Subtilisin/kexin Type 9 (PCSK9)
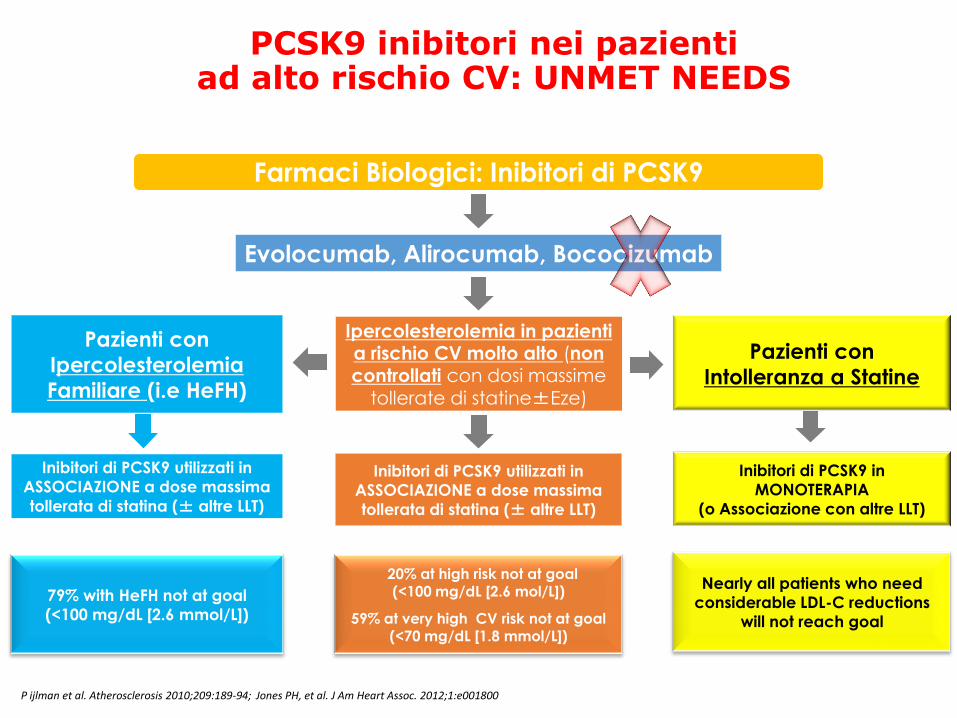
Ipercolesterolemia in pazienti a rischio CV molto alto (non controllati con dosi massime
tollerate di statine±Eze)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
Pazienti con
Ipercolesterolemia
Familiare (i.e HeFH)
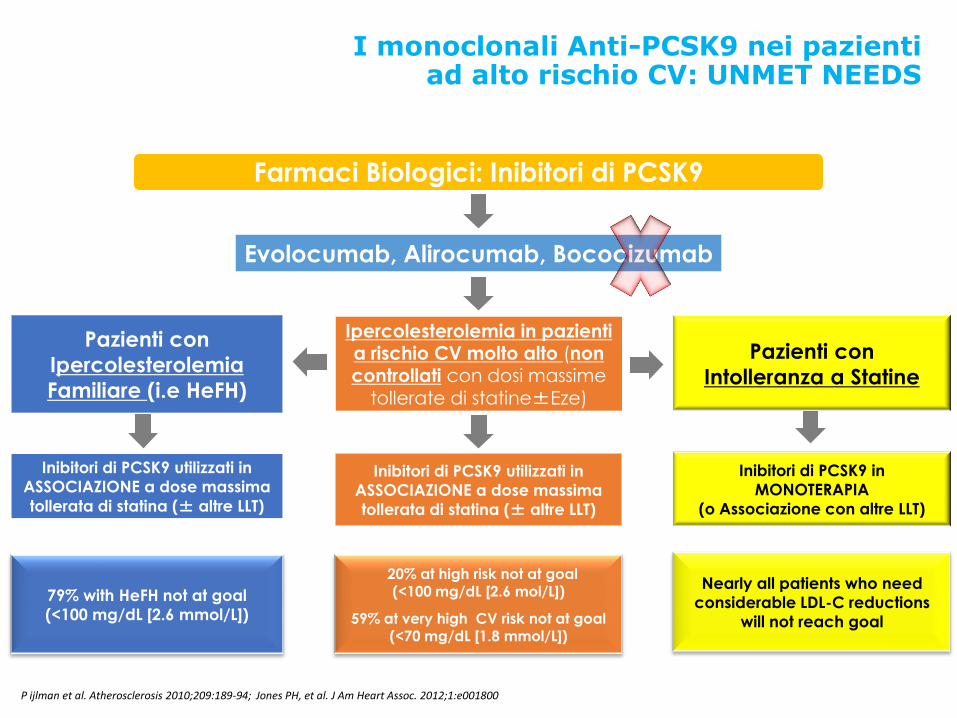
PCSK9 inibitori nei pazienti ad alto rischio CV: UNMET NEEDS
Farmaci Biologici: Inibitori di PCSK9
Evolocumab, Alirocumab, Bococizumab
Inibitori di PCSK9 in
MONOTERAPIA
(o Associazione con altre LLT)
Pazienti con
Intolleranza a Statine
79% with HeFH not at goal
(<100 mg/dL [2.6 mmol/L])
20% at high risk not at goal (<100 mg/dL [2.6 mol/L])
59% at very high CV risk not at goal (<70 mg/dL [1.8 mmol/L])
Nearly all patients who need
considerable LDL-C reductions
will not reach goal
P ijlman et al. Atherosclerosis 2010;209:189-94; Jones PH, et al. J Am Heart Assoc. 2012;1:e001800
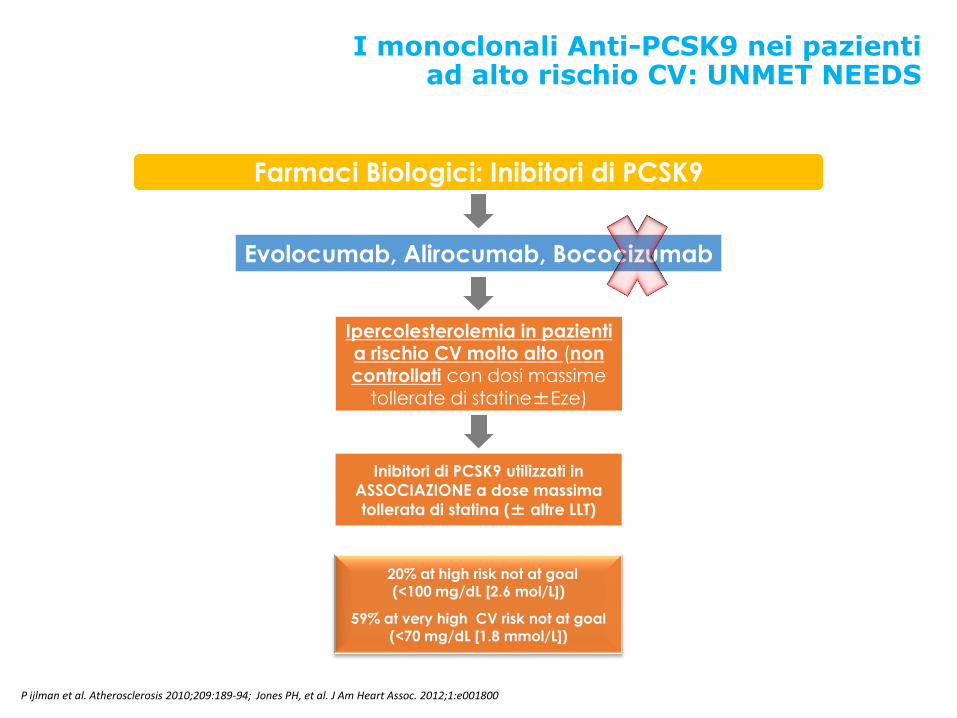
Ipercolesterolemia in pazienti a rischio CV molto alto (non controllati con dosi massime
tollerate di statine±Eze)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
I monoclonali Anti-PCSK9 nei pazienti ad alto rischio CV: UNMET NEEDS
Farmaci Biologici: Inibitori di PCSK9
Evolocumab, Alirocumab, Bococizumab
20% at high risk not at goal (<100 mg/dL [2.6 mol/L])
59% at very high CV risk not at goal (<70 mg/dL [1.8 mmol/L])
P ijlman et al. Atherosclerosis 2010;209:189-94; Jones PH, et al. J Am Heart Assoc. 2012;1:e001800
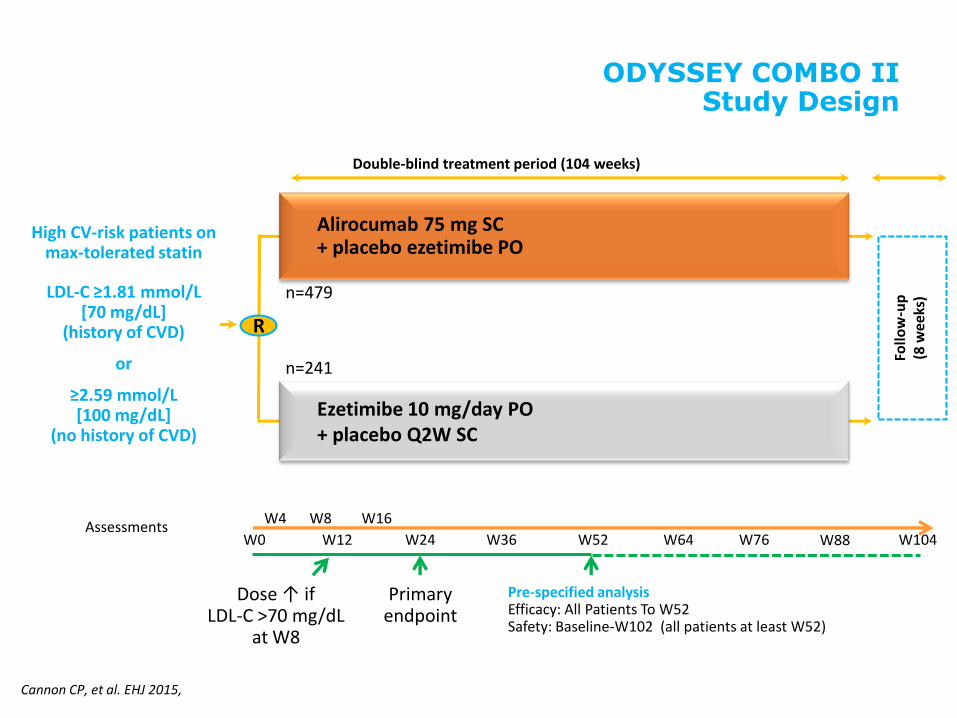
ODYSSEY COMBO II Study Design
Double-blind treatment period (104 weeks)
High CV-risk patients on max-tolerated statin
LDL-C ≥1.81 mmol/L [70 mg/dL]
(history of CVD)
or
≥2.59 mmol/L [100 mg/dL]
(no history of CVD)
R
n=479
n=241
Assessments W0
W4 W8
W12
W16
W24 W36 W52
Primary endpoint
W64 W76 W104
Dose ↑ if LDL-C >70 mg/dL
at W8
W88
Follo
w-u
p
(8 w
eeks
)
Alirocumab 75 mg SC + placebo ezetimibe PO
Ezetimibe 10 mg/day PO + placebo Q2W SC
Pre-specified analysis Efficacy: All Patients To W52 Safety: Baseline-W102 (all patients at least W52)
Cannon CP, et al. EHJ 2015,
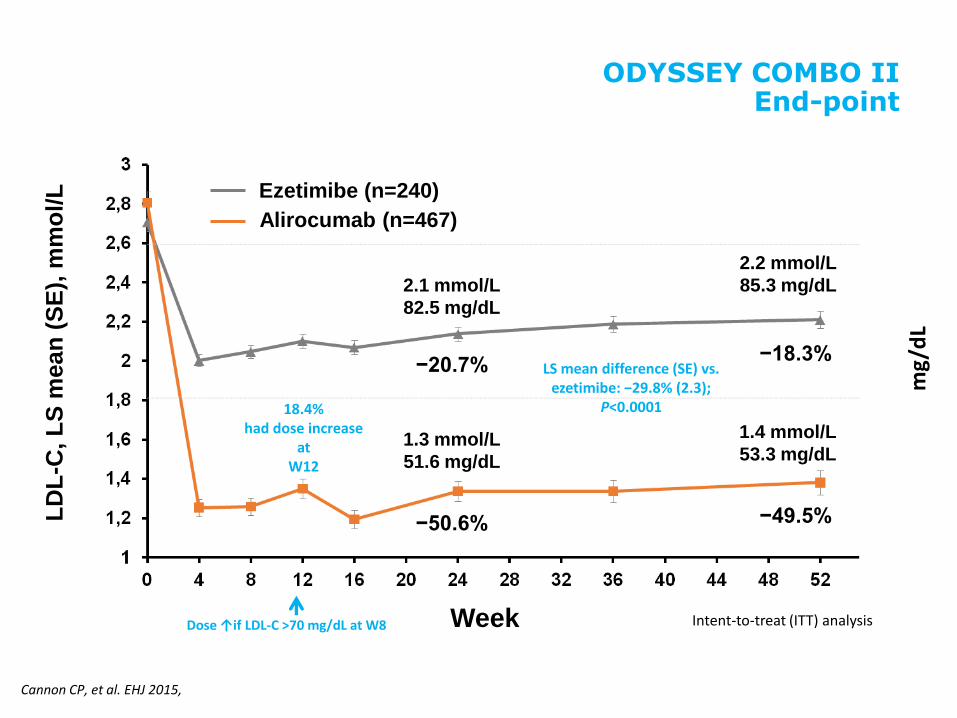
LD
L-C
, L
S m
ean
(S
E),
mm
ol/
L
Ezetimibe (n=240)
Week
2.1 mmol/L
82.5 mg/dL
1.3 mmol/L
51.6 mg/dL
Alirocumab (n=467)
2.2 mmol/L
85.3 mg/dL
1.4 mmol/L
53.3 mg/dL
mg/
dL
Intent-to-treat (ITT) analysis Dose ↑if LDL-C >70 mg/dL at W8
−20.7%
−50.6%
−18.3%
−49.5%
Cannon CP, et al. EHJ 2015,
LS mean difference (SE) vs. ezetimibe: −29.8% (2.3);
P<0.0001 18.4% had dose increase
at W12
ODYSSEY COMBO II End-point
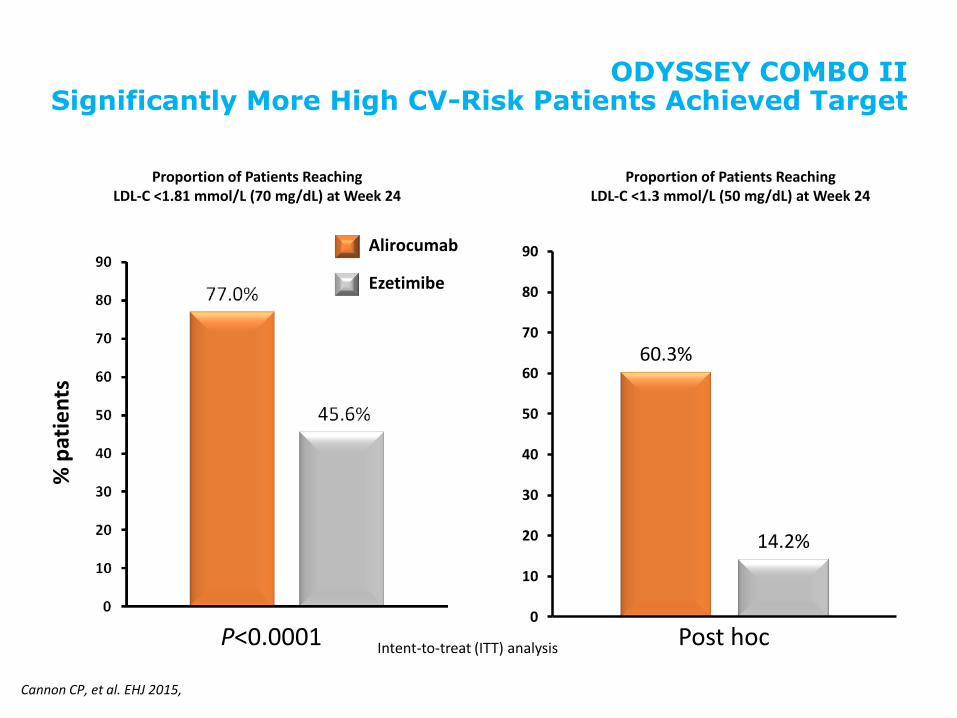
ODYSSEY COMBO II Significantly More High CV-Risk Patients Achieved Target
Proportion of Patients Reaching LDL-C <1.81 mmol/L (70 mg/dL) at Week 24
% p
atie
nts
P<0.0001 Intent-to-treat (ITT) analysis
60.3%
14.2%
0
10
20
30
40
50
60
70
80
90
Proportion of Patients Reaching LDL-C <1.3 mmol/L (50 mg/dL) at Week 24
% p
atie
nts
Ezetimibe
Alirocumab
Post hoc
Cannon CP, et al. EHJ 2015,
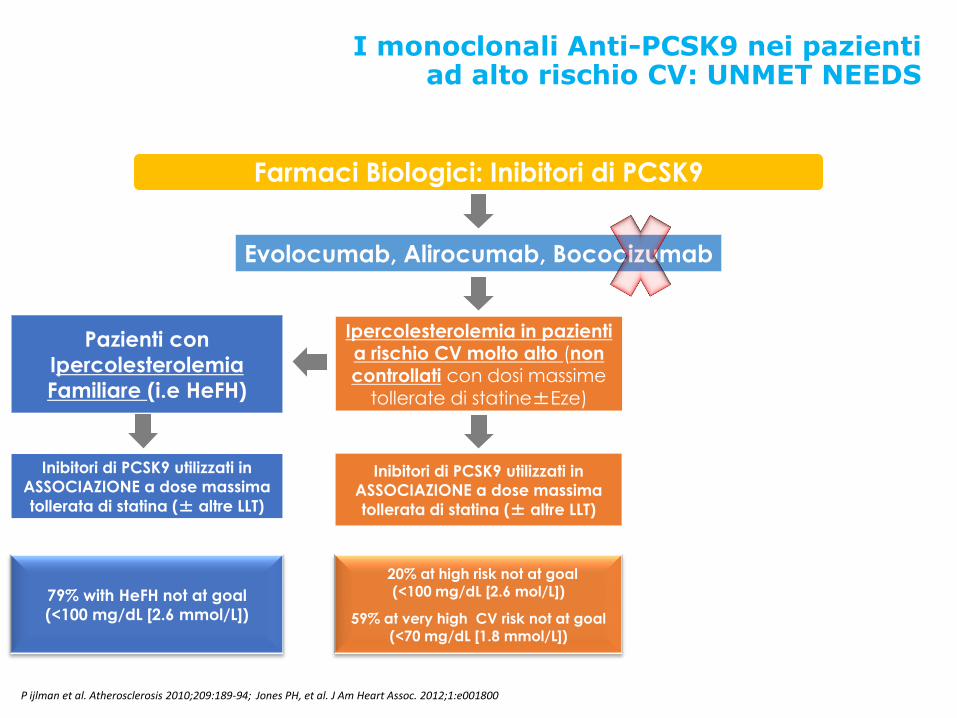
Ipercolesterolemia in pazienti a rischio CV molto alto (non controllati con dosi massime
tollerate di statine±Eze)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
I monoclonali Anti-PCSK9 nei pazienti ad alto rischio CV: UNMET NEEDS
Farmaci Biologici: Inibitori di PCSK9
Evolocumab, Alirocumab, Bococizumab
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
Pazienti con
Ipercolesterolemia
Familiare (i.e HeFH)
79% with HeFH not at goal
(<100 mg/dL [2.6 mmol/L])
20% at high risk not at goal (<100 mg/dL [2.6 mol/L])
59% at very high CV risk not at goal (<70 mg/dL [1.8 mmol/L])
P ijlman et al. Atherosclerosis 2010;209:189-94; Jones PH, et al. J Am Heart Assoc. 2012;1:e001800
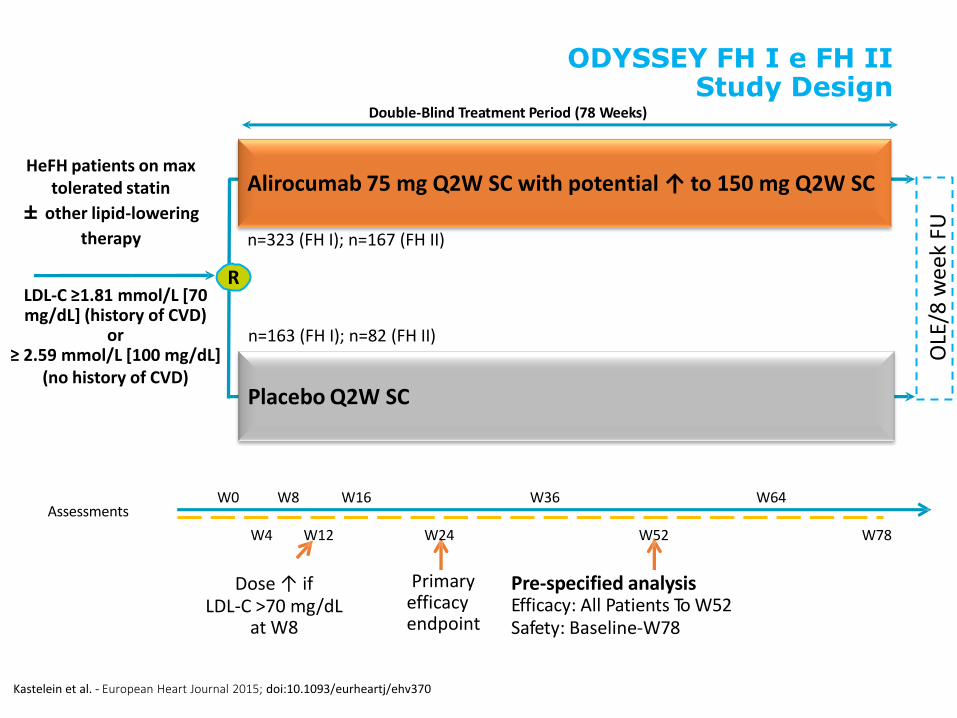
ODYSSEY FH I e FH II Study Design
Placebo Q2W SC
HeFH patients on max tolerated statin
± other lipid-lowering
therapy
OLE
/8 w
eek
FU
Alirocumab 75 mg Q2W SC with potential ↑ to 150 mg Q2W SC
Assessments W0 W8 W16 W36
W52 W78
Double-Blind Treatment Period (78 Weeks)
Primary efficacy endpoint
W64
W4 W12 W24
Dose ↑ if LDL-C >70 mg/dL
at W8
Pre-specified analysis Efficacy: All Patients To W52 Safety: Baseline-W78
R LDL-C ≥1.81 mmol/L [70 mg/dL] (history of CVD)
or ≥ 2.59 mmol/L [100 mg/dL]
(no history of CVD)
Kastelein et al. - European Heart Journal 2015; doi:10.1093/eurheartj/ehv370
n=323 (FH I); n=167 (FH II)
n=163 (FH I); n=82 (FH II)
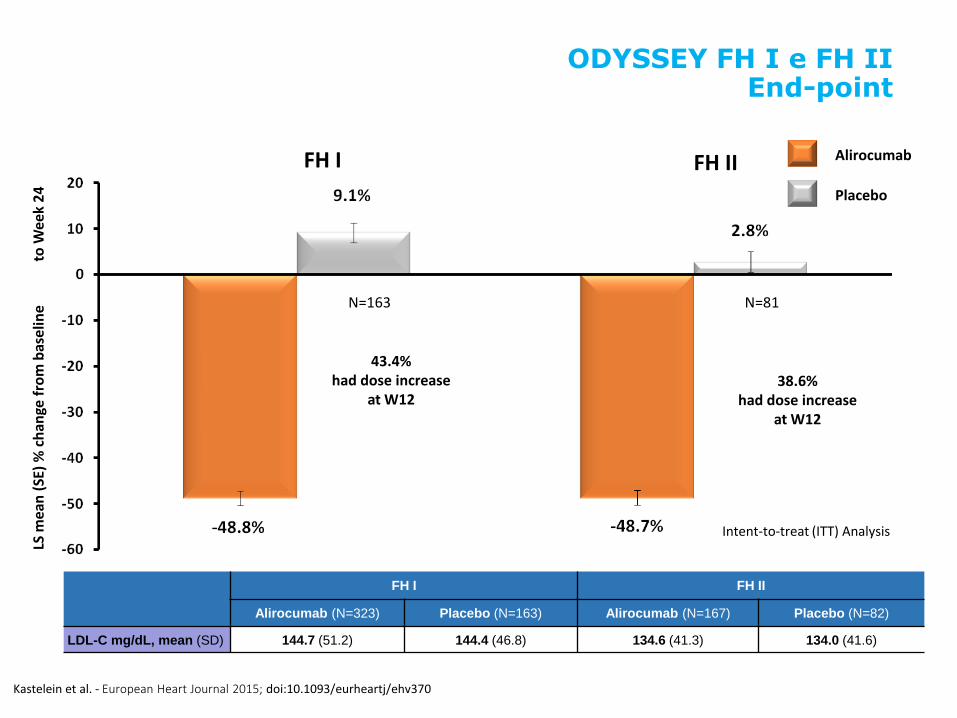
LS m
ean
(SE
) %
ch
ange
fro
m b
ase
line
t
o W
eek
24
N=163
Alirocumab
N=81
FH I
Placebo
FH II
43.4% had dose increase
at W12 38.6%
had dose increase at W12
Intent-to-treat (ITT) Analysis
Kastelein et al. - European Heart Journal 2015; doi:10.1093/eurheartj/ehv370
FH I FH II
Alirocumab (N=323) Placebo (N=163) Alirocumab (N=167) Placebo (N=82)
LDL-C mg/dL, mean (SD) 144.7 (51.2) 144.4 (46.8) 134.6 (41.3) 134.0 (41.6)
ODYSSEY FH I e FH II End-point
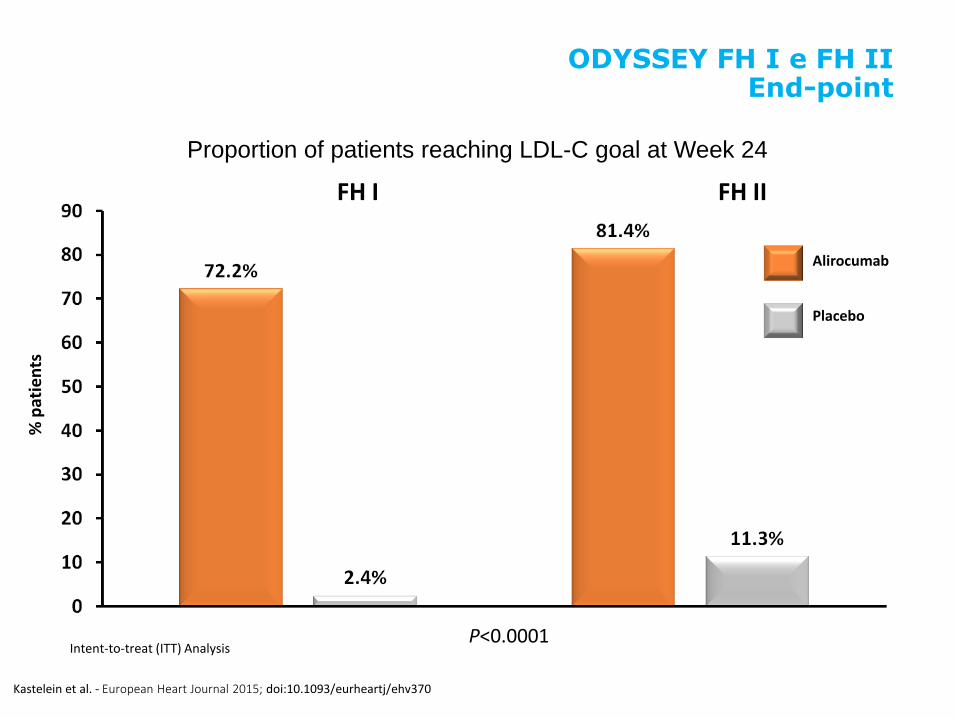
P<0.0001
% p
atie
nts
Placebo
Proportion of patients reaching LDL-C goal at Week 24
FH I FH II
Alirocumab
Intent-to-treat (ITT) Analysis
ODYSSEY FH I e FH II End-point
Kastelein et al. - European Heart Journal 2015; doi:10.1093/eurheartj/ehv370
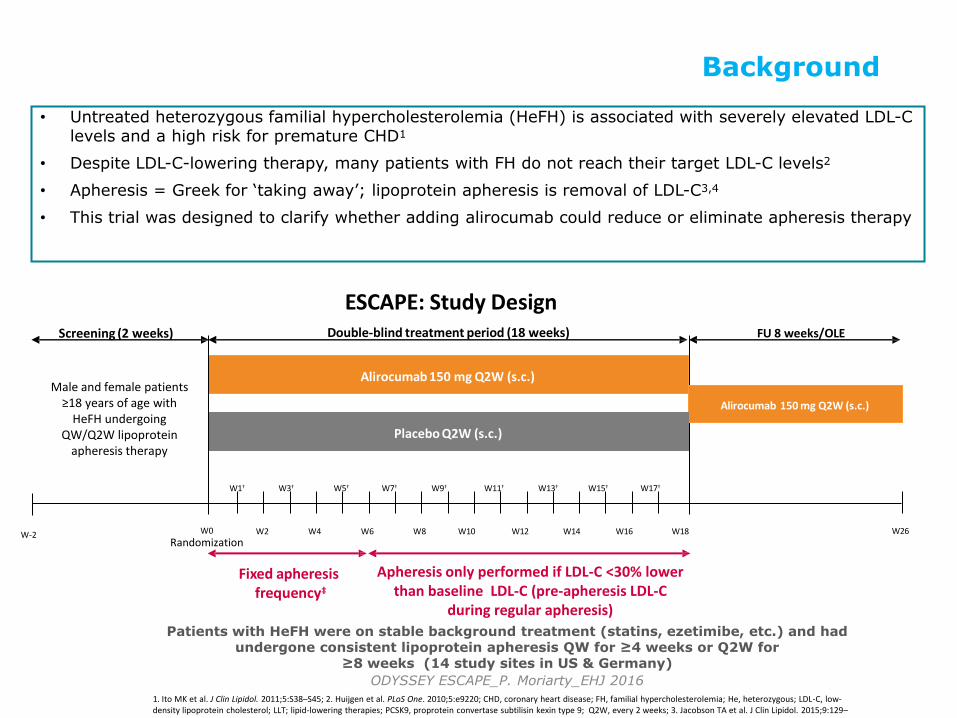
Background
Patients with HeFH were on stable background treatment (statins, ezetimibe, etc.) and had undergone consistent lipoprotein apheresis QW for ≥4 weeks or Q2W for
≥8 weeks (14 study sites in US & Germany)
ODYSSEY ESCAPE_P. Moriarty_EHJ 2016
1. Ito MK et al. J Clin Lipidol. 2011;5:S38–S45; 2. Huijgen et al. PLoS One. 2010;5:e9220; CHD, coronary heart disease; FH, familial hypercholesterolemia; He, heterozygous; LDL-C, low-density lipoprotein cholesterol; LLT; lipid-lowering therapies; PCSK9, proprotein convertase subtilisin kexin type 9; Q2W, every 2 weeks; 3. Jacobson TA et al. J Clin Lipidol. 2015;9:129–169; 4. Reiner Z et al. Eur Heart J. 2011; 32:1769–1818
• Untreated heterozygous familial hypercholesterolemia (HeFH) is associated with severely elevated LDL-C levels and a high risk for premature CHD1
• Despite LDL-C-lowering therapy, many patients with FH do not reach their target LDL-C levels2
• Apheresis = Greek for ‘taking away’; lipoprotein apheresis is removal of LDL-C3,4
• This trial was designed to clarify whether adding alirocumab could reduce or eliminate apheresis therapy
Apheresis only performed if LDL-C <30% lower than baseline LDL-C (pre-apheresis LDL-C
during regular apheresis)
FU 8 weeks/OLE Screening (2 weeks)
W12
Alirocumab 150 mg Q2W (s.c.)
W-2
Placebo Q2W (s.c.)
W9†
W6 W4 W18 W16 W26
Fixed apheresis frequency‡
ESCAPE: Study Design Double-blind treatment period (18 weeks)
Alirocumab 150 mg Q2W (s.c.)
W0
Randomization
W1† W13†
W2
W5† W7†
W8 W10
W11† W3†
W14
W15† W17†
Male and female patients ≥18 years of age with
HeFH undergoing QW/Q2W lipoprotein
apheresis therapy
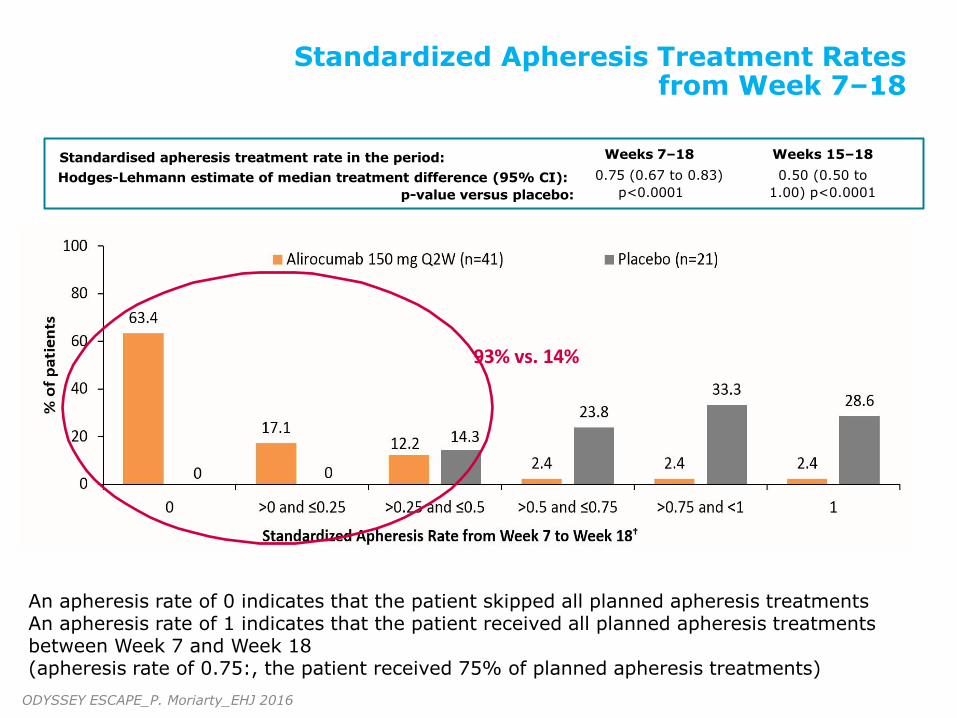
Standardized Apheresis Treatment Rates from Week 7–18
An apheresis rate of 0 indicates that the patient skipped all planned apheresis treatments An apheresis rate of 1 indicates that the patient received all planned apheresis treatments between Week 7 and Week 18 (apheresis rate of 0.75:, the patient received 75% of planned apheresis treatments)
Standardised apheresis treatment rate in the period:
Hodges-Lehmann estimate of median treatment difference (95% CI):
p-value versus placebo:
Weeks 7–18
0.75 (0.67 to 0.83)
p<0.0001
Weeks 15–18
0.50 (0.50 to
1.00) p<0.0001
93% vs. 14%
ODYSSEY ESCAPE_P. Moriarty_EHJ 2016
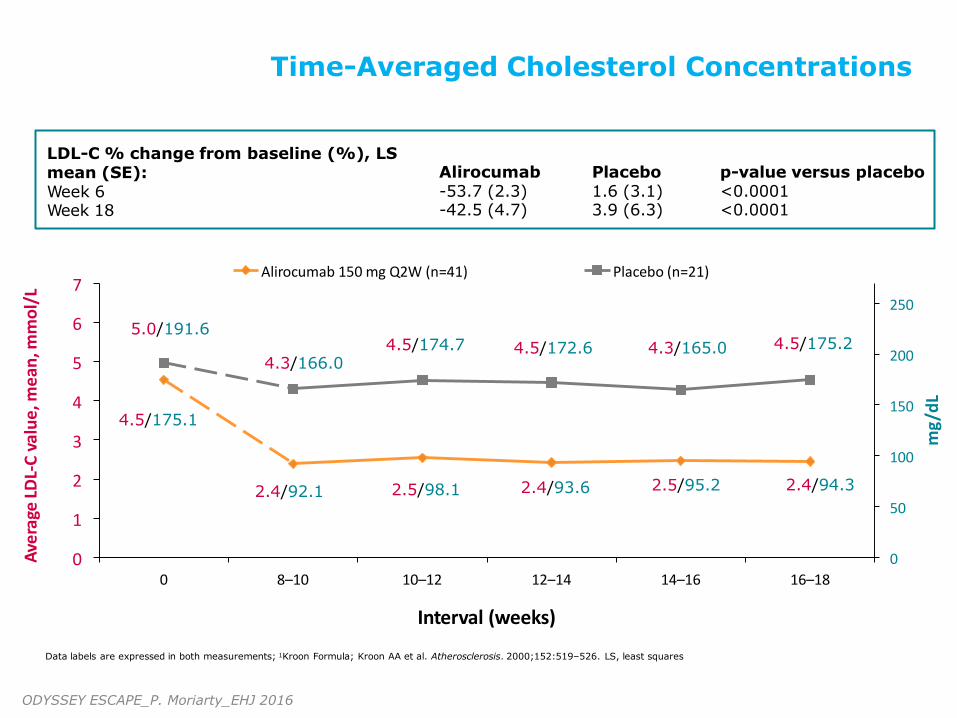
Time-Averaged Cholesterol Concentrations
0 8–10 10–12 12–14 14–16
Interval (weeks) Data labels are expressed in both measurements; 1Kroon Formula; Kroon AA et al. Atherosclerosis. 2000;152:519–526. LS, least squares
LDL-C % change from baseline (%), LS mean (SE): Week 6 Week 18
Alirocumab -53.7 (2.3) -42.5 (4.7)
Placebo 1.6 (3.1) 3.9 (6.3)
p-value versus placebo <0.0001 <0.0001
0
50
100
150
200
250
0
1
2
3
4
5
6
7
16–18
mg
/dL
Ave
rage
LD
L-C
val
ue
, me
an, m
mo
l/L
Alirocumab 150 mg Q2W (n=41) Placebo (n=21)
4.3/166.0 4.5/174.7 4.3/165.0 4.5/172.6 4.5/175.2
2.4/92.1 2.5/98.1 2.4/93.6 2.5/95.2 2.4/94.3
4.5/175.1
5.0/191.6
ODYSSEY ESCAPE_P. Moriarty_EHJ 2016
Ipercolesterolemia in pazienti a rischio CV molto alto (non controllati con dosi massime
tollerate di statine±Eze)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
Inibitori di PCSK9 utilizzati in
ASSOCIAZIONE a dose massima
tollerata di statina (± altre LLT)
Pazienti con
Ipercolesterolemia
Familiare (i.e HeFH)
I monoclonali Anti-PCSK9 nei pazienti ad alto rischio CV: UNMET NEEDS
Farmaci Biologici: Inibitori di PCSK9
Evolocumab, Alirocumab, Bococizumab
79% with HeFH not at goal
(<100 mg/dL [2.6 mmol/L])
20% at high risk not at goal (<100 mg/dL [2.6 mol/L])
59% at very high CV risk not at goal (<70 mg/dL [1.8 mmol/L])
Inibitori di PCSK9 in
MONOTERAPIA
(o Associazione con altre LLT)
Pazienti con
Intolleranza a Statine
Nearly all patients who need
considerable LDL-C reductions
will not reach goal
P ijlman et al. Atherosclerosis 2010;209:189-94; Jones PH, et al. J Am Heart Assoc. 2012;1:e001800
• STATO ATTUALE: Diagnosi difficile perché non vi è consenso unanime e la segnalazione di mialgia è soggettiva e influenzata da comorbidità
• UPDATE OPERATIVO: valutare presenza di SI utilizzando: 1. sintomi 2. livelli di CK 3. Drug re-challenge (≥2 statine)
• SCOPO: Massimizzare la probabilità di identificare pazienti con reale SI attraverso combinazione di symptom score (standardizzato), livelli di CK e risposta a “repetitive statin rechallenge»
Efficacy and safety of alirocumab versus ezetimibe,
in patients with statin intolerance defined by
placebo run-in and statin rechallenge arm
Patrick M. Moriarty1, Paul D. Thompson2, Christopher P. Cannon3, John R. Guyton4, Jean Bergeron5, Franklin J. Zieve6, Eric Bruckert7, Terry A. Jacobson8, Marie T. Baccara-Dinet9, Jian Zhao10, Yunling Du10,
Robert Pordy11, Daniel Gipe11
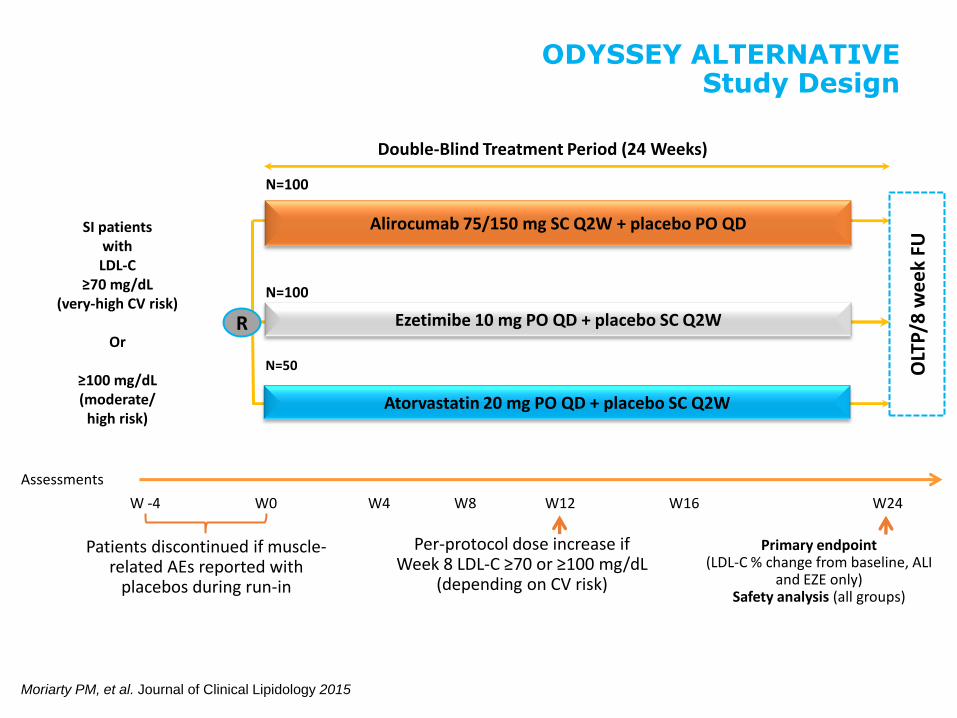
Double-Blind Treatment Period (24 Weeks)
Alirocumab 75/150 mg SC Q2W + placebo PO QD
N=100
Ezetimibe 10 mg PO QD + placebo SC Q2W
N=100
W8 W16
Primary endpoint (LDL-C % change from baseline, ALI
and EZE only) Safety analysis (all groups)
W4 W12 W24
Per-protocol dose increase if Week 8 LDL-C ≥70 or ≥100 mg/dL
(depending on CV risk)
ODYSSEY ALTERNATIVE Study Design
SI patients with LDL-C
≥70 mg/dL (very-high CV risk)
Or
≥100 mg/dL (moderate/
high risk)
Assessments
W0 W -4
Patients discontinued if muscle-related AEs reported with
placebos during run-in
Atorvastatin 20 mg PO QD + placebo SC Q2W
N=50 OLT
P/8
we
ek
FU
Moriarty PM, et al. Journal of Clinical Lipidology 2015
R
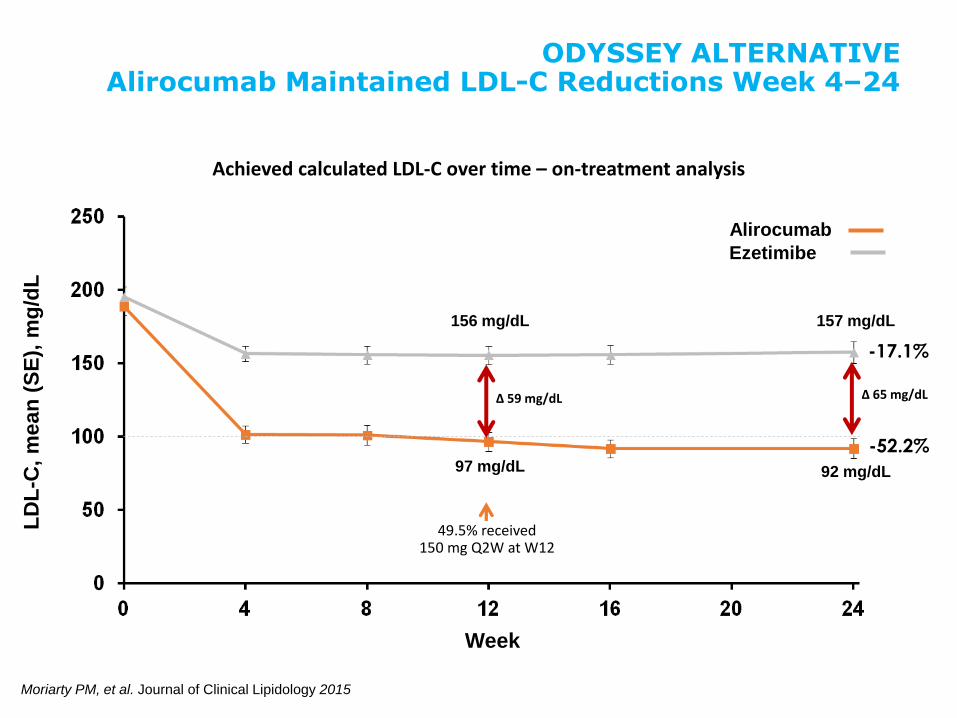
ODYSSEY ALTERNATIVE Alirocumab Maintained LDL-C Reductions Week 4–24
Week
156 mg/dL
97 mg/dL
157 mg/dL
92 mg/dL
Ezetimibe
Alirocumab
LD
L-C
, m
ea
n (
SE
), m
g/d
L
Achieved calculated LDL-C over time – on-treatment analysis
49.5% received 150 mg Q2W at W12
Δ 59 mg/dL Δ 65 mg/dL
Moriarty PM, et al. Journal of Clinical Lipidology 2015
-52.2%
-17.1%
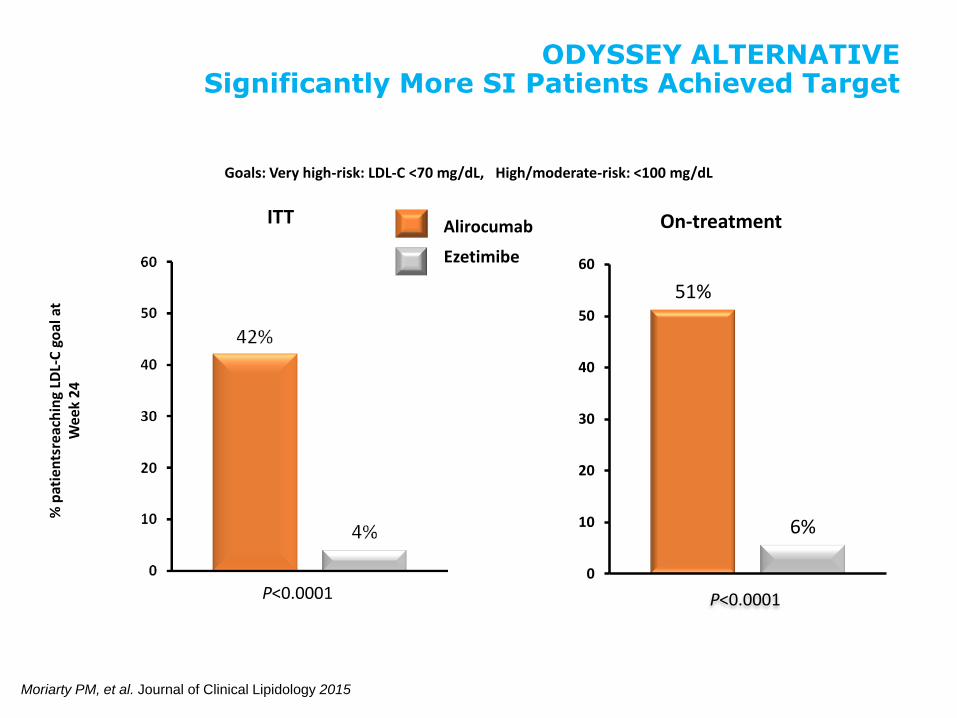
Goals: Very high-risk: LDL-C <70 mg/dL, High/moderate-risk: <100 mg/dL
P<0.0001
% p
atie
nts
reac
hin
g LD
L-C
go
al a
t W
eek
24
Ezetimibe
Alirocumab
51%
6%
0
10
20
30
40
50
60
P<0.0001
ITT On-treatment
ODYSSEY ALTERNATIVE Significantly More SI Patients Achieved Target
Moriarty PM, et al. Journal of Clinical Lipidology 2015
Anticorpo monoclonale Anti PCSK9*: ALIROCUMAB
• Alirocumab: cos è e come agisce
• Efficacia su LDL-C (in associazione a statine)
• Quando impiegarlo (popolazioni Target)
• Potenziali benefici su eventi CV
*Proprotein Convertase Subtilisin/kexin Type 9 (PCSK9)
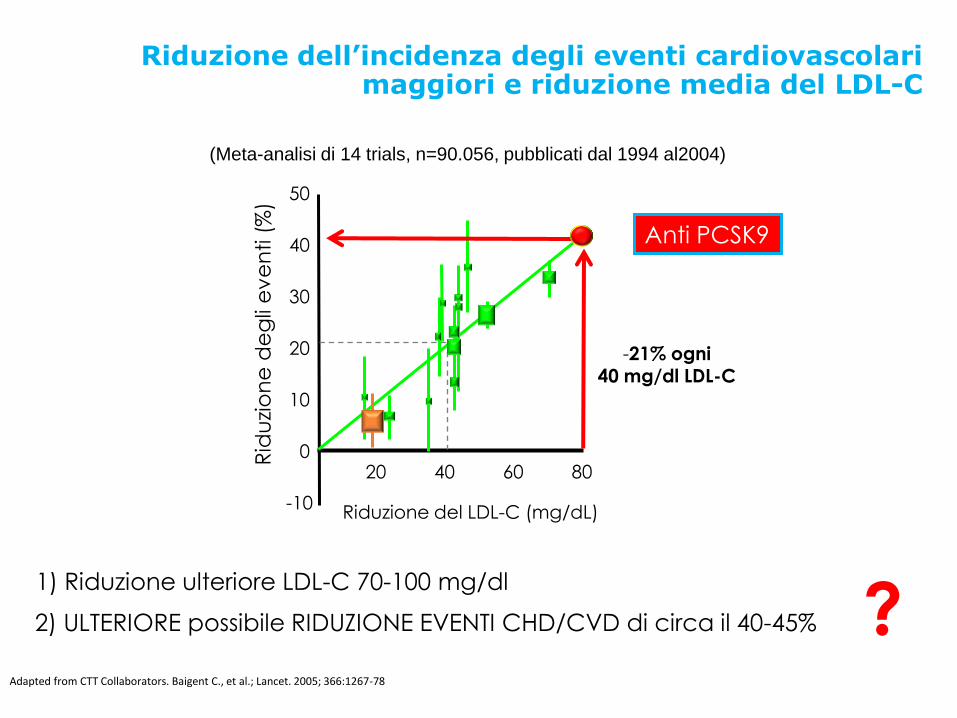
Riduzione dell’incidenza degli eventi cardiovascolari maggiori e riduzione media del LDL-C
Adapted from CTT Collaborators. Baigent C., et al.; Lancet. 2005; 366:1267-78
1) Riduzione ulteriore LDL-C 70-100 mg/dl
-10
0
40
50
30
20
10
20 40 60 80
Riduzione del LDL-C (mg/dL)
Rid
uzi
on
e d
eg
li e
ve
nti (
%)
-21% ogni 40 mg/dl LDL-C
?
Anti PCSK9
(Meta-analisi di 14 trials, n=90.056, pubblicati dal 1994 al2004)
2) ULTERIORE possibile RIDUZIONE EVENTI CHD/CVD di circa il 40-45%
Robinson JG et al. NEJM 2015; 372:1489-99.
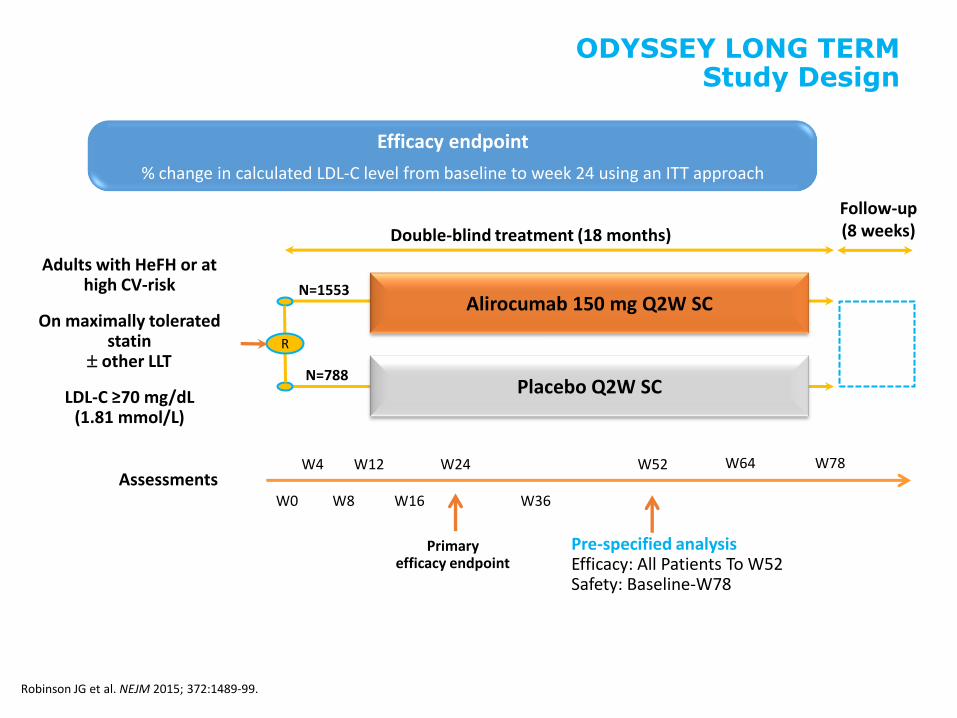
Adults with HeFH or at high CV-risk
On maximally tolerated statin
other LLT
LDL-C ≥70 mg/dL (1.81 mmol/L)
Double-blind treatment (18 months)
N=1553
N=788
R
Follow-up (8 weeks)
Alirocumab 150 mg Q2W SC
Placebo Q2W SC
Assessments W0
W4
W8
W12
W16
W24
W36
W52
Primary efficacy endpoint
W64 W78
Robinson JG et al. NEJM 2015; 372:1489-99.
ODYSSEY LONG TERM Study Design
Pre-specified analysis Efficacy: All Patients To W52 Safety: Baseline-W78
Efficacy endpoint
% change in calculated LDL-C level from baseline to week 24 using an ITT approach
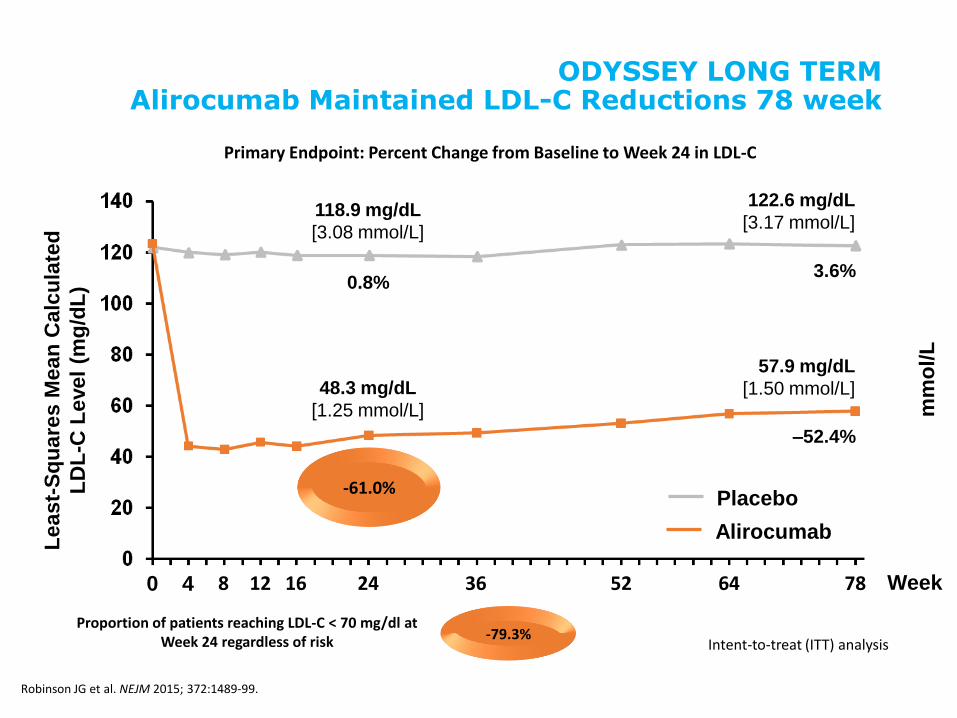
ODYSSEY LONG TERM Alirocumab Maintained LDL-C Reductions 78 week
Placebo
Alirocumab
Least-
Sq
uare
s M
ean
Calc
ula
ted
LD
L-C
Level
(mg
/dL
)
118.9 mg/dL
[3.08 mmol/L]
48.3 mg/dL
[1.25 mmol/L]
122.6 mg/dL
[3.17 mmol/L]
57.9 mg/dL
[1.50 mmol/L]
0.8% 3.6%
–52.4%
mm
ol/L
Week 0 4 8 12 16 24 36 52 64 78
Robinson JG et al. NEJM 2015; 372:1489-99.
Primary Endpoint: Percent Change from Baseline to Week 24 in LDL-C
Intent-to-treat (ITT) analysis
-61.0%
Proportion of patients reaching LDL-C < 70 mg/dl at Week 24 regardless of risk -79.3%
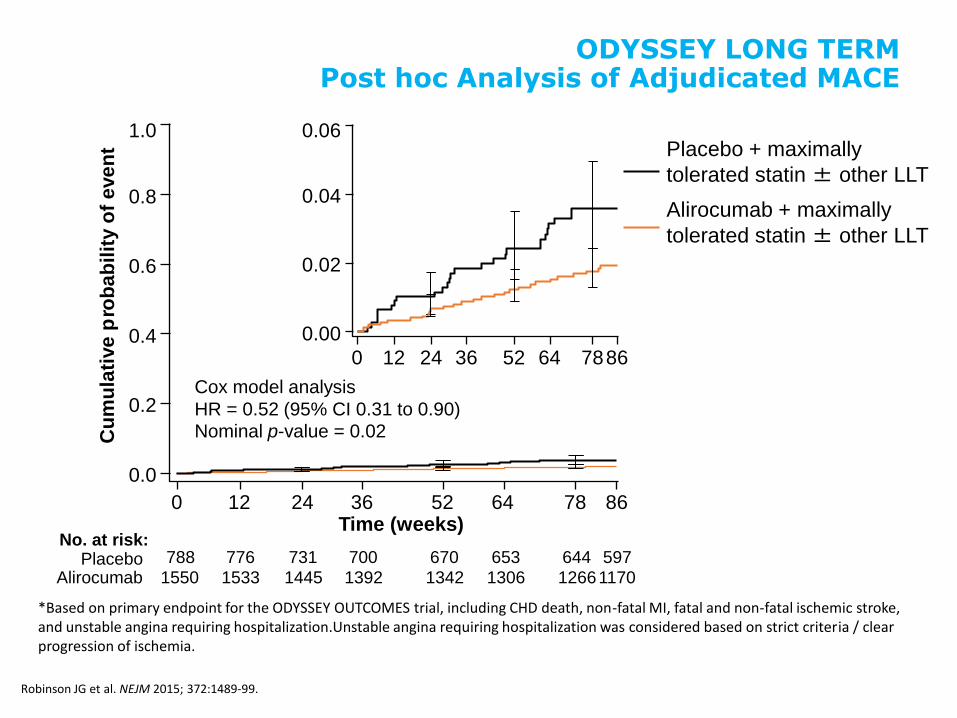
*Based on primary endpoint for the ODYSSEY OUTCOMES trial, including CHD death, non-fatal MI, fatal and non-fatal ischemic stroke, and unstable angina requiring hospitalization.Unstable angina requiring hospitalization was considered based on strict criteria / clear progression of ischemia.
Placebo + maximally
tolerated statin ± other LLT
Alirocumab + maximally
tolerated statin ± other LLT
Cu
mu
lati
ve
p r o
ba
bil
ity o
f e
ve
nt
Time (weeks)
Cox model analysis
HR = 0.52 (95% CI 0.31 to 0.90)
Nominal p-value = 0.02
No. at risk: Placebo
Alirocumab
788 776 731 700 670 653 644 597
1550 1533 1445 1392 1342 1306 1266 1170
1.0
0.8
0.6
0.4
0.2
0.0
0 12 24 36 52 64 78 86
0.06
0.04
0.02
0.00
0 12 24 36 52 64 78 86
ODYSSEY LONG TERM Post hoc Analysis of Adjudicated MACE
Robinson JG et al. NEJM 2015; 372:1489-99.
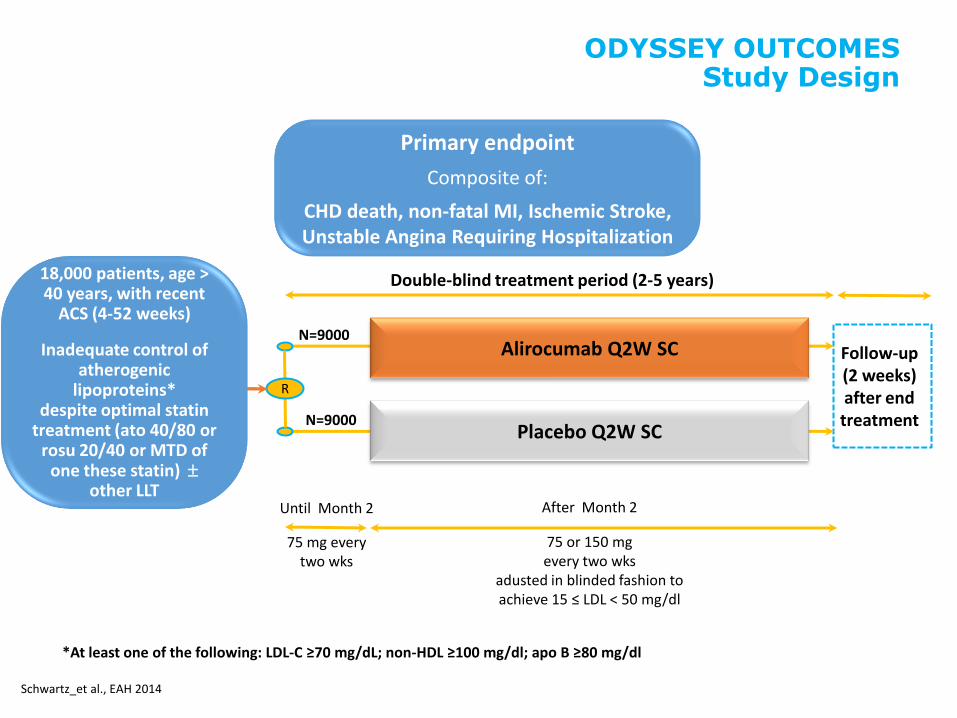
Double-blind treatment period (2-5 years)
N=9000
N=9000
R
Follow-up (2 weeks) after end treatment
Alirocumab Q2W SC
Placebo Q2W SC
Until Month 2
ODYSSEY OUTCOMES Study Design
Primary endpoint
Composite of:
CHD death, non-fatal MI, Ischemic Stroke, Unstable Angina Requiring Hospitalization
Schwartz_et al., EAH 2014
*At least one of the following: LDL-C ≥70 mg/dL; non-HDL ≥100 mg/dl; apo B ≥80 mg/dl
75 mg every two wks
After Month 2
75 or 150 mg every two wks
adusted in blinded fashion to achieve 15 ≤ LDL < 50 mg/dl
18,000 patients, age > 40 years, with recent
ACS (4-52 weeks)
Inadequate control of atherogenic
lipoproteins* despite optimal statin
treatment (ato 40/80 or rosu 20/40 or MTD of
one these statin) other LLT
Alirocumab Pooled Safety Overall
EAS 2015
M. Farnier, D. Gaudet, V. Valcheva, P. Minimi, K. Miller, B. Cariou
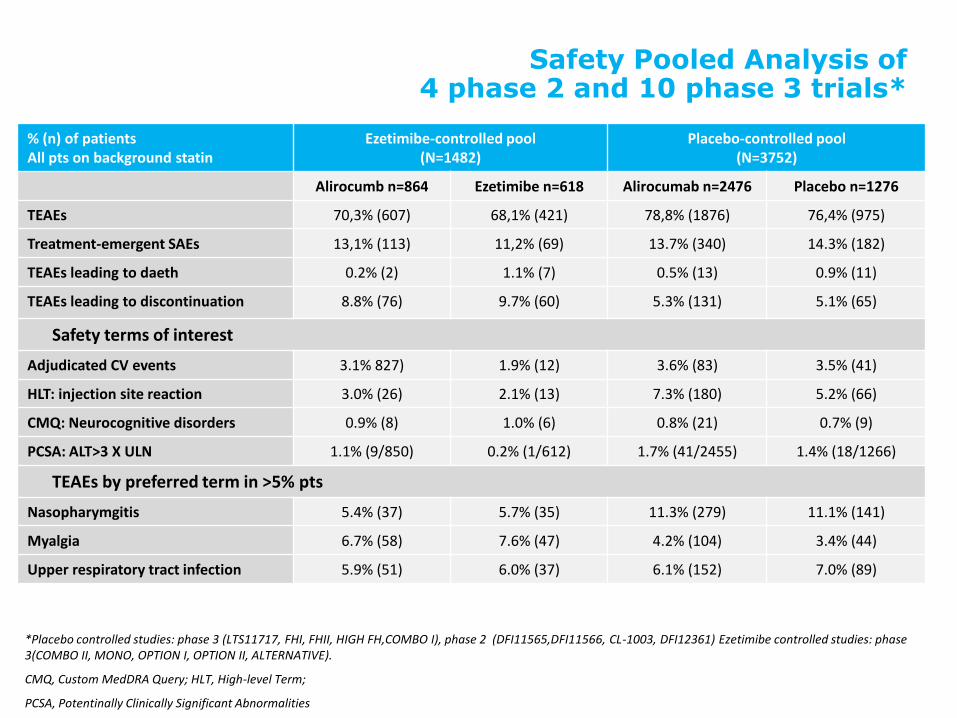
Safety Pooled Analysis of 4 phase 2 and 10 phase 3 trials*
% (n) of patients All pts on background statin
Ezetimibe-controlled pool
(N=1482) Placebo-controlled pool
(N=3752)
Alirocumb n=864 Ezetimibe n=618 Alirocumab n=2476 Placebo n=1276
TEAEs 70,3% (607) 68,1% (421) 78,8% (1876) 76,4% (975)
Treatment-emergent SAEs 13,1% (113) 11,2% (69) 13.7% (340) 14.3% (182)
TEAEs leading to daeth 0.2% (2) 1.1% (7) 0.5% (13) 0.9% (11)
TEAEs leading to discontinuation 8.8% (76) 9.7% (60) 5.3% (131) 5.1% (65)
Safety terms of interest
Adjudicated CV events 3.1% 827) 1.9% (12) 3.6% (83) 3.5% (41)
HLT: injection site reaction 3.0% (26) 2.1% (13) 7.3% (180) 5.2% (66)
CMQ: Neurocognitive disorders 0.9% (8) 1.0% (6) 0.8% (21) 0.7% (9)
PCSA: ALT>3 X ULN 1.1% (9/850) 0.2% (1/612) 1.7% (41/2455) 1.4% (18/1266)
TEAEs by preferred term in >5% pts
Nasopharymgitis 5.4% (37) 5.7% (35) 11.3% (279) 11.1% (141)
Myalgia 6.7% (58) 7.6% (47) 4.2% (104) 3.4% (44)
Upper respiratory tract infection 5.9% (51) 6.0% (37) 6.1% (152) 7.0% (89)
*Placebo controlled studies: phase 3 (LTS11717, FHI, FHII, HIGH FH,COMBO I), phase 2 (DFI11565,DFI11566, CL-1003, DFI12361) Ezetimibe controlled studies: phase 3(COMBO II, MONO, OPTION I, OPTION II, ALTERNATIVE).
CMQ, Custom MedDRA Query; HLT, High-level Term;
PCSA, Potentinally Clinically Significant Abnormalities
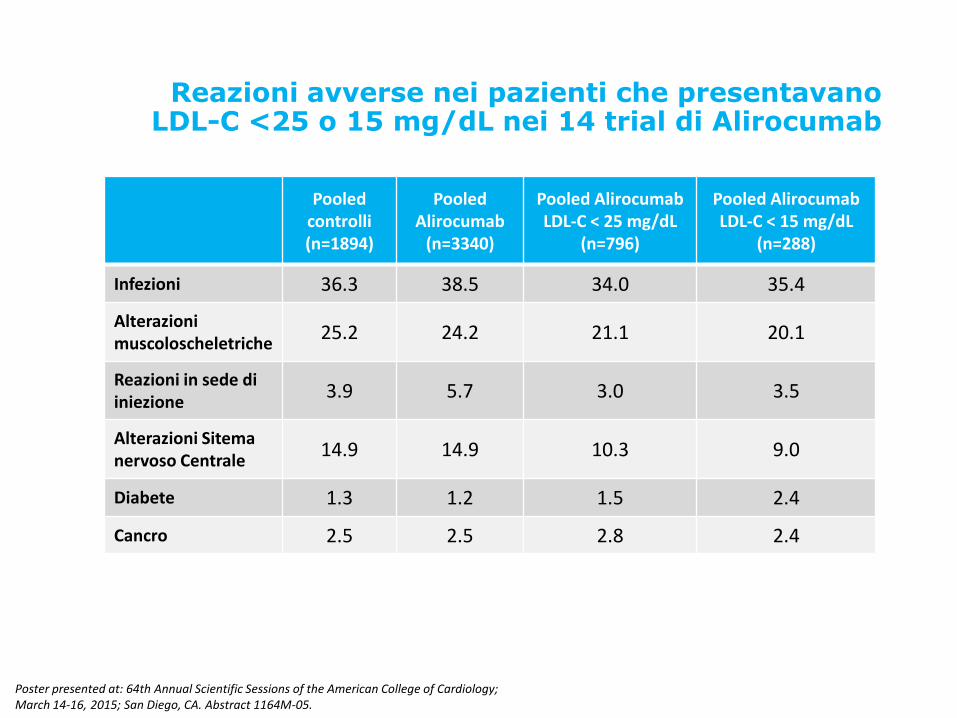
Reazioni avverse nei pazienti che presentavano LDL-C <25 o 15 mg/dL nei 14 trial di Alirocumab
TEAE : Treatment Emergent Adverse Event
Pooled controlli (n=1894)
Pooled Alirocumab
(n=3340)
Pooled Alirocumab LDL-C < 25 mg/dL
(n=796)
Pooled Alirocumab LDL-C < 15 mg/dL
(n=288)
Infezioni 36.3 38.5 34.0 35.4
Alterazioni muscoloscheletriche
25.2 24.2 21.1 20.1
Reazioni in sede di iniezione
3.9 5.7 3.0 3.5
Alterazioni Sitema nervoso Centrale
14.9 14.9 10.3 9.0
Diabete 1.3 1.2 1.5 2.4
Cancro 2.5 2.5 2.8 2.4
Poster presented at: 64th Annual Scientific Sessions of the American College of Cardiology; March 14-16, 2015; San Diego, CA. Abstract 1164M-05.
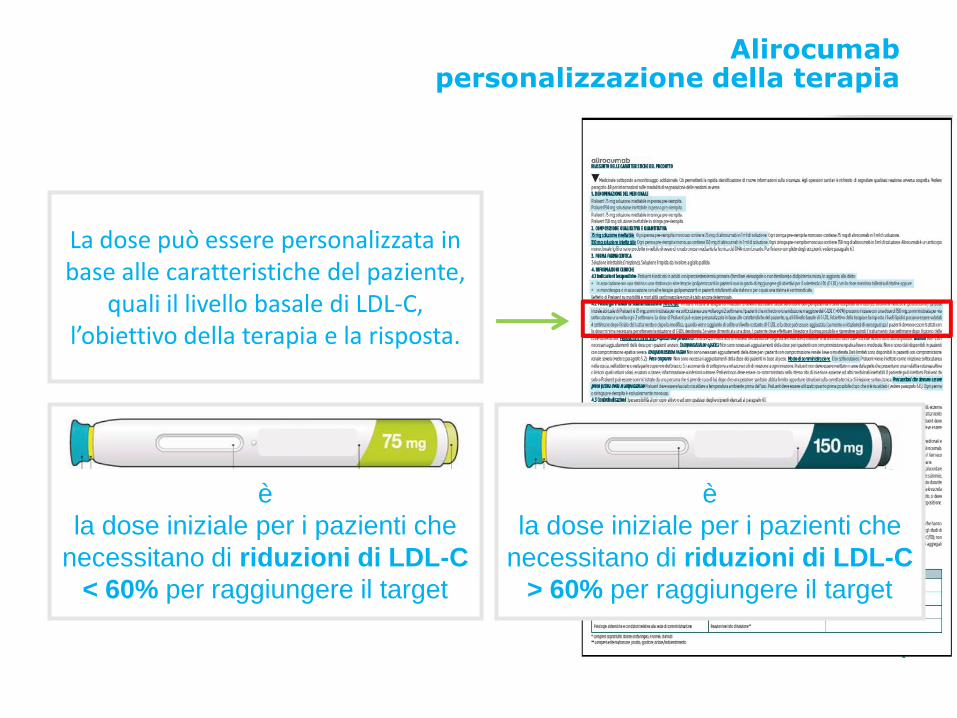
Alirocumab personalizzazione della terapia
La dose può essere personalizzata in base alle caratteristiche del paziente,
quali il livello basale di LDL-C, l’obiettivo della terapia e la risposta.
PRALUENT 75 mg è
la dose iniziale per i pazienti che
necessitano di riduzioni di LDL-C
< 60% per raggiungere il target
PRALUENT 150 mg è
la dose iniziale per i pazienti che
necessitano di riduzioni di LDL-C
> 60% per raggiungere il target
Alirocumab Final clinical considerations
Sarah L. Greig Am J Cardiovasc Drugs: DOI 10.1007/s40256-016-0166-3
• Fully human monoclonal antibody against PCSK9
• Administered as a subcutaneous injection of 75 or 150 mg once every 2
weeks
• Significantly reduces LDL-C levels in patients with heFH or nonFH
(including those with statin intolerance), whether used as monotherapy
or added to statin or non-statin LLT
• Has favorable effects on other lipid parameters,including non-HDL-C
and Lp(a)
• Efficacy maintained in the longer-term
• Generally well tolerated