La termorizotomia trigeminale percutanea: note tecniche per una lesione anatomicamente selettiva
Upload
trinhtuyenCategory
view
219download
0
Quando è
realmente utile
la chiusura
percutanea
dell’auricola
sinistra?
Gennaro Santoro , Firenze
Fondazione CNR-Regione Toascana G.Monasterio
per la Ricerca Medica e la Sanità Pubbica

DISCLOSURE INFORMATION
negli ultimi due anni non ho avuto rapporti di finanziamento con soggetti portatori di interessi commerciali in campo sanitario
NESSUN CONFLITTO DI INTERESSE
Gennaro Santoro
Firenze
Profilassi dello stroke cardioembolico in
FA
Le opzioni terapeutiche
Terapia farmacologica
Terapia meccanica percutanea
Terapia meccanica chirurgica
(non valvolare)
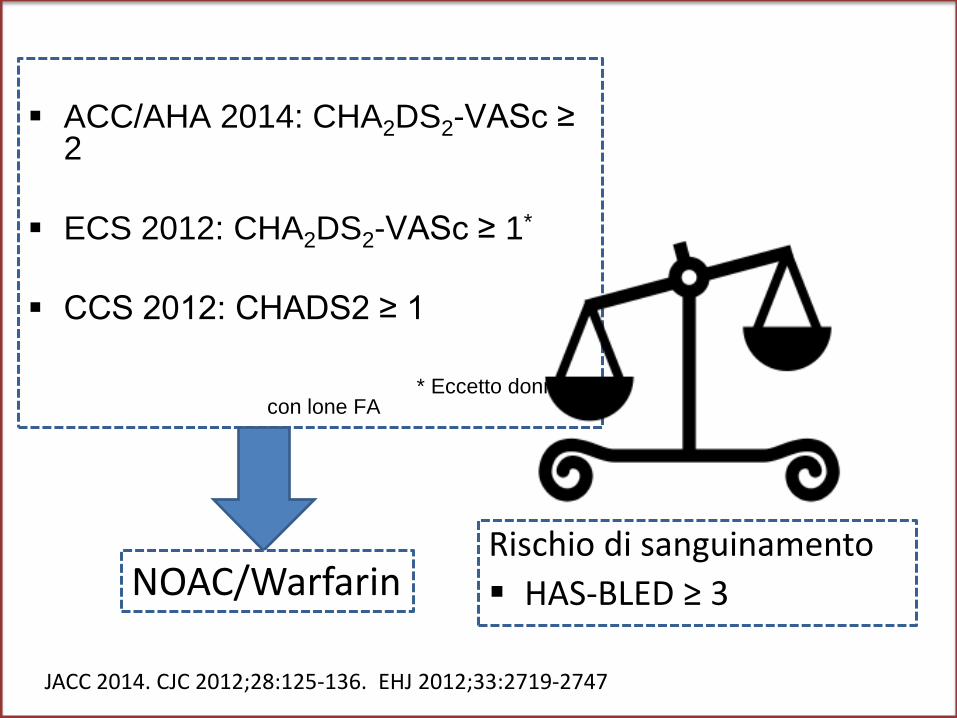
ACC/AHA 2014: CHA2DS2-VASc ≥ 2
ECS 2012: CHA2DS2-VASc ≥ 1*
CCS 2012: CHADS2 ≥ 1
* Eccetto donne con lone FA
JACC 2014. CJC 2012;28:125-136. EHJ 2012;33:2719-2747
Rischio di sanguinamento
HAS-BLED ≥ 3 NOAC/Warfarin
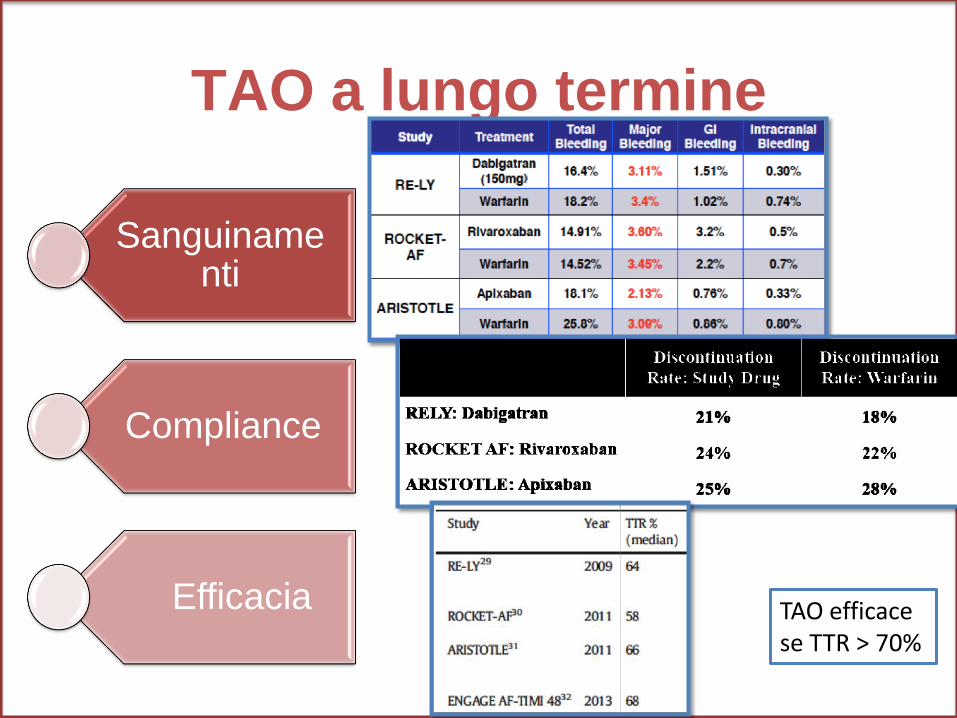
TAO a lungo termine
Sanguinamenti
Compliance
Efficacia TAO efficace se TTR > 70%
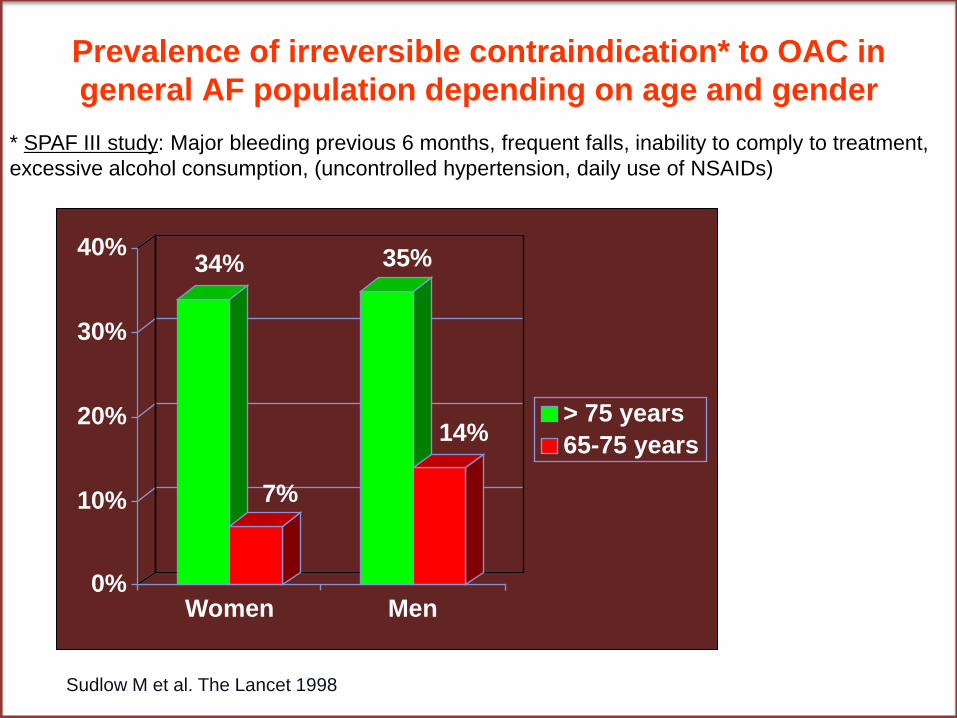
Prevalence of irreversible contraindication* to OAC in
general AF population depending on age and gender
* SPAF III study: Major bleeding previous 6 months, frequent falls, inability to comply to treatment,
excessive alcohol consumption, (uncontrolled hypertension, daily use of NSAIDs)
34%
7%
35%
14%
0%
10%
20%
30%
40%
Women Men
> 75 years
65-75 years
Sudlow M et al. The Lancet 1998
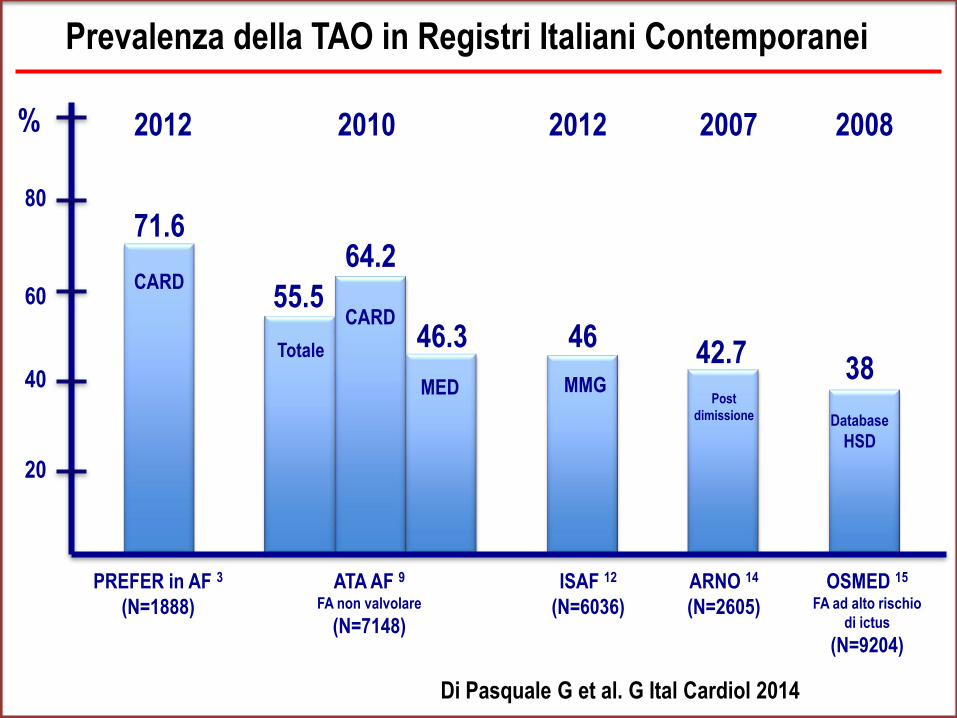
55.5
% 2012 2010 2012 2007 2008
71.6 64.2
46.3 46 42.7
38
Prevalenza della TAO in Registri Italiani Contemporanei
CARD
CARD
Totale
MED MMG Post
dimissione Database
HSD
PREFER in AF 3
(N=1888)
ATA AF 9
FA non valvolare
(N=7148)
ISAF 12
(N=6036)
ARNO 14
(N=2605)
OSMED 15
FA ad alto rischio
di ictus
(N=9204)
20
40
60
80
Di Pasquale G et al. G Ital Cardiol 2014
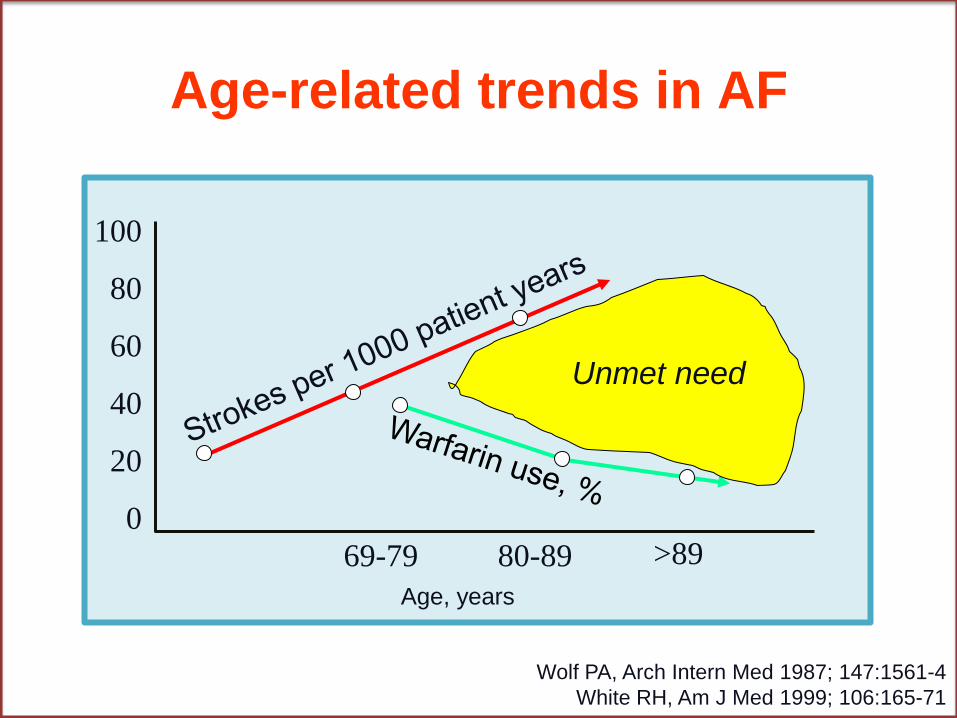
Age-related trends in AF
Age, years
69-79 80-89 >89
100
80
60
40
20
0
Unmet need
Wolf PA, Arch Intern Med 1987; 147:1561-4
White RH, Am J Med 1999; 106:165-71
Profilassi dello stroke cardioembolico in
FA
Le opzioni terapeutiche
Terapia farmacologica
Terapia meccanica percutanea
Terapia meccanica chirurgica
(non valvolare)
PERCHÉ CHIUDERE L’AURICOLA SINISTRA?
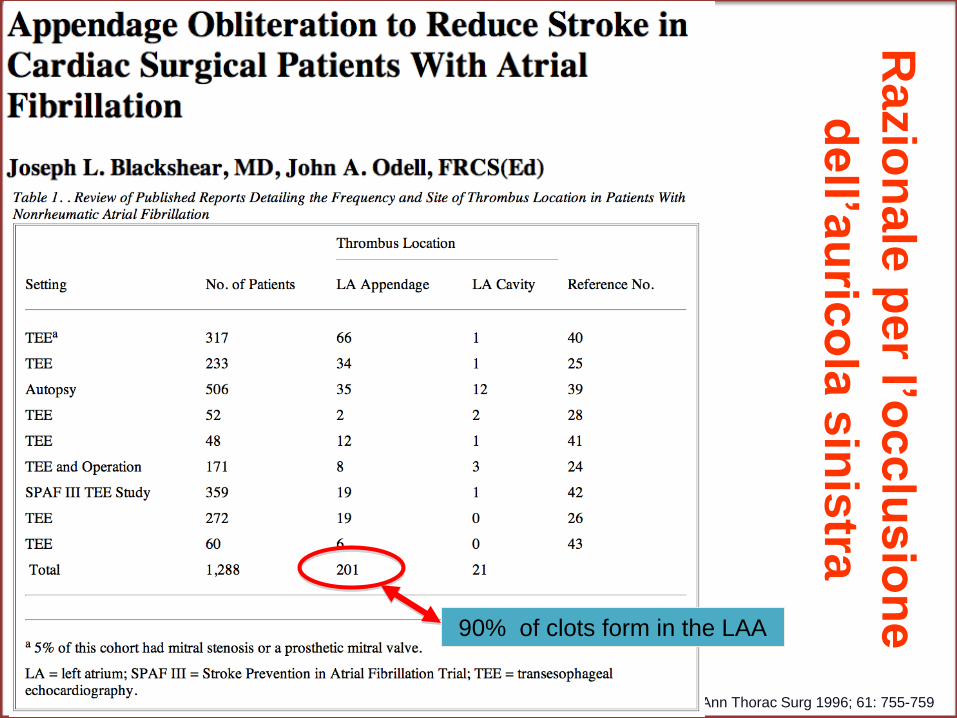
Ra
zio
na
le p
er l’o
cc
lus
ion
e
dell’a
uric
ola
sin
istra
Ann Thorac Surg 1996; 61: 755-759
90% of clots form in the LAA
COME CHIUDERE L’AURICOLA SINISTRA?
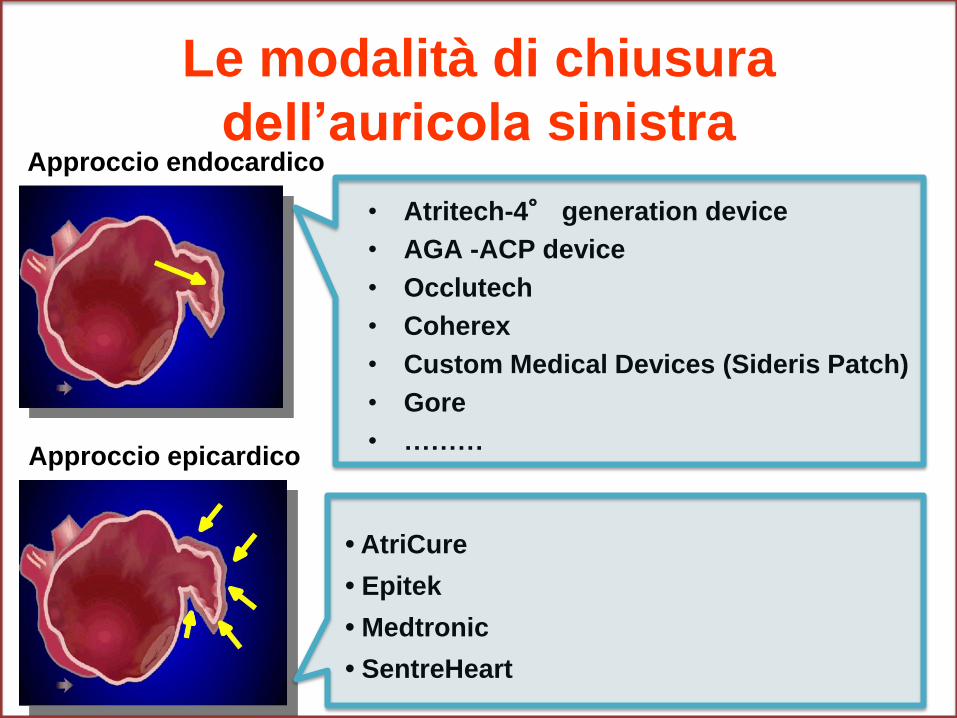
Le modalità di chiusura
dell’auricola sinistra
• Atritech-4° generation device
• AGA -ACP device
• Occlutech
• Coherex
• Custom Medical Devices (Sideris Patch)
• Gore
• ………
Approccio endocardico
Approccio epicardico
• AtriCure
• Epitek
• Medtronic
• SentreHeart
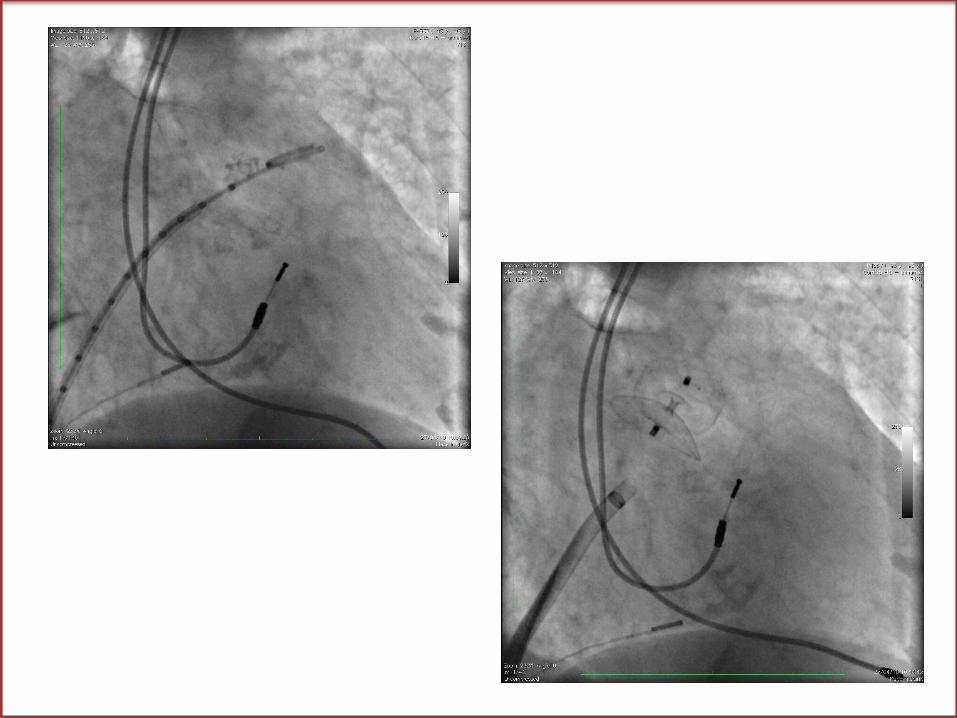

Monitoraggio della Procedura
Posizione del device
Concovità lieve del disco
Spazio fra disco e lobo
Lieve tenting posteriore del lobo
Assenza di flusso in auuricola sinistra
RISULTATI CLINICI DELLA CHIUSURA PERCUTANEA
Studi osservazionali
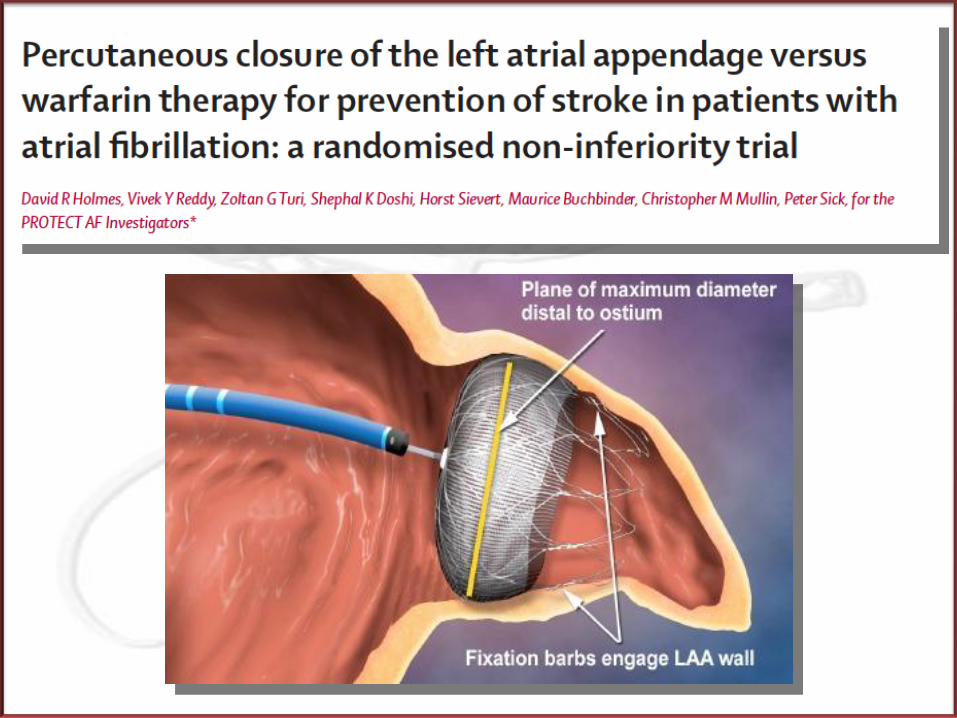
PROTECT AF Clinical Trial Design
Prospective, randomized study of WATCHMAN LAA Device vs. Long-term Warfarin Therapy
2:1 allocation ratio device to control Non-inferiority comparison 800 Patients enrolled from Feb 2005 to Jun 2008-707
randomized 59 Enrolling Centers (U.S. & Europe) Follow-up Requirements
TEE follow-up at 45 days, 6 months and 1 year Clinical follow-up biannually up to 5 years Regular INR monitoring while taking warfarin
Enrollment continues in Continued Access Registry
Primary Efficacy Endpoint All stroke: ischemic or hemorrhagic
• deficit with symptoms persisting more than 24 hours or • symptoms less than 24 hours confirmed by CT or MRI
Cardiovascular and unexplained death: includes sudden death, MI, CVA, cardiac arrhythmia and heart failure
Systemic embolization
Primary Safety Endpoint Device embolization requiring retrieval Pericardial effusion requiring intervention Cranial bleeds and gastrointestinal bleeds Any bleed that requires ≥ 2uPRBC
NB: Primary effectiveness endpoint contains safety events
PROTECT AF Trial Endpoints
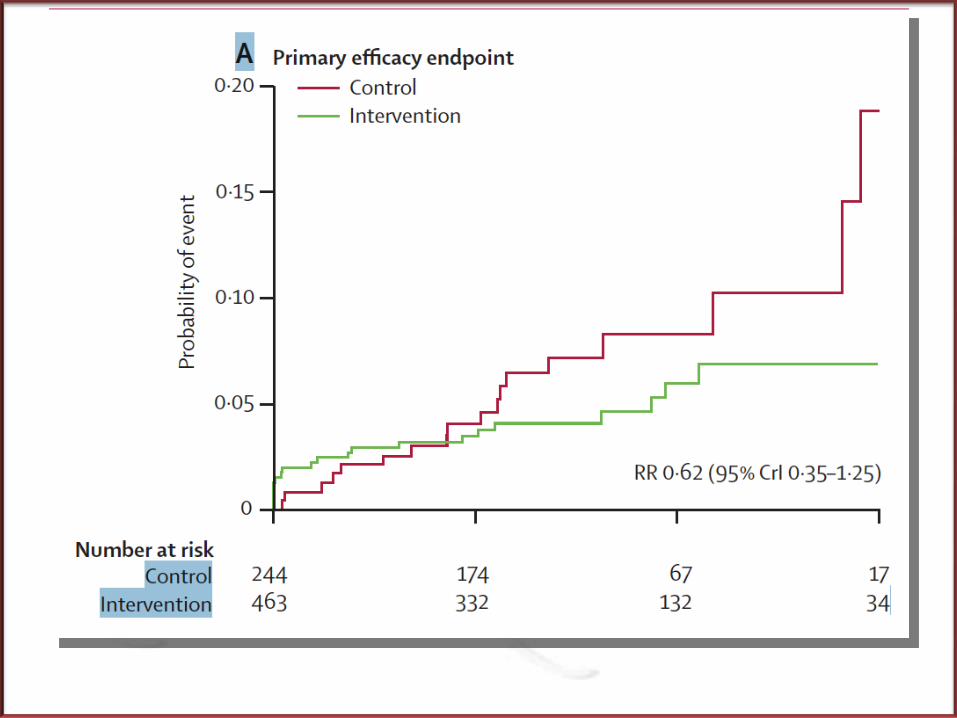
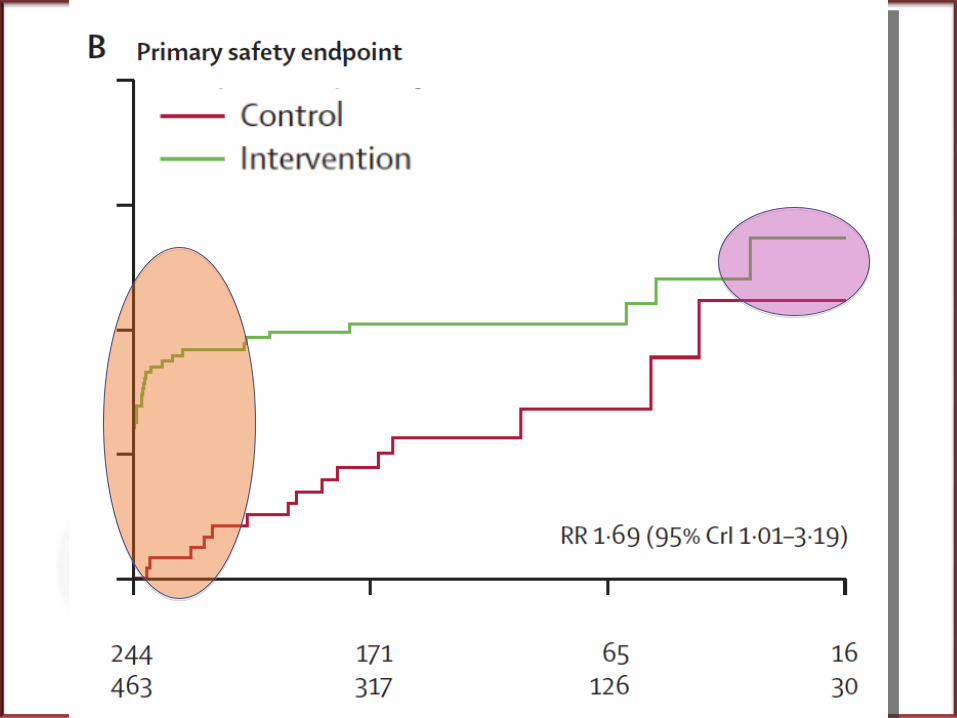
Lancet 2009
0,7
0,8
0,9
1,0
0 365 730 1095
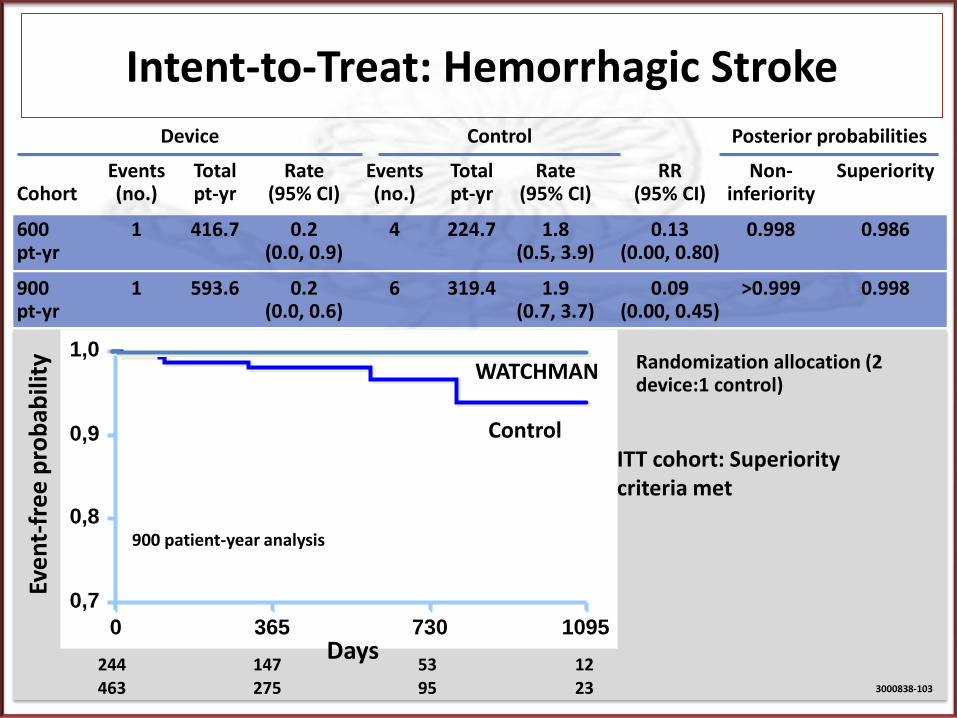
Intent-to-Treat: Hemorrhagic Stroke
ITT cohort: Superiority criteria met
Eve
nt-
fre
e p
rob
abili
ty
Days 244 147 53 12
463 275 95 23
WATCHMAN
Control
3000838-103
900 patient-year analysis
Events Total Rate Events Total Rate RR Non- Superiority Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority
600 1 416.7 0.2 4 224.7 1.8 0.13 0.998 0.986 pt-yr (0.0, 0.9) (0.5, 3.9) (0.00, 0.80)
900 1 593.6 0.2 6 319.4 1.9 0.09 >0.999 0.998 pt-yr (0.0, 0.6) (0.7, 3.7) (0.00, 0.45)
Device Control Posterior probabilities
Randomization allocation (2 device:1 control)
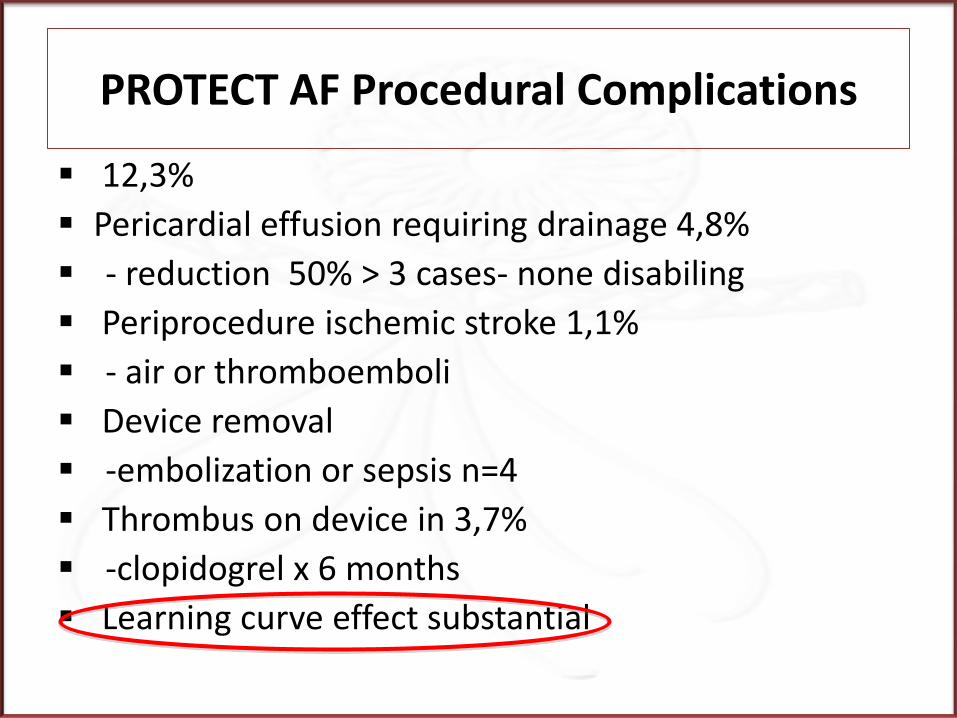
12,3%
Pericardial effusion requiring drainage 4,8%
- reduction 50% > 3 cases- none disabiling
Periprocedure ischemic stroke 1,1%
- air or thromboemboli
Device removal
-embolization or sepsis n=4
Thrombus on device in 3,7%
-clopidogrel x 6 months
Learning curve effect substantial
PROTECT AF Procedural Complications
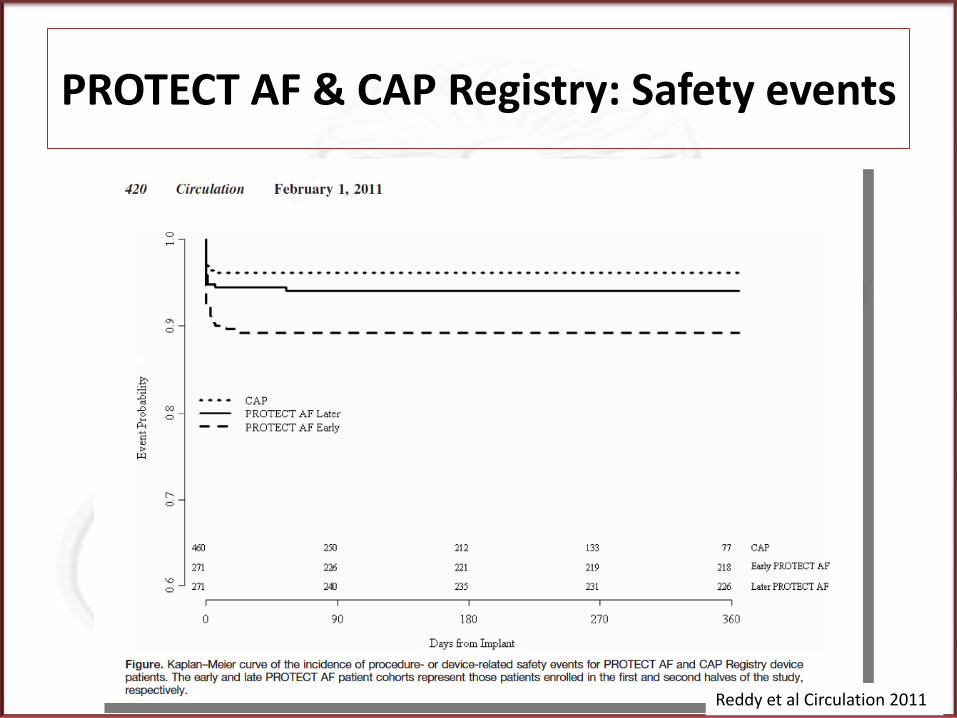
Reddy et al Circulation 2011
PROTECT AF & CAP Registry: Safety events
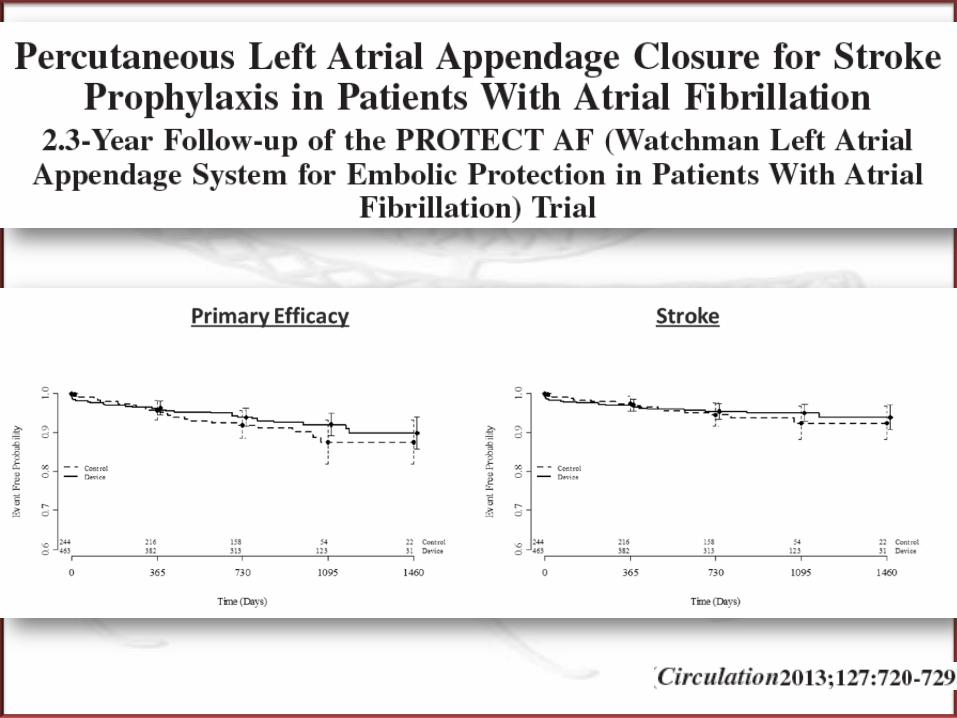
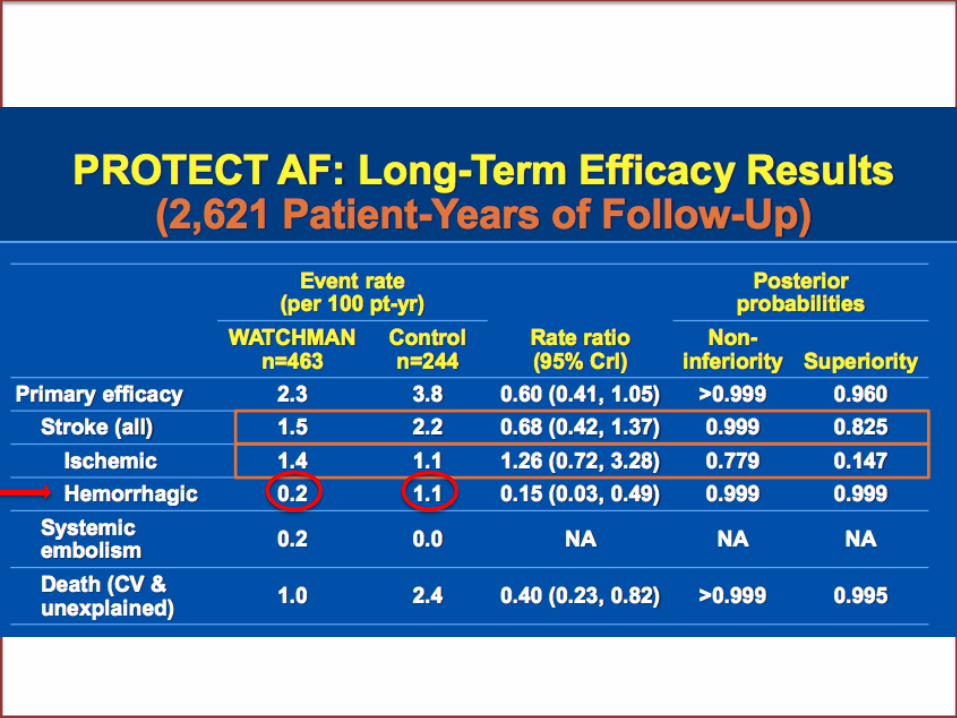
PROTECT-AF follow up
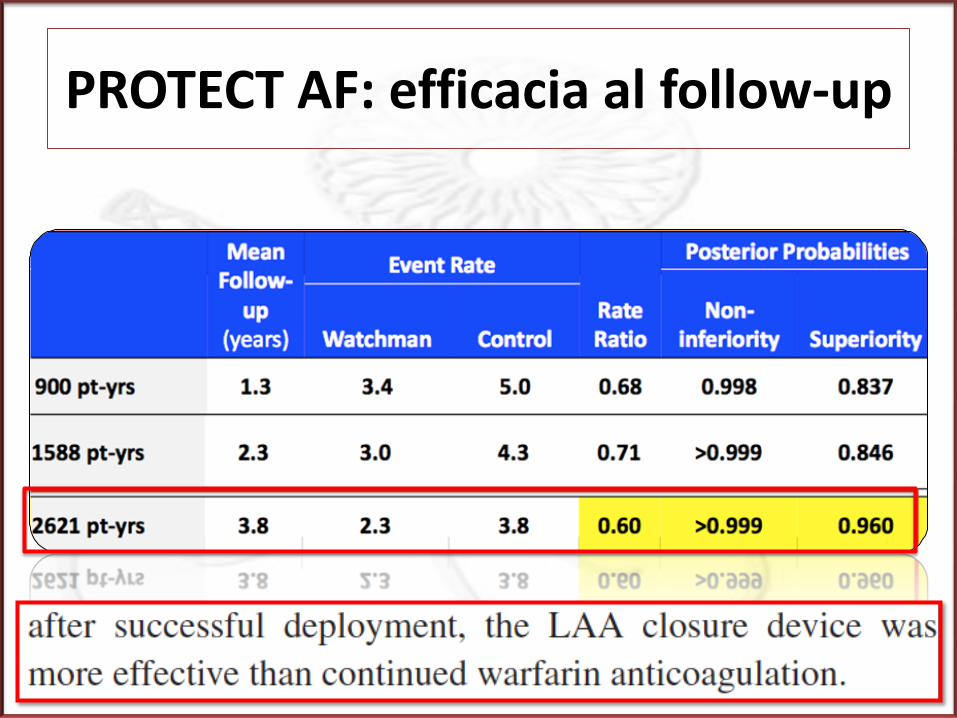
PROTECT AF: efficacia al follow-up
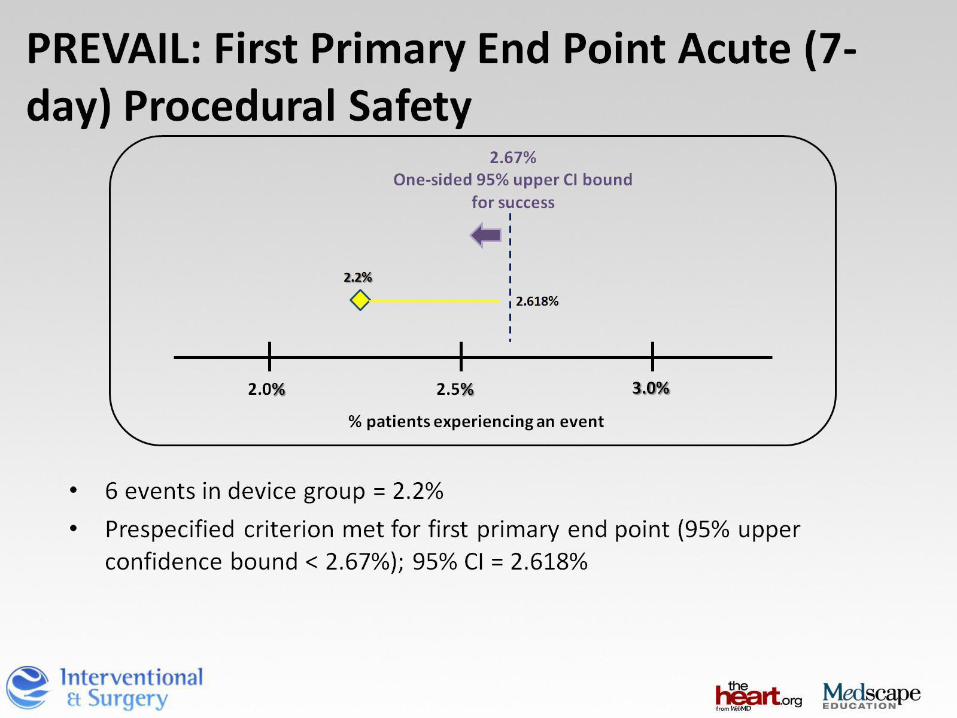
WATCHMAN – PREVAIL
Primary Efficacy Endpoint All stroke: ischemic or hemorrhagic
deficit with symptoms persisting more than 24 hours or symptoms less than 24 hours confirmed by CT or MRI
Cardiovascular and unexplained death: includes sudden death, MI, CVA, cardiac arrhythmia and heart failure
Systemic embolization
Late ischemic Efficacy Endpoint Ischemic stroke or SE excluding the first 7 days after randomization
Early safety primary endpoint All cause of death Ischemic stroke SE Device/procedure related events
between randomization and within 7 days of the procedure
3 CO-PRIMARY ENDPOINTS
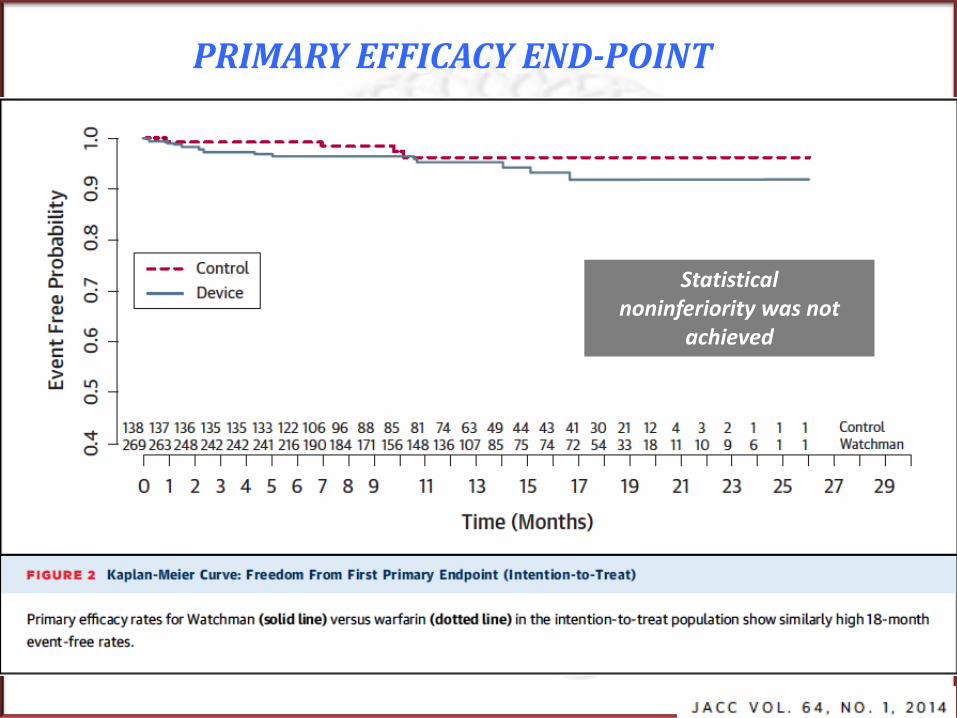
PRIMO END POINT PRIMARY EFFICACY END-POINT
Statistical noninferiority was not
achieved
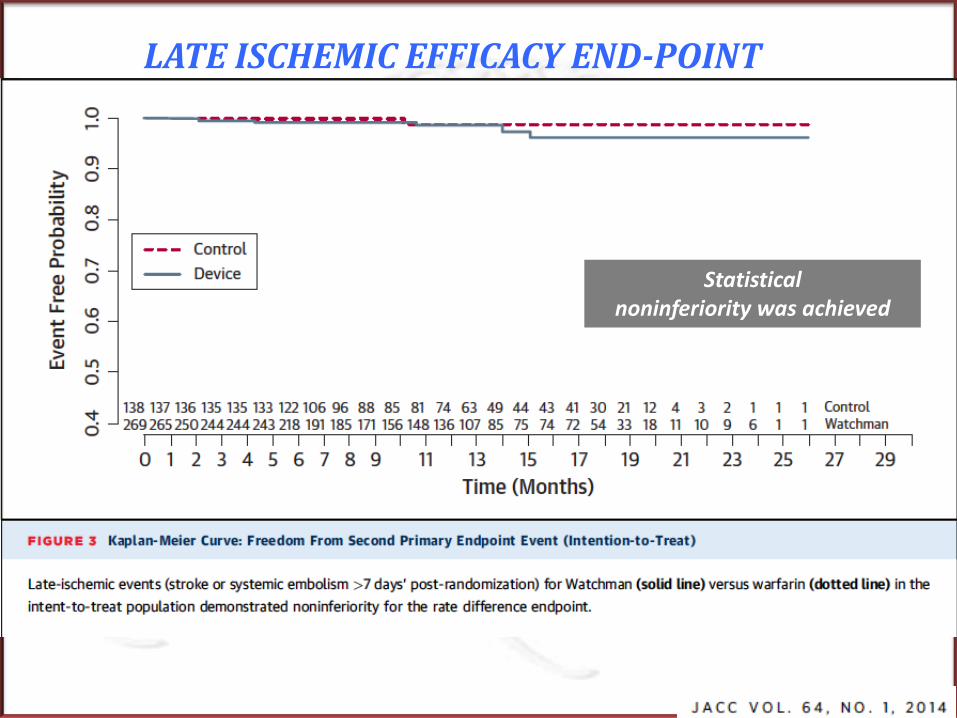
SECONDO END POINT LATE ISCHEMIC EFFICACY END-POINT
Statistical noninferiority was achieved

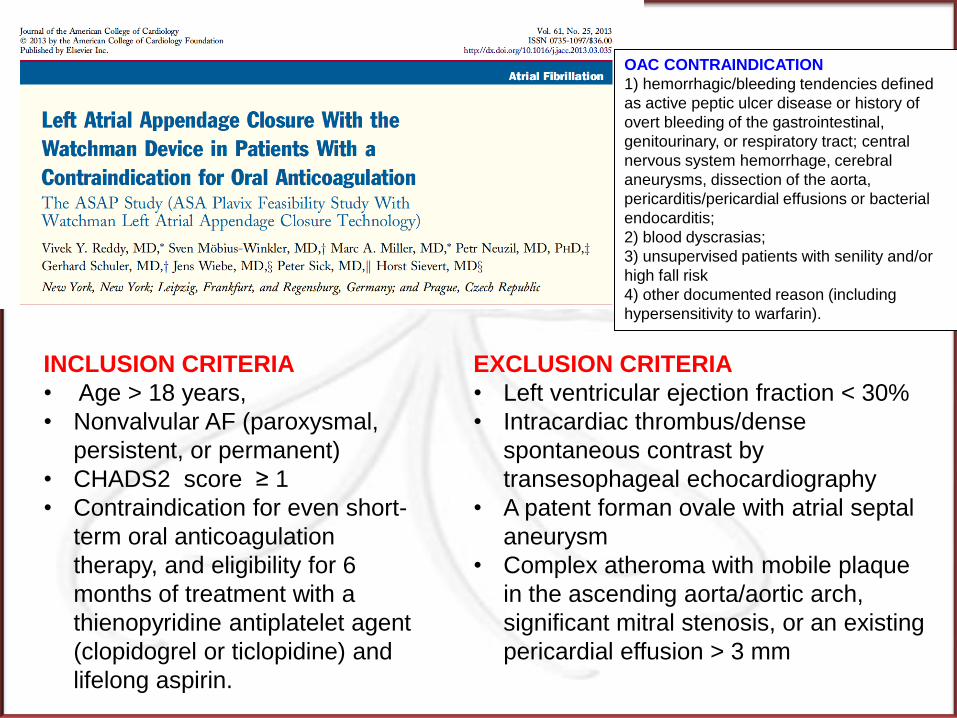
INCLUSION CRITERIA
• Age > 18 years,
• Nonvalvular AF (paroxysmal,
persistent, or permanent)
• CHADS2 score ≥ 1
• Contraindication for even short-
term oral anticoagulation
therapy, and eligibility for 6
months of treatment with a
thienopyridine antiplatelet agent
(clopidogrel or ticlopidine) and
lifelong aspirin.
EXCLUSION CRITERIA
• Left ventricular ejection fraction < 30%
• Intracardiac thrombus/dense
spontaneous contrast by
transesophageal echocardiography
• A patent forman ovale with atrial septal
aneurysm
• Complex atheroma with mobile plaque
in the ascending aorta/aortic arch,
significant mitral stenosis, or an existing
pericardial effusion > 3 mm
OAC CONTRAINDICATION
1) hemorrhagic/bleeding tendencies defined
as active peptic ulcer disease or history of
overt bleeding of the gastrointestinal,
genitourinary, or respiratory tract; central
nervous system hemorrhage, cerebral
aneurysms, dissection of the aorta,
pericarditis/pericardial effusions or bacterial
endocarditis;
2) blood dyscrasias;
3) unsupervised patients with senility and/or
high fall risk
4) other documented reason (including
hypersensitivity to warfarin).
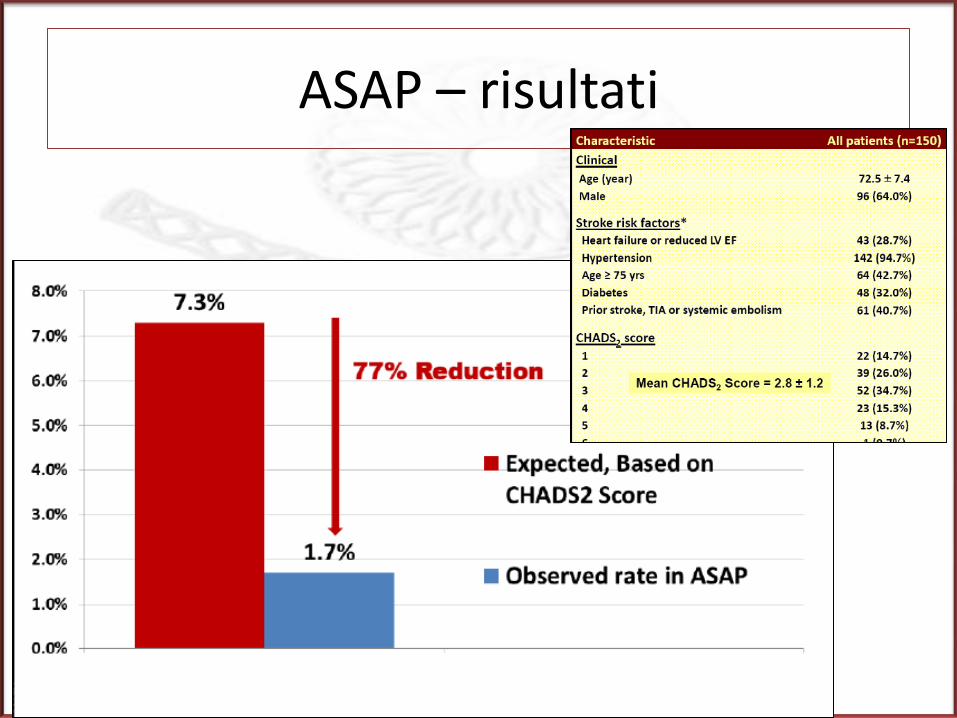
ASAP – risultati

ACP
Risultati con ACP
• Successo procedurale: 97,6%
• Stroke periprocedurale: 0,38%
• Embolizzazione del device: 0,67%
• Versamento pericardico (trattato): 1,25%
• Complicanze periprocedurali: 2,8%
• Stroke al follow-up: 0,62%
Meier B et al, Europace 2014
EuroIntervention 2014, in press
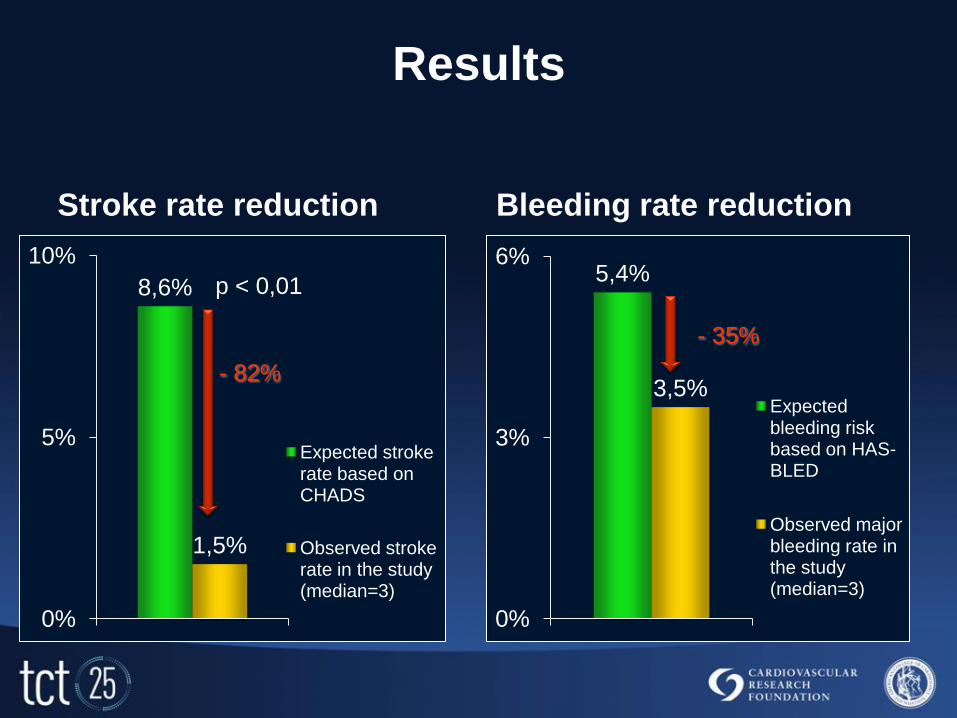
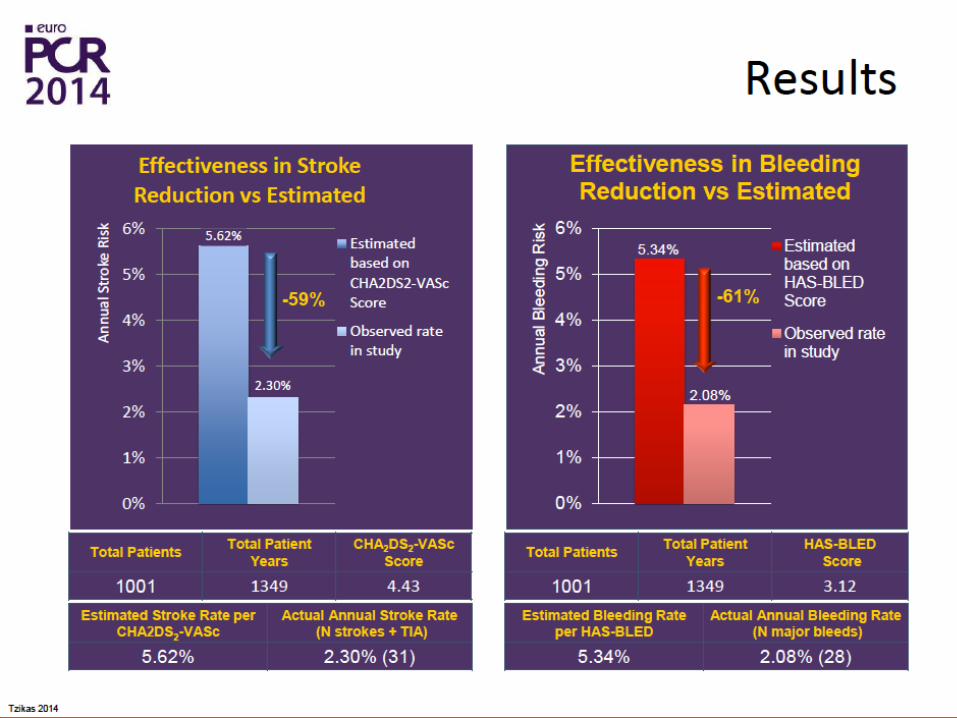
Results
Stroke rate reduction
8,6%
1,5%
0%
5%
10%
Expected stroke rate based on CHADS
Observed stroke rate in the study (median=3)
Bleeding rate reduction
5,4%
3,5%
0%
3%
6%
Expected bleeding risk based on HAS-BLED
Observed major bleeding rate in the study (median=3)
p < 0,01
- 82%
- 35%
INDICAZIONI ALLA CHIUSURA PERCUTANEA
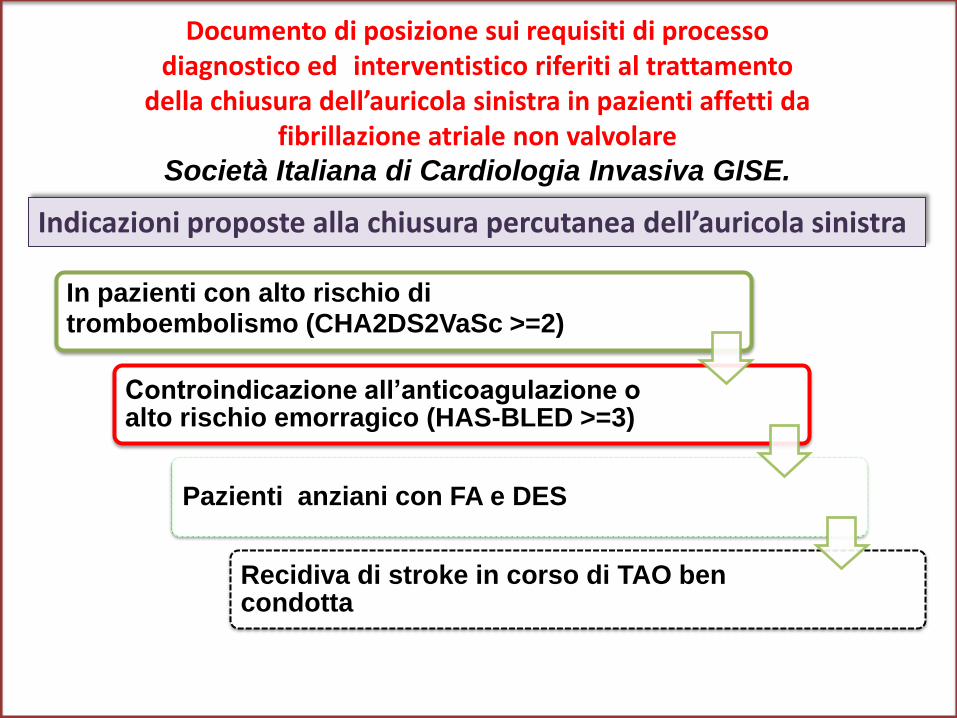
Indicazioni proposte alla chiusura percutanea dell’auricola sinistra
Documento di posizione sui requisiti di processo diagnostico ed interventistico riferiti al trattamento
della chiusura dell’auricola sinistra in pazienti affetti da fibrillazione atriale non valvolare
Società Italiana di Cardiologia Invasiva GISE.
In pazienti con alto rischio di tromboembolismo (CHA2DS2VaSc >=2)
Controindicazione all’anticoagulazione o alto rischio emorragico (HAS-BLED >=3)
Pazienti anziani con FA e DES
Recidiva di stroke in corso di TAO ben condotta
Indicazioni
• NICE 2010 –
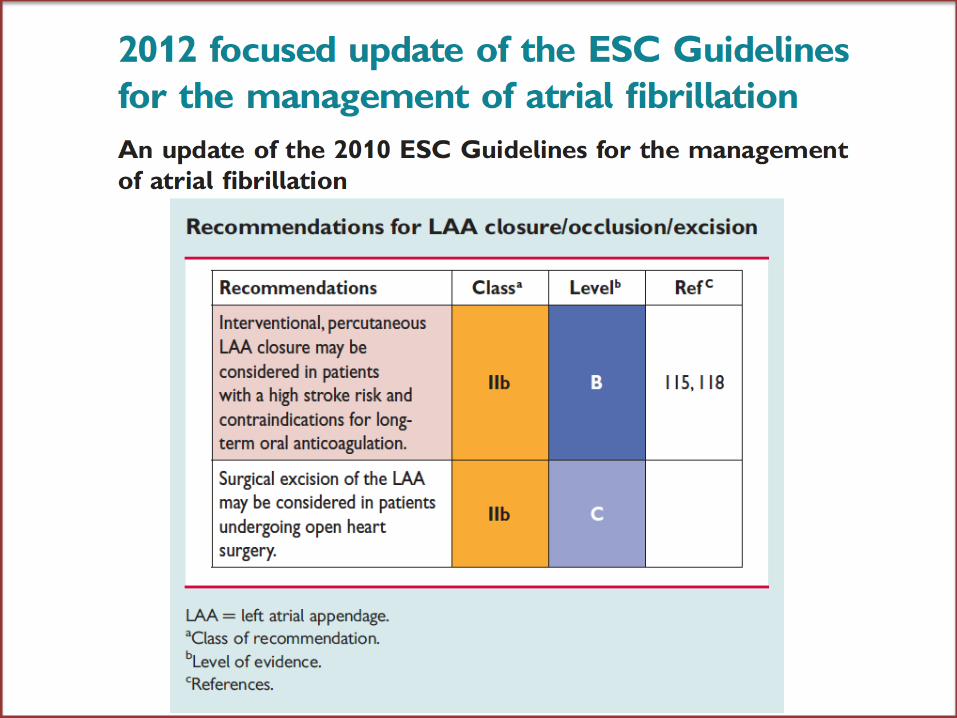
• ESC 2012 –
• GISE/AIAC 2014 –
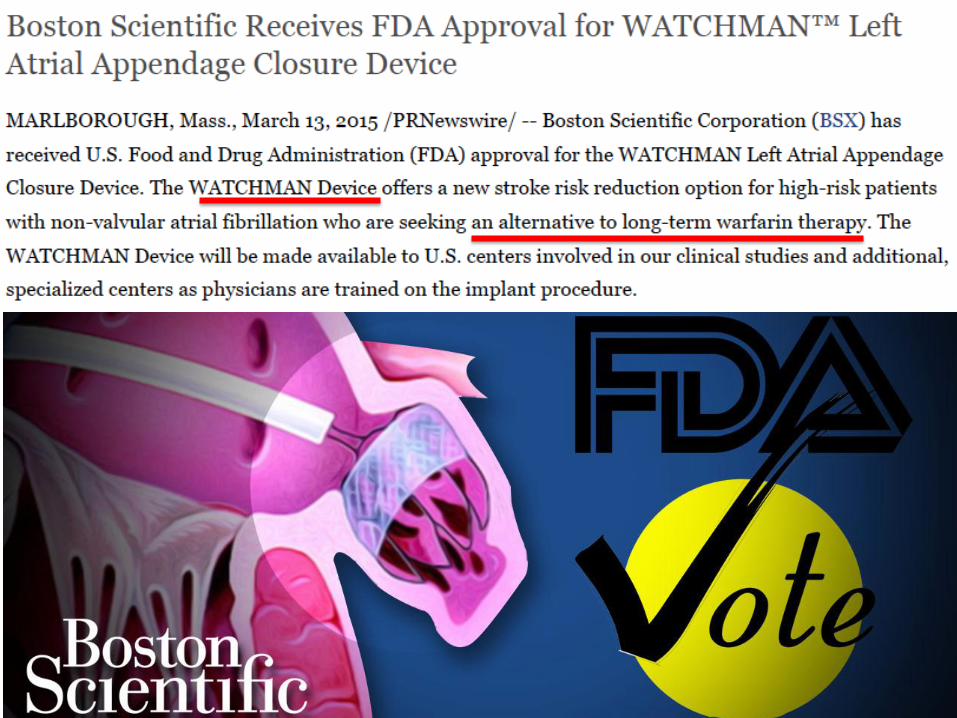
• FDA – Watchman
• EHRA/EAPCI 2014
Contraindication to OAC
Increased bleeding risk
As alternative to oral
anticoagulation
Cardiochirurgia
• NICE 2010 – Cardiac surgery on-site
• EHRA/EAPCI 2014 – Cardiac surgery center at 60 min (operating
room)
• GISE/AIAC 2014 – Cardiac surgery on-site

Thank you for your
attention!
Clinical
Cardiologist Neurologist
Cardiac
Surgeon
Electrophysiologist
Echo
Team Interventional
Cardiologist