Nuove terapie ed indicazioni nella leucemia linfatica cronica · Nuove terapie ed indicazioni nella...
39
Nuove terapie ed indicazioni nella leucemia linfatica cronica PHBE/IBR/0217/0003 Paolo Ghia Lab of B Cell Neoplasia – Division of Experimental Oncology Strategic Research Program on CLL – Department of Onco-Hematology Università Vita-Salute San Raffaele – Milano IsJtuto ScienJfico San Raffaele – Milano
Transcript of Nuove terapie ed indicazioni nella leucemia linfatica cronica · Nuove terapie ed indicazioni nella...
Nuove terapie ed indicazioni nella leucemia linfatica cronica
PHBE/IBR/0217/0003
PaoloGhia
LabofBCellNeoplasia–DivisionofExperimentalOncologyStrategicResearchProgramonCLL–DepartmentofOnco-Hematology
UniversitàVita-SaluteSanRaffaele–MilanoIsJtutoScienJficoSanRaffaele–Milano

aPFSrepresenta,veonly;cannotbeusedtocompareregimensdirectlybecauseresultsaredrawnfromacrosstrialswithdifferentpa,entcharacteris,csB:bendamus,ne;C:cyclophosphamide;CIT:chemoimmunotherapy;CLL:chroniclymphocy,cleukemia;F:fludarabine;PFS:progression-freesurvival;R:rituximab
1.ShanafeltT.HematologyAmSocHematolEducProgram2013;2013:158–167.2.EichhorstB,etal.ASH2014(Abstract19;oralpresenta,on).
Single-agentalkyla,ngagents(e.g.chlorambucil)
BRforpa,entsnotsuitableforFCR2
Purineanalogs(e.g.fludarabine)
Combina,onchemotherapy(e.g.FC)
Chemoimmunotherapy(e.g.FCR)
1960s 1970s 1980s 1990s 2000s 2010s
1220
34
58
43
2014-16
Noveltargetedagents:
idelalisib,ibru,nibandVenetoclax
RepresentaJvePFS/TFS(months)1,a
CLLtreatmenthasevolvedovermulJpledecades

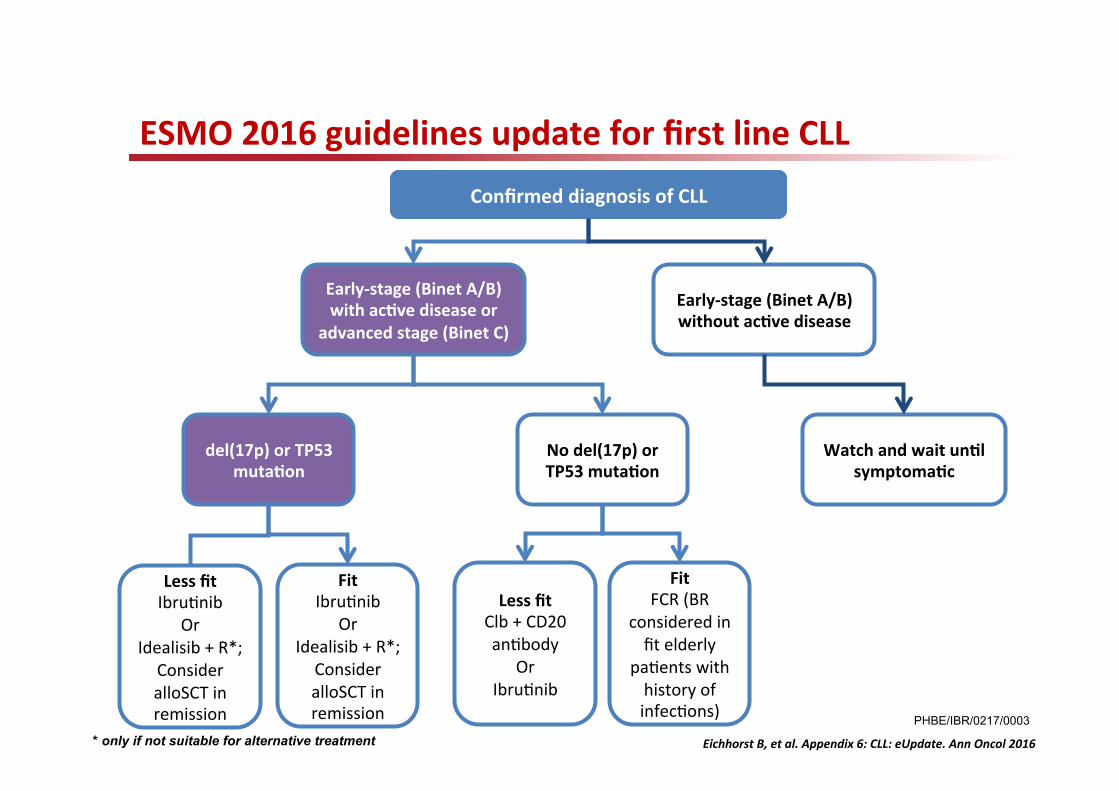
ESMO2016guidelinesupdateforfirstlineCLLConfirmeddiagnosisofCLL
Early-stage(BinetA/B)withacJvediseaseor
advancedstage(BinetC)
Early-stage(BinetA/B)withoutacJvedisease
WatchandwaitunJlsymptomaJc
del(17p)orTP53mutaJon
FitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
LessfitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
Nodel(17p)orTP53mutaJon
FitFCR(BR
consideredinfitelderly
pa,entswithhistoryofinfec,ons)
LessfitClb+CD20an,body
OrIbru,nib
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016* only if not suitable for alternative treatment
• Disease relapse is not a criterion to re-start therapy unless the disease is progressive and symptomatic
• Second-line treatment decisions should follow the same indications as those used for first-line treatment
Hallek, M. iwCLL 2017 (invited oral presentation)
Secondlinetreatmentdecisions

ConfirmeddiagnosisofCLL
Early-stage(BinetA/B)withacJvediseaseor
advancedstage(BinetC)
Early-stage(BinetA/B)withoutacJvedisease
WatchandwaitunJlsymptomaJc
del(17p)orTP53mutaJon
FitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
LessfitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
Nodel(17p)orTP53mutaJon
FitFCR(BR
consideredinfitelderlypa,entswithhistoryofinfec,ons)
LessfitClb+CD20an,body
OrIbru,nib
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016* only if not suitable for alternative treatment
ESMO2016guidelinesupdateforfirstlineCLL

LongtermremissionswithFCR
1.FischerK,etal.Blood2016;127:208–215;2.ThompsonPA,etal.Blood2016;127:303–309.
NIGHV-M,MRDneg 35IGHV-M,MRDpos 34IGHV-UM,MRDneg 35IGHV-UM,MRDpos 66
75
50
25
0
100
Time(Years)
Percen
tProgression
-Free
1 2 3 4 5 160 6 7 8 9 101112131415
CLL81
p<0.0001
MDACC2
IGHV,immunoglobulinheavychain;M,mutated;MDACC,MDAndersonCancer;UM,unmutated.
N
FCRIGHVMpa,ents 113FCIGHVMpa,ents 117FCRIGHVUMpa,ents 197FCIGHVUMpa,ents 195
0.8
0.6
0.4
0.2
0
1.0
Time(Months)
Prob
abilityofP
FS
12 24 36 48 60 960 72 84
p<0.001bylog-ranktest
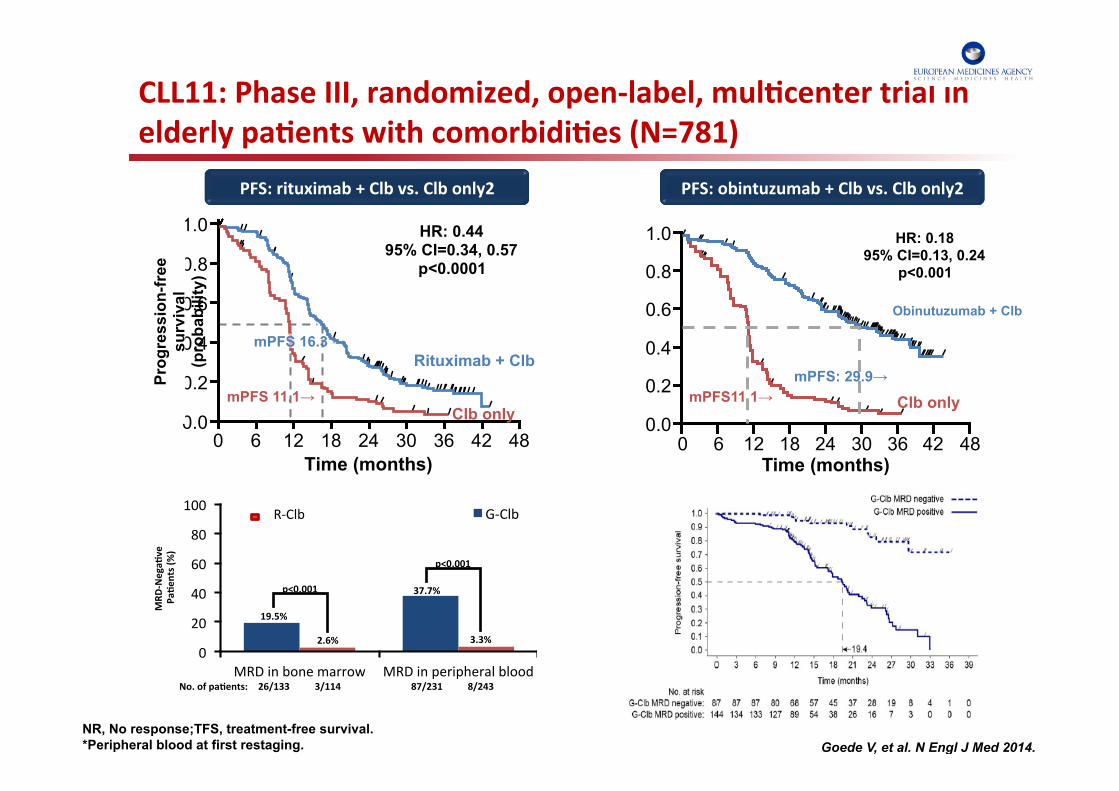
CLL11:PhaseIII,randomized,open-label,mulJcentertrialinelderlypaJentswithcomorbidiJes(N=781)
Goede V, et al. N Engl J Med 2014. NR, No response;TFS, treatment-free survival. *Peripheral blood at first restaging.
0
20
40
60
80
100
MRDinbonemarrow MRDinperipheralblood
G-ClbR-Clb
MRD
-NegaJ
ve
PaJe
nts(%)
26/133No.ofpaJents: 3/114 87/231 8/243
19.5%
2.6%
37.7%
3.3%
p<0.001
p<0.001
PFS:rituximab+Clbvs.Clbonly2
Time (months) 0 6 12 18 24 30 36 42 48
1.0
0.8
0.6
0.4
0.2
0.0 mPFS 11.1→
mPFS 16.3 → Rituximab + Clb
Clb only
HR: 0.44 95% CI=0.34, 0.57
p<0.0001
Prog
ress
ion-
free
su
rviv
al
(pro
babi
lity)
HR: 0.18 95% CI=0.13, 0.24
p<0.001
Obinutuzumab + Clb
Clb only
Time (months)
mPFS11.1→ mPFS: 29.9→
1.0
0.4
0.0
0.2
0.8
0.6
0 6 12 18 30 36 24 42 48
PFS:obintuzumab+Clbvs.Clbonly2

ConfirmeddiagnosisofCLL
Early-stage(BinetA/B)withacJvediseaseor
advancedstage(BinetC)
Early-stage(BinetA/B)withoutacJvedisease
WatchandwaitunJlsymptomaJc
del(17p)orTP53mutaJon
FitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
LessfitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
Nodel(17p)orTP53mutaJon
FitFCR(BR
consideredinfitelderlypa,entswithhistoryofinfec,ons)
LessfitClb+CD20an,body
OrIbru,nib
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016* only if not suitable for alternative treatment
ESMO2016guidelinesupdateforfirstlineCLL

1.Halleketal.Blood.2008;111:5446-5456;2.Halleketal,Blood.2012;e-lejer,June04,2012 Burger J et al, NEJM 2015
RESONATE-2 (PCYC-1115) Study Design
PaJents(N=269)• Treatment-naïveCLL/SLLwithac,vedisease
• Age≥65years• Forpa,ents65-69years,comorbiditythatmayprecludeFCR
• del17pexcluded• Warfarinuseexcluded
ibruJnib420mgoncedailyunJlPDorunacceptabletoxicity
chlorambucil0.5mg/kg(tomaximum0.8mg/kg)days1and15of28-daycycleupto12cycles
*Pa,entswithIRC-confirmedPDenrolledintoextensionStudy1116forfollow-upandsecond-linetreatmentperinves,gator’schoice(includingibru,nibforpa,entsprogressingonchlorambucilwithiwCLLindica,onfortreatment).
! Phase3,open-label,mul,center,interna,onalstudy! Primaryendpoint:PFSasevaluatedbyIRC(2008iwCLLcriteria)1,2! Secondaryendpoints:OS,ORR,hematologicimprovement,safety
IRC-confirmedprogression
PCYC-1116ExtensionStudy*
Inclbarm,n=43
crossedovertoibru,nib
StraJficaJonfactors• ECOGstatus(0-1vs.2)• Raistage(III-IVvs.≤II)
RANDOMIZE1:1
PHBE/IBR/0217/0003

Updated Efficacy and Safety from the Phase 3 Resonate-2 Study:IbruJnibAsFirst-LineTreatmentinPaJents≥65YearswithCLL/SLL
Barr et al., ASH 2016; abstr.# 234
CRratesconJnuetoimprove:7%@12mo"15%@24mo"18%@29mo
ibruJnib(n=136) vs chlorambucil
(n=133)
follow-up18,4months"29months
n=55 crossed over to ibrutinib following PD
OverallSurvivalMedian PFS not reached
n=55 crossed over to ibrutinib following PD
• PFS@18mo:90%"PFS@24mo:89%• PFSbenefitacrossallsub-groups• (FitpaJents:medianPFSFCR"55mo;BR"42mo)
Progression-FreeSurvival

AreWeHarmingOurPaJentswithoutMRD?
0 3 6 9 12 15 18 21 24 27 30 33 36 39
1.0
0.8
0.6
0.4
0.2
0.0
Time (months)
GCLLSGCLL11:Obinutuzumab+chlorambucil2
1.Barretal.,ASH2016;2.GoedeV,etal.NEnglJMed2014
G-Clb
R-Clb
15.2 26.7
Stratified HR: 0.39 95% CI: 0.31–0.49 p<0.0001
NoMRD-negaJvecaseswerereported
RESONATE-2:Ibru,nibvschlorambucil1
! 88%reducJonintheriskofprogressionordeathforpaJentsrandomizedtoibruJnib
! 41%ofpaJentsreceivingchlorambucilhavecrossedovertoreceiveibruJnib
ConfirmeddiagnosisofCLL
Early-stage(BinetA/B)withacJvediseaseor
advancedstage(BinetC)
Early-stage(BinetA/B)withoutacJvedisease
WatchandwaitunJlsymptomaJc
del(17p)orTP53mutaJon
FitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
LessfitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
Nodel(17p)orTP53mutaJon
FitFCR(BR
consideredinfitelderly
pa,entswithhistoryofinfec,ons)
LessfitClb+CD20an,body
OrIbru,nib
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016* only if not suitable for alternative treatment
ESMO2016guidelinesupdateforfirstlineCLL
PHBE/IBR/0217/0003
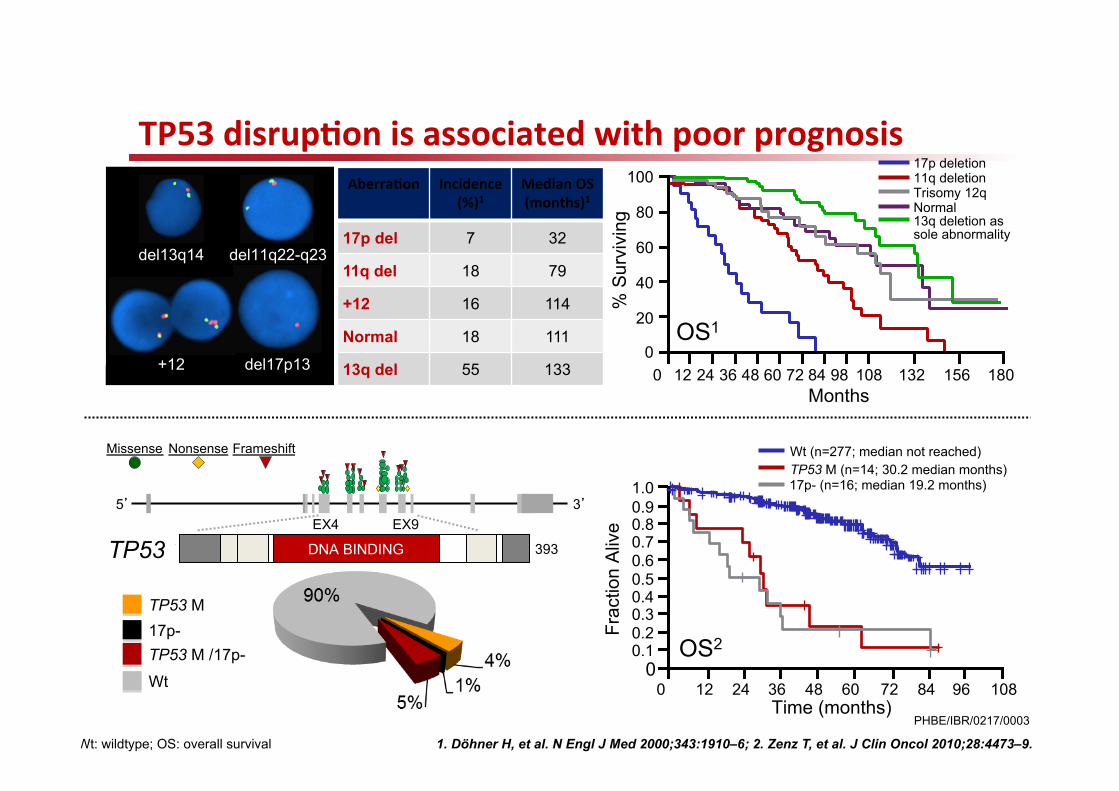
TP53disrupJonisassociatedwithpoorprognosis
Wt: wildtype; OS: overall survival
Nonsense Missense Frameshift
5’ 3’
1 DNA BINDING
EX4 EX9
393 TP53
TP53 M 17p- TP53 M /17p-
Wt
AberraJon Incidence(%)1
MedianOS(months)1
17p del 7 32
11q del 18 79
+12 16 114
Normal 18 111
13q del 55 133
13q deletion as sole abnormality
17p deletion
Normal Trisomy 12q 11q deletion
Months
% S
urvi
ving
0 12 24 36 48 60 72 84 98 108 132 156 180
100
80
40
20
0
60
Wt (n=277; median not reached) TP53 M (n=14; 30.2 median months) 17p- (n=16; median 19.2 months)
Time (months)
Frac
tion
Aliv
e
0 OS2
0 12 24 36 48 60 72 84 96 108
1.0
0.4
0.1 0.2 0.3
0.5 0.6
0.9 0.8 0.7
del13q14
del17p13 +12
del11q22-q23
OS1
1. Döhner H, et al. N Engl J Med 2000;343:1910–6; 2. Zenz T, et al. J Clin Oncol 2010;28:4473–9.
PHBE/IBR/0217/0003
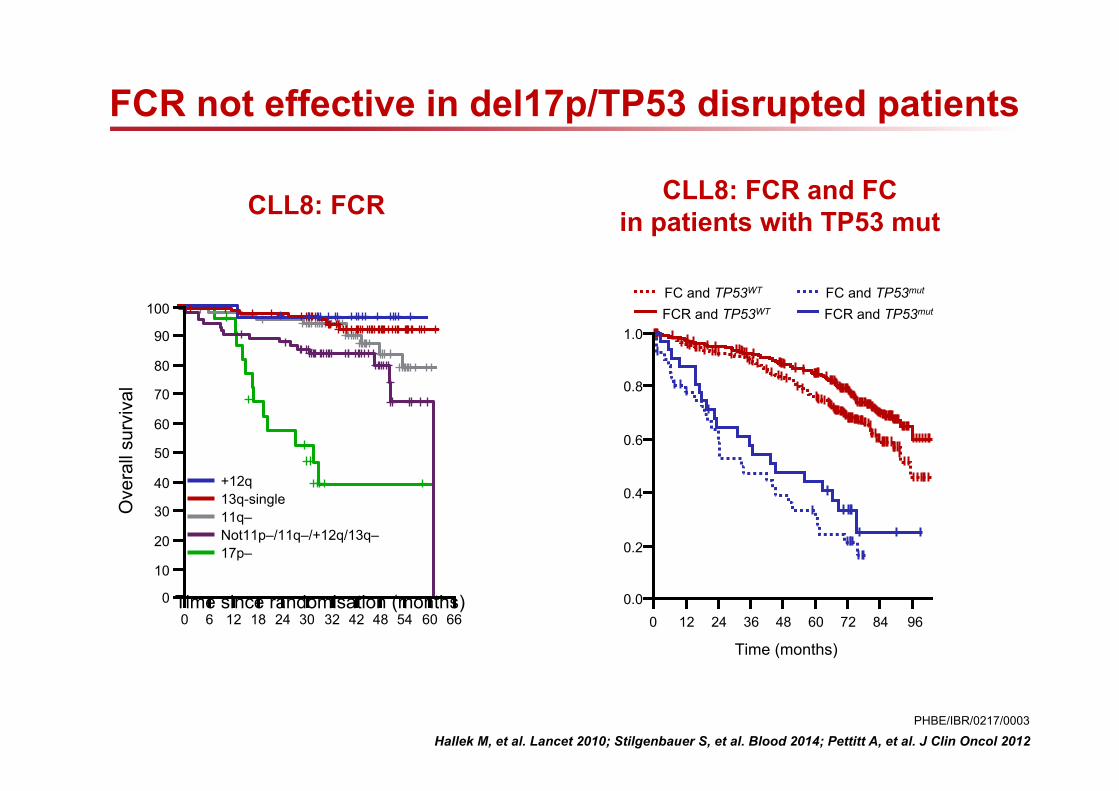
FCR not effective in del17p/TP53 disrupted patients
Hallek M, et al. Lancet 2010; Stilgenbauer S, et al. Blood 2014; Pettitt A, et al. J Clin Oncol 2012
CLL8: FCR and FC in patients with TP53 mut
FC and TP53WT FC and TP53mut
FCR and TP53WT FCR and TP53mut
Time (months)
0.0
0.2
0.4
0.6
0.8
1.0
24 36 48 60 72 84 0 12 96
Ove
rall
surv
ival
Time since randomisation (months)
+12q 13q-single 11q– Not11p–/11q–/+12q/13q– 17p–
0 6 18 30 32 42 48 66 24 12 54 60 0
10
50
70
100
30
40
60
80
90
20
CLL8: FCR
PHBE/IBR/0217/0003

Pro
gre
ssio
n-F
ree
Su
rviv
al
(%)
Months
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24
|
|| | | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||||||| |
|| |||
| |
|
|| |||||||||||||||||| || ||||
|||||||||| |
|||
|
|
|
|
|
||||
|
|
|||
| | ||||||||||||
|
N at Riskibrutinib lymphocytosis, yes 133 130 126 120 113 49 5 3ibrutinib lymphocytosis, no 59 55 49 48 40 20 4
ofatumumab lymphocytosis, yes 24 17 9 3 1 0ofatumumab lymphocytosis, no 166 140 106 60 28 2
ibrutinib lymphocytosis, yesibrutinib lymphocytosis, noofatumumab lymphocytosis, yesofatumumab lymphocytosis, no
Pro
gre
ssio
n-F
ree
Su
rviv
al
(%)
Months
ibrutinib 1 prior therapyibrutinib >1 prior therapyofatumumab 1 prior therapyofatumumab >1 prior therapy
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24
N at Riskibrutinib 1 prior therapy 35 35 34 33 30 17 2 1
ibrutinib >1 prior therapy 160 152 143 136 124 52 7 2ofatumumab 1 prior therapy 54 46 35 19 9
ofatumumab >1 prior therapy 142 112 80 44 20 2
| | | ||||||||| | || ||||||||||||| || | |
|| |
||| | | | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||| | | ||||||||||||||||||||||||||||||||||||||||| |
|||| | |
||
|
||
||
| | || |
||||
|
|
||
|
|
| || ||
|||||
|
N at Riskibrutinib del17p, yes 63 59 53 52 47 26 5 2ibrutinib del17p, no 132 128 124 117 107 43 4 1
ofatumumab del17p, yes 64 45 29 15 9 2ofatumumab, del17p, no 132 113 86 48 20
Pro
gre
ssio
n-F
ree
Su
rviv
al
(%)
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24
|| | |||||||||||||||||| || ||||||||||||||||||| |
|| ||
| | |
|| | | | | |||||||||||||||||||||||||||||||||||||||||||||||||||||||| | ||||||||||||||||||||||||||||||||||||| ||| |
||
|
|
|
| ||
||||
|
|||
|
|
||
| | | |||||||
|||
Months
ibrutinib del17p, noibrutinib del17p, yes
ofatumumab, del17p, noofatumumab del17p, yes
ibrutinibdel17p, no
ibrutinibdel17p, yes
Median PFS (mo) NR NRHazard Ratio 1.314
(95% CI) (0.698-2.473)Log-Rank P value 0.396
8.2 5.91.413
(1.017-1.963)0.039
ofatumumab,del17p, no
ofatumumabdel17p, yes
ibrutinib>1 priortherapy
ibrutinib1 prior
therapy
Median PFS (mo) NR NR
Hazard Ratio 3.108
(95% CI) (0.959-10.07)
Log-Rank P value 0.046
8.0 8.2
1.238
(0.870-1.763)
0.235
ofatumumab>1 priortherapy
ofatumumab1 prior
therapy
ibrutiniblymphocytosis,
yes
ibrutiniblymphocytosis,
no
Median PFS (mo)
Hazard Ratio
(95% CI)
Log-Rank P value
NRNR
0.584
(0.308-1.107)
0.096
ibruJnibdel17p,no
ibruJnibdel17p,yes
ofatumumabdel17p,no
ofatumumabdel17p,yes
MedianPFS(mo) NR NR 8.2 5.9
HazardraJo 1.314 1.413
(95%CI) (0.698-2.473) (1.017-1.963)
Pvalue 0.396 0.039
Thornton et al, EHA 2015 Vienna
No Difference in PFS With or Without Del17p
0 2 4 6 8 1 0 1 2 1 4 1 6 1 8 2 0 2 2 2 4 2 60
2 0
4 0
6 0
8 0
1 0 0
T im e (m o n th s )
No del 64 61 59 59 52 37 21 14 11 8 4 1 1 1Del 46 41 36 36 33 30 22 12 8 4 3 0
Del17p/TP53mut: Present vs Not Present
Del17p/TP53mut (n=46) No del17p/TP53mut (n=64)
Median PFS (95% CI) p-value No del 20.3 mo (19.4, ‒ )
0.94 Del 16.6 mo (13.9, ‒ )
Prog
ress
ion
free
sur
viva
l (%
)
Sharman, ASH, 2014, Abstract 330
PHBE/IBR/0217/0003

TP53 Network
• ERIC aims to advance assessment of TP53 aberrations through education about: – Importance of testing all cases needing
therapy, before first and later lines of treatment
– Quality of appropriate techniques in diagnostic laboratories to ensure reliable and comparable results between institutions # Certification of laboratories
Thessaloniki
Brno
Uppsala
Ulm London
Novara Madrid
Paris Amsterdam
Copenhagen
Bellinzona
www.ericll.org. 1L: first-line; 2L: second-line Pospisilova S, et al. Leukemia 2012; 26:1458–1461.
Diseasestage Clinicaltrial GeneralpracJce Comment
Diagnosis Recommended Notindicated
ResultsofTP53muta,ontes,ngwillnotinfluenceini,alwatchandwaitstrategy
1Ltreatment Recommended Desirable Pa,entswithTP53muta,onshouldbeenteredontoaclinicaltrialexploringnewtherapeu,cagents>2Ltreatment Recommended DesirablePatients should be treated with BCR
pathway inhibitor Recommended
Updatecomingsoon

ConfirmeddiagnosisofCLL
Early-stage(BinetA/B)withacJvediseaseor
advancedstage(BinetC)
Early-stage(BinetA/B)withoutacJvedisease
WatchandwaitunJlsymptomaJc
del(17p)orTP53mutaJon
FitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
LessfitIbru,nib
OrIdealisib+R*;
ConsideralloSCTinremission
Nodel(17p)orTP53mutaJon
FitFCR(BR
consideredinfitelderly
pa,entswithhistoryofinfec,ons)
LessfitClb+CD20an,body
OrIbru,nib
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016* only if not suitable for alternative treatment
ESMO2016guidelinesupdateforfirstlineCLL
PHBE/IBR/0217/0003

Idelalisibinfirstline:changesin2016
March September April May June July August
2016
EC: European Commission; EMA: European Medicines Agency; CHMP: Committee for Medicinal Products for Human Use; PJP: Pneumocystis jirovecii pneumonia; PRAC: Pharmacovigilance Risk Assessment Committee
EMA press release (8 July 2016; available at www.ema.europa.eu). EMA press release (22 July 2016; available at www.ema.europa.eu).
Zydelig SmPC (Date TBC 2016; available at www.ema.europa.eu).
8 July • PRAC concluded its review of idelalisib and recommended idelalisib-treated patients:
• receive PJP prophylaxis during treatment and for up to 6 months after treatment end • are regularly monitored for CMV infection if CMV serology is positive at start of treatment or if
there is a history of CMV infection • Patients with evidence of CMV viraemia and clinical signs of infection should have their
treatment interrupted until the infection is resolved • are monitored for infection and have regular blood tests for white cell counts
• PRAC also concluded that idelalisib can again be initiated in first-line CLL treatment, in patients with del(17p)/TP53 mutation who are ineligible for other therapies
15 September. Final EC decision
22 July • The CHMP confirmed the PRAC recommendations
PHBE/IBR/0217/0003
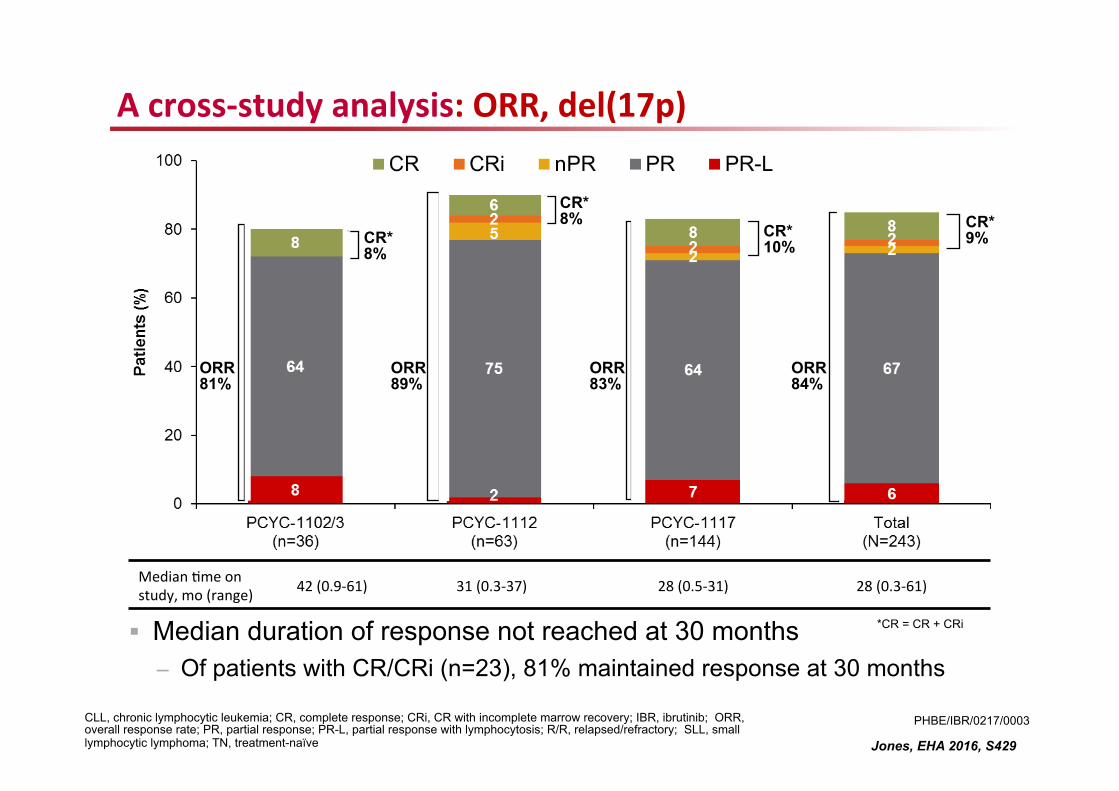
Across-studyanalysis:ORR,del(17p)
Median,meonstudy,mo(range) 42(0.9-61) 31(0.3-37) 28(0.5-31) 28(0.3-61)
CR* 8%
CR* 8%
CR* 10%
CR* 9%
ORR 81%
ORR 89%
ORR 83%
ORR 84%
*CR = CR + CRi ! Median duration of response not reached at 30 months – Of patients with CR/CRi (n=23), 81% maintained response at 30 months
CLL, chronic lymphocytic leukemia; CR, complete response; CRi, CR with incomplete marrow recovery; IBR, ibrutinib; ORR, overall response rate; PR, partial response; PR-L, partial response with lymphocytosis; R/R, relapsed/refractory; SLL, small lymphocytic lymphoma; TN, treatment-naïve Jones, EHA 2016, S429
PHBE/IBR/0217/0003

Results:PFSandOS,del(17p)
12-moOS,%(95%CI)
24-moOS,%(95%CI)
30-moOS,%(95%CI)
85%(80,89) 75%(68,80) 67%(59,74)
MedianOSnotreached
! With a median (range) study duration of 28 (0.3-61+) months, median PFS and OS were not reached
12-moPFS,%(95%CI)
24-moPFS,%(95%CI)
30-moPFS,%(95%CI)
80%(74,84) 63%(57,69) 55%(48,62)
MedianPFSnotreached
CLL, chronic lymphocytic leukemia; IBR, ibrutinib; OS, overall survival; PFS, progression-free survival; R/R, relapsed/refractory; SLL, small lymphocytic lymphoma
PFS OS
Jones, EHA 2016, S429
PHBE/IBR/0217/0003

21
EMA approval for Venclyxto on 08DEC16
• Venclyxto monotherapy is conditionally approved for the treatment of
chronic lymphocytic leukaemia (CLL) in the presence of 17p deletion or TP53 mutation in adult patients who are unsuitable for or have failed a B-cell receptor pathway inhibitor
• Venclyxto monotherapy is conditionally approved for the treatment of CLL in without 17p deletion or TP53 mutation in adult patients who have failed both chemoimmunotherapy and a B-cell receptor pathway inhibitor
VenetoclaxWE&CAdvisoryBoardI2016PHBE/IBR/0217/0003
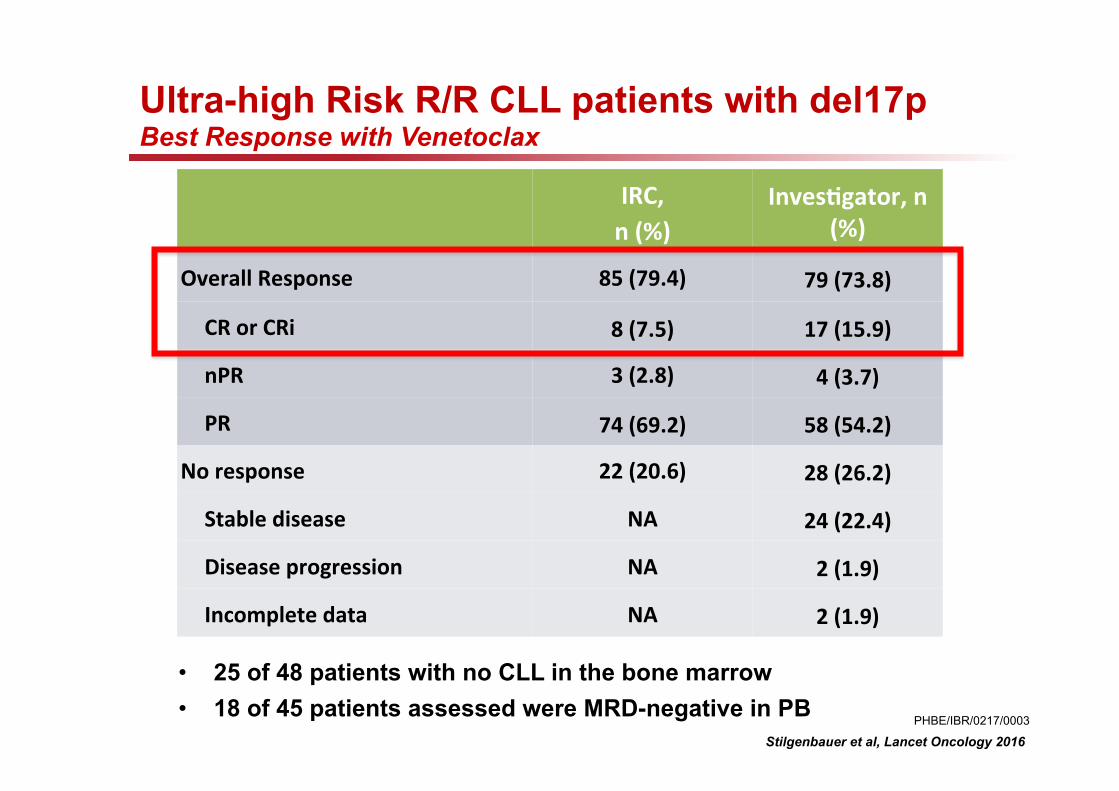
IRC,n(%)
InvesJgator,n(%)
OverallResponse 85(79.4) 79(73.8)
CRorCRi 8(7.5) 17(15.9)
nPR 3(2.8) 4(3.7)
PR 74(69.2) 58(54.2)
Noresponse 22(20.6) 28(26.2)
Stabledisease NA 24(22.4)
Diseaseprogression NA 2(1.9)
Incompletedata NA 2(1.9)
• 25 of 48 patients with no CLL in the bone marrow • 18 of 45 patients assessed were MRD-negative in PB
Stilgenbauer et al, Lancet Oncology 2016
Ultra-high Risk R/R CLL patients with del17p Best Response with Venetoclax
PHBE/IBR/0217/0003

! Of 45 patients tested, 18 achieved MRD-negativity in
peripheral blood
MRD-Negativity
Cumulative Incidence of Response
Stilgenbauer et al, Lancet Oncology 2016
PFS and OS (N=107)
• 12-month estimates (95% CI): – PFS: 72.0% (61.8, 79.8) – OS: 86.7% (78.6, 91.9)
PHBE/IBR/0217/0003

24
Ibru,nib
FCRClb+an,-CD20
TP53statusIGHVstatus
Chemo+an,CD20
Age,CIRS,Crclearance
ClinicalstageiwCLLcriteria
W&W Tx
BR
Suitability
Venetoclax Idelalisib+R
Modified from Rossi D., iwCLL 2017 (invited oral presentation)
CANTREATMENTDECISIONBEINFORMEDBYBIOMARKERS?

ESMO2015clinicalpracJceguidelinesforR/RCLL
RelapsedCLLrequiringtreatmentorrefractoryCLL
Earlyrelapse(within24–36monthsarerchemoimmunotherapy)
FitClinicalstudyBCRinhibitor
(±R)Considerallo-
SCTinremission
LessfitClinicalstudyBCRinhibitor
(±R)(BRorFCR-Litemaybeconsideredifnodel(17p)or
TP53muta,on)
Laterelapse(≥24–36monthsarerchemoimmunotherapy)
del(17p)orTP53mutaJon
FitClinicalstudy
RepeatfrontlineorchangetoBR/
FCRorBCRinhibitor(±R)
LessfitClinicalstudy
RepeatfrontlineorchangetoBRorBCRinhibitor
(±R)
Nodel(17p)orTP53mutaJon
Treatasperearlyrelapse
EichhorstB,etal.AnnOncol2015;26(Suppl5):v78–v84

ImpressiveOverallresponserate(ORR)
a Number of evaluable patients
R: rituximab Furman et al, NEJM 2014; Coutre SE, et al. EHA 2014; Byrd et al, NEJM 2014.
Idelalisib + R
(n=102a) O
RR
±95
% C
I (%
) Placebo
+ R (n=101a)
Odds ratio: 17.3 p<0.0001
RESONATE:IbruJnibversusofatumumab1
Previously-treatedCLL
Study116(secondinterimanalysis):Idelalisib+Rversusplacebo+R2,3
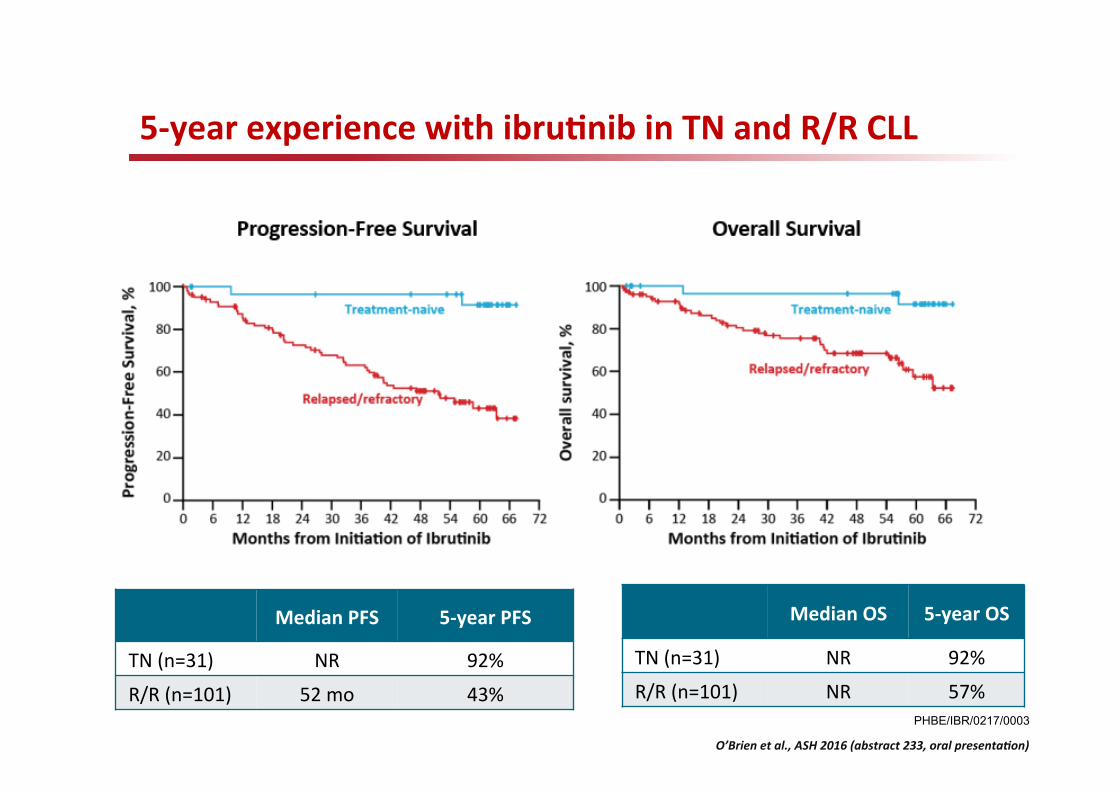
MedianPFS 5-yearPFS
TN(n=31) NR 92%
R/R(n=101) 52mo 43%
MedianOS 5-yearOS
TN(n=31) NR 92%
R/R(n=101) NR 57%
5-yearexperiencewithibruJnibinTNandR/RCLL
O’Brienetal.,ASH2016(abstract233,oralpresentaZon)
PHBE/IBR/0217/0003
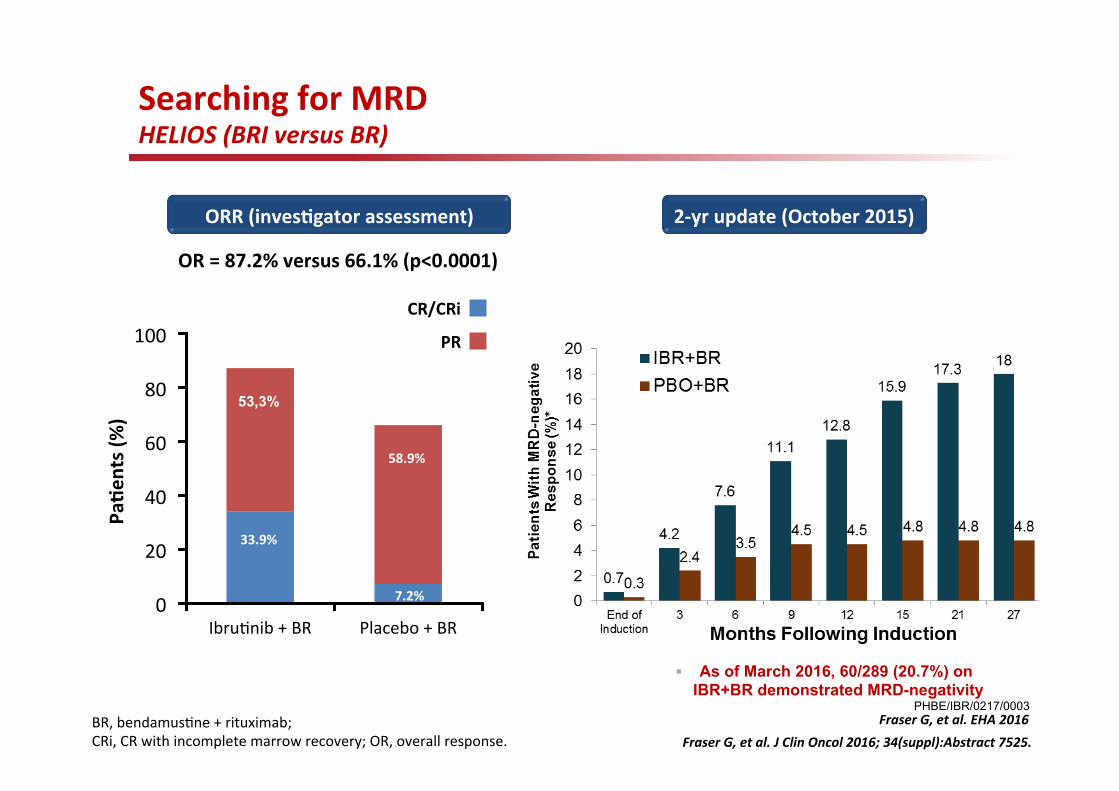
SearchingforMRDHELIOS(BRIversusBR)
FraserG,etal.JClinOncol2016;34(suppl):Abstract7525.BR,bendamus,ne+rituximab;CRi,CRwithincompletemarrowrecovery;OR,overallresponse.
! As of March 2016, 60/289 (20.7%) on IBR+BR demonstrated MRD-negativity
2-yrupdate(October2015)
FraserG,etal.EHA2016
ORR(invesJgatorassessment)
53,3%
0
20
40
60
80
100
Ibru,nib+BR Placebo+BR
7.2%
PaJe
nts(%)
OR=87.2%versus66.1%(p<0.0001)
PR
CR/CRi
58.9%
33.9%
PHBE/IBR/0217/0003
29
EMAapprovalforVenclyxtoon08DEC16
• Venclyxto monotherapy is conditionally approved for the treatment of
chronic lymphocytic leukaemia (CLL) in the presence of 17p deletion or TP53 mutation in adult patients who are unsuitable for or have failed a B-cell receptor pathway inhibitor
• Venclyxto monotherapy is conditionally approved for the treatment of CLL in without 17p deletion or TP53 mutation in adult patients who have failed both chemoimmunotherapy and a B-cell receptor pathway inhibitor
VenetoclaxWE&CAdvisoryBoardI2016PHBE/IBR/0217/0003

Roberts AW, et al. N Engl J Med 2016; 374(4): 311-22; EHA 2016 P209
80% MRD-neg (% of CR) 35%
CompleteresponseswithBCL2inhibitors:ABT-199
PHBE/IBR/0217/0003

Brander, EHA 2016 P223
M13-365: Venetoclax Combined with Rituximab in Patients with R/R CLL/SLL
* Two discontinued with no evidence of progression. Seymour JF et al, Lancet Oncol 2017
NoneoftheMRD-negaJvepaJentshaveprogressed;
2paJentswithMRD-posiJveCR/CRihadasymptomaJcprogression
55%ofpaJentsMRD-negaJve(27/49)
11paJentsstoppedvenetoclaxarerachievinganobjecJveresponse(9MRD-negaJve);
9remaininfollow-up*
Venetoclax+RituximabinPaJentswithR/RCLLM13-365(N=49)
*
*
#
0 5 10 15 20 25 30 35 40
TimeonvenetoclaxTimeoffvenetoclax
# MRD-negaJvePR* DisconJnuedfromstudy
AsymptomaJcprogression
PHBE/IBR/0217/0003

ESMO2015clinicalpracJceguidelinesforR/RCLL
RelapsedCLLrequiringtreatmentorrefractoryCLL
Earlyrelapse(within24–36monthsarerchemoimmunotherapy)
FitClinicalstudyBCRinhibitor
(±R)Considerallo-
SCTinremission
LessfitClinicalstudyBCRinhibitor
(±R)(BRorFCR-Lite
maybeconsideredifnodel(17p)orTP53
mutaJon)
Laterelapse(≥24–36monthsarerchemoimmunotherapy)
del(17p)orTP53mutaJon
FitClinicalstudy
RepeatfrontlineorchangetoBR/
FCRorBCRinhibitor(±R)
LessfitClinicalstudy
RepeatfrontlineorchangetoBRorBCRinhibitor
(±R)
Nodel(17p)orTP53mutaJon
Treatasperearlyrelapse
EichhorstB,etal.AnnOncol2015;26(Suppl5):v78–v84
PaJentsnotrespondingnorprogressingupontherapywithkinaseinhibitorsmightbeswitchedtoadifferentkinaseinhibitorortoBCL2antagonistswhenavailable(accordingtoclinicaltrials)
EichhorstB,etal.Appendix6:CLL:eUpdate.AnnOncol2016
PHBE/IBR/0217/0003

RESONATE:SeriousAdverseEvents(SAEs)
Diarrhea
0% 20% 40% 60% 80% 100%
Grade 1
Grade 2
Grade 3
Grade 4
Fatigue
Nausea
Pyrexia
Anemia
Cough
Neutropenia
Upper respiratory tract infection
Arthralgia
Peripheral edema
Constipation
Muscle spasms
Sinusitis
Thrombocytopenia
Vomiting
Pneumonia
! 13 (7%) of ibrutinib-treated patients discontinued due to AE/unacceptable toxicity Thornton et al, ICML 2015

RESONATE: SeriousAdverseEvents(SAEs)
Adverse event, % Ibrutinib (n=195)
Ofatumumab (n=191)
Median treatment duration 8.6 months 5.3 months Subjects reporting ≥1 SAE 42% 30% Reporting ≥1 AE grade ≥3 57% 47%
Any infection grade ≥3 24% 22% Atrial fibrillation 5% 1%
Grade ≥3 AE atrial fibrillation 3% 0% Any hemorrhage 44% 12%
Major hemorrhage 1% 2%
Byrd et al. NEJM 2014

5-yearexperiencewithibruJnibinTNandR/R
O’Brien et al., ASH 2016 (abstract 233, oral presentation)
• Dose reductions and dose discontinuations due to AEs occurred more frequently in R/R patients than in TN patients, and during the first year after treatment compared with subsequent time periods.

Pooled analysis: Treatment-emergent AEs and laboratory abnormalities
AE,n(%)
Idelalisibmonotherapy(n=354) IdelalisibcombinaJontherapy(n=406)
Anygrade Grade≥3 Anygrade Grade≥3
Pyrexia 96(27) 7(2) 169(42) 47(12)Diarrhea/coli,s 131(37) 38(11) 161(40) 68(17)Fa,gue 112(32) 6(2) 130(32) 13(3)Nausea 91(26) 5(1) 125(31) 30(7)Cough 80(22) 3(1) 118(29) 21(5)Rash 60(17) 7(2) 99(24) 30(7)Chills 49(14) 0 86(21) 23(6)Pneumonia 47(13) 40(11) 74(18) 56(14)Cons,pa,on 39(11) 0 68(17) 1(<1)Dyspnea 43(12) 7(2) 68(17) 10(3)Abdominalpain 40(11) 4(1) 67(17) 5(1)Vomi,ng 53(15) 5(1) 60(15) 18(4)Decreasedappe,te 46(13) 8(2) 62(15) 2(<1)
Includespa,entsreceivingidelalisibinStudies101-02,101-07,101-08,101-09,101-10,101-11,101-99and312-0116
CoutréS, et al. EHA 2015, oral presentation #433;).
Laboratoryabnormality,n(%)
Idelalisibmonotherapy(n=354) IdelalisibcombinaJontherapy(n=406)
Anygrade Grade≥3 Anygrade Grade≥3
HematologicNeutropenia 162(46) 83(23) 234(58) 151(37)Anemia 102(29) 18(5) 145(36) 34(8)Thrombocytopenia 94(27) 37(11) 143(35) 50(12)
TransaminasesALT/ASTeleva,on 176(50) 56(16) 190(47) 53(13)
Ghia et al, EHA 2016, poster #226; Li et al, poster #594; Robak et al, poster #1063; Vinson et al, poster #1078

NumberofPaJents(%)a AnyGrade Grade3/4AnyAdverseEvent(AE) 115(99) 96(83)Diarrhea 60(52) 2(2)Upperrespiratorytractinfec,on 56(48) 1(1)
Nausea 55(47) 2(2)Neutropenia 52(45) 48(41)Fa,gue 46(40) 4(3)Cough 35(30) 0Pyrexia 30(26) 1(1)Anemia 29(25) 14(12)Headache 28(24) 1(1)Cons,pa,on 24(21) 1(1)Thrombocytopenia 24(21) 14(12)Arthralgia 21(18) 1(1)Vomi,ng 21(18) 2(2)Peripheraledema 18(16) 0Hyperglycemia 17(15) 10(9)
Roberts AW, NEJM 2016
NumberofPaJents(%)b TotalAnyseriousadverseevent(SAE) 52(45)Febrileneutropenia 7(6)Pneumonia 5(4)Upperrespiratorytractinfec,on 4(3)Immunethrombocytopenia 3(3)Tumorlysissyndrome 3(3)Diarrhea 2(2)Fluidoverload 2(2)Hyperglycemia 2(2)Prostatecancer 2(2)Pyrexia 2(2)a Listed are adverse events that were reported in ≥15% irrespective of cause. Pre-existing grade 1 or 2 laboratory abnormalities are not reported, unless the grade increased. b Serious adverse events (SAEs) occurring in at least 2 patients; excludes SAEs related to disease progression in 2 patients. AE, adverse event; SAE, serious adverse event; TLS, tumor lysis syndrome
– Clinical TLS was observed in 3 patients with high tumor burden who were treated with doses of ≥ 50 mg/day; 2 of these patients had severe sequelae
– Following data review, the expansion cohort was enrolled under a protocol that incorporated amended dosing, prophylaxis and monitoring for TLS
– No clinical events of TLS were seen after a change in the dosing and administration protocol
Davids et al, EHA 2016, poster #225
ABT-199 monotherapy phase 1 in CLL Adverse Events
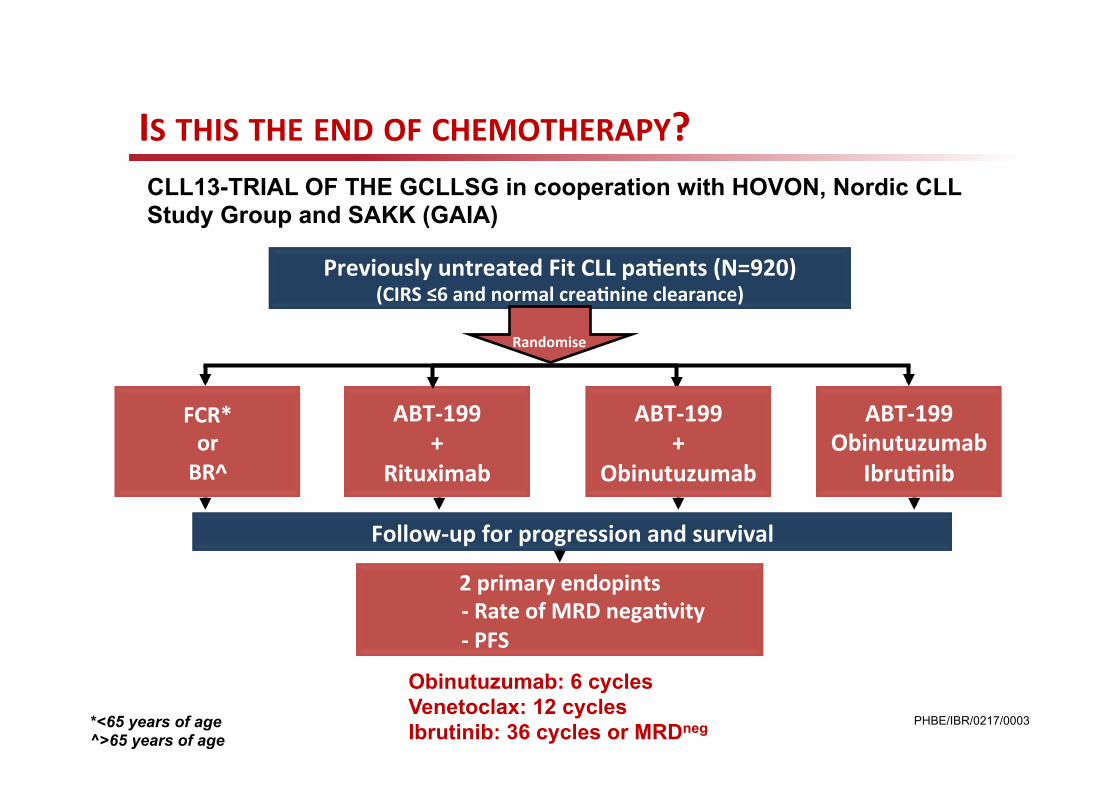
ISTHISTHEENDOFCHEMOTHERAPY?
PreviouslyuntreatedFitCLLpaJents(N=920)(CIRS≤6andnormalcreaJnineclearance)
FCR*orBR^
ABT-199+
Rituximab
Randomise
Follow-upforprogressionandsurvival
ABT-199+
Obinutuzumab
ABT-199Obinutuzumab
IbruJnib
2primaryendopints -RateofMRDnegaJvity -PFS
*<65 years of age ^>65 years of age
Obinutuzumab: 6 cycles Venetoclax: 12 cycles Ibrutinib: 36 cycles or MRDneg
CLL13-TRIAL OF THE GCLLSG in cooperation with HOVON, Nordic CLL Study Group and SAKK (GAIA)
PHBE/IBR/0217/0003

Laboratory of B Cell Neoplasia Lydia Scarfò, Andreas Agathangelidis, Maria Gounari,
Alessandra Rovida, Tania Veliz-Rodriguez, Engin Bojnik, Pamela Ranghetti, Federica Barbaglio, Cristina Scielzo
Laboratory of Lymphocyte Activation Eleonora Maria Fonte, Maria Giovanna Vilia,
Marta Muzio
Strategic Research Program on CLL Lydia Scarfò, Piera Angelillo, Maria Colia,
Virginia Sgarlato, Stefania Cresta, Eloise Scarano
Università Vita-Salute San Raffaele Istituto Scientifico San Raffaele
Department of Onco-Hematology Division of Experimental Oncology
CERTH, Thessaloniki Anna Vardi, Stavroula Ntoufa,
Aliki Xochelli, Anastasia Hadzidimitrious,
Kostas Stamatopoulos
Uppsala University, Uppsala Lesley Ann Sutton, Panayotis
Baliakas, Viktor Ljungstrom, Richard Roseqnuist
©Janssen-CilagN
V-PHBE/IBR/0217/0003vu/erErikPresent,Antw
erpseweg15-17,2340Beerse”