Nuove evidenze sulla terapia antitrombotica cronica nella ... · Nuove evidenze sulla terapia...
46
Nuove evidenze sulla terapia antitrombotica cronica nella CAD e PAD Dott. Marco Marini SOD Cardiologia-Emodinamica-UTIC AOU Ospedali Riuniti di Ancona
Transcript of Nuove evidenze sulla terapia antitrombotica cronica nella ... · Nuove evidenze sulla terapia...
Nuove evidenze sulla terapia antitrombotica
cronica nella CAD e PAD
Dott. Marco Marini
SOD Cardiologia-Emodinamica-UTIC
AOU Ospedali Riuniti di Ancona
Nuove evidenze sulla terapia antitrombotica
cronica nella CAD e PAD
Qual’è la percentuale di rischio residuo di
eventi aterotrombotici in pazienti con
CAD e PAD?
< 5%
5-10%
>10%
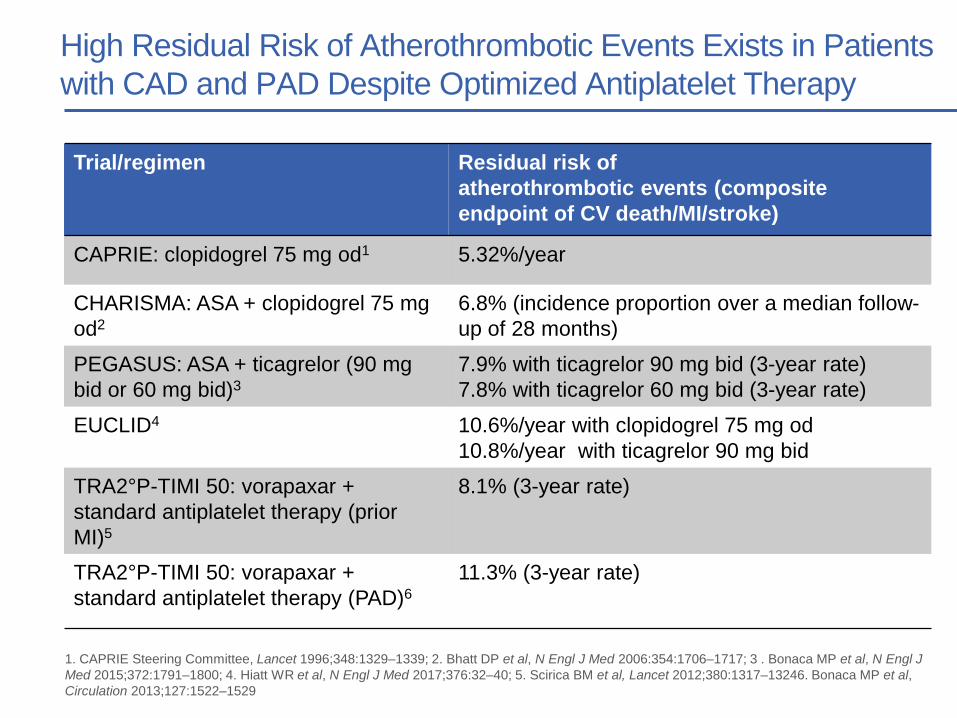
High Residual Risk of Atherothrombotic Events Exists in Patients
with CAD and PAD Despite Optimized Antiplatelet Therapy
Trial/regimen Residual risk of
atherothrombotic events (composite
endpoint of CV death/MI/stroke)
CAPRIE: clopidogrel 75 mg od1 5.32%/year
CHARISMA: ASA + clopidogrel 75 mg
od2
6.8% (incidence proportion over a median follow-
up of 28 months)
PEGASUS: ASA + ticagrelor (90 mg
bid or 60 mg bid)3
7.9% with ticagrelor 90 mg bid (3-year rate)
7.8% with ticagrelor 60 mg bid (3-year rate)
EUCLID4 10.6%/year with clopidogrel 75 mg od
10.8%/year with ticagrelor 90 mg bid
TRA2°P-TIMI 50: vorapaxar +
standard antiplatelet therapy (prior
MI)5
8.1% (3-year rate)
TRA2°P-TIMI 50: vorapaxar +
standard antiplatelet therapy (PAD)6
11.3% (3-year rate)
1. CAPRIE Steering Committee, Lancet 1996;348:1329–1339; 2. Bhatt DP et al, N Engl J Med 2006:354:1706–1717; 3 . Bonaca MP et al, N Engl J
Med 2015;372:1791–1800; 4. Hiatt WR et al, N Engl J Med 2017;376:32–40; 5. Scirica BM et al, Lancet 2012;380:1317–13246. Bonaca MP et al,
Circulation 2013;127:1522–1529
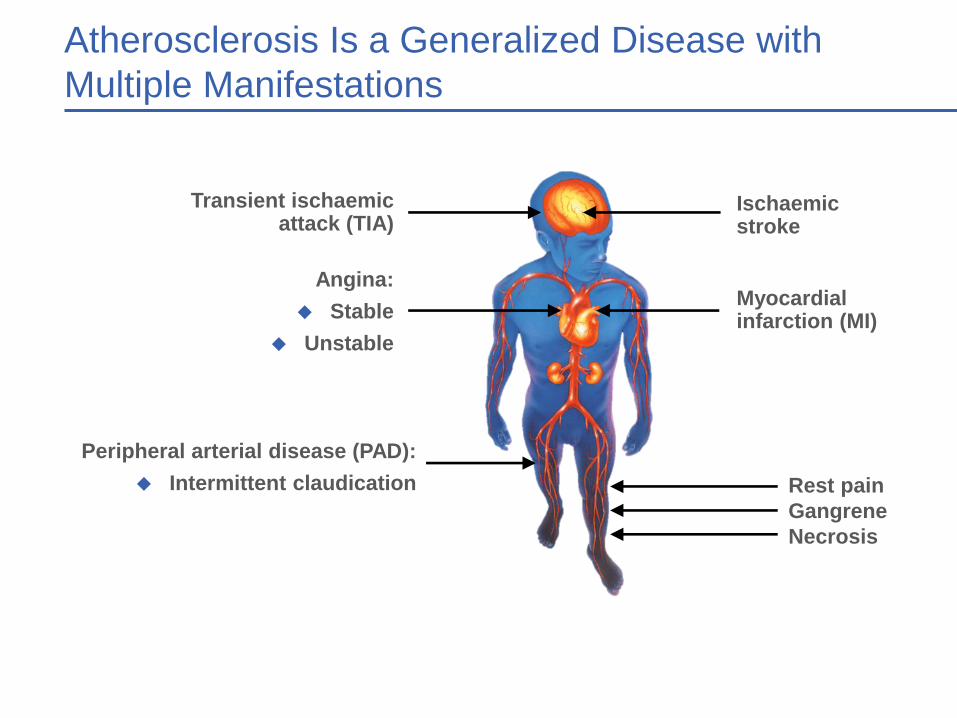
Atherosclerosis Is a Generalized Disease with
Multiple Manifestations
Ischaemic stroke
Myocardial infarction (MI)
Transient ischaemic attack (TIA)
Angina:
Stable
Unstable
Peripheral arterial disease (PAD):
Intermittent claudication Rest pain
Gangrene
Necrosis
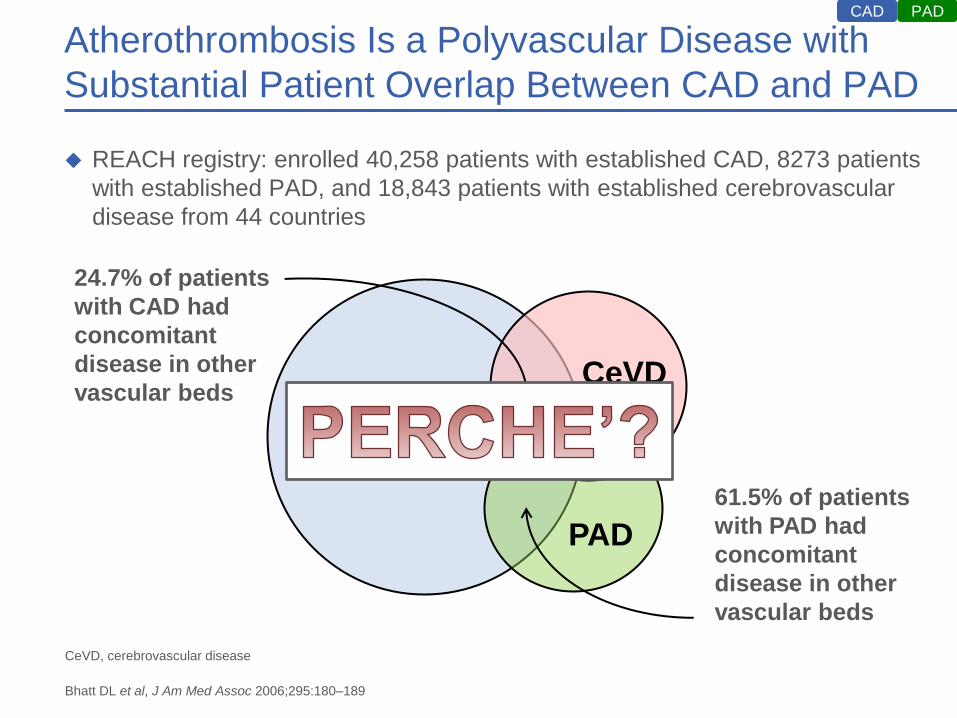
Atherothrombosis Is a Polyvascular Disease with
Substantial Patient Overlap Between CAD and PAD
REACH registry: enrolled 40,258 patients with established CAD, 8273 patients
with established PAD, and 18,843 patients with established cerebrovascular
disease from 44 countries
PAD CAD
CeVD, cerebrovascular disease
Bhatt DL et al, J Am Med Assoc 2006;295:180–189
CAD
PAD
CeVD
61.5% of patients
with PAD had
concomitant
disease in other
vascular beds
24.7% of patients
with CAD had
concomitant
disease in other
vascular beds
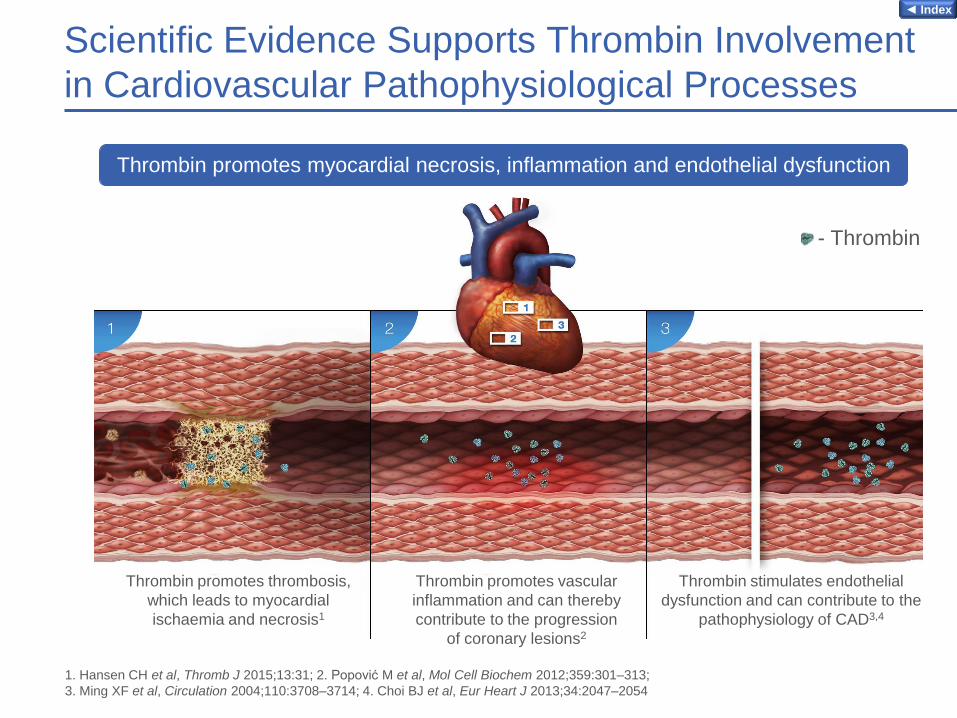
Scientific Evidence Supports Thrombin Involvement
in Cardiovascular Pathophysiological Processes
Thrombin promotes myocardial necrosis, inflammation and endothelial dysfunction
Thrombin promotes thrombosis,
which leads to myocardial
ischaemia and necrosis1
Thrombin promotes vascular
inflammation and can thereby
contribute to the progression
of coronary lesions2
Thrombin stimulates endothelial
dysfunction and can contribute to the
pathophysiology of CAD3,4
- Thrombin
1. Hansen CH et al, Thromb J 2015;13:31; 2. Popović M et al, Mol Cell Biochem 2012;359:301–313;
3. Ming XF et al, Circulation 2004;110:3708–3714; 4. Choi BJ et al, Eur Heart J 2013;34:2047–2054
◄ Index

Both Fibrin and Platelets Are Present in Thrombi
from Patients with Myocardial Infarction
Immunofluorescent micrographs of aspirated thrombi from patients
with acute MI show of GPIIb/IIIa (marker for platelets) and fibrin
Platelets Fibrin Platelets and fibrin
GP, glycoprotein
Yamashita A et al, Am J Cardiol 2006;97:26–28
GPIIb/IIIa
CAD
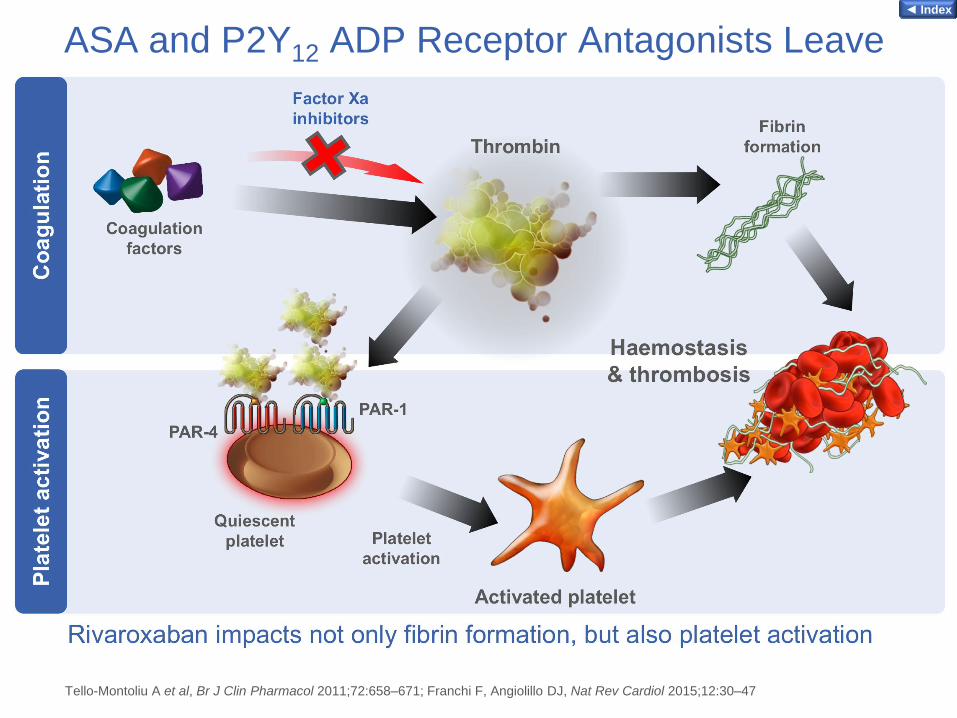
ASA and P2Y12 ADP Receptor Antagonists Leave
Thrombin-Mediated Pathways in Platelets Uninhibited
Tello-Montoliu A et al, Br J Clin Pharmacol 2011;72:658–671; Franchi F, Angiolillo DJ, Nat Rev Cardiol 2015;12:30–47
◄ Index
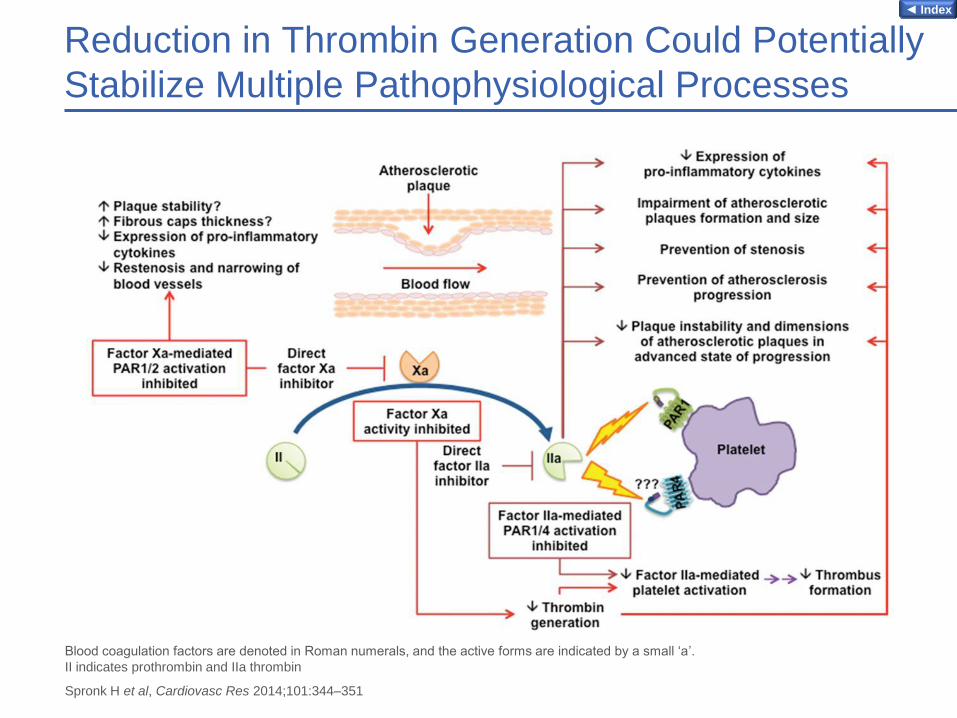
Reduction in Thrombin Generation Could Potentially
Stabilize Multiple Pathophysiological Processes
Blood coagulation factors are denoted in Roman numerals, and the active forms are indicated by a small ‘a’.
II indicates prothrombin and IIa thrombin
Spronk H et al, Cardiovasc Res 2014;101:344–351
◄ Index
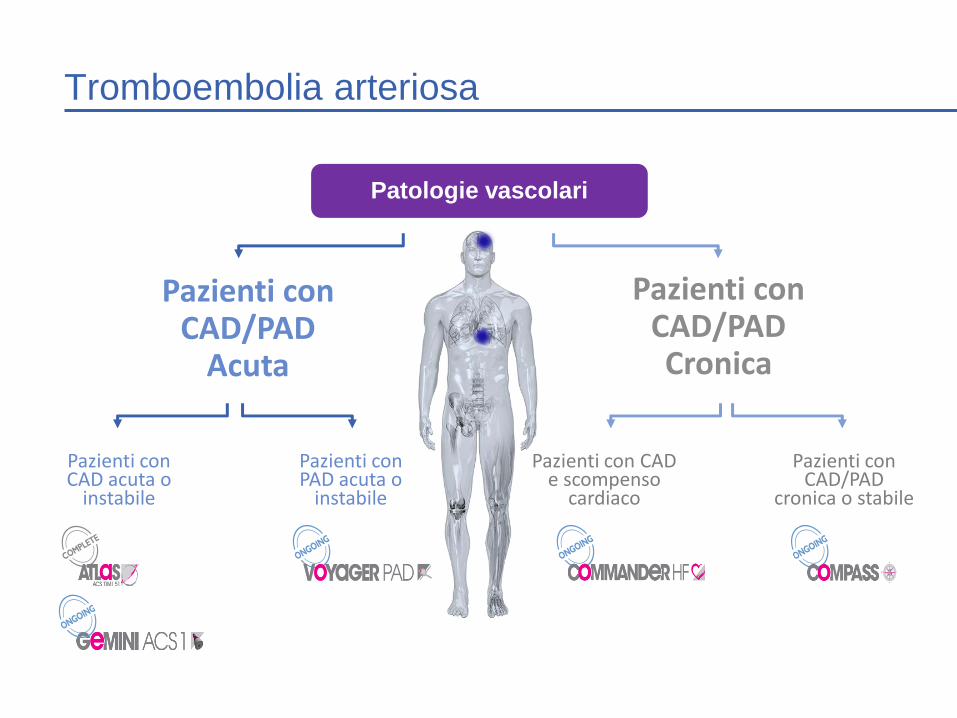
Tromboembolia arteriosa
Pazienti con CAD/PAD
Acuta
Pazienti con CAD acuta o
instabile
Pazienti con CAD e scompenso
cardiaco
Pazienti con CAD/PAD Cronica
Patologie vascolari
Pazienti con PAD acuta o
instabile
Pazienti con CAD/PAD
cronica o stabile
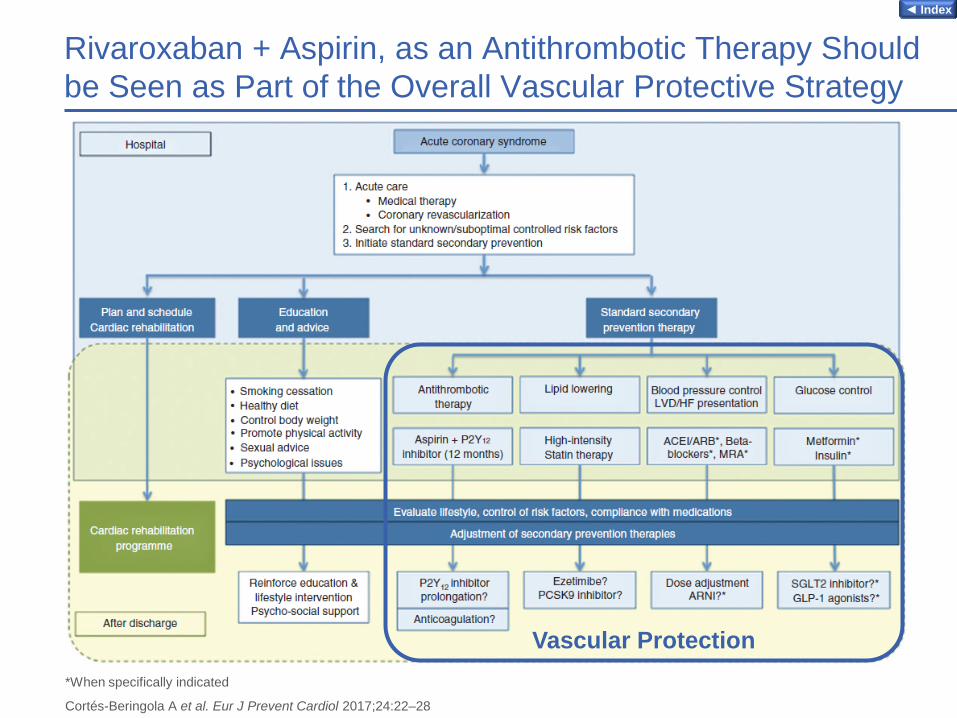
Rivaroxaban + Aspirin, as an Antithrombotic Therapy Should
be Seen as Part of the Overall Vascular Protective Strategy
*When specifically indicated
Cortés-Beringola A et al. Eur J Prevent Cardiol 2017;24:22–28
Vascular Protection
◄ Index
Cosa ha ridotto nei pazienti con PAD la
terapia antiaggregante?
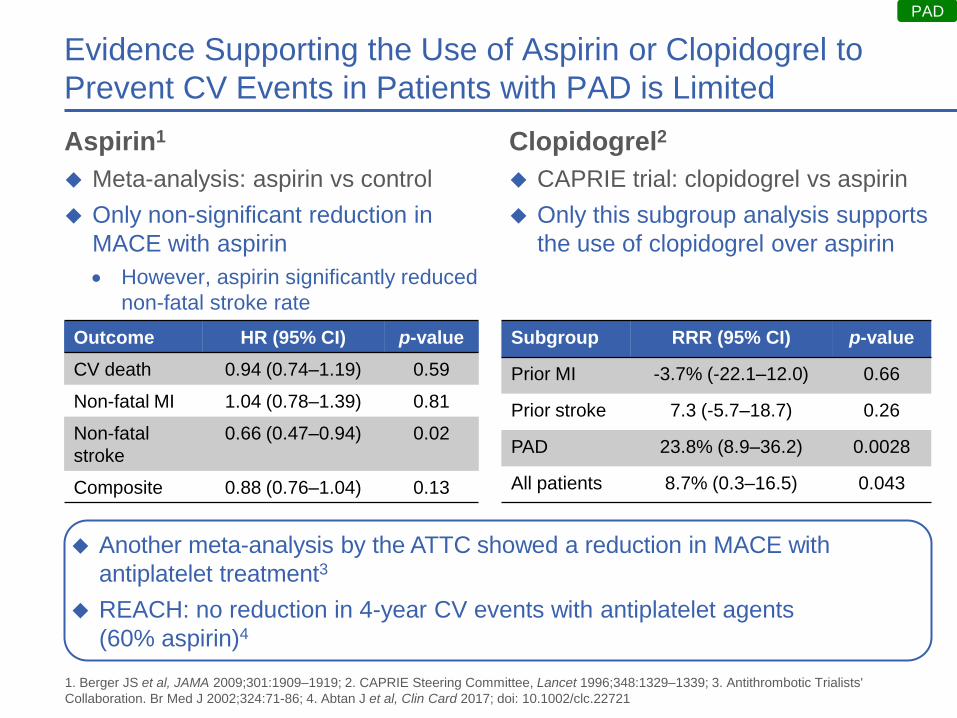
Evidence Supporting the Use of Aspirin or Clopidogrel to
Prevent CV Events in Patients with PAD is Limited
Aspirin1
Meta-analysis: aspirin vs control
Only non-significant reduction in
MACE with aspirin
However, aspirin significantly reduced
non-fatal stroke rate
Clopidogrel2
CAPRIE trial: clopidogrel vs aspirin
Only this subgroup analysis supports
the use of clopidogrel over aspirin
Outcome HR (95% CI) p-value
CV death 0.94 (0.74–1.19) 0.59
Non-fatal MI 1.04 (0.78–1.39) 0.81
Non-fatal
stroke
0.66 (0.47–0.94) 0.02
Composite 0.88 (0.76–1.04) 0.13
Subgroup RRR (95% CI) p-value
Prior MI -3.7% (-22.1–12.0) 0.66
Prior stroke 7.3 (-5.7–18.7) 0.26
PAD 23.8% (8.9–36.2) 0.0028
All patients 8.7% (0.3–16.5) 0.043
Another meta-analysis by the ATTC showed a reduction in MACE with
antiplatelet treatment3
REACH: no reduction in 4-year CV events with antiplatelet agents
(60% aspirin)4
PAD
1. Berger JS et al, JAMA 2009;301:1909–1919; 2. CAPRIE Steering Committee, Lancet 1996;348:1329–1339; 3. Antithrombotic Trialists'
Collaboration. Br Med J 2002;324:71-86; 4. Abtan J et al, Clin Card 2017; doi: 10.1002/clc.22721
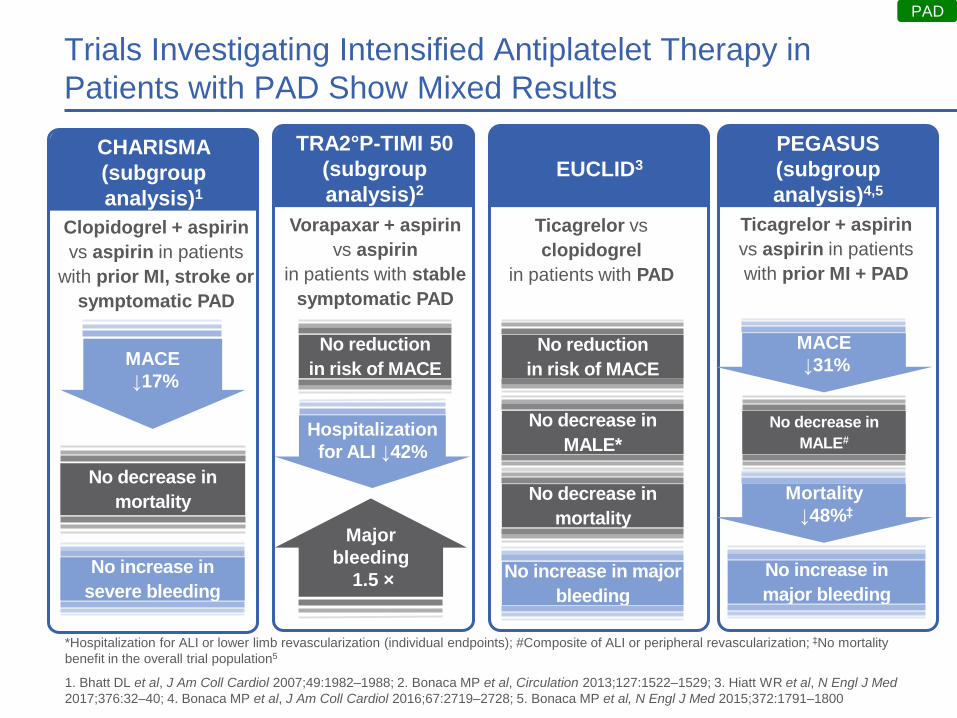
Trials Investigating Intensified Antiplatelet Therapy in
Patients with PAD Show Mixed Results
*Hospitalization for ALI or lower limb revascularization (individual endpoints); #Composite of ALI or peripheral revascularization; ‡No mortality
benefit in the overall trial population5
1. Bhatt DL et al, J Am Coll Cardiol 2007;49:1982–1988; 2. Bonaca MP et al, Circulation 2013;127:1522–1529; 3. Hiatt WR et al, N Engl J Med
2017;376:32–40; 4. Bonaca MP et al, J Am Coll Cardiol 2016;67:2719–2728; 5. Bonaca MP et al, N Engl J Med 2015;372:1791–1800
Clopidogrel + aspirin
vs aspirin in patients
with prior MI, stroke or
symptomatic PAD
CHARISMA
(subgroup
analysis)1
No increase in
severe bleeding
No decrease in
mortality
Ticagrelor vs
clopidogrel
in patients with PAD
EUCLID3
No reduction
in risk of MACE
No increase in major
bleeding
PAD
MACE
↓17%
Vorapaxar + aspirin
vs aspirin
in patients with stable
symptomatic PAD
TRA2°P-TIMI 50
(subgroup
analysis)2
Major
bleeding
1.5 ×
No reduction
in risk of MACE
Hospitalization
for ALI ↓42%
No decrease in
MALE*
No decrease in
mortality
Ticagrelor + aspirin
vs aspirin in patients
with prior MI + PAD
PEGASUS
(subgroup
analysis)4,5
No increase in
major bleeding
No decrease in
MALE#
MACE
↓31%
Mortality
↓48%‡
Current recommendations and unmet needs
Current Management of PAD
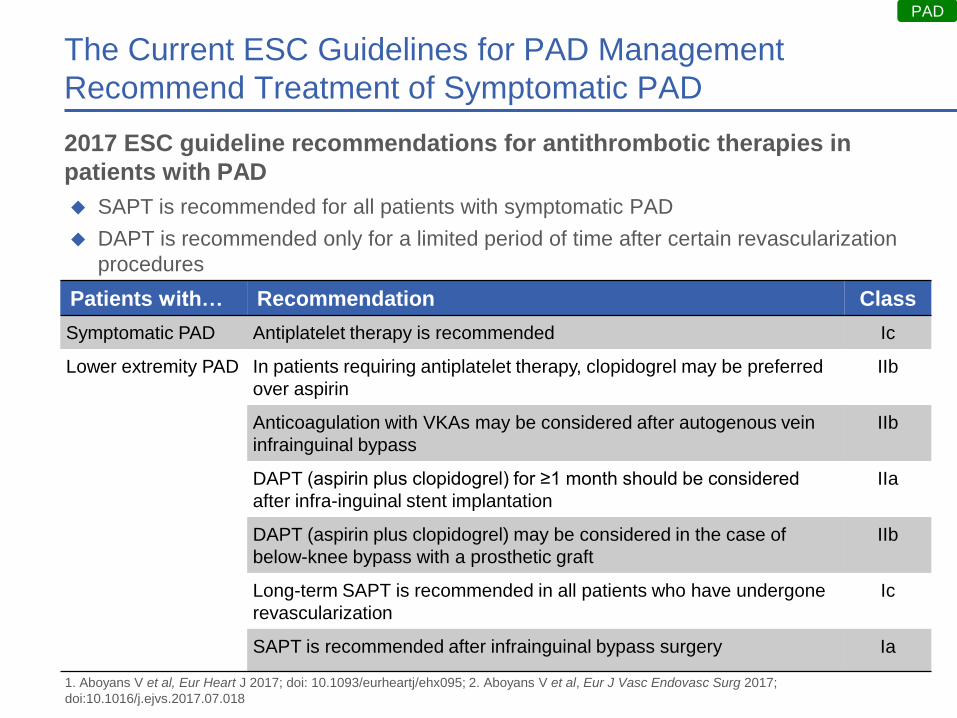
The Current ESC Guidelines for PAD Management
Recommend Treatment of Symptomatic PAD
PAD
Patients with… Recommendation Class
Symptomatic PAD Antiplatelet therapy is recommended Ic
Lower extremity PAD In patients requiring antiplatelet therapy, clopidogrel may be preferred
over aspirin
IIb
Anticoagulation with VKAs may be considered after autogenous vein
infrainguinal bypass
IIb
DAPT (aspirin plus clopidogrel) for ≥1 month should be considered
after infra-inguinal stent implantation
IIa
DAPT (aspirin plus clopidogrel) may be considered in the case of
below-knee bypass with a prosthetic graft
IIb
Long-term SAPT is recommended in all patients who have undergone
revascularization
Ic
SAPT is recommended after infrainguinal bypass surgery Ia
1. Aboyans V et al, Eur Heart J 2017; doi: 10.1093/eurheartj/ehx095; 2. Aboyans V et al, Eur J Vasc Endovasc Surg 2017;
doi:10.1016/j.ejvs.2017.07.018
SAPT is recommended for all patients with symptomatic PAD
DAPT is recommended only for a limited period of time after certain revascularization
procedures
2017 ESC guideline recommendations for antithrombotic therapies in
patients with PAD
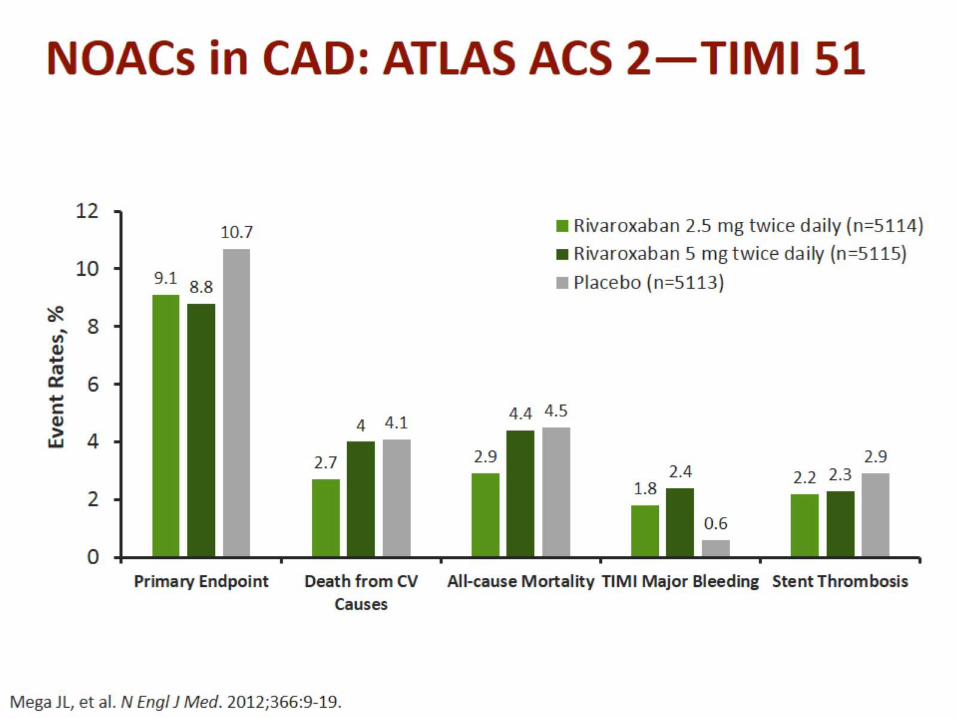
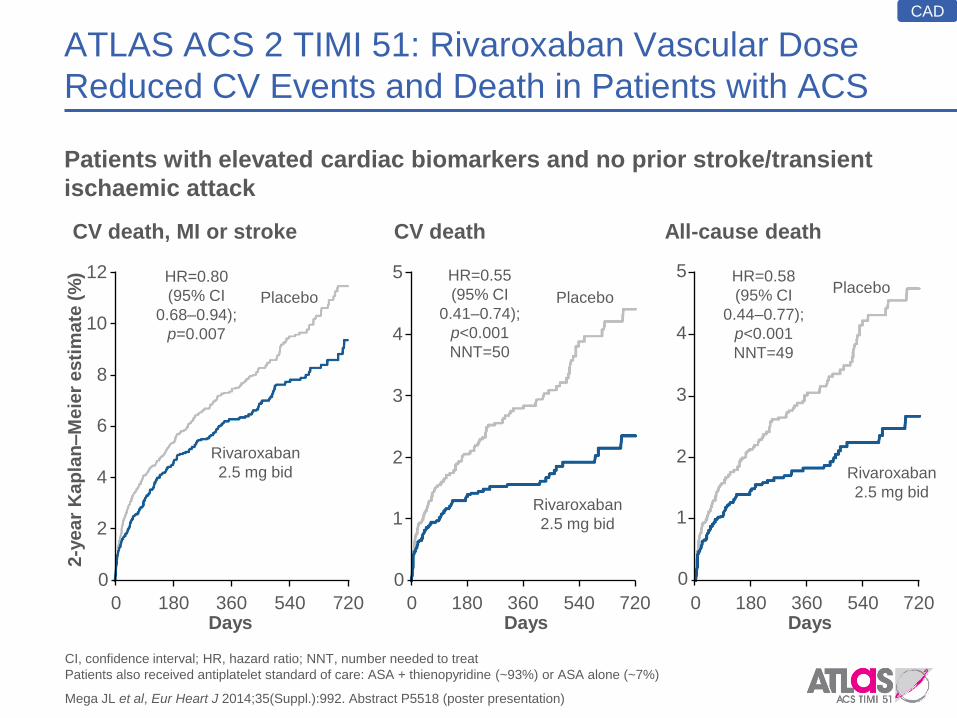
ATLAS ACS 2 TIMI 51: Rivaroxaban Vascular Dose
Reduced CV Events and Death in Patients with ACS
Patients with elevated cardiac biomarkers and no prior stroke/transient
ischaemic attack
CAD
CV death, MI or stroke
12
Days
2-y
ea
r K
ap
lan–M
eie
r e
sti
ma
te (
%) HR=0.80
(95% CI
0.68–0.94);
p=0.007
Rivaroxaban
2.5 mg bid
Placebo
0
720 0 540 360 180
10
8
6
4
2
CV death
0
5
Days
HR=0.55
(95% CI
0.41–0.74);
p<0.001
NNT=50
Rivaroxaban
2.5 mg bid
Placebo
720 0 540 360 180
4
3
2
1
All-cause death
5
Days
HR=0.58
(95% CI
0.44–0.77);
p<0.001
NNT=49
Rivaroxaban
2.5 mg bid
Placebo
0
720 0 540 360 180
4
3
2
1
CI, confidence interval; HR, hazard ratio; NNT, number needed to treat
Patients also received antiplatelet standard of care: ASA + thienopyridine (~93%) or ASA alone (~7%)
Mega JL et al, Eur Heart J 2014;35(Suppl.):992. Abstract P5518 (poster presentation)
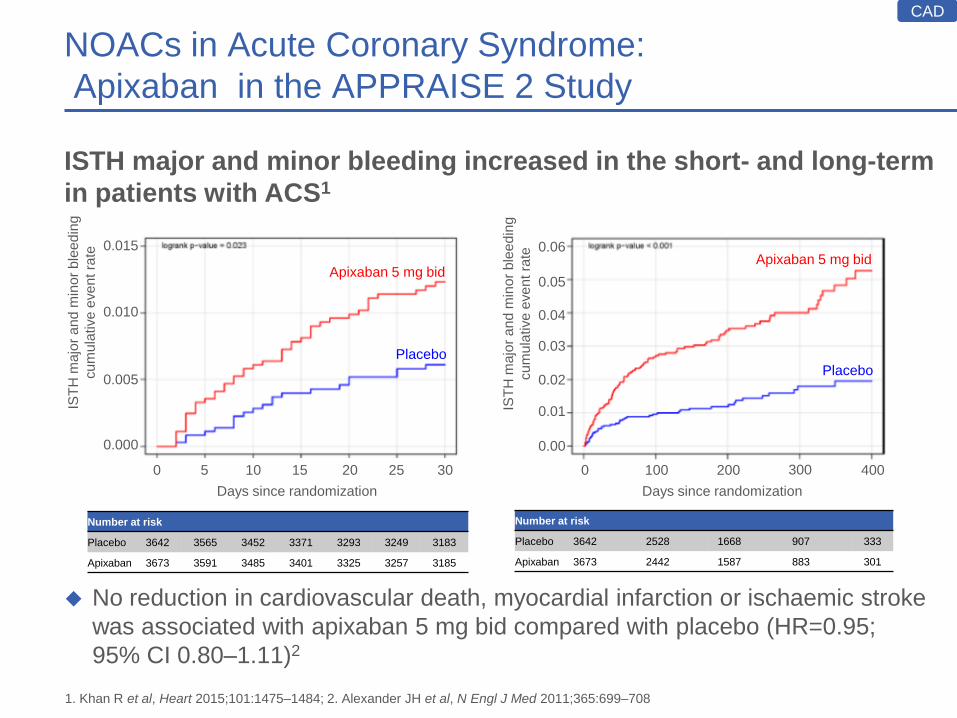
ISTH major and minor bleeding increased in the short- and long-term
in patients with ACS1
No reduction in cardiovascular death, myocardial infarction or ischaemic stroke
was associated with apixaban 5 mg bid compared with placebo (HR=0.95;
95% CI 0.80–1.11)2
NOACs in Acute Coronary Syndrome:
Apixaban in the APPRAISE 2 Study
1. Khan R et al, Heart 2015;101:1475–1484; 2. Alexander JH et al, N Engl J Med 2011;365:699–708
Number at risk
Placebo 3642 3565 3452 3371 3293 3249 3183
Apixaban 3673 3591 3485 3401 3325 3257 3185
0 5 10 15 20 25 30
IST
H m
ajo
r a
nd
min
or
ble
ed
ing
cu
mu
lative
eve
nt ra
te
0.000
0.005
0.010
0.015
Days since randomization
Apixaban 5 mg bid
Placebo
0 100 200 300 400
Number at risk
Placebo 3642 2528 1668 907 333
Apixaban 3673 2442 1587 883 301
Days since randomization
IST
H m
ajo
r a
nd
min
or
ble
ed
ing
cu
mu
lative
eve
nt ra
te
0.00
0.01
0.02
0.03
0.04
0.05
0.06 Apixaban 5 mg bid
Placebo
CAD
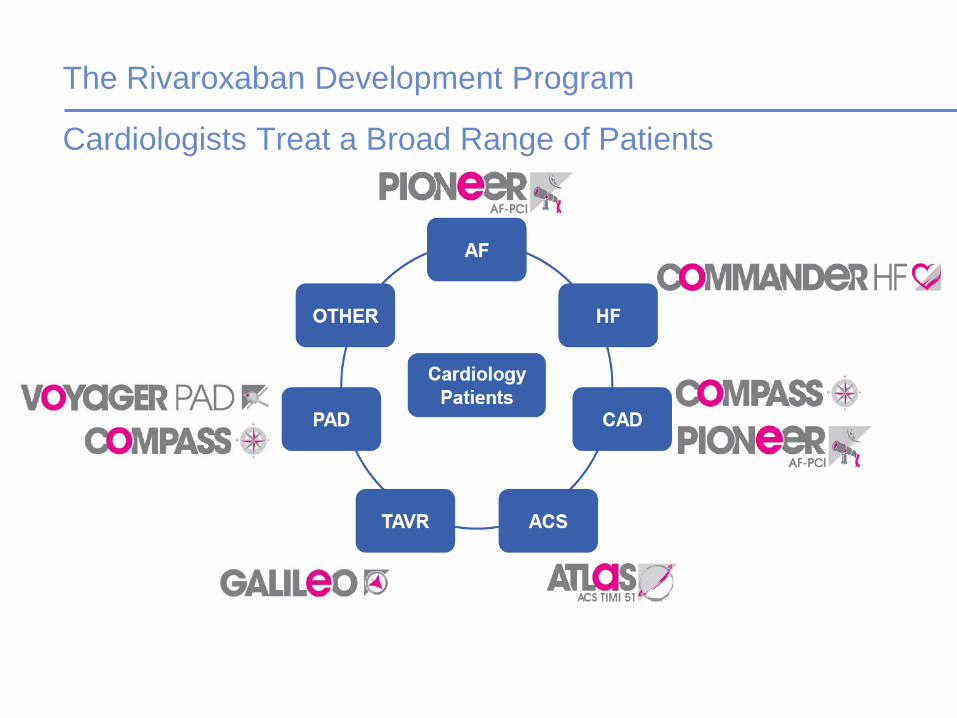
The Rivaroxaban Development Program
Cardiologists Treat a Broad Range of Patients
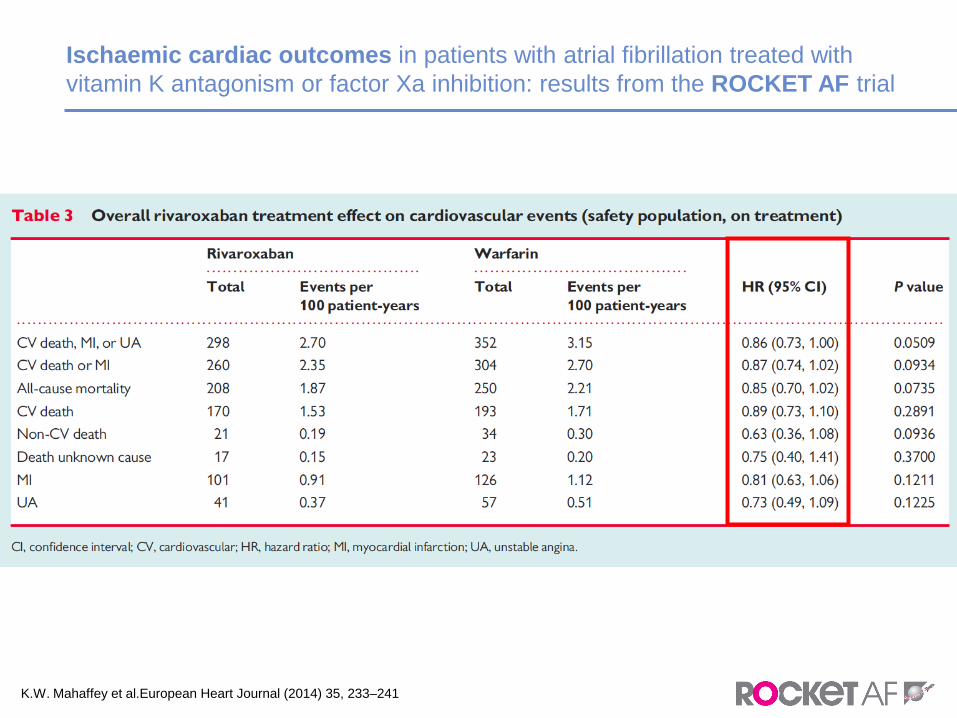
Ischaemic cardiac outcomes in patients with atrial fibrillation treated with
vitamin K antagonism or factor Xa inhibition: results from the ROCKET AF trial
K.W. Mahaffey et al.European Heart Journal (2014) 35, 233–241
…l’intuizione ed il coraggio di guardare oltre..
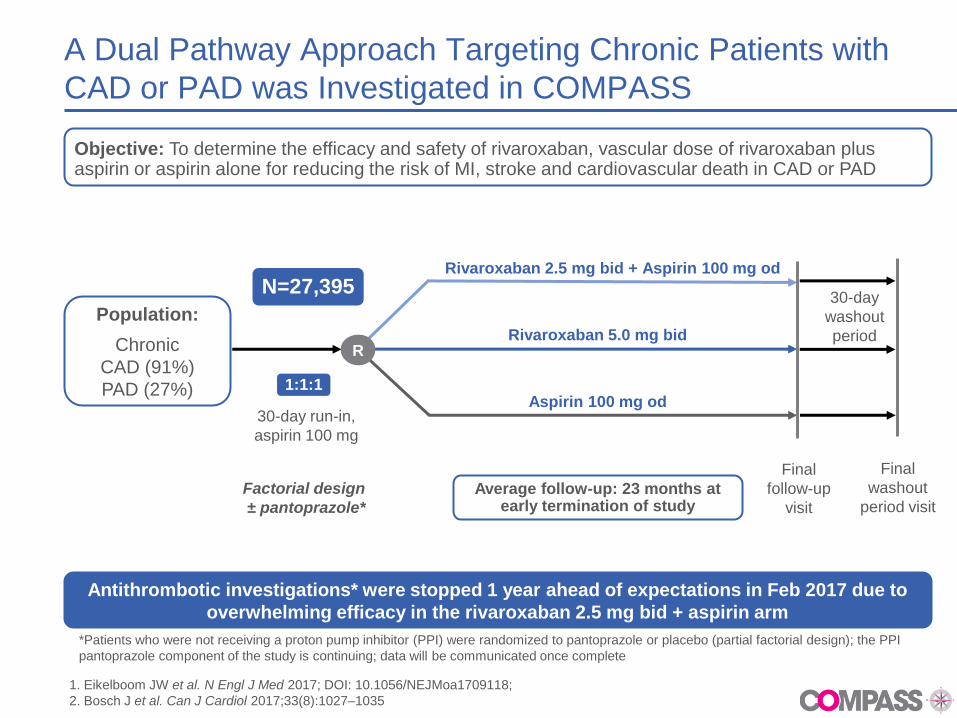
A Dual Pathway Approach Targeting Chronic Patients with
CAD or PAD was Investigated in COMPASS
Objective: To determine the efficacy and safety of rivaroxaban, vascular dose of rivaroxaban plus aspirin or aspirin alone for reducing the risk of MI, stroke and cardiovascular death in CAD or PAD
Antithrombotic investigations* were stopped 1 year ahead of expectations in Feb 2017 due to
overwhelming efficacy in the rivaroxaban 2.5 mg bid + aspirin arm
Rivaroxaban 5.0 mg bid
Aspirin 100 mg od
Rivaroxaban 2.5 mg bid + Aspirin 100 mg od
30-day
washout
period
30-day run-in,
aspirin 100 mg
Final
follow-up
visit
R
Final
washout
period visit
1:1:1
N=27,395
Population:
Chronic
CAD (91%)
PAD (27%)
*Patients who were not receiving a proton pump inhibitor (PPI) were randomized to pantoprazole or placebo (partial factorial design); the PPI
pantoprazole component of the study is continuing; data will be communicated once complete
1. Eikelboom JW et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1709118;
2. Bosch J et al. Can J Cardiol 2017;33(8):1027–1035
Average follow-up: 23 months at early termination of study
Factorial design
± pantoprazole*
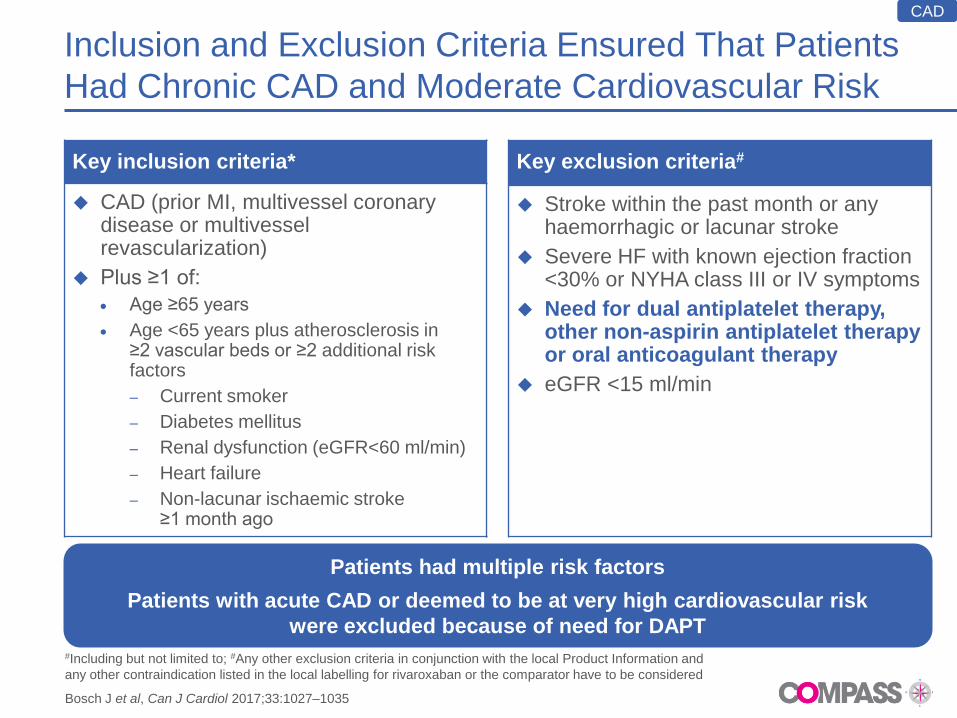
Inclusion and Exclusion Criteria Ensured That Patients
Had Chronic CAD and Moderate Cardiovascular Risk
Key inclusion criteria*
CAD (prior MI, multivessel coronary disease or multivessel revascularization)
Plus ≥1 of:
Age ≥65 years
Age <65 years plus atherosclerosis in ≥2 vascular beds or ≥2 additional risk factors
– Current smoker
– Diabetes mellitus
– Renal dysfunction (eGFR<60 ml/min)
– Heart failure
– Non-lacunar ischaemic stroke ≥1 month ago
Key exclusion criteria#
Stroke within the past month or any haemorrhagic or lacunar stroke
Severe HF with known ejection fraction <30% or NYHA class III or IV symptoms
Need for dual antiplatelet therapy, other non-aspirin antiplatelet therapy or oral anticoagulant therapy
eGFR <15 ml/min
#Including but not limited to; #Any other exclusion criteria in conjunction with the local Product Information and
any other contraindication listed in the local labelling for rivaroxaban or the comparator have to be considered
Bosch J et al, Can J Cardiol 2017;33:1027–1035
Patients had multiple risk factors
Patients with acute CAD or deemed to be at very high cardiovascular risk
were excluded because of need for DAPT
CAD
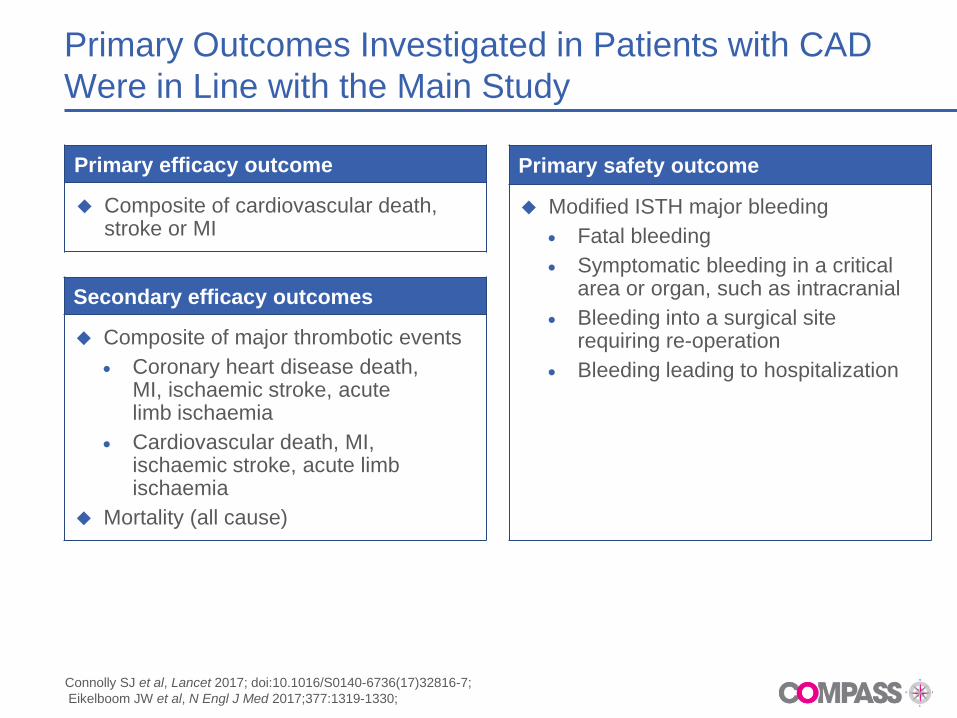
Primary Outcomes Investigated in Patients with CAD
Were in Line with the Main Study
Primary efficacy outcome
Composite of cardiovascular death, stroke or MI
Primary safety outcome
Modified ISTH major bleeding
Fatal bleeding
Symptomatic bleeding in a critical area or organ, such as intracranial
Bleeding into a surgical site requiring re-operation
Bleeding leading to hospitalization
Secondary efficacy outcomes
Composite of major thrombotic events
Coronary heart disease death, MI, ischaemic stroke, acute limb ischaemia
Cardiovascular death, MI, ischaemic stroke, acute limb ischaemia
Mortality (all cause)
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7;
Eikelboom JW et al, N Engl J Med 2017;377:1319-1330;
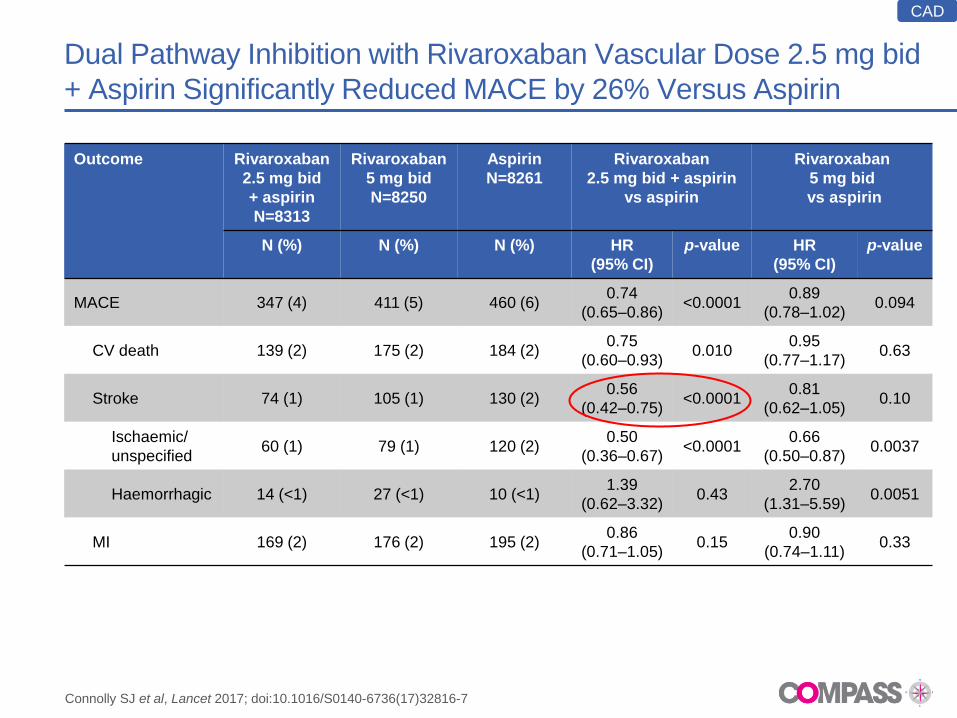
Dual Pathway Inhibition with Rivaroxaban Vascular Dose 2.5 mg bid
+ Aspirin Significantly Reduced MACE by 26% Versus Aspirin
Outcome Rivaroxaban
2.5 mg bid
+ aspirin
N=8313
Rivaroxaban
5 mg bid
N=8250
Aspirin
N=8261
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI)
p-value HR
(95% CI)
p-value
MACE 347 (4) 411 (5) 460 (6) 0.74
(0.65–0.86) <0.0001
0.89
(0.78–1.02) 0.094
CV death 139 (2) 175 (2) 184 (2) 0.75
(0.60–0.93) 0.010
0.95
(0.77–1.17) 0.63
Stroke 74 (1) 105 (1) 130 (2) 0.56
(0.42–0.75) <0.0001
0.81
(0.62–1.05) 0.10
Ischaemic/
unspecified 60 (1) 79 (1) 120 (2)
0.50
(0.36–0.67) <0.0001
0.66
(0.50–0.87) 0.0037
Haemorrhagic 14 (<1) 27 (<1) 10 (<1) 1.39
(0.62–3.32) 0.43
2.70
(1.31–5.59) 0.0051
MI 169 (2) 176 (2) 195 (2) 0.86
(0.71–1.05) 0.15
0.90
(0.74–1.11) 0.33
CAD
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
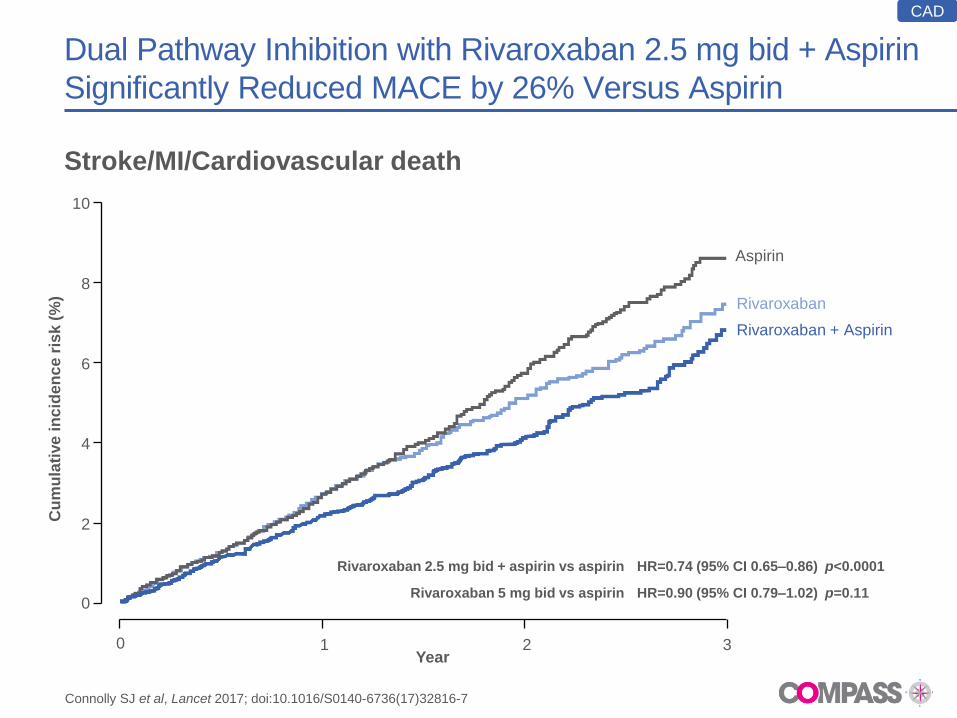
Dual Pathway Inhibition with Rivaroxaban 2.5 mg bid + Aspirin
Significantly Reduced MACE by 26% Versus Aspirin
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
Stroke/MI/Cardiovascular death
Cu
mu
lati
ve
in
cid
en
ce
ris
k (
%)
0
2
4
6
8
10
0 1 2 3
Rivaroxaban + Aspirin
Rivaroxaban
Aspirin
Year
Rivaroxaban 2.5 mg bid + aspirin vs aspirin
Rivaroxaban 5 mg bid vs aspirin
HR=0.74 (95% CI 0.65–0.86) p<0.0001
HR=0.90 (95% CI 0.79–1.02) p=0.11
CAD
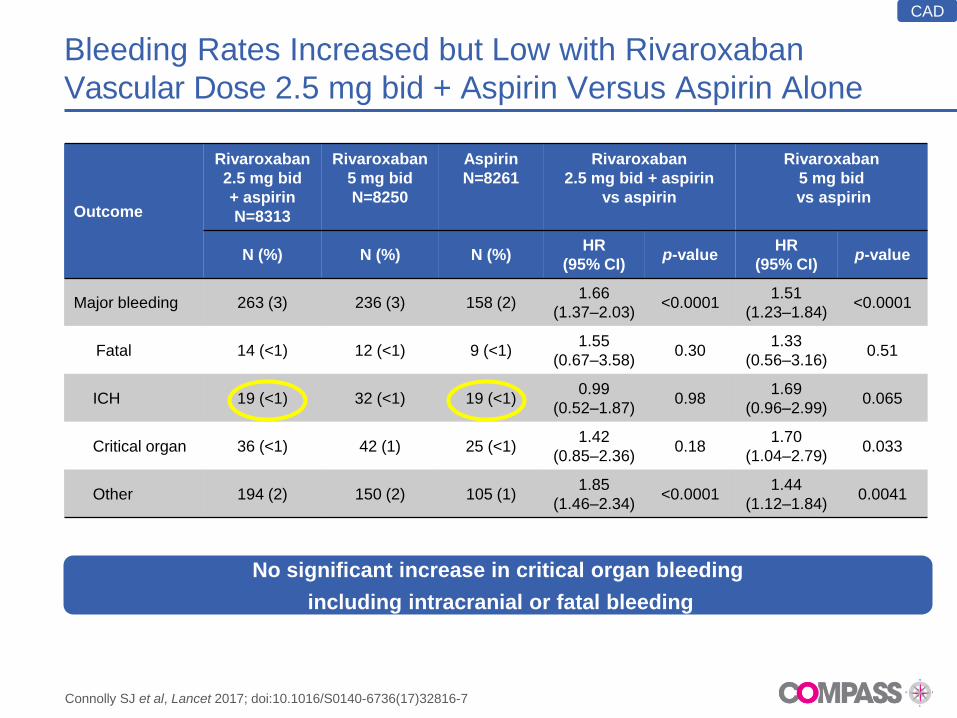
Bleeding Rates Increased but Low with Rivaroxaban
Vascular Dose 2.5 mg bid + Aspirin Versus Aspirin Alone
Outcome
Rivaroxaban
2.5 mg bid
+ aspirin
N=8313
Rivaroxaban
5 mg bid
N=8250
Aspirin
N=8261
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI) p-value
HR
(95% CI) p-value
Major bleeding 263 (3) 236 (3) 158 (2) 1.66
(1.37–2.03) <0.0001
1.51
(1.23–1.84) <0.0001
Fatal 14 (<1) 12 (<1) 9 (<1) 1.55
(0.67–3.58) 0.30
1.33
(0.56–3.16) 0.51
ICH 19 (<1) 32 (<1) 19 (<1) 0.99
(0.52–1.87) 0.98
1.69
(0.96–2.99) 0.065
Critical organ 36 (<1) 42 (1) 25 (<1) 1.42
(0.85–2.36) 0.18
1.70
(1.04–2.79) 0.033
Other 194 (2) 150 (2) 105 (1) 1.85
(1.46–2.34) <0.0001
1.44
(1.12–1.84) 0.0041
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
CAD
No significant increase in critical organ bleeding
including intracranial or fatal bleeding
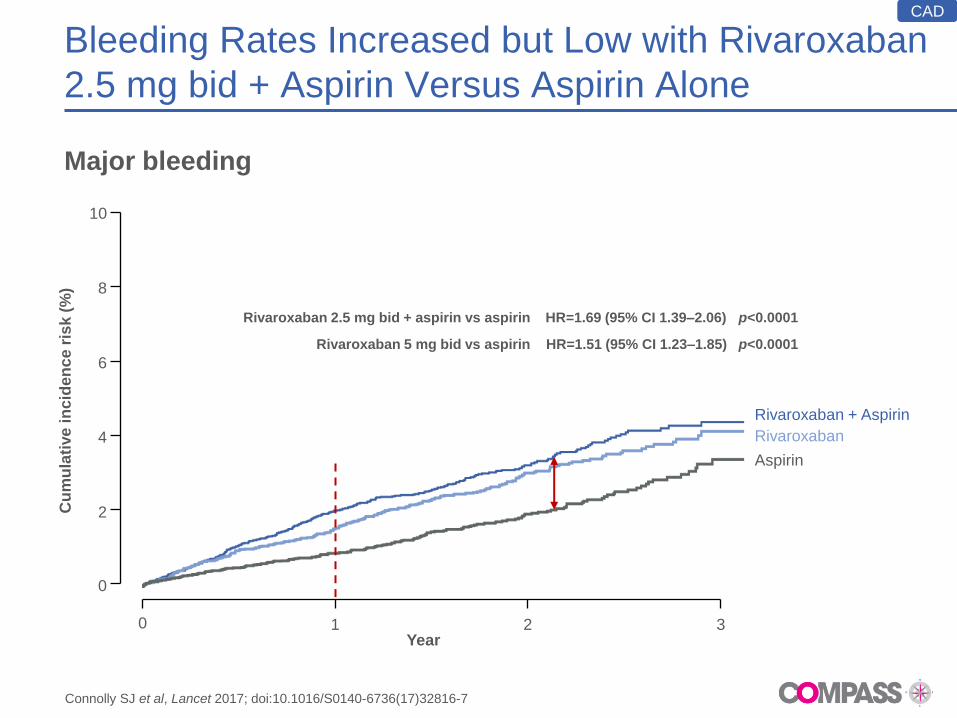
Bleeding Rates Increased but Low with Rivaroxaban
2.5 mg bid + Aspirin Versus Aspirin Alone
Major bleeding
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
CAD
Aspirin
Rivaroxaban
Rivaroxaban + Aspirin
Year
Rivaroxaban 2.5 mg bid + aspirin vs aspirin
Rivaroxaban 5 mg bid vs aspirin
HR=1.69 (95% CI 1.39–2.06) p<0.0001
HR=1.51 (95% CI 1.23–1.85) p<0.0001
Cu
mu
lati
ve
in
cid
en
ce
ris
k (
%)
0
2
4
6
8
10
0 1 2 3
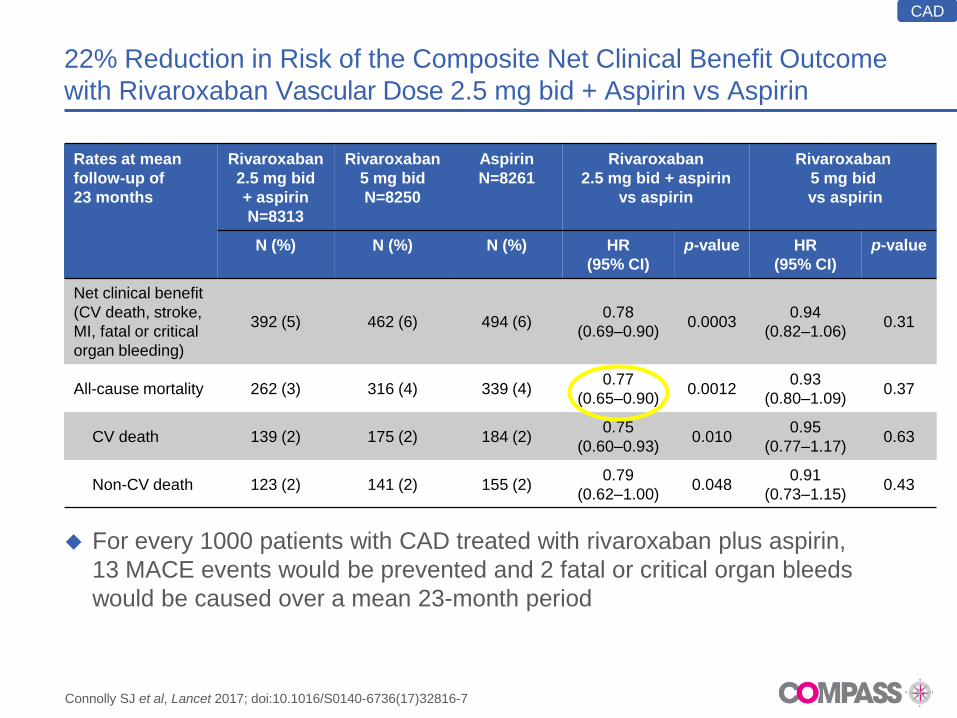
22% Reduction in Risk of the Composite Net Clinical Benefit Outcome
with Rivaroxaban Vascular Dose 2.5 mg bid + Aspirin vs Aspirin
For every 1000 patients with CAD treated with rivaroxaban plus aspirin,
13 MACE events would be prevented and 2 fatal or critical organ bleeds
would be caused over a mean 23-month period
Rates at mean
follow-up of
23 months
Rivaroxaban
2.5 mg bid
+ aspirin
N=8313
Rivaroxaban
5 mg bid
N=8250
Aspirin
N=8261
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI)
p-value HR
(95% CI)
p-value
Net clinical benefit
(CV death, stroke,
MI, fatal or critical
organ bleeding)
392 (5) 462 (6) 494 (6) 0.78
(0.69–0.90) 0.0003
0.94
(0.82–1.06) 0.31
All-cause mortality 262 (3) 316 (4) 339 (4) 0.77
(0.65–0.90) 0.0012
0.93
(0.80–1.09) 0.37
CV death 139 (2) 175 (2) 184 (2) 0.75
(0.60–0.93) 0.010
0.95
(0.77–1.17) 0.63
Non-CV death 123 (2) 141 (2) 155 (2) 0.79
(0.62–1.00) 0.048
0.91
(0.73–1.15) 0.43
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
CAD
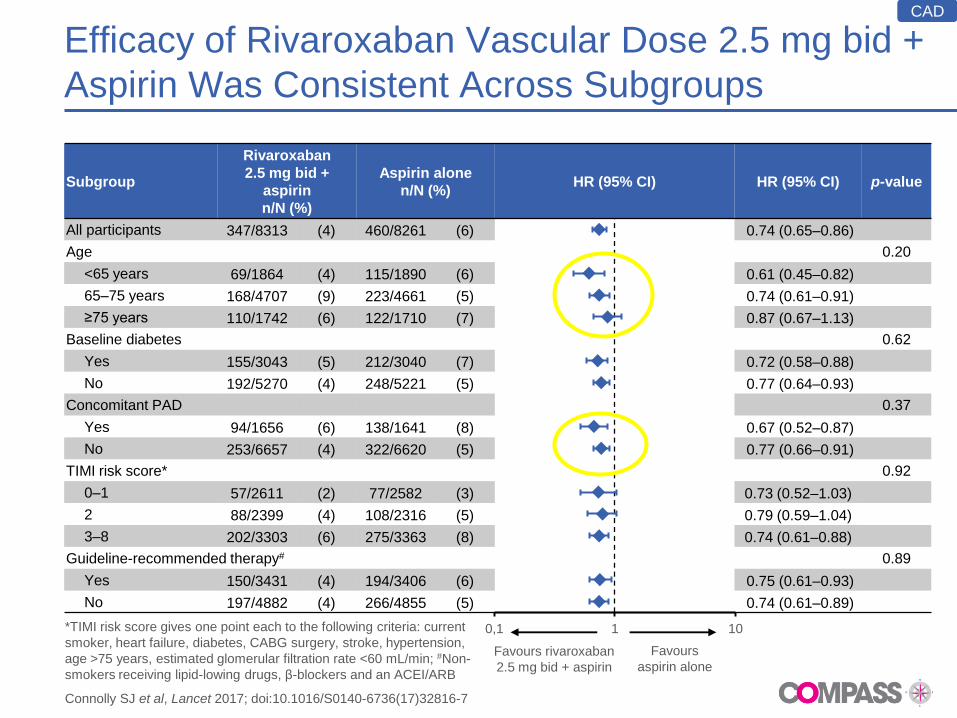
Efficacy of Rivaroxaban Vascular Dose 2.5 mg bid +
Aspirin Was Consistent Across Subgroups
Subgroup
Rivaroxaban
2.5 mg bid +
aspirin
n/N (%)
Aspirin alone
n/N (%) HR (95% CI) HR (95% CI) p-value
All participants 347/8313 (4) 460/8261 (6) 0.74 (0.65–0.86)
Age 0.20
<65 years 69/1864 (4) 115/1890 (6) 0.61 (0.45–0.82)
65–75 years 168/4707 (9) 223/4661 (5) 0.74 (0.61–0.91)
≥75 years 110/1742 (6) 122/1710 (7) 0.87 (0.67–1.13)
Baseline diabetes 0.62
Yes 155/3043 (5) 212/3040 (7) 0.72 (0.58–0.88)
No 192/5270 (4) 248/5221 (5) 0.77 (0.64–0.93)
Concomitant PAD 0.37
Yes 94/1656 (6) 138/1641 (8) 0.67 (0.52–0.87)
No 253/6657 (4) 322/6620 (5) 0.77 (0.66–0.91)
TIMI risk score* 0.92
0–1 57/2611 (2) 77/2582 (3) 0.73 (0.52–1.03)
2 88/2399 (4) 108/2316 (5) 0.79 (0.59–1.04)
3–8 202/3303 (6) 275/3363 (8) 0.74 (0.61–0.88)
Guideline-recommended therapy# 0.89
Yes 150/3431 (4) 194/3406 (6) 0.75 (0.61–0.93)
No 197/4882 (4) 266/4855 (5) 0.74 (0.61–0.89)
0,1 1 10
Favours rivaroxaban
2.5 mg bid + aspirin
Favours
aspirin alone
*TIMI risk score gives one point each to the following criteria: current
smoker, heart failure, diabetes, CABG surgery, stroke, hypertension,
age >75 years, estimated glomerular filtration rate <60 mL/min; #Non-
smokers receiving lipid-lowing drugs, β-blockers and an ACEI/ARB
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
CAD
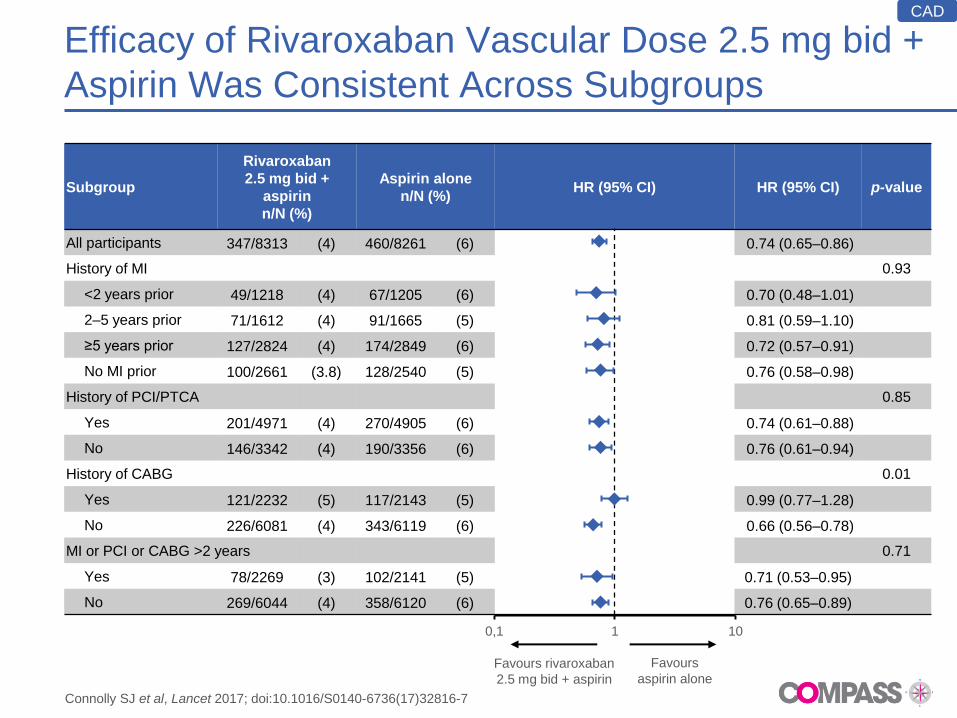
Efficacy of Rivaroxaban Vascular Dose 2.5 mg bid +
Aspirin Was Consistent Across Subgroups
Subgroup
Rivaroxaban
2.5 mg bid +
aspirin
n/N (%)
Aspirin alone
n/N (%) HR (95% CI) HR (95% CI) p-value
All participants 347/8313 (4) 460/8261 (6) 0.74 (0.65–0.86)
History of MI 0.93
<2 years prior 49/1218 (4) 67/1205 (6) 0.70 (0.48–1.01)
2–5 years prior 71/1612 (4) 91/1665 (5) 0.81 (0.59–1.10)
≥5 years prior 127/2824 (4) 174/2849 (6) 0.72 (0.57–0.91)
No MI prior 100/2661 (3.8) 128/2540 (5) 0.76 (0.58–0.98)
History of PCI/PTCA 0.85
Yes 201/4971 (4) 270/4905 (6) 0.74 (0.61–0.88)
No 146/3342 (4) 190/3356 (6) 0.76 (0.61–0.94)
History of CABG 0.01
Yes 121/2232 (5) 117/2143 (5) 0.99 (0.77–1.28)
No 226/6081 (4) 343/6119 (6) 0.66 (0.56–0.78)
MI or PCI or CABG >2 years 0.71
Yes 78/2269 (3) 102/2141 (5) 0.71 (0.53–0.95)
No 269/6044 (4) 358/6120 (6) 0.76 (0.65–0.89)
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
0,1 1 10
Favours rivaroxaban
2.5 mg bid + aspirin
Favours
aspirin alone
CAD
Persistent Reduction in MACE with Dual Pathway
Inhibition; Increased Bleeding only in the First Year
Rivaroxaban
2.5 mg bid + aspirin
n/N (%)
Aspirin alone
n/N (%) HR (95% CI) HR (95% CI)
MACE
<1 year 176/8313 (2) 221/8261 (3) 0.79 (0.65–0.96)
1–<2 years 113/7228 (2) 169/7125 (2) 0.66 (0.52–0.83)
>2 years 58/3655 (2) 70/3621 (2) 0.82 (0.58–1.16)
Major bleeding
<1 year 163/8313 (2) 70/8261 (1) 2.32 (1.75–3.07)
1–<2 years 70/7189 (1) 59/7183 (1) 1.19 (0.84–1.68)
>2 years 30/3626 (1) 30/3628 (1) 1.05 (0.63–1.75)
Net clinical benefit
<1 year 207/8313 (2) 237/8261 (3) 0.87 (0.72–1.04)
1–<2 years 124/7201 (2) 182/7112 (3) 0.67 (0.53–0.84)
>2 years 61/3637 (2) 75/3604 (2) 0.80 (0.57–1.12)
All death
<1 year 117/8313 (1) 145/8261 (2) 0.80 (0.63–1.02)
1–<2 years 93/7323 (1) 120/7242 (2) 0.77 (0.59–1.01)
>2 years 52/3743 (1) 74/3762 (2) 0.70 (0.49–1.00)
Landmark analysis for key efficacy and safety outcomes
Connolly SJ et al, Lancet 2017; doi:10.1016/S0140-6736(17)32816-7
0,1 1 10
Favours rivaroxaban
2.5 mg bid + aspirin
Favours
aspirin alone
CAD
COMPASS PAD Analysis
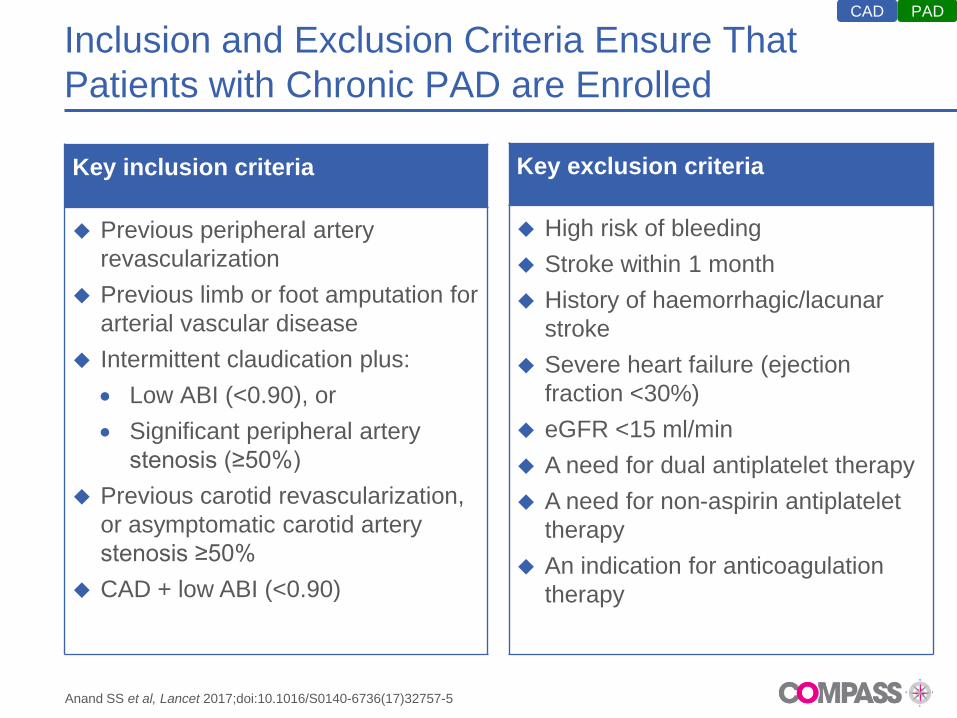
Inclusion and Exclusion Criteria Ensure That
Patients with Chronic PAD are Enrolled
Key inclusion criteria
Previous peripheral artery
revascularization
Previous limb or foot amputation for
arterial vascular disease
Intermittent claudication plus:
Low ABI (<0.90), or
Significant peripheral artery
stenosis (≥50%)
Previous carotid revascularization,
or asymptomatic carotid artery
stenosis ≥50%
CAD + low ABI (<0.90)
Key exclusion criteria
High risk of bleeding
Stroke within 1 month
History of haemorrhagic/lacunar
stroke
Severe heart failure (ejection
fraction <30%)
eGFR <15 ml/min
A need for dual antiplatelet therapy
A need for non-aspirin antiplatelet
therapy
An indication for anticoagulation
therapy
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
PAD CAD
PAD-Specific Limb Outcomes Were Added to
Main Study Outcomes for COMPASS
Primary cardiovascular outcome was MACE, defined as:
Composite of cardiovascular death, stroke or MI
Key composite outcomes for PAD:
Primary limb outcome was major adverse limb events (MALE),
defined as development of ALI or CLI and major amputations not included in
ALI or CLI
The composite of MACE and MALE
The composite of MACE, MALE and major amputations not included in
ALI or CLI
PAD
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
ALI, acute limb ischaemia; CAD, coronary artery disease; CLI, chronic limb ischaemia; MACE, major
adverse cardiovascular events; MI, myocardial infarction; PAD, peripheral artery disease
Major Adverse Limb Events and Major Amputation
Were Included in PAD-Specific Net Clinical Benefit
Primary safety outcome: modified ISTH
Major bleeding defined as:
– Fatal bleeding, or
– Bleeding into a critical organ, or
– Surgical site bleeding requiring reoperation, or
– Bleeding requiring hospitalization
Net clinical benefit outcome defined as:
MACE
MALE including major amputation
Fatal bleeding
Bleeding into a critical organ
PAD
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5

Dual Pathway Inhibition with Rivaroxaban Vascular Dose 2.5 mg
bid + Aspirin Reduced MACE by 28% Versus Aspirin Alone
Outcome
Rivaroxaban
2.5 mg bid
+ aspirin
N=2492
Rivaroxaban
5 mg bid
N=2474
Aspirin
N=2504
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI) p-value
HR
(95% CI) p-value
MACE 126 (5) 149 (6) 174 (7) 0.72 (0.57–
0.90) 0.0047
0.86
(0.69–1.08) 0.19
CV
death 64 (3) 66 (3) 78 (3)
0.82
(0.59–1.14) –
0.86
(0.62–1.19) –
Stroke 25 (1) 43 (2) 47 (2) 0.54
(0.33–0.87) –
0.93
(0.61–1.40) –
MI 51 (2) 56 (2) 67 (3) 0.76
(0.53–1.09) –
0.84
(0.59–1.20) –
PAD
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
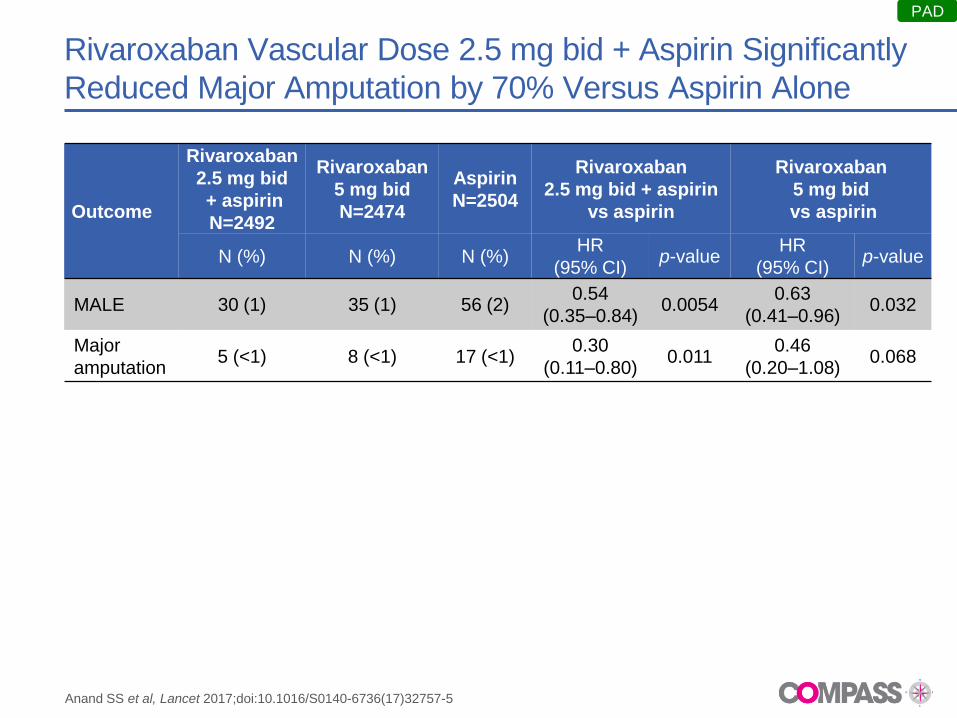
Rivaroxaban Vascular Dose 2.5 mg bid + Aspirin Significantly
Reduced Major Amputation by 70% Versus Aspirin Alone
Outcome
Rivaroxaban
2.5 mg bid
+ aspirin
N=2492
Rivaroxaban
5 mg bid
N=2474
Aspirin
N=2504
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI) p-value
HR
(95% CI) p-value
MALE 30 (1) 35 (1) 56 (2) 0.54
(0.35–0.84) 0.0054
0.63
(0.41–0.96) 0.032
Major
amputation 5 (<1) 8 (<1) 17 (<1)
0.30
(0.11–0.80) 0.011
0.46
(0.20–1.08) 0.068
PAD
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
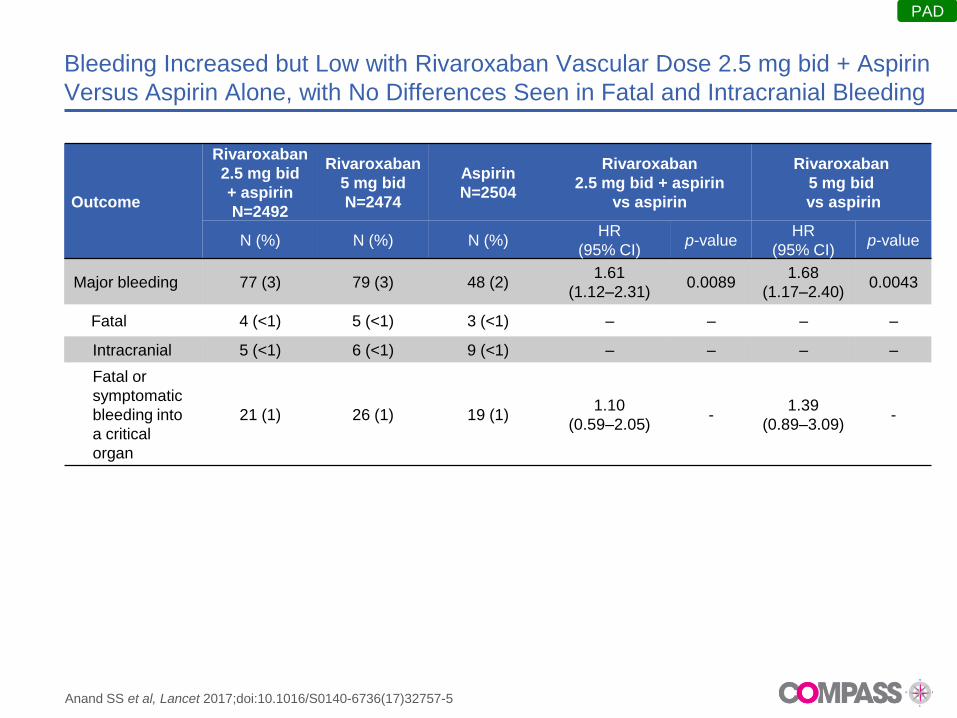
Bleeding Increased but Low with Rivaroxaban Vascular Dose 2.5 mg bid + Aspirin
Versus Aspirin Alone, with No Differences Seen in Fatal and Intracranial Bleeding
Outcome
Rivaroxaban
2.5 mg bid
+ aspirin
N=2492
Rivaroxaban
5 mg bid
N=2474
Aspirin
N=2504
Rivaroxaban
2.5 mg bid + aspirin
vs aspirin
Rivaroxaban
5 mg bid
vs aspirin
N (%) N (%) N (%) HR
(95% CI) p-value
HR
(95% CI) p-value
Major bleeding 77 (3) 79 (3) 48 (2) 1.61
(1.12–2.31) 0.0089
1.68
(1.17–2.40) 0.0043
Fatal 4 (<1) 5 (<1) 3 (<1) – – – –
Intracranial 5 (<1) 6 (<1) 9 (<1) – – – –
Fatal or
symptomatic
bleeding into
a critical
organ
21 (1) 26 (1) 19 (1) 1.10
(0.59–2.05) -
1.39
(0.89–3.09) -
PAD
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
Vascular Dose Rivaroxaban Showed Improved Outcomes for
PAD Patients with a Need for Increased Vascular Protection
Rivaroxaban vascular dose 2.5 mg BID plus aspirin reduced the
composite endpoint of stroke, MI or CV death by 28%.
MALE by 46%
Major amputations by 70%
Despite an expected increase in major bleeding events with
Rivaroxaban 2.5 mg BID plus aspirin, no significant increase was
observed in fatal or critical organ bleeding
This dual pathway inhibition of Rivaroxaban vascular dose and aspirin
represents a major advance in the management of PAD and is the only
available therapeutic option to significantly reduce both MACE and
MALE
PAD
*Defined as CV death, MI, stroke, MALE, major amputation, fatal bleeding or critical organ bleeding
Anand SS et al, Lancet 2017;doi:10.1016/S0140-6736(17)32757-5
CONCLUSIONI…. uno sguardo al futuro… che prospettive?
CONCLUSIONI
La forza dell’equilibrio…
Rischio ischemico
Rischio emorragico
Antiaggregazione
+
Rivaroxaban 2,5 x 2