La Sindrome miasteniforme di Lambert-Eaton · La Sindrome miasteniforme di Lambert-Eaton. D.M....
28
La Sindrome miasteniforme di Lambert-Eaton D.M. Bonifati U.O.C Neurologia, Ospedale Ca’ Foncello, Treviso Bolzano 12 Maggio 2017
Transcript of La Sindrome miasteniforme di Lambert-Eaton · La Sindrome miasteniforme di Lambert-Eaton. D.M....

La Sindrome miasteniforme di
Lambert-EatonD.M. Bonifati
U.O.C Neurologia, Ospedale Ca’ Foncello,
Treviso
Bolzano 12 Maggio 2017
LA STORIA DI UN PAZIENTE CON SINTOMI AUTONOMICI DOPO UN VIAGGIO IN CINA
Uomo di 66 anni.
Lamenta la comparsa 3 anni prima di severi sintomi autonomici dopo un viaggio in cina in particolare ipotensione posturale (80/50), xerostomia e xeroftalmia.
Fin dall’esordio era presente anche una stanchezza prossimale ai 4 arti attribuita alla marcata ipotensione a un concomitante quadro depressivo.La stanchezza era prevalente agli AAII molto variabile da un giorno all’altro.
Mai sintomi oculari e non chiari sintomi bulbari tranne una lieve disartria e una voce lievemente ipofonica dopo conversazione prolungata. Uno screening immunologico era negativo ed era stata esclusa la S. di Sjogren.
Anamnesticamente : depressione di lunga data in terapia con Paroxetina. Sostituzione valvolare mitralica 10 anni prima per endocardite. Ipercolesterolemia in statine, ipoacusia.
Bolzano 12 Maggio 2017
LA STORIA DI UN PAZIENTE CON SINTOMI AUTONOMICI DOPO UN VIAGGIO IN CINA
…..all’inizio “alcune volte mi cadeva la testa e dovevo sostenerla con le mani”.
L’esame neurologico era nella norma compresi i test di affaticabilità tranne una marcia lievemente atassica e dei ROT assenti che ricomparivano deboli dopo una contrazione isometrica.
EMG con stimolazione ripetitiva: anormale risposta decrementale a bassa frequenza.
Anti-recettore dell’acetilcolina: negativi.
Anticorpi anti-canali del Calcio: 300 pmol/L (v.n 0.0–24.5 pmol/L).
PET total body: negative.
Conclusione: LEMS non paraneoplatica. Iniziato trattamento sintomatico e con corticosteroidi con netto miglioramento della forza ma anche lentamente dei sintomi autonomici.

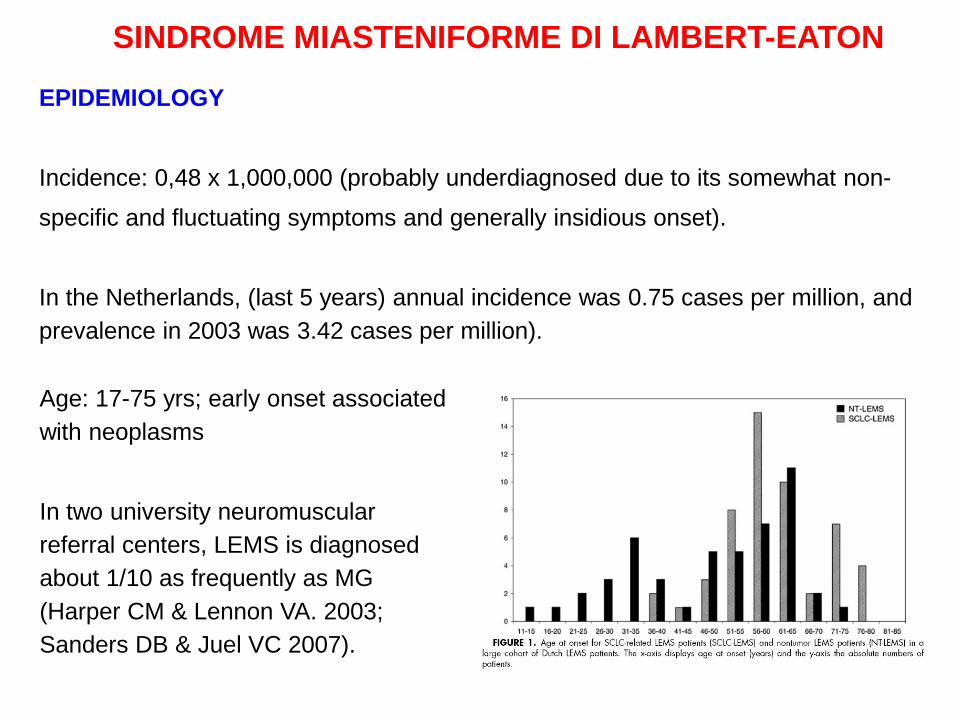
EPIDEMIOLOGY
Incidence: 0,48 x 1,000,000 (probably underdiagnosed due to its somewhat non-specific and fluctuating symptoms and generally insidious onset).
In the Netherlands, (last 5 years) annual incidence was 0.75 cases per million, and prevalence in 2003 was 3.42 cases per million).
SINDROME MIASTENIFORME DI LAMBERT-EATON
Age: 17-75 yrs; early onset associated with neoplasms
In two university neuromuscular referral centers, LEMS is diagnosed about 1/10 as frequently as MG (Harper CM & Lennon VA. 2003; Sanders DB & Juel VC 2007).
PATHOPHYSIOLOGY
Presynaptic pathology in LEMS was first demonstrated by in vivo microelectrode studies of intercostal muscles in an LEMS patient (Elmqvist D, Lambert EH. Mayo Clin Proc 1968).
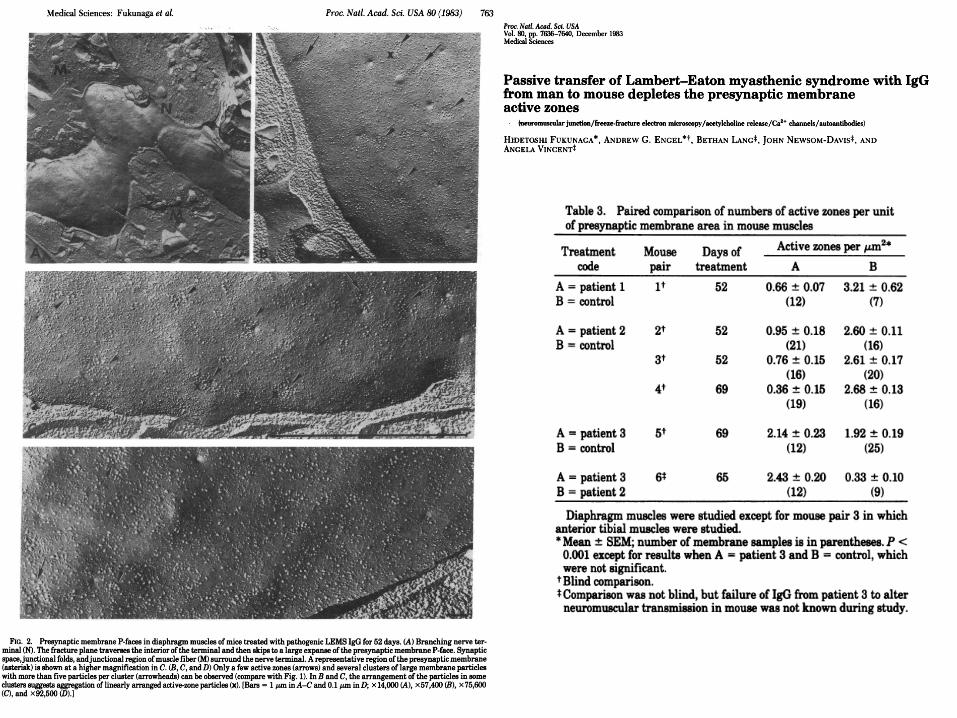
• Morphological (Fukunaga et al., 1983) and electrophysiological (Lang et al., 1983) LEMS features in mice injected with human LEMS IgG;
• Reduced quantal release of acetylcholine (ACh) from the nerve terminal reflects a reduction in the number of functional cell surface VGCC. (Lang et al., 1987).
B Mahadeva,L H. Phillips II Seminars in Neurology 28 (2); 2008


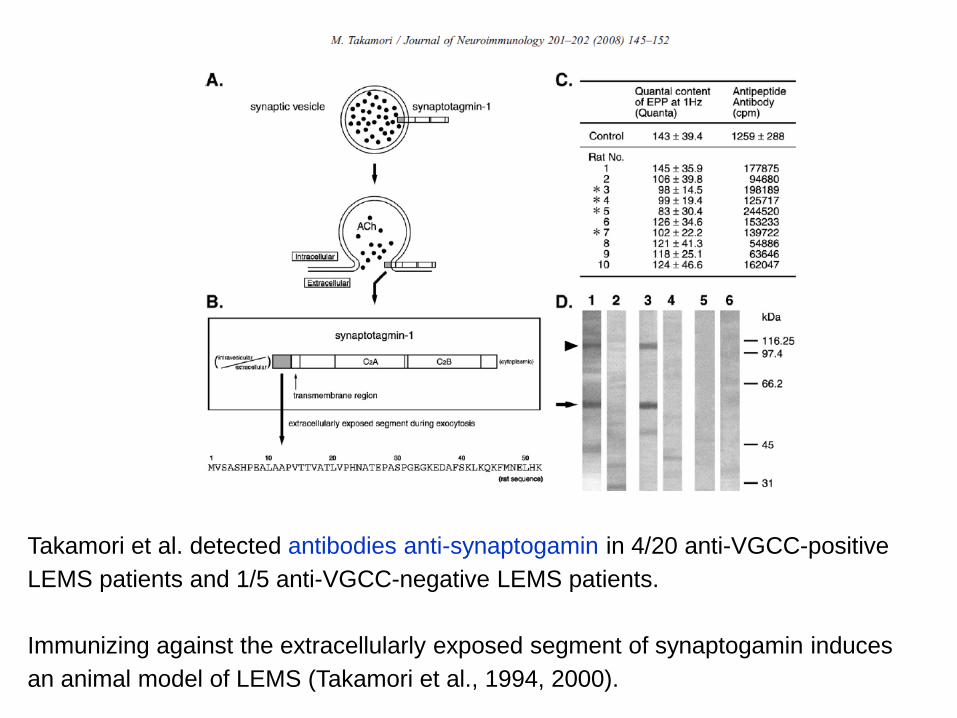
Takamori et al. detected antibodies anti-synaptogamin in 4/20 anti-VGCC-positive LEMS patients and 1/5 anti-VGCC-negative LEMS patients.
Immunizing against the extracellularly exposed segment of synaptogamin induces an animal model of LEMS (Takamori et al., 1994, 2000).
PATHOPHYSIOLOGY
VGCC antibodies can be detected in 85% of all LEMS patients. Specificity in pts with distinct muscle weakness is nearly 100%. False positives: Hypergammaglobulinemia; Chronic liver disorders; Infections
Among SCLC pts without any symptoms of muscle weakness or autonomic dysfunction, 3–5% have VGCC antibodies.
With calcium influx being hampered by the VGCC antibodies, presynaptic compensatory mechanisms influence acetylcholine release.
VGCC antibodies and LEMS can also coexist with central nervous system disease. Among SCLC patients diagnosed with paraneoplastic subacute cerebellar degeneration, 16% were found with concomitant LEMS, and 24% with increased VGCC antibody levels. Cerebellar ataxia has been reported also in a few nonparaneoplastic LEMS patients with VGCC antibodies.
Onset: Gradual and insidious onset of proximal lower extremity weakness (82%), fatigue, and dry mouth. CA-LEMS has been associated with more rapid disease evolution than NCA-LEMS. The weak muscles may be sore and tender.
Weakness may be:
Proximal > Distal
Legs (98%) & Arms (82%)
Respiratory muscles (15%): rarely severe
Disphagia (22%)
Some patients initially experience facilitation of strength with exercise and reduced strength if exercise is sustained. It may worsen with high temperature and fever
Fatigability (33%)
CLINICAL SYMPTOMS
AUTONOMIC DYSFUNCTION (Lambert 1956; Lambert 1971).
Most patients report dry mouth or an unpleasant metallic taste early in the course of LEMS, although they may not volunteer this symptom unless prompted. Impotence in men, orthostatic hypotension, and constipation are also observed, although these are less specific complaints. Pupils are often dilated and poorly reactive. There is reduced sweting.Autonomic function studies are abnormal even in those who are asymptomatic.
ASSOCIATION WITH CANCER
Subsequently, LEMS has been associated with an underlying cancer in about 50% of patients.Small-cell lung carcinoma (SCLC) is clearly the most common associated malignancy, although other primary tumors have rarely been associated with LEMS (non-SCLC; lymphoma; leukemia; malignant thymoma; and carcinomas of breast, colon, prostate, larynx, and gallbladder). Although LEMS onset may precede the diagnosis of cancer, an underlying cancer is usually discovered within the first 2 years, and nearly always within 4 years
LEMS SubgroupsLEMS without neoplasm (SCLC)
Epidemiology: Male (50%) > Female (50%) Median age: 49.5 years
Slow progression with normal life expectancy
Better prognosis with better clinical score at onset
No correlation with: Anti-P/Q-VGCC antibody titers
Lymphoma may be detected on follow-up (6%)
Associated immunologic disorders
• Frequency: 27%
• Common types: Myasthenia gravis; Pernicious anemia; Thyroid;Systemic lupus erythematosus; Celiac disease; Vitiligo; Diabetes
LEMS SubgroupsLEMS with neoplasm: Especially small cell lung cancer
Epidemiology: Male (70%) > Female (30%); Median age: 58 years
Clinical
• Respiratory failure more common
• Weight loss more common
• Shortened life expectancy: Probably related to neoplasm
• High ESR
LEMS without anti-(VGCC) antibodies• Frequency: 15% of LEMS patients
• Clinical features: Similar to antibody positive group
• Less associated small cell lung cancer: 12% vs 60% with antibodies
• Serum IgG reduces quantal content of end plate potentials
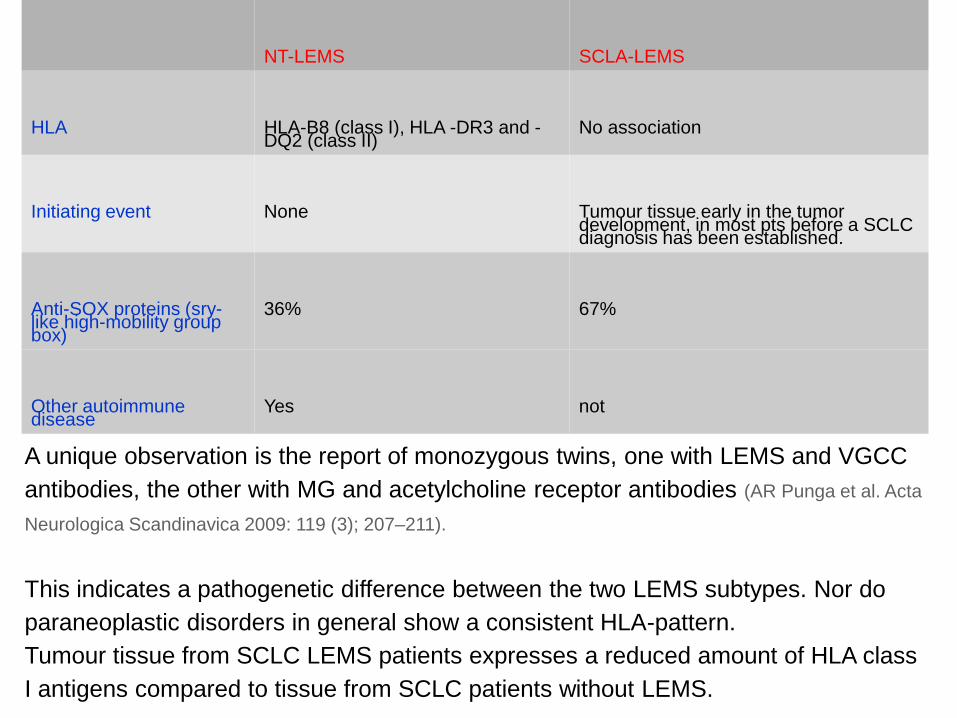
A unique observation is the report of monozygous twins, one with LEMS and VGCC antibodies, the other with MG and acetylcholine receptor antibodies (AR Punga et al. Acta
Neurologica Scandinavica 2009: 119 (3); 207–211).
This indicates a pathogenetic difference between the two LEMS subtypes. Nor do paraneoplastic disorders in general show a consistent HLA-pattern. Tumour tissue from SCLC LEMS patients expresses a reduced amount of HLA class I antigens compared to tissue from SCLC patients without LEMS.
NT-LEMS SCLA-LEMS
HLA HLA-B8 (class I), HLA -DR3 and -DQ2 (class II)
No association
Initiating event None Tumour tissue early in the tumordevelopment, in most pts before a SCLC diagnosis has been established.
Anti-SOX proteins (sry-like high-mobility groupbox)
36% 67%
Other autoimmune disease
Yes not
Once a diagnosis of LEMS has been confirmed, or even suspected, starts
the search for a SCLC. If the initial search is negative, the screening
should be repeated after 3 months, and then every 6 months up till 2
years after LEMS debut (EFNS guidelines).
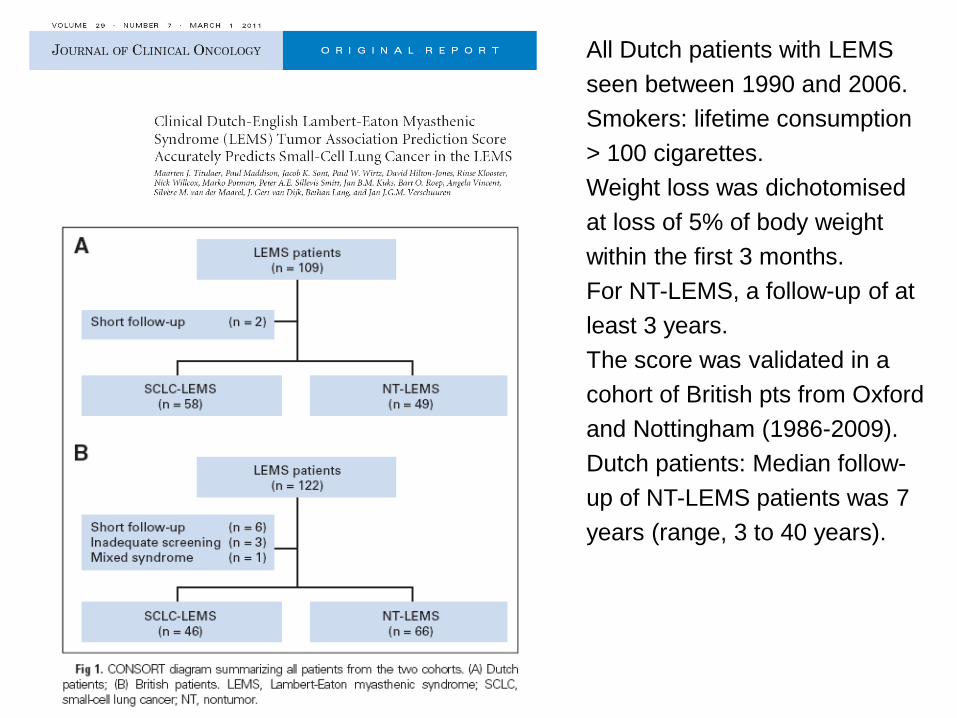
All Dutch patients with LEMS seen between 1990 and 2006. Smokers: lifetime consumption > 100 cigarettes. Weight loss was dichotomised at loss of 5% of body weight within the first 3 months.For NT-LEMS, a follow-up of at least 3 years.The score was validated in a cohort of British pts from Oxford and Nottingham (1986-2009). Dutch patients: Median follow-up of NT-LEMS patients was 7 years (range, 3 to 40 years).
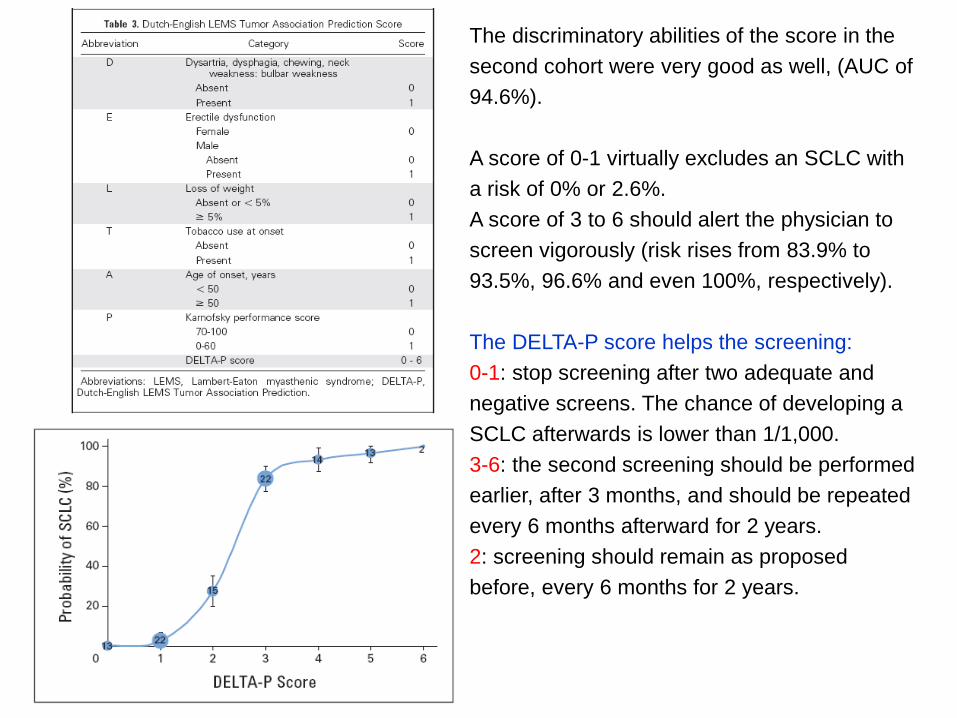
The discriminatory abilities of the score in the second cohort were very good as well, (AUC of 94.6%).
A score of 0-1 virtually excludes an SCLC with a risk of 0% or 2.6%. A score of 3 to 6 should alert the physician to screen vigorously (risk rises from 83.9% to 93.5%, 96.6% and even 100%, respectively).
The DELTA-P score helps the screening: 0-1: stop screening after two adequate and negative screens. The chance of developing a SCLC afterwards is lower than 1/1,000.3-6: the second screening should be performed earlier, after 3 months, and should be repeated every 6 months afterward for 2 years. 2: screening should remain as proposed before, every 6 months for 2 years.

SYMPTOMATIC TREATMENT: 3,4-diaminopyridine (3,4-DAP):
3,4 diaminopyridine is an aminopyridine that blockspresynaptic voltage-gated potassium channelsresulting in prolonged nerve action potentials withincreased calcium entry into presynaptic neurons.
In animals: more potent in improving neuromusculartransmission (Molgo 1980) and less convulsant (Lechat 1968)
than 4-AP.
The first use of 3,4-DAP was in 3 people with LEMS without lung cancer who all derived significant clinical and electrophysiological benefit from intravenous and then oral preparations of 3,4-DAP (Lundh 1983).
Follow-up data collected after a mean treatment duration of 5 yrs demonstrated prolonged beneficial clinical effects with minimal side effects at daily doses less than 60 mg of 3,4-DAP (Lundh 1993).
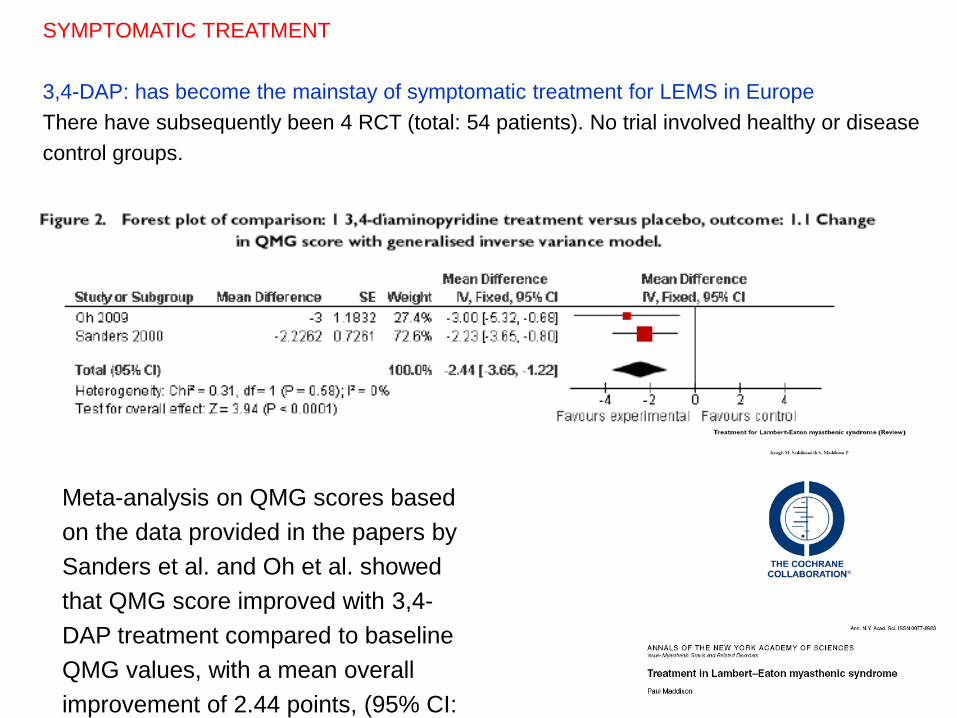
Meta-analysis on QMG scores based on the data provided in the papers by Sanders et al. and Oh et al. showed that QMG score improved with 3,4-DAP treatment compared to baseline QMG values, with a mean overall improvement of 2.44 points, (95% CI:
SYMPTOMATIC TREATMENT
3,4-DAP: has become the mainstay of symptomatic treatment for LEMS in EuropeThere have subsequently been 4 RCT (total: 54 patients). No trial involved healthy or disease control groups.
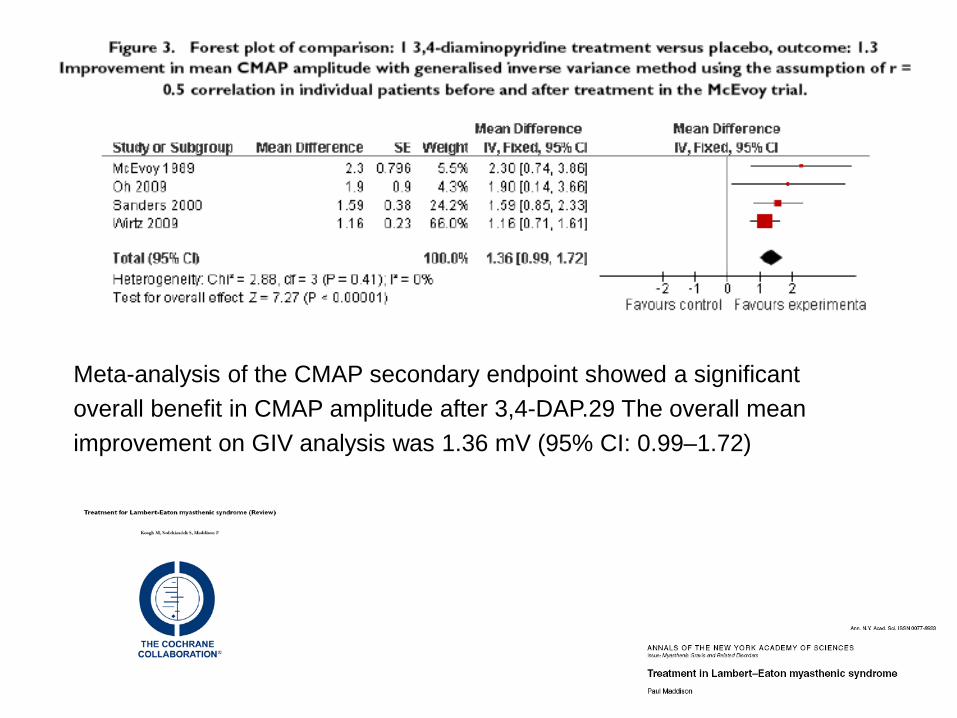
Meta-analysis of the CMAP secondary endpoint showed a significant overall benefit in CMAP amplitude after 3,4-DAP.29 The overall mean improvement on GIV analysis was 1.36 mV (95% CI: 0.99–1.72)

Phase 3, randomized, double-blind, study. 38 pazienti (disegno complesso) Amifampridine phosphate for 7–91 days, followed by randomizationto continue amifampridine phosphate for 14 days or placebo (7-day taper, 7-day placebo). The primary efficacy endpoints were changes from baseline at day 14 in Quantitative Myasthenia Gravis and Subject Global Impression scores. Results: The coprimary efficacy end points and 1 of the secondary efficacy end points were met, showing a significant benefit of aminfampridine phosphateover placebo at Day 14. All 5 primary, secondary, and tertiary endpoints achieved statistical significance at Day 8. Amifampridine phosphate was well tolerated; the most common adverse eventswere oral and digital paresthesias, nausea, and headache.
Muscle Nerve 53: 717–725, 2016
THERAPY
Limited but moderate to high quality evidence from randomised controlled trials showed that:over days 3,4-diaminopyridine, or for up to 8 weeks IVIg,
Acetylcholinesterase inhibitors may provide modest, transient improvement in strength and in autonomic symptoms, particularly dry mouth. The effect of acetylcholinesterase inhibitors is increased when they are used in combination with an agent that augments quantal release such diaminopyridine.
IVIGFollowing a single case report (Bird 1992), a randomised, double-blind placebo-controlled cross-over trial was conducted in 9 noncancer LEMS pts (Bain 1996).There were significant improvements in myometric strength measures , peaking at 2-4 weeks, and declining by 8 weeks associated with a significant decline in serum VGCC antibody titres. An EFNS guideline concludes that intravenous immunoglobulin may be tried in LEMS.
DAP significantly improves strength and autonomic function in most LES patients in clinical trials. More than 85% of patients exhibit significant improvement with DAP.DAP is dosed orally beginning at 5 to 10 mg x 3-4 times daily to a maximum of 60 mg/day.
The onset of effect begins within 20 to 30 minutes of oral dosing and lasts 4 to 5 hours. A maximum response to a particular dosage regimen is observed after about 3 days. The effect of DAP may be enhanced and prolonged with concurrent use of pyridostigmine.
Until recently, oral 3,4-DAP was available as an unlicensed formulation. A phosphate salt formulation of oral 3,4-DAP (amifampridine) has recently been licensed.
Common side effects: perioral and digital paresthesias, headaches, fatigue, insomnia, abdominal pain, anxiety, blurred vision, diarrhea, dizziness, palpitiations, and epigastric discomfort. . Serious side effects: seizures (> 100 mg/day); theoretical risk for cardiac arrhythmias in prolonged QT syndrome or other cardiac conduction abnormalities (fare ECG); although no organ toxicity has been reported, periodic blood monitoring for hematologic, hepatic, and renal function is also recommended.
Symptomatic Treatment Summary

Mycophenolate and cyclosporine have been recommended,.Rituximab:a positive treatment result in a few patients has recently been reported. To date, 2 patients with severe symptoms of LEMS, resistant to multiple oral immunosuppressant agents, have been treated with Rituximab with marked clinical benefit at 1 year, but short of remission. No significant side effects.

Paolo Carrari e Andrea Pagetta

Grazie