La scelta terapeutica nel carcinoma ovarico avanzato...
71
La scelta terapeutica nel carcinoma ovarico avanzato guidata da istotipo e caratteristiche biomolecolari: novità e prospettive future Dr.ssa Lorena Incorvaia Tutor Roberto Sabbatini Azienda Ospedaliera Universitaria Policlinco «P.Giaccone» Palermo
Transcript of La scelta terapeutica nel carcinoma ovarico avanzato...
La scelta terapeutica nel carcinoma ovarico avanzato guidata da istotipo e
caratteristiche biomolecolari: novità e prospettive future
Dr.ssa Lorena Incorvaia
Tutor Roberto Sabbatini
Azienda Ospedaliera Universitaria Policlinco
«P.Giaccone» Palermo

Ovarian Cancer: setting the scene
5 Y survival <25% for stage III/IV
Minimal improvement in ovarian cancer mortality rates – no new front-line
therapy for >20 years

Cisplatin
Cisplatin
Paclitaxel
Carboplatin
Paclitaxel
Platinum Paclitaxel
Bevacizumab
0
5
10
15
20
25
30
1990 1993 1998 2013
DFS
Survie depuis rechute
Survie globale
Survival from recurrence
Overall survival
The overall survival increase in ovarian cancer is mainly due
to the treatment of recurrent disease
Primary Treatment
Cytoreductive surgery + platinum based
Carboplatin-Paclitaxel PFS = 16-23 m
OS = 31-65 m
Intraperitoneal
Chemotherapy
PFS = + 5.5 m
OS = + 15 m
Weekly Carboplatin-
Paclitaxel
PFS = + 10.8 m
Carboplatin-Paclitaxel +
bevacizumab
PFS = + 4 m
First line treatment options
in advanced ovarian cancer at present
Karam A, et al. Annals of oncology 2017
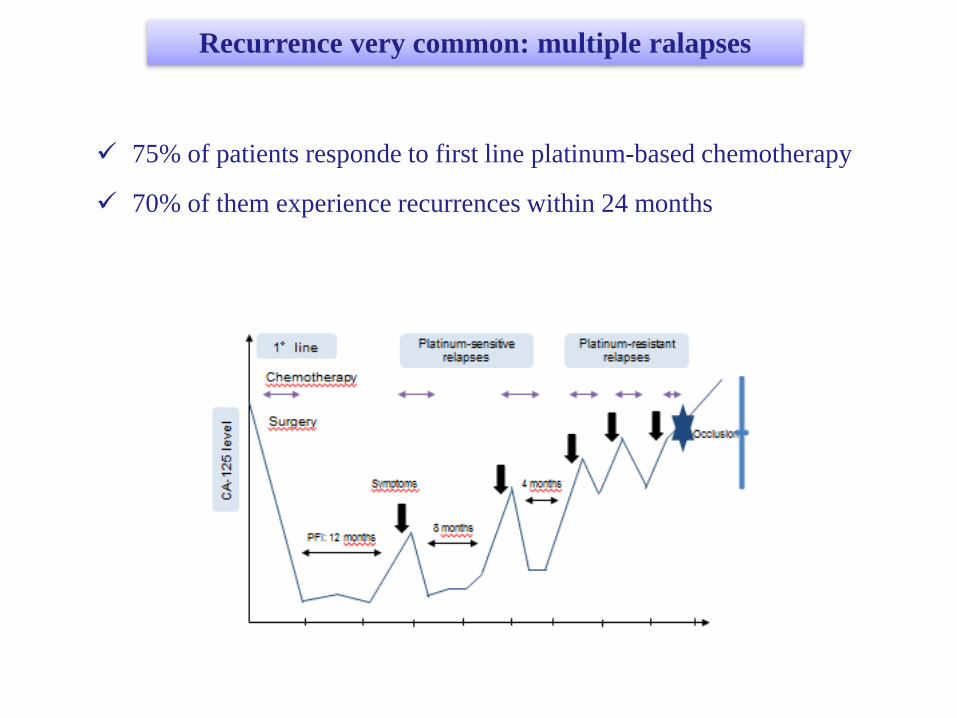
Recurrence very common: multiple ralapses
75% of patients responde to first line platinum-based chemotherapy
70% of them experience recurrences within 24 months
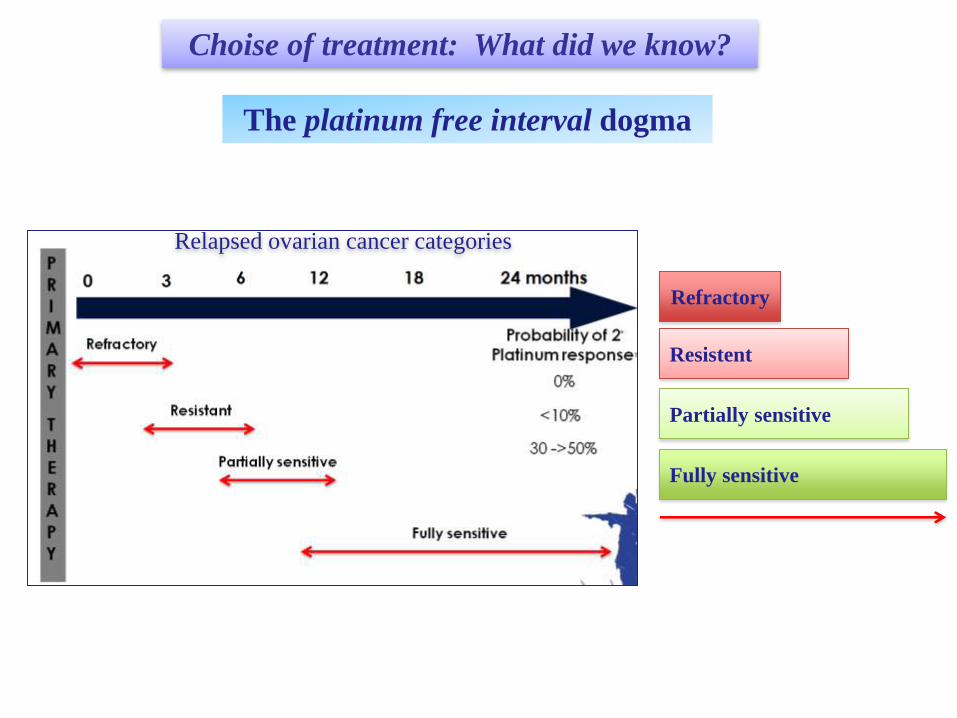
The platinum free interval dogma
Refractory
Resistent
Partially sensitive
Fully sensitive
Relapsed ovarian cancer categories
Choise of treatment: What did we know?

Epithelial ovarian tumors: from singular to plural
Choise of treatment: What do we know today?
The backstage….

Epithelial Ovarian cancer is not a unique disease
Epithelial ovarian
tumors

Impact of histological subtype

Prognostic impact of separating HGSOC and LGSOC

Histology more important?
Refractory
Resistent
Partially sensitive
Fully sensitive
Relapsed ovarian cancer categories
Choise of treatment: What do we know today?

Treatment guidance by histologic type
WHO 2014 diagnostic criteria

Low grade serous cancer
- Young age at diagnosis
- Chemoresistance
- Prolonged overall survival
- May arise de novo or following
diagnosis of serous borderline
tumor
- Aberrations within the MAP
kinase signaling pathway
Farley et al. Lancet Oncol 2013 Friday et al. Cancer Res 2008
Ras
MEK
ERK
Other substrates
Frequent mutations in SBTs and low-grade
serous carcinomas
Raf
MAPK
P P
P
P P
P P
MAPK Elk
SA
P Target
genes
Nucleus
Y Growth factor
SBT: serous borderline tumour
• Selumetinib, trametinib
– Potent
– Selective
– Orally available
– Non-ATP competitive inhibitor of
the mitogen-activated protein kinase
(MAPK), MEK-1/2

Recurrent or persistent
low-grade serous
carcinomas of the ovary,
fallopian tube or
primary peritoneum
MEK162
CT
(liposomal doxorubicin,
Paclitaxel
or topotecan)
MILO Study

Hormonal Maintenance Therapy for Women with Low-Grade Serous
Carcinoma of the
Ovary or Peritoneum
David M. Gershenson, MD
• High frequency of ER and PR expression in LGSC
Wong et al. Int J Gynecol Pathol 2007
• Hormonal therapy for recurrent LGSC associated with ORR = 9%, SD = 66%,
median PFS = 7.4 mo
Gershenson et al. Gynecol Oncol 2012
• LGSC similar to luminal breast cancer: Worse prognosis for women age < 35 y
Gershenson et al. J Clin Oncol 2015
Rationale

Stage II-
IV
LGSC
Primary
Cytoreductive
Surgery
Platinum-
Based Chemotherapy
Surveillance
N = 134
Hormonal Maintenance
Therapy
N = 70
David M. Gershenson, MD
ASCO 2016
Hormonal Maintenance Therapy for Women with Low-Grade Serous
Carcinoma of the
Ovary or Peritoneum

Group Median
PFS (mo)
95% CI P-
Value
SURV
(n = 121) 29.9 24.5, 35.2
< .001
HMT
(n = 27) 81.1 55.2, 106.9
ALL
(N = 148) 33.0 28.4, 37.7
p<.001
Results: PFS in Patients NED at Completion of
Chemotherapy
David M. Gershenson, MD
ASCO 2016

Results: OS in Patients NED at Completion of
Chemotherapy
Group Median
OS (mo)
95% CI P-
Value
SURV
(n = 121) 106.8 72.8, 140.7
.04
HMT
(n = 27) 191.3 93.5, 289.1
ALL
(N = 148) 115.7 86.5, 144.9
David M. Gershenson, MD
ASCO 2016

Choise of treatment: What do we know today?
From singular to plural
Molecular profile

Epithelial Ovarian cancer: Molecular profiling
Epithelial ovarian
tumors

What did we know? What do we know today?
Family history OC/BC
Age at diagnosis
BRCA1/BRCA2
Germline Mutations
BRCA mutation is not
correlate to age and
family history
Beyond gBRCA1/BRCA2:
Not only germline mutations: somatic!
Not only BRCA: “HRD phenotype”
BRCA testing
prognostic and predictive value:
BIOMARKER!
Molecular Profiling of High-Grade Serous Ovarian Cancer
Surveillance
program
Prophylactic
surgery

• Approximately 35%-40% of BRCA 1-2 mutation carriers do not have a
family history of cancer
BRCA mutation is not correlated to age and family history
• At least 25% of BRCA 1-2 mutation carriers are >60 yrs old
Available evidence
Median Age BRCA 1/2
Yrs
BRCA 1 +
Yrs
BRCA 2 +
Yrs
Alsop et al. 60 53 60
Soegaard et al. 61 49
Risch et al. 56 51 57
Malander et al. 59 57
Song et al. 59 52 57
Age is not a good predictor of BRCA mutation
BRCA Mutation Carriers
Who Lack a Family History (%)
Walsh et al. 27
Soegaard et al. 54
Malander et al. 8
Risch et al. 37
Alsop et al. 44
Song et al. 39
Family history is not a good predictor of BRCA mutation

BRCA mutation is not correlated to histotype
Alsop K, et al. J Clin Oncol 2012; 30: 2654–63.
BRCA mutation in 14.1% of the studied population
16.6% of serous histotype
22.6% of high grade serous subtype
Available evidence
6.3% of clear cell subtype
8.4% of endometrioid subtype

Total population
(%)
Serous (%)
Endometrioid (%)
Clear Cell (%)
Mucinous (%)
Alsop et al.
14.1 16.6 8.4 6.3 NA
Risch et al.
13.2 18.0 7.1 7.1 0
Soegaard et al.
5.8 5.4 5.4 9.1 0
Jacobi et al.
13.9 10.8 0 0 0
Malander et al.
8 7.6 13.0 12.5 0
Soergaard M. et al., Clin Cancer Rev. 2008; Risch HA et al., JNCI 2006; Alsop K et al., JCO 2012 Malander S. et al., EJC, 2004; Jacobi CE et al., Genet Med, 2007
Available evidence
Histotype is not a good predictor of BRCA mutation

What did we know? What do we know today?
Family history OC/BC
Age at diagnosis
BRCA1/BRCA2
Surveillance
program
Prophylactic
surgery
BRCA mutation is not
correlate to age and
family history
Beyond BRCA1/BRCA2:
“Beyond HR repair genes”
“HRD phenotype”
BRCA test: prognostic and
predictive value:
BIOMARKER!

1. Prognostic
Patients with BRCA mutated ovarian cancer show a significantly more
favourable prognosis
BRCA: impact of germline mutations
Bolton KL, et al. JAMA. 2012;307(4):382-390. Zhong Q et al. Clin Cancer Res. 2014;21(1):211-220.
5-year survival:
•BRCA1 – 44%
•BRCA2 – 61%
•No mutation – 25%
Bolton KL, et al. JAMA. 2012;307(4):382-390. Zhong Q et al. Clin Cancer Res. 2014;21(1):211-220.
Bolton KL, et al. JAMA. 2012;307(4):382-390. Zhong Q et al. Clin Cancer Res. 2014;21(1):211-220.

Pts with gBRCA mutations have a longer survival than in
women with sporadic ovarian cancer
1. Prognostic

BRCA: impact on patient therapy
2. Predictive
Improved survival in
BRCA-mutated ovarian
cancer patients treated
with Intraperitoneal
cisplatin and paclitaxel
Lesnock JL, Br J Cancer, 2013

BRCA: impact on patient therapy
2. Predictive

BRCA: impact on patient therapy
2. Predictive
Trabectedin in patients with BRCA-mutated and BRCAness
phenotype Advanced Ovarian Cancer (AOC): Phase II Prospective
MITO-15 Study

BRCA: impact on patient therapy
2. Predictive
Analysis of OV-301 according to BRCA status
Monk BJ Ann Oncol 2015
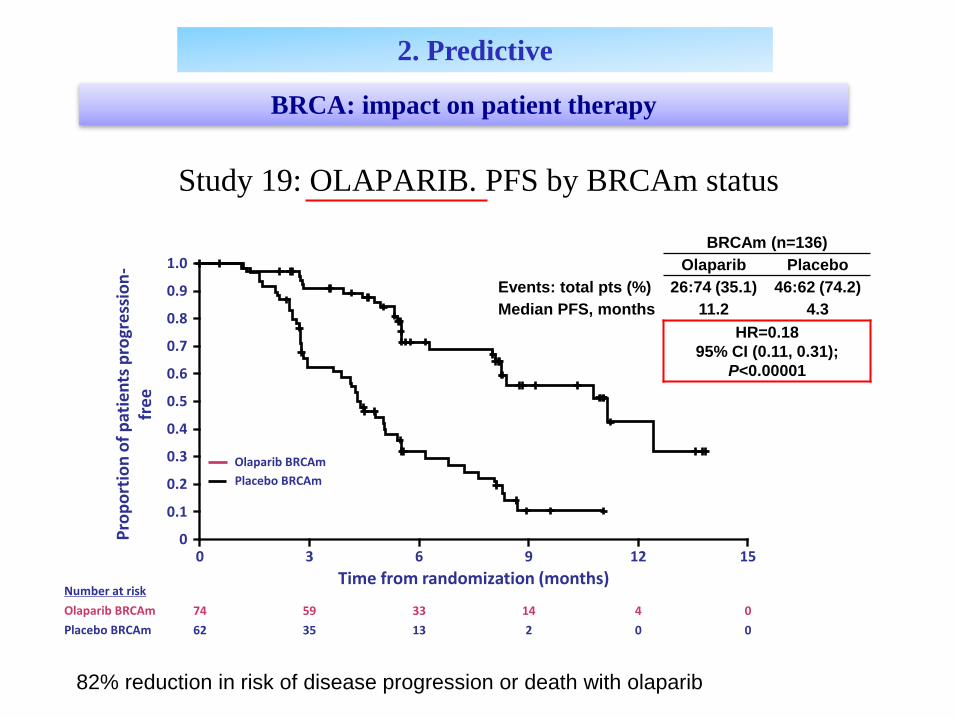
Study 19: OLAPARIB. PFS by BRCAm status
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
atie
nts
pro
gre
ssio
n-
fre
e
3 6 9 12 15
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
82% reduction in risk of disease progression or death with olaparib
Olaparib BRCAm
Placebo BRCAm
Number at risk
Olaparib BRCAm
Placebo BRCAm
74 59 33 14 4 0
62 35 13 2 0 0
BRCAm (n=136)
Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2)
Median PFS, months 11.2 4.3
HR=0.18
95% CI (0.11, 0.31);
P<0.00001
BRCA: impact on patient therapy
2. Predictive

SOLO-1, -2, -3
Randomized phase III studies of Olaparib in OC

No. at risk
Olaparib Placebo
196 99
182 70
156 37
134 22
118 18
104 17
89 14
82 12
32 7
29 6
3 0
2 0
0 0
100
90
80
70
60
50
40
30
20
10
0
Pro
gres
sio
n-f
ree
surv
ival
(%
)
Months since randomization
0 3 6 9 12 15 18 21 24 27 30 33 36
19.1
Olaparib
Placebo
5.5
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 107 (54.6) 80 (80.8)
Median PFS, months 19.1 5.5
HR 0.30
95% CI 0.22 to 0.41
P<0.0001
Median follow-up was 22.1 months in the olaparib group and 22.2 months for placebo
Presented by Pujade-Lauraine at SGO 2017 annual meeting
SOLO 2, PFS by investigator assessment

Abbreviations: MMR, mismatch repair; BER, base excision repair; NHEJ, nonhomologous end-
joining; HRR, homologous recombination repair; NER, nucleotide excision repair; TLJ, translesional
joining.
Major interactive pathways involved in DNA damage and repair
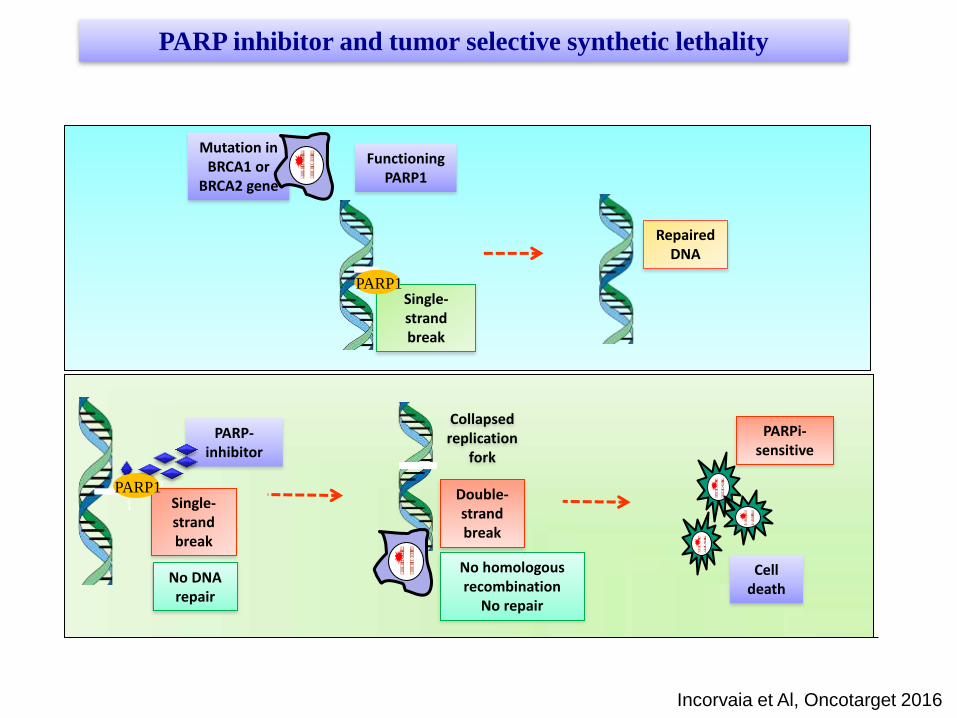
Functioning PARP1
Single-strand break
PARP1
Repaired DNA
Mutation in BRCA1 or
BRCA2 gene
Cell death
PARP
1
PARP-inhibitor
No DNA repair
Single-strand break
Collapsed replication
fork
Double-strand break
No homologous recombination
No repair
PARPi-sensitive
PARP inhibitor and tumor selective synthetic lethality
PARP1
Incorvaia et Al, Oncotarget 2016

Age and family history are not sufficient
criteria for BRCA testing
Histologic type (except mucinous) is not a
sufficient criterio for BRCA testing
Key points
BRCA is predictive of PARP-inhibitor
sensitivity
BRCA testing for all women with epitelial ovarian cancer, regardless of age,
histologic type and family history

What did we know? What do we know today?
Family history OC/BC
Age at diagnosis
BRCA1/BRCA2
Surveillance
program
Early
diagnosis
Prophylactic
surgery
Tumor risk
reduction
BRCA mutation is not
correlate to age and
family history
Beyond BRCA1/BRCA2:
“Beyond HR repair genes”
“HRD phenotype”
BRCA test: prognostic and predictive
value
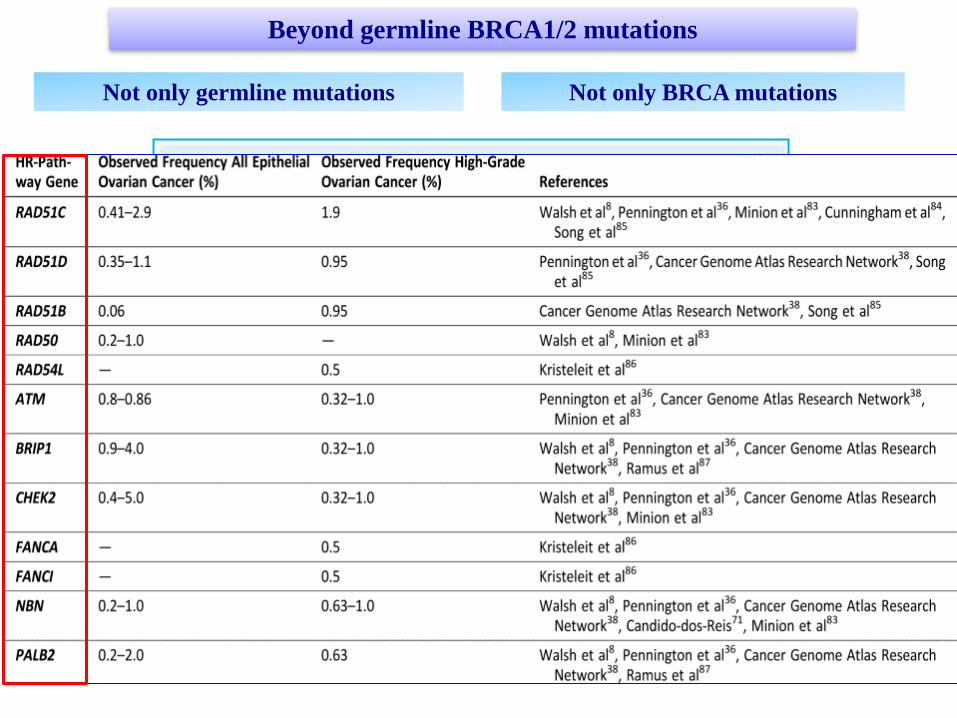
Beyond germline BRCA1/2 mutations
Not only germline mutations Not only BRCA mutations

HR gene mutations are not restricted to
BRCA

Sensitivity to DNA repair inhibitors?
BRCA-like signature
Beyond BRCA: “HRD phenotype”
BRCA germline
mutation
BRCA somatic
mutation
HR mutation,
non-BRCA

Parp-inhibitor trials for sporadic, BRCA WT, ovarian cancer:
Do we have one?
Rucaparib,
Ariel 3 trial
Niraparib,
NOVA trial
2 Randomised maintenance trials following platinum-based chemotherapy in
BRCAm and BRCAwt
gBRCAmut
Non-gBRCAmut
gBRCAmut
BRCA-like
Biomarker negative

Homologous Recombination Deficiency (HRD) Assay
Do we have one?
ARIEL 2, ASCO 2015
Biomarker
negative
gBRCAmut
BRCA-like
ORR
80%
ORR
29%
ORR
10%
Rucaparib,
Ariel 2 trial

McNeish IA, et al. J Clin Oncol. 2015;
Homologous Recombination Deficiency (HRD) Assay
Do we have one?

• Loss of heterozygosity (LOH)
• Telomeric allelic imbalance (TAI)
• Large-scale state transitions (LST)
HRD score is sum of LOH + TAI + LST scores
- Presented evidence of correlation between HRD score and in
vitro/in vivo response to niraparib in 106 tumor samples
Thus:
- Two assays under further evaluation, as key elements in 2 randomized
maintenance trials, with niraparib and rucaparib in sporadic and BRCAm-
associated ovarian cancer
Developed HRD score in the NOVA trial incorporating 3 components:
Homologous Recombination Deficiency (HRD) Assay
Do we have another?
Haluska P et al, NCI/EORTC/AACR 2014 (Eur J Cancer. 2014)
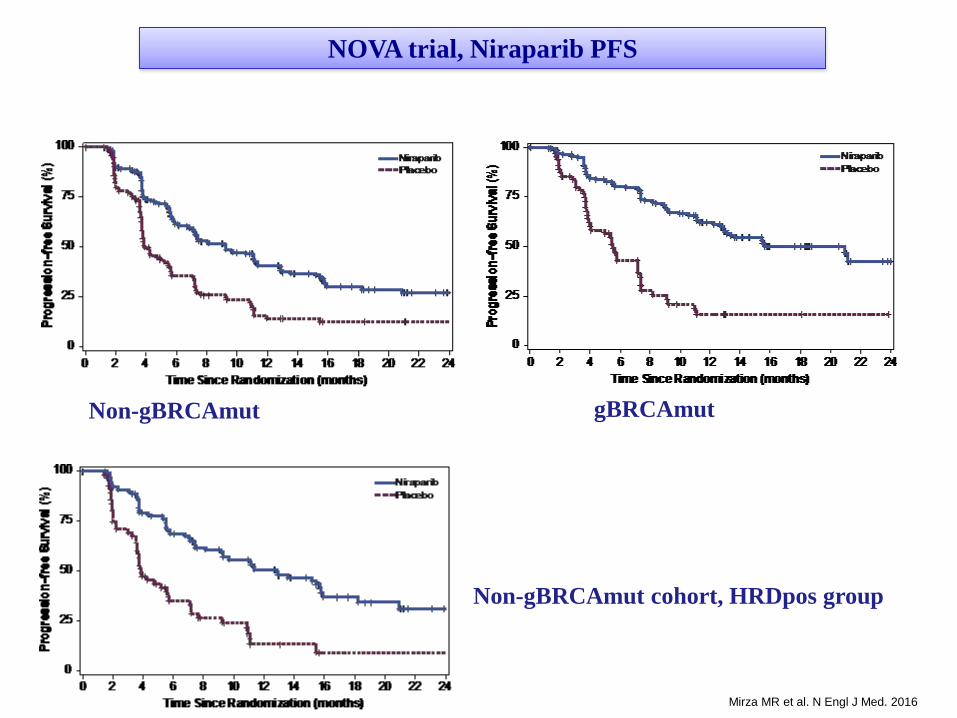
gBRCAmut Non-gBRCAmut
Non-gBRCAmut cohort, HRDpos group
NOVA trial, Niraparib PFS
Mirza MR et al. N Engl J Med. 2016

Germline
BRCA1/BRCA2 “HRD phenotype”
Olaparib
Niraparib
Rucaparib
….....
Molecular Profiling of High-Grade Serous Ovarian Cancer

Refractory
Resistent
Partially sensitive
Fully sensitive
Choise of treatment: What do we know today?
Molecular biology more important?

Identifying the HR Deficiency Signature
Identifying the subset of BRCA-like tumors, which respond to HRR-
directed therapy
OC and HR: How the debate is evolving?
Need for Biomarkers!
Panel testing: Which molecular alterations most important?
Sensitivity to targeted therapy? Clinically relevant?
Heterogeneity! How can we account for heterogeneity and dynamic changes that
occur in response to a given targeted therapy?

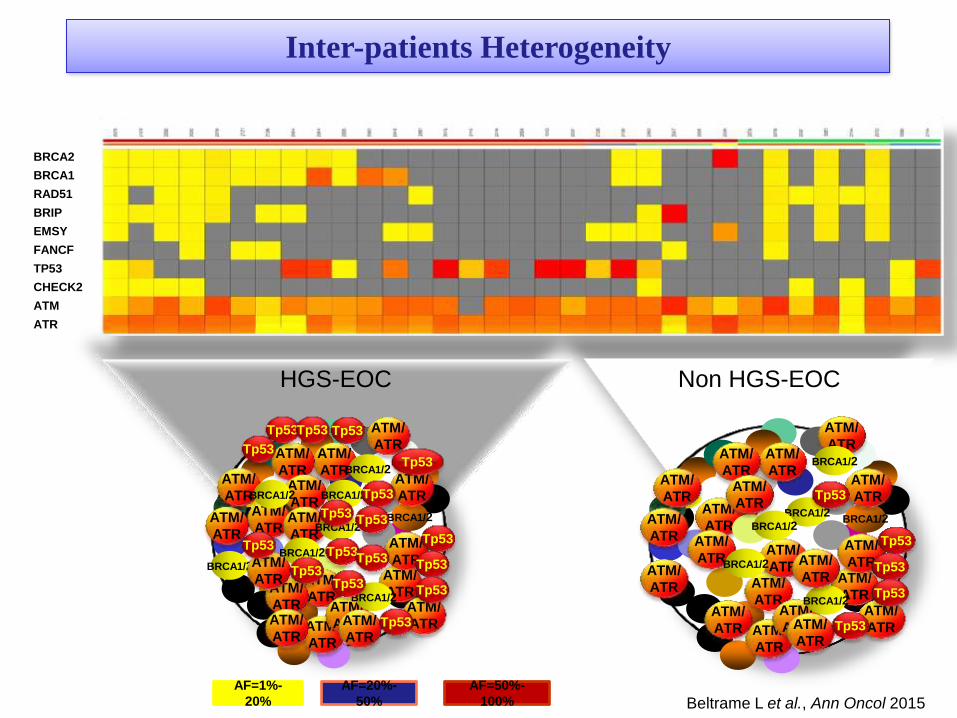
Tumor Heterogeneity
BRCA2
BRCA1
RAD51
BRIP
EMSY
FANCF
TP53
CHECK2
ATM
ATR
BRCA1/2
ATM/
ATR
BRCA1/2
Tp53
ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
Tp53
Tp53
Tp53 Tp53
Tp53
Tp53 Tp53
Tp53
Tp53
Tp53
Tp53
Tp53
Tp53 Tp53
Tp53
Tp53
Beltrame L et al., Ann Oncol 2015
BRCA1/2
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR ATM/
ATR
ATM/
ATR
ATM/
ATR ATM/
ATR
ATM/
ATR
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
Tp53
Tp53
Tp53
Tp53
Tp53
ATM/
ATR
AF=1%-
20%
AF=20%-
50%
AF=50%-
100%
Non HGS-EOC HGS-EOC
Inter-patients Heterogeneity

BRCA2
BRCA1
RAD51
BRIP
EMSY
FANCF
TP53
CHECK2
ATM
ATR
BRCA1/2
Tp53
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
Tp53
Tp53 Tp53
Tp53
Tp53
Tp53
Tp53
Tp53 Tp53
ATM/
ATR
ATM/
ATR
BRCA1/2
BRCA1/2
Tp53
Tp53
AF=1%-20% AF=20%-50% AF=50%-100%
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
BRCA1/2
Tp53
Tp53 Tp53
ATM/
ATR
ATM/
ATR
BRCA1/2
BRCA1/2 Tp53
HGS-EOC Non- HGS-EOC
Spatial and Temporal Heterogeneity

Where to go next?
Until we identify actionable target, the severe genomic
instability found across HGSOC remains the fulcrum

HRD
Synthetic Lethality
iPARP

Leverage
DNA damage
response
(DDR)
New opportunities…..
Clinical Synthetic Lethality
Targeting the molecular and
microenvironmental
characteristics of tumor
Endogenous tumor factors
HRD
TP53
Cell cycle regulation
Exogenous tumor factors
Hypoxia
Immune activation
Glucose metabolism
Chemical
synthetic
lethality
Contextual
synthetic
lethality
+

Hypoxia
Hypoxia downregulates
key genes in the
homologous-
recomination and
mismatch-repair pathway
(RAD 51, RAD 52,
BRCA, MSH2, and
MSH6)
Hypoxia is presumed to be generated locally by angiogenesis
inhibitors
Leveraging hypoxia to induce HRD-like environment

Leverage
DNA damage
response
(DDR)
Testing the hypothesis: PARPi + VEGFRi
Targeting the molecular and
microenvironmental
characteristics of tumor
Endogenous tumor factors
HRD
TP53
Cell cycle regulation
Exogenous tumor factors
Hypoxia
Immune activation
Glucose metabolism
Chemical
synthetic
lethality
Contextual
synthetic
lethality
+
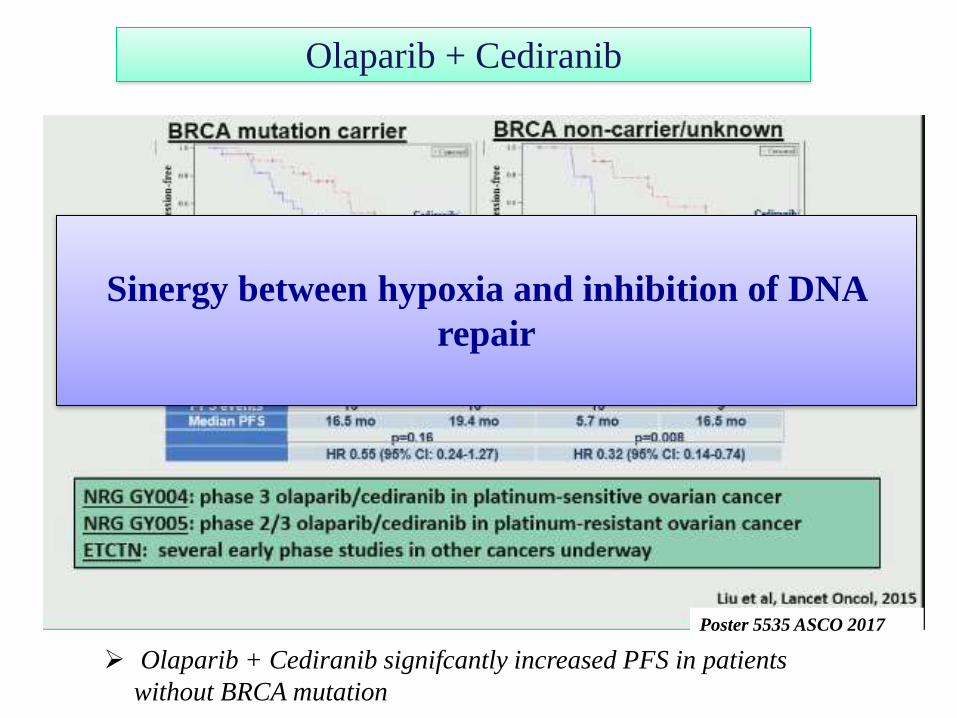
Olaparib + Cediranib
Olaparib + Cediranib signifcantly increased PFS in patients
without BRCA mutation
Sinergy between hypoxia and inhibition of DNA
repair
Poster 5535 ASCO 2017

Leverage
DNA damage
response
(DDR)
New opportunities…..
Clinical Synthetic Lethality
Targeting the molecular and
microenvironmental
characteristics of tumor
Endogenous tumor factors
HRD
TP53
Cell cycle regulation
Exogenous tumor factors
Hypoxia
Immune activation
Glucose metabolism
Chemical
synthetic
lethality
Contextual
synthetic
lethality
+

Targeting cell cycle to inhibit DDR

Cell cycle checkpoint abrogation:
CHK1/2 inhibitor

Cell cycle checkpoint abrogation:
Wee-1 inhibitor (AZ1775)

Wee-1i + Carboplatin/paclitaxel in TP 53 mut
HGSOC
Oza and colleagues ASCO 2015
In combination con carboplatin, promosing activity in “platinum-
resistant” disease with p53 mutations.

Leverage
DNA damage
response
(DDR)
New opportunities…..
Clinical Synthetic Lethality
Targeting the molecular and
microenvironmental
characteristics of tumor
Endogenous tumor factors
HRD
TP53
Cell cycle regulation
Exogenous tumor factors
Hypoxia
Immune activation
Glucose metabolism
Chemical
synthetic
lethality
Contextual
synthetic
lethality
+

Ovarian Cancer
Immunogenic
T cell infiltration
affect outcome

Anti PD1/PDL1
-ORR 15%
-Very rarely long lasting responses
Other Studies
-Disis et Al, Avelumab: ORR 9.7%
-Brahmer et al, Nivolumab: 17 pts, 1 PR, 2 SD

Leverage
DNA damage
response
(DDR)
Testing the hypothesis: PARPi + Immunotherapy
Targeting the molecular and
microenvironmental
characteristics of tumor
Endogenous tumor factors
HRD
TP53
Cell cycle regulation
Exogenous tumor factors
Hypoxia
Immune activation
Glucose metabolism
Chemical
synthetic
lethality
Contextual
synthetic
lethality
+
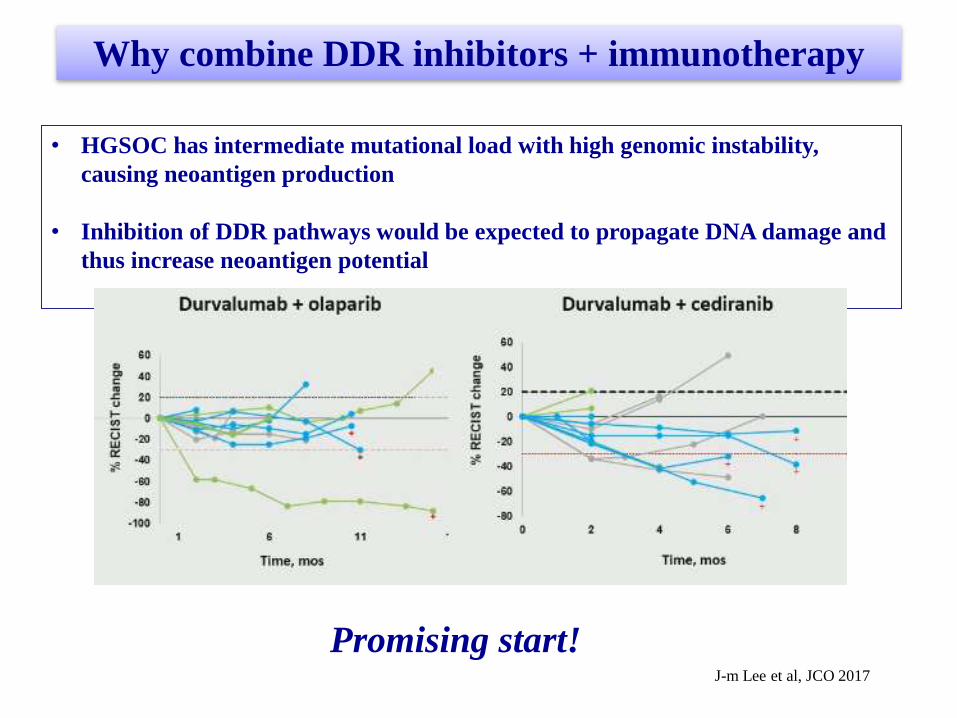
Why combine DDR inhibitors + immunotherapy
• HGSOC has intermediate mutational load with high genomic instability,
causing neoantigen production
• Inhibition of DDR pathways would be expected to propagate DNA damage and
thus increase neoantigen potential
Promising start!
J-m Lee et al, JCO 2017

On going Clinical Trials

The range of
DNA
opportunities
Combine with
other DNA
repair targets
Cell cycle
dysregulation
Epigenetic
generation of
HRD
Hypoxia
Immunotherapy
combinations

?
?
?
?
? ?
?
?
Navigating the new information….
Options likely will increase in tandem with our
understanding as long as we keep asking relevant
questions….
Is it possible to prospectively profile tumors to guide therapy choice?
Individualized Medicine in Ovarian Cncer: Are we there yet?

OC is a tumor where new knowledge has changed the landscape
Treatment according to histotype and molecular definitions is the future!
Antiangiogenic agents and parp inhibitors are changing the natual history
of ovarian cancer disease.
Understanding DNA repair and DDR continues to evolve and offers
opportunities for therapeutic intervention, leveraging clinical synthetic
lethality
Defining combination therapies with the optimal potential to be synthetic
lethal
Further defining biomarkers, beyond BRCA, to more effectively select
patients for individualized medicine in ovarian cancer
Conclusions
Thanks!