La Nefrologia nel Paziente Critico - ante.it Ante 2010/10 La... · Direttore Scientifico Seminario...
34
Dr. Filippo Aucella Direttore Scientifico Seminario ANTE 2010 Direttore S. C. di Nefrologia e Dialisi, IRCCS “Casa Sollievo della Sofferenza” San Giovanni Rotondo La Nefrologia nel Paziente Critico
-
Upload
nguyenxuyen -
Category
Documents
-
view
213 -
download
0
Transcript of La Nefrologia nel Paziente Critico - ante.it Ante 2010/10 La... · Direttore Scientifico Seminario...

Dr. Filippo AucellaDirettore Scientifico Seminario ANTE 2010
Direttore S. C. di Nefrologia e Dialisi, IRCCS “Casa Sollievo della Sofferenza”San Giovanni Rotondo
La Nefrologia nel
Paziente Critico








Criteria for consideration of BP
• Progressive deterioration despite intensive support therapy;
• Depression of midbrain function: hypoventivation, hypothermia, hypotension;
• Complications of coma;
• Impairment of normal drug excretory function: hepatic, cardiac, renal failure;
• Agents with delayed effects (mushrooms or paraquat) ;
• Hepatic failure (?)
• ESRD and Al intoxication ;
• Regional HP for anticancer drug toxicity.

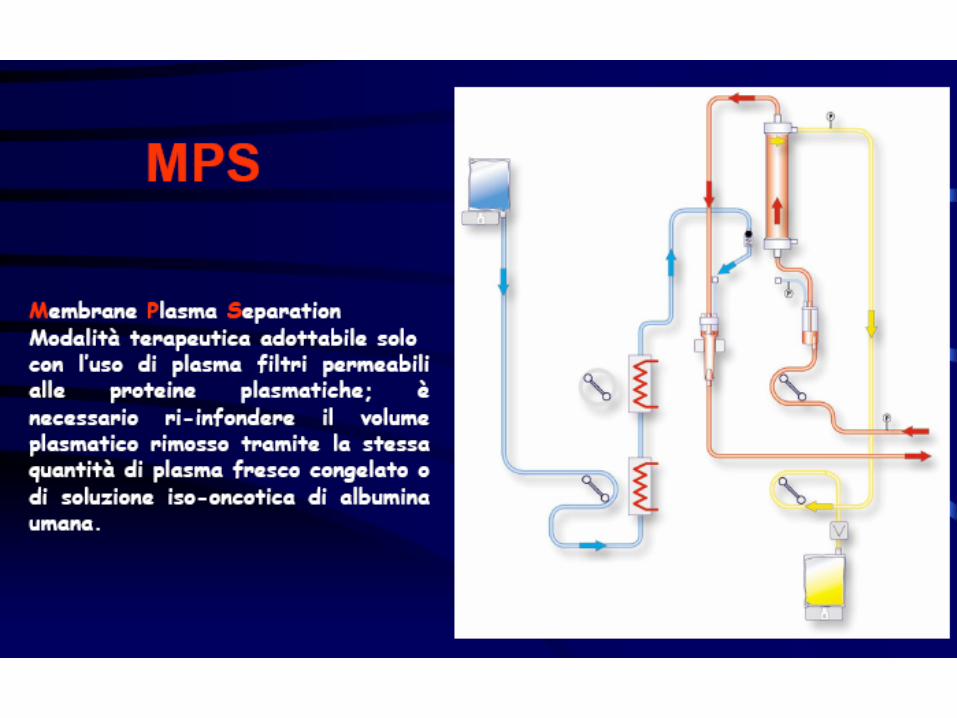
Choosing between HD or HP
Toxin characteristics
• Low molecular weight HD
• High molecular weight HP
• Water solubility HD
• Lipid solubility HP
• Low protein binding HD
• High protein binding HP
Patients characteristics
• Renal failure HD
• Acid-base problems HD
• Electrolytes problems HD
• Hypotension HP
• Haemodynamic instability HP
• Low platelet count HD



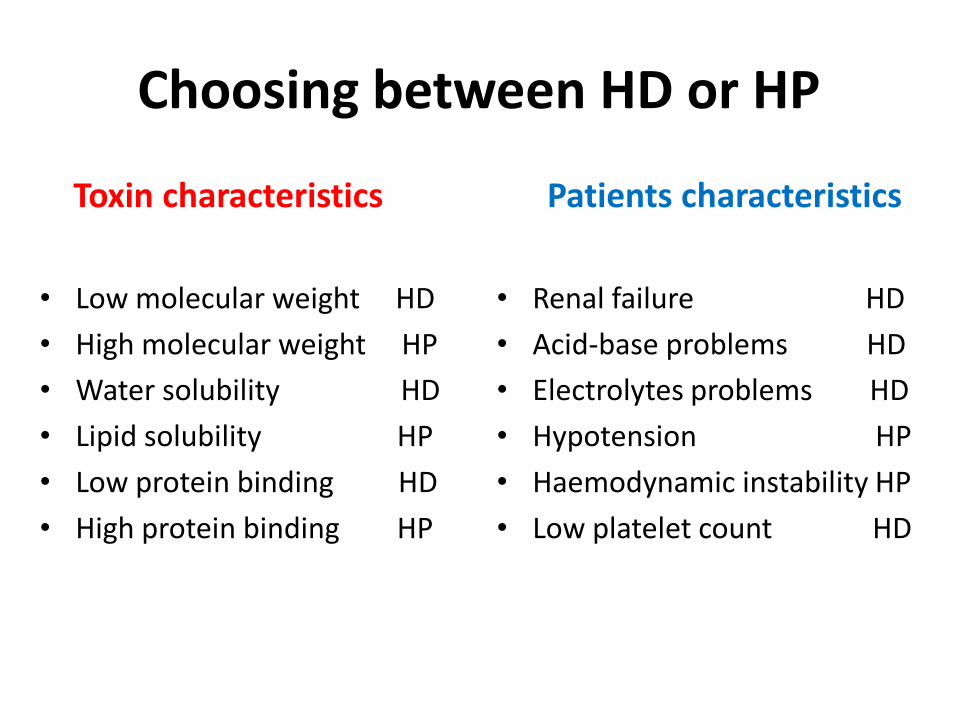
In vitro removal of therapeutic drugs with a novel adsorbent system
Reiter K et al, Blood Purif 2002
BetaSorb™ is designed as an
adjunctive treatment to traditional
high-flux HD. Target are MMW
toxins not cleared well by HD. The
marker is β2μ. Studies show that
reduced levels of β2μ lead to a
reduction in morbidities like
amyloidosis, hospital stays, and
lowers mortality rates compared to
patients on high-flux HD.
Effective removal of:
• Digoxin
• Theophylline
• Phenobarbital
• Phenytoin
• Carbamazepine
• Valproic acid
• Glycopeptide antibiotics
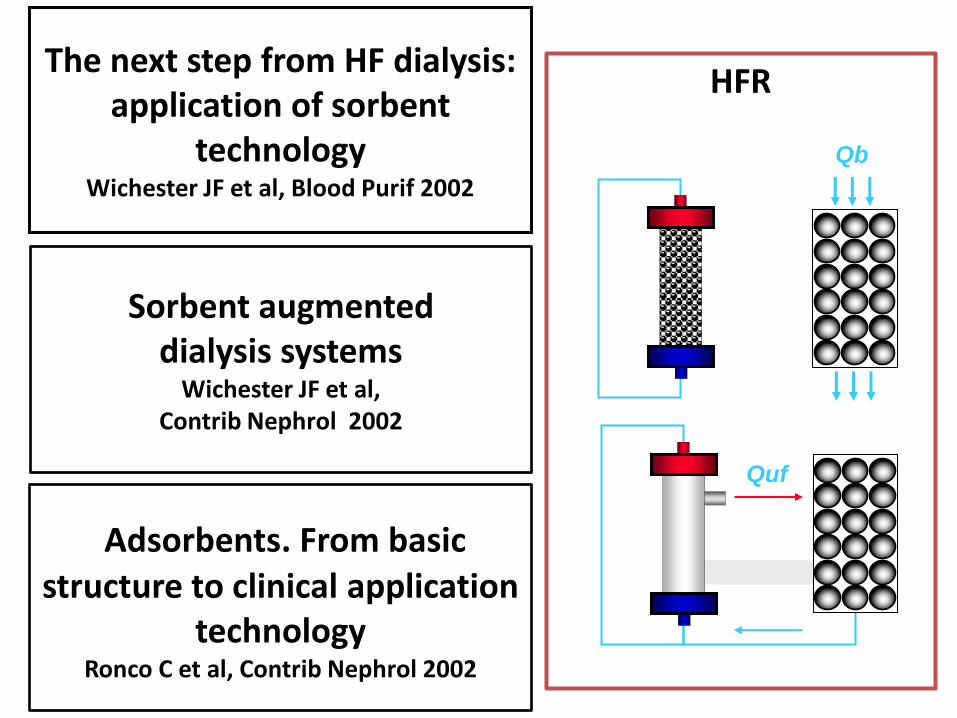
The next step from HF dialysis: application of sorbent
technologyWichester JF et al, Blood Purif 2002
Sorbent augmenteddialysis systems
Wichester JF et al, Contrib Nephrol 2002
Adsorbents. From basicstructure to clinical application
technologyRonco C et al, Contrib Nephrol 2002
Qb
Quf
HFR







Renal Dysfunction is Common in Patients with Acute Decompensated Heart Failure (n = 105,388)
0
10
20
30
40
50
<15 15-29 30-59 60-89 >90
Estimated GFR, ml/min
Pati
en
ts (
%)
Heywood JT, et al. Heart Failure Reviews 2004
80% of patients have at least
moderate renal dysfunction
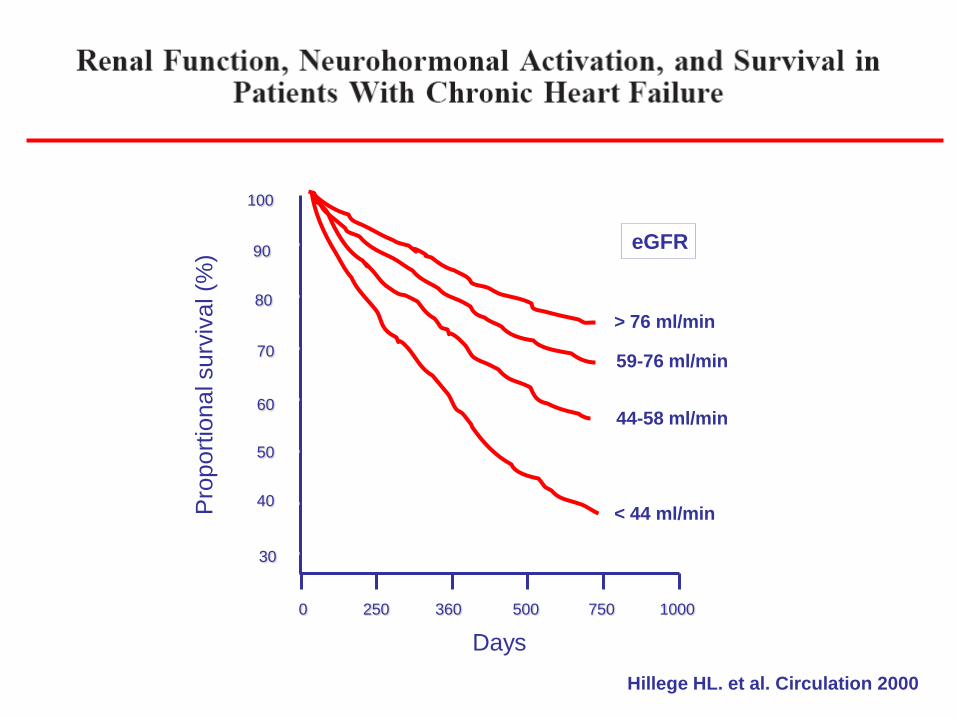
Hillege HL. et al. Circulation 2000
Days
100
90
80
70
60
50
40
30
0 250 360 500 750 1000
> 76 ml/min
59-76 ml/min
44-58 ml/min
< 44 ml/minPro
port
ional surv
ival (%
)
eGFR
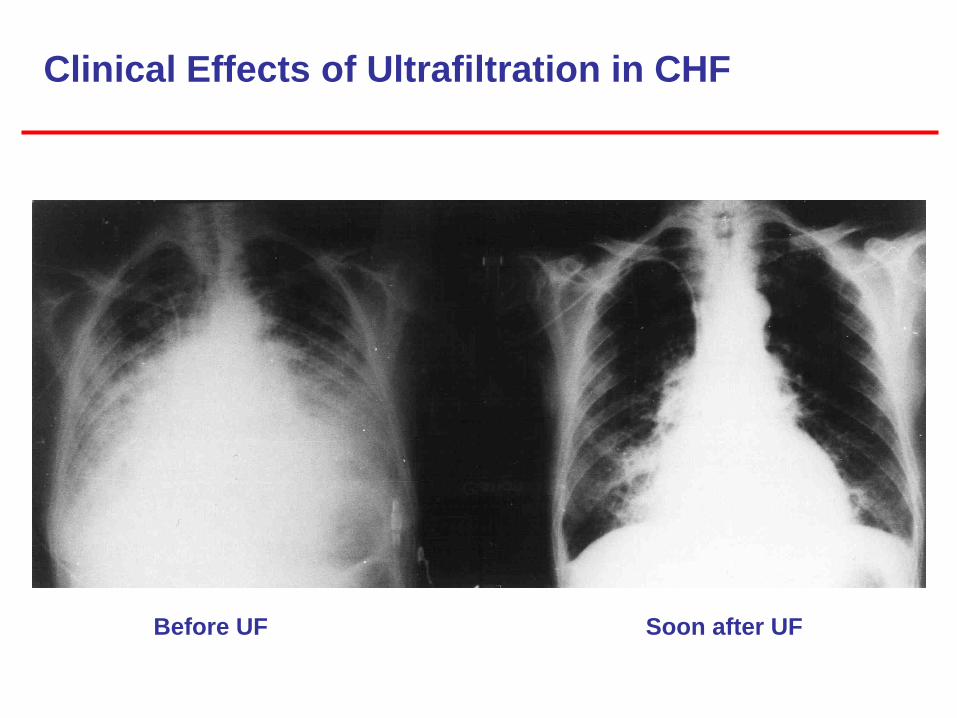
Clinical Effects of Ultrafiltration in CHF
Before UF Soon after UF

“Mini-invasive” Ultrafiltration

Costanzo MR for the UNLOAD invest. JACC 2007

Giorni di ospedalizzazioneG
IOR
NI D
I
RIC
OV
ER
O
GIO
RN
I D
I
RIC
OV
ER
O
MESIINIZIO D.P. MESIINIZIO D.P.
Ricoveri per motivi cardiologici
Ricoveri per complicanze della D.P.
P<0,05 P<0,05

Frazione di eiezioneF
RA
ZIO
NE
DI
EIE
ZIO
NE
(%
)
INIZIO D.P. 4 MESI 8 MESI 12 MESI
0
10
20
30
40
50
60
FE
%
Inizio DP 4 mesi 8 mesi 12 mesi

Funzionalità renaleC
RE
AT
ININ
A (
mg
/dl)
INIZIO D.P. 3 MESI 6 MESI 12 MESI9 MESI
INIZIO D.P. 3 MESI 6 MESI 12 MESI9 MESI
UR
EA
(m
g/d
l)