La gestione terapeutica delle MICI in Pediatria: un update. · delle MICI in Pediatria: un update....
53
La gestione terapeutica delle MICI in Pediatria: un update. Paolo Lionetti
-
Upload
trinhkhanh -
Category
Documents
-
view
218 -
download
0
Transcript of La gestione terapeutica delle MICI in Pediatria: un update. · delle MICI in Pediatria: un update....

La gestione terapeutica delle MICI in Pediatria:
un update.
Paolo Lionetti

The Paediatric IBD Porto Group
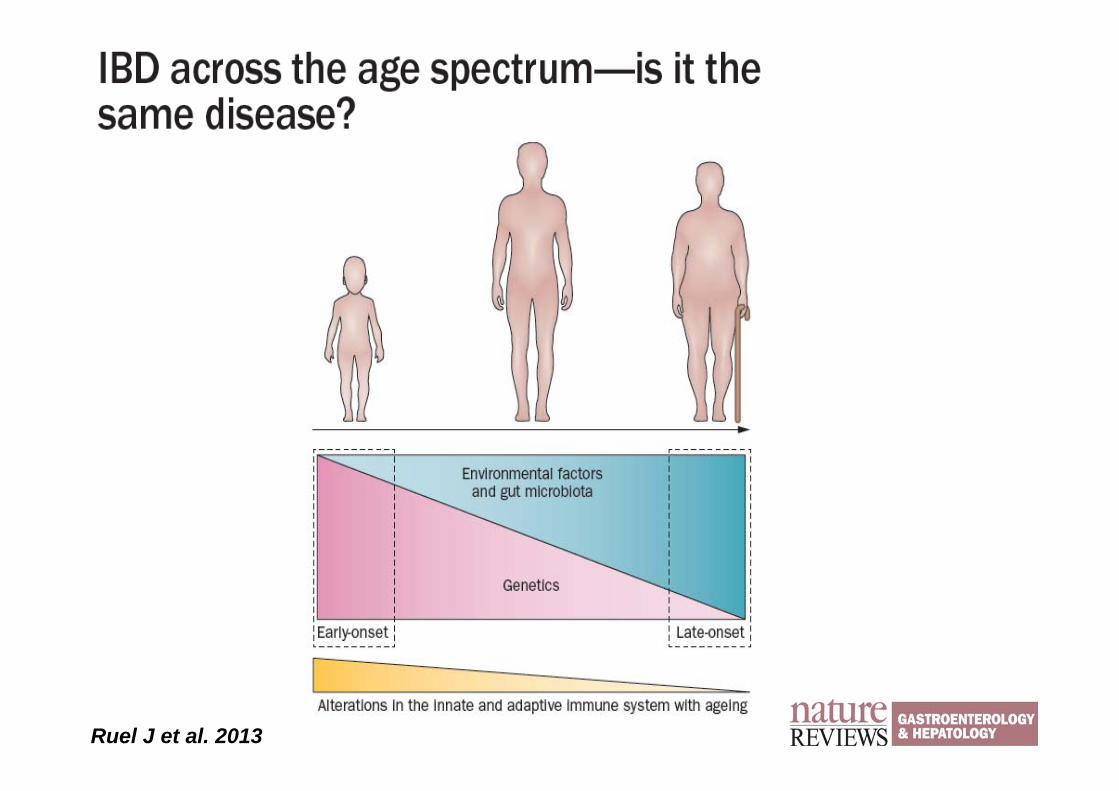
Ruel J et al. 2013
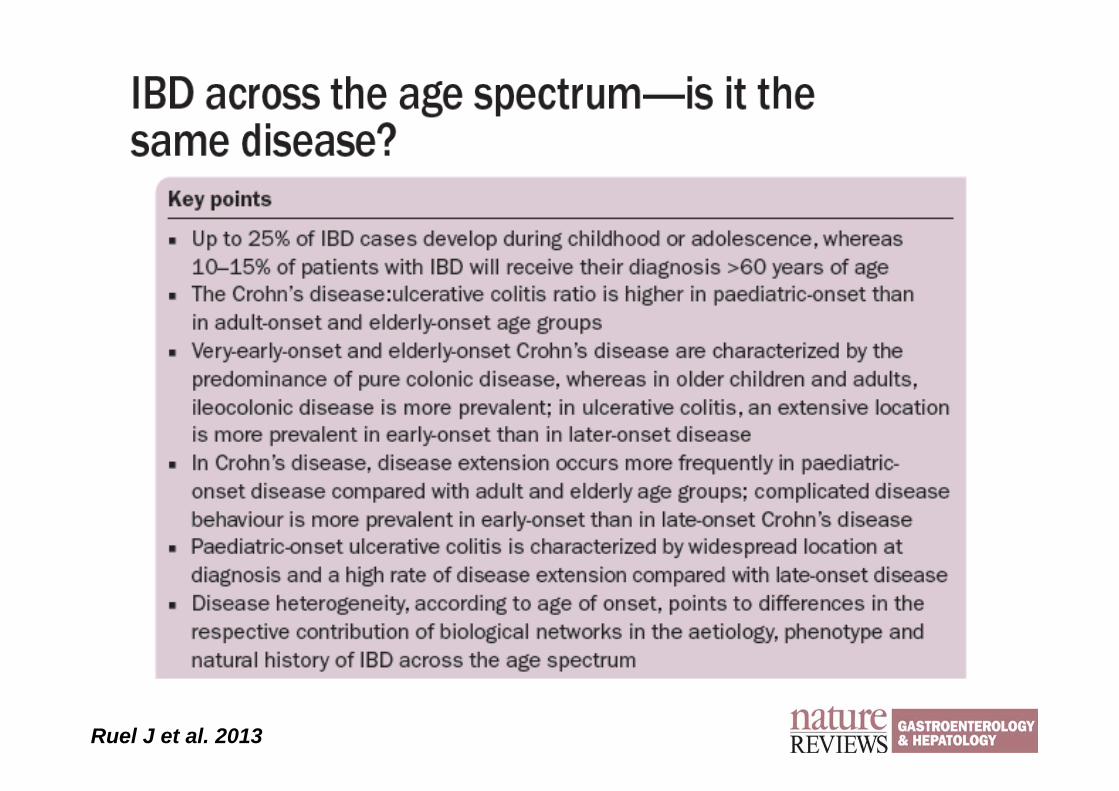
Ruel J et al. 2013
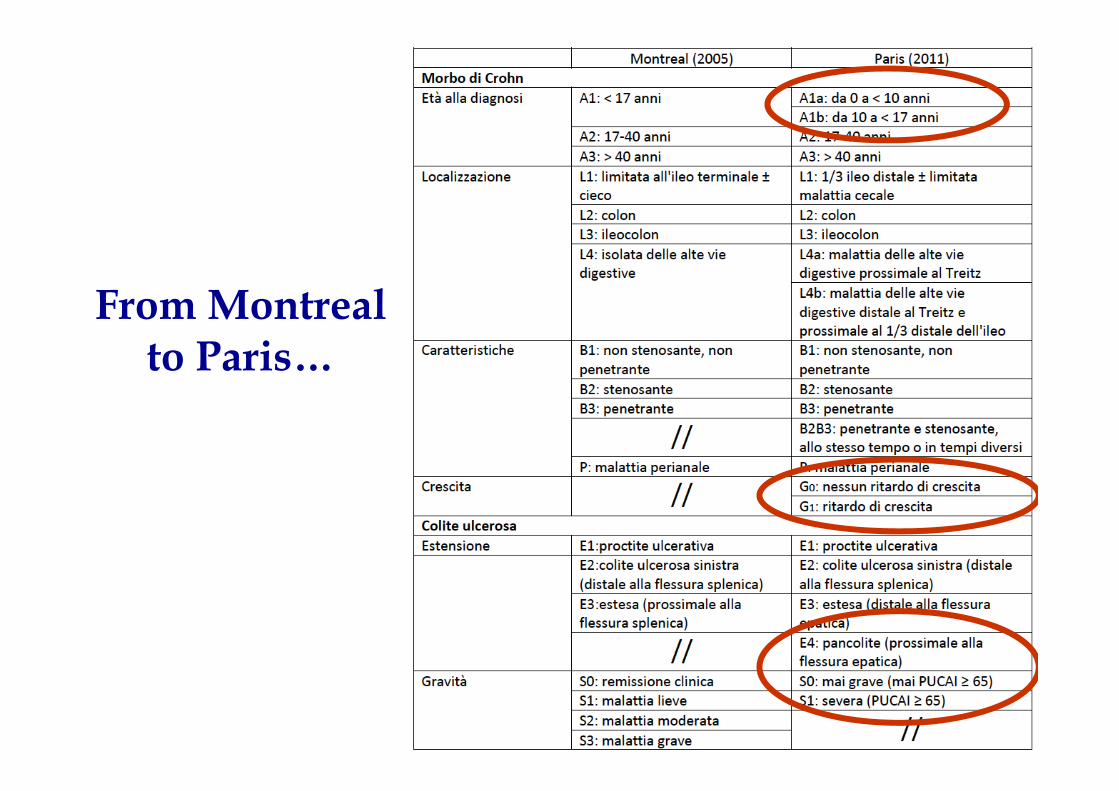
From Montreal to Paris…
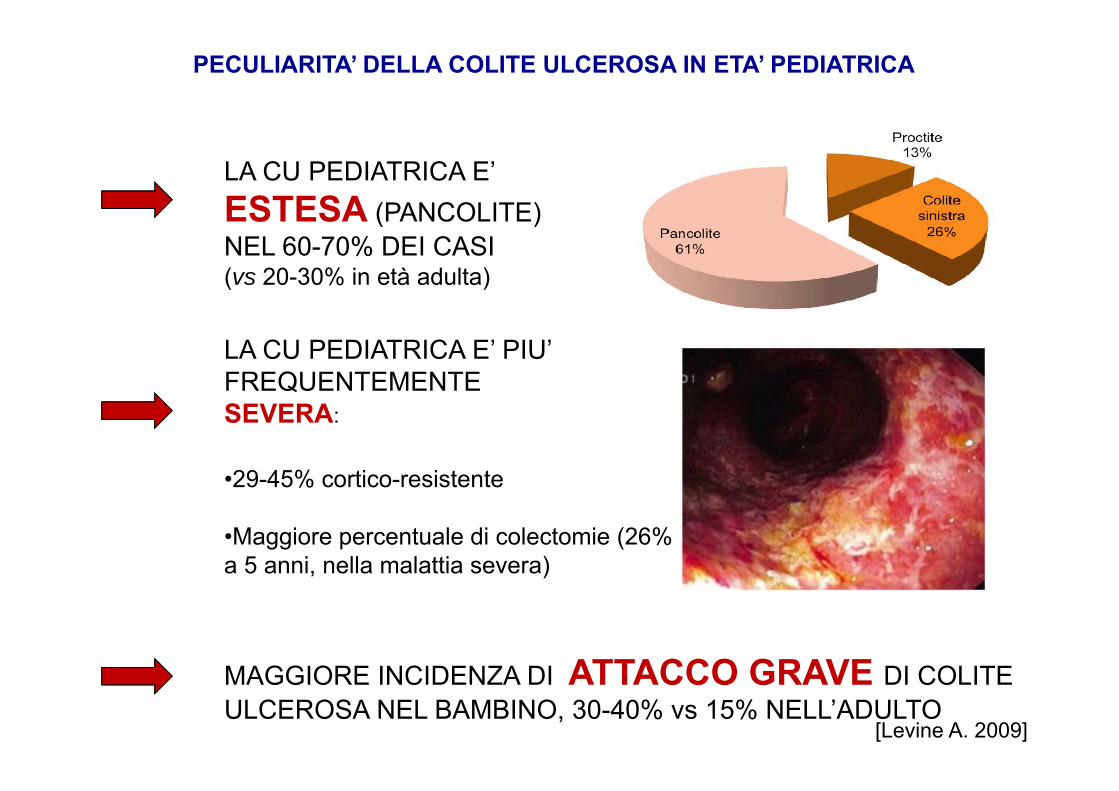
LA CU PEDIATRICA E’ ESTESA (PANCOLITE) NEL 60-70% DEI CASI (vs 20-30% in età adulta)
•29-45% cortico-resistente
•Maggiore percentuale di colectomie (26% a 5 anni, nella malattia severa)
PECULIARITA’ DELLA COLITE ULCEROSA IN ETA’ PEDIATRICA
MAGGIORE INCIDENZA DI ATTACCO GRAVE DI COLITE ULCEROSA NEL BAMBINO, 30-40% vs 15% NELL’ADULTO
LA CU PEDIATRICA E’ PIU’ FREQUENTEMENTESEVERA:
[Levine A. 2009]
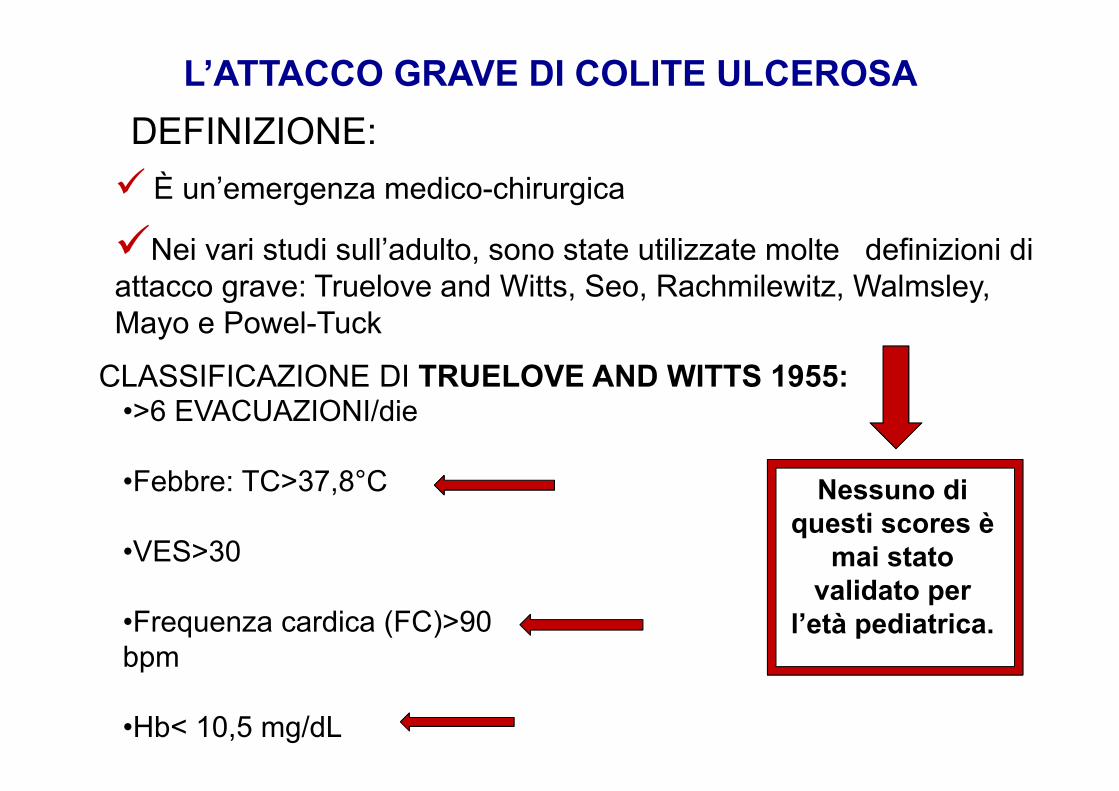
L’ATTACCO GRAVE DI COLITE ULCEROSA
CLASSIFICAZIONE DI TRUELOVE AND WITTS 1955:•>6 EVACUAZIONI/die
•Febbre: TC>37,8°C
•VES>30
•Frequenza cardica (FC)>90 bpm
•Hb< 10,5 mg/dL
Nessuno di questi scores è
mai stato validato per
l’età pediatrica.
Nei vari studi sull’adulto, sono state utilizzate molte definizioni di attacco grave: Truelove and Witts, Seo, Rachmilewitz, Walmsley, Mayo e Powel-Tuck
DEFINIZIONE: È un’emergenza medico-chirurgica
The Paediatric IBD Porto Group
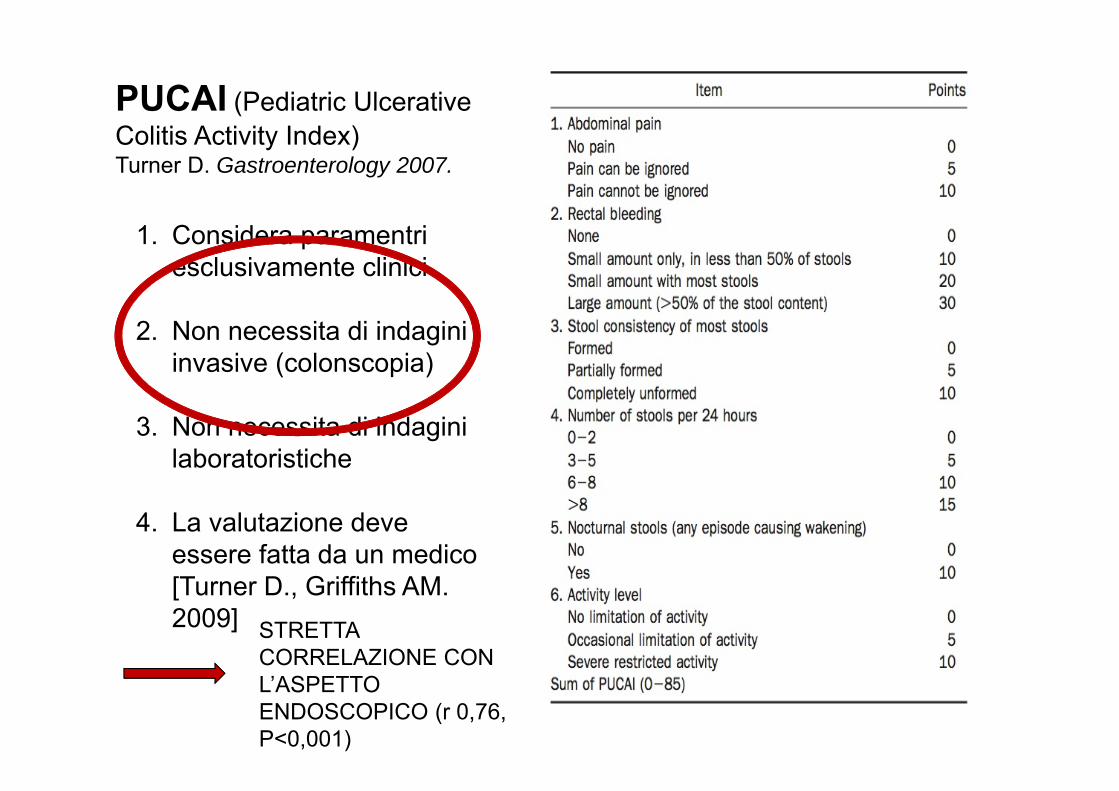
PUCAI (Pediatric Ulcerative Colitis Activity Index) Turner D. Gastroenterology 2007.
1. Considera paramentri esclusivamente clinici
2. Non necessita di indagini invasive (colonscopia)
3. Non necessita di indagini laboratoristiche
4. La valutazione deve essere fatta da un medico [Turner D., Griffiths AM. 2009] STRETTA
CORRELAZIONE CON L’ASPETTO ENDOSCOPICO (r 0,76, P<0,001)
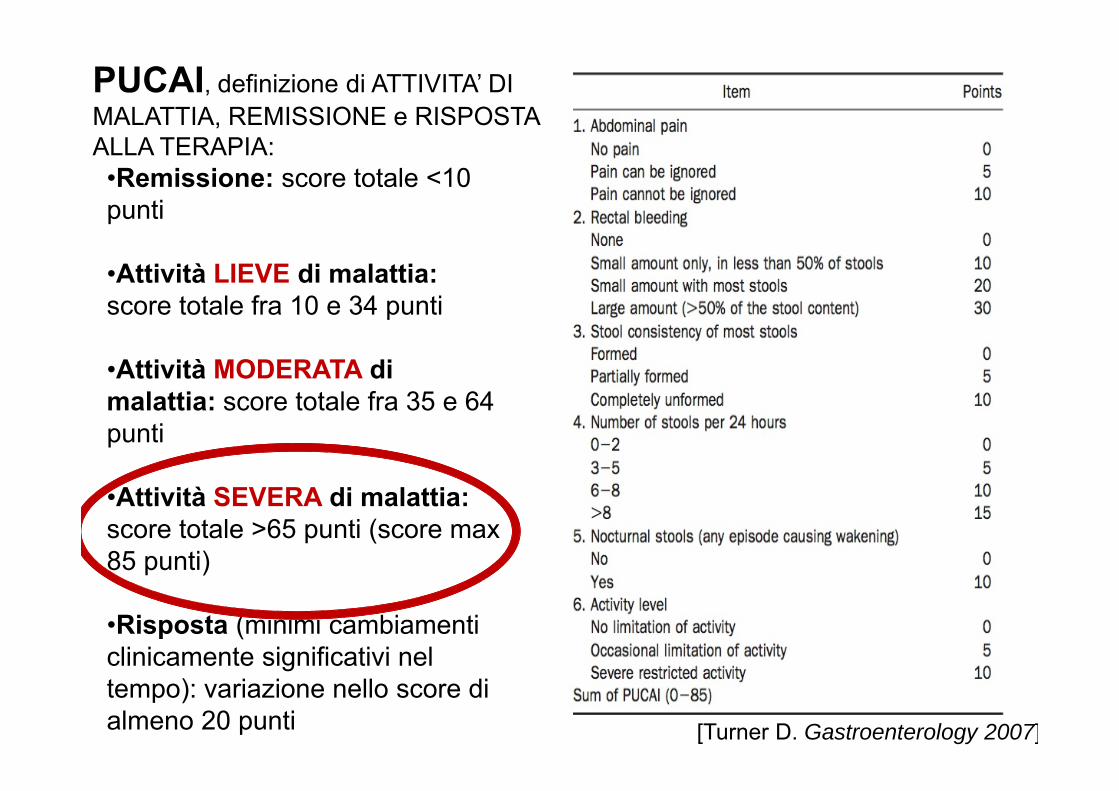
PUCAI, definizione di ATTIVITA’ DI MALATTIA, REMISSIONE e RISPOSTA ALLA TERAPIA:•Remissione: score totale <10 punti
•Attività LIEVE di malattia: score totale fra 10 e 34 punti
•Attività MODERATA di malattia: score totale fra 35 e 64 punti
•Attività SEVERA di malattia: score totale >65 punti (score max 85 punti)
•Risposta (minimi cambiamenti clinicamente significativi nel tempo): variazione nello score di almeno 20 punti [Turner D. Gastroenterology 2007]
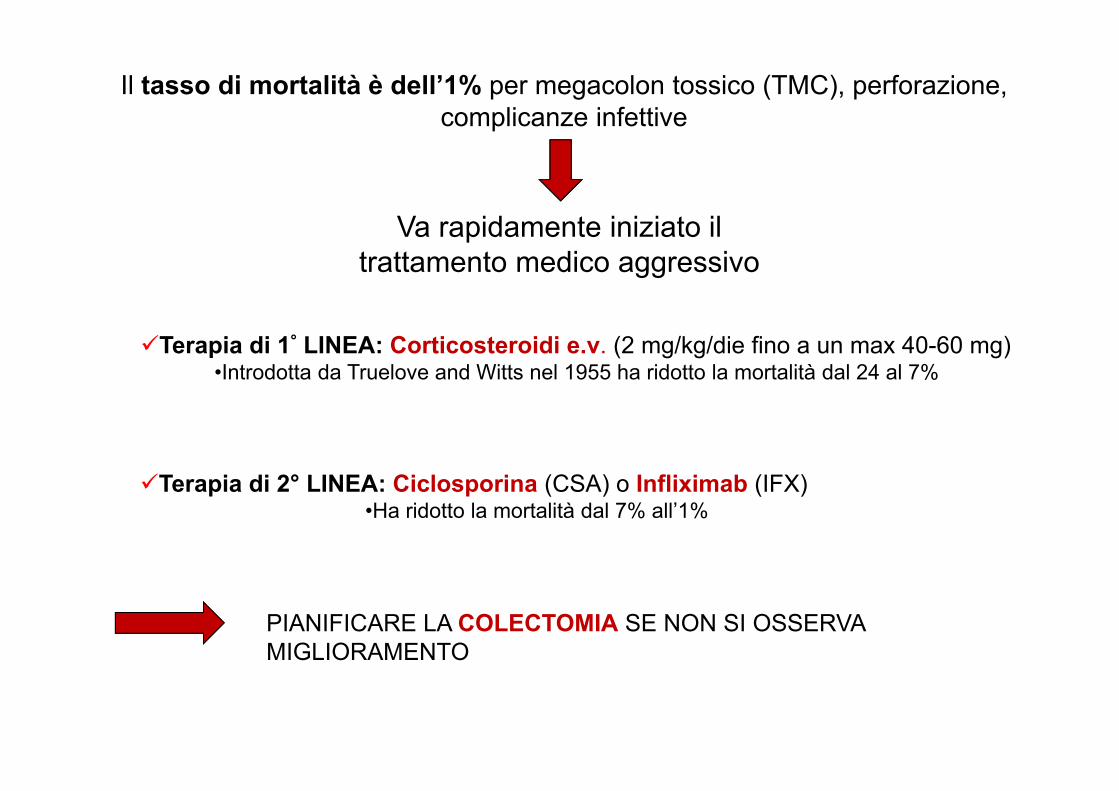
Il tasso di mortalità è dell’1% per megacolon tossico (TMC), perforazione, complicanze infettive
Va rapidamente iniziato il trattamento medico aggressivo
Terapia di 1° LINEA: Corticosteroidi e.v. (2 mg/kg/die fino a un max 40-60 mg)•Introdotta da Truelove and Witts nel 1955 ha ridotto la mortalità dal 24 al 7%
Terapia di 2° LINEA: Ciclosporina (CSA) o Infliximab (IFX)•Ha ridotto la mortalità dal 7% all’1%
PIANIFICARE LA COLECTOMIA SE NON SI OSSERVA MIGLIORAMENTO

Acute severe ulcerative colitis:
Monitoring of disease activity during admission (100% consensus)
Initial treatmentCorticosteroid (100% consensus)
Acute severe ulcerative colitis: the pediatric perspective
When to introduce a second line treatment ?
CyA or Infliximab ?
When treatment success or failure should be determined in children on second line medical treatment

RETTOSCOPIA
Quadro compatibile con COLITE ULCEROSA con segni di attività endoscopica

PUCAI giorno 1
85
PUCAI ≥ 65 severe disease
(sensitivity 92%, specificity 94%)
RIVALUTAZIONE 3°E 5° GIORNO
Inflamm Bowel Dis 2011;17:440–449
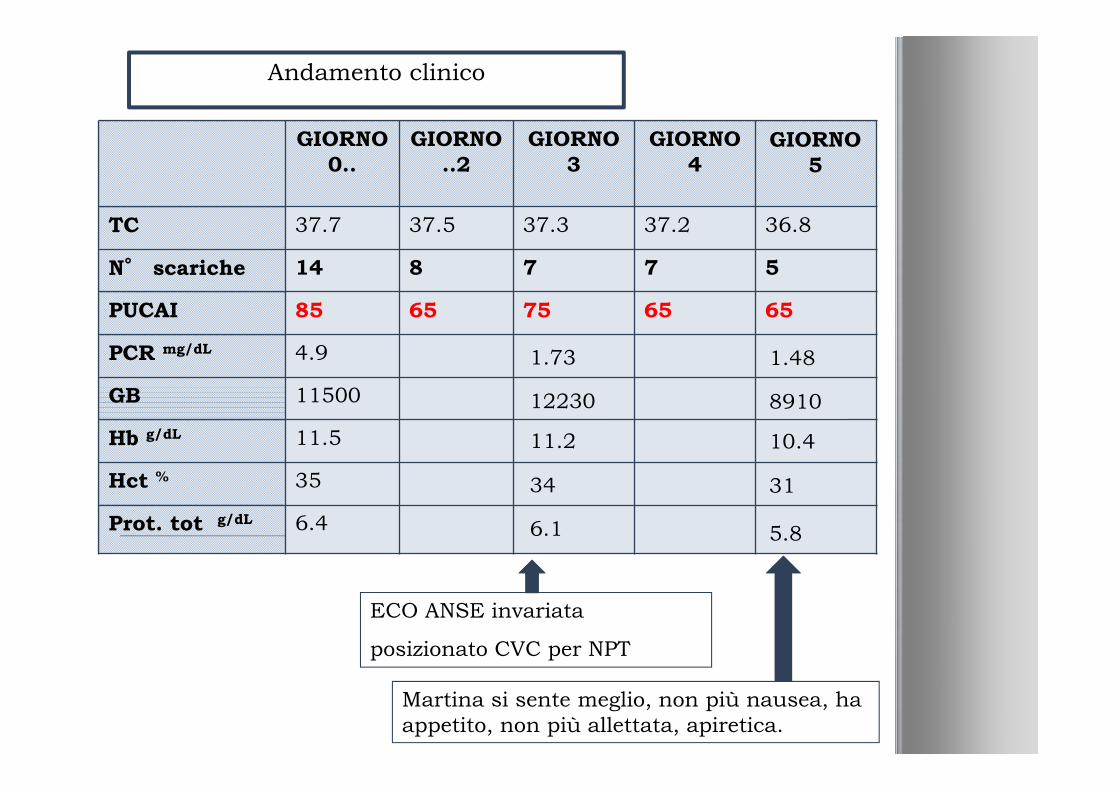
GIORNO 0..
GIORNO ..2
GIORNO 3
GIORNO 4
TC 37.7 37.5 37.3 37.2 36.8
N° scariche 14 8 7 7 5
PUCAI 85 65 75 65 65
PCR mg/dL 4.9
GB 11500
Hb g/dL 11.5
Hct % 35
Prot. tot g/dL 6.4
Andamento clinico
ECO ANSE invariata
posizionato CVC per NPT
Martina si sente meglio, non più nausea, ha appetito, non più allettata, apiretica.
1.73
12230
11.2
34
6.1
1.48
8910
10.4
31
5.8
GIORNO 5
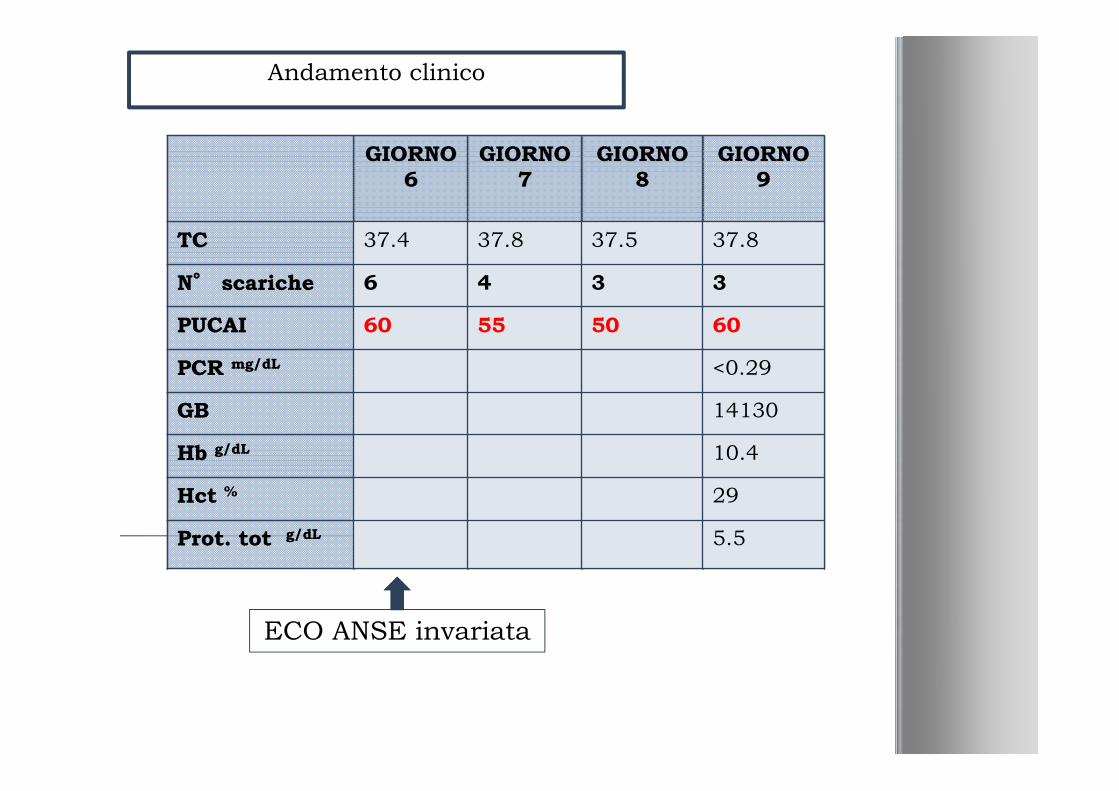
Andamento clinico
ECO ANSE invariata
GIORNO 6
GIORNO 7
GIORNO 8
GIORNO 9
TC 37.4 37.8 37.5 37.8
N° scariche 6 4 3 3
PUCAI 60 55 50 60
PCR mg/dL
GB
Hb g/dL
Hct %
Prot. tot g/dL
GIORNO 6
GIORNO 7
GIORNO 8
GIORNO 9
TC 37.4 37.8 37.5 37.8
N° scariche 6 4 3 3
PUCAI 60 55 50 60
PCR mg/dL <0.29
GB 14130
Hb g/dL 10.4
Hct % 29
Prot. tot g/dL 5.5

Andamento clinico
Passa steroide per osInizio alimentazioneper os e riduce NP
Dimissione
GIORNO 10
GIORNO 11
GIORNO 12..
GIORNO ..14..
GIORNO ..17
TC 37 36.2 36.4 36.2 36.2
N° scariche 1 4 2 1 1
PUCAI 45 25 20 5 0
PCR mg/dL
GB
Hb g/dL
Hct %
Prot. tot g/dL
GIORNO 10
GIORNO 11
GIORNO 12..
GIORNO ..14..
GIORNO ..17
TC 37 36.2 36.4 36.2 36.2
N° scariche 1 4 2 1 1
PUCAI 45 25 20 5 0
PCR mg/dL <0.29
GB 12980
Hb g/dL 11
Hct % 32
Prot. tot g/dL 6.8
INFLIXIMAB
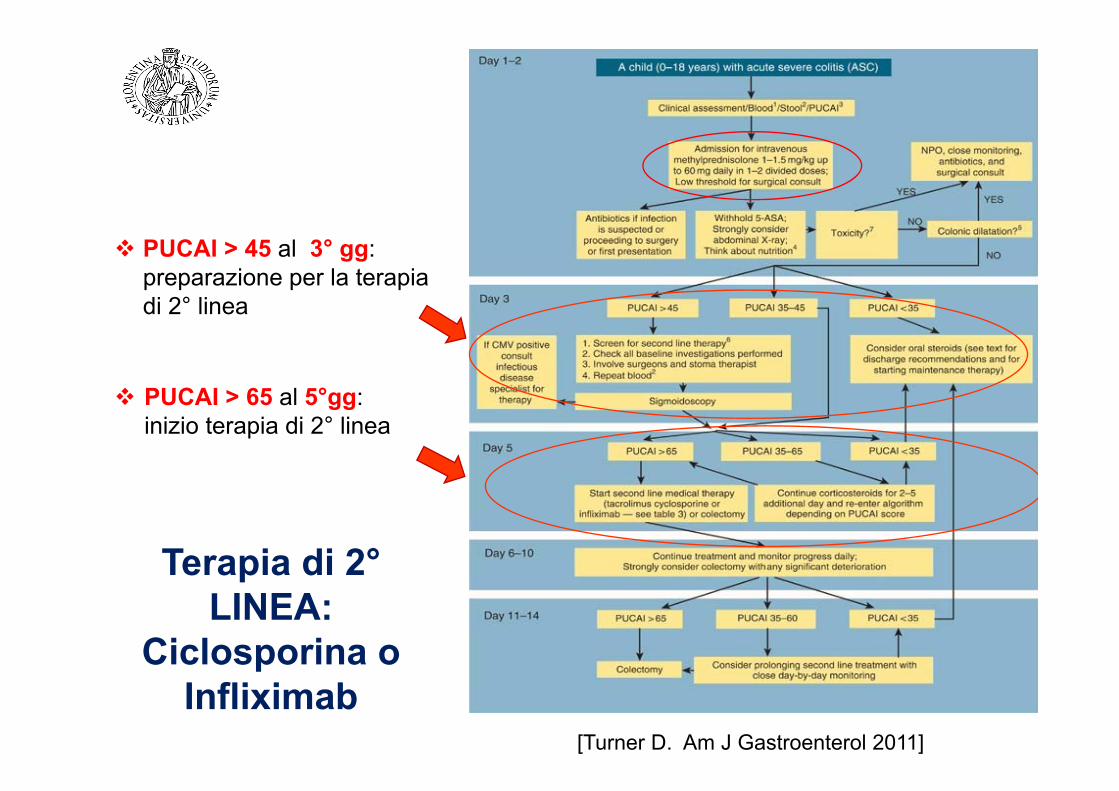
[Turner D. Am J Gastroenterol 2011]
PUCAI > 45 al 3° gg: preparazione per la terapia di 2° linea
PUCAI > 65 al 5°gg: inizio terapia di 2° linea
Terapia di 2°LINEA:
Ciclosporina o Infliximab

0,00%0,00%
12,50%
7,10%
0,00%
4,20%3,60%
8,30%
9,70%
4,40%
2%
12,20%
10,30%
8,60%
2,40%
0,00%
2,60%
6,70%
5%
0,80%0,70%
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
PERCENTUALE DI ATTACCHI GRAVI RISPETTO AL TOTALE DEI PAZIENTI SEGUITI PER CU PER ANNO
18 attacchi/166 pazienti (13,5%)
42 attacchi/125 pazienti (33,6%)
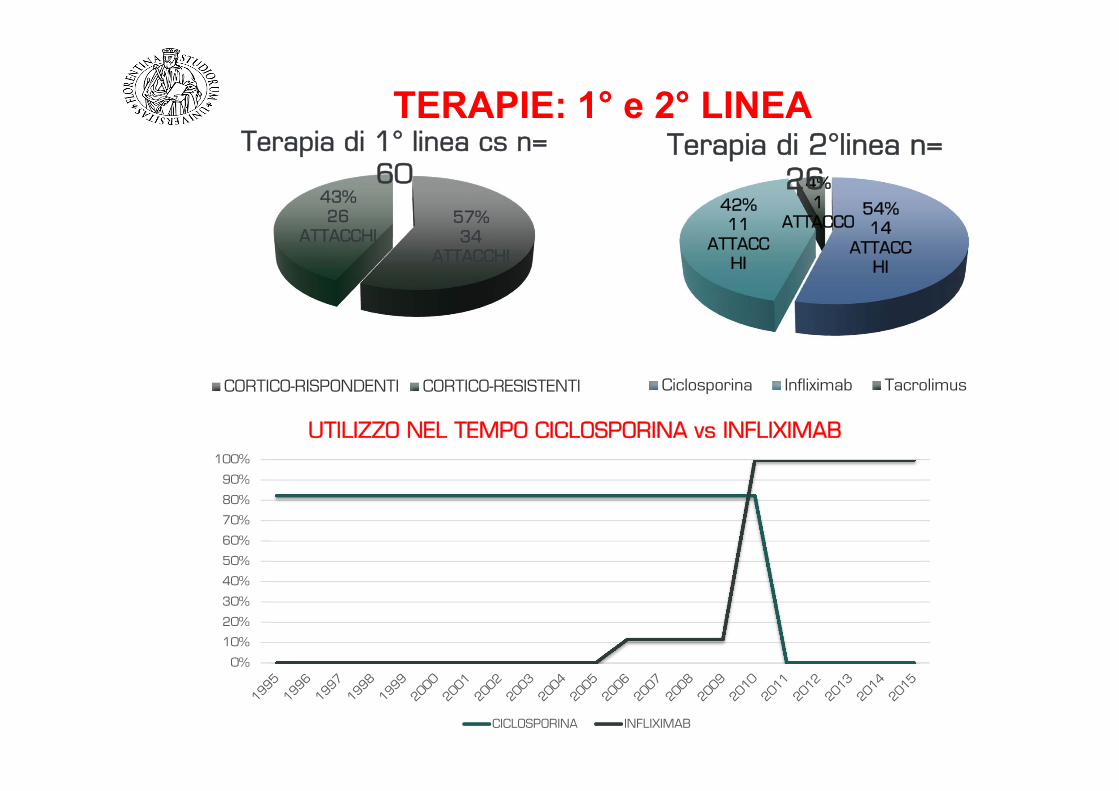
57%34
ATTACCHI
43%26
ATTACCHI
Terapia di 1° linea cs n= 60
CORTICO-RISPONDENTI CORTICO-RESISTENTI
54%14
ATTACCHI
42%11
ATTACCHI
4%1
ATTACCO
Terapia di 2°linea n= 26
Ciclosporina Infliximab Tacrolimus
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
UTILIZZO NEL TEMPO CICLOSPORINA vs INFLIXIMAB
CICLOSPORINA INFLIXIMAB
TERAPIE: 1° e 2° LINEA

Is there a preferred surgery in children ?
The pouch procedures (i.e., ileoanal pouch or ileal pouch– anal anastomosis), also known as “restorative proctocolectomy,” are likely superior to a straight pullthrough (i.e., ileoanal anastomosis) because they are associated with acceptable early complication rates, lower early stool frequency, and better long-term continence.
Ileorectal anastomosis cannot be recommended for most children because of the high rate of failure, requiring removal of the remaining rectum.
The advantages of the restorative proctocolectomy need to be balanced against the risk of chronic pouchitis and reduced fertility.
Joint ECCO and ESPGHAN evidence-based consensus guidelines
J. Pediatr. Gastroenterol. Nutr. 2012 Sep; 55(3): 340-61
Joint ECCO and ESPGHAN evidence-based consensus guidelines on the management
of pediatric ulcerative colitis
1.Endoscopic evaluation is recommended at diagnosis, before major treatment changes and when the clinical assessment is in question; endoscopic evaluation in children is not routinely recommended during flares which are not severe or during clinical remission aside from cancer surveillance [EL4, RG C]
Joint ECCO and ESPGHAN evidence-based consensus guidelines on the management
of pediatric ulcerative colitis
Biologics 1.Infliximab should be considered for treatment of children
with persistently active, or steroid-dependent UC, uncontrolled by 5-ASA and thiopurines [Pediatrics EL1b RG B, Adults EL1b, RG B]
2.Infliximab may be considered for steroid-refractory (whether oral or intravenous) disease. If infliximab has been initiated during an acute episode in a thiopurine-naïve patient, it can be used as a bridge to thiopurine. In that case, infliximab may be discontinued after approximately 4-8 months [Pediatrics EL4, RG C, Adults EL1b, RG B]
3.Adalimumab should only be used in those who lost response or were intolerant to infliximab [Pediatrics EL4, RG C , Adults EL1b, RG B]
Therapy goals
The aims of therapy in pediatric CD traditionally have been:• relieve symptoms• optimize growth• improve quality of life • while minimizing drug toxicity.
The notion that achieving mucosal healing may potentially change the natural history of the disease and decrease the need for surgery has placed “deep remission” (meaning mucosal healing) in the center of interest as being the desired treatment target.

Therapy goals
• Early treatment with biologics and immunomodulatory agents improve rates of mucosal healing and clinical remission in adults and in pediatric CD patients.
• Induction of complete mucosal healing with IFX in early‐stage CD predicted sustained clinical remission and steroid‐free remission in adults
• The risks and benefits of treat to target strategies when patients are in remission are still controversial
• Evidence to base firm recommendations for:‐escalating medical therapy to achieve this target in low risk patients‐selection of patients for early aggressive immunotherapyremains difficult to ascertain.
Therapy goals
• The necessary degree of mucosal healing and the necessary depth of transmural healing are still unclear.
• Pediatric MRI‐based inflammatory and damage scores are under development, similar to the MaRIA and Lemann‐scores developed for adult CD, and offer the opportunity to evaluate more than simply mucosal healing
• Non‐invasive biomarkers of mucosal healing such as fecal calprotectin are particularly useful for children to monitoring resolution or recurrence of intestinal inflammation, but the cutoff value in each scenario that should trigger change in management is still elusive.
Therapy goals
• Linear growth impairment is a unique feature of pre‐pubertal pediatric patients with CD and is mainly a consequence of chronic inflammation.
• Peak bone mass, reached by late adolescence, acts as the "bone bank" for life and is decreased in approximately half of children with CD, especially in those malnourished.
• Growth and bone density restoration can be considered a marker of disease control and successful therapy in children, but this is not always achieved despite early introduction of immunomodulators and biologics.
• Failure to control inflammation and monitor linear growth and bone health may result in children not achieving their genetic growth
Therapy goals
• Although there are many arguments in favor of using early immunomodulatoryand biologic therapies to induce mucosal healing, the selection of ideal candidates who are at high‐risk for poor disease outcome must depend on predictive factors.
• The following factors can be considered as potentially predictive for poor outcome– deep colonic ulcerations on endoscopy– persistent severe disease despite adequate induction therapy – extensive (pan‐enteric) disease – marked growth retardation (> ‐2.5 height Z scores), – severe osteoporosis – stricturing and penetrating disease at onset
– severe perianal disease
• These factors suggestive of poor outcome should lead to optimization of therapy with agents that have been shown to modify the natural history of disease:immunomodulators, biologics or when appropriate surgical resection.
Induzione della remissione
Terapia nutrizionale
Steroidi Antibiotici
NUTRITIONAL THERAPY
• STATEMENT 1• Exclusive Enteral Nutrition (EEN) is recommended as first
line therapy to induce remission in children with active luminal CD [EL1] 96% agreement
• STATEMENT 2• Partial Enteral Nutrition should not be used for induction of
remission [EL2] 100% agreement
Terapia nutrizionale
• EEN and mucosal healing• Mucosal healing rates in children treated with EEN are reported in six
studies with 19% to 75%. Differences in the definition of mucosal healing in these studies limit the ability to summarize the results.
• The only RCT to include improvement in mucosal healing as an outcome of EEN compared with steroids demonstrated a clear superiority after 10 weeks of EEN with rates of 74% vs. 33%, respectively.
• Duration of remission after EEN is controversial in the literature with some studies showing shorter and some longer intervals to relapse as compared with steroids.
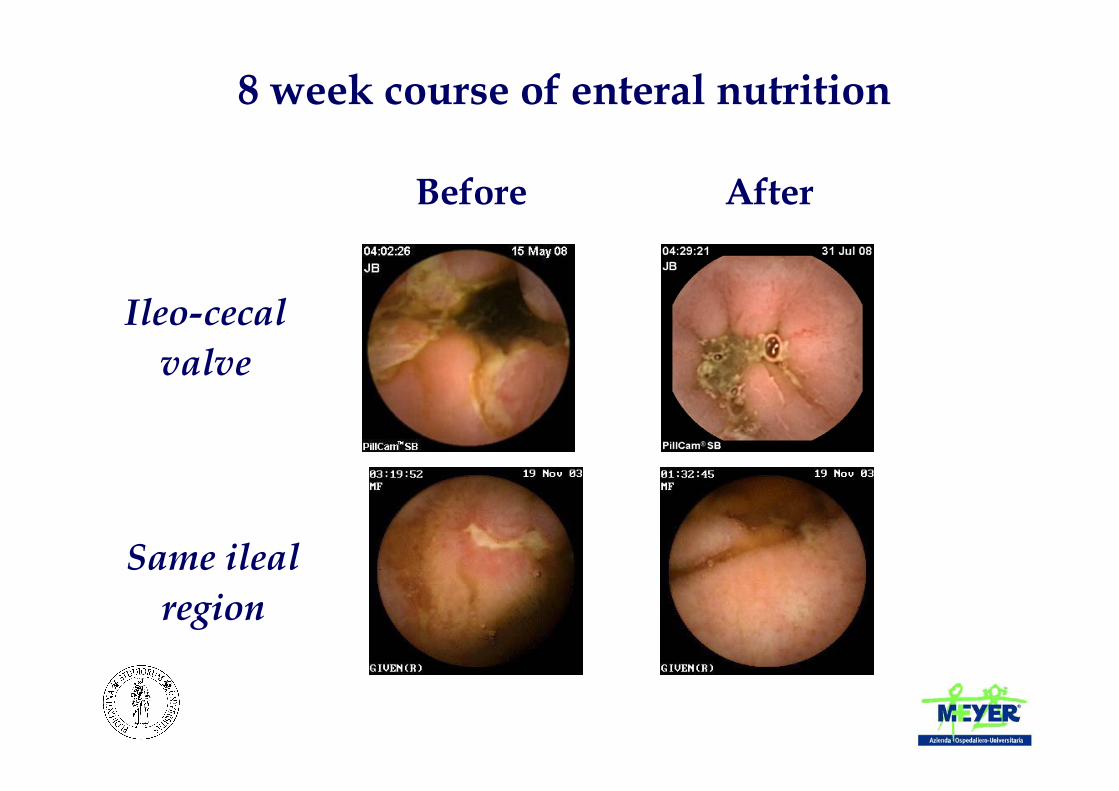
8 week course of enteral nutrition
Before After
Ileo-cecal valve
Same ileal region
GLUCOCORTICOSTEROIDS
• STATEMENT 3• Oral corticosteroids are recommended for inducing remission in children
with moderate to severe active luminal CD if EEN is not an option [EL2 (Pediatrics), EL1 (Adults)] 96% agreement
• STATEMENT 4• In children with mild to moderate ileo‐cecal CD, budesonide may be used
as alternative to systemic steroids for induction of remission [EL2 (Pediatrics) EL2 (Adults)] 96% agreement
• STATEMENT 5• Steroids should not be used as a maintenance therapy (EL4) 100%
agreement
Mantenimento remissione
Thiopurines
• STATEMENT 8• Thiopurines (azathioprine or 6‐mercaptopurine) are
recommended as one option for maintenance of steroid free remission in children at risk for poor disease outcome [EL2 (pediatrics), EL1 (adults) 96% agreement
• STATEMENT 9• Thiopurines alone are not recommended as induction
therapy (EL3) 100% agreement
METHOTREXATE
• STATEMENT 10• Methotrexate is recommended as one option for
maintenance of steroid free remission in children at risk for poor disease outcome (EL4 (Pediatrics) EL1 (adults)) 96% agreement
• STATEMENT 11• Methotrexate can be used as a primary maintenance
therapy or in thiopurine failure (EL 4 (Pediatrics), EL1 (Adults)) 92% agreement
Biologics (anti‐TNF therapy)
• STATEMENT 12• Anti‐TNF therapy is recommended for inducing and maintaining remission in children with
chronically active luminal CD despite prior optimized immunomodulator therapy (EL2) 100% agreement
• STATEMENT 13• Anti‐TNF therapy is recommended for inducing remission in children with active steroid‐
refractory disease (EL2) 100% agreement
• STATEMENT 14• Anti‐TNF therapy is recommended as primary induction and maintenance therapy for
children with active perianal fistulising disease in combination with appropriate surgical intervention [EL2] 84% agreement
• STATEMENT 15• Regularly scheduled and not episodic treatment should be used to maintain remission in
patients responding to induction therapy with anti‐TNF agents [EL2] 100% agreement
BiologicsPractice points:
1. Anti‐TNF therapy is the preferred strategy to treat active perianal fistulizing disease after appropriate medical (antibiotics) and surgical (e.g. fistula/abscess drainage, seton placement) management of the perianal lesions
2. Anti‐TNF therapy as primary induction therapy may be considered for selected children with high risk for poor outcome
3. Anti TNF‐agents should be considered early in the treatment plan for severe extraintestinal manifestations (e.g. severe arthritis, pyoderma gangrenosum).
4. Primary efficacy of anti‐TNF therapy should be evaluated after the second or third dose and should be discontinued if no significant response is observed (i.e. primary treatment failure)
5. Available data suggest that for patients previously naïve to anti‐TNF therapy, both IFX and ADA show comparable efficacy and adverse‐events profile and could be offered to the patient according to availability, route of delivery, patient preference, cost, and local regulations
BiologicsPractice points
6. Insufficient evidence to define the risk/benefit ratio for mono‐ or combo‐ therapy in all CD children; combo therapy for the first 6 months may be associated with a lower rate of antibodies development and loss of response; benefit weighed against eventually increased lymphoma risk with thiopurines on an individual basis (also based on predictors of disease outcome). The use of concomitant low dose MTX may be safer but is less evidence‐based
7. Pre‐medication with acetaminophen, steroids or anti‐histamines are not routinely indicated prior to anti‐TNF therapy
8. Testing for tuberculosis (chest radiograph, PPD skin test and/or quantiferon) prior to anti‐TNF therapy is obligatory
9. IFX should be administered at 5mg/kg with 3 induction doses over 6 weeks (week 0‐2‐6) followed by maintenance therapy of 5mg/kg every 8 weeks.
10. Higher doses up to 10mg/kg and/or shorter intervals to every 4 weeks may be required in those losing response to the drug or when the drug level is low. Physicians should consider reducing IFX dose when trough levels are above 8‐10μg/ml and remission is achieved
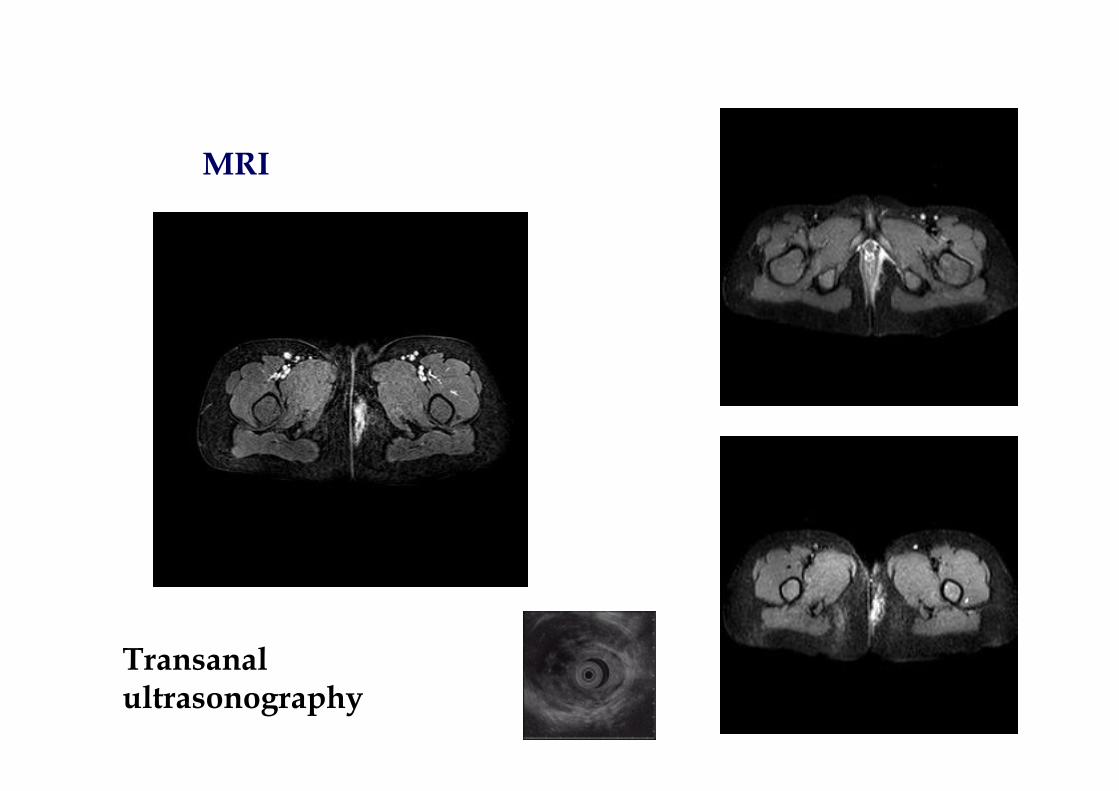
MRI
Transanal ultrasonography
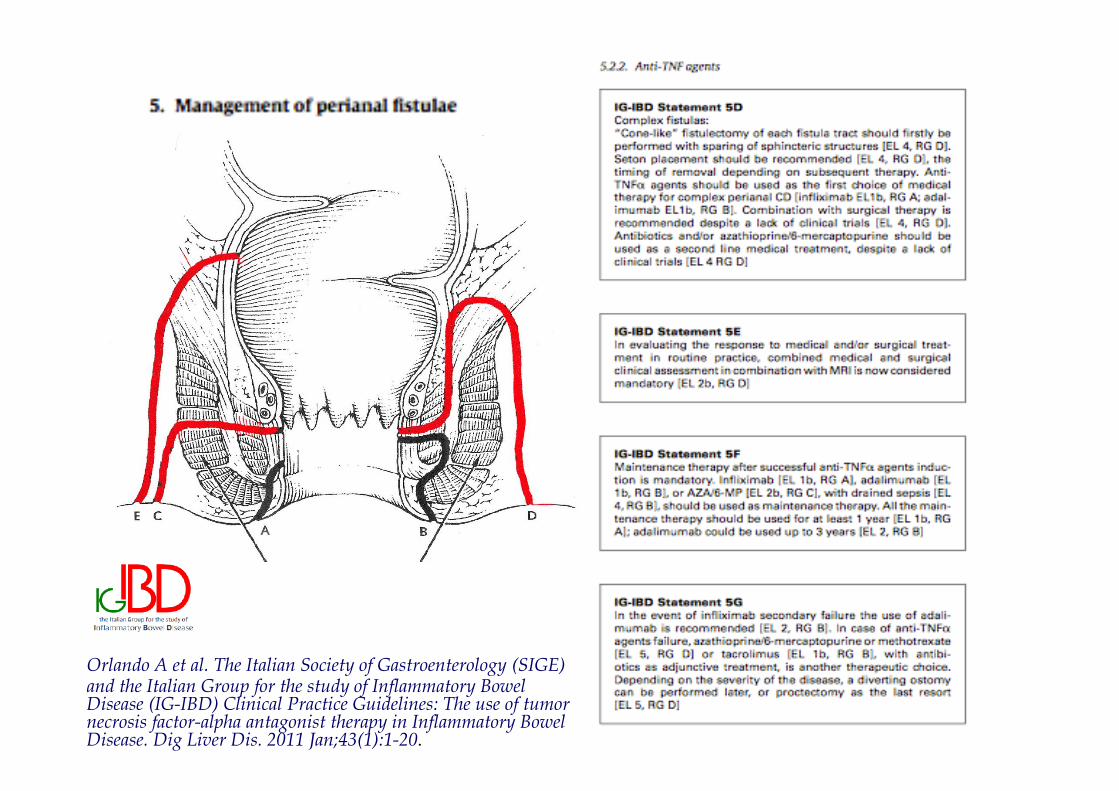
Orlando A et al. The Italian Society of Gastroenterology (SIGE) and the Italian Group for the study of Inflammatory Bowel Disease (IG-IBD) Clinical Practice Guidelines: The use of tumor necrosis factor-alpha antagonist therapy in Inflammatory Bowel Disease. Dig Liver Dis. 2011 Jan;43(1):1-20.

The Paediatric IBD Porto Group
The Paediatric IBD Porto Group

THALIDOMIDE
• STATEMENT 16
• Even if there are some reports showing efficacy of Thalidomie in refractory pediatric CD there are insufficient data to recommend thalidomide therapy (EL4) 88% agreement
Practice points:• Due to the numerous potential side effects and to its teratogenicity, thalidomide as
maintenance therapy is restricted to a very selected cohort • Thalidomide maintenance alternative for anti‐TNF agent responders who do not tolerate or
lost response to biologic anti‐TNF agents• Careful neurological and psychological examination and assessment of vibration sensitivity at
regular intervals (6‐monthly) is indicated• Thalidomide starting doses of 50 mg daily orally are usually administered in adult patients
and then subsequently increased according to response and tolerance; this seems appropriate also for adolescents with CD, however, reduced doses should be considered for young children. Dosing of 2mg/kg was suggested
• Contraception is mandatory when appropriate

JAMA 2014
Maintenance therapy after surgery
• STATEMENT 22• Maintenance treatment is recommended in children and
adolescents after surgically induced remission (EL 2 (pediatrics)) 92% agreement
• STATEMENT 23• Thiopurines may be used as first choice drug for post‐operative
maintenance therapy (EL3 (pediatrics), EL2 (adults)), while supplementary enteral nutrition (EL3 (pediatrics) EL2 (adults)) or anti‐TNF‐agents (EL 3 (pediatrics)), are also possible options in selected patients 84% agreement