Il rischio cardiorenale e la sua progressione. La …...Brenner BM et al New Engl J Med...
39
IL RISCHIO CARDIORENALE E LA SUA PROGRESSIONE: LA SFIDA FUTURA DELLA NEFROLOGIA MANTOVA 05-03-2005 Gherardo Buccianti
Transcript of Il rischio cardiorenale e la sua progressione. La …...Brenner BM et al New Engl J Med...

IL RISCHIO CARDIORENALE ELA SUA PROGRESSIONE:
LA SFIDA FUTURA DELLANEFROLOGIA
MANTOVA 05-03-2005
Gherardo Buccianti

• ESH-ESC 2003
• JNC7 2003
– Stratificazione del rischio cardiovascolare.Le nuove linee guida hanno funzione nonsolo prescrittiva ma soprattutto educativa
• K/DOQI CKD Classification– AJKD 2003

Prevalenza dell’IRC
0,1 %
0,2 %
4,3 %
3,0 %
3,3 %
30 - 59
60 - 89
> 90
15 - 29
<155
3
2
4
1

0,1 %
0,2 %
4,3 %
3,0 %
3,3 %
30 - 59
60 - 89
> 90
15 - 29
<155
3
2
4
1NKF-K/DOQINKF-K/DOQI
ESRD
IRC
Albuminuria
Microalbuminuria
CHF
CVE
CAD, LVH,Ispessimentointimale
Età, ipertensione, Diabete, obesità Malattia CV
Sarnak et al AJKD 2000

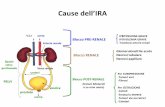
PROBABILI IPOTESI PATOGENETICHE
• La malattia renale e quella vascolare hanno simili meccanismiemodinamici e metabolici di progressione, in presenza di duepatologie non correlate
• La malattia renale precede e peggiora quella vascolare tramitel’accumulo di AGEs, attivanti numerosi fattori di crescita einducenti disfunzione endoteliale e aterosclerosi
• La patologia vascolare accelera quella renale inducendoipertensione glomerulare e conseguente progressione
• Meccanismi fisiopatologici comuni alle due patologie conducono auna combinazione delle tre ipotesi. La prevalenza di ciascunfattore fisiopatologico sull’altro determinerà la velocità diprogressione di una delle due patologie.
CARDIO-RENAL CONNECTIONMacIsaac RJ et alCurrent Opinion inNephrology, 2004

PROBABILI IPOTESI PATOGENETICHE
ECFV, CO, MAP, HEMODYNAMIC CONTROL
RENALFAILURE
HEARTFAILURE
CARDIO-RENAL CONNECTION
NO/ROS BALANCE
SYMPNERVOUSSYSTEM
RAS INFLAM

IRC E MORTALITA’
0,1 %
0,2 %
4,3 %
3,0 %
3,3 %
30 - 59
60 - 89
> 90
15 - 29
<155
3
2
4
1
RR=1.2
RR=3.2
RR=5.9
RR Globale RR cardiovascolare
RR=1.4
RR=2.8
RR=3.1
Go AS et al (mod) N Engl J Med 2004

Livelli di creatinina serica normale-alta e rischio CVnell’ipertensione: lo studio PIUMA
Follow-up, anniSchillaci G. et al., Arch Intern Med 2001
Q1 creat. s. (≤ 0.94 m; ≤ 0.79 f) Q2 creat. s. (0.95-1.04 m; 1.05-1.17 f) Q3 creat. s. (1.05-1.17 m; 0.87-0.95 f) Q4 creat. s. (≥ 1.18 m; ≥ 0.96 f)
0.9
0.8
0.6
0.5 (%) E
vent
i CV
per
pazi
ente
-ann
o
Sopr
avvi
venz
a se
nza
even
ti C
v
1
0.7
00 2 4 6 8
Q1
Q2
Q3
N= 1829, p < 0.003 con il test log-ranghi
Quartili di creatinina sierica
p < 0.05 Q1vs Q4
0
1
2
3
4
10
Q41 2 3 4
RR 1.30 (C.I. 1.07-1.59), p 0.01 per ogni 0.23 mg/dL ↑ Creat. S.
Corretto per età, sesso, fumo, colesterolo, LVH, protU, BP, Tx

La disfunzione renale lieve comporta un aumento dellamortalità CV nella popolazione generale:
lo studio Hoorn
RMA Henry et al., Kidney Intern 2002
RR di CVD (indipendentemente da PA, Htn, diabete, Hcyst.) :
•1.49 (CI 1.28- 1.73) per ogni ↑ di SD in creat. s.
•1.47 (CI 1.04- 2.08) per ogni ↓ di SD clear. creat.Formula di Cockroft-Gault
(140-età)*peso corporeo/(creat.*72)* .85 se disesso femminile
•1.77 (CI 1.33- 2.34) per ogni ↓ di SD clear. creat.Formula di Levey
170* (creat.) -0.999 * (età) –0.176 * (urea) -0.170 * (alb) 0.318 * 0.762 se di sesso femminile
95
90
Prop
orzi
one
di p
z se
nza
mor
te C
V
100
850 2 4 6 8
Follow-up, anni
N= 631,
età 64±7, creat. S. basale 91.7±19 umol/L;
Tertile Superiore, GFR > 72.2
Tertile medio, 63.4 <GFR ≥72.2
10
Tertile inferiore, ≤63.4
p <0.001

0
10
20
30
La disfunzione renale lieve è un forte fattore di rischio CV:lo studio HOT
Eve
nti /
100
0 pa
zien
ti-an
no
Mod
ifica
to d
a R
uilo
pe L
M, J
ASN
200
1
RR= 2
P < 0.001RR= 2.9
P < 0.0001RR= 3.2
P < 0.001
Eventi CV maggioriMortalità CV Mortalità Totale
Creat. S < 1.5 Creat. S > 1.5
Tutti i dati sono aggiustati per PA, età, sesso, fumo, precedente rischio CV, diabete, colesterolo totale.
Clear. Cr. > 60 Clear. Cr. < 60RR= 1.6
P < 0.001RR= 1.8
P < 0.001
RR= 1.6
P < 0.001
n= 18597
0
10
20

0
10
20
30
40
50
1 2 3 4
Eve
nts p
er 1
000
patie
nts y
ears
3238 37
49
STUDIO HOPE
<0.93 0.93-1.08 1.09-1.22 >1.22
Mann JFE et al, KI 2003

OUTCOMES OF PATIENTS WITH ANDWITHOUT CKD
62.5
30.6
15.9
51.1
34.9
17.8
8.6
23.1
0
10
20
30
40
50
60
70
CKD (n= 759) non CKD (n= 3519)
composite
Cardiac
Stroke
Mortality
%
Pl creat= 1.39±0.4 Pl creat= 0.86±0.19
Weiner DE et al AJKD 2004

36.410.59 173HOPE
29.13.16 321INSIGHT
12.32.518 790HOT
Clear. Creat.(< 60-70 ml/min) %
Creatinina Sierica(> 1.5, m; > 1.4 f) %N
Prevalenza della disfunzione renale lieve nelpaziente iperteso

Prevalenza di microalbuminuria nei pazienticon ipertensione arteriosa
Mod da Diercks et al Can J Cardiol 2002; 18: 525-35
38
29
33,7
6,7 6,14,1
19,9
0
10
20
30
40
Bigazzi, 1992 Calvino,1999
Grandi, 2000 Pontremoli,1997
Palatini, 1996 Jensen, 1997 media*

Albuminuria e rischio CV nell’ipertensioneessenziale: lo studio LIFE
Ris
chio
Rel
ativ
o
End-point composito: mortalità CV e globale, ictus e IMA
Modificato da Wachtell K et al. Ann Intern Med 2003
0,5
1,5
2,5
3,5
n= 7143 pazienti non diabetici
Decili di ACR1 2 3 4 5 6 7 8 9 10

Proteinuria come fattore predittivo di eventicardiovascolari nel DM tipo 2
0.9
0.8
0.6
0.5
Inci
denz
a (%
)
Sopr
avvi
venz
a se
nza
even
ti C
V
1
0.7
00 10 20 30 40 50 60 70 80 90
Mesi
AB
C
Totale: p < 0.001
A: U-Prot < 150 mg/L B: U-Prot 150–300 mg/L C: U-Prot > 300 mg/L
Miettinen H et al. Stroke 1996;27:2033-2039.
Ictus Coronaropatie
p < 0.001
0
10
20
30
40

LA PRESENZA DI ALBUMINURIA, ESPRESSIONE DIUNA PERDITA DELL’INTEGRITA’ DELLA BARRIERA
EMATOURINARIA, INDICA UNA LESIONEMICROVASCOLARE, ESPRESSIONE DI DANNO
ALL’AUTOREGOLAZIONE RENALE CHE RENDE ILGLOMERULO VULNERABILE AGLI EFFETTI DELLE
VARIAZIONI PRESSORIE
IL SOLO CONTROLLO OTTIMALE DELLA PRESSIONEARTERIOSA CON RIDUZIONE/SCOMPARSA DELLA
MICROALBUMINURIA PUO’ PREVENIRE ILPASSAGGIO DALLA MICRO- ALLA MACRO-
PATOLOGIA VASCOLARE
Weir MR et al Current Op 2005

Trial e Prevenzione secondaria (prevenzione dellamacroalbuminuria nei microalbuminurici)
studio # pz follow-up farmaci esito
Ravid, ‘93 94 5 aa enalapril vs placebo ena > placebo
Lacourciere, ‘93 21 3 aa captopril vs convenz capto > conv
Lebowitz, ‘94 75 3 aa enalapril vs convenz ena > conv
Sano, ‘94 56 4 aa enalapril vs nifedipina ena > nifed
Velussi, ‘96 18 3 aa cilazapril vs amlodipina cilaz = amlo
Mosconi, ‘96 13 2.7 aa enalapril vs nitrendipina ena = nitren
Agardh, ‘96 335 1 a lisinopril vs nifedipina lis > nifed
Chan, ‘00 34 5.5 aa enalapril vs nifedipina ena > nifed
ABCD, ‘00 150 5.3 aa enalapril vs nisoldipina ena = nisol

Trial e Prevenzione terziaria (declino del GFR nei pazientimacroalbuminurici)
studio # pz follow-up farmaci esito
Lebowitz, ‘94 46 3 aa enalapril vs convenz ena = conv
Bakris, ‘96 52 6 a lisinopril vs verapamil lis = verap > vs atenololo atenoloNielsen, ‘97 43 3.5 aa lisinopril vs atenololo lis = aten
Bakris, ‘98 37 1 a trandolapril vs verapamil trand+verap >> vs trand + verap singoli
Fogari, ‘99 51 2 aa ramipril vs nitrendipina ram = nitrend
ABCD, ‘00 82 5.3 aa enalapril vs nisoldipina ena = nisol
Chan, ‘00 25 5.5 aa enalapril vs nifedipina ena = nifed
MicroHOPE*, ‘00 1140 4.5 aa ramipril vs placebo ram > plac
REIN 1997 352 2.5 aa ramipril vs placebo ram>plac
*Riduzione RR combinato microvascolare nefropatia, dialisi e laserretina 16%

RENAALTasso di progressione della patologia renale
(Pendenza mediana di 1/sCr)
Losartan Placebo0
-.02
-.04
-.06
-.08
dl/m
g/an
no -0,056
-0,069
p=0,01riduzione del 18%
(+TC) (+TC)Brenner BM et al New Engl J Med 2001;345(12):861-869.

RENAALComponenti primari
ESRD
Mesi
% c
on e
vent
o
0 12 24 36 480
10
20
30
p=0,002Riduzione del rischio:
28% P
L
ESRD o decesso
P (+ TC)L (+ TC)
Mesi
% c
on e
vent
o
0 12 24 36 480
10
20
30
40
50
751 714 625 375 69762 715 610 347 42
PL
p=0,010
Riduzione del rischio: 20%
Raddoppio della creatininasierica
Mesi
% c
on e
vent
o
p=0,006Riduzione del rischio:
25%
751 692 583 329 52762 689 554 295 36P (+ TC)
L (+ TC)
0 12 24 36 480
10
20
30
P
L
P (+ TC)L (+ TC) 751 714 625 375 69
762 715 610 347 42
Brenner BM et al New Engl J Med 2001;345(12):861-869.

Determination ofGFR – iohexol method
• Non-ionic, low osmolar radiocontrast agent
• Exogenous marker of GFR
• Minute quantities detected by HPLC
• Minimal extrarenal elimination
• Single-sample iohexol clearance 3–4 h after3–5 ml injection
• Lower limit of accuracy is 2–3 ml/minRippin et al. J Diabetes Complications 2002;16:195–200

Primary endpoint: GFR after 5years
0
10
20
30
40
50
60
70
80
90
100
Telmisartan Enalapril
Baseline After 5 years
-14.8
-17.9-20
-18
-16
-14
-12
-10
-8
-6
-4
-2
0
Telmisartan Enalapril
Telmisartan Enalapril
Change in GFR*Total GFR *
* p=NS

Soggetti(%)
0 6 12 18 24 30 36 42 48 54Follow-up
(mesi)
60
0
10
20
30
40
50
60
70
IDNT Endpoint PrimarioCombinato:Tempo al raddoppio diCreatinina Sierica, ESRD, o Morte
Irbesartan
Amlodipina
Controllo
Lewis EJ et al. N Engl J Med 2001;345:851-860.
RRR 20%P=0.02
P=0.69
RRR 23%P=0.006

0 6 12 18 24 30 36 42 48 54Tempo di Follow-up (mesi)
010
2030
4050
60
% d
i paz
ient
i con
radd
oppi
o de
lla C
reat
. o E
SRD
PAS < 132 mm HgPAS 132 - 141 mm HgPAS 142 - 153 mm Hg PAS > 153 mm Hg
Impatto della riduzione di PAS sulla progressione deldanno renale: lo studio IDNT
Pohl MA et al, ASN Philadelphia 2002 SU.PO583
Valore di P95% CIRR
< 0.00011.09 - 1.221.16Δ 10 mmHg dellaPAS a 12 mesi
0.0651.00 - 1.111.05Δ 10 mmHg dellaPAS basale

The Covalent Group, Inc.
CAMELOT Results—Cumulative EventRates
Cum
ulat
ive
even
ts, p
ropo
rtio
n
Months0 6 12 18 24
0
0.25
0.20
0.15
0.10
0.5
PlaceboEnalaprilNORVASC
No. at riskPlacebo 655 588 558 525488Enalapril 673 608 572 553529NORVASC 663 623 599 574535
31% Risk reduction for NORVASC vs placebo (P=0.003)19% Risk reduction for NORVASC vs enalapril (P=0.10)
15% Risk reduction for enalapril vs placebo (P=0.16)
NNT : 16 (amlodipine vs placebo)
JAMA NOV 2004

The Covalent Group, Inc.
NORMALISE Results—IVUS LOWESSPlots
LOWESS Plot of Change in Percent LOWESS Plot of Change in Percent AtheromaAtheroma Volume Volumevs Change in BP in the Combined Treatment Groupvs Change in BP in the Combined Treatment Group
Cha
nge
in P
erce
ntA
ther
oma
Volu
me
-40 -30 -10 0 20-2.0
2.5
2.0
1.0
0
-1.0
10-20
1.5
0.5
-0.5
-1.5
The solid line represents the continuous relationship,surrounded
by the dashed lines representing 95% confidence intervals.
Change in Blood Pressure, mm Hg
LOWESS indicates locally weighted scatterplot smoothing.

EPIDEMIOLOGIA DELL’INSUFFICIENZACARDIACA
2
5
10
0
2
4
6
8
10
POPOLAZIONE
GENERALE
> 80 ANNI
Muller LW Cardiology Clinic 2001
%

PREVALENZA DI PAZIENTI CON Hb< 12 g/dlNELLE VARIE CLASSI NYHA
9,1
19,2
52,6
79,1
0
10
20
30
40
50
60
70
80
NYHA I NYHA II NYHA III NYHA IV
Pereira AA et al KI 2003

TERAPIA DELL’ANEMIA IN 179 PAZIENTICON IRC E SCOMPENSO CARDIACO
Silveberg D et al NDT 2003
POSTPREPOSTPRE
68.3±36.165.3±45EPOUI/Kg/sett
13.1±1.310.4±1.112.9±1.210.5±1Hb %
39.8±8*34.8±13.537.6±11.7*35±15.5FE %
2.53±0.42*3.89±0.242.55±0.48*3.91±0.25NYHA
0.13±1.54-1.18±1.490.21±1.3-1.12±1.3Δ GFRml/min
2.2±0.85 2.14±0.802.55±0.48 2.37±1.14Creat mg/dl
(95)NON DIABETICI(84)DIABETICI

ACETIL CoA
HMG CoA
MEVALONATO
ISOPENTENIL PIROFOSFATO ISOPENTENIL tRNA
GERANIL PIROFOSFATO
UBICHINONE DOLICOLI
SQUALENE
COLESTEROLO
MEVALONATO PIROFOSFATO
FARNESIL PIROFOSFATO
HMG CoA-REDUTTASI
LE STATINE: INIBIZIONE DELLA SINTESI DELCOLESTEROLO

ATORVASTATINA RIDUCE LAPROTEINURIA
-60
-50
-40
-30
-20
-10
0
-12 -6 0 3 6 9 12
* ** ***: p<0.05**: p<0.01
Bianchi et al AJKD 2003


PI-3K
AkteNOS
AGII
ERK
Nitric Oxidestatine
IRS-1 e IRS-2

Azione delle statine
Riduzione del colesterolo
Riduzione Ox-LDL
PPAR
R-OH
Effetto pleiotropico
AkteNOS

CRF

0 24 48 72 96mesi
Intervento multifattoriale per la protezione CV nelpaziente a elevato rischio
End
poin
t pri
mar
io c
ompo
sito
%0
10
20
30
40
50
Tx Conv.
Tx Int.
P= 0.007Nefropatia 0.39 (0.17-0.87) 0.003
Retinopatia 0.42 (0.21-0.86) 0.02
Neuropatia Aut. 0.37 (0.18-0.79) 0.002
Neuropatia Perif. 1.09 (0.54-2.22) 0.66
0
Int Tx. migliore Tx Conv. migliore
10.5 1.5 2.0
Variabile RR (C.I.) P
Modificato da Gaede P et al. N Eng J Med 2003
BP,mmHg 146/78 132/73HbA1c,% 9.0 7.9LDL-C,mg/dl 118 81ASP+STAT,% 45 86ACE±ARB,% 70 97

DIFFERENTE COMPORTAMENTO DELCARDIOLOGO E DEL NEFROLOGO DI
FRONTE AL RISCHIO CARDIOVASCOLAREGLOBALE NELL’IRC
• CARDIOLOGO: Di fronte alla malattia coronaricamaggior aggressività con una terapia antiipertensivapiù sostenuta
• NEFROLOGO: Non tiene conto della valutazioneecocardiografica in caso di CAD e non somministra β-bloccanti. I pazienti in ERSD sono trattati in manierasubottimale

LA SFIDA FUTURA DELLANEFROLOGIA
• Rallentare/arrestare la progressionedell’insufficienza renale nel pazientecardiopatico
• Rallentare/arrestare la progressionedella cardiopatia nel pazientenefropatico