Il paziente critico tra DEA ed UTIC Gestione del … Occhetta SSD Elettrofisiologia e...
45
Eraldo Occhetta SSD Elettrofisiologia e Cardiostimolazione Dipartimento Cardiologico AOU Maggiore della Carità - Novara Il paziente critico tra DEA ed UTIC Gestione del paziente con tempesta aritmica
Transcript of Il paziente critico tra DEA ed UTIC Gestione del … Occhetta SSD Elettrofisiologia e...
Eraldo Occhetta SSD Elettrofisiologia e
Cardiostimolazione Dipartimento Cardiologico
AOU Maggiore della Carità - Novara
Il paziente critico tra DEA ed UTIC
Gestione del paziente con
tempesta aritmica
Storm �elettrico� o �aritmico�: Situazione clinica caratterizzata da tachiaritmie ventricolari gravi e subentranti con altissimo rischio di morte per il paziente
Prima dell�avvento degli ICD tale situazione clinica era piuttosto rara da vedersi in DEA/UTIC in quanto il paziente non arrivava alle aree intensive. La situazione era quasi sempre correlata ad:
- ischemie/infarti miocardici acuti o gravi squilibri elettrolitici con TV/FV subentranti che richiedevano numerose e continue defibrillazioni esterne
- Torsioni di punta in QT lungo spontaneo o iatrogeno
Su queste situzioni: Pochi lavori di letteratura, sostanzialmete focalizzati alle problematiche terapeutiche
- Intravenous Amiodarone Multicenter Trial Group
- Levine JH, et al. JACC 1996; 27:67-75 - Scheinman MM, et al. Circulation 1995; 92:3264-3272 - Kowey PR, et al. Circulation 1995; 92:3255-3263
- Blocco del simpatico - Nademanee K, et al. Circulation 2000; 102:742-747
- Sedazione profonda con Propofol - Burjorjee J, et al. Can J Anaesth 2002; 49:973-977
L�avvento degli ICD ha cambiato lo scenario: l�ICD interviene interrompendo le gravi tachiaritmie
ventricolari Viene così evitata la morte improvvisa Ma puo� verificarsi che l�aritmia riparta entro breve tempo, con nuovo intervento dell�ICD Tale situazione puo� persistere se rimane la causa di aritmia (ischemia/squilibrio elettrolitico/ecc.): l�ICD puo� intervenire con numerosi shock nel giro di poco tempo
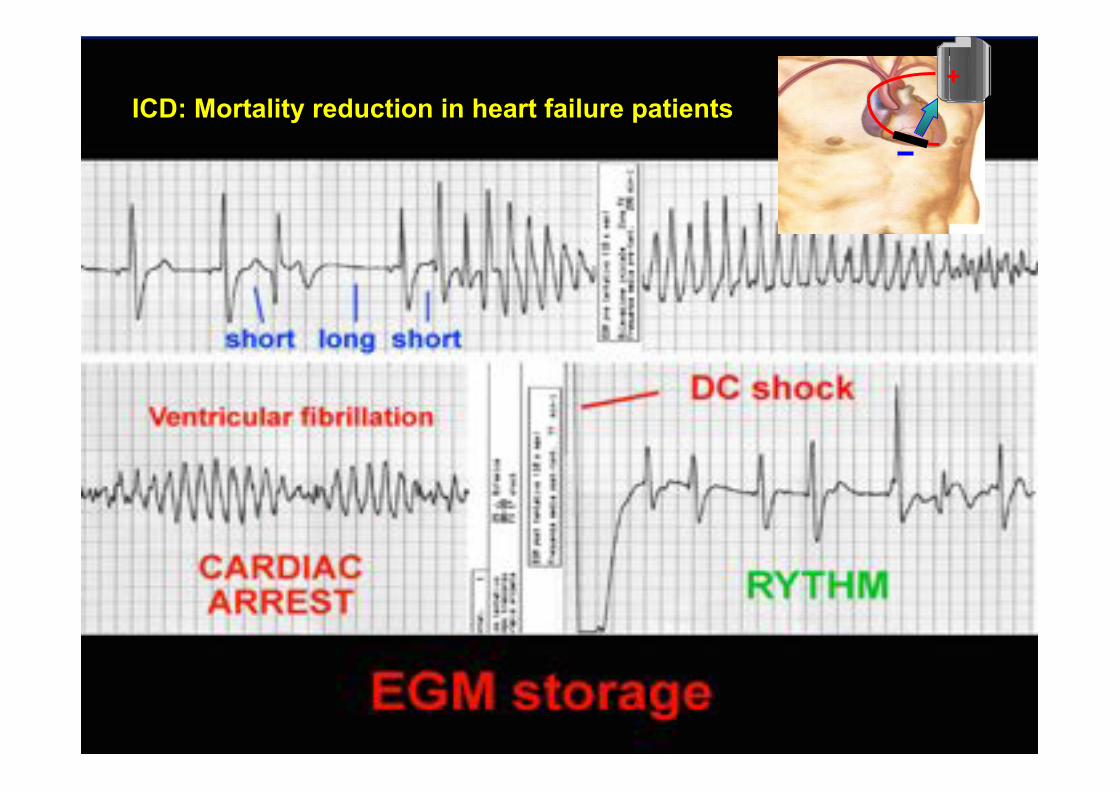
ICD: Mortality reduction in heart failure patients +
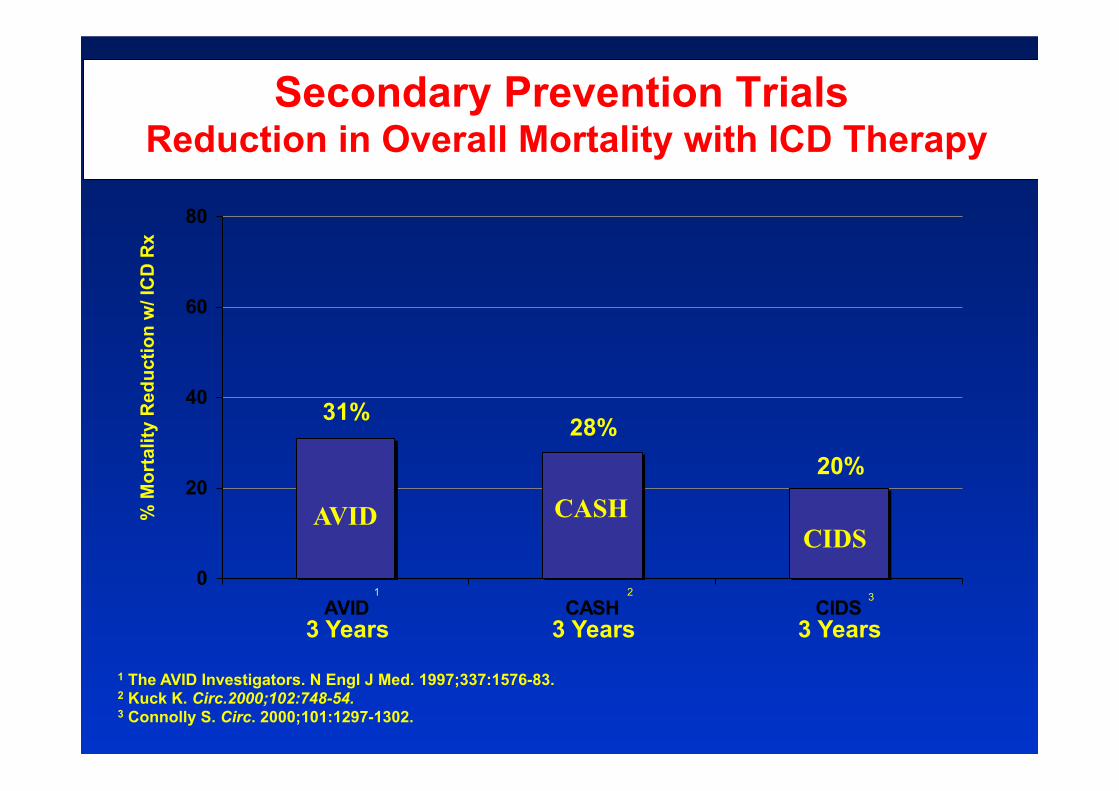
1 The AVID Investigators. N Engl J Med. 1997;337:1576-83. 2 Kuck K. Circ.2000;102:748-54. 3 Connolly S. Circ. 2000;101:1297-1302.
0
20
40
60
80
AVID CASH CIDS1 2 3
31% 28% 20%
% M
orta
lity
Red
uctio
n w
/ IC
D R
x
Secondary Prevention Trials Reduction in Overall Mortality with ICD Therapy
3 Years 3 Years 3 Years
AVID CASH CIDS
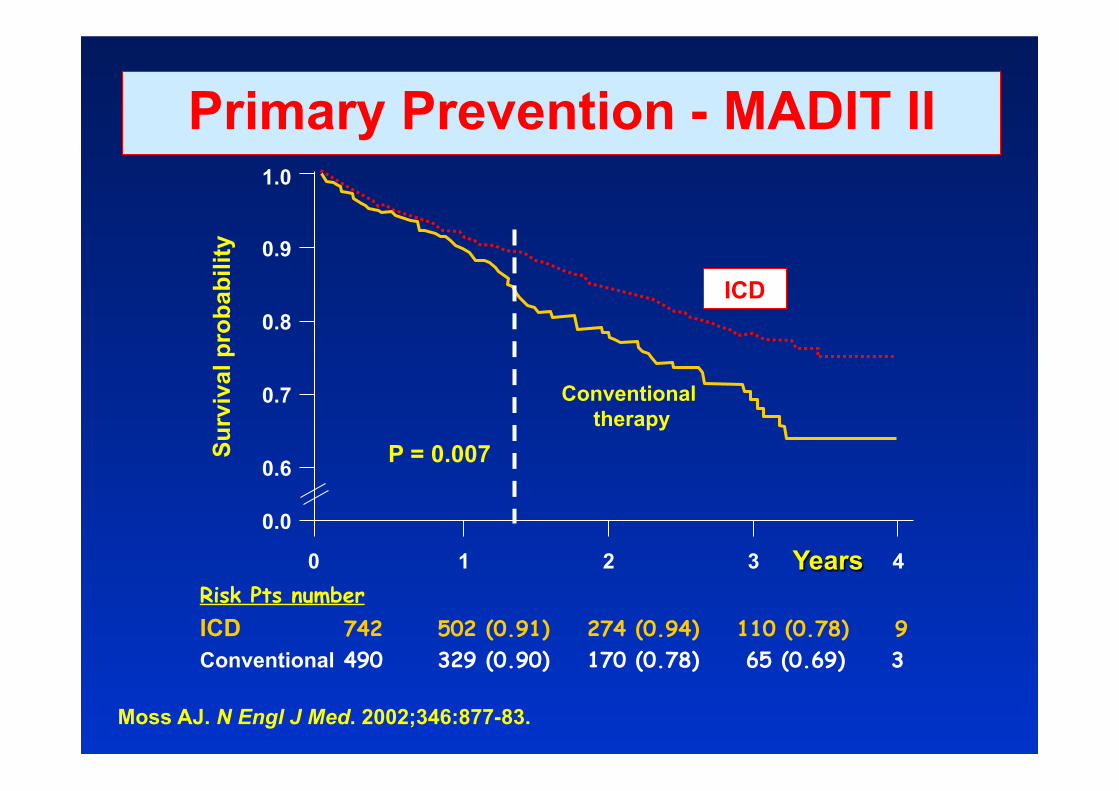
Primary Prevention - MADIT II
ICD
Conventional therapy
P = 0.007
1.0
0.9
0.8
0.7
0.6
0.0
Surv
ival
pro
babi
lity
0 1 2 3 4 Years Risk Pts number ICD 742 502 (0.91) 274 (0.94) 110 (0.78) 9 Conventional 490 329 (0.90) 170 (0.78) 65 (0.69) 3
Moss AJ. N Engl J Med. 2002;346:877-83.
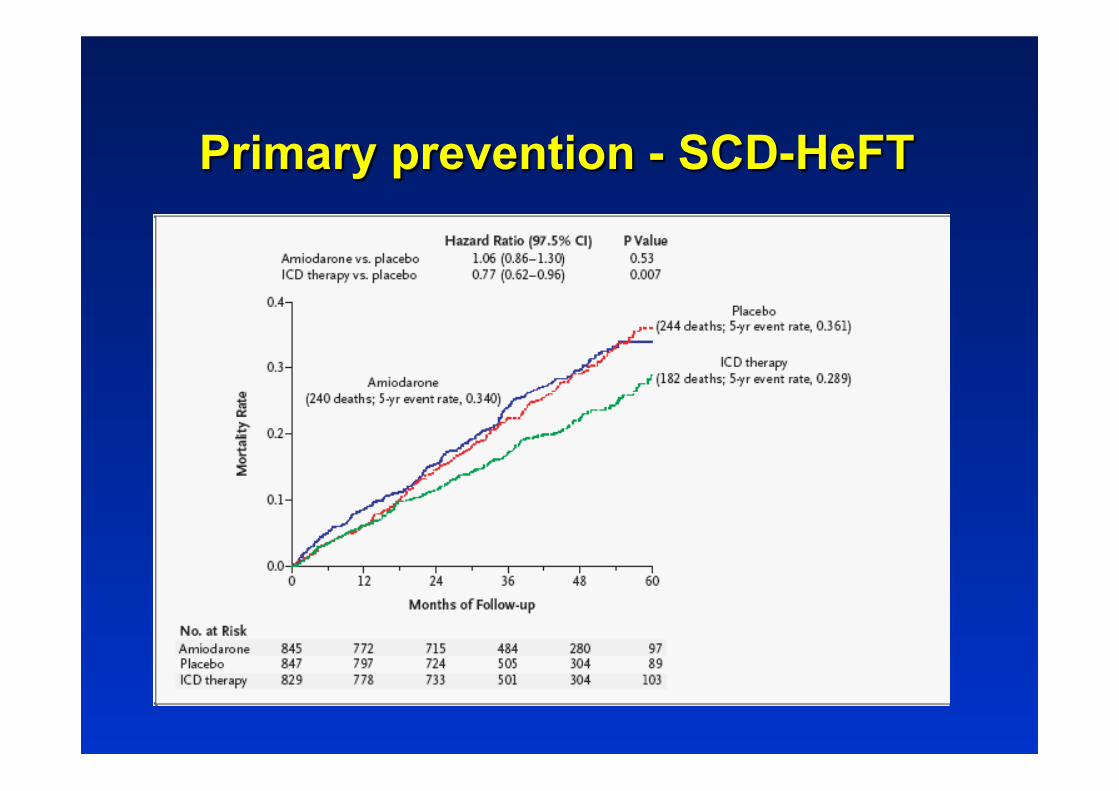
Primary prevention - SCD-HeFT

Electrical storm Inappropriate ICD shock ICD system malfunctions Mechanical Problems (infections, decubitus, pain, …) Psichological problems (themself, shock related, ….)
ICD PROBLEMS

11
Electrical storm in ICD patients:
( =/> 3 episodes/24 hours) - a dramatic experience for the patient - a hard emergency for the cardiologic equipe (physicians and nurses)
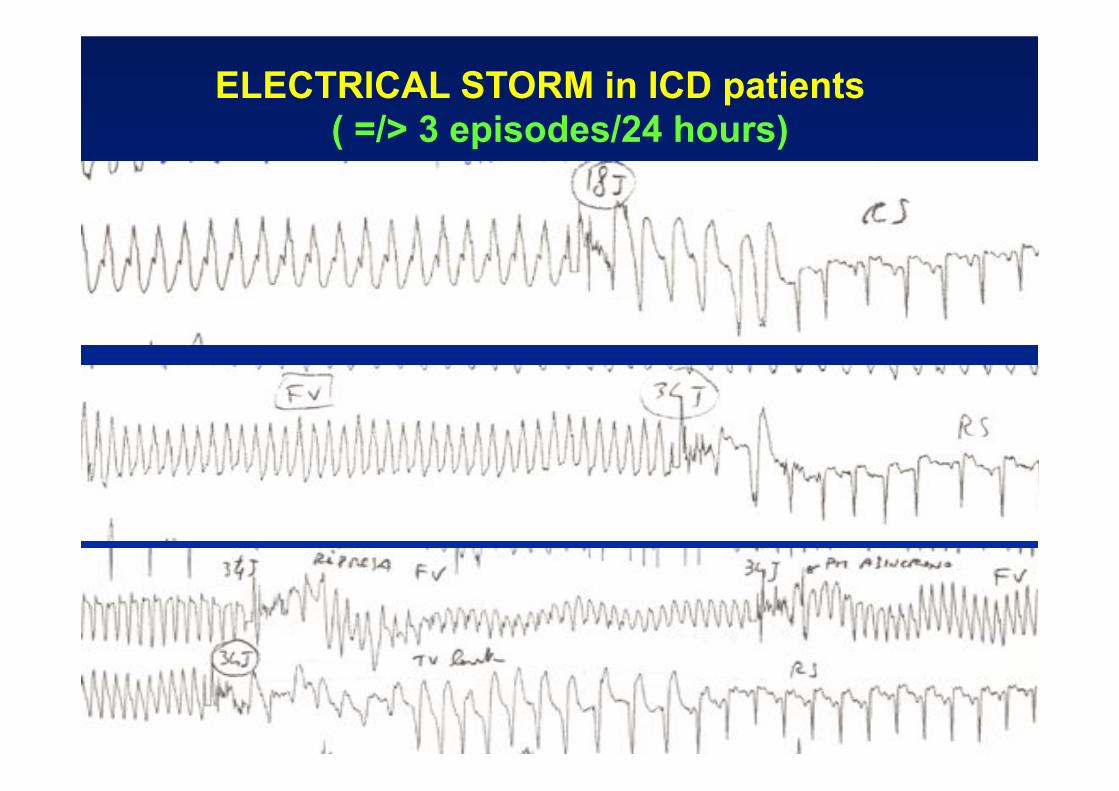
ELECTRICAL STORM in ICD patients ( =/> 3 episodes/24 hours)
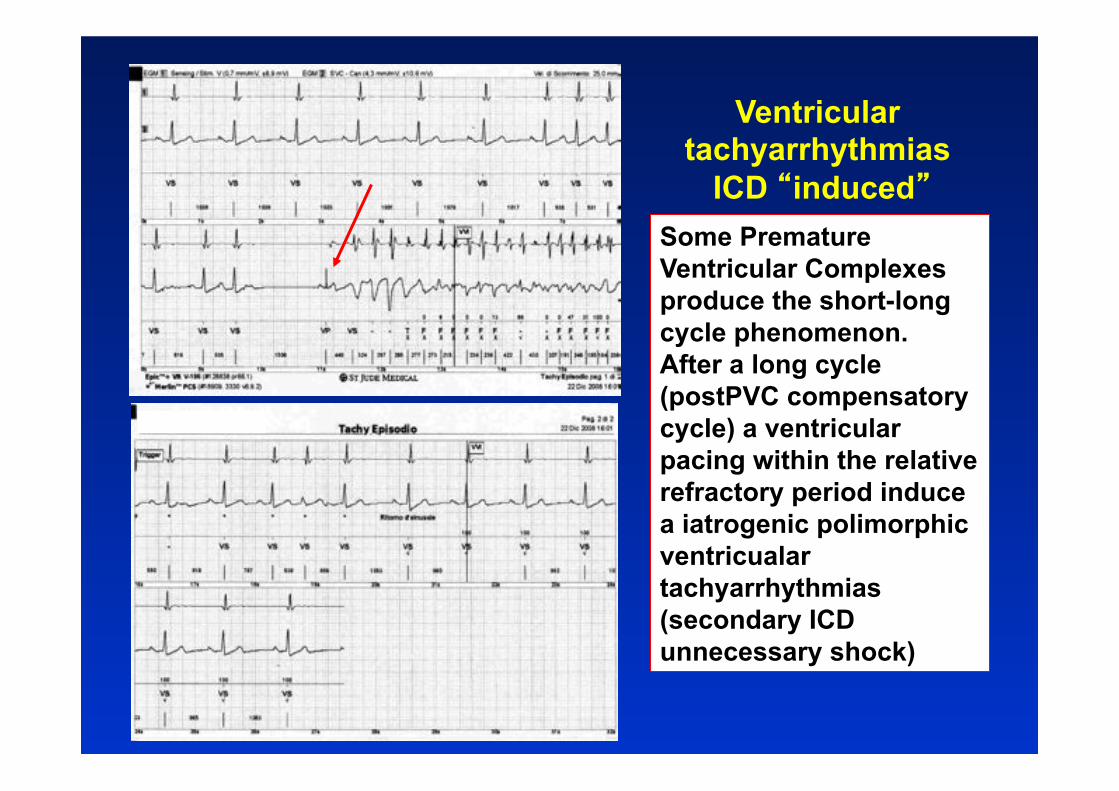
Some Premature Ventricular Complexes produce the short-long cycle phenomenon. After a long cycle (postPVC compensatory cycle) a ventricular pacing within the relative refractory period induce a iatrogenic polimorphic ventricualar tachyarrhythmias (secondary ICD unnecessary shock)
Ventricular tachyarrhythmias
ICD �induced�

Electrical storm in ICD patients Licterature
Incidence: 10-20% of ICD patients Occurrence: 24 hours after implant
(problema all�inizio con impianti epicardici) during normal follow up pre-dead phase
Mean of episodes number: 8
range: 3 - 50 % of hospitalization: 85%
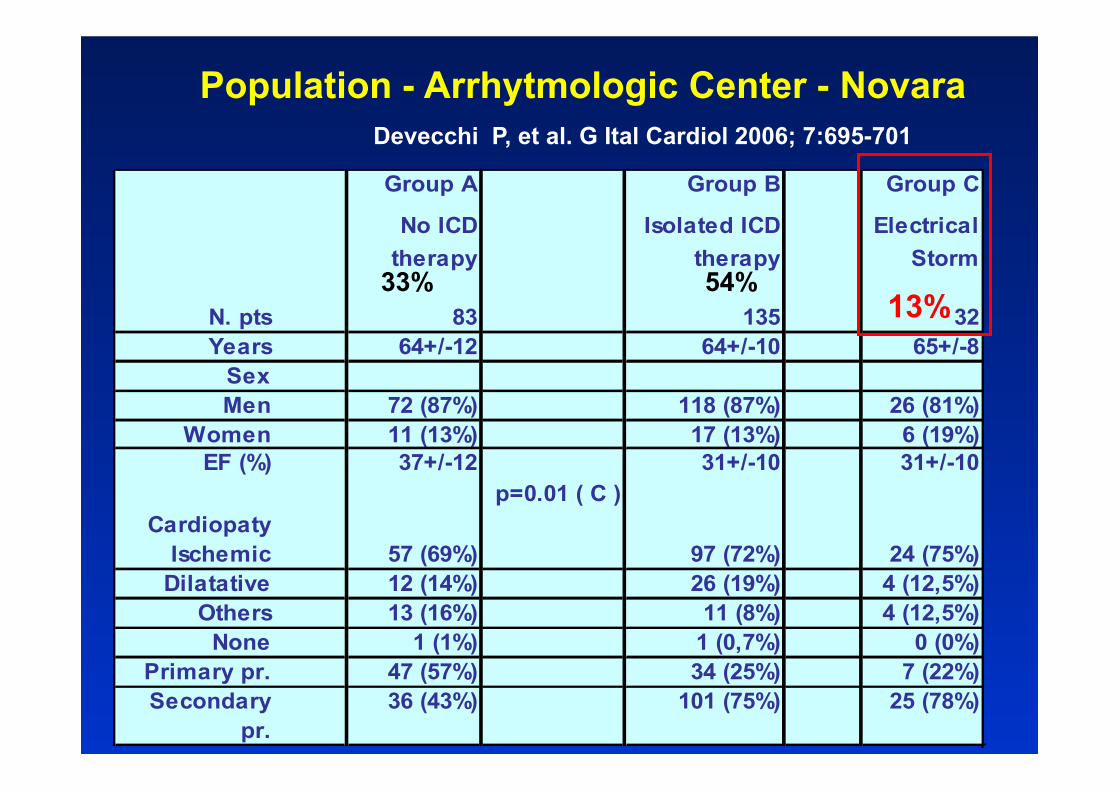
Group A Group B Group C
No ICD therapy
Isolated ICD therapy
Electrical Storm
N. pts 83 135 32Years 64+/-12 64+/-10 65+/-8
SexMen 72 (87%) 118 (87%) 26 (81%)
Women 11 (13%) 17 (13%) 6 (19%)EF (%) 37+/-12 31+/-10 31+/-10
p=0.01 ( C )Cardiopaty
Ischemic 57 (69%) 97 (72%) 24 (75%)Dilatative 12 (14%) 26 (19%) 4 (12,5%)
Others 13 (16%) 11 (8%) 4 (12,5%)None 1 (1%) 1 (0,7%) 0 (0%)
Primary pr. 47 (57%) 34 (25%) 7 (22%)Secondary
pr. 36 (43%) 101 (75%) 25 (78%)
Population - Arrhytmologic Center - Novara
13% 54% 33%
Devecchi P, et al. G Ital Cardiol 2006; 7:695-701

32 patients with Electrical Storm • 50 episodes of storm (1,5/patient) • First storm: 42+/-37 months from implant • 14 patients (43%) had 2 episodes • 3 patients had 3 episodes • 1 patient had 4 episodes
Population - Arrhytmologic Center - Novara
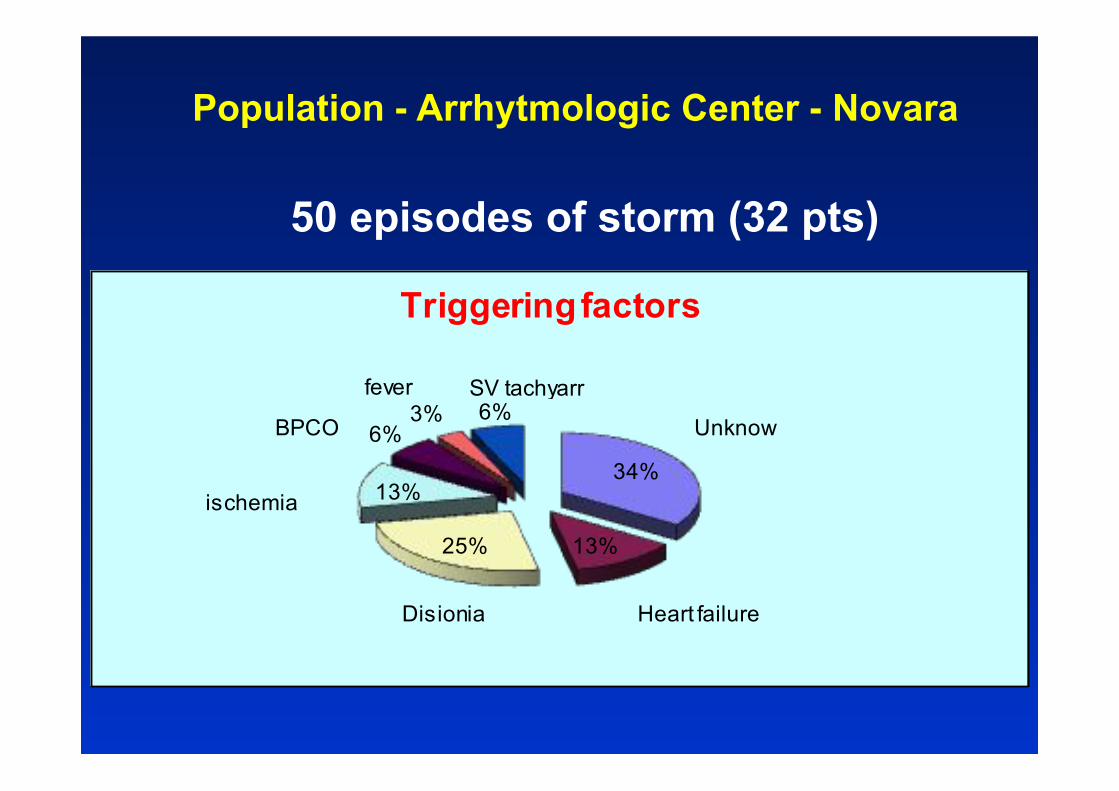
34%
13%25%
13%
6%3% 6%
Triggering factors
Unknow
SV tachyarr
Disionia
ischemia
Heart failure
BPCO
fever
50 episodes of storm (32 pts)
Population - Arrhytmologic Center - Novara

18
RESULTS – END POINT Cardiac MORTALITY and/or Cardiac Transplantation
B C A
Percentuale cumultiva di sopravvivenza
Tempo (giorni)
Pere
cntu
ale
Cum
ulat
iva
0
10
20
30
40
50
60
70
80
90
100
110
0 730 1460 2190 2920 3650 4380 5110
Cumulation Survival Curve
%
No shock STORM
ICD shock
Significato prognostico Storm aritmico Discrepanza in letteratura
Pazienti con storm aritmico non prognosticamente negativo:
- Credner SC, et al. JACC 1998; 32:1909-1915 (136 pts con ICD - Grene M, et al. Europace 2000; 2:263-269 (227 pts con ICD)
Storm aritmico come predittore di maggiore mortalità cardiaca: - Villacastin J, et al.Circulation 1996; 93:753-762 (80 pts con ICD) - Exner DV, et al. Circulation 2001; 103:2066-2071 (457 pts con ICD) - Gatzoulis K, et al. Europace 2005; 7:184-192 (169 pts con ICD) - Manolis AG, et al. MESPE J 2003; 3:135-138 (145 pts con ICD) - Verma A, et al. J Cardiovasc Electrophysiol 2004; 15:1265-1270 (208 pts con ICD)
Jordaens LJ, Mekel JM. Editoriale – Europace 2005; 7:181-183
Sottolineano come le maggiori casistiche danno un significato prognostico negativo allo storm -> mortalità aumentata per insufficienza cardiaca
In realtà la prognosi dipende molto di piu� dalla causa che induce lo storm e dalla persistenza della stessa.
Visione terapeutica
- Non mirata solo all�interruzione della tachiaritmia -> la causa puo� persistere e autoalimentare lo storm - Non mirata a farmaci antiaritmici ->
possono ridurre lo storm ma anche peggiorarlo con effetto «proaritmico»
- Mirata principalmente a cercare di capire e rimuovere la causa: - ischemia (PTCA/bypass) - squilibrio elettrolitico - studio ed eventuale rimozione di macrocircuiti di rientro ventricolare (mappaggio e ABLAZIONE)
La rivascolarizzazione miocardica come risoluzione del riscaldamento aritmico in pazienti con defibrillatore-cardiovertitore impiantabile (ICD): due casi clinici. Paffoni P, Bortnik M, Pedrigi C, Perucca A, Occhetta E, Vassanelli C. Italian Heart Journal Supplement 2000; 1(12):1591-1596.
1° caso: GL, m, 74 ys. 3 mesi dopo ICD: 70 shock appropriati per storm elettrico -> lidocaina 3 Bypass aorto-coronarici in urgenza
2° caso: CG, m, 68 ys. Rivascolarizzazione con bypass e impianto ICD Dopo 6 anni storm elettrico
-> PTCA su safena stenotica critica su coronaria destra
Catheter ablation of ventricular fibrillation triggers and electrical storm. Vern Hsen Tan, Jonathan Yap, li-Fern Hsu, Reginald Liew. (Singapore) Europace 03/2012; DOI:10.1093/europace/eus050
Ventricular tachycardia ablation in implantable cardioverter-defibrillator recipients: a need to catch up with current recommendations Katja Zeppenfeld. Europace (2012) 14(6): 778-780
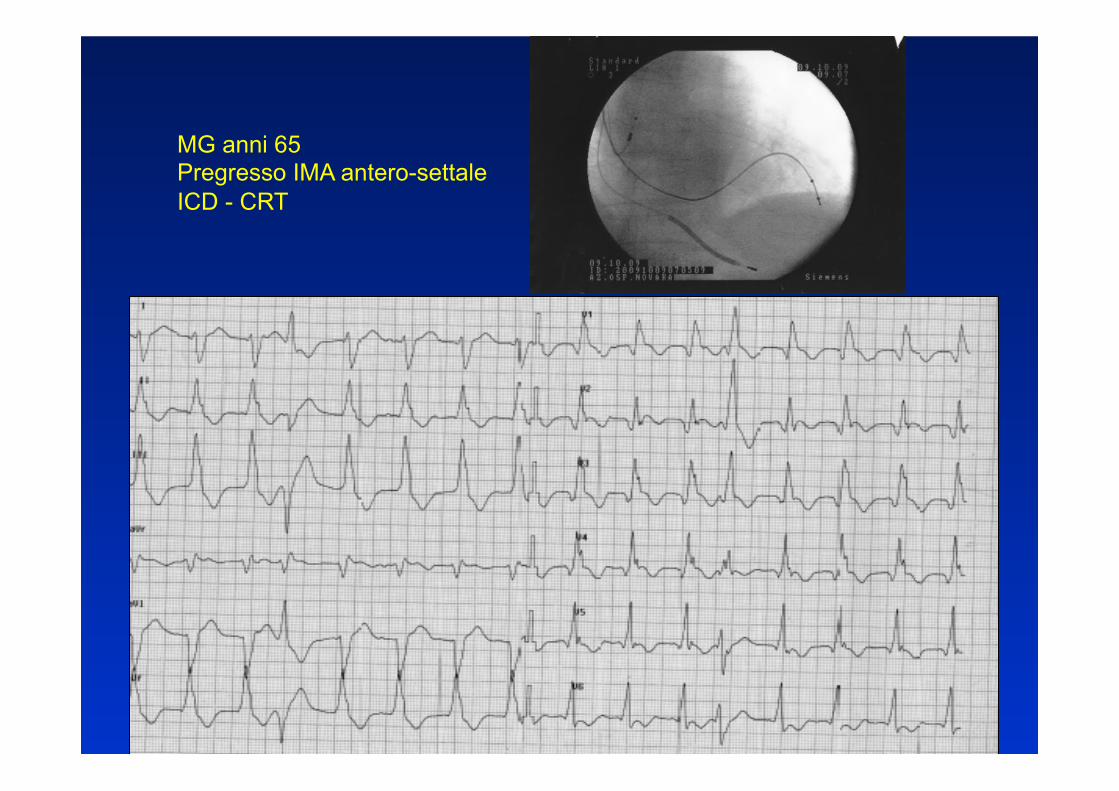
MG anni 65 Pregresso IMA antero-settale ICD - CRT
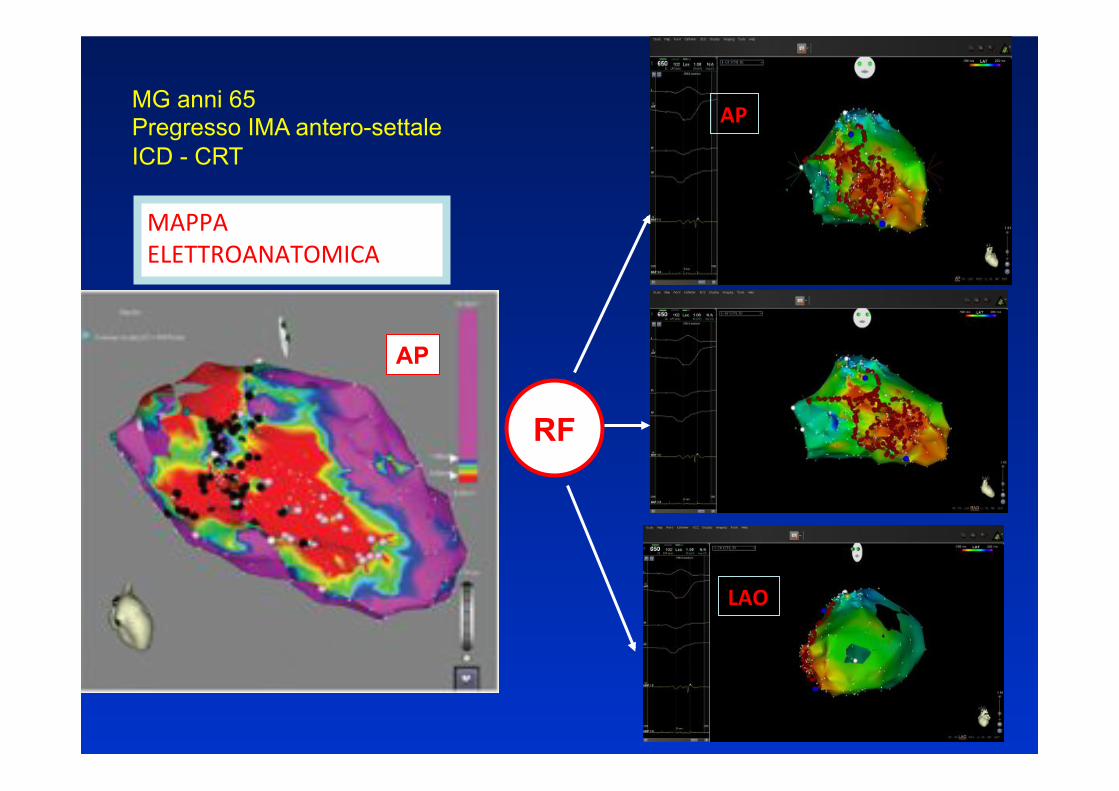
MG anni 65 Pregresso IMA antero-settale ICD - CRT
AP#
LAO#
AP
MAPPA$ELETTROANATOMICA$
RF
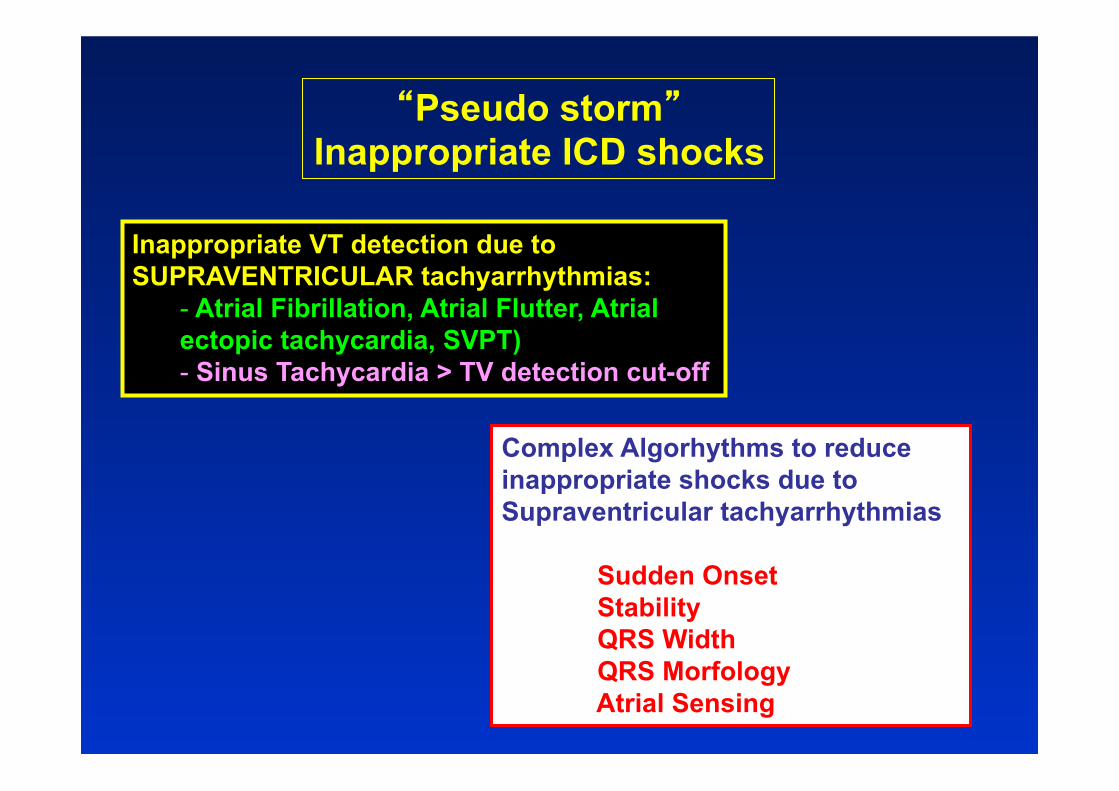
Inappropriate VT detection due to SUPRAVENTRICULAR tachyarrhythmias:
- Atrial Fibrillation, Atrial Flutter, Atrial ectopic tachycardia, SVPT) - Sinus Tachycardia > TV detection cut-off
Complex Algorhythms to reduce inappropriate shocks due to Supraventricular tachyarrhythmias
Sudden Onset Stability QRS Width QRS Morfology Atrial Sensing
�Pseudo storm� Inappropriate ICD shocks
OFF
SVT SVT
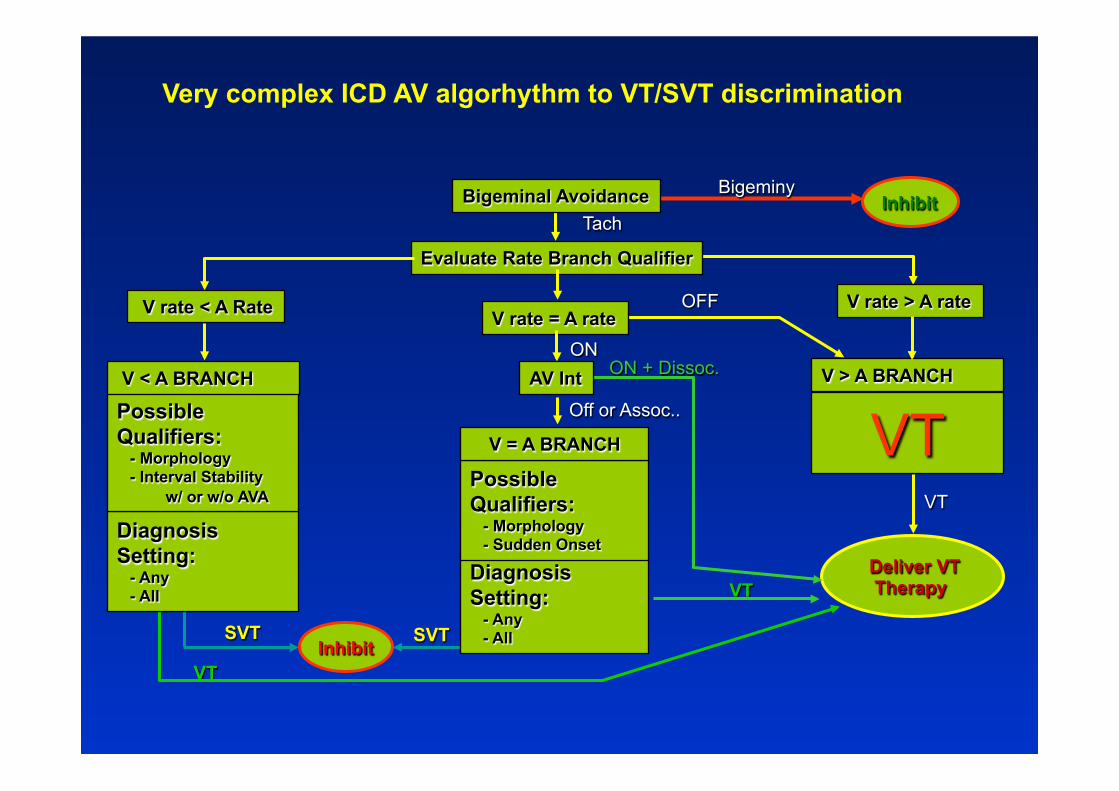
V rate > A rate
V > A BRANCH
Evaluate Rate Branch Qualifier
Tach
VT
Diagnosis Setting: - Any - All
Possible Qualifiers: - Morphology - Sudden Onset Diagnosis
Setting: - Any - All
Possible Qualifiers: - Morphology - Interval Stability w/ or w/o AVA
VT
Deliver VT Therapy
VT
Inhibit Bigeminy Bigeminal Avoidance
VT
ON + Dissoc.
V rate = A rate V rate < A Rate
V < A BRANCH AV Int ON
Off or Assoc..
V = A BRANCH
Inhibit
Very complex ICD AV algorhythm to VT/SVT discrimination
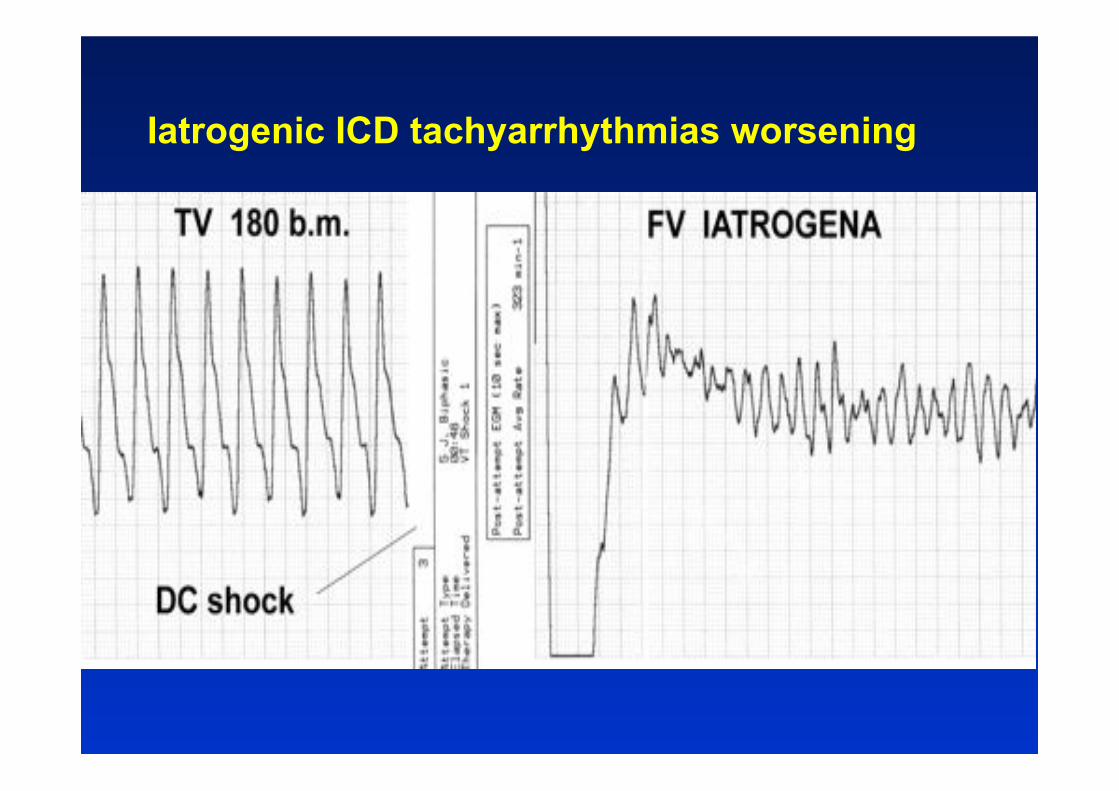
Iatrogenic ICD tachyarrhythmias worsening
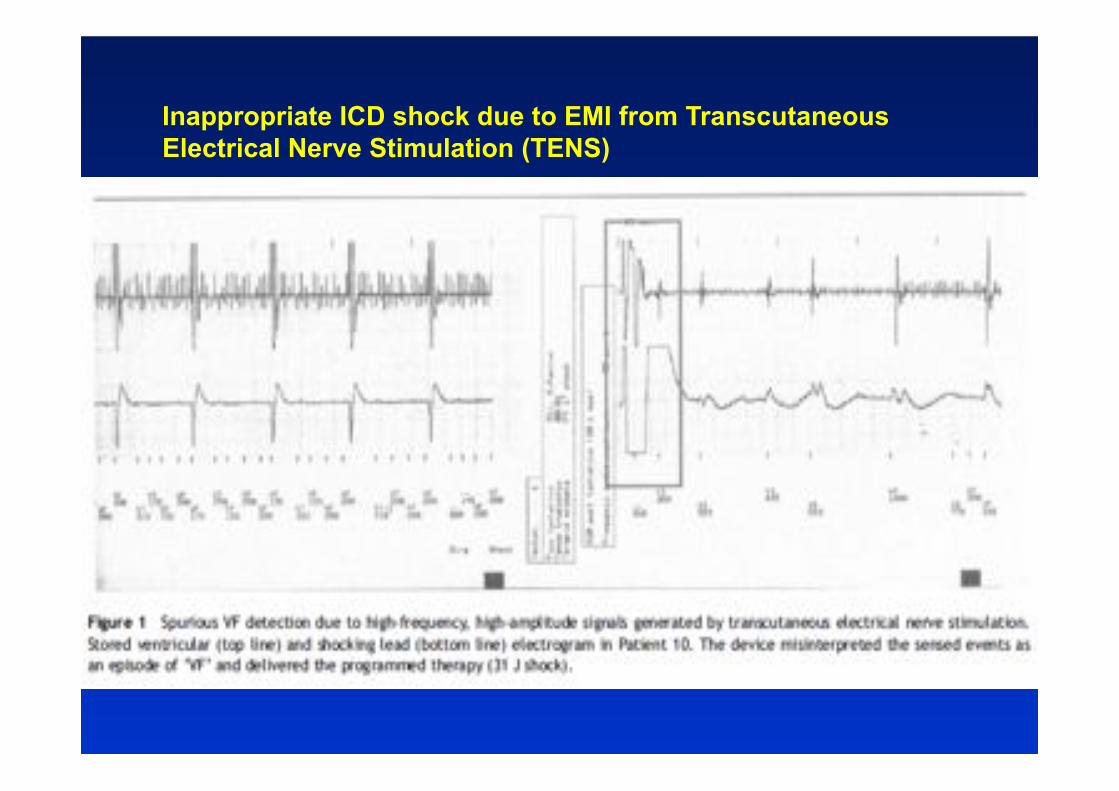
Inappropriate ICD shock due to EMI from Transcutaneous Electrical Nerve Stimulation (TENS)

�NOISES� due to a bad connection between lead and extension False VF detection and inappropriate shock ICD site change (abdominal -> pectoral) without extension

Abdominal myopotentials misdetected as VF potentials: pacing inhibition and inappropriate shock New additional pacing-sensing septal lead

TRIPLE signals detection: R1-R2-T waves Pseudo high rate (VF zone) and inappropriate shocks
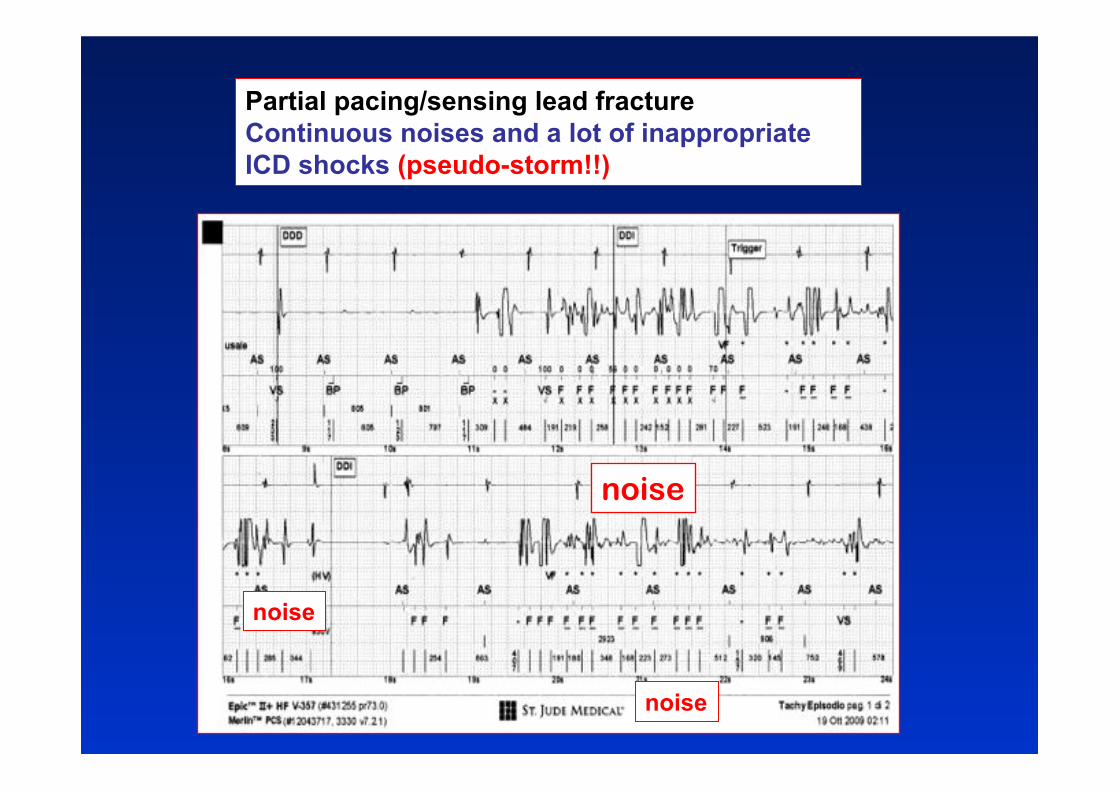
Partial pacing/sensing lead fracture Continuous noises and a lot of inappropriate ICD shocks (pseudo-storm!!)
noise
noise
noise
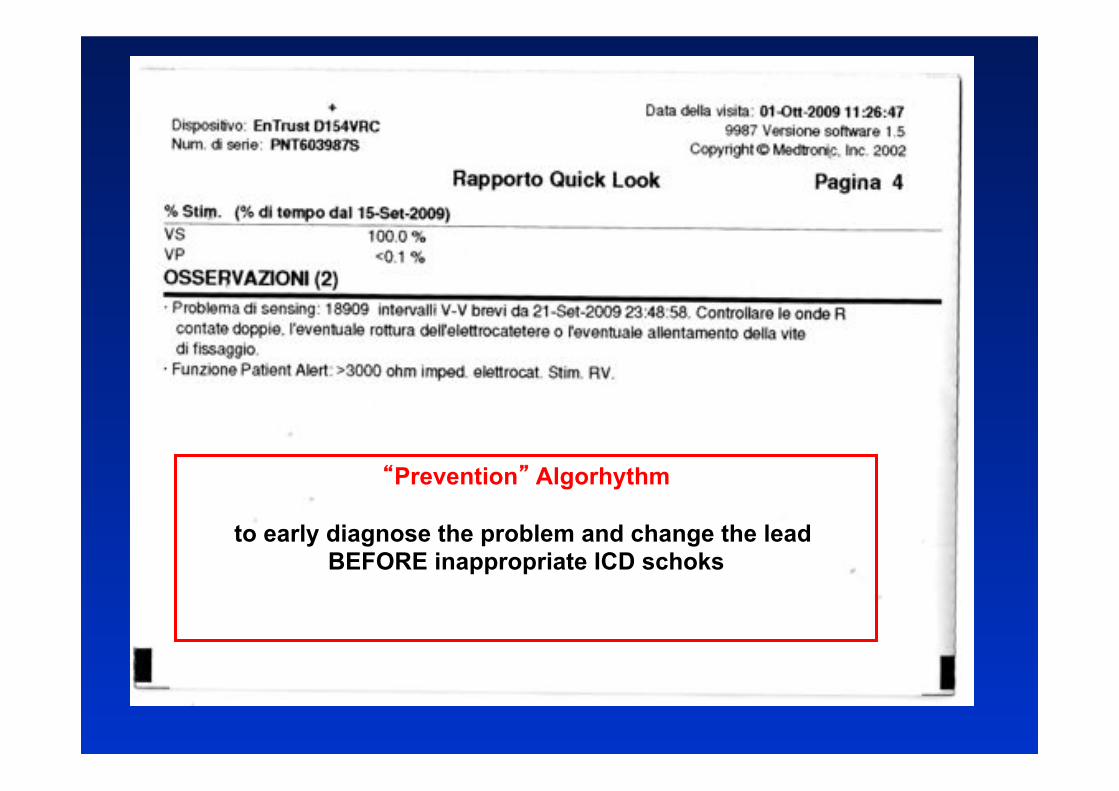
�Prevention� Algorhythm
to early diagnose the problem and change the lead BEFORE inappropriate ICD schoks
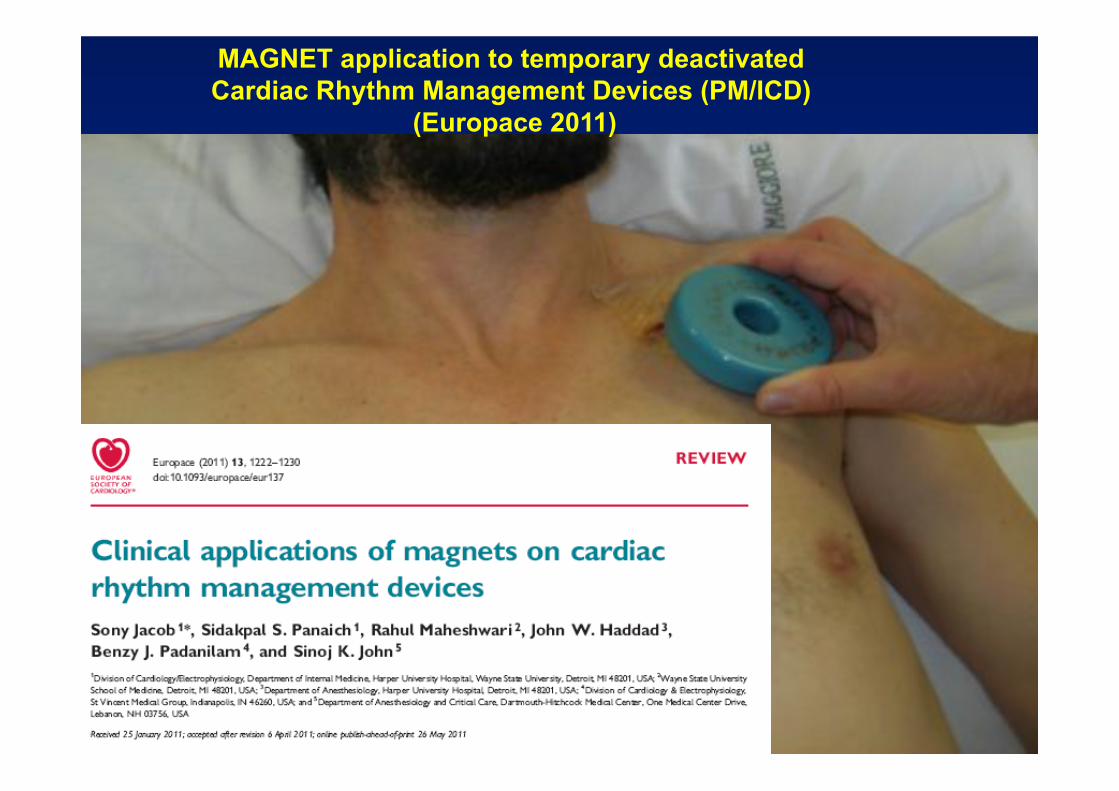
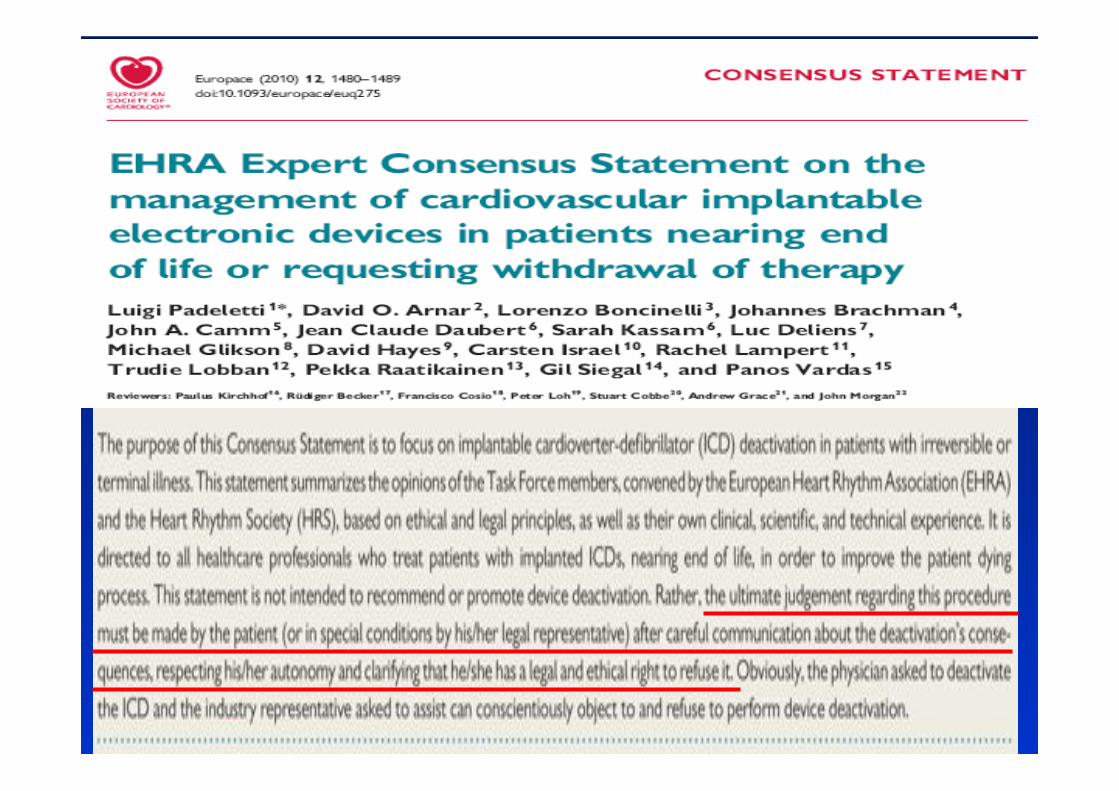
MAGNET application to temporary deactivated Cardiac Rhythm Management Devices (PM/ICD)
(Europace 2011)
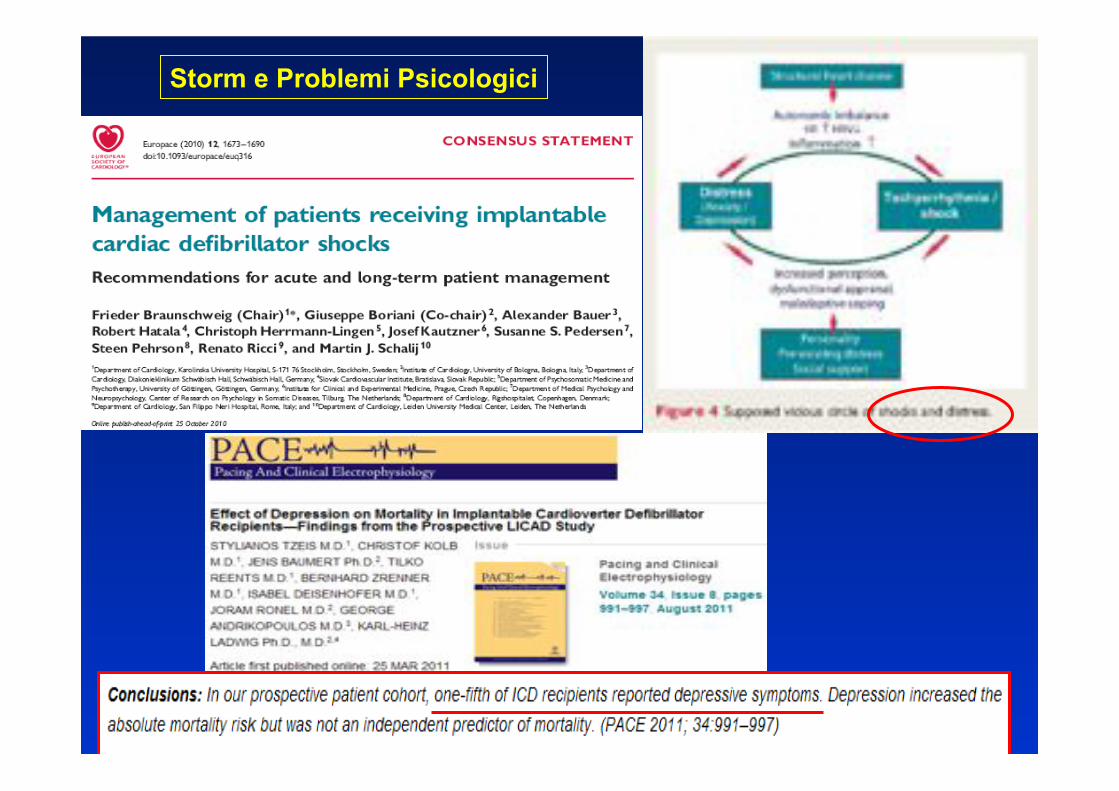
Storm e Problemi Psicologici
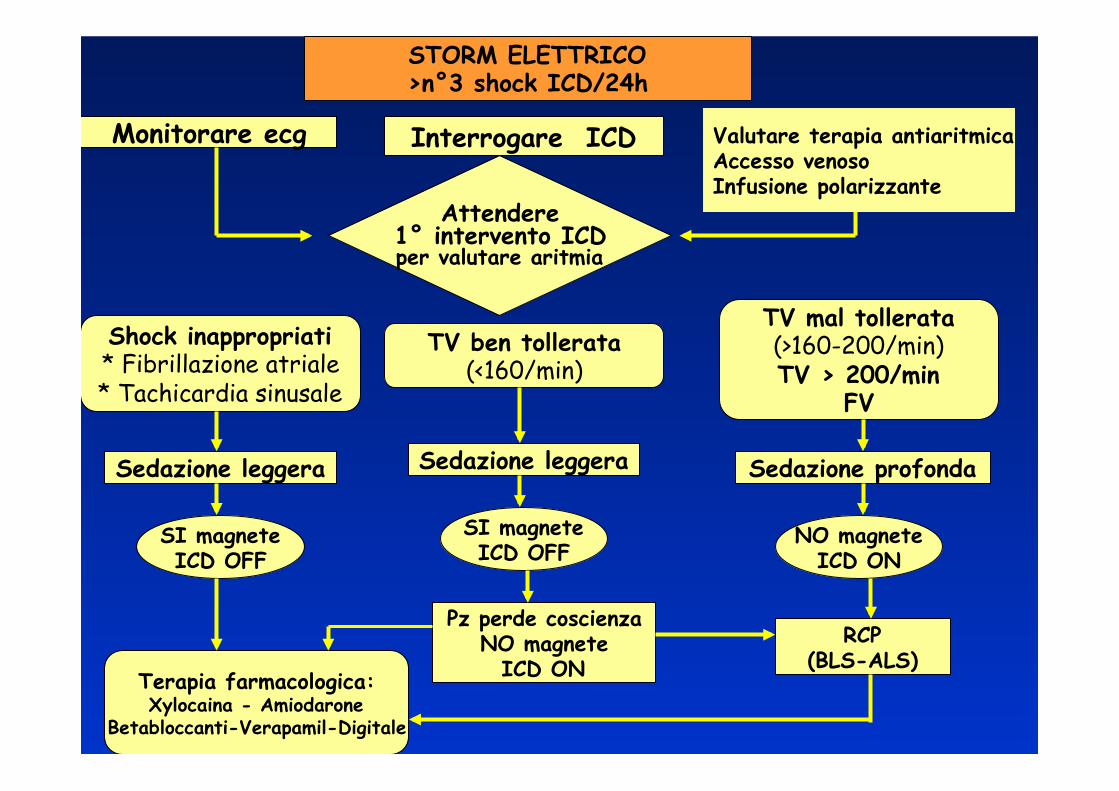
STORM ELETTRICO >n°3 shock ICD/24h
Monitorare ecg Valutare terapia antiaritmica Accesso venoso Infusione polarizzante
Interrogare ICD
Attendere 1° intervento ICD per valutare aritmia
Shock inappropriati * Fibrillazione atriale * Tachicardia sinusale
TV ben tollerata (<160/min)
TV mal tollerata (>160-200/min) TV > 200/min
FV
Sedazione leggera Sedazione leggera Sedazione profonda
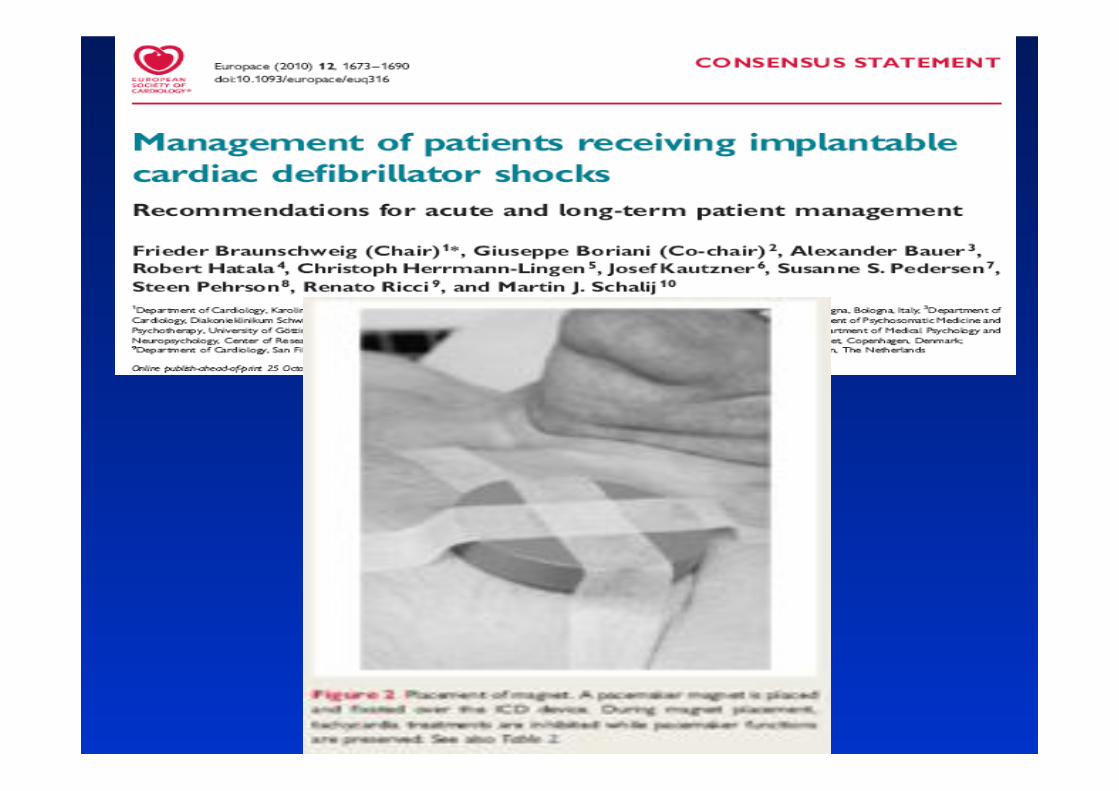
SI magnete ICD OFF
SI magnete ICD OFF NO magnete
ICD ON
Pz perde coscienza NO magnete
ICD ON RCP
(BLS-ALS) Terapia farmacologica: Xylocaina - Amiodarone
Betabloccanti-Verapamil-Digitale
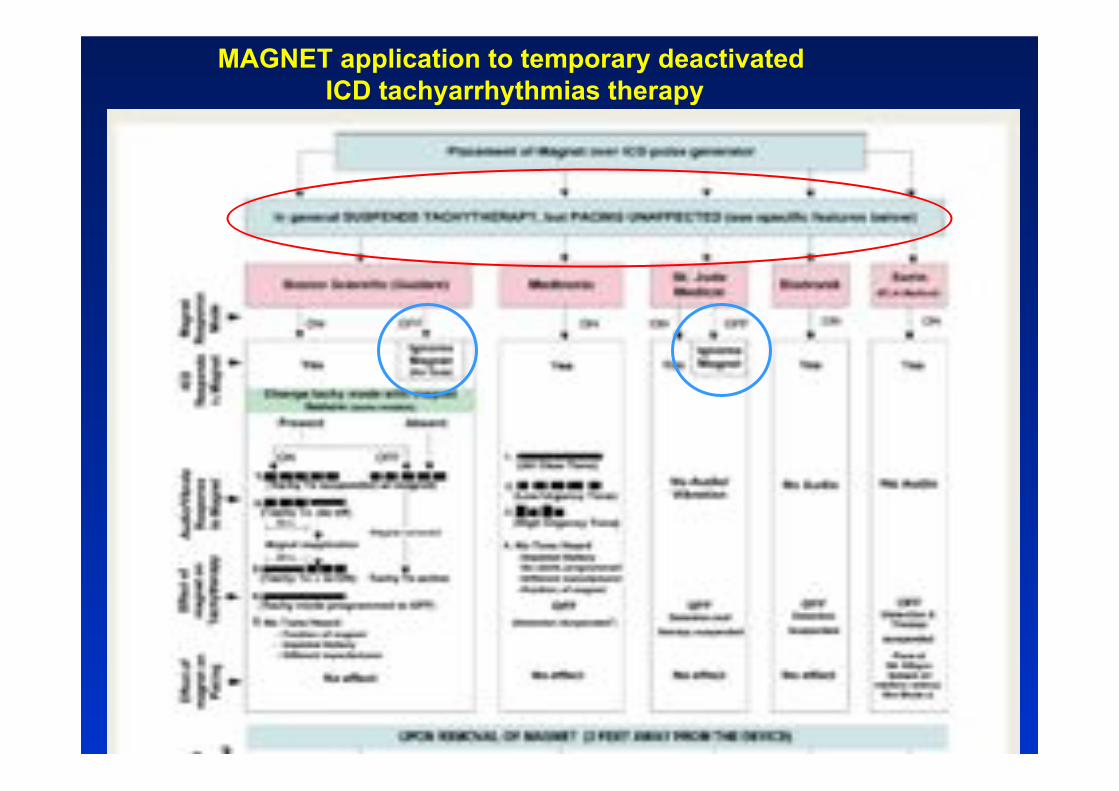
MAGNET application to temporary deactivated ICD tachyarrhythmias therapy
45
Electrical storm in ICD patients: - a dramatic experience for the patient - a hard emergency for the cardiologic equipe
(physicians and nurses)
Conclusione
Grazie per l�attenzione