Clin monit nm apice2002
85
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA) Clinical monitoring: muscle relaxants Claudio Melloni Direttore Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
-
Upload
claudio-melloni -
Category
Health & Medicine
-
view
133 -
download
0
description
Clinical monitoring of muscle relaxants
Transcript of Clin monit nm apice2002

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Clinical monitoring:muscle relaxants
Claudio Melloni
Direttore Servizio di Anestesia e Rianimazione
Ospedale di Faenza(RA)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Innervator Fisher & Paykel e TOfWatch Organon

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Residual curarization
Is the main problem?

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
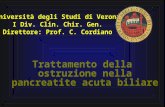
Frequency of residual curarization
0
5
10
15
20
25
30
35
40
45
% of patients postop
Viby 1979
Beemer
Pedersen
Bevanpanc

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Ballard et al.Residual curarization in the recovery room after
vecuronium.BJA 2000;84:394-
Incidence of residual block following vecu evaluated in the RR in 565 patients:
nerve stimulator not used and block not antagonized
RE:clinicallly significant residual block found in 42% of patients;33% extubated before the arrival in RR.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Is your practice different?

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
POPC after pancuronium and atracurium(Pedersen AAS 1992;36;312-18)
0
2
4
6
8
10
12
%
POPC
panc
atrac
1559
1057

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Viby Mogensen et al,AAS 1997
• 693 paz.randomizzati,cieco
• chir elettiva
• monitoraggio periop con Myotest e Tof
• confronto fra 1-5-2 ED95 diatrac,vecu,panc.
• Antagonismo se necessario;
• estubaz a tof eguale, tattile e resp adeguata.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Paralisi residua e % di tof<0.40 in RR,subito dopo trasferimento
0
5
10
15
20
25
30
35
40
45
Tof <0.70 tof<0.40
panc
atrac
vecu

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Residual neuromuscular block and POPC
TOFR Panc Atrac & vecu
>0.7 4,8% 5,4%
<0.7 16,9%* 4,2%

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Andamento temporale del tof <0.80 nella RR
0
10
20
30
40
50
0 5 10 15 20 30 40 50
min
% t
of<
0.8
0
panc
atrac
vecu

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Risk of POPC following abdominal surgery
0
10
20
30
40
50
60
70
20 30 40 50 60 70 80
age
%panc
vecu & atra

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Postoperative pulmonary complications
0
5
10
15
20
%
popc popc conbloccoresiduo
popcsenzabloccoresiduo
pancvecu
atracpanc
vecu
atrac

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Popc secondo il tipo di chirurgia
0
2
4
6
8
10
12
14
16
%
popc
addom
ortop
ginecol

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Fattori di rischio per POPC nello studio AAS 1997
Tipo di chirurgia;freq * 2-10(addominale) età:ogni 10 anni * 1.68 durata di anestesia(> o < 200 min)*3.3 panc e tof<0.70:*5

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
How to avoid residual nmblock
Do not use long acting nmb Monitoring!!! At a minimun,measure TOFR at the end
of the case without antagonizing or before antagonizing
consider always the response to nerve stimulation together with clinical signs and symptoms…..

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Clinical tests of postoperative
neuromuscular recovery
Unreliable» sustained eye opening
» tongue protrusion
» arm lift to opposite shoulder
» normal TV
» normal or near normal VC
» max insp pressure < = 25 cmH2O
Reliable» sustained head lift for 5
sec» sustained arm lift for 5
sec» sustained hand grip for
5 sec» sustained tongue
depressor test» max insp press > 50
cm H2O

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Kirkegaard H,Heier T,Caldwell JE Efficacy of tactile guided reversal from cisatracurium
induced neuromuscular block.Anesthesiology 2002;96:45-50
Anest with fent/prop/N2O cisatrac 0.15 mg/kg neostigmine 0.07 mg/kg administered at
reappearance of I,II,III,IV of TOF;tactile vs Meccanomyography contralateral.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Time from neostigmine administration to TOFR
0.70
0,00
5,00
10,00
15,00
20,00
25,00
I twitch II twitch III twitch IV twitch
low
max
min
mediana

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Time from neostigmine administration to TOFR 0.80
0
10
20
30
40
50
60
70
80
I twitch II twitch III twitch IV twitch
low
max
min
mediana

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Time from neostigmine administration to TOFR 0.90
0
10
20
30
40
50
60
70
80
I twitch II twitch III twitch IV twitch
low
max
min
mediana

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
MMG magnitude of the first TOF twitch(T1) measured at the reappearance of each of the 4
tactile TOF responses.
0
10
20
30
40
50
60
70
80
I twitch II twitch III twitch IV twitch
T1
%
low
max
min
mediana

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Kirkegaard H,Heier T,Caldwell JE Efficacy of tactile guided reversal from cisatracurium induced
neuromuscular block.Anesthesiology 2002;96:45-50
This study shows that achieving a TOFR of 0.90 in <10 min following neostigmine reversal is not a realistic goal;therefore counting the number of tactile responses to tof stimulation cannot be used as a guide for neostigmine admninistration if the end point of reversal is a TOFR of 0.90 or higher within
10 min;but is a good predictor of TOFR 0.70.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Kopman et al.Relationship of the train of four fade ratio to clinical signes and symptoms of
residual paralysis in awake volunteers.Anesthesioloogy,1997;86:765-71.
Volontari sani infusione di mivacurium monitoraggio Datex 221 NMT valutazione;stretta di mano sollev,testa & gamba per 5 sec. Ritenzione di abbassalingua

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Clinical signs of residual weakness vs
tof at the AP(Kopman,Anesthesiology,1997;86:765-71)
0,000,100,200,300,400,500,600,700,800,90
lowest tof highest tof
at which test passed or failed
head lift
leg lift
retain tonguedepressor

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Osservazioni cliniche sulla relazione fra tof e correlati di forza:
disturbi visivi sempre con tof di 0.90(diplopia,diff.seguire oggetti in moto,ecc)
forza dei masseteri ridotta sempre sollev.testa e gamba sempre possibile > 0.60 stretta di mano variabile,ma 83% del basale a tof
0.90 per tof < 0.75 tutti disturbati

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Conclusioni delle correlazioni fra segni clinici di forza muscolare e tof
Capacità di ritenzione dell’abbassalingua è un test più sensibile del sollevamento del capo
tof <1 ancora residuano disturbi visivi e senso generalizzato di fatica
tof = 1 (o altri monitoraggi) per dimissione in chirurgia ambulatoriale??

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Assiomi della ripresa nm.
TOF > 0.70 sicuro indice della ripresa nm……….. Ali HH, Wilson RS, Savarese JJ, Kitz RJ: The effect of tubocurarine on indirectly elicited train-of-four muscle response and respiratory measurements in humans. Br J Anaesth 47:570-4, 1975
Brand JB, Cullen DJ, Wilson NE, Ali HH: Spontaneous recovery from nondepolarizing neuromuscular blockade: Correlation between clinical and evoked responses. Anesth Analg 56:55-8, 1977

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Mutazioni occorse
Esplosione della chirurgia ambulatoriale pressione per la diminuzione della
spesa sanitaria aumento delle persone anziane e
debilitate anche in chir amb. Disponibilità di nuovi farmaci

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Rivalutazione della pratica clinica
Età e stato di salute differiscono fra volontari sani e pazienti!
La prassi clinica e l’utilizzo dei miorilassanti variano fra i diversi centri ambulatoriali
il monitoraggio degli effetti nm non è praticato in ospedale,figurarsi nei centri ambulatoriali!
I metodi di monitoraggio usati da Kopman et al si applico ad una ampia gamma di situazioni cliniche.
Esistono pesanti pressioni economiche per la diminuzione della spesa sanitaria.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Implicazioni del lavoro di Kopman:1
I paz chirurgici sono in genere più anziani e ammalati dei volontari sani dello studio di Kopman/( ASA 1, entro il 15% del peso ideale,tra 23—33 anni….)
gli effetti residui dei miorilassanti è probabile possano essere + significativi nella pratica ambulatoriale con pazienti + anziani e debilitati.
Si potrebbe arguire che i paz.con sedazione residua siano meno attenti a disturbi visivi e
debolezza dei muscoli facciali;ma è anche vero che dal punto di vista della sicurezza i paz postop siano esposti a rischio maggiore di aumento della morbilità,poichè la debolezza residua nm può essere aggravata da residui dell’anestesia.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Implicazioni del lavoro di Kopman:2
mivacurium non è rappresentativo dei miorilassanti usati in chir amb;il mercato è dominato dai miorilassanti ad azione intermedia quali vecuronium, atracurium, rocuronium, cisatracurium
se una paralisi residua permane per un’ora dopo interruzione del mivac,caratterizzato da un RI di pochi min,che succede dopo la somministrazione dei mioril a durata intermedia(RI 20-30 min )?

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Conclusions form Kopman,Brull,Erikkson…..
indicators of recovery of nm function should be changed.
The TOF ratio <0.9 was also associated with functional impairment of the pharynx and upper correlated volunteers' subjective feelings of partial neuromuscular weakness with the clinical counterpart of neuromuscular recovery. All subjects had significant signs and symptoms of residual paralysis at a TOF ratio of 0.7 and satisfactory recovery of neuromuscular function after mivacurium-induced neuromuscular block required return of the TOF ratio to >0.9 . According to these studies, the absence of muscle relaxant-induced clinical effects may be defined as the return to a TOF ratio ³0.9 at the AP.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Eriksson LI, Sato M, Severinghaus JW. Effect of a vecuronium-induced partial block on hypoxic ventilatory response. Anesthesiology 1993;
78:693-9. Eriksson LI. Reduced hypoxic chemosensitivity in
partially paralysed man: a new property of muscle relaxants? Acta Anaesthesiol Scand 1996;
40:520-3. When awake volunteers received vecuronium, atracurium, and
pancuronium in small doses to stabilize the adductor pollicis (AP) mechanical train-of-four (TOF) ratio at 0.7, reflex hyperventilation induced by hypoxemia was depressed, whereas the ventilatory response to hypercapnia was entirely normal. Absence of hypoxemia-induced reflex hyperventilation was observed when the TOF ratio returned to 0.9 .

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Corpi carotidei
Sito nicotinico
Sito muscarinico
nmb
atropina
ipossia

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Chemrorecet perif
Chemrecett.centr SNC
Ipossia
ipercapnia iperventilazione

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Conclusioni
Esiste evidenza sperimentale e clinica che i nmb nondepolarizzanti inteferiscano con il controllo della ventilazione in condizioni di ipossia,verosimilmente attraverso una depressione reversibile della attività chemorecettoriale dei corpi carotidei implicazioneclinica

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Problems of tactile or visual assesmentProblems of tactile or visual assesmentusingusing
STST
basalbasal
frequence..frequence..
TOFTOF
fade assessment needsexperiencefade assessment needsexperience
sensibility when IV reappears:whichis the IV/I ratio > 25-30%?sensibility when IV reappears:whichis the IV/I ratio > 25-30%?
tetanictetanic
fade assessmentneeds experiencefade assessmentneeds experience
do not repeat < 5min..do not repeat < 5min..

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Correlazione soggettiva-oggettiva(palpazione-meccanomiografia)
1 Twitch= T110%
3 twitches=T1 25%

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
tactile assessmenttactile assessment
TetanusTetanus
DBSDBS
TOFTOF

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Clinical signsClinical signscorrelation with residual forcecorrelation with residual force
patient cooperation!patient cooperation!
tonguedepressorclenching
tonguedepressorclenching
head lift> 5 sechead lift> 5 sec
arm or leglift> 5 secarm or leglift> 5 sec
sustainedhand gripstrenght
sustainedhand gripstrenght

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
clinical signsclinical signsreliable vs not reliablereliable vs not reliable
TV normalTV normal unreliableunreliable
Neg Press < 25 mmHgNeg Press < 25 mmHgunreliableunreliable
Neg press < 50 mmHgNeg press < 50 mmHgreliablereliable
coughcough unreliableunreliable
eye openingeye openingunreliableunreliable
tongue protrusiontongue protrusionunreliableunreliable
before patient cooperationri....before patient cooperationri....

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
faccia da culo te e tua mamma l’ha detto pischerl
Fisinternatiuonalchler Switzerland.Intensive Care Med 2000 Oct;26(10):1428-33)
0
5
10
15
20
25
30
35
poi
mia
tua
sua nostra
ecce

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Special neuromuscular
monitoring
Mantiene quello che promette?

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)Servi zi o di Anestesia e Rianimazione Ospedale di Faenza(RA)
TOF,DBS , Tetanus

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Drenck NE, Ueda N, Olsen NV, et al. Manual evaluation of residual curarization using double burst stimulation: A comparison with train-of-
four. Anesthesiology 1989; 70:578-81
- Double burst stimulation (DBS) is a new mode of stimulation developed to reveal residual neuromuscular blockade under clinical conditions. The stimulus consists of two short bursts of 50 Hz tetanic stimulation, separated by 750 ms, and the response to the stimulation is two short muscle contractions. Fade in the response results from neuromuscular blockade as with train-of-four stimulation (TOF). The authors compared the sensitivity of DBS and TOF in the detection of residual neuromuscular blockade during clinical anaesthesia. Fifty-two healthy patients undergoing surgery were studied. For both stimulation patterns the frequencies of manually detectable fade in the response to stimulation were determined and compared at various electromechanically measured TOF ratios. A total of 369 fade evaluations for DBS and TOF were performed. Fade frequencies were statistically significantly higher with DBS than with TOF, regardless of the TOF ratio level. Absence of fade with TOF implied a 48% chance of considerable residual relaxation as compared with 9% when fade was absent with DBS. The results demonstrate that DBS is more sensitive than TOF in the manual detection of residual neuromuscular blockade.
:
AB

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Probability of being within defined TOFR intervals when different clinical fade evaluations are given
(Drenck NE, Ueda N, Olsen NV, et al. Manual evaluation of residual curarization using double burst stimulation: A comparison with train-of-four.
Anesthesiology 1989; 70:578-81)
0
10
20
30
40
50
60
%
no tof fade no tof,no dbs fade fade in dbs,not tof
tof<0.4
tof 0.41-0.50
tof 051-0.60
tof 0.61-0.70
tof >0.70

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Dbs 3-3 Drenck NE, Ueda N, Olsen NV, et al. Manual evaluation of residual curarization
using double burst stimulation: A comparison with train-of-four. Anesthesiology 1989; 70:578-81)
Absence of fade with tof implies a 52% probability than tof>0.60
absence of fade with dbs implies a tof >0.60 in 91% of cases
only tOFR<0.40 can be assessedd manually therefore,evaluation of DBS is relevant only
when there is no fade to tof

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Conclusions:Drenck NE, Ueda N, Olsen NV, et al. Manual evaluation of residual curarization
using double burst stimulation: A comparison with train-of-four. Anesthesiology 1989; 70:578-81)
absence of fade to DBS normally excludes severe residual nm blockade(tofr<0.60) BUT DOES NOT NECESSARILY INDICATE ADEQUATE CLINICAL RECOVERY.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Meccanomiographic vs tactileevaluation
Meccanomiographic vs tactileevaluation
Drenck et al.Anesthesiology 79;578:1989.Drenck et al.Anesthesiology 79;578:1989.
qualitative tofevaluation
qualitative tofevaluation
48% chances ofevaluating a real fade48% chances ofevaluating a real fade
qualitative DBSevaluation
qualitative DBSevaluation
9% chances of nondiscerning a real fade9% chances of nondiscerning a real fade

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Viby-Mogensen J, Jensen NH, Engbæk J, Ørding H, Skovgaard LT, Chæmmer-Jørgensen B. Tactile and
visual evaluation of response to train-of-four nerve stimulation. Anesthesiology 1985; 63:440-
3.
Diaz/tps/N2O 66%/haloth 0.75-1.5% IOT with SCC ,then panc simult MMG in one arm & visual/tactile
evaluation in the opposite. Experienced and (inexperienced)
anesthesiologists 6 different TOFR forn every patient

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Viby-Mogensen et al Tactile and visual evaluation of response to train-of-four nerve stimulation.
Anesthesiology 1985; 63:440-3.
0
10
20
30
40
50
60
70
80
90
100
fade observed
%
inexp.observers exp.observers
true tofr <0.30
true tof 0.31-0.40
true tof 0.41-0.50
true tof 0.51-0.60
true tof 0.61-0.70
true tof>0.70

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Threshold fade by 3 very experienced observers (Viby-Mogensen et al. Tactile and visual evaluation of
response to train-of-four nerve stimulation. Anesthesiology 1985; 63:440-3)
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
visual manual
onset
offset

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Threshold fade by 3 very experienced observers (Viby-Mogensen et al. Tactile and visual evaluation of
response to train-of-four nerve stimulation. Anesthesiology 1985; 63:440-3.)
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
visual onset visual recovery manual onset manual recovery
TO
FR
max
min
mean

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Which is the TOFR level that can be reliably detected visually by observing tetanic fade of the AP in response to 100-Hz, 5-s tetanus in anesthetized patients.?

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baurain M,Hennart DA,Godschalx A,Huybrechts I,Nasrallah G,d'Hollander AA., Cantraine F.Visual
Evaluation of Residual Curarization in Anesthetized Patients Using One Hundred-Hertz, Five-Second
Tetanic Stimulation at the Adductor Pollicis Muscle .Anesth Analg 1998; 87:185–9 We were looking for a clinical test to indicate a train-of-four (TOF) ratio of approximately 0.9. We
compared the adductor pollicis muscle (AP) visually evaluated response to ulnar nerve 100-Hz, 5-s tetanus (RF100 Hz) with the measured AP TOF ratio in 30 ASA physical status I or II adult anesthetized (propofol, sufentanil, N2O/O2) patients. After the induction of anesthesia, the left ulnar nerve was stimulated at the wrist (single twitch and TOF) and the resultant isometric force was measured. When TOF was assessed, the independent investigators, unaware of the left AP-
measured TOF ratios, visually evaluated the presence or absence of AP fading elicited by right ulnar nerve 100-Hz, 5-s tetanus. The 30 patients were randomly allocated to receive either 0.5 mg/kg atracurium (n = 15) or 0.1 mg/kg vecuronium (n = 15). The neuromuscular blockade was allowed to resolve spontaneously. A multiple logistic regression analysis was performed by computing the 771 visual observations. The probabilities of success of 100-Hz, 5-s tetanus to detect TOF ratios of 0.8, 0.85, and 0.9 were 99%, 96%, and 67%, respectively. The sensitivity and specificity of 100-Hz, 5-s tetanus as an indicator of TOF ratios of 0.85 and 0.9 are 100% and 75%, 54% and 67%, respectively. We conclude that RF100 Hz visual assessment seems to be highly sensitive in evaluating residual paralysis, as the absence of RF100 Hz visual fading at the AP is compatible with a TOF ratio >0.85. Implications: After the administration of muscle relaxants, the absence of visual fading at the adductor pollicis, elicited in anesthetized patients by 100-Hz, 5-s tetanus, is compatible with a train-of four ratio >0.85. Therefore, clinical observation of fading after 100-Hz, 5-s tetanus seems to be a highly sensitive test in evaluating residual paralysis.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baurain et al.Visual Evaluation of Residual Curarization in Anesthetized Patients Using One
Hundred-Hertz, Five-Second Tetanic Stimulation at the Adductor Pollicis Muscle .Anesth Analg 1998;
87:185–9

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baurain et al.Visual Evaluation of Residual Curarization in Anesthetized Patients Using One Hundred-Hertz, Five-Second Tetanic Stimulation at the Adductor Pollicis Muscle .Anesth Analg
1998; 87:185–9

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Saitoh, Y.1*; Narumi, Y.1; Fujii, Y.2; Ueki, M.3
Tactile evaluation of fade of the train-of-four and double-burst stimulation using the anaesthetist's non-dominant hand Br. J. Anaesth. 1999; 83:275-
278 We have studied detection of fade in response to train-of-four (TOF),
double-burst stimulation3,3 (DBS3,3) or DBS3,2, assessed tactilely by the anaesthetist using the index finger of the non-dominant hand and the thumb of the patient, compared with that assessed when the index finger of the dominant hand was used. The probability of detection of any fade in response to TOF or DBS3,3 using the non-dominant hand was significantly less than when the dominant hand was used (P<0.05). The probability of identification of fade in response to DBS3,2 assessed using the non-dominant hand was comparable with that evaluated using the dominant hand when TOF ratios were 0–0.9, but when TOF ratios reached 0.91–1.00, detection using the non-dominant hand was significantly less common than with the dominant hand (12% vs 33%; P<0.05). Using the non-dominant hand, the probability of detection of fade in response to ulnar nerve stimulation was less than that with the dominant hand and only the absence of DBS3,2 fade ensured sufficient recovery of neuromuscular block.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Saitoh Y,Nakazawa K, Makita K,Tanaka H, Amaha K.Evaluation of Residual Neuromuscular Block
Using Train-of-Four and Double Burst Stimulation at the Index Finger Anesth Analg 1997; 84:1354
We examined the percentage of tactile detection of fade in response to train-of-four (TOF), double burst stimulation3,3 (DBS3,3), or DBS3,2 at the index finger compared with that at the thumb during continuous infusion of vecuronium. One hundred five adult patients were studied. At TOF ratios (T4/T1) of 0.41–0.70, fades in response to TOF were more frequently identified by tactile means at the index finger than at the thumb (58% vs 26%, P < 0.05). Similarly, at TOF ratios of 0.61–0.90, fades in response to DBS3,3 were more frequently detected at the index finger than at the thumb (55% vs 15%, P < 0.05), and at TOF ratios of 0.81–1.00, the percentage of detection of fade in response to DBS3,2 was higher at the index finger than at the thumb (72% vs 40%, P < 0.05). In addition, baseline displacement of the index finger or thumb during tactile assessment of fade in response to neurostimulation was measured videographically. The baseline displacement of the index finger was significantly less than that of the thumb (P < 0.05). In summary, the percentage of tactile detection of fade in response to neurostimulation at the index finger is higher than at the thumb, and the absence of fade in response to DBS3,3 at the index finger is a good indicator of adequate recovery from neuromuscular block. This is probably because of the smaller baseline displacement of the index finger.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
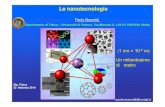
Percentage of tactile detection of fade in response to TOF at the index finger compared with that at the thumb during
continuous infusion of vecuronium (Saitoh Y,Nakazawa K, Makita K,Tanaka H, Amaha K.Evaluation of Residual Neuromuscular Block Using Train-of-Four and
Double Burst Stimulation at the Index Finger Anesth Analg 1997; 84:1354)
0
10
20
30
40
50
60
70
80
90
100
true TOFR
index thumb
<0,20
0,21--0.30
0,31-0,40
0,41-0,50
0,51-0,60
0,61-0,70
0,71-0,80
0,81-0,90
>0,90
True tof

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Percentage of tactile detection of fade in response to DBS 3,3 at the index finger compared with that at the thumb
during continuous infusion of vecuronium (Saitoh Y,Nakazawa K, Makita K,Tanaka H, Amaha K.Evaluation of Residual Neuromuscular Block Using Train-of-Four and Double Burst Stimulation at the Index Finger Anesth Analg 1997; 84:1354)
0
10
20
30
40
50
60
70
80
90
100
true TOFR
index thumb
0-0,40
0,41-0,50
0,51-0.60
0,61-0,70
0,71-0,80
0,81-0,90
>0,90
At TOFR>0.60 fade at index 55% vs thumb 15%

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
THE END

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Fruergaard K, Viby-Mogensen J, Berg H, El-Mahdy AM. Tactile evaluation of the response to double burst stimulation
decreases, but not eliminates, the problem of postoperative residual paralysis. Acta
Anaesthesiol Scand 1998; 42:1168-74 BACKGROUND: Routine perioperative monitoring with accelero-myography might prevent residual block, whereas
routine tactile evaluation of the response to train-of-four (TOF) nerve stimulation does not. The purpose of this prospective, randomised and blinded study was to evaluate the effect of manual evaluation of the response to double burst stimulation (DBS3.3) upon the incidence of residual block. METHODS: Sixty adult patients scheduled for elective abdominal surgery were included in the study. Pancuronium 0.08 to 0.1 mg kg-1 was given for relaxation and tracheal intubation. For maintenance of neuromuscular block, pancuronium 1-2 mg was administered. The patients were randomly allocated into two groups. In group DBS (double burst stimulation) the degree of block during anaesthesia was assessed by manual evaluation of the response to TOF nerve stimulation. During reversal, when no fade was detectable in the TOF response, the stimulation pattern was changed to DBS3.3. The trachea was extubated when the anaesthetist judged the neuromuscular function to have recovered adequately and no fade in the DBS3.3 response could be felt. In group CC (clinical criteria) patients were managed without the use of a nerve stimulator, and the level of neuromuscular block and reversal were evaluated solely on the basis of clinical criteria. In both groups, the TOF ratio was measured by mechanomyography immediately after tracheal extubation. Also, the ability to sustain head lift for 5 s, to protrude the tongue, to open the eyes, and to lift one arm to the opposite shoulder were tested. RESULTS: The TOF ratio, as measured immediately after tracheal extubation, was significantly lower in group CC than in group DBS (means: 0.68 and 0.78, respectively), and the incidence of residual neuromuscular block defined as a TOF ratio < 0.7 was significantly higher in group CC than in group DBS (57 and 24%, respectively). The time from the first TOF measurement until the TOF ratio reached 0.8 was significantly longer in group CC than in group DBs (means: 11.5 and 6.2 min, respectively). No significant differences between the two groups of patients were found in duration of anaesthesia, in times from end of surgery to injection of neostigmine, tracheal extubation or TOF ratio 0.8, in dose of pancuronium, or in any other postoperative variable. CONCLUSION: Routine perioperative manual evaluation of the responses to TOF and DBS3.3 decreased the incidence and the degree of residual block following the use of pancuronium. It did not, however, exclude clinically significant residual paralysis, nor did it influence the amount of pancuronium used during the operation, the duration of anaesthesia or the time from end of surgery to tracheal extubation or to sufficient recovery of neuromuscular function (TOF = 0.8).

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Shorten GD, Merk H, Sieber T. Perioperative train-of-four monitoring
and residual curarization. Can J Anaesth 1995; 42:711-15
It has been suggested that perioperative train-of-four (TOF) monitoring does not reduce the incidence of postoperative residual curarization (PORC). The purpose of this study was to examine whether the use of tactile assessment of the response of the adductor pollicis to supramaximal TOF stimulation of the ulnar nerve at the wrist during anaesthesia affected the incidence of PORC. Thirty-nine ASA I or II surgical patients were studied during thiopentone/fentanyl N2O/enflurane anaesthesia. Pancuronium (70-100 micrograms.kg-1) was used to facilitate tracheal intubation and additional pancuronium increments used to maintain surgical relaxation. The requirement for incremental doses of pancuronium and adequacy of recovery following reversal were assessed according to random allocation, either with (Group A; n = 20) or without (Group B; n = 19) access to TOF monitoring. Patients in the two groups received neostigmine in similar doses (Group A: 53 micrograms.kg-1 (5.9); Group B: 55 micrograms.kg-1 (5.4)). On arrival of the patient to the recovery area, neuromuscular function was assessed electromyographically (using the Datex NMT 221 to measure TOF ratio) and clinically. The incidence of PORC (TOF ratio < 70%) was greater in Group B (47%) than in Group A (15%) (P = 0.029). We conclude that the use of perioperative TOF monitoring decreases the incidence of pancuronium-induced PORC.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Pedersen T, Viby-Mogensen J, Bang U, Olsen NV, Jensen E, Engbæk J. Does
perioperative tactile evaluation of the train-of-four response influence the frequency of postoperative residual
neuromuscular blockade? Anesthesiology 1990; 73:835-9
The authors conducted a randomized controlled clinical trial to evaluate the usefulness of perioperative manual evaluation of the response to train-of-four (TOF) nerve stimulation. A total of 80 patients were divided into four groups of 20 each. For two groups (one given vecuronium and one pancuronium), the anesthetists assessed the degree of neuromuscular blockade during operation and during recovery from neuromuscular blockade by manual evaluation of the response to TOF nerve stimulation. In the other two groups, one of which received vecuronium and the other pancuronium, the anesthetists evaluated the degree of neuromuscular blockade solely by clinical criteria. The use of a nerve stimulator was found to have no effect on the dose of relaxant given during anesthesia, on the need for supplementary doses of anticholinesterase in the recovery room, on the time from end of surgery to end of anesthesia, or on the incidence of postoperative residual neuromuscular blockade evaluated clinically. The median (and range of) TOF ratios recorded in the recovery room were 0.75 (0.33-0.96) and 0.79 (0.10-0.97) in the vecuronium groups monitored with and without a nerve stimulator, respectively. These ratios were significantly higher than those found in the pancuronium groups, which wre 0.66 (0.06-0.90) and 0.63 (0.29-0.95), respectively. However, no difference was found between the vecuronium and pancuronium groups in the number of patients showing clinical signs of residual neuromuscular blockade, as evaluated by the 5-s head-lift test.(ABSTRACT TRUNCATED AT 250 WORDS).

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Fawcett WJ, Dash A, Francis GA, Liban JB, Cashman JN. Recovery from neuromuscular blockade: residual curarisation following
atracurium or vecuronium by bolus dosing or infusions. Acta Anaesthesiol Scand 1995; 39:288-
93. AB - We conducted a survey of the incidence of Postoperative Residual Curarisation
(PORC) in two groups of patients following the use of atracurium or vecuronium. In the first group (B) the neuromuscular blocking drugs were administered by bolus dosing, and in the second group (I) by continuous fusion. On arrival in the recovery room, neuromuscular function was assessed both by compound evoked electromyogram (EMG) in a train of four pattern and also clinically, by the ability to sustain a headlift for > 5 seconds, and to cough. Results were obtained from 150 patients (100 in group B and 50 in group I). The incidence of PORC, as defined by a train of four ratio of < 0.7, on arrival in the recovery room was 12% in group B, and 24% in group I. Clinical criteria of adequate neuromuscular reversal revealed different results, with the majority of patients being unable to perform either clinical test on arrival in recovery. Those patients in whom a peripheral nerve stimulator was used intra-operatively did not have a reduced incidence of PORC. We have demonstrated that PORC is still a common occurrence even with intermediate duration of action neuromuscular blocking drugs.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baillard C, Gehan G, Reboul-Marty J, Larmignat P, Samama CM, Cupa M. Residual curarization in the recovery room after vecuronium. Br J Anaesth 394-5; 2000:84.
2: Viby-Mogensen J, Jørgensen BC, Ørding M. Residual curarization in the recovery room. Anesthesiology 1979; 50:539-41.
3: Bevan DR, Smith CE, Donati F. Postoperative neuromuscular blockade: a comparison between atracurium, vecuronium, and pancuronium. Anesthesiology 1988; 69:272-6.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Residual curarization in the recovery room after vecuronium†
Short Communication
AUTHOR(S): Baillard, C.1*; Gehan, G.1; Reboul-Marty, J.2; Larmignat, P.1; Samama, C. M.1; Cupa, M.1
Br. J. Anaesth. 2000; 84
residual block after anaesthesia(propof/fent/isof)
only vecuronium but no anticholinesterase 568 consecutive patients on admission to the recovery room. The ulnar
nerve was stimulated submaximally using TOF stimulation (30 mA). Postoperative residual curarization was defined as a TOF ratio <0.7

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baillard, C.1*; Gehan, G.1; Reboul-Marty, J.2;
Larmignat, P.1; Samama, C. M.1; Cupa, M
. Of the 568 patients, 239 (42%) had a TOF <0.7 in the recovery room. These patients had received a larger cumulative dose of vecuronium than patients who had full recovery (mean 7.7 (SD 3.6) mg vs 6.2 (2.7) mg; P<0.05) and a shorter time had elapsed since the last vecuronium dose (117 (70) min vs 131 (80) min; P<0.05). Of 435 patients whose trachea was extubated, 145 (33%) exhibited inadequate recovery from neuromuscular block. Six of these had one or no response to TOF stimulation and were reintubated. In the remaining 139 patients, neuromuscular block was successfully antagonized. Only 20 patients (3.5%) remembered TOF stimulation when questioned 2 h later in the recovery room, and discomfort associated with it was assessed using a visual analogue scale before discharge. We conclude that it is necessary to antagonize residual block produced by vecuronium.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Baillard, C.1*; Gehan, G.1; Reboul-Marty, J.2;
Larmignat, P.1; Samama, C. M.1; Cupa, M

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Inadequate recovery from nm block:lieteraure data
author year Nmblocker
Admmode
Assessment:intraop/RR
% ofinadeqreversal
Baillard 200 BJA Vecu intermittent
Clinical/accel
42%

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Bevan DR, Kahwaji R, Ansermino LM, et al. Residual block after mivacurium with or without edrophonium reversal
in adults and children. Anesthesiology 1996; 84:362-7.
AB - BACKGROUND: The rapid recovery from mivacurium- induced neuromuscular block has encouraged omission of its reversal. The purpose of this study was to determine, in children and in adults, whether failure to reverse mivacurium neuromuscular block was associated with residual neuromuscular block on arrival in the postanesthesia care unit. METHODS: In 50 children, aged 2-12 yr, and 50 adults, aged 20-60 yr, anesthesia was induced and maintained with propofol and fentanyl, and neuromuscular block was achieved by an infusion of mivacurium, to maintain one or two visible responses to train-of-four (TOF) stimulation of the ulnar nerve. At the end of surgery, mivacurium infusion was stopped, and 10 min later, reversal was attempted with saline or 0.5 mg x kg(-1) edrophonium by random allocation. On arrival in the postanesthesia care unit, a blinded observer assessed patients clinically and by stimulation of the ulnar nerve with a Datex electromyogram in the uncalibrated TOF mode. RESULTS: Children arrived in the postanesthesia care unit 8.2 +/- 3-4 min after reversal of neuromuscular block and showed no sign of weakness, either clinically or by TOF stimulation. Although TOF ratio was greater in children who had received edrophonium (1.00 +/- 0.05 vs. 0.93 +/- 0.01, P<0.01), TOF was >0.7 in all children. Adults arrived in the postanesthesia care unit 12.9 +/- 5.3 min after reversal of neuromuscular block(P<0.01 vs. children). Six in the saline group demonstrated weakness (two required immediate reversal of neuromuscular block, and TOF was <0.7 in four others), compared with TOF <0.7 in only one of the edrophonium group (P<0.05). CONCLUSIONS: This study demonstrated that, in adults, failure to reverse mivacurium neuromuscular block was associated with an increased incidence of residual block. Such weakness was not observed in children receiving similar anesthetic and neuromuscular blocking regimens.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Dubois PE,Broka S,Joucken KL. TOF-Tube Anesth Analg 2000; 90:232
We would like to present a hand and forearm protection device that optimizes the monitoring of neuromuscular function by accelero-myography in a maximum of surgical procedures while reducing spatial obstructions and offering maximal protection to the patient. In our opinion, this constitutes an evolution compared with the setting systems currently used for this purpose.
The structure is tubular () and made out of rigid composite materials. Its limited length (35 cm) prevents any compression lesion around the elbow. Its large diameter ovoid section (13 cm ´ 11 cm) allows the inserting of hands of any size and insures total thumb mobility. Two of the extremities on this apparatus are cut off in order to permit the fingers and the fore-arm to be set, whereas an internal fixation insures the stability of the wrist. A groove located on the upper part of the tube allows for the adaptation of an elastic preload of the thumb, thereby improving the reproduction of the measures (). The symmetrical structure allows bilateral use. The tubular form prevents any thermal variation.
The whole set exhibits minimal encumbrances and is compatible with most surgical installations.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
TOF-Tube LETTER TO THE EDITOR
Dubois, Philippe E., MD; Broka, Serge
M., MD; Joucken, Kurt L., MDAnesth Analg 2000; 90:232

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Biblio da cercare Fawcett WJ, Dash A, Francis GA, Liban JB, Cashman JN. Recovery from neuromuscular
blockade: residual curarisation following atracurium or vecuronium by bolus dosing or infusions. Acta Anaesthesiol Scand 1995; 39:288-93.
Fruergaard K, Viby-Mogensen J, Berg H, El-Mahdy AM. Tactile evaluation of the response to double burst stimulation decreases, but not eliminates, the problem of postoperative residual paralysis. Acta Anaesthesiol Scand 1998; 42:1168-74
Beemer GH, Reeves JH, Bjorksten AR. Accurate monitoring of neuromuscuiar blockade using a peripheral nerve stimulator: a review. Anaesth Intensive Care 1990; 18A90‑496.
Hayes AH, Mirakhur RK, Breslin DS, at al. Postoperative residual block after intermediate‑acting neuromuscular blocking drugs. Anaesthesia 2001; 56:312‑318.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Different muscle groups resistanceDifferent muscle groups resistanceShows sequential relationshipsShows sequential relationships
DiaphragmDiaphragmmm.larinxmm.larinxadductorpollicis
adductorpollicis

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Saddler JM, Bevan JC, Donati F, Bevan DR, Pinto MB. Comparison of double-burst and train-of-four stimulation to assess neuromuscular blockade in
children. Anesthesiology 1990; 73:401-3
Double-burst stimulation (DBS), a new technique to evaluate neuromuscular function, consists of two 50-Hz trains of 60-ms duration and 750 ms apart. DBS was compared with train-of-four (TOF) stimulation in 21 children aged 3-10 yr, during halothane anesthesia. On one arm the ulnar nerve was stimulated supramaximally with TOF stimulation every 12 s and the force of the evoked contraction of the adductor pollicis measured with an FTO3 force transducer and recorded on paper. Atracurium (0.4-0.5 mg.kg-1) was administered. During recovery from neuromuscular blockade, TOF stimulation was interrupted periodically and DBS substituted. The same stimulation patterns were applied to the ulnar nerve of the other arm simultaneously, and the clinical anesthesiologist was asked to estimate the degree of fade with both. There was good correlation between the measured TOF ratio (ratio of fourth to first response) and DBS ratio (ratio of second to first response). The TOF and DBS ratios above which fade could no longer be appreciated manually were (mean +/- SEM) 0.44 +/- 0.03 and 0.67 +/- 0.04 (P = 0.0002). Corresponding ranges were 0.3-0.8 for TOF and 0.4-0.9 for DBS, but DBS fade was always apparent if TOF fade could be detected. Therefore, in children, DBS is more sensitive than is TOF stimulation for the clinical assessment of recovery from neuromuscular blockade.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Saddler et al Comparison of double-burst and train-of-four stimulation to assess neuromuscular
blockade in children. Anesthesiology 1990; 73:401-3
Children 3-10 years TPS/N2O/haloth atracurium 0.4-0.5 mg/kg MMG TOF vs DBS,MMG vs tactile.visual

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Saddler et al Comparison of double-burst and train-of-four stimulation to assess neuromuscular
blockade in children. Anesthesiology 1990; 73:401-3
TOF & DBS linearly related close to 1 anesthesioogist tended to overestimate
recovery with tof and DBS fade could no longer be detected at a
value of TOF 0.44+/-0.03 with DBS fade detected until tof 0,67+/-
0.04

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
17 O'Hara DA, Fragen RJ, Shanks CA. Comparison of visual and measured train‑of‑four recovery after vecuronium‑induced neuromuscular blockade using two anaesthetic techniques. Br J Anaesth 1986; 58:1300‑1302.
18 Kopman AF. Tactile evaluation of train‑of‑four count as an indicator of reliability of antagonism of vecuronium‑ or atracurium‑induced neuromuscular blockade. Anesthesiology 1991; 75:588‑593.
19 Lien CA, Belmont MR, Abalos A, at al. The nature of spontaneous recovery from mivacurium‑induced neuromuscular block. Anesth AnaIg 1999; 88:648653,
20 Eriksson U, Sundman E, Olsson R, at al. Functional assessment of the pharynx at rest and during swallowing in partially paralyzed humans, Simultaneous videomanometry and mechanomyography of awake human volunteers. Anesthesiology 1997; 87:1035‑1043.
21 Eriksson LI, Sato M, Severinghaus JW. Effect of a vecuronium‑induced partial neuromuscular block on hypoxic ventilatory response. Anesthesiology 1993; 78:693‑699.
22 Viby‑Mogensen J, Jorgensen BC, Ording H. Residual curarization in the recovery room. Anesthesiology 1979; 50:539‑541,

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
31 Eikermann M, Groeben H, Peters J. Prediction of the effects of partial neuromuscular blockade on pulmonary function by accelerography and mechanomyography of adductor pollicis muscle [Abstract]. Anesthesiology 2001; 95:A1021.



![Riduttori per Servomotori - RS & RT 28 - ATTI srl · - 12 - Riduttori per Servomotori - RS & RT Selezione RS RT i 2accT [Nm] T2ISO [Nm] T2max [Nm] n 1 [rpm] n1max [rpm] [arcmin]Ct](https://static.fdocumenti.com/doc/165x107/5f143d4e9680b36af56f47a5/riduttori-per-servomotori-rs-rt-28-atti-srl-12-riduttori-per-servomotori.jpg)