Andrea M.Isidori Dipartimento di Fisiopatologia Medica Dir. Prof. Andrea Lenzi.
53
Andrea M.Isidori Dipartimento di Fisiopatologia Medica Dir. Prof. Andrea Lenzi
-
Upload
ambra-di-bella -
Category
Documents
-
view
222 -
download
2
Transcript of Andrea M.Isidori Dipartimento di Fisiopatologia Medica Dir. Prof. Andrea Lenzi.

Andrea M.IsidoriDipartimento di Fisiopatologia Medica
Dir. Prof. Andrea Lenzi

Alterazioni funzionali degli organi interessati dal tumore primitivo
Alterazioni funzionali degli organi interessati dalla crescita metastatica
Effetti conseguenti all’azione di mediatori noti ed ignoti(fattori di crescita, citokine, ormoni)
prodotti dal tumore o derivanti dall’azione di autoAb prodotti dall’organismo contro le cellule tumorali
Sindromi paraneoplastiche
Effetti tossici Effetti metabolici
Effetti sistemici delle neoplasieEffetti sistemici delle neoplasie

Tumor Host InteractionsTumor Host Interactions
Local and Systemic Effects (primary site) Metastases (secondary site)( dedifferentation) Cancer Cachexia Paraneoplastic Syndromes
EndocrinopathiesNeuromyopathies Gastrointestinal motility syndromesOsteochondral DisordersVascular PhenomenaFeverDermatological Syndromes

Paraneoplastic syndromesParaneoplastic syndromes
Le Sindromi paraneoplastiche, per definizione, sono fenomeni legati all’interazione neoplasia-ospitefenomeni legati all’interazione neoplasia-ospite, ma NON direttamente riconducibili ad effetti metastatici, compressivi, tossici, infettivi o metabolici tumorali.
Sono importanti poiché: Si associano a severa morbilità e mortalità (es. Cushing’s) Sono spesso un “presenting symptom” di una neoplasia
misconosciuta (early diagnosis) e un riconoscimento precoce spesso ottimizza le possibilità di intervento
Rientrano nella diagnosi differenziale di sindromi comuni (ipercalcemia, iponatriemia, ipopotassiemia)
4

Paraneoplastic syndromesParaneoplastic syndromes
Le neoplasie più frequentemente associate a sindromi paraneoplastiche sono: Lung carcinoma (most common) Renal carcinoma Hepatocellular carcinoma Leukemias Lymphomas Breast tumors Ovarian tumors Neural cancers Gastric cancers Pancreatic cancers
5

Cancer CachexiaCancer Cachexia
Progressive weakness, loss of appetite, anemia and profound weight loss (>20 lbs.)
Often correlates with tumor size and extent of metastases
Etiology includes a generalized increase in metabolism and central effects of tumor on hypothalamus
Probably related to macrophage production of TNF-and IL-1

Endocrine syndromes
Cutaneous or dermatologic syndromes
Hematologic syndromes
Neurologic syndromes
Osteoarticular or rheumatologic syndromes
Ocular syndromes


I primi reports su sindromi endocrine in pazienti affetti da neoplasie maligne non endocrine risalgono agli anni ’20...
Lancet 1928
A case of pluriglandular syndrome: diabetes of bearded women.
Brown WH
Surg Gynecol Obster 1923
Parathyroid hyperplasia and bone destruction in generelized carcinomatosis.
Klemperer P


Paraneoplastic Endocrine
Syndromes
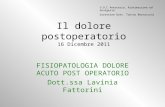
PTHrP, TGFs, ILs, Vit D, PTH
HYPERCALCEMIA
ONCOGENIC OSTEOMALACIA
ACROMEGALY
GYNECOMASTIA
HYPONATRIEMIA
CUSHING’s
HYPOGLYCEMIA
DIVERSE SYNTOMS
HCG
FGF23
GH, GHRH
IGF II
ACTH, CRH
Vasopressin, ANP
HPL, PRL, VIP, Renin, LH, GRP
Spectrum of paraneoplastic endocrine
HYPERGLYCEMIA
Glucagone, GH,

Endocrine Pathology 2003
Paraneoplastic Endocrine Syndromes: A Review
DeLellis RA, Xia L.
“…A number of criteria have been proposed for the diagnosis of paraneoplastic endocrine syndromes…
Demonstration of elevated hormone concentrations in the blood
Finding of normal or suppressed endogenous hormone production
Demonstration of hormone concentration gradients across the tumor
Biochemical or clinical resolution of the syndrome following surgery, radiotherapy or chemotherapy
Demonstration of hormone messenger RNA Demonstration of hormone messenger RNA and corresponding hormonal product in and corresponding hormonal product in tumoral cellstumoral cells

Endocrine Pathology 2003
Paraneoplastic Endocrine Syndromes: A Review
DeLellis RA, Xia L.
Meccanismi patogenetici
Theory of randon genetic derepression
Attivazione di geni normalmente inattivi per effetto di mutazioni o modificazioni epigenetiche
Dedifferentiation Theory
Regressione delle cellule tumorali ad uno stato maturativo precoce con produzione di proteine e
ormoni fetali ed embrionali (ex. PTHrP)

Hypercalcemia (Cancer is the most common cause of hypercalcemia by either humoral or metastatic mechanisms)Squamous cell lung cancer (PTH-like
peptide)Multiple myeloma and T-cell lymphoma (IL-1
and perhaps TGF-)Renal cell carcinoma (prostaglandins)Breast (& Prostate) carcinoma, usually by
bone metastasisParathyroid carcinoma (PTH)
Paraneoplastic Syndromes Endocrinopathies

Paraneoplastic Syndromes Endocrinopathies
Inappropriate ADH syndrome (Hyponatremia)Small cell undifferentiated lung cancer
(vassopressin-like hormone.Hypothalamic tumors (vasopressin)
Cushing’s SyndromeSmall cell undifferentiated lung cancer
(ACTH) released through cleavage of pro-opiomelano-cortin gene product.
MTC, Thymoma, Ovarian Cancer, Mesothelioma

Ipercalcemia 0,1% della popolazione generale fino a 3-5% >50aa
Fino al 58% dei pz adulti oncologici ospedalizzati 0,5-1,3% in età pediatrica <5% tumori maligni tratto genitale femminile
Mieloma, K squamoso del polmone (quasi nel 100% dei casi), K mammario, k renale, k del tratto genitale femminile, Linfoma HTLV,
Am J Med 1997
Hypercalcemia of Malignancy
Mundy G, Guise TA

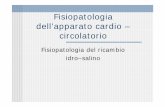
Primary hyperparathyroidism Primary hyperparathyroidism
23%23%
Paraneoplastic syndromeParaneoplastic syndrome
MetastasisMetastasis
72%72%(lung, breast cancer, multiple myeloma(lung, breast cancer, multiple myeloma))
Granulomatous desease (tuberculosis, sarcoidosis) Granulomatous desease (tuberculosis, sarcoidosis)
Genetic disorders (Familial hypocalciuric hypercalcemia) Genetic disorders (Familial hypocalciuric hypercalcemia)
Long immobilizationLong immobilization
Medications (lithium, thiazide diuretics, supplements) Medications (lithium, thiazide diuretics, supplements)
DehydrationDehydration
Hyperparathyroidism and cancer are Hyperparathyroidism and cancer are responsible responsible for more than 90%for more than 90% of sustained of sustained hypercalcemia. hypercalcemia.
Hypercalcemia

Ipercalcemia osteolitica localizzata (Localized Osteolytic Hypercalcemia -LOH-): da produzione locale di fattori paracrini, quali citochine (IL-6, TGFa e b, TNFa), prostaglandina E e metaboliti della Vitamina D, con effetto stimolatorio sugli osteoclasti
Ipercalcemia Maligna (Humoral Hypercalcemia of Malingnancy -HHM-):
da produzione di PTH-RP (PTH-related peptide) o più raramente di PTH
IpercalcemiaAssenza di metastasi ossee
PTH ridotto, PTHrP aumentato

Il PTHrP viene individuato nella seconda metà degli anni ’80, espresso in innumerevoli tessuti normali (es. endometrio, placenta, miometrio e decidua durante la gravidanza)
3 ISOFORME
La porzione NH2-terminale è simile a quella del PTH e determina simili effetti biologici, mentre il resto della molecola possiede altre funzioni (es. regolazione proliferazione cellulare/apoptosi)
Dosabile con metodo RIA (kit specifici per la porzione C-terminale), PCR, IRMA
New Engl J Med 1988
Humoral Hypercalcemia of cancer. Identification of a novel parathyroid hormone-like peptide
Broadus AE, Mangin M, Ikeda K, Insogna KL, Weir EC, Burtis WJ, Stewart AF
Cancer 1991
Immunohistochemical evaluation of PTHrP in human lung cancer and normal tissue with newly developed monoclonal antibody
Kitazawa S et al
New Engl J Med 2000
The physiology of parathyroid hormone related protein
Strewler GJ

It has become recently appreciated that the hypercalcemia of malignancy is commonly caused by the increased production of parathyroid hormone-related protein (PTHrP) by the cancer. In fact, the demonstration of increased PTHrP production in a patient with hypercalcemia is regarded as pathognomonic of malignancy. The authors describe a patient with a benign ovarian lesion that produced PTHrP and caused hypercalcemia. They identify other reports of hypercalcemia associated with hypercalcemia and benign tumors, and refer to this syndrome as the humoral hypercalcemia of benignancy. Although apparently rare, a benign PTHrP-producing tumor should be considered in the differential diagnosis of hypercalcemia.
Am J Clin Pathol 1996
The Humoral hypercalcemia of benignancy. A newly appreciated syndrome - Knecht TP et al
PTHrP nelle lesioni tumorali BENIGNE…

• Nel 10-20% dei pz oncologici si presenta come emergenza metabolica• Emergenza per Ca >14 mg/dl (3.5 mmol/L)• Gravità dei sintomi correlata alla velocità di aumento del calcio ionizzato e alla sua concentrazione, alle condizioni generali del e malattie concomitanti
IPERCALCEMIA NEOPLASTICA IPERCALCEMIA NEOPLASTICA
LIVELLI CORRETTI DI CALCIO SIERICOCalcio misurato + [ 0.8 x (4.0 – albumina sierica) ]
TrattamentoTrattamentoIdratazione: NaCl ev 0,25-1 L/h (controllare PVC)Diuretici dell’ansa (furosemide): 20-40 mg ev ogni 2-4h (controllo elettroliti)Bisfosfonati evCalcitonina sc/ev 4-8 U/kg ogni 6-12hCorticosteroidi (cortone acetato-prednisone)Emodialisi

La Seconda più frequente S. ParaneoplasticaLa Seconda più frequente S. Paraneoplastica
Microcitoma polmonare (60%), NET, k tratto urogenitaleMicrocitoma polmonare (60%), NET, k tratto urogenitale
Iposodiemia (<130 mmol/L) / Sodiuria >20 mEq/LIposodiemia (<130 mmol/L) / Sodiuria >20 mEq/LOsmo urin > 100 mOsm/L / Osm plasma < 260 mOsm/LOsmo urin > 100 mOsm/L / Osm plasma < 260 mOsm/L
J Intern Med 1995
Syndrome of Inappropriate secretion of antidiuretic hormone (SIADH) in malignant diseases
Sorensen JB, Anderson MD, Hansen HH
Ann NY Acad Sci 1992
Oxytocin and vasopressin: from genes to peptide
Gainer H, Wray S
Paraneoplastic SIADH

Hypovolaemic
GI losses DiureticsMucosal lossesPancreatitis Sodium depletion post diuretics
Urinary Na<20 mmol/l Urinary Na>40 mmol/l
DiureticsAddison’s diseaseCerebral salt wastingSalt wasting nephropathy
Euvolaemic
HypothyroidismSIADH with ongoing fluid restrictionPrimary polydipsiaInappropriate fluid replacement
SIADH
ACTH deficiency
HypervolaemicCirrhosisCardiac failureNephrotic syndrome
Cardiac failure or cirrhosison diuretic therapy
30-40%
Causes of hyponatraemia

DesmopressinSelective serotonin reuptakeinhibitorsCarbamazepineProstaglandinsTricyclic antidepressantsPhenothiazinesHaloperidol3,4-MethylenedioxymethamphetamineQuinolonesLeveteiracetamCyclophosphamideVincristine
Malignancy
Drugs
Small cell lung cancer 75% dei casiNasopharyngeal cancerMesotheliomaGI tract malignancyPancreatic malignancyGU tract malignancyLymphomaSarcoma
Pneumonia, especially LegionellaMycoplasmaTuberculosisAbscessVasculitisPositive pressure ventilation
Pulmonary
TumourMeningitisEncephalitisAbscessVasculitisSubarachnoid haemorrhageSubdural haemorrhageTraumatic brain injury
Intracranial pathology

Between 1964 and 2002:
413 patients with CS were investigated
60 had an adrenal adenoma,
30 had an adrenal carcinoma,
5 had macronodular adrenal hyperplasia,
274 of pituitary origin (CD)
44 from an ectopic source of ACTH

A COMPARISION BETWEEN THE A COMPARISION BETWEEN THE TWO LARGEST SERIES TWO LARGEST SERIES
ON ECTOPIC ACTH SYNDROMEON ECTOPIC ACTH SYNDROME
EUROPEEUROPE (UK)(UK) vs. vs. USA USA (NIH)(NIH)
(n=40)(n=40) (n=90) (n=90)
MedianMedian follow-up follow-up 60m 60m 26m 26m
Are there regional differences in the ectopic ACTH syndrome in different parts of the developed world
in tertiary referral centres?

ECTOPIC ACTH SYNDROME
4 patients had markedly fluctuant levels of ACTH – cyclical Cushing’s syndrome1 pancreatic carcinoid1 thymic carcinoid1 bronchial carcinoid1 occult source

LUNG 47.5% (major organ)
- CARCINOID 30%- SCLC 17.5%
Intrathoracic in general 55%
OCCULT 12.5%
LUNG 42.2% (major organ)
- CARCINOID 38%- SCLC 3%- Tumorlets 0.9%
Intrathoracic in general 52%
OCCULT 19%
St. Bartholomew’s NIH

ECTOPIC ACTH ECTOPIC ACTH SYNDROMESYNDROME 40 patients
26 revealed on imaging (overt)14 not apparent
○ 9 became apparent (covert)○ 5 remained hidden (occult)
Barts experience: 1969-2001 (Isidori et al., 2005)

COVERTCOVERT ECTOPIC ACTH SYNDROME
Of 9 tumours not initially identified:
Revealed by CT 4Revealed by whole-body catheter *
2Found at surgery/autopsy 3
USING MODERN CROSS-SECTIONAL IMAGINGVIRTUALLY ALL ECTOPICS WHICH CAN BE
FOUND WILL BE FOUND
(Isidori et al., 2005)*before high-quality CT

Mean ACTH levels:Overt 207 ng/lCovert 125 ng/l
Mean Cortisol levelsOvert 1422 nmol/lCovert 1065
nmol/l
Mean K+ levelsOvert 2.7 mmol/lCovert 2.8
mmol/l
Hypokalaemia in 70%
Mean ACTH levels:Overt 205 ng/lCovert 109 ng/l
Mean UFCOvert 8810
nmol/24hCovert 12170
nmol/24h
Mean K+ levelsOvert 3.4 mmol/lCovert 3.5 mmol/l
Hypokalaemia in 74%
St. Bartholomew’s NIH

ECTOPIC ACTH SYNDROMEDynamic Stimulation Tests
High-dose dexamethasone suppression○ 91% show absent suppression (>50%)
CRH stimulation test○ 94% show absent rise (>20%)
One patient showed a response to both tests (1/40=2%)

ECTOPIC ACTH SYNDROME:NIH experience
High-dose dexamethasone suppression○ 86% show absent suppression (UFC)
CRH stimulation test○ 92% show absent rise (>20%)
Dynamic Stimulation Tests

ECTOPIC ACTH SYNDROME
BILATERAL INFERIOR PETROSAL SINUS SAMPLING
1/12 patients showed a central gradient >3 (mesothelioma)At NIH, 1/67 patients showed a central gradient (esthesioneuroblastoma)
Therefore, false positive responses in 2/79 (~2%)

ECTOPIC ACTH SYNDROMETUMOUR MARKERS
28% show raised gastrin28% show raised calcitonin10% show raised urinary 5-HIAA
At NIH31% show raised calcitonin30% show raised 5-HIAA

ECTOPIC ACTH SYNDROMEWHOLE BODY VENOUS CATHETER STUDIES
4/22 WERE POSITIVE○ 2 thymic carcinoids○ 1 mediastinal lymph node○ 1 medullary thyroid carcinoma
BUT THESE WERE ALL STUDIED BEFORE HIGH-RESOLUTION CT SCANNING

IMAGING
CT LOCALISED TUMOUR IN 82% (NIH=92%)
111In-octreotide localised tumor in 2/8 (25%)At NIH, 21/43 (49%) were positiveBUT IT VERY RARELY IDENTIFIES TUMOURS
NOT OTHERWISE SEEN!
ECTOPIC ACTH SYNDROME

TREATMENT
28/40 treated with steroidogenesis inhibitors for median 9 months
MetyraponeKetoconazoleMitotane
One patient needed intravenous etomidate
ECTOPIC ACTH SYNDROME

TREATMENT
12 patients had primary resection, 10 curative
12 patients had bilateral adrenalectomy14 patients received radiotherapy11 patients received chemotherapy2 patients received 131I-MIBG therapy
CONCLUSION – Control cortisol excess, remove tumour where possible, consider removing adrenals where not
ECTOPIC ACTH SYNDROME

Kaplan-Meier survival curve for ectopic ACTH patients
0.0
00
.25
0.5
00
.75
1.0
0
0 100
200
300Survival
(months)
Small cell NET mets
NET
(Isidori et al., 2005)

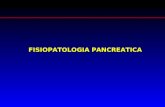
Prevalence of Tumours responsible of EAS
Percentage(%)
0
10
20
30
40
50
60
Lung
/Med
iast
. Car
cino
ids
Lung
SC
LC /
Ade
nok
Thym
ic tu
mou
rs
Med
ulla
ry T
hyro
id K
Isle
t Cel
l Tum
ours
Pheo
chro
moc
ytom
asG
I car
cino
ids
GI a
deno
carc
inom
as
Dis
sem
inat
ed N
ETLo
caliz
ed N
ET
Mis
cella
neou
s Tu
mou
rs
Nev
er-fo
und
Thoracic Tumours
Abdominal Tumours
Total n=383


WDHA syndrome (watery diarrhea, hypokalemia, and achlorhydria) - caused by tumor production of vasoactive intestinal polypeptide (VIP).Islet cell tumors, Intestinal carcinoid
tumors Polycythemia - caused by tumor
production of erythropoietinsRenal cell carcinoma, Cerebellar
hemangioma, Hepatocarcinoma
Paraneoplastic Syndromes Endocrinopathies


Paraneoplastic GI dismotility syndromes
A small proportion of patients with occult or established neoplasms develop a gastrointestinal motility disorder, referred to as paraneoplastic dysmotility.
The diagnosis of a paraneoplastic dysmotility requires the onset of gastrointestinal dysmotility associated with the presence of a tumor and presence of specific serum antibodies
45
Kashyap P and Farrugia G, Gastroenterol Clin North Am. 2008

Clinical presentation of a para-neoplastic dysmotility syndrome
Pseudoachalasia Gastroparesis Paraneoplastic chronic
intestinal pseudoobstruction (CIPO)
Chronic constipation
46
Kashyap P and Farrugia G, Gastroenterol Clin North Am. 2008

47Autoimmunity Reviews 6 (2007) 162–168
autonomic paraneoplastic neurological Hu-related
syndromes

Treatment of paraneoplastic Treatment of paraneoplastic dysmotility dysmotility No treatments have been convincingly shown
to alter outcome (steroids, cyclophosphamide, plasmapheresis, immunoglobulin)
Treatment of the underlying primary malignancy
Nutritional support either enterally or parenterally
Prokinetics, treatment of bacterial overgrowth One additional management strategy is to use
high dose IV steroids for 3 days and if there is a clinical response switch to 6-mercatopurine or azathioprine (difficult in the case of chemotherapy)
48
Kashyap P and Farrugia G, Gastroenterol Clin North Am. 2008


Da autoanticorpi contro la desmoplakina I, proteina dei desmosomi delle cellule epiteliali. Le lesioni bollose pemfigoidi sono conseguenza della perdita della normali adesioni intercellulari a livello dell’epidermide.
Pemfigo
Iperpigmentazione vellutata, di colore marrone scuro o nero, a livello di ascelle, aree sottomammarie e pieghe inguinaliSoprattutto K gastrico.
Acanthosis nigricans
Placca eritematosa, simile ad un eczemaQuando localizzata a livello delle areole mammarie è quasi sempre associata a K duttale della mammella, mentre la malattia di Paget extramammaria si associa in circa il 50% dei casi a neoplasie genitali.
Malattia di Paget
Linfomi, timoma, sarcomi ed altre neoplasie, soprattutto ematologiche

Miopatia infiammatoria associata ad un rash cutaneo violaceo, più evidente nelle aree esposte al sole, edema ed eritema periorbitale, placche eritematose a livello delle articolazioni metacarpofalangee e interfalangee prossimali (papule di Gottron)K polmone, stomaco, utero, ovaio
Dermatomiosite
IttiosiAssociata ai linfomi di HodgkinPlacche cutanee a scaglie
Comparsa improvvisa o aumento in numero e dimensioni di cheratosi seborroicaNeoplasie gastrointestinali
Snd di Leser-Trèlat
Snd di SweetDermatosi neutrofila febbrile acuta (febbre, leucocitosi neutrofila, placche o noduli eritematosi a livello di testa, collo e arti superioriIn particolare in corso di leucemia acuta mieloblastica, sindromi mielodisplastiche e malattie mieloproliferative.

Paraneoplastic Syndromes
Think about it…