w .g en r aom it Introduzioneccgm.it/wp-content/uploads/approccio-farmacologico-ubaldi.pdf · 1...
16
1 Diverso approccio farmacologico alla induzione della ovulazione e superovulazione in donne con alterazioni endocrino-metaboliche Filippo Maria Ubaldi M.D. M.Sc. CLINICA VALLE GIULIA, Rome I Master di Medicina della Riproduzione Umana Padova, 2009-2010 www.generaroma.it Introduzione www.generaroma.it L’induzione dell’ovulazione o superovulazione in donne con anovulatorieta’ e alterazioni del ciclo spesso corre- correlate a problematiche endocrino-metaboliche pre- prevede l’utilizzo di farmaci con diverse modalita’ di somministrazione Le pazienti che possono usufruire di questo tipo di trat- tamento rientrano principalmente in due categorie: Introduzione www.generaroma.it 1) Amenorree ipogonadotrope (ipogonadismo ipogonadotropo o amenorrea ipotalamica) amenorrea di tipo I (WHO) 2) Sindrome dell’Ovaio Policistico (amenorrea iperandrogenica) amenorrea di tipo II (WHO) 3) Amenorrea ipergonadotropa (ipogonadismo ipergonadotropo amenorrea di tipo III (WHO) www.generaroma.it Fattori ambientali SNC Ipotalamo Ipofisi Ovaio Utero Mestruazioni Progesterone Estrogeni FSH LH GnRH IV compartimento III comp. II comp. I comp.
-
Upload
trannguyet -
Category
Documents
-
view
216 -
download
0
Transcript of w .g en r aom it Introduzioneccgm.it/wp-content/uploads/approccio-farmacologico-ubaldi.pdf · 1...

1
Diverso approccio farmacologico alla induzione della ovulazione e
superovulazione in donne con alterazioni endocrino-metaboliche
Filippo Maria UbaldiM.D. M.Sc.
CLINICA VALLE GIULIA, Rome
I Master di Medicina della Riproduzione Umana
Padova, 2009-2010
www.generaroma.it
Introduzione
www.generaroma.it
L’induzione dell’ovulazione o superovulazione in donne
con anovulatorieta’ e alterazioni del ciclo spesso corre-
correlate a problematiche endocrino-metaboliche pre-
prevede l’utilizzo di farmaci con diverse modalita’ di
somministrazione
Le pazienti che possono usufruire di questo tipo di trat-
tamento rientrano principalmente in due categorie:
Introduzione
www.generaroma.it
1) Amenorree ipogonadotrope (ipogonadismo
ipogonadotropo o amenorrea ipotalamica)
amenorrea di tipo I (WHO)
2) Sindrome dell’Ovaio Policistico (amenorrea
iperandrogenica) amenorrea di tipo II
(WHO)
3) Amenorrea ipergonadotropa (ipogonadismo
ipergonadotropo amenorrea di tipo III
(WHO)
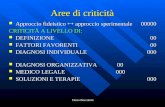
www.generaroma.it
Fattori ambientali SNC
Ipotalamo
Ipofisi
Ovaio
Utero Mestruazioni
ProgesteroneEstrogeni
FSH LH
GnRH
IV compartimento
III comp.
II comp.
I comp.
2
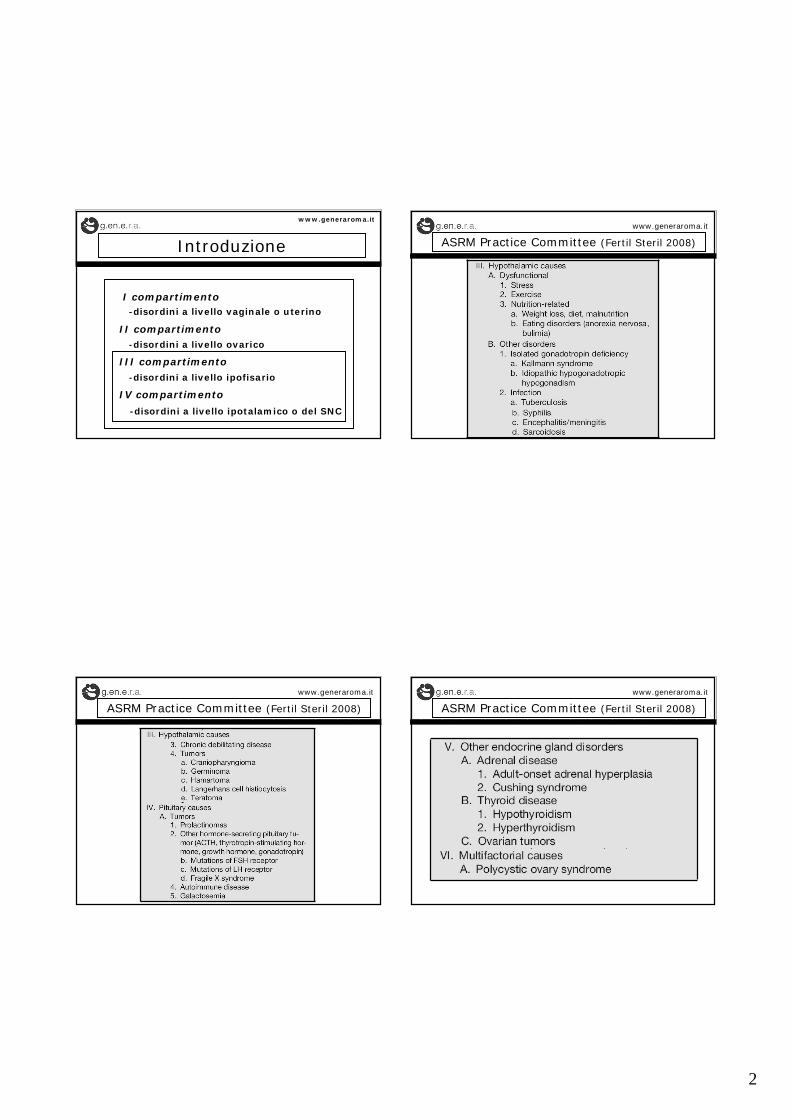
Introduzione
www.generaroma.it
I compartimento-disordini a livello vaginale o uterino
II compartimento-disordini a livello ovarico
III compartimento-disordini a livello ipofisario
IV compartimento
-disordini a livello ipotalamico o del SNC
ASRM Practice Committee (Fertil Steril 2008)
www.generaroma.it
ASRM Practice Committee (Fertil Steril 2008)
www.generaroma.it
ASRM Practice Committee (Fertil Steril 2008)
www.generaroma.it

3
Amenorrea ipotalamicawww.generaroma.it
GnRH pulsatile
Gonadotropine
Clomifene Citrato
Terapie
Amenorrea ipotalamica: GnRH pulsatilewww.generaroma.it
Miller ‘83
Mason ‘84
Hurley ‘84
Santoro ‘86
Filicori ‘ 8720-30 % grav/ciclo60-90 % grav/paziente
Letteratura:GnRH pulsatile
utilizzato in varie
condizioni di ano-
vulatorieta’
Amenorrea ipotalamica: GnRH pulsatilewww.generaroma.it
Amenorrea ipotalamica: GnRH pulsatilewww.generaroma.it
SottocuteEndovena
Via di somministrazione
Dosaggi: 2.5 - 20 mg/pulseIntervallo pulse: 60’ - 90’ - 120’

4
Amenorrea ipotalamica: GnRH pulsatilewww.generaroma.it
Effetti collaterali
Drop-out
Cefalea, nausea
Orticaria, broncospasmo, ipotensione
Tromboflebite (somministrazione e.v.)
Ematomi (somministrazione s.c.)
Endocardite (somministrazione e.v.)
Scarsa compliance
Hypogonadotropic hypogonadismwww.generaroma.it
Conclusions: In isolated hypogonadotropic hypogonadism
patients it is consistent with the two-cell two-gonadotro-
pin hypothesis, that both gonadotropins are required to
accomodate their synergistic action for appropriate stero-
idogenesis. The superior efficacy of hMG compared with
FSH-HP is beyond question
Results of ovulation induction using hMG or FSH-HP in hypogonadotropic hypogonadism patients
Shoham Z et al., Fertility Sterility 56(6):1048, 1991
FSH-HP: amps (<0,04); leading follicle (<0,05)serum E2 (<0,002); endometrial thic-
kness (<0,02); ovulation rate (<0,05)
Hypogonadotropic hypogonadismwww.generaroma.it
Extensive clinical testing in patient suffering from se-
vere deficiency in LH and FSH has demonstrated that
serum LH levels >0,5 IU/L are necessary to provide
adequate LH support to FSH-induced follicular deve-
lopment when endogenous LH secretion is absent.
O’Dea, 2002
Sufficient LH supply can be delivered by
a daily injection of 75 IU r-LH
Hypogonadotropic hypogonadismwww.generaroma.it
A daily dose of 75 IU rec-LH in addition to rec-FSH
is effective in the majority of women in promoting
optimal follicular development and steroidogenesis
in WHO I women and safe in all of them. Good preg-
nancy rate can be achieved.
The European Recombinant Human LH Study Group. J.Clin.Endocrinol. Metab. 1998
The Spanish Collaborative Group on Female Hypogonado-trophic Hypogonadism. Hum. Reprod. 2001
5
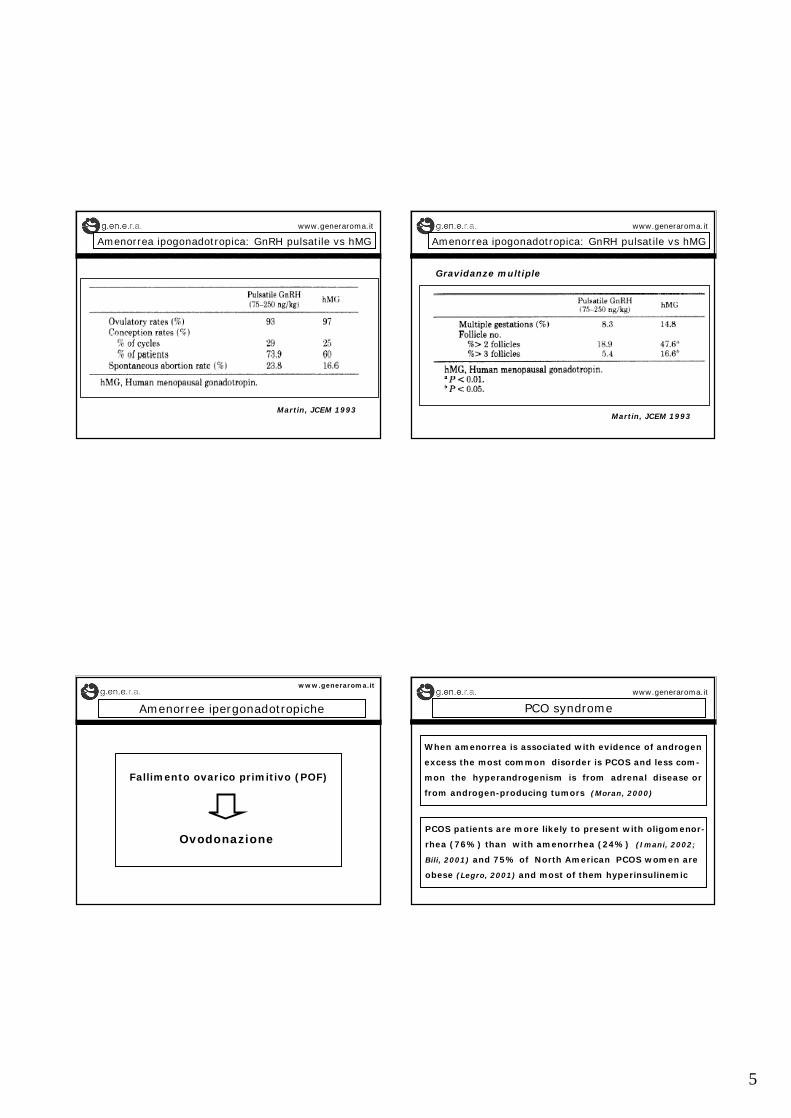
Amenorrea ipogonadotropica: GnRH pulsatile vs hMG
www.generaroma.it
Martin, JCEM 1993
Amenorrea ipogonadotropica: GnRH pulsatile vs hMG
www.generaroma.it
Martin, JCEM 1993
Gravidanze multiple
Amenorree ipergonadotropiche
www.generaroma.it
Fallimento ovarico primitivo (POF)
Ovodonazione
PCO syndromewww.generaroma.it
When amenorrea is associated with evidence of androgen
excess the most common disorder is PCOS and less com-
mon the hyperandrogenism is from adrenal disease or
from androgen-producing tumors (Moran, 2000)
PCOS patients are more likely to present with oligomenor-
rhea (76%) than with amenorrhea (24%) (Imani, 2002;
Bili, 2001) and 75% of North American PCOS women are
obese (Legro, 2001) and most of them hyperinsulinemic

6
PCOSwww.generaroma.it
PCOS is one of the most common endocrinopathies af-
fecting 5-10% of women of reproductive age with a lot
of controversies regarding both its diagnosis and treat-
ment (ESHRE/ASRM-Sponsored PCOS Consensus Whorkshop 2008)
Revised 2003 diagnostic criteria of PCOS
1) Oligo- and/or anovulation
2) Clinical or biochemical signs of hyperandrogenism
3) Policistic ovaries(2 out of 3 criteria)
PCO/PCOS classificationwww.generaroma.it
(The Rotterdam ESHRE/ASRM-sponsored PCOS consensus)
Diagnostic criteria of polycistic ovaries (PCO)
1) Presence of >12 follicles (2-9 mm in diameter)
2) and/or increased ovarian volume (>10 ml)
A woman having PCO in the absence of an ovulatorydisorder or hyperandrogenism (“asymptomatic” PCO)should not be considered as having PCOS
“Asymptomatic” PCO ovaries if stimulated for IVFbehave like the ovaries of PCOS women at increased
risk for hyperstimulation and OHSS (McDougall 1992)
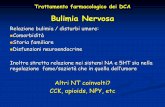
PCO syndromewww.generaroma.it
Hyperinsulinemia due to insuline resistance occurs in 80%
of women with PCOS and central obesity but also in 40%
of lean women with PCOS (Dunaif, 1997) due to a post-re-
ceptor defect affecting glucose transport, unique to PCOS
PCOS
HYPERINSULINEMIA
Central obesity
+
Ovarianandrogenproduction
SHBG
Free testosterone
5 alphareductase
ANOVULATION
FSH forovulationinduction
Multifollicularresponse
pregnancymiscarriage
Hirsutism/Acne
PCOS: suggested treatmentwww.generaroma.it
Various interventions have been proposed:
o Lifestyle modification (diet, exercise)
o Insulin-sensitizing agents
o Laparoscopic ovarian drilling
o Clomiphene Citrate (and aromatase inhibitors)
o Gonadotropins with or without GnRH analogues
Ovulation induction
Controlled ovarian hyperstimulation for IUI or IVF

7
PCOS obese: lifestyle modificationwww.generaroma.it
PERDITA DI PESO
La diminuzione del 5-10% del peso corporeo la severita’
dell’irsutismo e dell’acne, ripristina la regolarita’ del ciclo
e l’ovulazione nel 60-70% delle pazienti soprattutto con
WRH (obesita visceale) (Pasquali 1989) e protegge per il
diabete tipo 2, migliorando la dislipidemia.
MECCANISMI: riduzione insulina, riduzione androgeni
DA SEGNALARE: miglioramento della efficacia di tutte le
terapie farmacologiche per la induzione ovulazione
PCOS obese: lifestyle modificationwww.generaroma.it
PREGNANCY (%)
0,067WOMEN WITH LIVE BIRTH (%)
0,077,6WOMEN PREGNANT (%)
0,018MISCARRIAGES (%)
0,053TREATMENT
0,027SPONTANEOUS
0,0 %90 %RESUMED OVULATION
- 0,4 ± 1,4 a- 3,7 ± 1,6CHANGE IN BMI (Kg/m2)
“DROP-OUT”(N = 20)
COMPLETED(N = 67)
Clark, 1998a = P<0.01
Perdita di peso e outcome clinico
PCOS obese: lifestyle modificationwww.generaroma.it
Effetti Parametri
Ridotta
Migliorata
Ridotta
Migliorata
Uguale / aumentato
Uguale / ridotto
grasso totale e viscerale
Hirsutism scoreCicli mestruali (n°)Ovulation and pregnancy rateAcanthosis nigricans
TestosteroneAndrostenedioneInsulina
Insulino sensibilità
SHBG
LH
Perdita di peso e modifiche sull’assetto ormonale, sul metabolismo e caratteristiche cliniche in PCOS obese
PCOS obese: ipoglicemizzanti oraliwww.generaroma.it
FARMACI IPOGLICEMIZZANTI (Metformina)
MECCANISMI: riduzione della concentrazione plasma-
tica di insulina e androgeni; ripristino dell’ovulazione
METFORMINA: da 500mg x 3 a 850mg x 3/die
EFFETTI COLLATERALI: diarrea, disturbi neurovegetativi
La metformina non induce ipoglicemia nelle pazienti
normoglicemiche

8
PCOS obese: metforminawww.generaroma.it
E’ stato dimostrato che questo farmaco, da solo
o in combinazione con farmaci induttori della
ovulazione, è utile per il ripristino dell’ovula-
zione e per l’ottenimento di una gravidanza in
pazienti affette da PCOS
Nestler et al., New Engl J Med. 1998; Fertil Steril 2002
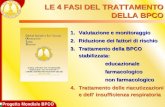
Change in frequency of menstruation (cycle/month)
www.generaroma.it
1.25
1.00
0.75
0.50
0.25
0.00
-0.25
-0.50
Metformina Placebo
Moghetti, J Clin Endo Metab 2000
Metformina e fertilita’ in PCOSwww.generaroma.it
Migliori risultati ovulatori su cicli spontanei o indotti da clomifene citrato (Nestler, 1998-2002; Moghetti, 2000; Ibanez, 2001; Vandermolen, 2001; Kelly, 2002; Kocak, 2002; Fleming, 2002; Yarali, 2002)
Incremento della fecondazione ovocitaria con ICSI(Stadtmauer et al 2001)
Ridotto rischio di OHSS in seguito a trattamenti farma-cologici di induzione dell’ovulazione (De Leo et al 1999)
Aumento della pregnancy rates dopo cicli di induzione dell’ovulazione (Stadtmauer et al 2001, Vandermolen, 2001; Batukan et al 2002, Kocak et al 2002, Heard et al 2002)
PCOS: ovulation inductionwww.generaroma.it
CC is the treatment of first choice in anovulatory women-low cost
-oral route is patient friendly
-few adverse effects
-little ovarian response monitoring
-aboundant data regarding the safety of the drug
Efficacy
70-85% of patients with PCOS will ovulate after CC(Homburg 2005; Messinis 2005)
Life-table analysis indicates a conception rate of up to22% per cycle in those ovulating on CC (Hammond 1983;Kousta 1997; Heijkemans 2003; Messinis 2005)
9
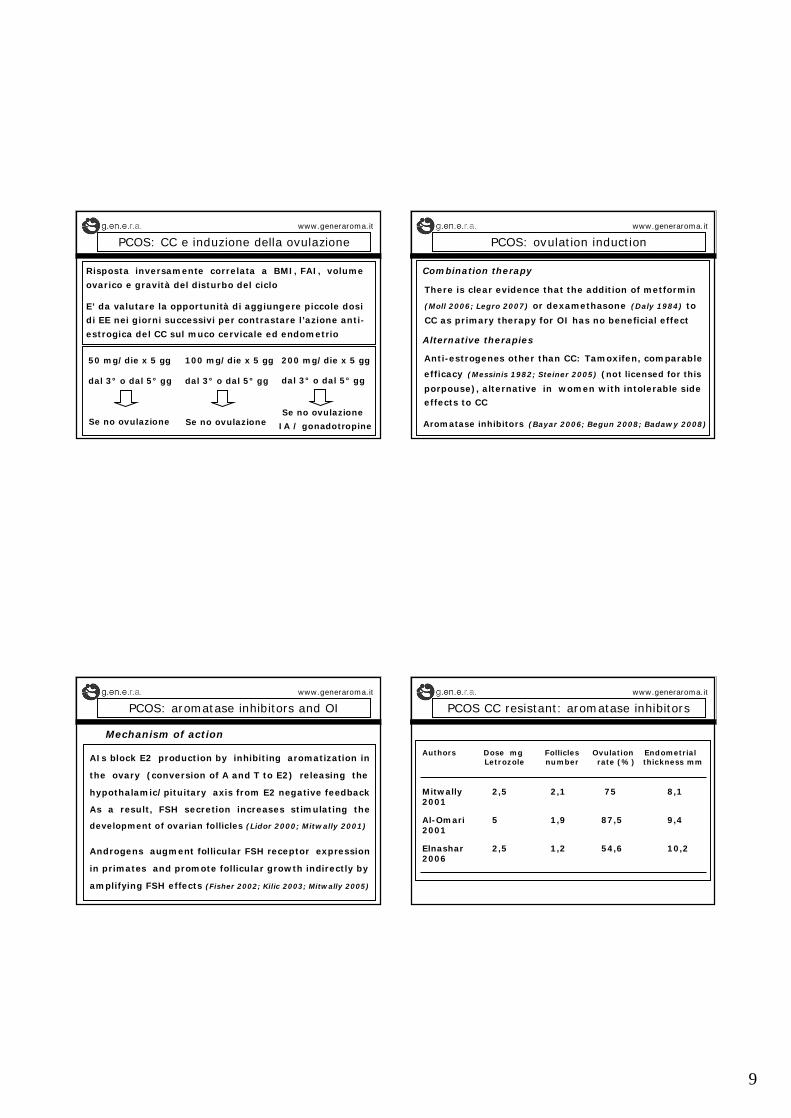
PCOS: CC e induzione della ovulazionewww.generaroma.it
Risposta inversamente correlata a BMI, FAI, volume
ovarico e gravità del disturbo del ciclo
E’ da valutare la opportunità di aggiungere piccole dosi
di EE nei giorni successivi per contrastare l’azione anti-
estrogica del CC sul muco cervicale ed endometrio
50 mg/die x 5 gg
dal 3° o dal 5° gg
Se no ovulazione
100 mg/die x 5 gg
dal 3° o dal 5° gg
Se no ovulazione
200 mg/die x 5 gg
dal 3° o dal 5° gg
Se no ovulazione
IA / gonadotropine
PCOS: ovulation inductionwww.generaroma.it
Combination therapy
There is clear evidence that the addition of metformin
(Moll 2006; Legro 2007) or dexamethasone (Daly 1984) to
CC as primary therapy for OI has no beneficial effect
Anti-estrogenes other than CC: Tamoxifen, comparable
efficacy (Messinis 1982; Steiner 2005) (not licensed for this
porpouse), alternative in women with intolerable side
effects to CC
Alternative therapies
Aromatase inhibitors (Bayar 2006; Begun 2008; Badawy 2008)
PCOS: aromatase inhibitors and OIwww.generaroma.it
AIs block E2 production by inhibiting aromatization in
the ovary (conversion of A and T to E2) releasing the
hypothalamic/pituitary axis from E2 negative feedback
As a result, FSH secretion increases stimulating the
development of ovarian follicles (Lidor 2000; Mitwally 2001)
Androgens augment follicular FSH receptor expression
in primates and promote follicular growth indirectly by
amplifying FSH effects (Fisher 2002; Kilic 2003; Mitwally 2005)
Mechanism of action
PCOS CC resistant: aromatase inhibitorswww.generaroma.it
Authors Dose mg Follicles Ovulation EndometrialLetrozole number rate (%) thickness mm
Mitwally 2,5 2,1 75 8,12001
Al-Omari 5 1,9 87,5 9,42001
Elnashar 2,5 1,2 54,6 10,22006

10
AI vs CC in PCOS (RCTs): clinical resultswww.generaroma.it
Authors Dose mg Pregnancy (%) PLet CC Let CC
Atay 2,5 100 21% 9% ns2006
Bayar 2,5 100 22% 17% ns2006
Sohrabvand 2,5 100 33% 16% ns2006
Begun 7,5 150 40% 18% <0,052008
Total 43/152 (28%) 23/157 (14%) 0,005
Aromatase Inhibitors: safety considerationswww.generaroma.it
ASRM 2005: Higher risks of congenital cardiac and bone
malformations in the newborns (Biljan, Fertil Steril, 2005)
Babies born after CC or AI treatments in Canada: 2001-2005
Treatment Letrozole Letrozole+FSH CC CC+FSH
No. of newborns 252 262 293 104
Birth weight (gr.) 3287,3 3248,4 3158,8 3322,5
Age of mother 33,1 32,4 32,9 33,9
Major malformation 6/514 (1,2%) P=0,07 12/397 (3%)
Minor malformation 9/514 (1,6%) P=0,8 7/397 (1,8%)
Tulandi, 2006
Ovulation induction with gonadotropinswww.generaroma.it
13-44% of PCOS will not ovulate with CC or AI
(Guzick, 1998; Kovacs, 2001; Slowey 2001; Mitwally 2001; Al-Omari 2001Homburg 2005; Messinis 2005; Elnashar 2006; Atay 2006; Begun 2008)
Gonadotropins
1) Type of gonadotropins
2) Stimulation protocols
Ovulation induction: type of gonadotropinswww.generaroma.it
In PCOS with high LH, u-FSH or rec-FSH have theore-
thical advantages over HMG, but whether this claimed
advantage extends into clinical practice is uncertain
Issue 2, 2008

11
FSH vs HMG: ovulation rate www.generaroma.it
FSH vs HMG: pregnancy rate www.generaroma.it
FSH vs HMG: multiple pregnancy rate www.generaroma.it
FSH vs HMG: miscarriage rate www.generaroma.it
12
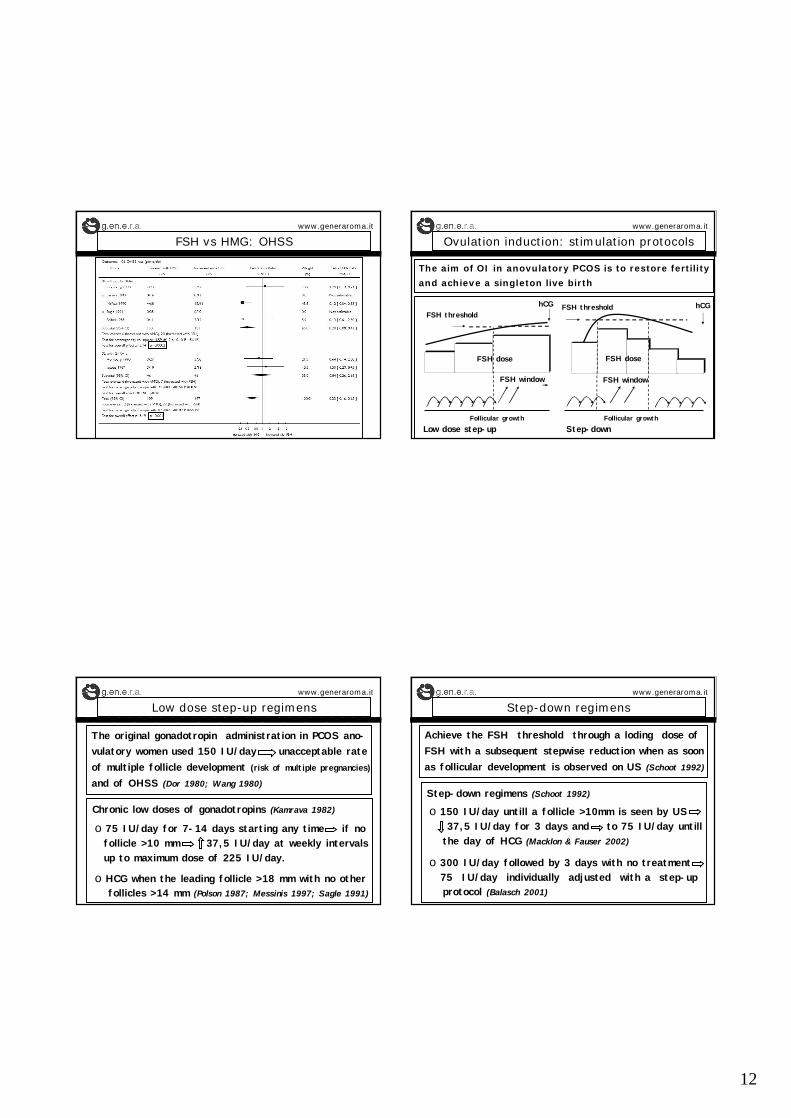
FSH vs HMG: OHSS www.generaroma.it
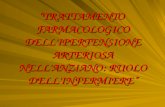
Ovulation induction: stimulation protocolswww.generaroma.it
The aim of OI in anovulatory PCOS is to restore fertility
and achieve a singleton live birth
FSH threshold hCG
FSH window
Follicular growth
FSH dose
FSH thresholdhCG
FSH window
FSH dose
Follicular growthLow dose step-up Step-down
Low dose step-up regimenswww.generaroma.it
The original gonadotropin administration in PCOS ano-vulatory women used 150 IU/day unacceptable rateof multiple follicle development (risk of multiple pregnancies)
and of OHSS (Dor 1980; Wang 1980)
Chronic low doses of gonadotropins (Kamrava 1982)
o HCG when the leading follicle >18 mm with no otherfollicles >14 mm (Polson 1987; Messinis 1997; Sagle 1991)
o 75 IU/day for 7-14 days starting any time if nofollicle >10 mm 37,5 IU/day at weekly intervalsup to maximum dose of 225 IU/day.
Step-down regimenswww.generaroma.it
Achieve the FSH threshold through a loding dose of FSH with a subsequent stepwise reduction when as soonas follicular development is observed on US (Schoot 1992)
Step-down regimens (Schoot 1992)
o 150 IU/day untill a follicle >10mm is seen by US37,5 IU/day for 3 days and to 75 IU/day untill
the day of HCG (Macklon & Fauser 2002)
o 300 IU/day followed by 3 days with no treatment75 IU/day individually adjusted with a step-upprotocol (Balasch 2001)

13
Step-down regimenswww.generaroma.it
To optimize treatment with the stepdown regimen:
o First cycle with a dose finding low-dose step-upprotocol to determine the FSH threshold (Imani 2002)
o Starting daily dose is the effective response dose ofthe first cycle increased by 37,5 IU. Comparing thefirst step-up and the second step down cycle no dif-ferences in terms of monofollicular development andpregnancy rates (van Santbrink & Fauser 2003)
Combination with GnRH analogueswww.generaroma.it
LH serum levels may interfere with fertility (?):
- premature oocyte maturation (Jacobs 1990)
- deleterius effect on granulosa cell steroidogenesis(Willi 1996; Willi 1998)
- increased pregnancy loss (Regan 1990; Balen 1993)(not confirmed by more recent data Rai 2000; Oliveira 2007)
No in pregnancy rates (Dodson 1987; Fleming 1988)
The use of GnRH agonists is not justified (Hughes 2004)
o Risk of OHSS (Homburg 1990; Scheele 1993; van der Meer 1996)
o Risk of multiple pregnancy (Homburg 1993; Clifford 1996)
o Costs and disconfort
Combination with GnRH analogueswww.generaroma.it
Issue 2, 2004
Combination with GnRH analogue:ovulation rate
www.generaroma.it

14
Combination with GnRH analogue:ovulation rate
www.generaroma.it
Combination with GnRH analogues: OHSS rate www.generaroma.it
Ultrasound monitoringwww.generaroma.it
o Baseline assessment of the ovary before starting OIo Accurate assessment of follicles >10mmo Cycle cancellation when >3 follicles >16mm (Calaf 2003)
- >4 follicles >14mm (Hughes 2006) - >2 follicles >14mm (Fahri 1996)- >3-4 follicles >10mm (Tur 2001; Dickei 2005) - >1 follicle >16mm >1 foll. >12mm (Leader 2006)
It is prudent to withhold HCG administration with >2 follicles of >16mm or with one 1 follicle >16mm and 2follicles of >14mm under the age of 38
(ESHRE/ASRM-Sponsored PCOS Consensus Whorkshop 2008)
Low dose step-up vs step-down: efficacywww.generaroma.it
(ESHRE/ASRM-Sponsored PCOS Consensus Whorkshop 2008)
15
Ovulation induction and IUI www.generaroma.it
Because subfertility is mainly due to anovulation in PCOSOI is the main treatmentNo RCTs in women with PCOS comparing OI and sponta-neous intercourses vs OI and IUI
In PCOS associated to mild male factor or after havingfailed OI and spontaneous intercourses, OI and IUI maybe considered (Cohlen, 2000)
Careful monitoring is essential to reduce the risk ofOHSS and multiple pregnancies (ESHRE Capri Workshop, 2003)
and in case TV ultrasound-guided aspiration of the su-pernumerary follicles (De Geyter, 1996)
Ovarian superovulation and IVF www.generaroma.it
o Anovulation is not an indication for IVF
o After failure of weight reduction, CC, or ovarian dril-ling OI with gonadotropins risks of multiple pregnancies.
o It may be argued to replace OI with IVF(Eijkemans 2005)
in order to make single embryo transfer with risksof multiple pregnancies (Papanikolau, 2006; Heijnen, 2007)
o PCOS with associated pathologies (tubal damage, seve-re endometriosis, PGD, severe male factor) IVF
COH and IVF: gonadotropins of choice? www.generaroma.it
Data from IVF cycles irrespective for indication for IVFare not in concordance
Meta-analysis (Daya, 2002)- rec-FSH significantly higher pregnancy rate- total dose of rec-FSH significantly lower- spontaneous abortion, multiple pregnancy and
OHSS rates comparable For every 19 patients treated 1 additional patient
would conceive when treated with rec-FSH
COH and IVF: gonadotropins of choice? www.generaroma.it
Meta-analysis (Al-Inany, 2002)- comparable pregnancy rate between
u-FSH vs rec-FSH
Meta-analysis (van Weley, 2003)- significantly increased pregnancy rate
with HMG in GnRH-a cyclesProspective study (Goldfarb, 2003)
- significantly increased implantation ratewith rec-FSH
No firm conclusions can be reached regardingthe superiority of one gonadotropin in IVF-PCOS

16
COH and IVF: combination with GnRH-analogue
www.generaroma.it
Suppression of LH with GnRH-agonist may reduce the incidence of spontaneous abortion (Homburg 1993)
Spontaneous abortion was not affected by using HMG vs u-FSH (Balen 1993; Homburg 1993)
GnRH-antagonists: no controlled study that compareagonists and antagonists in IVF PCOS patients
Theoretical advantage to reduce the incidence ofOHSS by GnRH agonist induced LH surge to trig-ger ovulation (Engmann 2008; Kol 2008)
Conclusionswww.generaroma.it
CC is the treatment of first choice in anovulatory wo-men. AIs are effective in OI in PCOS women and mayhave better clinical results than CC. Some concernsare risen on their safety and actually are off-labelled
No differences in term of ovulation, clinical pregnancymultiple pregnancy and miscarriage rates between FSHand HMG. Significantly increased OHSS with HMG
Low-dose step-up and step down protocols are compa-rable in term of ovulation rate and clinical outcome inOI. Combination with GnRH-analogs risk of OHSS
Conclusionswww.generaroma.it
US monitoring must be very accurate. During OI it isprudent to withhold HCG administration with >2 foll. of >16mm or with one 1 foll. >16mm and 2 foll. of >14mm under the age of 38
No firm conclusions can be reached regarding the su-periority of one gonadotropin in IVF-PCOSThe combination of GnRH-agonists might the riskof miscarriageThe combination of GnRH-antagonists might the riskof OHSS by GnRH agonist induced LH surge to trig-ger ovulation
CLINICA VALLE GIULIA, Rome
www.generaroma.it
Gynaecology:
Filippo Ubaldi
Elena Baroni
Silvia Colamaria
Fabio Sapienza
Maddalena Giuliani
Embriology:
Laura Rienzi
Stefania Romano
Roberta Maggiulli
Laura Albricci
Antonio Capalbo
Centre for Reproductive Medicine