RISK ANALYSIS FOR SEVERE TRAFFIC ACCIDENTS IN ROAD TUNNELS (PART I)
Central Annals of Otolaryngology and Rhinology
Cite this article: Comacchio F, Markova V, Accordi D, Covizzi F, Magnavita P (2015) Primary Downbeat Spontaneous Nystagmus and Severe Hypomagnese-mia: Monitoring and Follow-Up. Ann Otolaryngol Rhinol 2(2): 1021.
*Corresponding authorFrancesco Comacchio, Otolaryngology Unit, Azienda Ospedaliera Padova, via Giustiniani 2, 35100, Padova, Italy, Tel:39-049-8212023; Fax :39-049-8218265; Email:
Submitted: 07 January 2015
Accepted: 03 February 2015
Published: 05 February 2015
Copyright© 2015 Comacchio et al.
OPEN ACCESS
Keywords•Downbeat nystagmus•Hypomagnesemia•Cerebellum•Paroxysmal positional vertigo
Case Report
Primary Downbeat Spontaneous Nystagmus and Severe Hypomagnesemia: Monitoring and Follow-UpFrancesco Comacchio*,Vera Markova, Daria Accordi, Francesca Covizzi and Paola MagnavitaDepartment of Neurosciences, University Hospital Padova, Italy
Abstract
Primary spontaneous down-beat nystagmus (PDBN) is characterized by slow upward ocular drifts and fast downward phases, and is the most common form of acquired ocular movements overcoming fixation. PDBN is essentially due to lesions at the cranio-cervical junction, or diseases of the lower brainstem and cerebellum. Intoxication due to lithium or anti-epileptic drugs, abuse of toluene, and metabolic disturbances such vitamin B1, B12 deficiency, have also been reported. Hypomagnesemia has rarely been reported as another possible cause of PDBN. We report here a case of reversible high-intensity PDBN, due to severe hypomagnesaemia with ataxia, objective vertigo and oscillopsia, although initial cerebellar MR imaging was normal. Monitoring of nystagmus according to magnesemia is reported and discussed.
ABBREVIATIONSPDBN: Primary Spontaneous Downbeat Nystagmus; VOR:
Vestibular Ocular Reflex; GABA: Gamma-Aminobutyric Acid; EGF: Epidermal Growth Factor; SPV: Slow-Phase Angular Velocity; MRI: Magnetic Resonance Imaging; GAD: Glutamic Acid Decarboxylase; CT: Computerized Tomography; ECG: Electrocardiogram.
INTRODUCTIONPrimary spontaneous down-beat nystagmus (PDBN) is
characterized by slow upward ocular drifts and fast downward phases, and is the most common form of acquired ocular movements overcoming fixation. It usually increases with lateral and downward gaze often with supine position [1]. PDBN is essentially due to lesions at the cranio-cervical junction, or diseases of the lower brainstem and cerebellum as, infarction, cerebellar and spinocerebellar degeneration syndromes like spinocerebellar ataxia, multisystem atrophy and sporadic adult onset ataxia, multiple sclerosis and developmental anomalies involving the pons and cerebellum. Intoxication due to lithium or anti-epileptic drugs, abuse of toluene, and metabolic disturbances such vitamin B1, B12 deficiency, have also been reported. PDBN has been attributed to damage to the brainstem-cerebellar loop. In patients with PDBN, the inhibitory GABAergic cerebellar input from the Purkinje cells to the vestibular nuclei is disrupted. This disruption is thought to decrease the downward
VOR tone provoking the upward slow phase eye movement [2]. The cerebellar floccules seems in fact to inhibits only anterior canal pathways (linked to upward eye movements), and not the posterior canal pathways (downward eye movements) [3], so lesions to the vestibule cerebellum remove inhibition from the anterior canal pathways and not from the posterior canal resulting in downbeat nystagmus. Autoimmune conditions can also cause PDBN as in the presence of anti-glutamic acid decarboxylase antibodies [4] or in paraneoplastic syndromes. Antibodies against GABAergic neurons may induce chemical denervation of the floccular neurons, which suppress the peripheral imbalance between the vertical semicircular canal systems, causing PDBN.
Hypomagnesemia has rarely been reported as another possible cause of PDBN. Magnesium is an essential cation involved in many biochemical and physiological processes in the body, and hypomagnesaemia has been associated with various neurological symptoms including ataxia, reversible mental status changes, seizure, aphasia and movement disorders. We report here a case of reversible high-intensity PDBN, due to severe hypomagnesaemia with ataxia, objective vertigo and oscillopsia, although initial cerebellar MR imaging was normal. The results of one month of nystagmus monitoring and correlation with seric magnesemia are discussed.
CASE PRESENTATIONA 78-year-old man presented to the Emergency Department
Central
Comacchio et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1021 (2015) 2/6
of Padova University Hospital, complaining of dizziness which had lasted two days, such severe instability that it was impossible for him to maintain normal posture, oscillopsy, arm tremors, anxiety, and nausea. His medical history revealed hypertension, chronic renal insufficiency, ischemic coronary disease, a previous aorto-bifemoral bypass for aorta aneurism and colic diverticulitis. In 2002, he had undergone radical cystectomy for cancer, with a completely normal follow-up for ten years. Three days before the onset of dizziness, the patient had suffered attacks of abdominal pain with diarrhoea. He frequently suffered from episodes of diverticulitis.
The emergency neurologic evaluation showed severe instability, arm tremors, and normal profound reflexes with normal extrinsic ocular motility. Cerebellar manoeuvres were correctly performed. A CT brain scan revealed diffuse white matter hypo density due to cerebrovascular chronic ischemia and slight cerebral and cerebellar atrophy, without acute vascular events. ECG results were within normal limits.
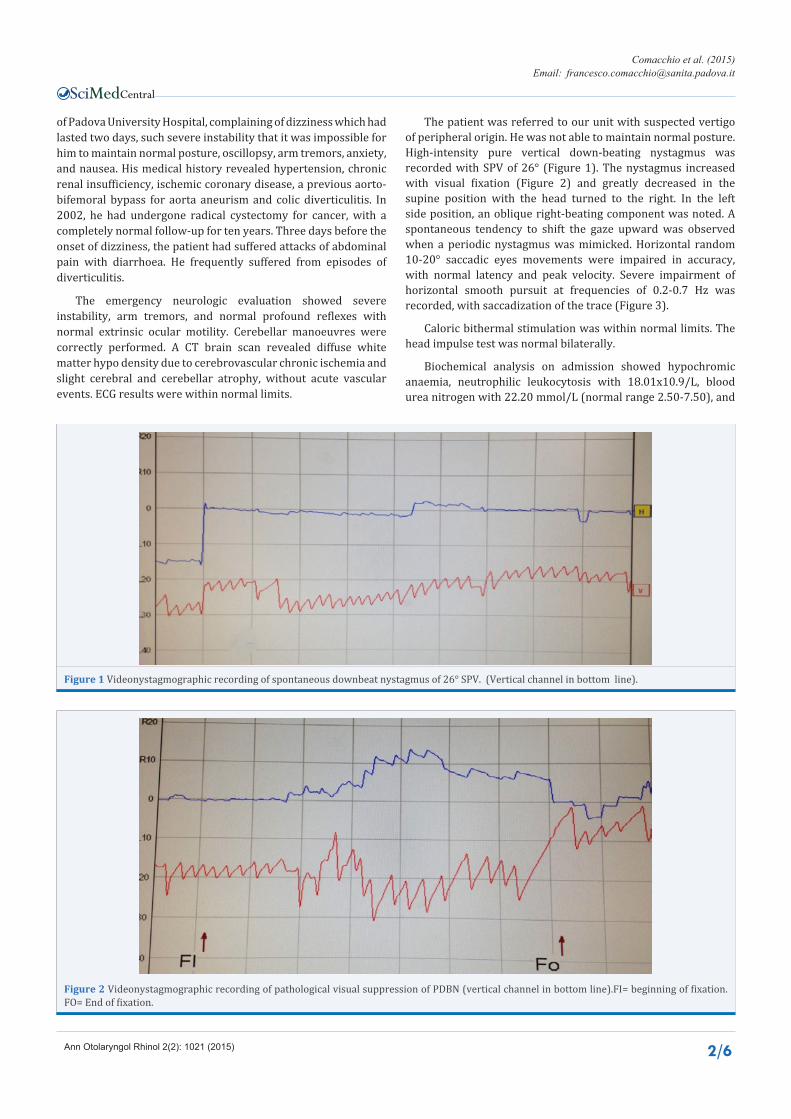
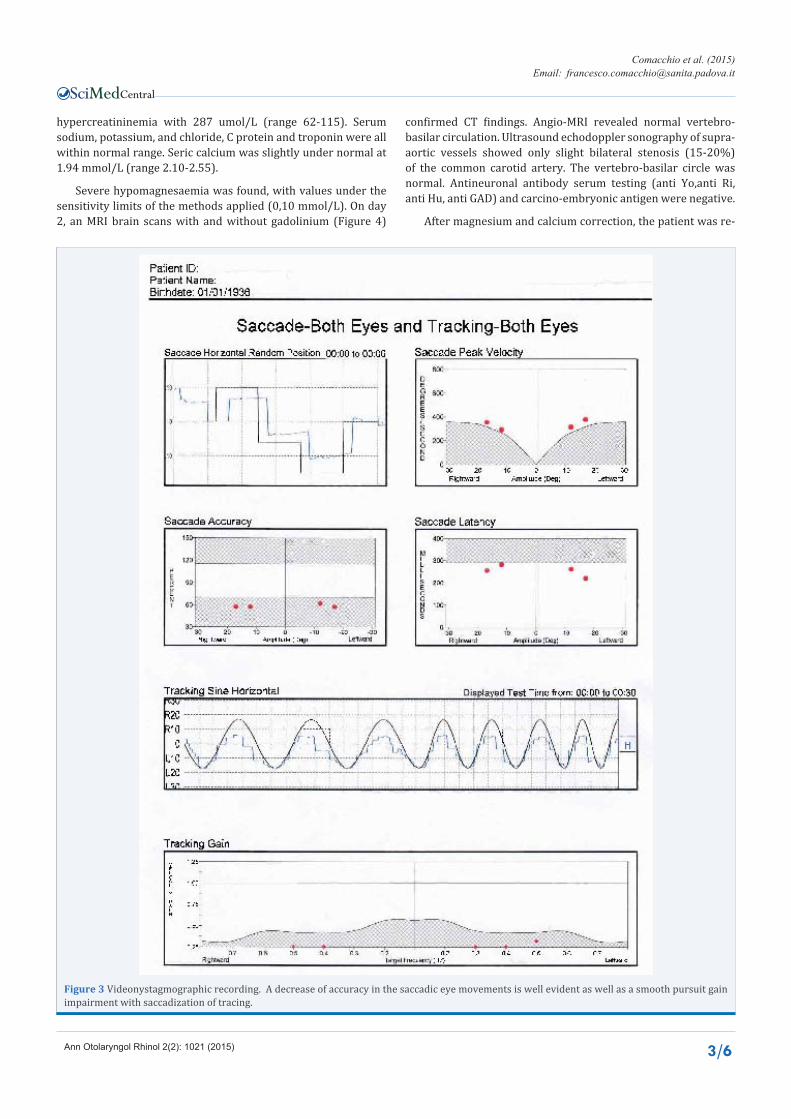
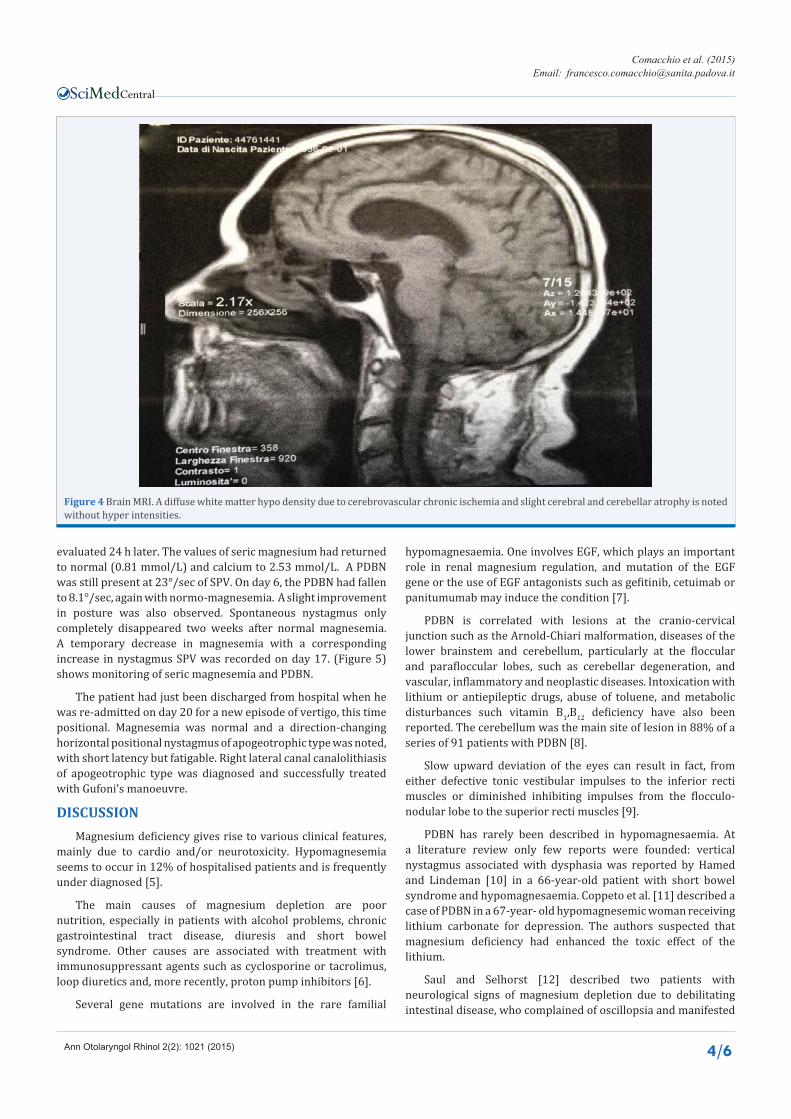
The patient was referred to our unit with suspected vertigo of peripheral origin. He was not able to maintain normal posture. High-intensity pure vertical down-beating nystagmus was recorded with SPV of 26° (Figure 1). The nystagmus increased with visual fixation (Figure 2) and greatly decreased in the supine position with the head turned to the right. In the left side position, an oblique right-beating component was noted. A spontaneous tendency to shift the gaze upward was observed when a periodic nystagmus was mimicked. Horizontal random 10-20° saccadic eyes movements were impaired in accuracy, with normal latency and peak velocity. Severe impairment of horizontal smooth pursuit at frequencies of 0.2-0.7 Hz was recorded, with saccadization of the trace (Figure 3).
Caloric bithermal stimulation was within normal limits. The head impulse test was normal bilaterally.
Biochemical analysis on admission showed hypochromic anaemia, neutrophilic leukocytosis with 18.01x10.9/L, blood urea nitrogen with 22.20 mmol/L (normal range 2.50-7.50), and
Figure 1 Videonystagmographic recording of spontaneous downbeat nystagmus of 26° SPV. (Vertical channel in bottom line).
Figure 2 Videonystagmographic recording of pathological visual suppression of PDBN (vertical channel in bottom line).FI= beginning of fixation. FO= End of fixation.
Central
Comacchio et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1021 (2015) 3/6
hypercreatininemia with 287 umol/L (range 62-115). Serum sodium, potassium, and chloride, C protein and troponin were all within normal range. Seric calcium was slightly under normal at 1.94 mmol/L (range 2.10-2.55).
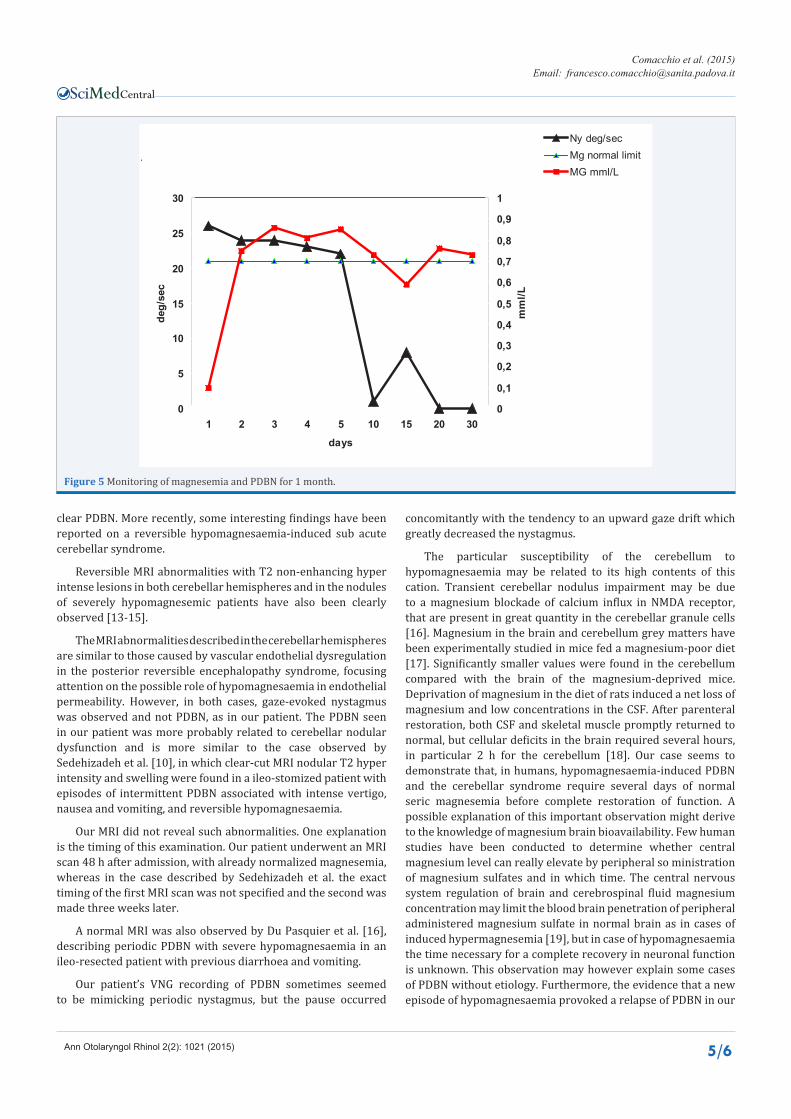
Severe hypomagnesaemia was found, with values under the sensitivity limits of the methods applied (0,10 mmol/L). On day 2, an MRI brain scans with and without gadolinium (Figure 4)
confirmed CT findings. Angio-MRI revealed normal vertebro-basilar circulation. Ultrasound echodoppler sonography of supra-aortic vessels showed only slight bilateral stenosis (15-20%) of the common carotid artery. The vertebro-basilar circle was normal. Antineuronal antibody serum testing (anti Yo,anti Ri, anti Hu, anti GAD) and carcino-embryonic antigen were negative.
After magnesium and calcium correction, the patient was re-
Figure 3 Videonystagmographic recording. A decrease of accuracy in the saccadic eye movements is well evident as well as a smooth pursuit gain impairment with saccadization of tracing.
Central
Comacchio et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1021 (2015) 4/6
Figure 4 Brain MRI. A diffuse white matter hypo density due to cerebrovascular chronic ischemia and slight cerebral and cerebellar atrophy is noted without hyper intensities.
evaluated 24 h later. The values of seric magnesium had returned to normal (0.81 mmol/L) and calcium to 2.53 mmol/L. A PDBN was still present at 23°/sec of SPV. On day 6, the PDBN had fallen to 8.1°/sec, again with normo-magnesemia. A slight improvement in posture was also observed. Spontaneous nystagmus only completely disappeared two weeks after normal magnesemia. A temporary decrease in magnesemia with a corresponding increase in nystagmus SPV was recorded on day 17. (Figure 5) shows monitoring of seric magnesemia and PDBN.
The patient had just been discharged from hospital when he was re-admitted on day 20 for a new episode of vertigo, this time positional. Magnesemia was normal and a direction-changing horizontal positional nystagmus of apogeotrophic type was noted, with short latency but fatigable. Right lateral canal canalolithiasis of apogeotrophic type was diagnosed and successfully treated with Gufoni’s manoeuvre.
DISCUSSIONMagnesium deficiency gives rise to various clinical features,
mainly due to cardio and/or neurotoxicity. Hypomagnesemia seems to occur in 12% of hospitalised patients and is frequently under diagnosed [5].
The main causes of magnesium depletion are poor nutrition, especially in patients with alcohol problems, chronic gastrointestinal tract disease, diuresis and short bowel syndrome. Other causes are associated with treatment with immunosuppressant agents such as cyclosporine or tacrolimus, loop diuretics and, more recently, proton pump inhibitors [6].
Several gene mutations are involved in the rare familial
hypomagnesaemia. One involves EGF, which plays an important role in renal magnesium regulation, and mutation of the EGF gene or the use of EGF antagonists such as gefitinib, cetuimab or panitumumab may induce the condition [7].
PDBN is correlated with lesions at the cranio-cervical junction such as the Arnold-Chiari malformation, diseases of the lower brainstem and cerebellum, particularly at the floccular and parafloccular lobes, such as cerebellar degeneration, and vascular, inflammatory and neoplastic diseases. Intoxication with lithium or antiepileptic drugs, abuse of toluene, and metabolic disturbances such vitamin B1,B12 deficiency have also been reported. The cerebellum was the main site of lesion in 88% of a series of 91 patients with PDBN [8].
Slow upward deviation of the eyes can result in fact, from either defective tonic vestibular impulses to the inferior recti muscles or diminished inhibiting impulses from the flocculo-nodular lobe to the superior recti muscles [9].
PDBN has rarely been described in hypomagnesaemia. At a literature review only few reports were founded: vertical nystagmus associated with dysphasia was reported by Hamed and Lindeman [10] in a 66-year-old patient with short bowel syndrome and hypomagnesaemia. Coppeto et al. [11] described a case of PDBN in a 67-year- old hypomagnesemic woman receiving lithium carbonate for depression. The authors suspected that magnesium deficiency had enhanced the toxic effect of the lithium.
Saul and Selhorst [12] described two patients with neurological signs of magnesium depletion due to debilitating intestinal disease, who complained of oscillopsia and manifested
Central
Comacchio et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1021 (2015) 5/6
.
0
5
10
15
20
25
30
1 2 3 4 5 10 15 20 30
days
deg/
sec
0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1
mm
l/L
Ny deg/secMg normal limitMG mml/L
Figure 5 Monitoring of magnesemia and PDBN for 1 month.
clear PDBN. More recently, some interesting findings have been reported on a reversible hypomagnesaemia-induced sub acute cerebellar syndrome.
Reversible MRI abnormalities with T2 non-enhancing hyper intense lesions in both cerebellar hemispheres and in the nodules of severely hypomagnesemic patients have also been clearly observed [13-15].
The MRI abnormalities described in the cerebellar hemispheres are similar to those caused by vascular endothelial dysregulation in the posterior reversible encephalopathy syndrome, focusing attention on the possible role of hypomagnesaemia in endothelial permeability. However, in both cases, gaze-evoked nystagmus was observed and not PDBN, as in our patient. The PDBN seen in our patient was more probably related to cerebellar nodular dysfunction and is more similar to the case observed by Sedehizadeh et al. [10], in which clear-cut MRI nodular T2 hyper intensity and swelling were found in a ileo-stomized patient with episodes of intermittent PDBN associated with intense vertigo, nausea and vomiting, and reversible hypomagnesaemia.
Our MRI did not reveal such abnormalities. One explanation is the timing of this examination. Our patient underwent an MRI scan 48 h after admission, with already normalized magnesemia, whereas in the case described by Sedehizadeh et al. the exact timing of the first MRI scan was not specified and the second was made three weeks later.
A normal MRI was also observed by Du Pasquier et al. [16], describing periodic PDBN with severe hypomagnesaemia in an ileo-resected patient with previous diarrhoea and vomiting.
Our patient’s VNG recording of PDBN sometimes seemed to be mimicking periodic nystagmus, but the pause occurred
concomitantly with the tendency to an upward gaze drift which greatly decreased the nystagmus.
The particular susceptibility of the cerebellum to hypomagnesaemia may be related to its high contents of this cation. Transient cerebellar nodulus impairment may be due to a magnesium blockade of calcium influx in NMDA receptor, that are present in great quantity in the cerebellar granule cells [16]. Magnesium in the brain and cerebellum grey matters have been experimentally studied in mice fed a magnesium-poor diet [17]. Significantly smaller values were found in the cerebellum compared with the brain of the magnesium-deprived mice. Deprivation of magnesium in the diet of rats induced a net loss of magnesium and low concentrations in the CSF. After parenteral restoration, both CSF and skeletal muscle promptly returned to normal, but cellular deficits in the brain required several hours, in particular 2 h for the cerebellum [18]. Our case seems to demonstrate that, in humans, hypomagnesaemia-induced PDBN and the cerebellar syndrome require several days of normal seric magnesemia before complete restoration of function. A possible explanation of this important observation might derive to the knowledge of magnesium brain bioavailability. Few human studies have been conducted to determine whether central magnesium level can really elevate by peripheral so ministration of magnesium sulfates and in which time. The central nervous system regulation of brain and cerebrospinal fluid magnesium concentration may limit the blood brain penetration of peripheral administered magnesium sulfate in normal brain as in cases of induced hypermagnesemia [19], but in case of hypomagnesaemia the time necessary for a complete recovery in neuronal function is unknown. This observation may however explain some cases of PDBN without etiology. Furthermore, the evidence that a new episode of hypomagnesaemia provoked a relapse of PDBN in our

Central
Comacchio et al. (2015)Email:
Ann Otolaryngol Rhinol 2(2): 1021 (2015) 6/6
patient seem to demonstrate that disappearing of nystagmus was not related to vestibular plasticity but to magnesium restoration. The normal vestibular function at calorics represents a further argument to exclude vestibular plasticity that, as known, has an important role in compensation when inducted by a sudden peripheral damage. Usually vestibular plasticity intrinsic in the central nervous system requires more than few days to suppress a central nystagmus.
Despite the many recognized causes of PDBN, in many cases its etiology still remains undiagnosed, meaning that we can only classify these cases as “idiopathic”. Wagner et al. [20] recently reported that no recognisable cause could be found in 38% of a large series of 117 cases of PDBN. In our opinion, careful anamnestic evaluation of previous gastro-intestinal disturbances, even minor, should always be carry out in patients with PDBN and normal MRI. The possibility of an episode of previous hypomagnesaemia should be taken into account, as the normal seric value does not exclude the possibility of cerebellar involvement in a phase of restoration, and most reported cases of magnesium-induced hypomagnesaemia presented anamnestically together with gastro-intestinal problems. Further studies are necessary to monitor possible MRI cerebellar alterations, in order to determine the exact duration of imaging impairment.
The observation in our case of paroxysmal positional vertigo as outcome of hypomagnesaemia may be a pure coincidence, related to bed rest or to the long-term admission, or may represent a speculative observation that magnesium plays a role in eolith metabolism. Our knowledge about this hypothesis is very poor. In constantly growing eoliths of fish, concentration of Mg was significantly lower than in otoconia of other fishes or animals. This is presumably due to the fact that Mg inhibits crystalline growth of calcium salts [21]. Our case may represent a stimulus for further studies to verify a possible role of hypomagnesaemia on eolith metabolism in humans.
REFERENCES1. Leigh RJ, Zee DS. The neurology of eye movement. 4th Edn, Oxford
University Press.2006. New York.
2. Marti S, Straumann D, Büttner U, Glasauer S. A model-based theory on the origin of downbeat nystagmus. Exp Brain Res. 2008; 188: 613-631.
3. Ito M, Nisimaru N, Yamamoto M. Specific patterns of neuronal connexions involved in the control of the rabbit’s vestibulo-ocular reflexes by the cerebellar flocculus. J Physiol. 1977; 265: 833-854.
4. Antonini G, Nemni R, Giubilei F, Gragnani F, Ceschin V, Morino S, et al. Autoantibodies to glutamic acid decarboxylase in downbeat nystagmus. J Neurol Neurosurg Psychiatry. 2003; 74: 998-999.
5. Whang R, Ryder KW. Frequency of hypomagnesemia and
hypermagnesemia. Requested vs routine. JAMA. 1990; 263: 3063-3064.
6. Hess MW, Hoenderop JG, Bindels RJ, Drenth JP. Systematic review: hypomagnesaemia induced by proton pump inhibition. Aliment Pharmacol Ther. 2012; 36: 405-413.
7. Groenestege WM, Thébault S, van der Wijst J, van den Berg D, Janssen R, Tejpar S, et al. Impaired basolateral sorting of pro-EGF causes isolated recessive renal hypomagnesemia. J Clin Invest. 2007; 117: 2260-2267.
8. Yee RD. Downbeat nystagmus: characteristics and localization of lesions. Trans Am Ophthalmol Soc. 1989; 87: 984-1032.
9. Marti S, Straumann D, Glasauer S. The origin of downbeat nystagmus: an asymmetry in the distribution of on-directions of vertical gaze-velocity Purkinje cells. Ann N Y Acad Sci. 2005; 1039: 548-553.
10. Hamed IA, Lindeman RD. Dysphagia and vertical nystagmus in magnesium deficiency. Ann Intern Med. 1978; 89: 222-223.
11. Coppeto JR, Monteiro ML, Lessell S, Bear L, Martinez-Maldonado M. Downbeat nystagmus. Long-term therapy with moderate-dose lithium carbonate. Arch Neurol. 1983; 40: 754-755.
12. Saul RF, Selhorst JB. Downbeat nystagmus with magnesium depletion. Arch Neurol. 1981; 38: 650-652.
13. Sedehizadeh S, Keogh M, Wills AJ. Reversible hypomagnesaemia-induced subacute cerebellar syndrome. Biol Trace Elem Res. 2011; 142: 127-129.
14. Boulos MI, Shoamanesh A, Aviv RI, Gladstone DJ, Swartz RH. Severe hypomagnesemia associated with reversible subacute ataxia and cerebellar hyperintensities on MRI. Neurologist. 2012; 18: 223-225.
15. Te Riele MG, Verrips A. Severe hypomagnesaemia causing reversible cerebellopathy. Cerebellum. 2014; 13: 659-662.
16. Du Pasquier R, Vingerhoets F, Safran AB, Landis T. Periodic downbeat nystagmus. Neurology. 1998; 51: 1478-1480.
17. Pereira TG, Morais Mda G. [Magnesium quantification in mouse brain and cerebellum grey matter]. Acta Med Port. 2005; 18: 257-260.
18. Chutkow JG. Metabolism of magnesium in central nervous system. Relationship between concentrations of magnesium in cerebrospinal fluid and brain in magnesium deficiency. Neurology. 1974; 24: 780-787.
19. McKee JA, Brewer RP, Macy GE, Phillips-Bute B, Campbell KA, Borel CO, et al. Analysis of the brain bioavailability of peripherally administered magnesium sulfate: A study in humans with acute brain injury undergoing prolonged induced hypermagnesemia. Crit Care Med. 2005; 33: 661-666.
20. Wagner JN, Glaser M, Brandt T, Strupp M. Downbeat nystagmus: aetiology and comorbidity in 117 patients. J Neurol Neurosurg Psychiatry. 2008; 79: 672-677.
21. Lychakov DV, Lavrova EA. [The content of electrolytes (Na, K, Ca, Mg) in vertebrate otoliths and otoconia]. Zh Evol Biokhim Fiziol. 1994; 30: 99-105.
Comacchio F, Markova V, Accordi D, Covizzi F, Magnavita P (2015) Primary Downbeat Spontaneous Nystagmus and Severe Hypomagnesemia: Monitoring and Follow-Up. Ann Otolaryngol Rhinol 2(2): 1021.
Cite this article