Presentazione di PowerPoint - pinguini.net · < 6 months NO unless > 6 months of age with positive...
50
G. MONTINI Orientiamoci nelle infezioni delle vie urinarie
Transcript of Presentazione di PowerPoint - pinguini.net · < 6 months NO unless > 6 months of age with positive...

G. MONTINIOrientiamoci nelle infezioni delle vie urinarie

IVU: EPIDEMIOLOGIA

RUOLO CIRCONCISIONE
RISCHIO CRESCENTE

Reni e vie urinarie sono sterili
L’ingresso dei batteri può portare a diverse condizioni:
– Batteriuria
– Cistite
– IVU febbrile con attivazione della risposta infiammatoria
Un adeguato flusso urinario e un uroepitelio intatto prevengono l’insorgenza di IVU.
E. coli ha P fimbriae che facilitano invasione uroepitelio
IVU: FISIOPATOLOGIA

Montini G. et al 2011

UTI: DIAGNOSI
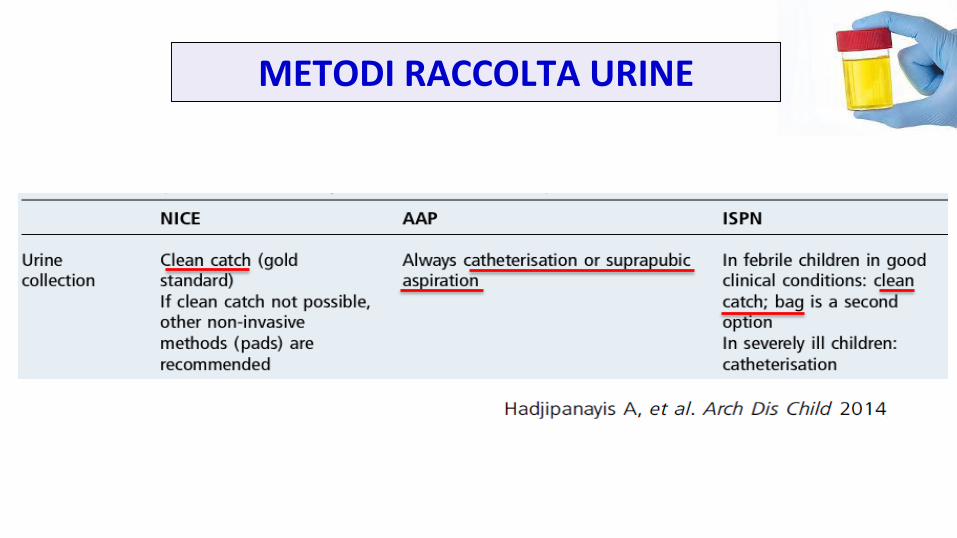
METODI RACCOLTA URINE
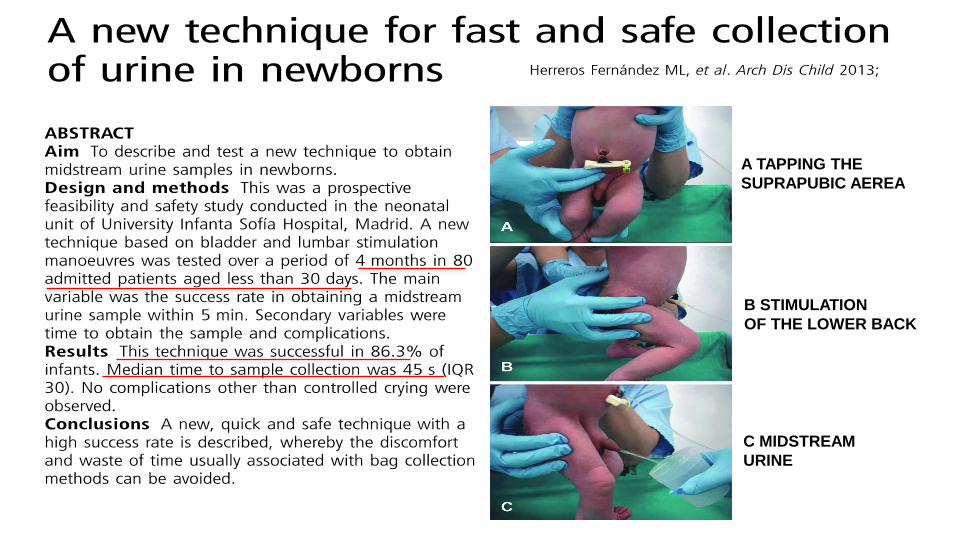
A TAPPING THE
SUPRAPUBIC AEREA
B STIMULATION
OF THE LOWER BACK
C MIDSTREAM
URINE
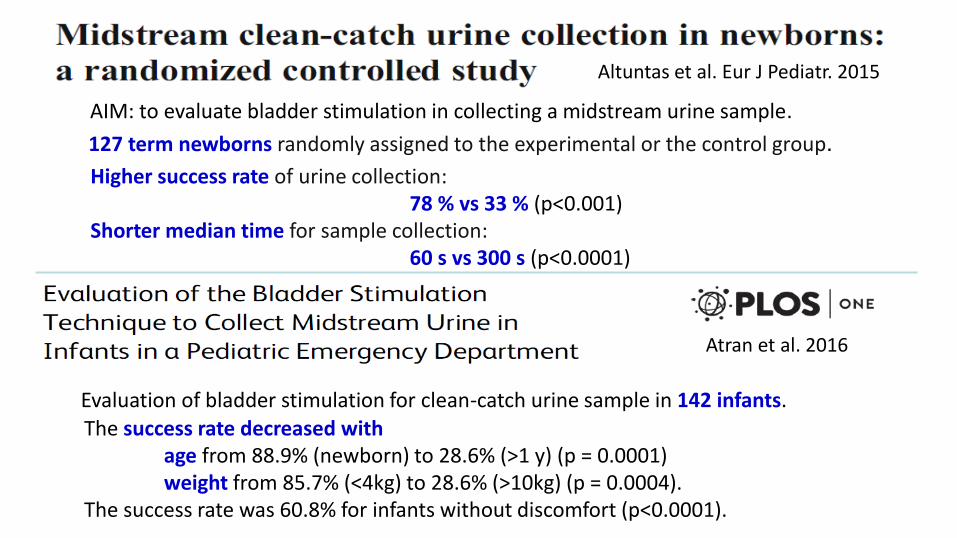
Higher success rate of urine collection:78 % vs 33 % (p<0.001)
Shorter median time for sample collection:60 s vs 300 s (p<0.0001)
Altuntas et al. Eur J Pediatr. 2015
127 term newborns randomly assigned to the experimental or the control group.
AIM: to evaluate bladder stimulation in collecting a midstream urine sample.
Evaluation of bladder stimulation for clean-catch urine sample in 142 infants.The success rate decreased with
age from 88.9% (newborn) to 28.6% (>1 y) (p = 0.0001) weight from 85.7% (<4kg) to 28.6% (>10kg) (p = 0.0004).
The success rate was 60.8% for infants without discomfort (p<0.0001).
Atran et al. 2016
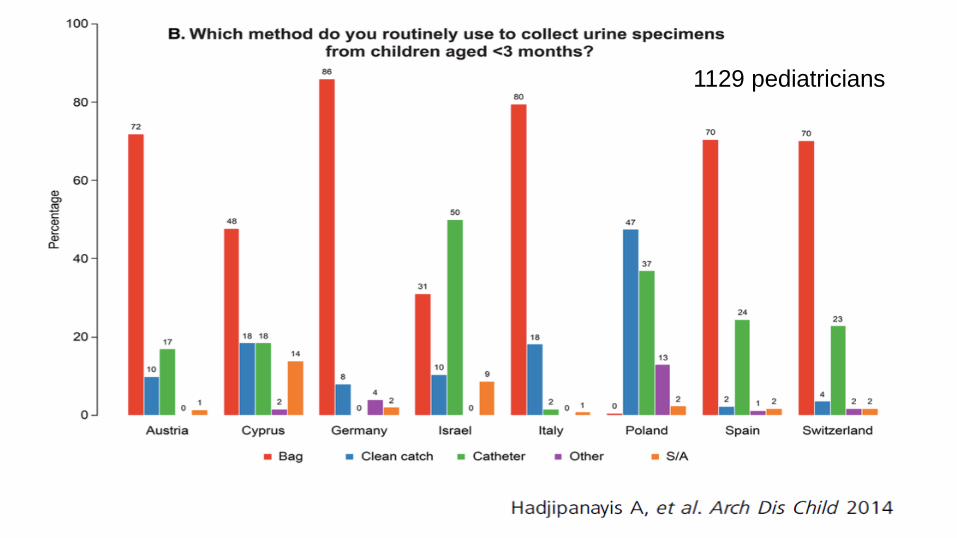
1129 pediatricians

DIAGNOSI IVUTAKE HOME MESSAGES
In caso di sospetta IVU eseguire esame urine
Se esame urine positivo per nitriti e/o leucociti eseguire urinocoltura
Effettuare urinocoltura preferenzialmente conclean-catch o mitto intermedio

TERAPIA
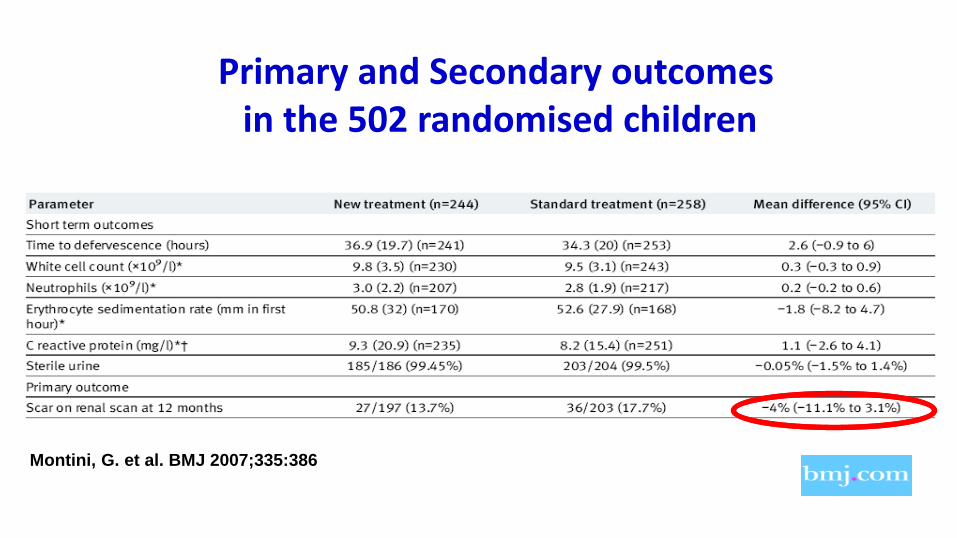
Primary and Secondary outcomesin the 502 randomised children
Montini, G. et al. BMJ 2007;335:386

Italian Society of Pediatric Nephrology

1129 pediatricians

• Antibiotici a spettro ristretto!!!!!Non sprecare antibiotici a largo spettro.
• Nitrofurantoina
• Trimetropim
• Fosfomicina
• Cotrimoxazolo (alta resistenza in Italia!!!!!)
IVU NON FEBBRILI = CISTITI

TERAPIA IVUTAKE HOME MESSAGES
Prediligere la via orale (amoxiclav o cefalosporina)
Terapia EV se condizioni generali compromesse, segni di sepsi o vomito
PIELONEFRITI = antibiotico ad ampio spettro per 7-14 giorni
CISTITI sempre terapia orale e per massimo 5 giorniAntibiotico a spettro ristretto
BAMBINOPICCOLO< 3 anni
BAMBINOGRANDE> 3 anni
GESTIONE DEL BAMBINO DOPO IVU
≠

COSA FARE NEL BAMBINO PICCOLO ?

Si esegue imaging per identificare:
• malformazioni ostruttive,
• reflusso vescico-ureterale,
• danno renale.
Tuttavia manca ancora un consenso su tipo dimalformazioni, grado di reflusso, e entità di dannorenale che è importante individuare
IMAGING DOPO PRIMA IVU FEBBRILE

Guidelines Ultrasound VCUG DMSA
NICE (2007) YESAtypical UTI;< 6 months
NOunless > 6 months of age with positive US or atypical UTI
YES> 6/12 m from UTI
AAP (2011) YES NO Unless abnormal US
NO
Italian (2012) YES NOUnless abnormal USor risk factors
YES>6/12 m from UTI if abnormal US or VUR
Australian (2014) YES if no 2°or 3° trimester US ;< 3 months;Atypical UTI
NO Unless abnormal US
NO
Canadian (2014) YES NO Unless abnormal US
NO
LINEE GUIDA PER IMAGING DOPO PRIMA IVU FEBBRILE
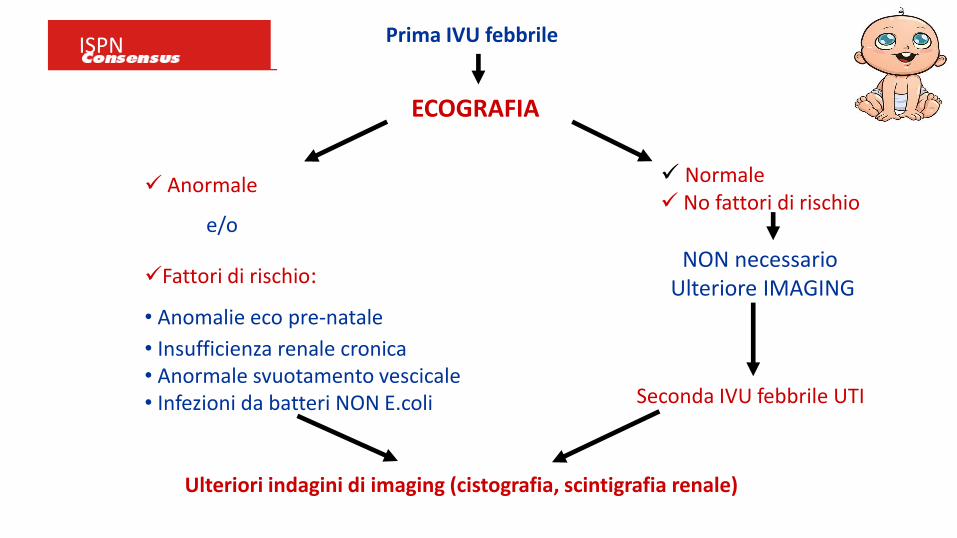
Prima IVU febbrile
ECOGRAFIA
Anormale
e/o
Fattori di rischio:
• Anomalie eco pre-natale
• Insufficienza renale cronica• Anormale svuotamento vescicale• Infezioni da batteri NON E.coli
Ulteriori indagini di imaging (cistografia, scintigrafia renale)
Normale No fattori di rischio
Seconda IVU febbrile UTI
NON necessarioUlteriore IMAGING
ISPN

1129 pediatricians

IMAGING DOPO IVU < 3 ANNITAKE HOME MESSAGES
Se IVU sotto i 3 annieffettuare ECO-RENALE sempre
Cistografia e Scintigrafia individuano anomalie anatomichereflusso vescico-ureterale e danno renaleEseguirle SOLO se US patologica o fattori di rischio

COSA FARE NEL BAMBINO GRANDE
> 3 ANNI?
RICERCAREDISFUNZIONE VESCICALE
E/O STIPSI
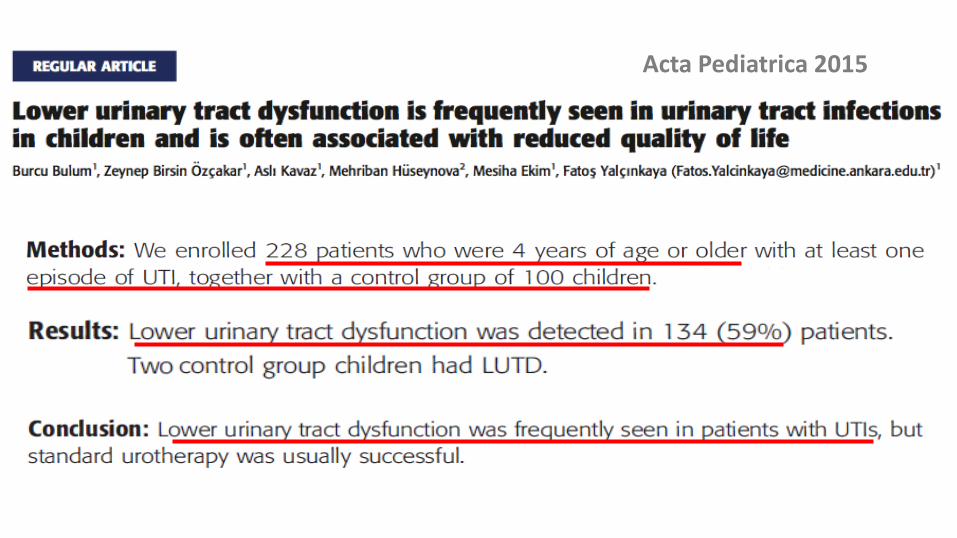
Acta Pediatrica 2015

Iperattività muscolo detrusore Iperattività sfintere esterno
Vescica piccola! Vescica grande!
INCOMPLETO RIEMPIMENTO INCOMPLETO SVUOTAMENTO
PATOGENESI
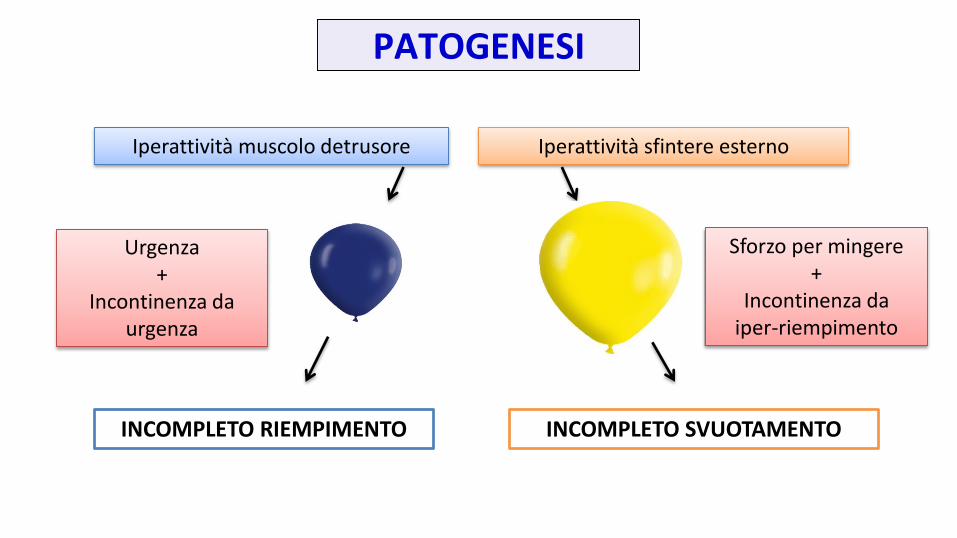
Iperattività muscolo detrusore Iperattività sfintere esterno
INCOMPLETO RIEMPIMENTO INCOMPLETO SVUOTAMENTO
Urgenza+
Incontinenza da urgenza
Sforzo per mingere+
Incontinenza da iper-riempimento
PATOGENESI

1. Frequenza : 4≤ normale ≥8 2. Incontinenza: perdita durante il giorno3. Urgenza: improvvisa necessità di mingere4. Esitazione: difficoltoso inizio della minzione5. Sforzo: impegno del torchio addominale6. Mitto debole7. Mitto intermittente8. Ritardo nell’iniziare la minzione9. Gocciolamento dopo la minzione10. Stipsi
ANAMNESI MINZIONALE:10 domande da fare sempre
Nei bambini> 5 anni

AUMENTO PRESSIONE ENDOVESCICALE
STASI URINARIA
ALTERATA PRODUZIONE DI MUCO e fattori “protettivi”
IVURICORRENTI
ISCHEMIA DELLA MUCOSA
Facilitato ingresso germi
RELAZIONE TRA IVU E DISFUNZIONE VESCICALE :
IL RUOLO DELLA AUMENTATA PRESSIONE VESCICALE

RESIDUO PM
AH AH!
BIOHAZARD
RELAZIONE TRA IVU E DISFUNZIONE VESCICALE :
RUOLO DELLO SVUOTAMENTO VESCICALE INCOMPLETO

OSTRUZIONE URINARIA FUNZIONALE
FECES
FECAL ACCUMULATION IN CHILDRENOBSTRUCTIVE CONSEQUENCES
• Compresses urethra and bladder neck
• Induces pelvic floor dysynergia tightens during emptying
• Produces abnormal, hesitant, interrupted or incomplete voiding
• Obstruction creates bladder instability
• Causes infrequent voiding and residual urine by confusing bladder
sensations

FECAL ACCUMULATION IN CHILDRENURINARY CONSEQUENCES
‐ Infrequent voiding residual urine
‐ Bladder instability VUR
‐ Fecal retention enteric bacteria
‐ Soiling perineal colonization
UTI !!!
1973 NEUMANN et alCHILDREN WITH UTI AND FECAL RETENTION
• CONSTIPATION CUREDUTI RECURRED IN 20%
• CONSTIPATION UNCUREDUTI RECURRED IN 88%
DYSFUNCTIONAL ELIMINATION OBSERVATIONS

1993 DOHIL et al BLADDER EMPTYING
66% OF CONSTIPATED CHILDREN LARGE RESIDUAL URINE VOLUMES
AFTER TREATMENT DECREASES TO 21%
DYSFUNCTIONAL ELIMINATION OBSERVATIONS

GESTIONE DOPO IVU >3 ANNITAKE HOME MESSAGES
Ricercare presenza diSTIPSIDISFUNZIONE VESCICALE
CORREGGERE stipsi e/o disfunzione vescicale per RIDURRE ilrischio di RECIDIVE


6.7%
5.7%
8%
27.5%
42.8%
n = 516
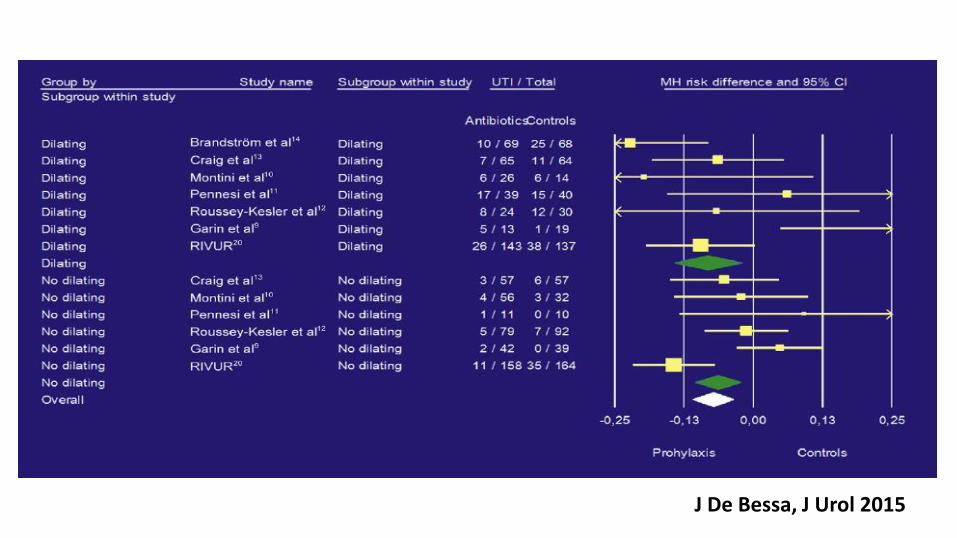
J De Bessa, J Urol 2015
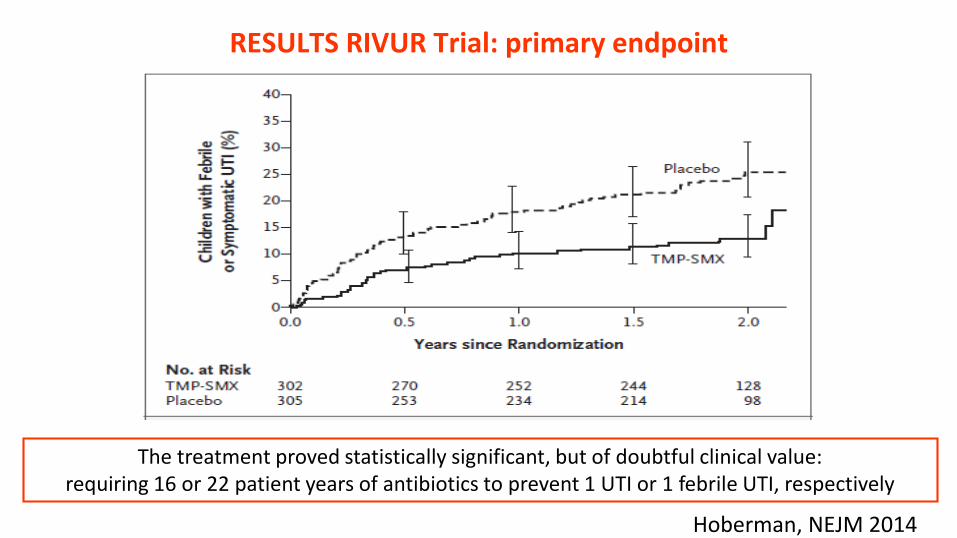
RESULTS RIVUR Trial: primary endpoint
The treatment proved statistically significant, but of doubtful clinical value: requiring 16 or 22 patient years of antibiotics to prevent 1 UTI or 1 febrile UTI, respectively
Hoberman, NEJM 2014
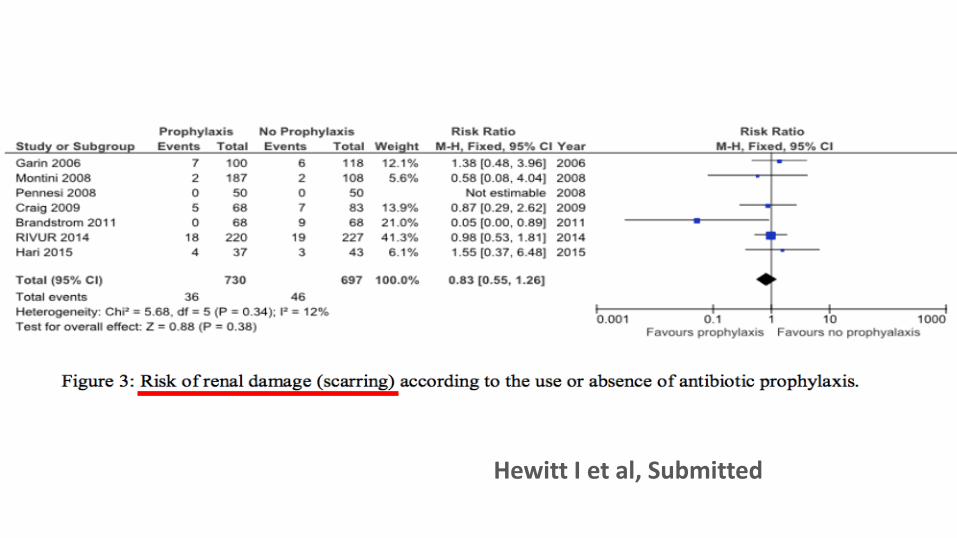
Hewitt I et al, Submitted

Guidelines Antibiotic prophylaxis Others interventions
NICE
Not for routine use
Treat dysfunctional elimination syndromes and constipation
Drink an adequate amount of fluid Do not delay voiding
AAP
Not for routine use Not considered
ISPN
For reflux III-V Recurrent febrile UTI*
Not considered
* ≥3 febrile UTIs within 12 months
PROFILASSI ANTIBIOTICA PER IVU: LINEE GUIDA
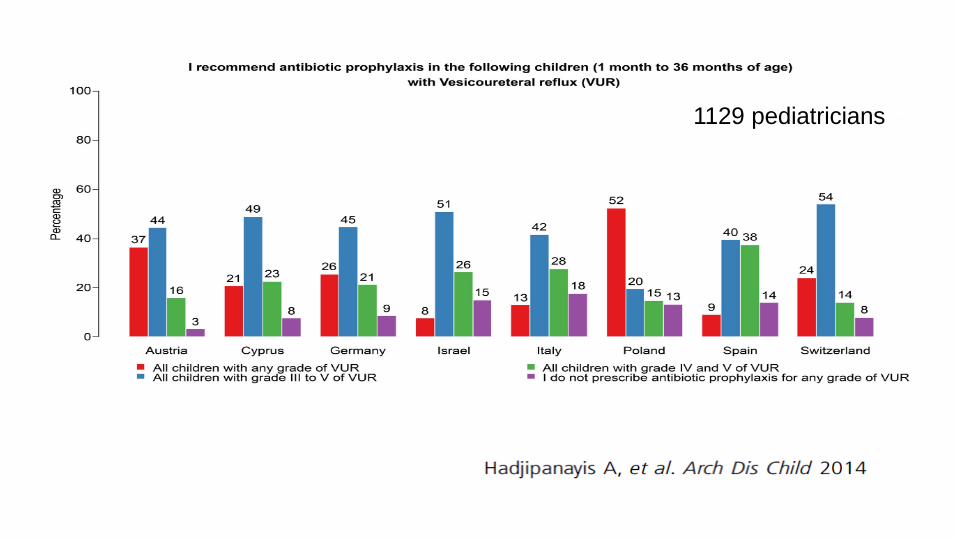
1129 pediatricians

THE PREDICT TRIAL
Antibiotic Prophylaxis and REnal Damage In Congenital abnormalities of the kidney and urinary Tract

14EUROPEAN COUNTRIES
PREDICT TRIAL: PAESI COINVOLTI

SEX N° %
FEMALE 34 22.1
MALE 120 77.9
AGE at registration Mean Median
(months) 2.4 2
RENAL DAMAGE N° %
NO 60 39
ONE KIDNEY 77 50
BOTH KIDNEYS 17 11
61% with RENAL DAMAGE
VUR GRADE N° %
III 39 25.3
IV 61 39.6
V 54 35.1
RANDOMIZED PATIENTS: 154BASELINE CHARACTERISTICS

PROFILASSI DOPO IVUTAKE HOME MESSAGES
Obiettivo: prevenire recidive IVU e conseguente danno renaleEFFICACIA CONTROVERSA
NON si esegue routinariamente in tutti i bambini
PROFILASSI raccomandata solo nei RVU di alto grado (III-IV-V)…per ora
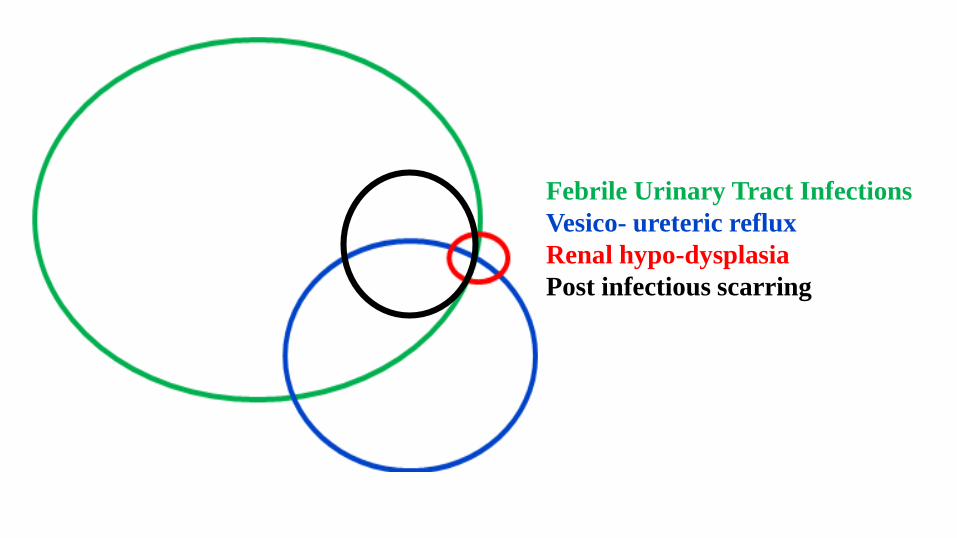
Febrile Urinary Tract Infections
Vesico- ureteric reflux
Renal hypo-dysplasia
Post infectious scarring

Current Understanding of Febrile Urinary Tract Infections and Renal Scarring.
Montini G et al. N Engl J Med 2011;365:239-250