M.Verri U.O. Anestesia e Rianimazione Universitaria Dir.Prof.R.Alvisi.
43
M.Verri U.O. Anestesia e Rianimazione Universit Dir.Prof.R.Alvisi
-
Upload
nunzio-pieri -
Category
Documents
-
view
218 -
download
2
Transcript of M.Verri U.O. Anestesia e Rianimazione Universitaria Dir.Prof.R.Alvisi.

M.VerriU.O. Anestesia e Rianimazione UniversitariaDir.Prof.R.Alvisi

Riconoscimento che qualche cosa non va• alterazione del sensorio• dispnea, tachipnea, alterazione della meccanica-dinamica ventilatoria• SpO2
• alterazione della PA• tachicardia, aritmia• contrazione della diuresi• T°• alterazione degli esami ematochimici• ecc.
• quanto sopra +
• iper-ipotermia / leucocitosi-leucopeniainfezione
Quanto non va ? Valutazione della gravità
• giudizio personale• scale di gravità
sepsi, sepsi grave, shock settico

TachicardiaIpotensione CVP PAOP
Ittero Enzimi Albumina PT
Stato di coscienza alterato, confusione, psicosi
FR > 20 atti/mPaO2 < 70 mm HgSaO2 < 90%PaO2/FiO2 300
Oliguria Anuria Creatinina
Piastrine PT/APTT Proteina C D-dimero
SOFA ?

3 2 1 0 1 2 3PA sist <70 71-80 81-100 101-199 >200FC <40 41-50 51-100 101-110 111-129 >130FR <9 9-14 15-20 21-29 >=30T °C <35 35-38.4 >=38.5AVPU Alert reagisce reagisce Non reagisce
Voce Pain Unresponsive
Modified Early Warning Score
Modified Early Warning Score
Cut-off >4Subbe CP et al Q J Med 2001; 94: 521-526
3 2 1 0 1 2 3SpO2 % <85 85-89 90-94 >=95Diuresi no <0.5 dialisi 0.5-3 >3 ml/Kg/hPA sist <70 70-79 80-99 100-179 >=180FC <40 40-49 50-99 100-114 115-129 >=130FR <10 10-19 20-29 30-39 >=40T °C <35 35-35.9 36.0-37.4 37.5-38.4 >=38.5GCS Alert Confuso reagisce Non reagisce
voce o solo dolore
Goldhill DR et al Anaesthesia 2005; 60: 547-553
Patient-At-Risk warning scorePatient-At-Risk warning score

Score 1 2 3 4
SNCGCS
13-14 10-12 6-9 <6
RESPIRATORIOPa/FiO2 (mmHg)
< 400 < 300 < 200 con supporto
resp
< 100
CARDIOVASCOLAREIpotensione
MAP < 70 mmHg
Dopa < 5 o DObutamin
a
Dopa > 5 oAdr < 0,1 o
Noradr < 0,1
Dopa > 15Adr > 0,1
Noradr > 0,1
COAGULAZIONEPiastrine(103/mm3)
< 150 <100 <50 <20
FEGATOBilirubina(mg/dl)
1,2-1,9 2,0-5,9 6,0-11,9 >12
RENALECreat (mg/dl) o Diur
1,2-1,9 2,0-3,4 3,5-4,9 o< 500
ml/24h
> 5,0< 200 ml/24 h
Sequential Organ Failure Assessment (SOFA)
Vincent JL, et al. Intensive Care Med 1996;22:707-10

S.C 37 aa
insuff.respiratoria
cardiopatia


• microbiologia• antibioticoterapia• rimozione sorgente
Ottimizzazione perfusione• volemia
• cristalloidi• colloidi• emocomponenti• emoderivati
• tono vascolare• vasocostrittori• vasodilatatori ??
• contrattilità miocardica• dobutamina• (dopamina)
• supporto respiratorio• sostituz.funzione renale• controllo glicemico• nutrizione• sedazione•prevenzione complicanze• ecc.
steroidi ?
Coupled Plasma Filtration AdsorptionCPFA
sono guarito !!!
ECMO

Special admission paths: sepsis R Ferrer, A.Navas, ML Martinez, A.Artigas
• Barochia AV, Cui X, Vitberg D, Suffredini AF, O’Grady NP, Banks SM. Bundled care for septic shock: an analysis of clinical trial. Crit Care Med 2010; 38(2).668-78• Ferrer R, Artigas A, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med 2009; 180(9):861-6• Levy MM, Dellinger RP, Bion J. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med 2010;36(2):222-31
• The key to success involves the implementation of a hospital wide system that recognizes septic patients early, and at the same time rapidly administers effective therapy ( sepsis-rapid response team)(?)
• The results of the meta-analysis are very consistent in showing that sepsis bundles improve survival by improving the way sepsis treatments are delivered
• Health care organizations traditionally favour investing in new technology and drugs, but are reluctant to invest in organizational development. For sepsis care bundles to succeed, this must change

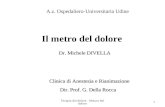
Sepsis is very complex!
Infectious agent?
Pro inflammatorymediator
earlyinhibitors
Receptor activation
Other factors?
Pro- inflammatorymediators
Signal pathway activation
Anti- inflammatorymediators
inhibitors Protein synthesis
Coagulation cascade
Inflammatory cascade
ROS
Da EMC 2010

Immunoinflammatory response of three hypothetical patients with sepsis.

• microbiologia• antibioticoterapia• rimozione sorgente
Ottimizzazione perfusione• volemia
• cristalloidi• colloidi• emocomponenti• emoderivati
• tono vascolare• vasocostrittori• vasodilatatori ??
• contrattilità miocardica• dobutamina• (dopamina)
• supporto respiratorio• sostituz.funzione renale• controllo glicemico• nutrizione• sedazione•prevenzione complicanze• ecc.
steroidi ?
Coupled Plasma Filtration AdsorptionCPFA
ECMO






Cardiac conditions considered to increase a patient’s risk of developing infective endocarditis, i.e. ‘at risk’ heart valve lesions.

The endocarditis risk in GUCH patients is substantially higher than in the general population, with marked variation between lesions.
It has to be emphasized that good oral hygiene and regular dental review have an essential role in reducing the risk of IE. Aseptic measures are mandatory during manipulation of venous catheters and during any invasive procedure in order to reduce the rate of healthcare-associated IE. GUCH patients should also be discouraged from getting piercings and tattoos.

The approach to antibiotic endocarditis prophylaxis has changed for several reasons.In short, transient bacteraemia occurs not only after dental procedures but frequently in the context of daily routine activities such as tooth brushing, flossing, or chewing.Due to the lack of scientific evidence for the efficacy of antibiotic prophylaxis, the estimated huge number of patients that may need to be treated to prevent one single case of IE, the small but existing risk of anaphylaxis, and the general problem of emergence of resistant microorganisms resulting from widespread, often inappropriate use of antibiotics, it is currently recommended by expert consensus to limit antibiotic prophylaxis to patients with the highest risk of IE undergoing the highest risk procedures (IIaC).

This recommendation includes the following patient groups:• Patients with a prosthetic valve or a prosthetic material used for cardiac valve repair• Patients with previous IE• Patients with CHD:
• a cyanotic CHD, without surgical repair, or with residual defects, palliative shunts, or conduits • a CHD after repair with prosthetic material whether placed by surgery or by percutaneous technique, up to 6 months after the procedure (until endothelialization)• a when a residual defect persists at the site of implantation of a prosthetic material or device by cardiac surgery or percutaneous technique.
The recommendation is limited to dental procedures requiring manipulation of the gingival or periapical region of the teeth or perforation of the oral mucosa. Antibiotics are not recommended for respiratory tract, gastrointestinal, genitourinary, dermatological, or musculoskeletal procedures unless there is an established infection.






Steroids◦ Consider intravenous hydrocortisone for adult septic shock when
hypotension remains poorly responsive to adequate fluid resuscitation and vasopressors. (2C)
◦ ACTH stimulation test is not recommended to identify the subset of adults with septic shock who should receive hydrocortisone. (2B)
◦ Hydrocortisone is preferred to dexamethasone. (2B)◦ Fludrocortisone (50μg orally once a day) may be included if an
alternative to hydrocortisone is being used which lacks significant mineralocorticoid activity. Fludrocortisone is optional if hydrocortisone is used. (2C)
◦ Steroid therapy may be weaned once vasopressors are no longer required. (2D)
• Hydrocortisone dose should be ≤300 mg/day. (1A)• Do not use corticosteroids to treat sepsis in the absence of shock
unless the patient’s endocrine or corticosteroid history warrants it. (1D)

Steroids
Negli ultimi anni l’uso dei corticosteroidi nello shock settico è risultato controverso
• Pro:– miglioramento emodinamico con più rapida sospensione dei vasopressori– > rapidità di risoluzione della disfunzione d’organo– < mortalità (?)
• Con:– mortalità tra responder e non responder– = rapidità nella sospensione dei vasopressori– > superinfezioni– debolezza neuromuscolare– intolleranza glucidica
Nov.2008

• Annane D, et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA 2002;288:862-870– Sì steroidi nello shock settico che
richiede vasopressori
• SprungCL, et al. The CORTICUS randomized, double-blind, placebo-controlled study of hydrocortisone therapy in patients with septic shock. N Engl J Med 2008;358:111-124– NO steroidi nello shock settico
Steroids

SteroidsRecommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American College of Critical Care Medicine
Crit Care Med 2008; 36:1937–1949
Recommendation 6:Hydrocortisone should be considered in the management strategy of patients with septic shock, particularly those patients who have responded poorly to fluid resuscitation and vasopressor agents.
Strength of Recommendations: 2B

Corticosteroids in the Treatment of Severe Sepsis and Septic Shock in Adults
Annane D, Bellissant E, Bollaert PE, et al. JAMA. 2009; 301:2362-2375
28-day mortality was modestly reduced (relative risk [RR] = 0.84, P = .05) and was also modestly reduced in the subset of studies reporting prolonged corticosteroid administration (RR = 0.84, P = .02). Treatment increased the proportion of patients achieving reversal of shock and reduced the length of intensive care unit stay without a detectable increase in gastrointestinal bleeding, superinfection, or neuromuscular complications. Corticosteroids did increase the risk for hyperglycemia and hypernatremia. The authors concluded that the prolonged use of corticosteroids safely reduces short-term mortality in patients with severe sepsis or septic shock.
Until a definitive clinical trial answers this question, corticosteroid use will continue to be highly variable and at the discretion of intensivists worldwide

Conclusions: Based on clinically meaningful thresholds (RRR[15–25%) for mortality reduction in severe sepsis or septic shock, the Bayesian approach to all three meta-analyses consistently showed that low-dose steroids were not associated with survival benefits. The probabilities of developing steroid- induced side effects (superinfections, bleeding, and hyperglycemia) were high for all analyses.

ConclusionPatients randomized to treatment with hydrocortisone demonstrated a faster decrease in total organ dysfunction/failure determined by the SOFA score, primarily driven by a faster improvement in cardiovascular organ dysfunction/failure.This organ dysfunction/failure improvement was not accompanied by a decreased mortality.
R. MorenoC. L. SprungD. AnnaneS. ChevretJ. BriegelD. KehM. SingerY. G. WeissD. PayenB. H. CuthbertsonJ.-L. Vincent

Ideal therapy for sepsis
Plasma
Reinfusate in
UF out
“bad molecules”
“good molecules”
SIRS = Systemic inflammatory response syndrome
CARS = Compensatory anti-inflammatoryresponse syndrome
Hyper-inflammation
Normal
Immunoparalysis

CPFA used successfully in non-ARF patients
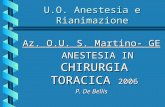
Hemodynamic response to coupled plasmafiltration-adsorption in human septic shock
Marco Formica, Carlo Olivieri, Sergio Livigni, Giulio Cesano, Antonella Vallero, Mariella Maio and Ciro Tetta
Intensive Care Med (2003) 29: 703-708
Objective: The objective was to examine the effect of repeated applications of coupled plasmafiltration-adsorption on the hemodynamic response in septic shock patients hospitalized in intensive care units (ICUs).
Conclusion: Coupled plasmafiltration-adsorption was a feasible and safe extracorporeal treatment and exerted a remarkable improvement in the hemodynamics, the pulmonary function, and the outcome in septic shock patients with or without concomitant ARF.

Anne-Corne´lie J. M. de Pont, MD, PhD Adult Intensive Care Unit Academic Medical Center University of Amsterdam Amsterdam, The Netherlands
…The improvement of blood purification techniques and membranes has generated new opportunities for the use of extracorporeal techniques in sepsis. Removal of both pro- and anti-inflammatory mediators by means of these new techniques is feasible and might add to the restoration of homeostasis by controlling excessive cytokine production (the so-called peak concentration hypothesis). Whether this approach will result in a better clinical outcome for patients with severe sepsis remains to be investigated.





• microbiologia• antibioticoterapia• rimozione sorgente
Ottimizzazione perfusione• volemia
• cristalloidi• colloidi• emocomponenti• emoderivati
• tono vascolare• vasocostrittori
• contrattilità miocardica• dobutamina
• supporto respiratorio• sostituz.funzione renale• controllo glicemico• nutrizione• sedazione•prevenzione complicanze• ecc.
steroidi ?
proteina C attivataricombinante ?(Drotrecogin)
sono guarito !!!

Da Intensive Care Med 2010;36(12): 2019-2029

Indications for echocardiography in suspected infective endocarditis. IE, infective endocarditis; TTE, transthoracic echocardiography; TOE, transoesophageal echocardiography. TOE is not mandatory in isolated right-sided native valve IE with good quality TTE examination and unequivocal echocardiographic findings.