MODULO 3 Lezione 1 DIAGNOSTICA DELLA RETINA · MODULO 3 | Lezione 1 DIAGNOSTICA DELLA RETINA...
43
MODULO 3 | Lezione 1 DIAGNOSTICA DELLA RETINA Giovanni Staurenghi, Alessandro Invernizzi, Marco Pellegrini Clinica Oculistica Ospedale Sacco Dipartimento di Scienze Biomediche e Cliniche “Luigi Sacco” Università degli Studi di Milano ARGOMENTI DI QUESTA LEZIONE : Retinografia Infrarosso Autofluorescenza del fondo oculare Angiografia con indocianina verde Tomografia ottica a coerenza - OCT
Transcript of MODULO 3 Lezione 1 DIAGNOSTICA DELLA RETINA · MODULO 3 | Lezione 1 DIAGNOSTICA DELLA RETINA...
MODULO 3 | Lezione 1 DIAGNOSTICA DELLA RETINAGiovanni Staurenghi, Alessandro Invernizzi, Marco Pellegrini Clinica Oculistica Ospedale SaccoDipartimento di Scienze Biomediche e Cliniche “Luigi Sacco” Università degli Studi di Milano
ARGOMENTI DI QUESTA LEZIONE :
Retinografia Infrarosso Autofluorescenza del fondo oculare Angiografia con indocianina verde Tomografia ottica a coerenza - OCT
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Heidelberg Engineering1,2, OD-OS1,2, Optos1,2, Ocular Instruments4, Quantel Medical1,2, Carl Zeiss
Meditec1, Alcon1,3, Allergan1,3, Bayer1,3, Boheringer1, Genentech1, GSK1,3, QLT1, Novartis1,3,
Roche1,3
Conflitti di interesse:
1 consulente, 2 finanziamenti per ricerca, 3 rimborsi per letture, 4 brevetti
ACCURATA DIAGNOSI
TERAPIA MIRATA
MIGLIORI RISULTATI, MAGGIORE COMPLIANCE DEL PAZIENTE , NOTEVOLE
RISPARMIO ECONOMICO
A seguire una flow-chart che indica le più appropriate strategie diagnostiche secondo le varie tipologie di paziente
LE TECNICHE DI IMAGING: APPROPRIATEZZA D’USO
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
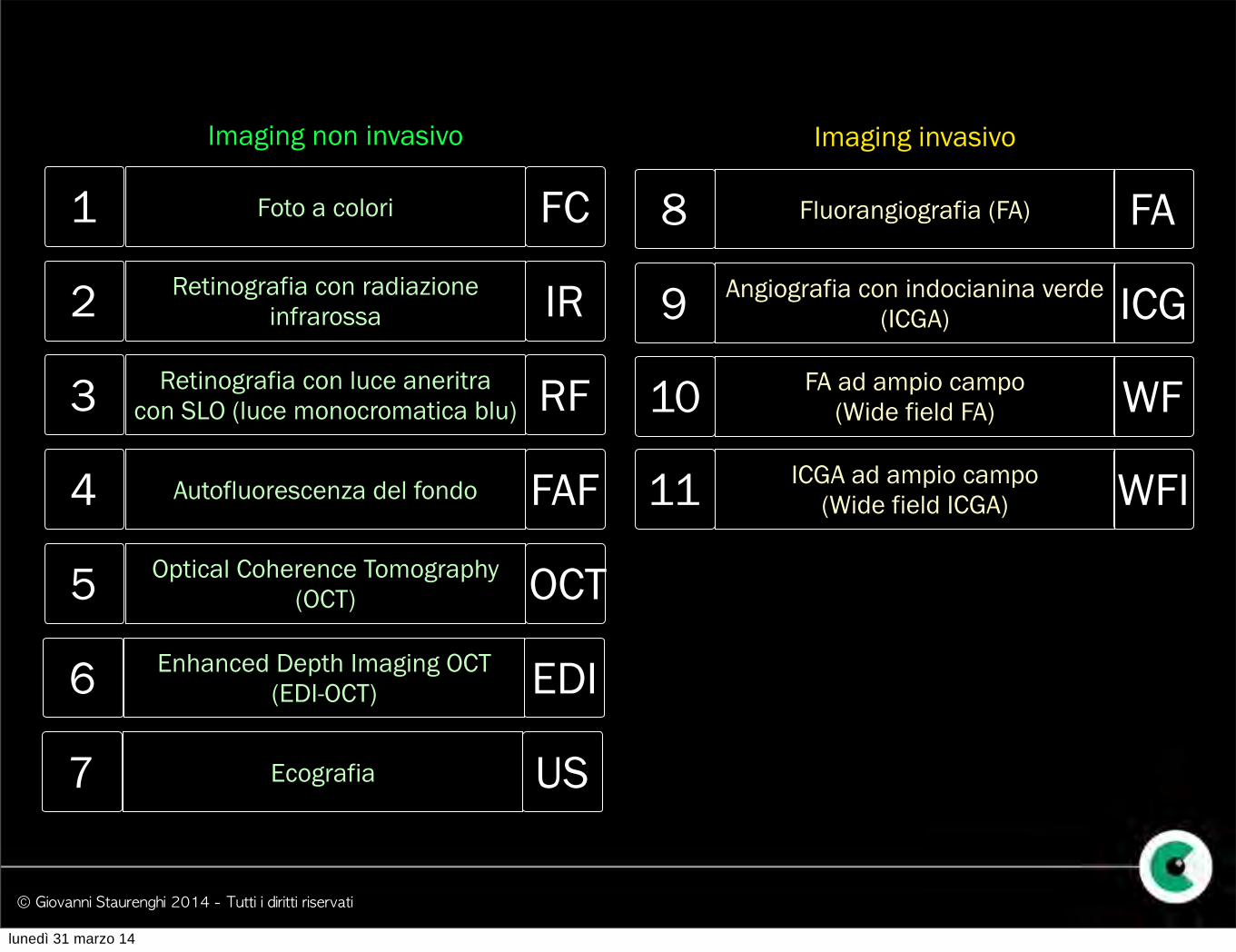
Optical Coherence Tomography (OCT)
Retinografia con radiazione infrarossa
Autofluorescenza del fondo
Fluorangiografia (FA)
Angiografia con indocianina verde (ICGA)
Retinografia con luce aneritra con SLO (luce monocromatica blu)
Imaging non invasivo Imaging invasivo
1
2
3
4
8
9FA ad ampio campo
(Wide field FA)10ICGA ad ampio campo
(Wide field ICGA)11
Foto a colori
5Enhanced Depth Imaging OCT
(EDI-OCT) 6
Ecografia7
FC
IR
RF
FAF
OCT
EDI
US
FA
ICG
WF
WFI
lunedì 31 marzo 14
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
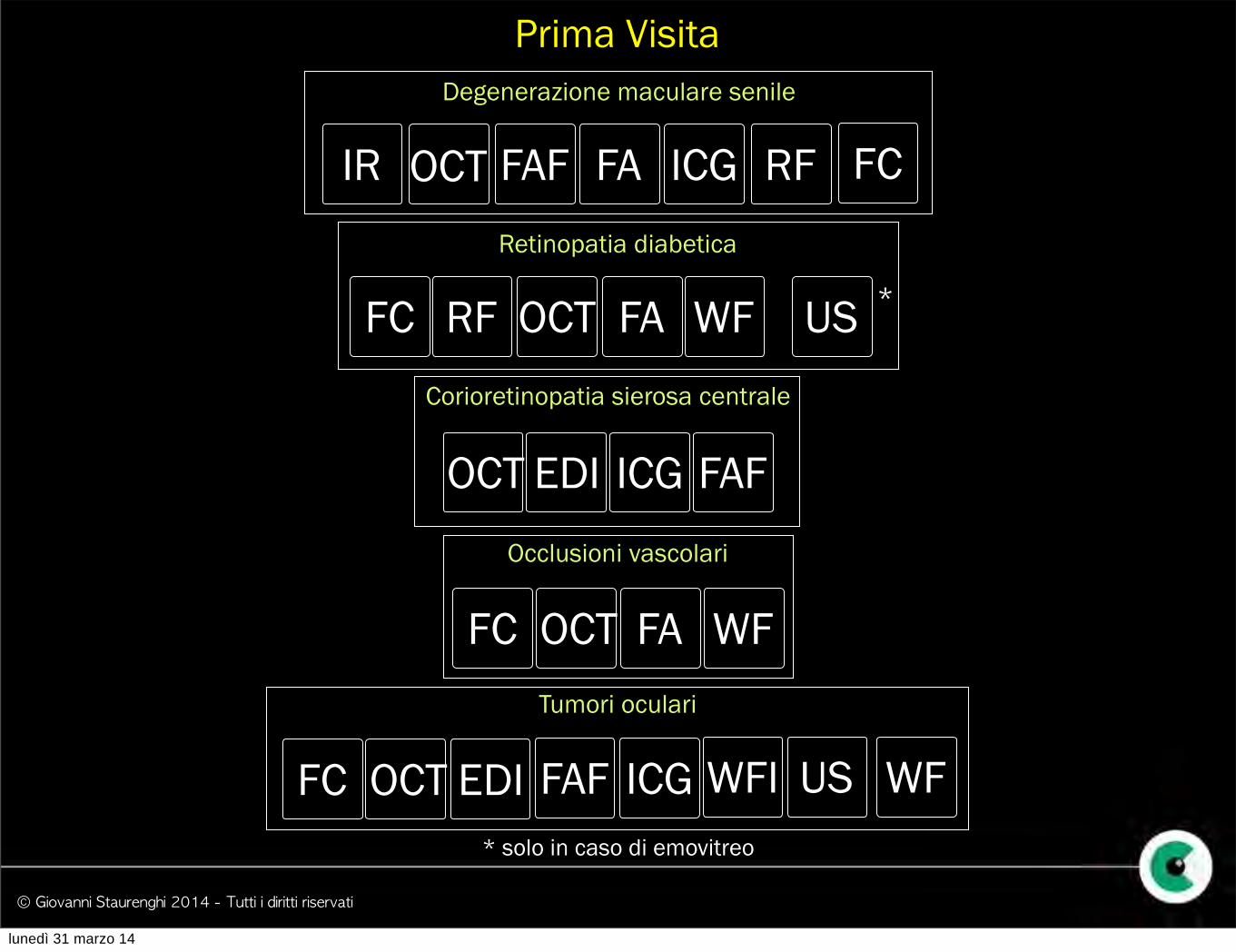
* solo in caso di emovitreo
Degenerazione maculare senile
OCT FAF FA ICG RFIRRetinopatia diabetica
RFFC FA WFOCT US *
Corioretinopatia sierosa centrale
OCT EDI ICG FAFOcclusioni vascolari
FC OCT FA WF
Prima Visita
FC
Tumori oculari
FC OCT EDI ICG WFI US WFFAF
lunedì 31 marzo 14
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
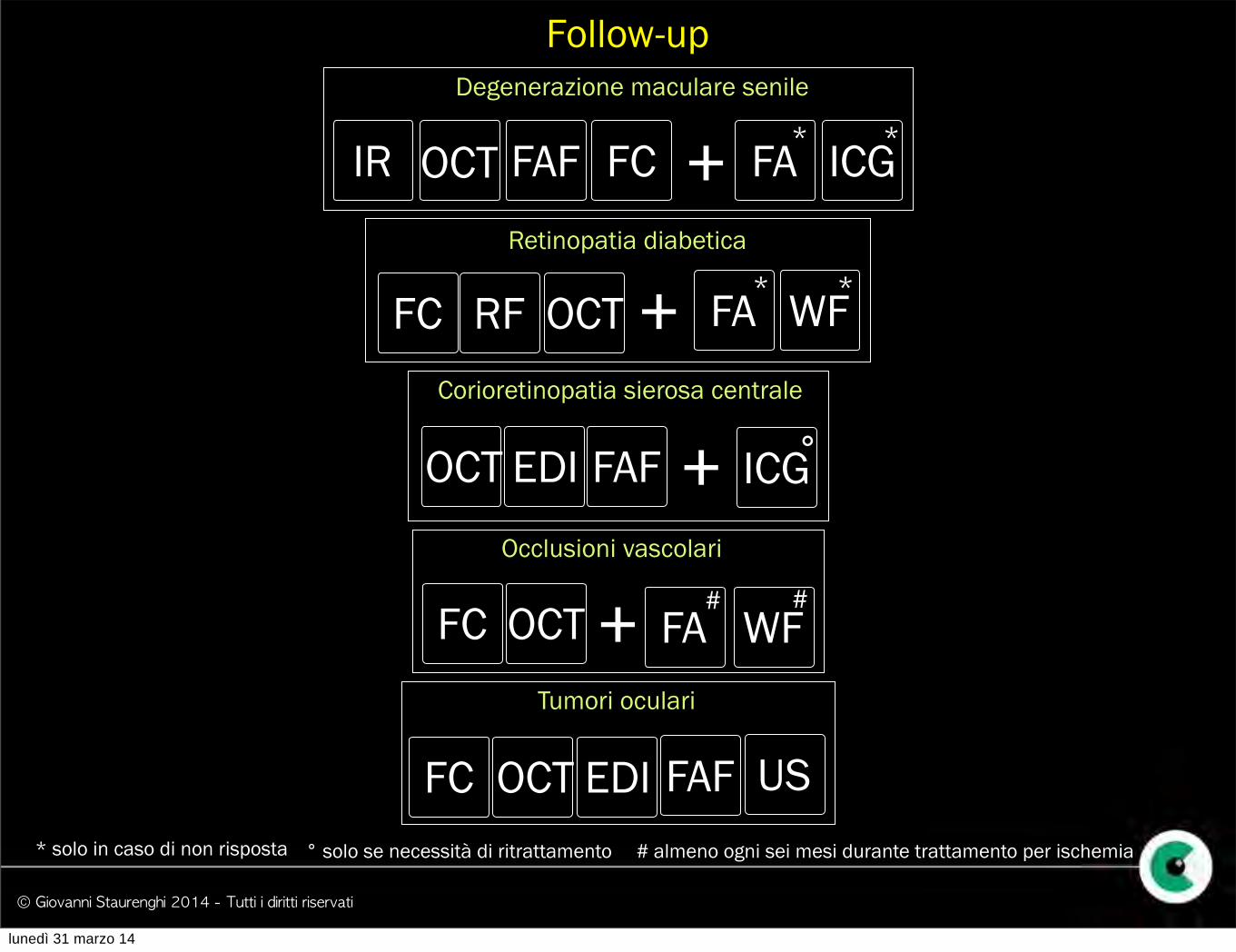
OCT
Follow-up
FA ICG
Degenerazione maculare senile
OCT FAFIR FC + * *
Retinopatia diabetica
RFFC WFOCT**
FA+Corioretinopatia sierosa centrale
OCT EDI FAF ICG°+
* solo in caso di non risposta ° solo se necessità di ritrattamento # almeno ogni sei mesi durante trattamento per ischemia
Occlusioni vascolari
FC OCT FA WF# #+
Tumori oculari
FC OCT EDI USFAF
lunedì 31 marzo 14

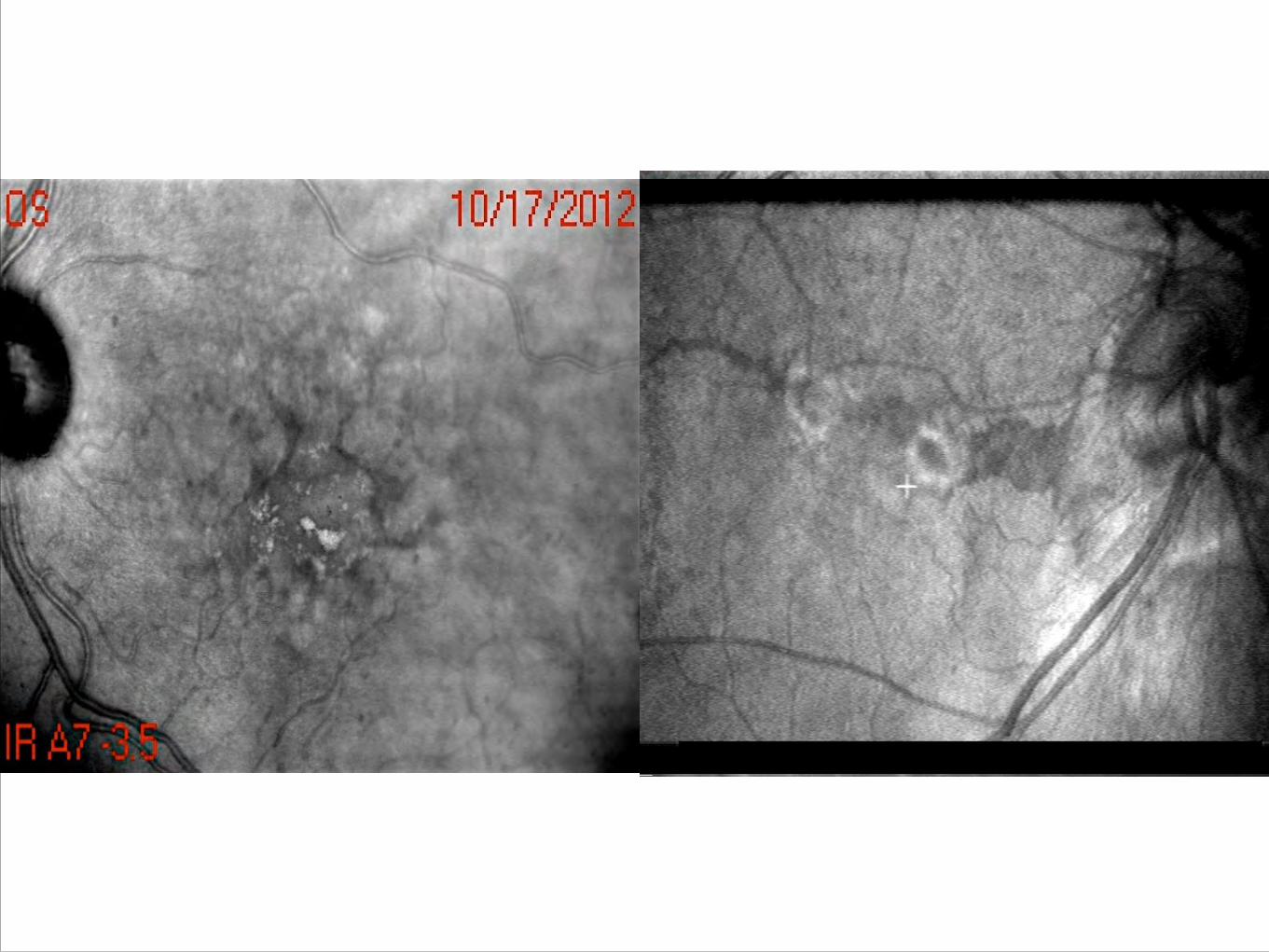
Retinografia Infrarosso
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
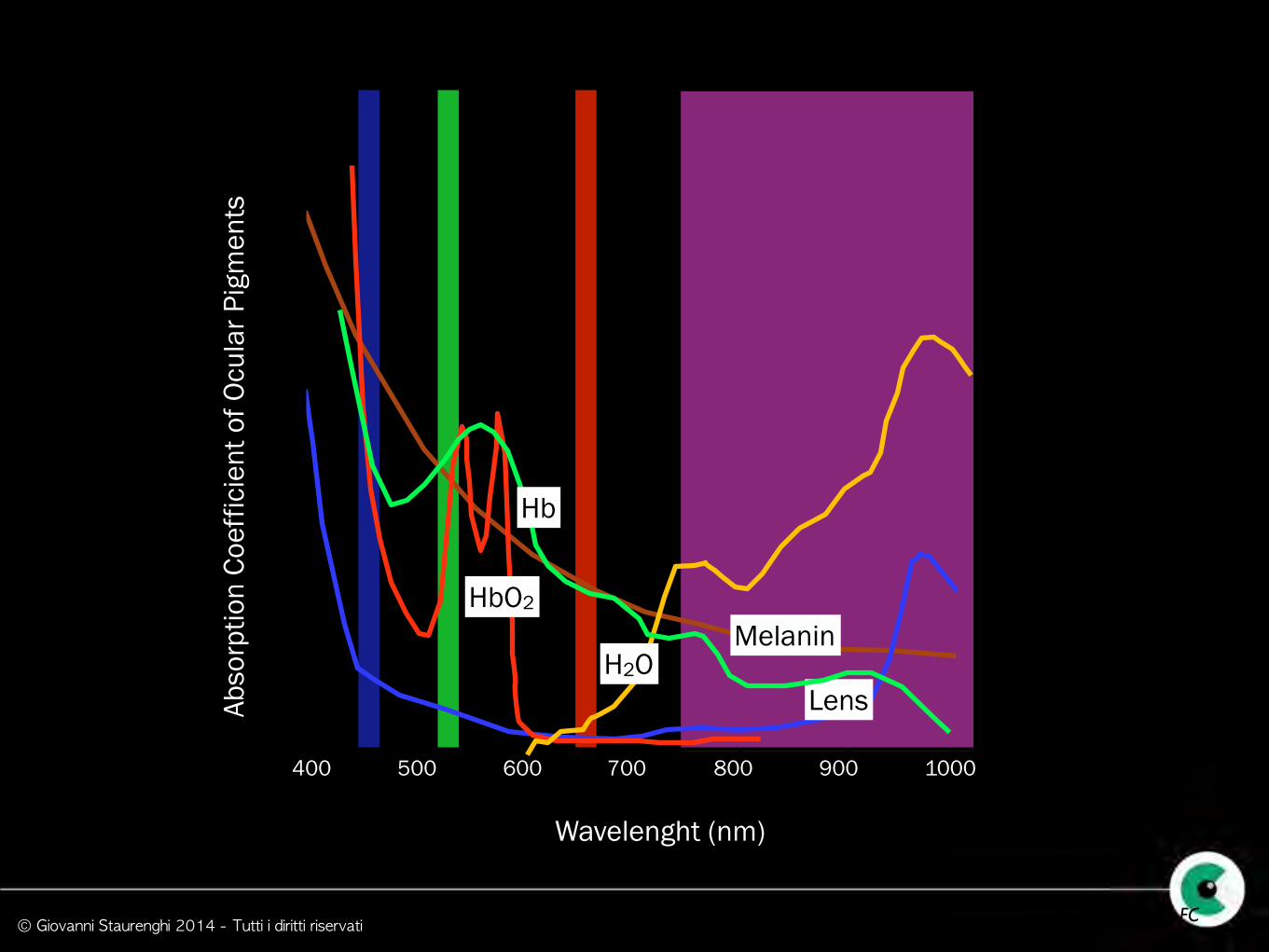
400 500 700 800 900 1000600
Lens
Wavelenght (nm)
Abso
rptio
n Co
effic
ient
of O
cula
r Pig
men
ts
H2O
HbO2
modified from Delori FC
Melanin
Hb
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Metodi e strumenti

© Giovanni Staurenghi 2014 - Tutti i diritti riservati
HRA Spectralis Nidek F10 Optos
Zeiss Cirrus
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
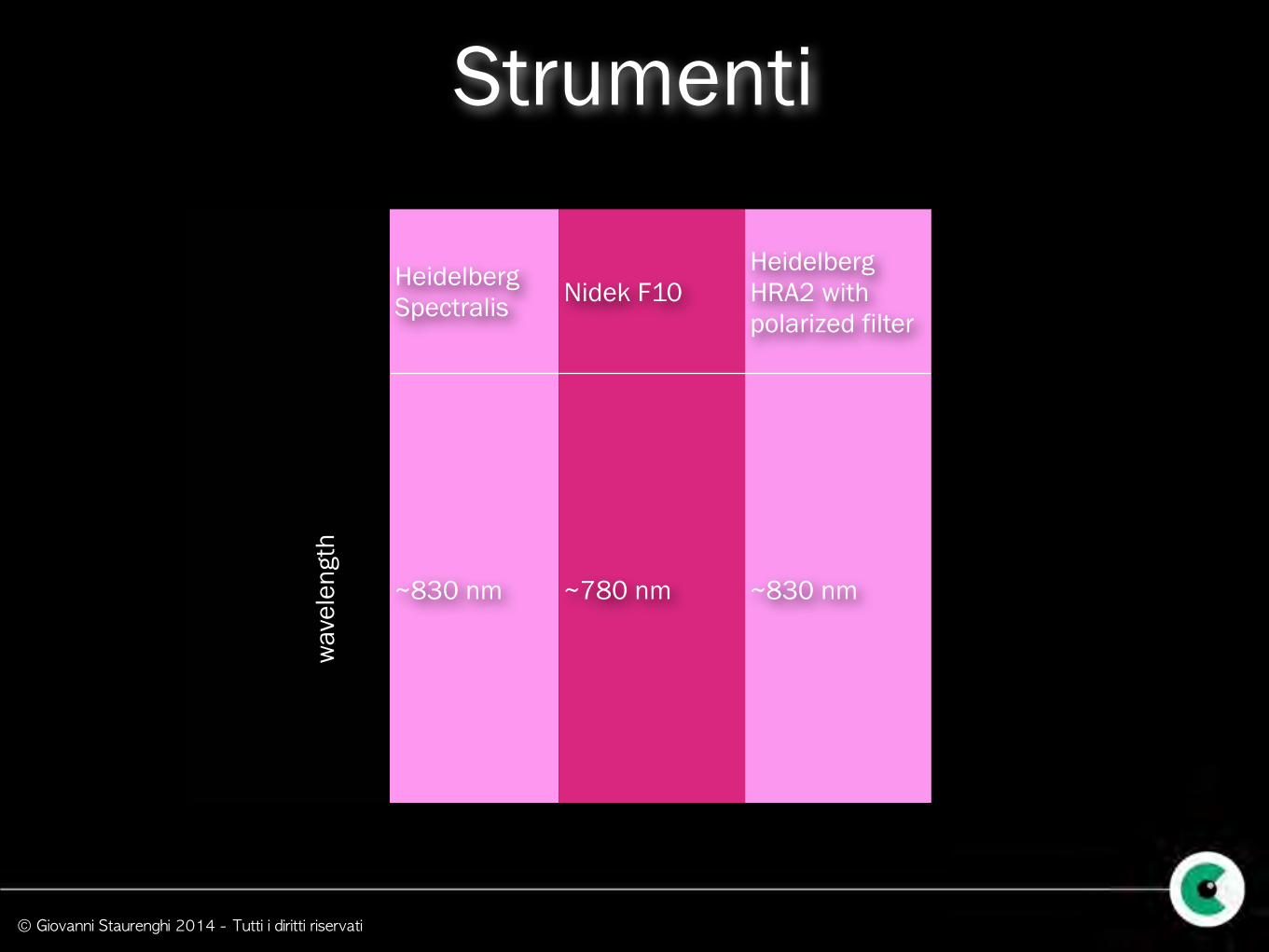
Strumenti
Heidelberg Spectralis Nidek F10
Heidelberg HRA2 with polarized filter
~830 nm ~780 nm ~830 nm
wav
elen
gth
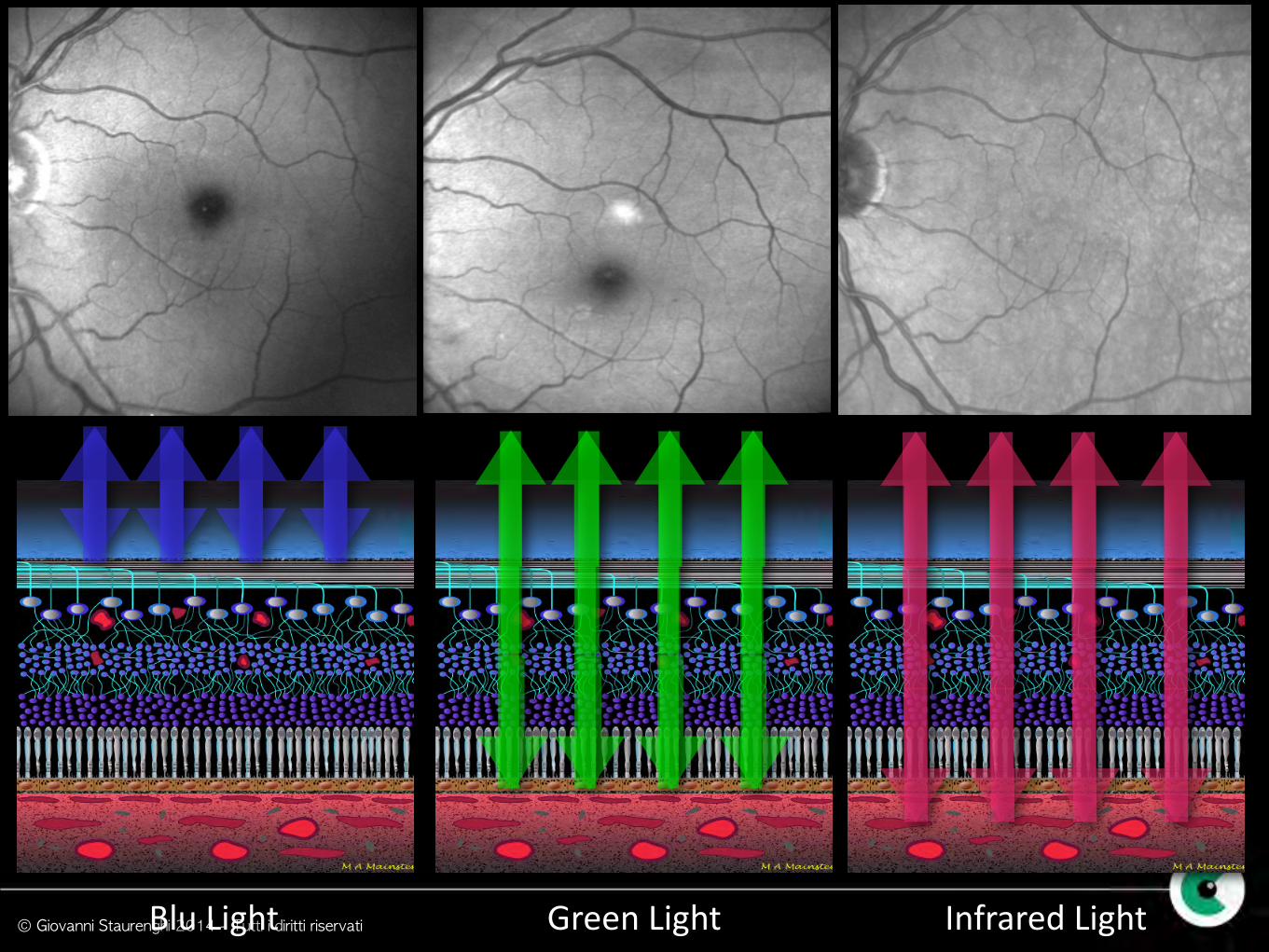
© Giovanni Staurenghi 2014 - Tutti i diritti riservatiBlu Light Green Light Infrared Light
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
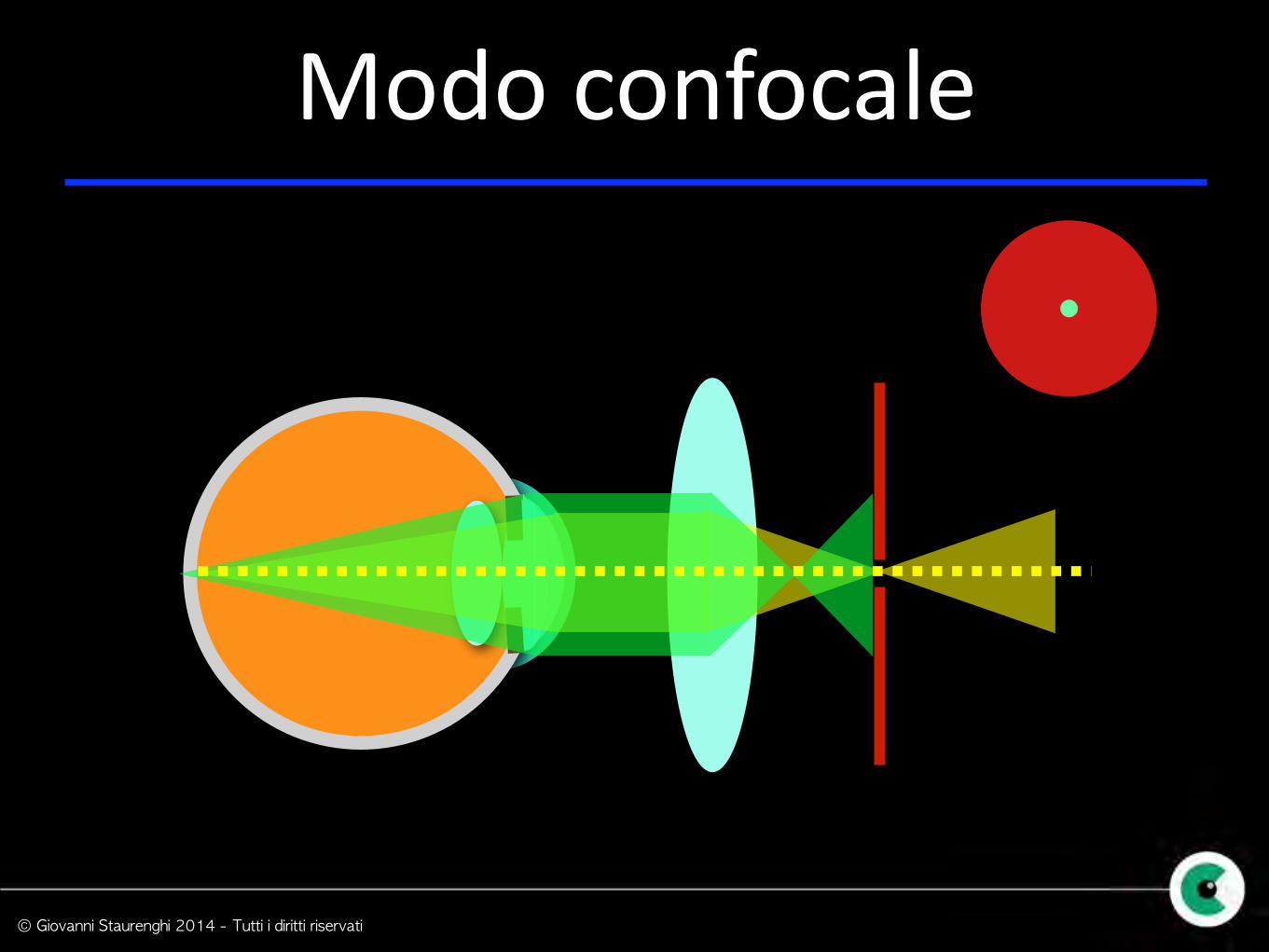
Modo confocale
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
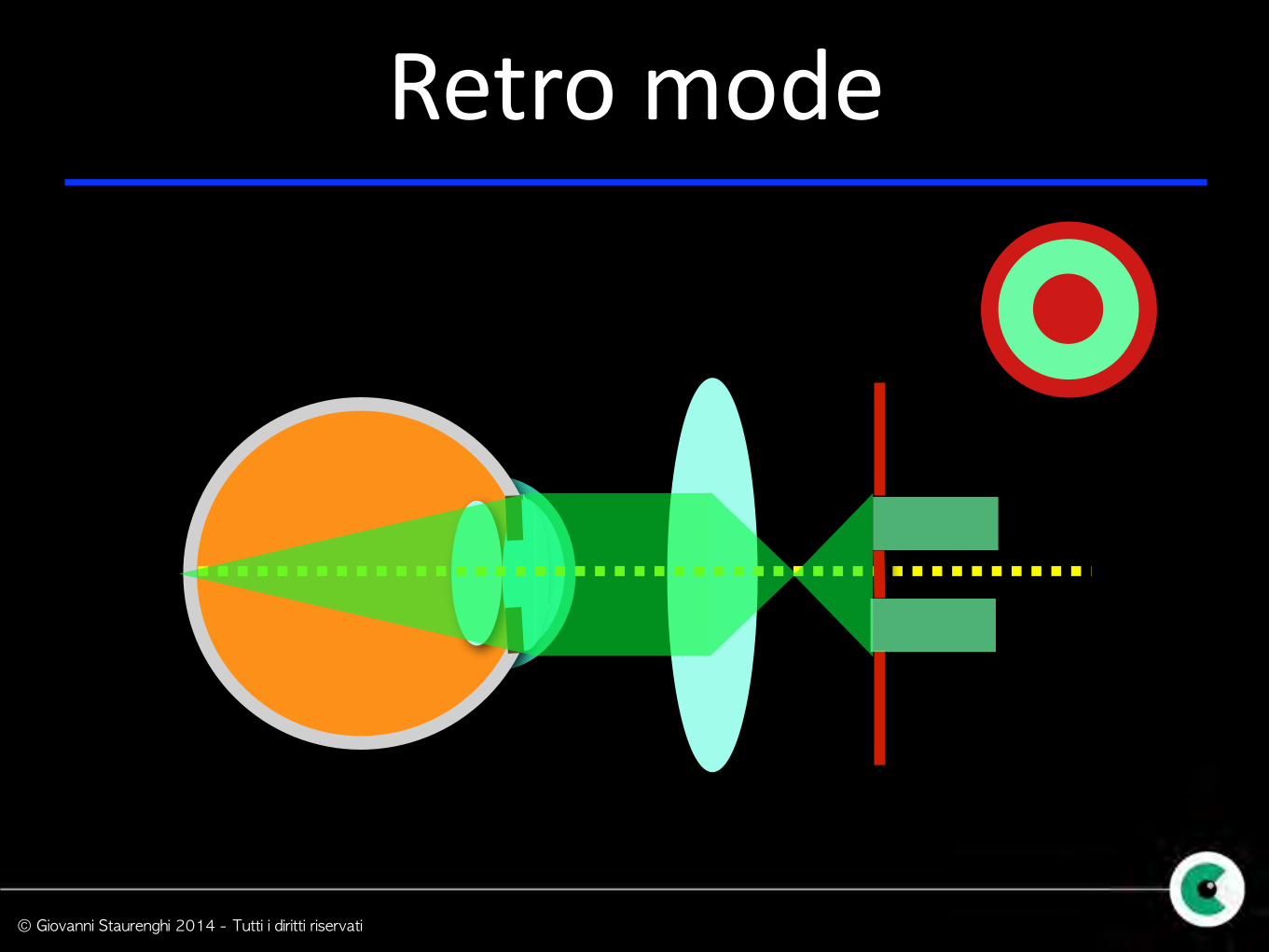
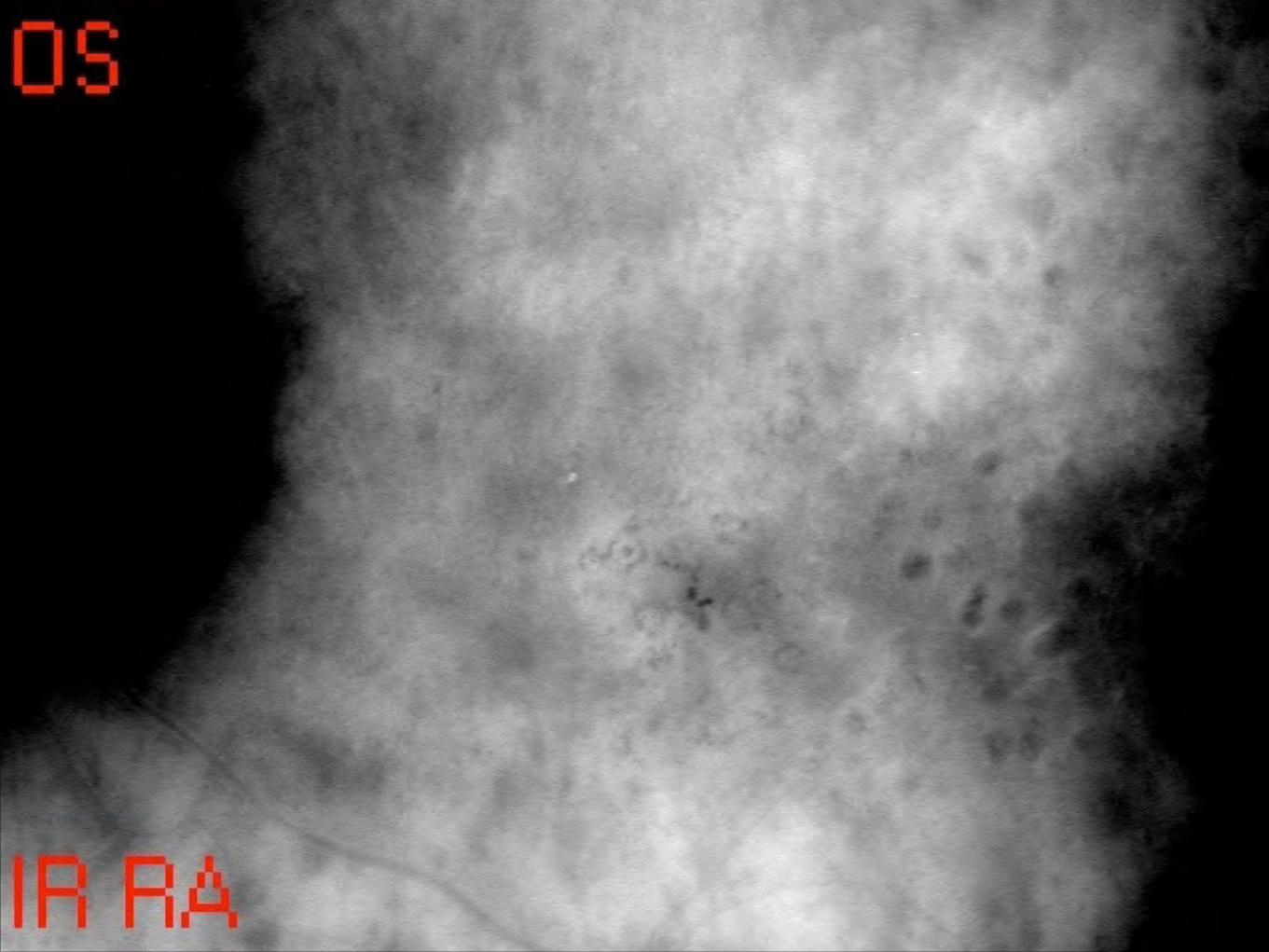
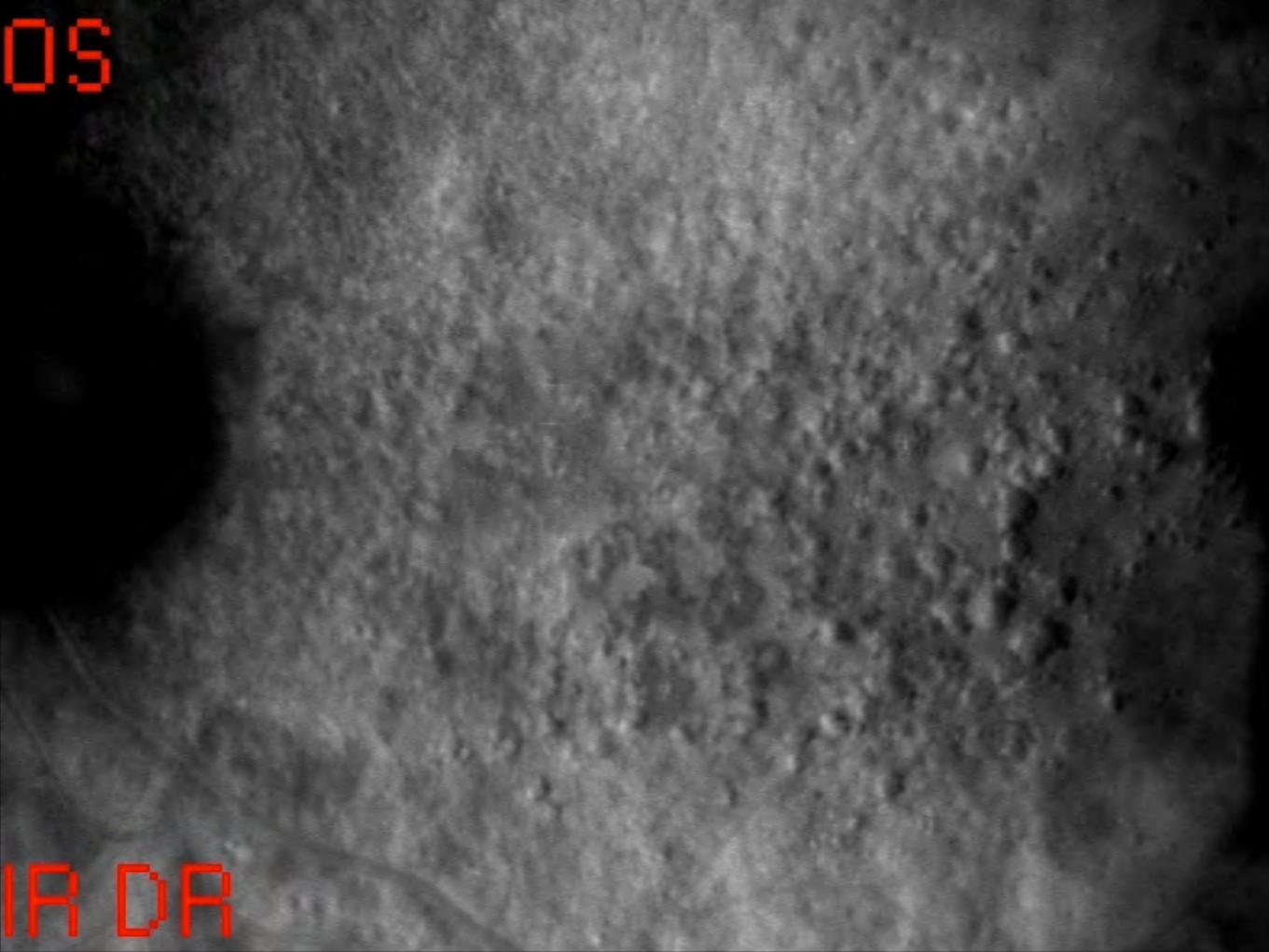
Retro mode
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
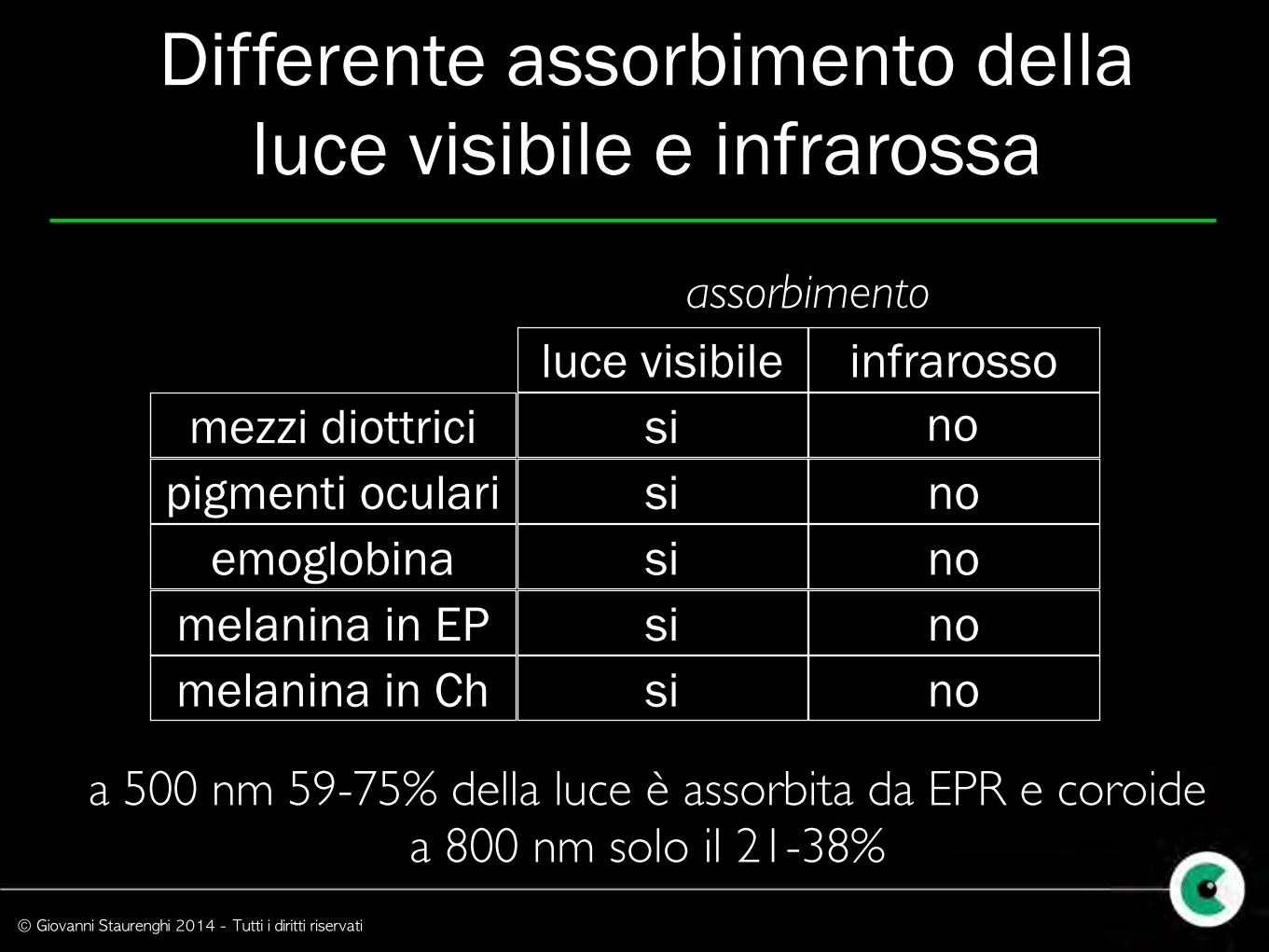
luce visibilemezzi diottrici
pigmenti oculariemoglobina
melanina in EPmelanina in Ch
infrarossosi
sisi
sisi
nonono
no
assorbimento
a 500 nm 59-75% della luce è assorbita da EPR e coroide a 800 nm solo il 21-38%
Differente assorbimento della luce visibile e infrarossa
no
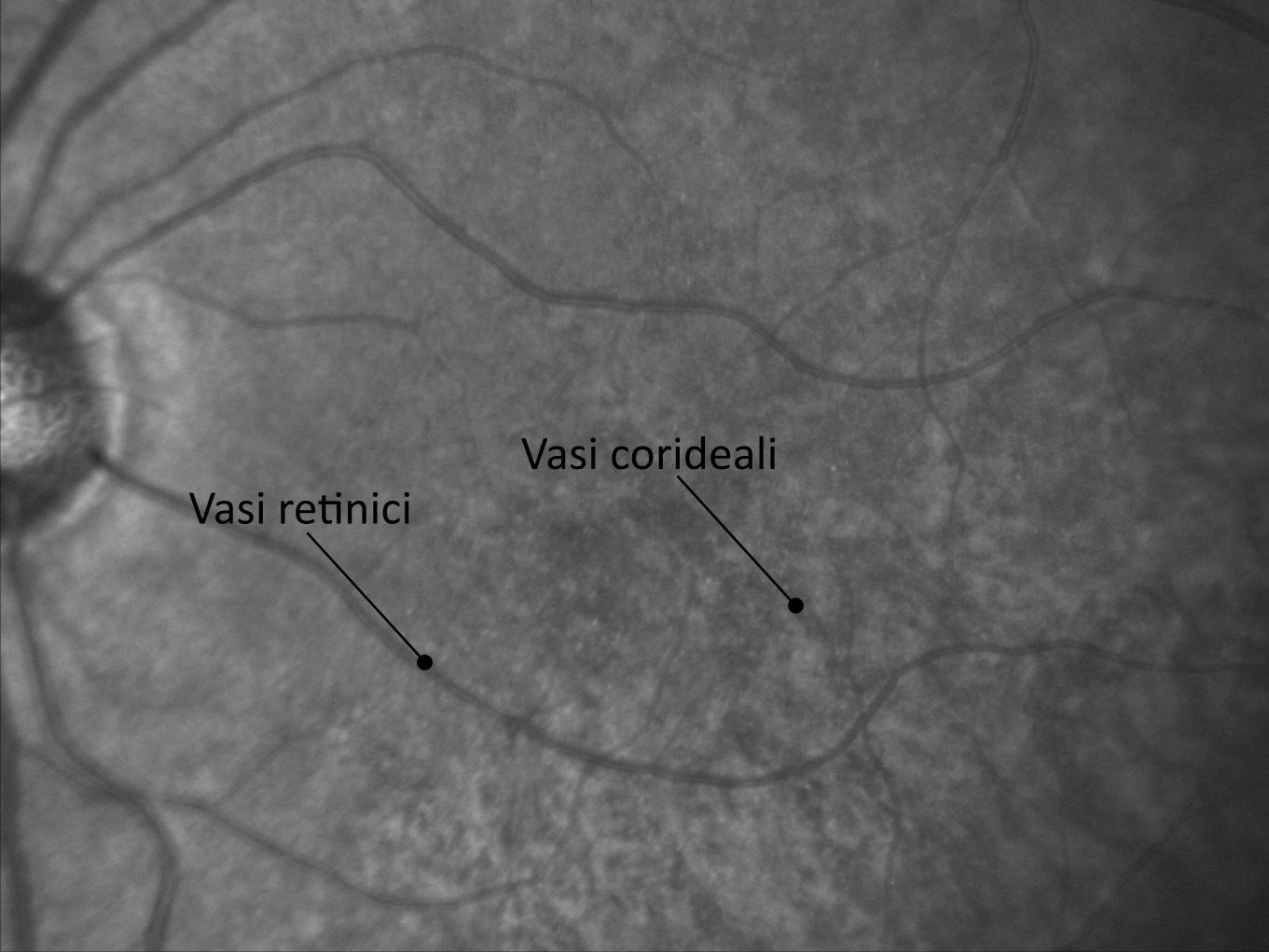
Vasi re9niciVasi corideali
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
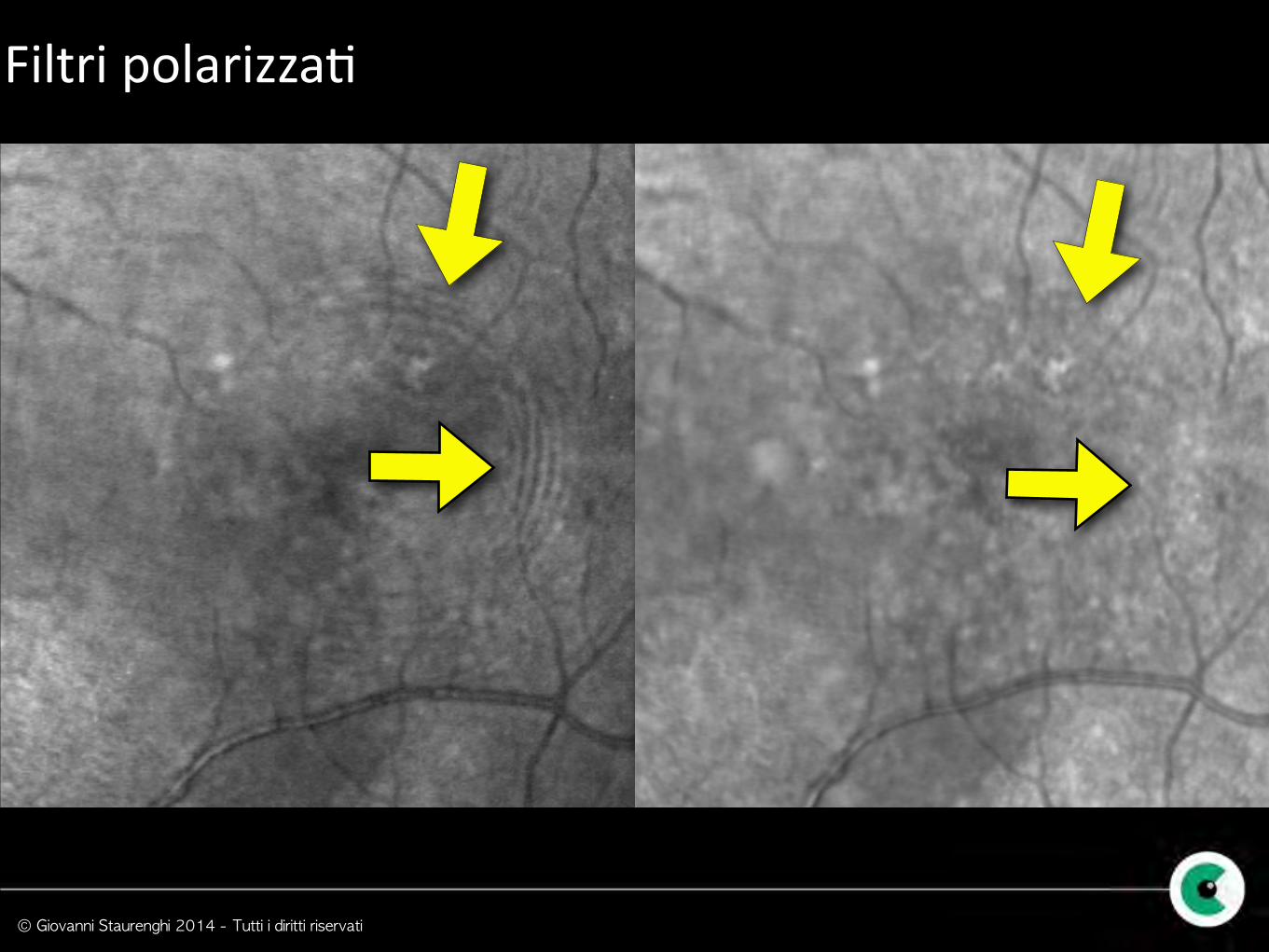
Filtri polarizza9

© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Visulizzazione di liquido intrare9nico
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
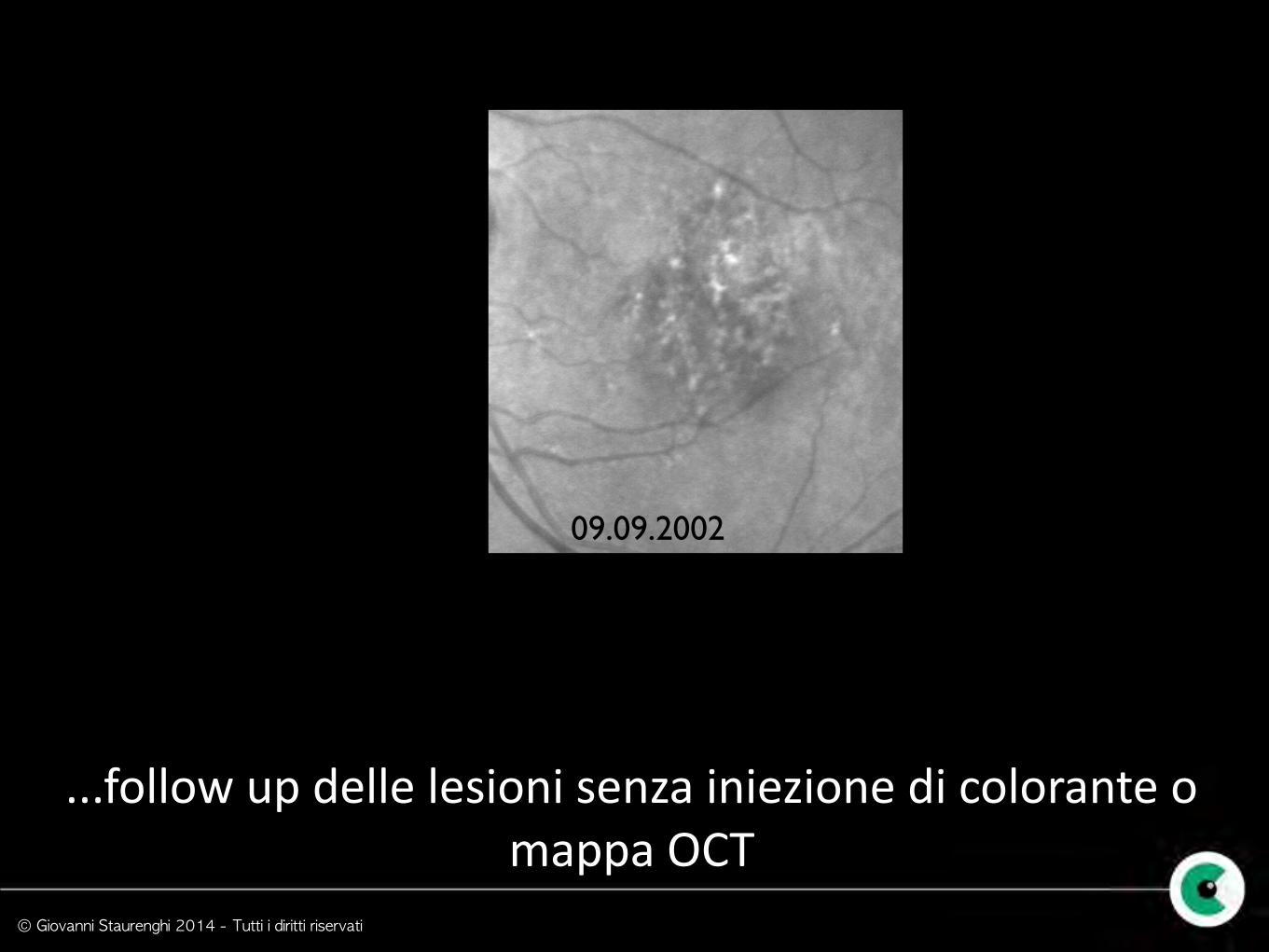
02.09.200110.10.200121.11.200115.01.200218.03.200209.09.2002
...follow up delle lesioni senza iniezione di colorante o mappa OCT
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Drusen
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
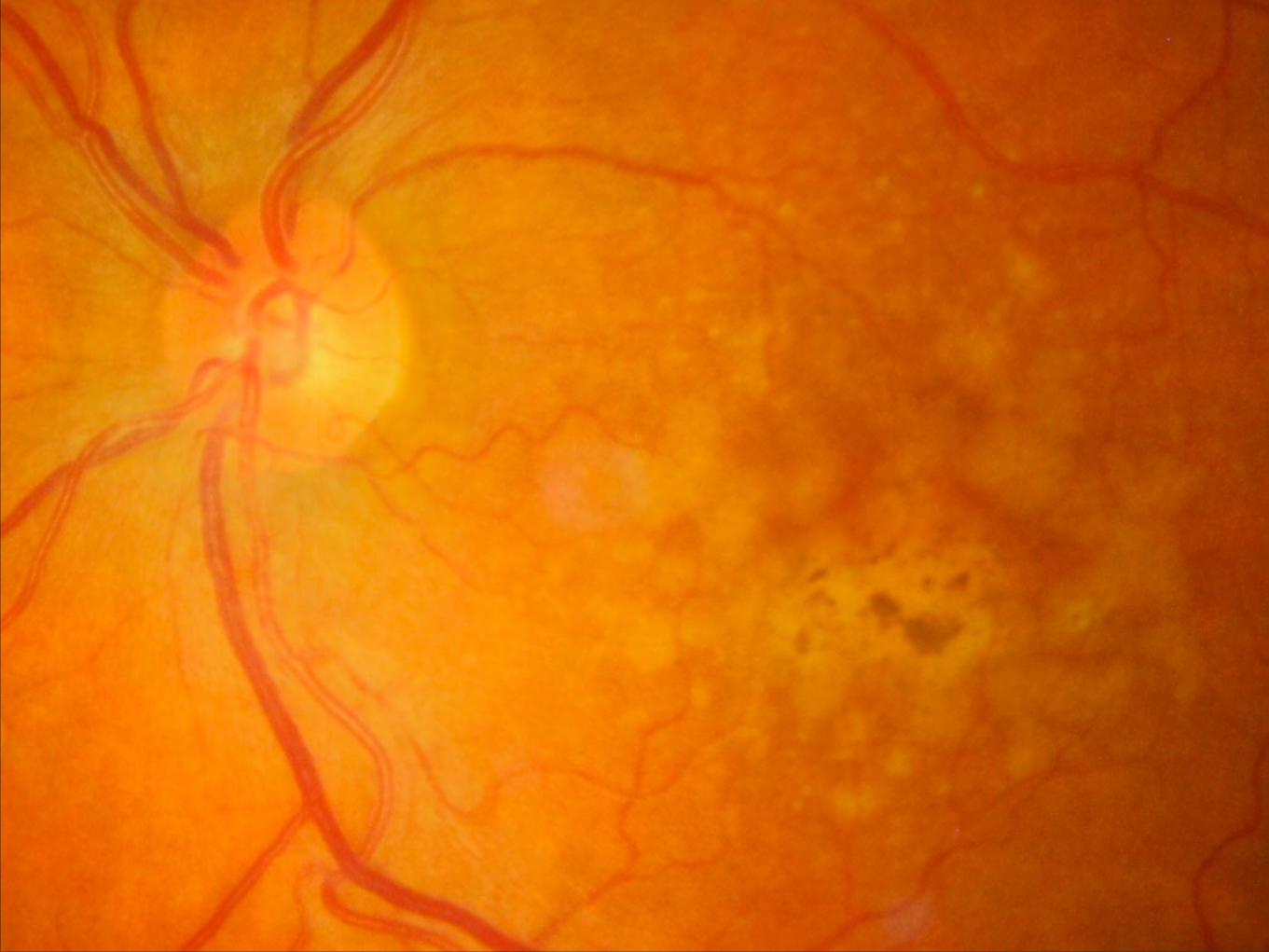
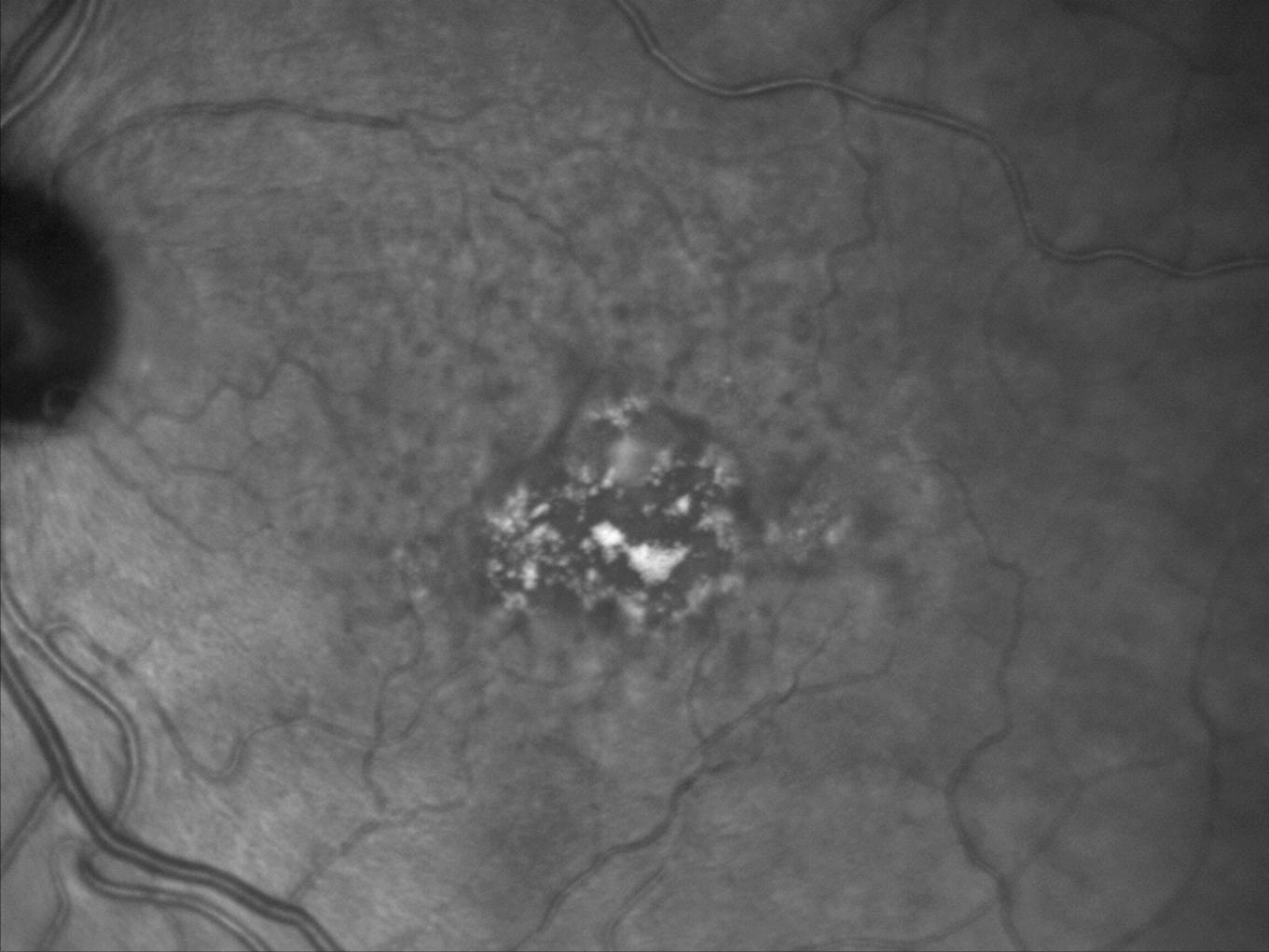
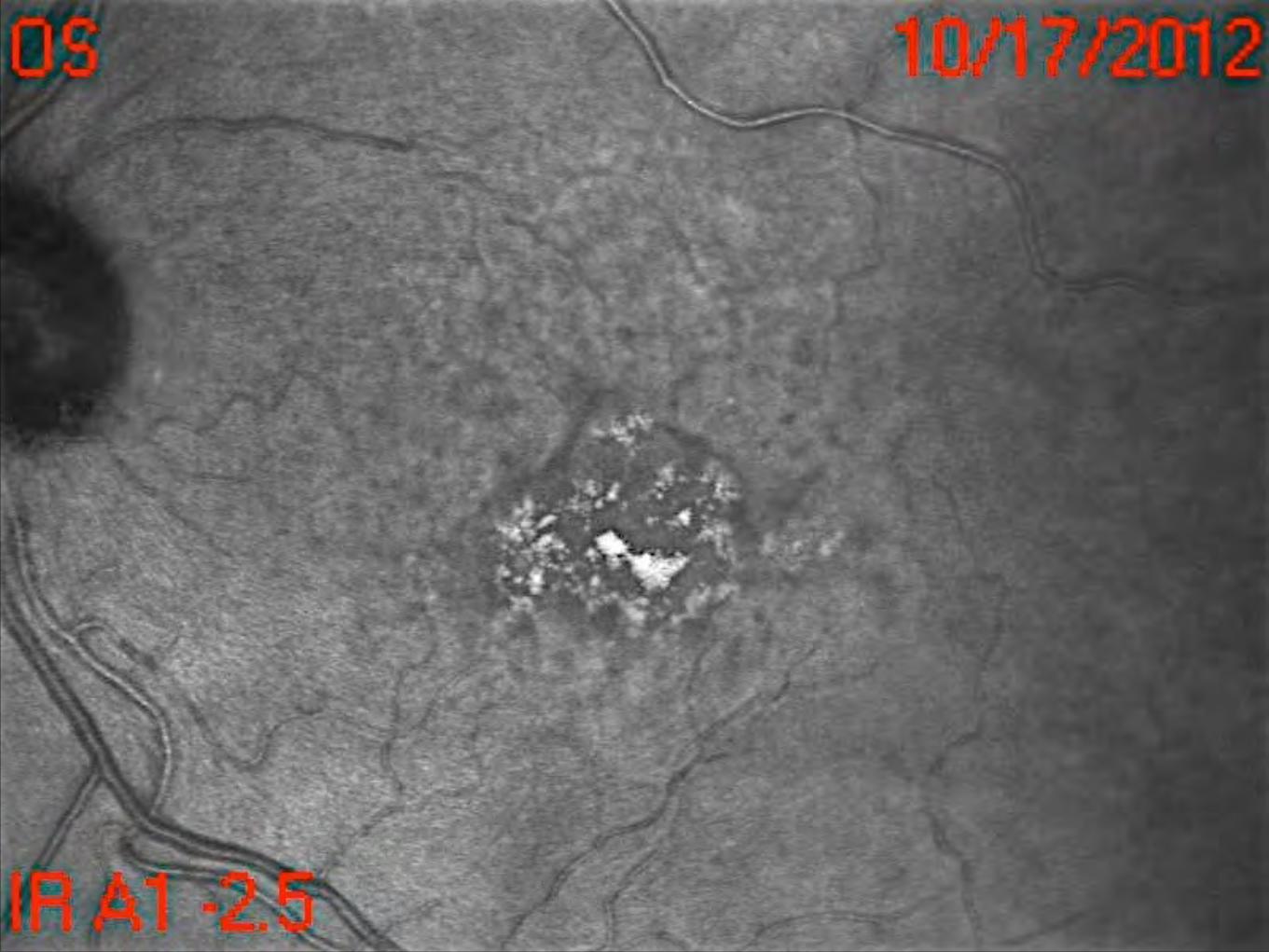
So* Drusen
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
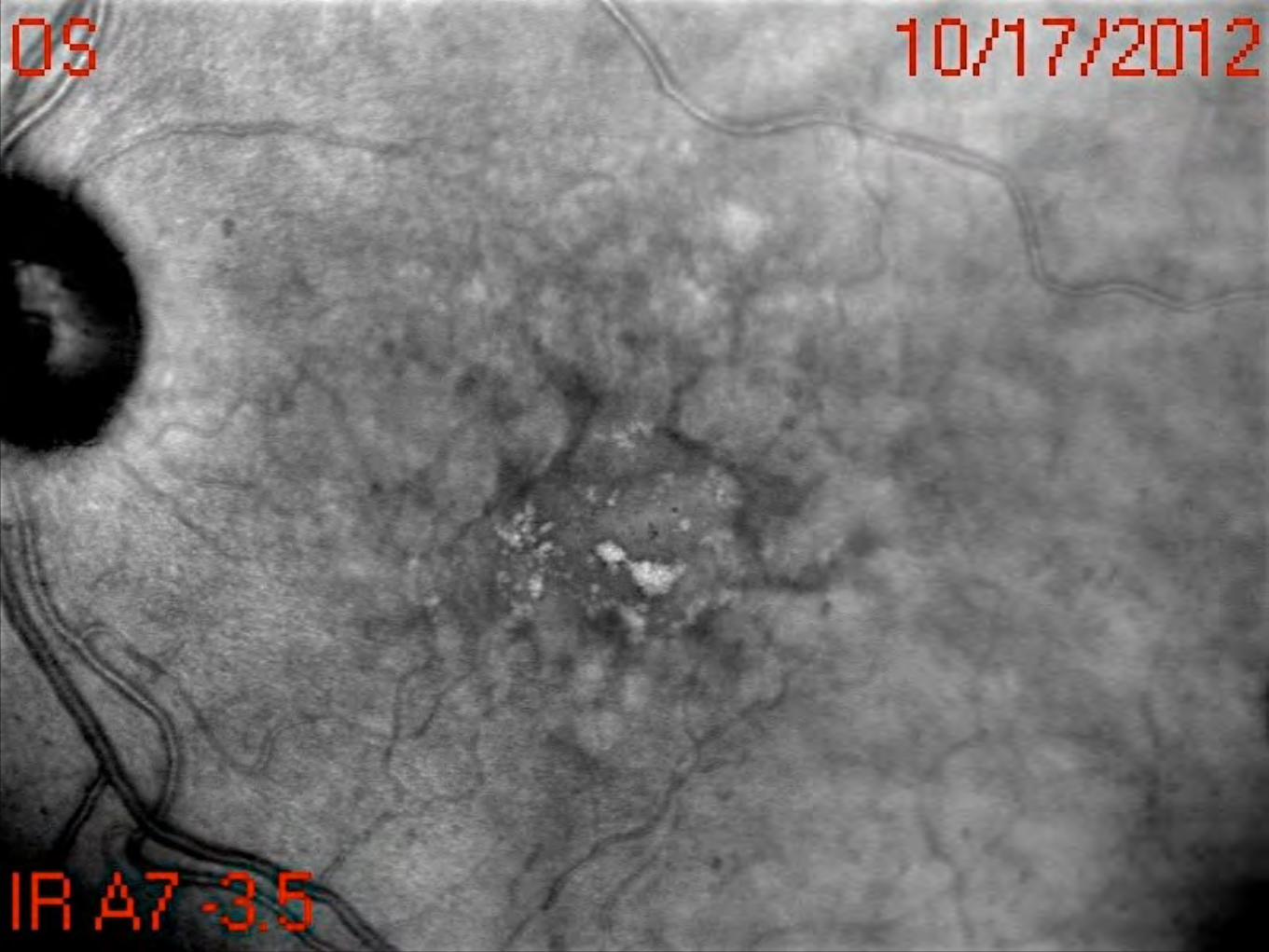
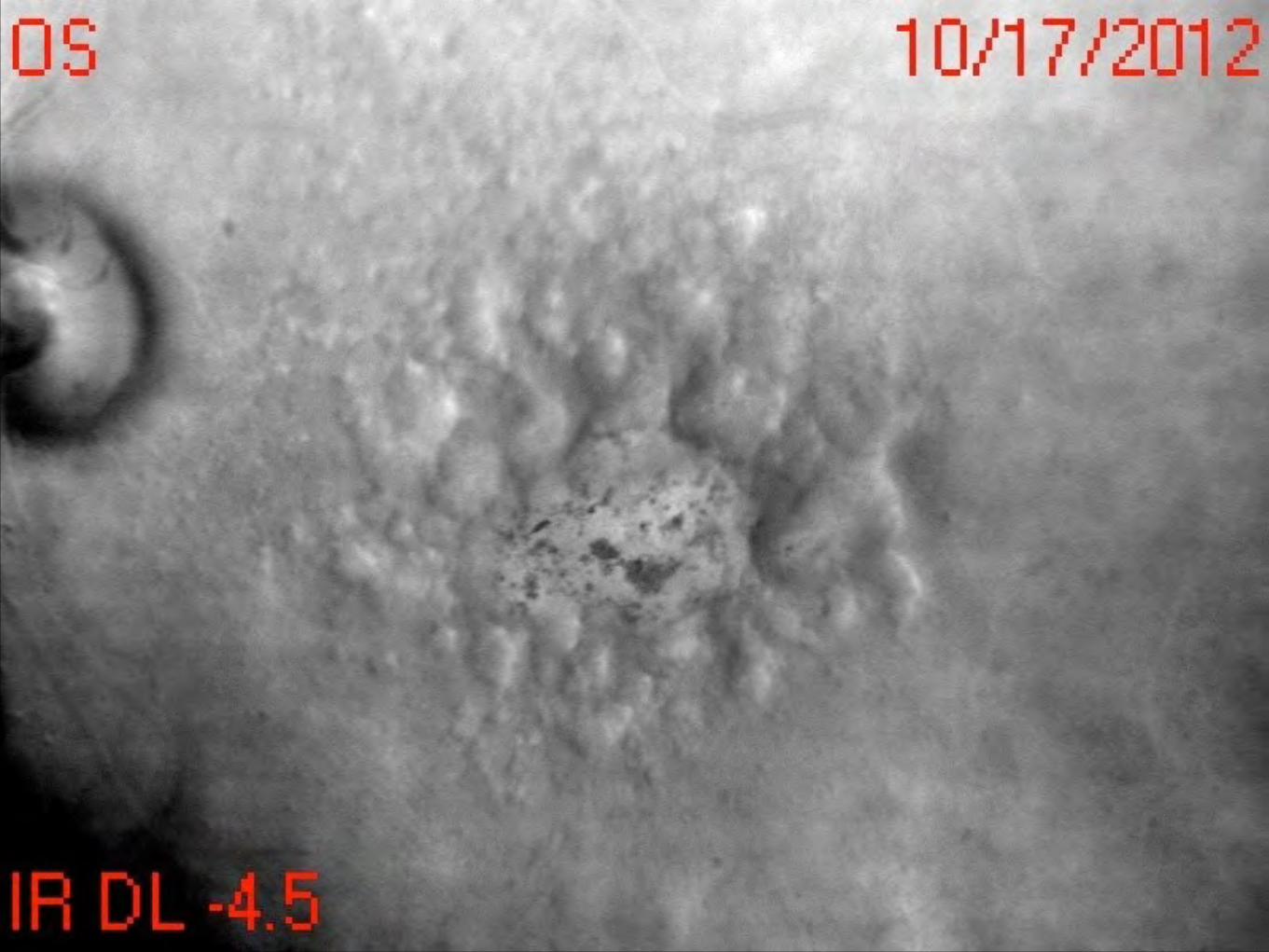
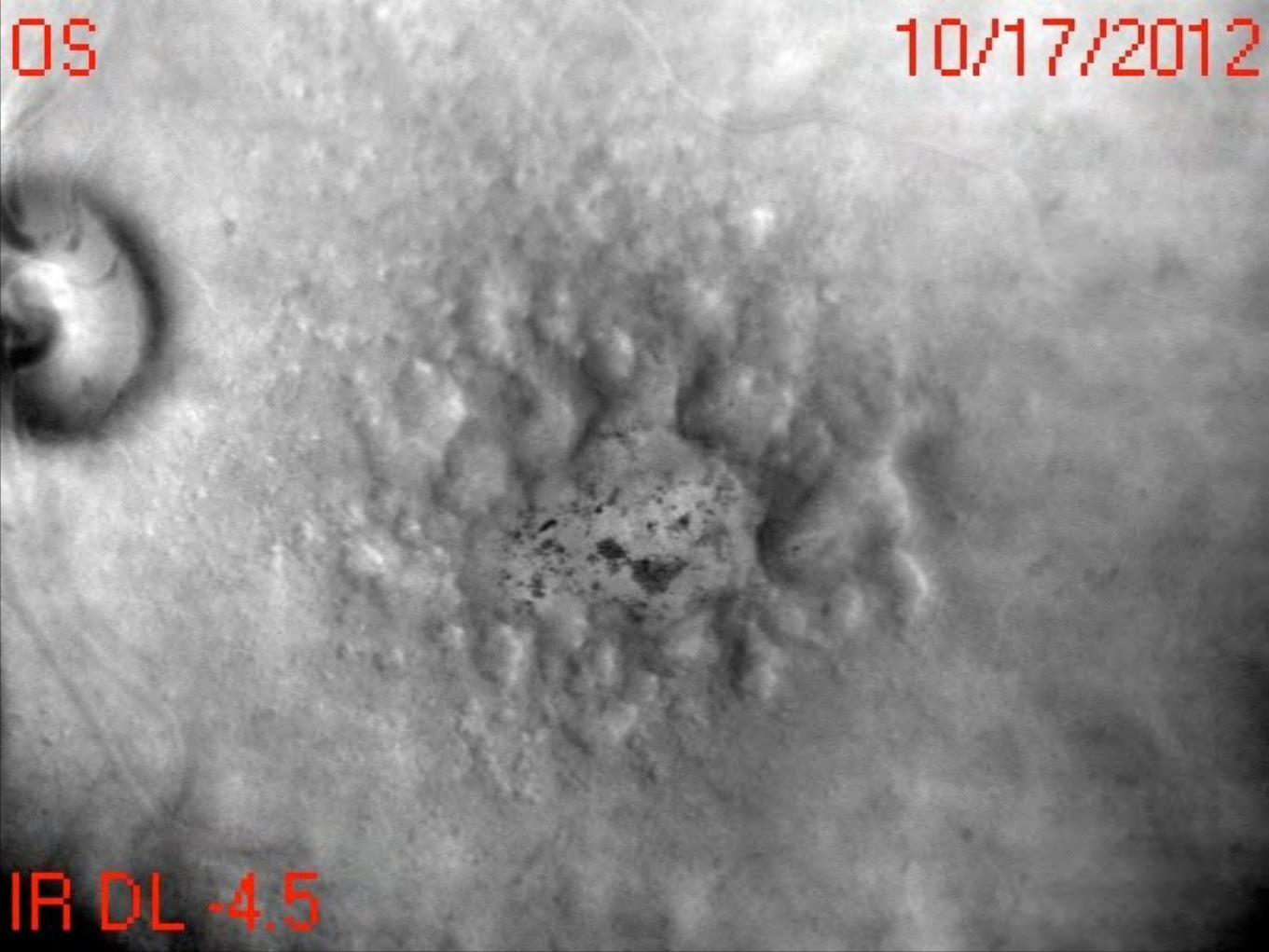
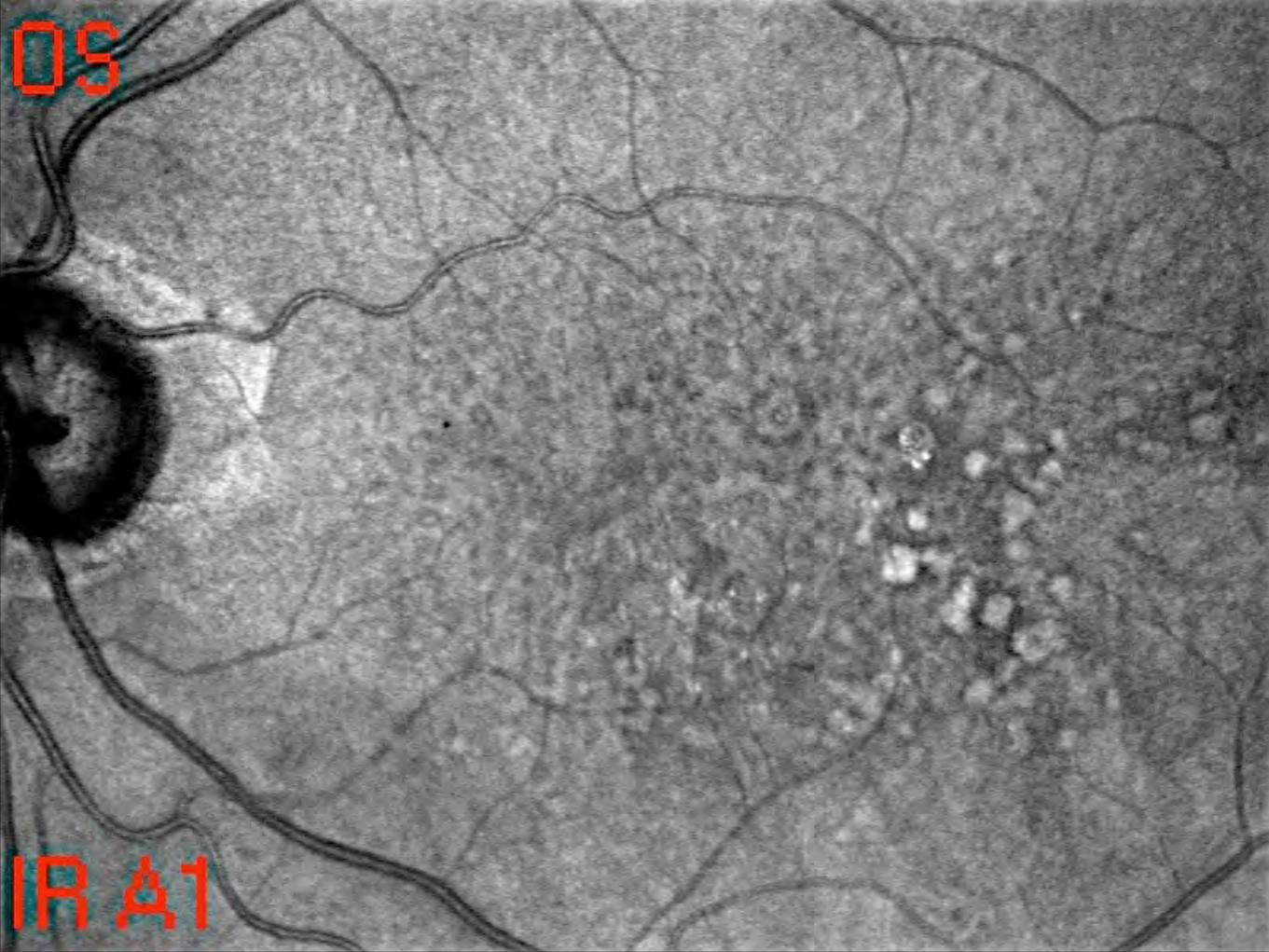
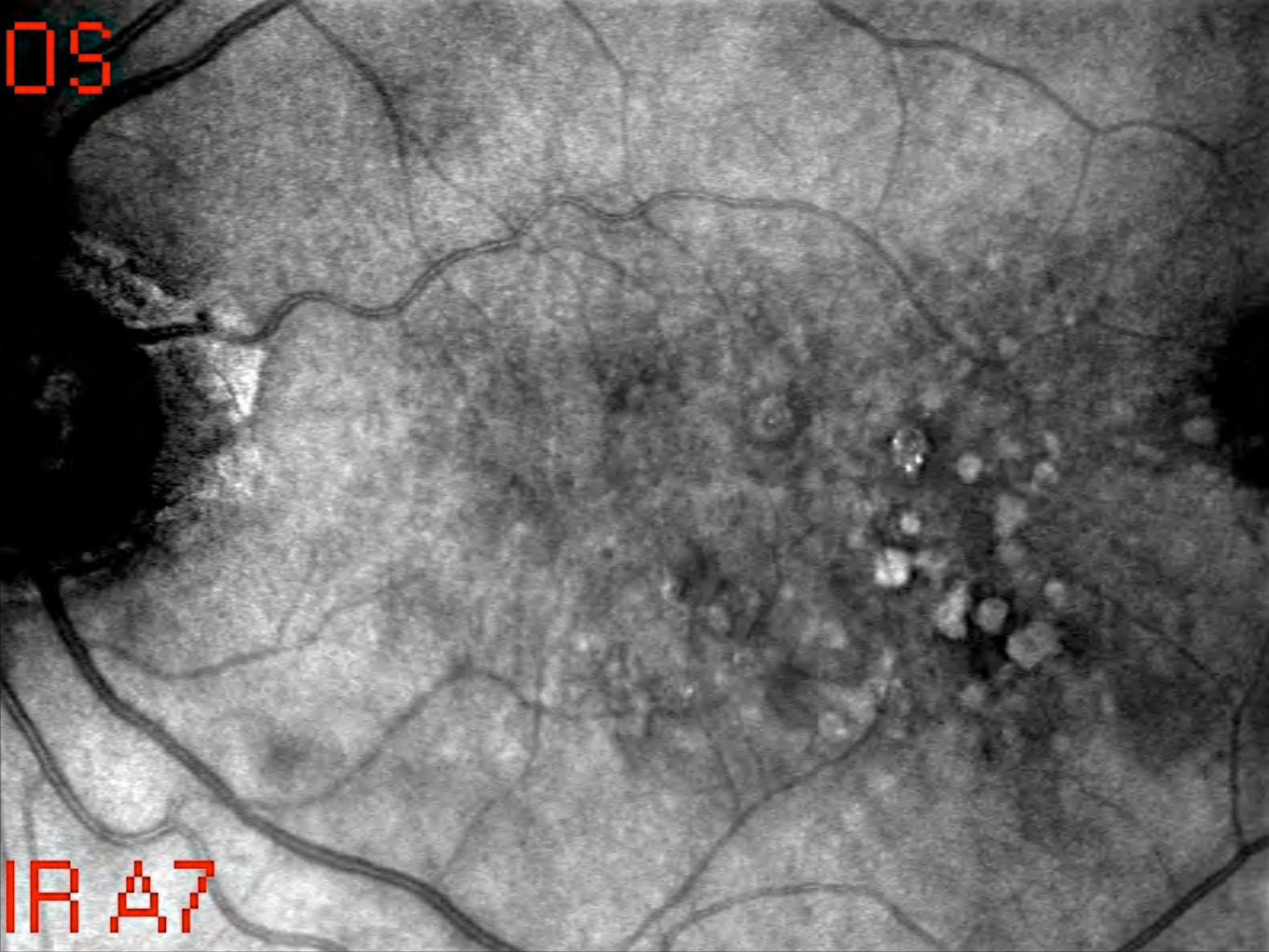
Re,cular Drusen
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
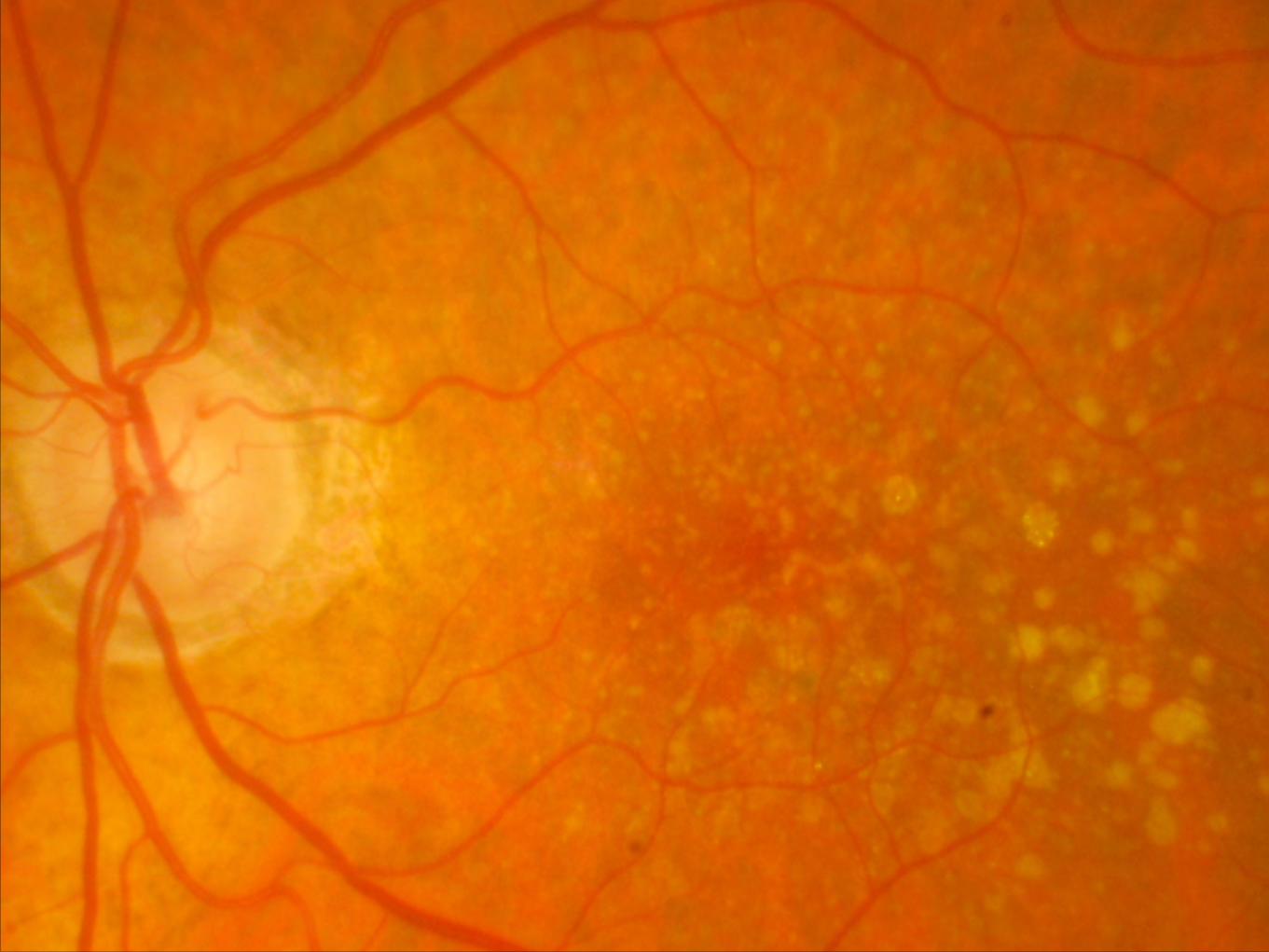
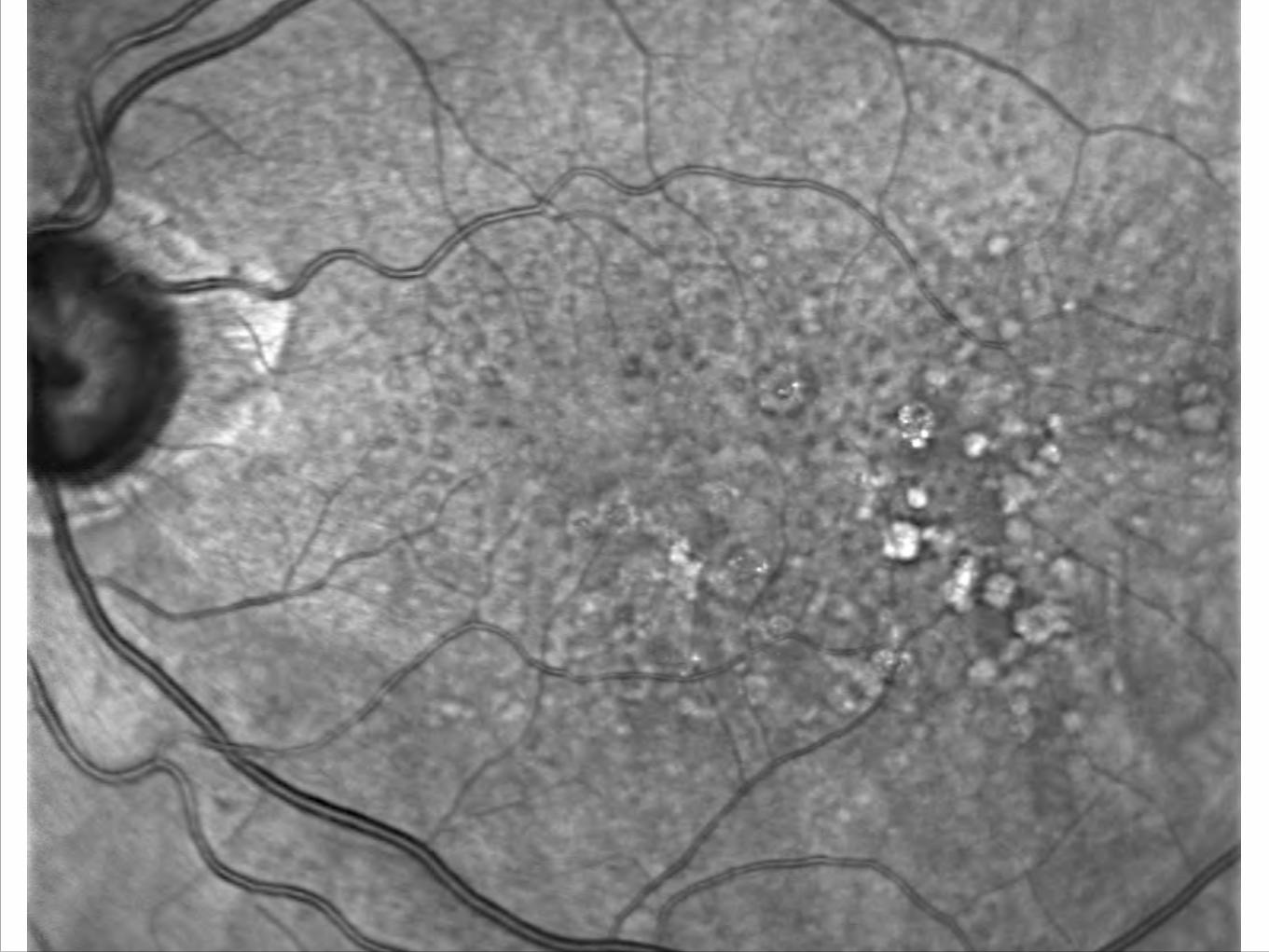
Re,cular Pseudodrusen
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Subre,nal drusenoid debris (SSD)
Chris&ne Curcio
disc in 46% of right and 55% of left eyes, while they were nevervisible in the center of macula.
DISCUSSION
In the present report the prevalence of RDR was much higherthan that previously reported. Furthermore, in this study, theprevalence was much higher on cSLO images (62%) whencompared with conventional fundus photography (18%).These results suggest that RDR represent a common pheno-typic biomarker in advanced atrophic AMD and that cSLOimaging is superior for detection of RDR compared with con-ventional fundus photography.
The identification of characteristic but subtle changes asso-ciated with RDR requires good image quality and careful anal-ysis. It may be challenging in the majority of subjects to acquireimages with even illumination and sharp focus over the entireframe. Despite good image quality, other phenotypic altera-tions such as soft or hard drusen may interfere with RDRdetection. In the present study, using a grading system thatdistinguishes between definite RDR and indefinite, there wasmoderate to good interobserver agreement (Armstrong JR, etal. IOVS 2005;46:ARVO E-Abstract 220/B194). Because we arenot yet able to define a clear-cut image quality threshold thatpermits one to exclude RDR, we consider the prevalence rateof 62% as the minimum RDR prevalence in our study cohort.Thus, RDR may be present even more frequently, but currentimaging technology may limit their detection.
Given the relatively high RDR prevalence in this cohort ofsubjects with GA, one could speculate that RDR represent adisease hallmark. Further, their absence might reflect the pres-ence of other diseases that mimic AMD phenotypic features.Atrophy of outer retinal layers (geographic atrophy) and asso-ciated choroidal neovascularization are obviously not specificfor AMD and occur in association with various complex andmonogenetic macular as well as diffuse retinal diseases. Tofurther explore the hypothesis that RDR represent an essentialdisease hallmark, we have initiated a genotype-phenotypestudy that will assess the correlation between AMD genetic riskfactors and the presence of RDR. Given both the markedly
improved detection and the superior interobserver reliabilitycompared with other imaging modalities, we believe that bothIR and FAF cSLO imaging are optimal choices for the charac-terization of RDRs in any future AMD natural history studies.
Several recent publications have reported that en face visi-ble RDR are spatially confined to locations that are anterior tothe RPE when visualized using an instrument that simultane-ously combines cSLO and SD-OCT imaging.17,28,29 This local-ization suggests that RDR may play a role in disease-relevantprocesses at the level of the photoreceptors. In contrast, pre-vious hypotheses on AMD pathogenesis have suggested thatchanges in drusen area or the location of drusen at the level ofthe RPE and Bruch’s membrane are of predominant impor-tance.
The histologic characterization of RDR is limited to a singlecase report in which the presence of RDR was related toabnormalities in the inner choroid.19 While frequently re-ported with OCT imaging, characterization of RDR with OCTmay be difficult; for example, it remains unclear if and towhich extent the highly reflective, focal SD-OCT alterations ofvariable extension above the RPE are caused by optical inter-ference. Although one might also speculate that RDR maycoexist together with already well-described extracellular ac-cumulation of material beneath the RPE as basal laminar de-posits and membranous debris, the latter alterations are not yetdetectable by currently imaging technology in the living hu-man eye. The high prevalence of RDR found in the presentstudy should in any case further prompt histopathological andbiochemical studies to elucidate the exact morphologic sub-strate of RDR and their molecular composition.
In accordance with previous reports, we confirmed thatRDR are most commonly located superior to the foveal centerin the outer macula and that they are correlated with increas-ing age and with female sex.19,24 The rare prevalence within3000 !m from the foveal center in this cross-sectional study ineyes affected from late-stage atrophic AMD does not indicatethat this area is an untypical location for RDR. Presence of GAis associated with the absence of RD. From this study it is notpossible to address the possible presence of RD in the perifo-veal area before GA developed. Using three-field FAF imaging,
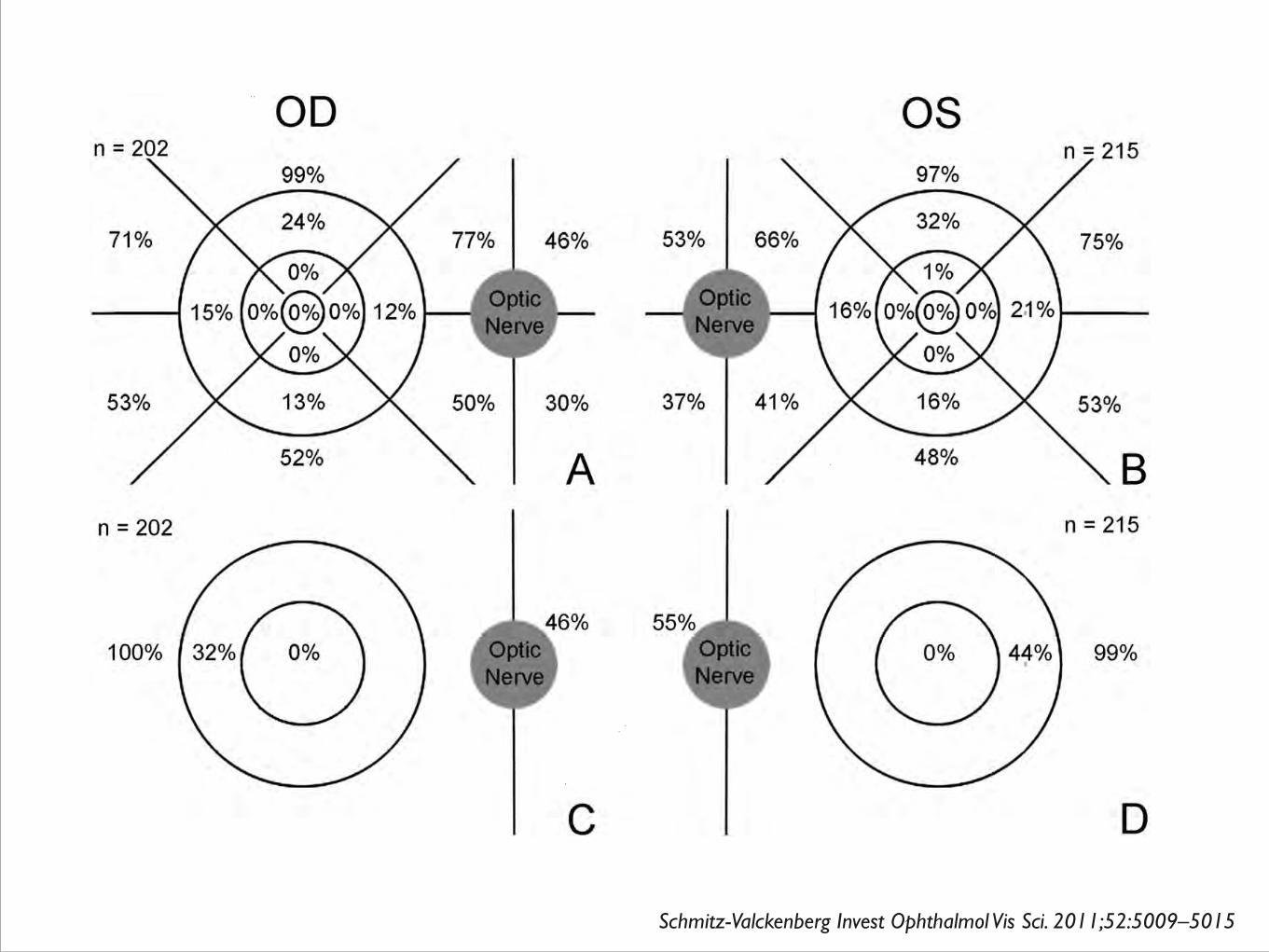
FIGURE 4. Diagrams showing the lo-cation of prevalent RDR as identifiedby three-field cSLO fundus autofluo-rescence imaging, illustrated sepa-rately for right (A, C: OD) and lefteyes (B, D: OS). The top row showsthe topographic presence for each ofthe 17 predefined fields (see also Fig.2); in the bottom row the presenceof drusen by four grouped areas isillustrated. Note that the central 3000!m were largely involved by atro-phic areas in this study populationwith all eyes showing patches of GA.Therefore, it cannot be excluded ifRDR were present before the devel-opment of atrophy.
IOVS, August 2011, Vol. 52, No. 9 Reticular Drusen in GA 5013
Schmitz-Valckenberg Invest Ophthalmol Vis Sci. 2011;52:5009–5015
© Giovanni Staurenghi 2014 - Tutti i diritti riservati Schmitz-Valckenberg Invest Ophthalmol Vis Sci. 2011;52:5009–5015
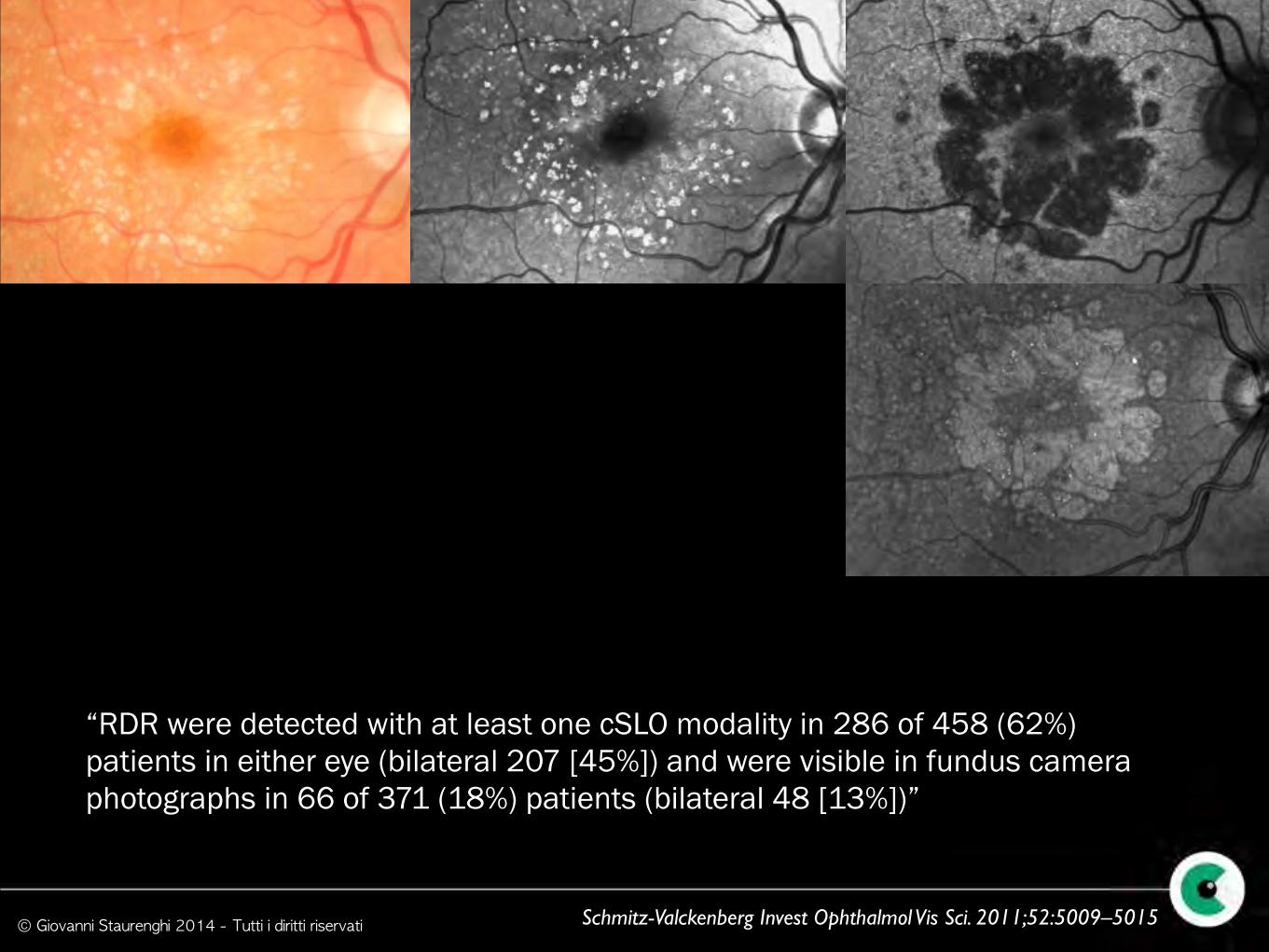
“RDR were detected with at least one cSLO modality in 286 of 458 (62%) patients in either eye (bilateral 207 [45%]) and were visible in fundus camera photographs in 66 of 371 (18%) patients (bilateral 48 [13%])”
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
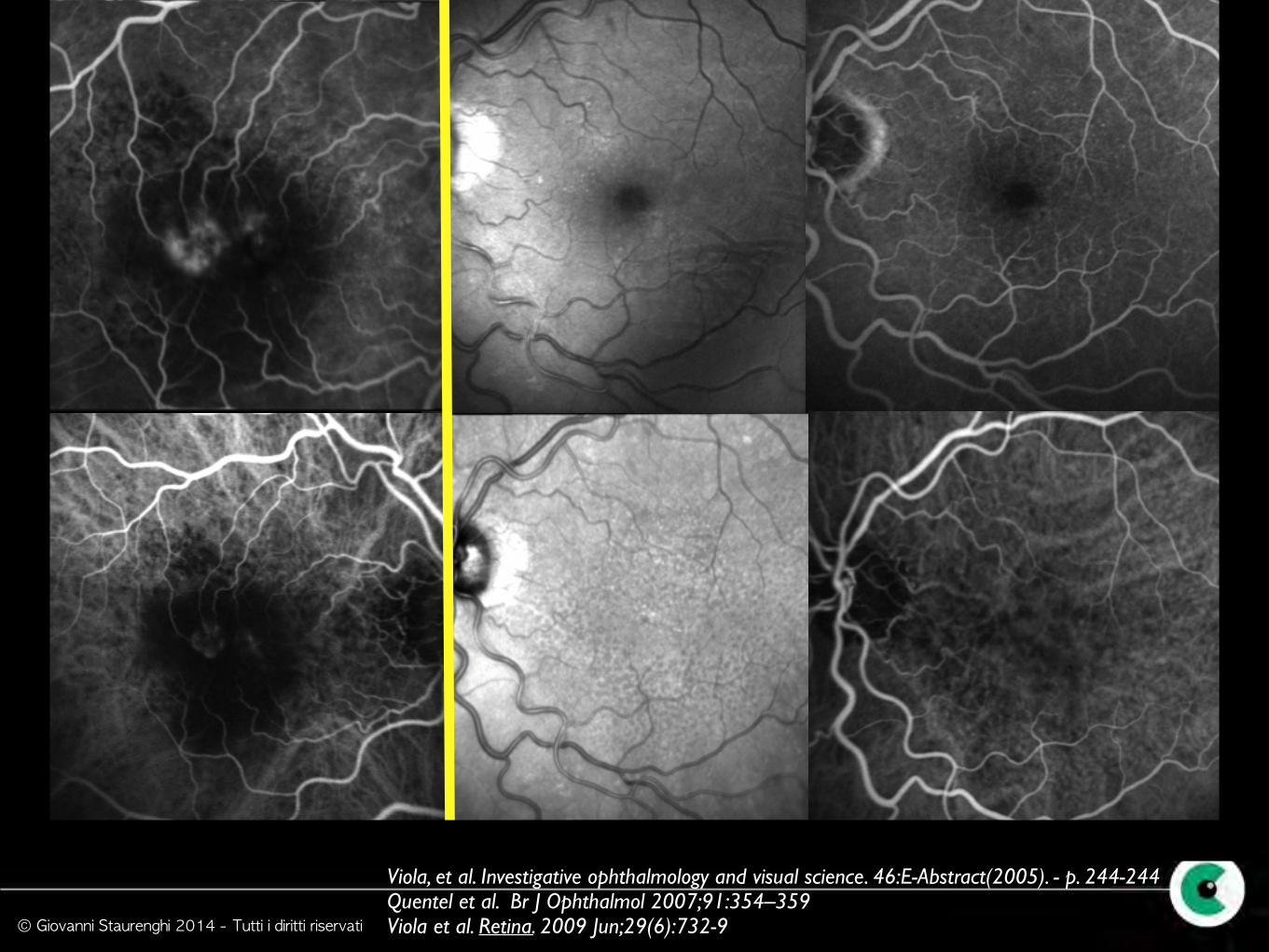
Viola, et al. Investigative ophthalmology and visual science. 46:E-Abstract(2005). - p. 244-244 Quentel et al. Br J Ophthalmol 2007;91:354–359 Viola et al. Retina. 2009 Jun;29(6):732-9
© Giovanni Staurenghi 2014 - Tutti i diritti riservati
Membrane neovascolari
coroideali
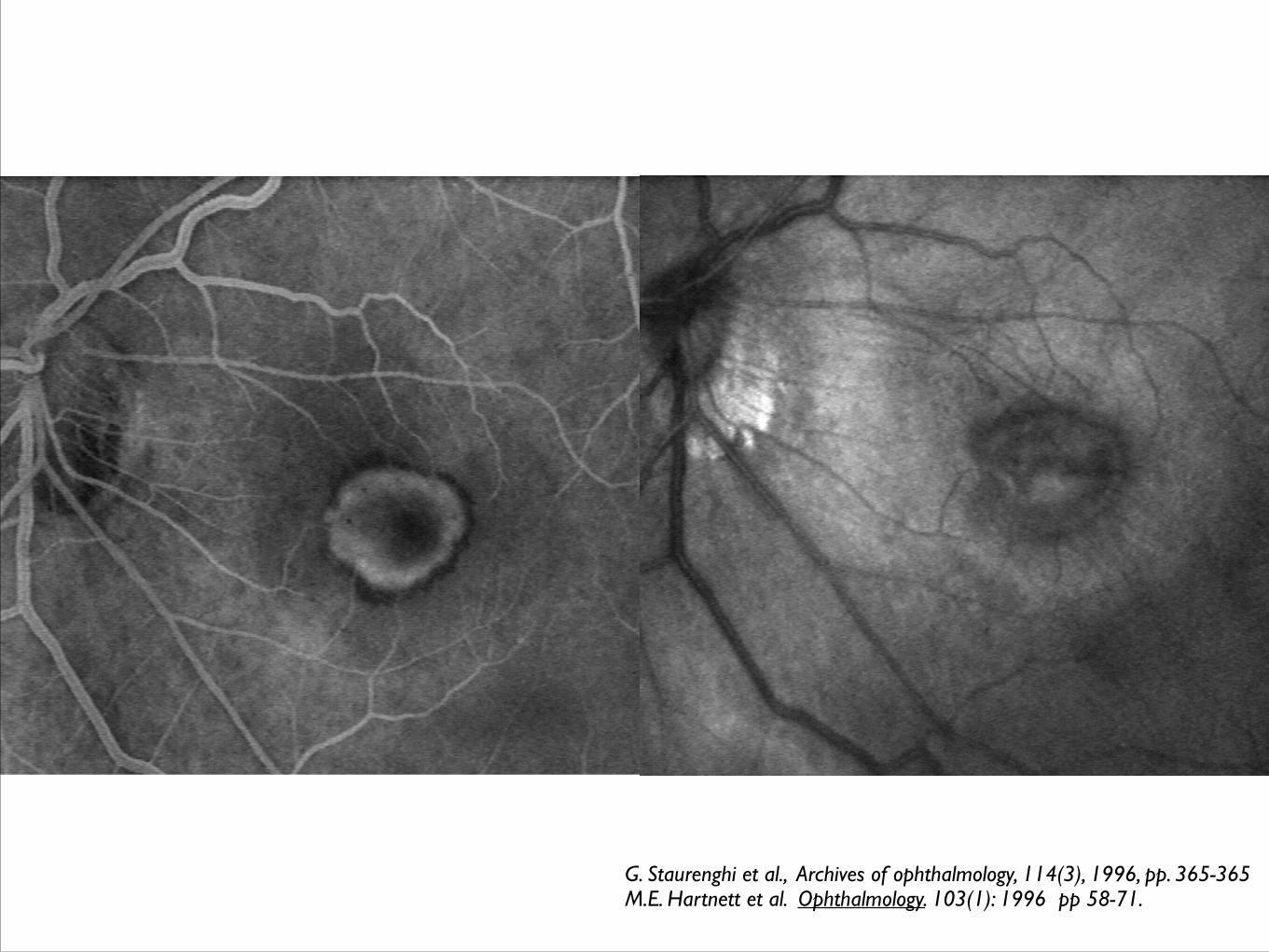
G. Staurenghi et al., Archives of ophthalmology, 114(3), 1996, pp. 365-365 M.E. Hartnett et al. Ophthalmology. 103(1): 1996 pp 58-71.