Milano, 28 maggio 2013
55
Cristiano Termine UONPIA Ospedale di Circolo, Fondazione Macchi di Varese Milano, 28 maggio 2013 Azienda Ospedaliera SPEDALI CIVILI BRESCIA ADHD: per una condivisione dei percorsi diagnostico-terapeutici DAL REGISTRO REGIONALE SESSIONE: COMORBIDITÀ
Transcript of Milano, 28 maggio 2013

Cristiano Termine UONPIA Ospedale di Circolo, Fondazione Macchi di Varese
Milano, 28 maggio 2013
Azienda Ospedaliera
SPEDALI CIVILI BRESCIA
ADHD: per una condivisione dei percorsi
diagnostico-terapeutici
DAL REGISTRO REGIONALE
SESSIONE: COMORBIDITÀ
COMPLETATA
492
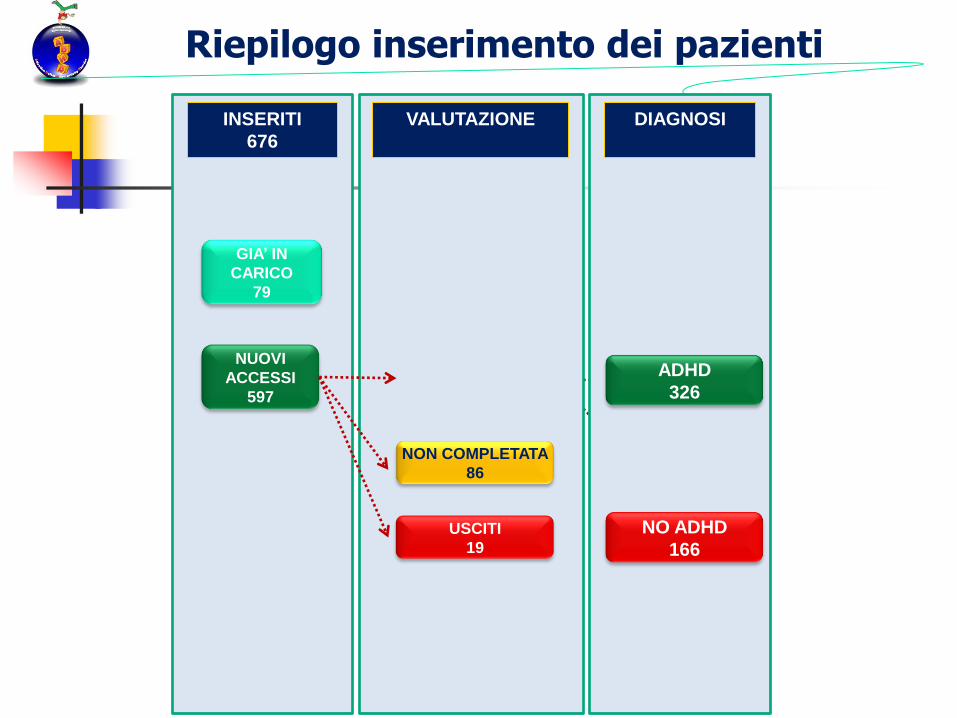
Riepilogo inserimento dei pazienti
GIA’ IN
CARICO
79
NUOVI
ACCESSI
597
DIAGNOSI
INSERITI
676
VALUTAZIONE
NON COMPLETATA
86
USCITI
19
ADHD
326
NO ADHD
166
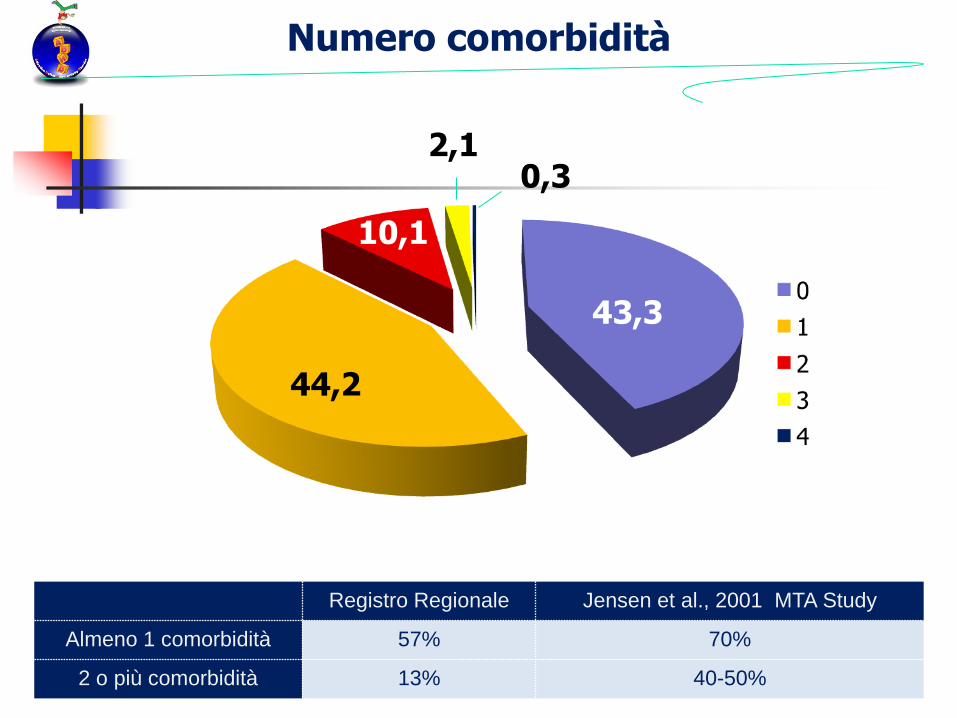
Numero comorbidità
Registro Regionale Jensen et al., 2001 MTA Study
Almeno 1 comorbidità 57% 70%
2 o più comorbidità 13% 40-50%
44,2
43,3
10,1
2,1 0,3
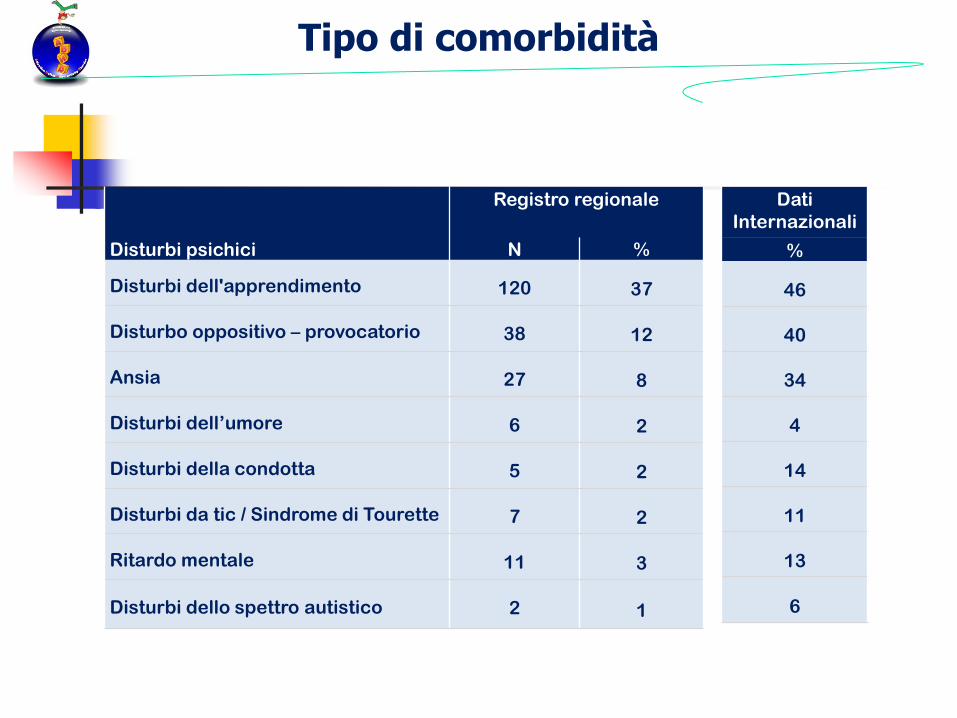
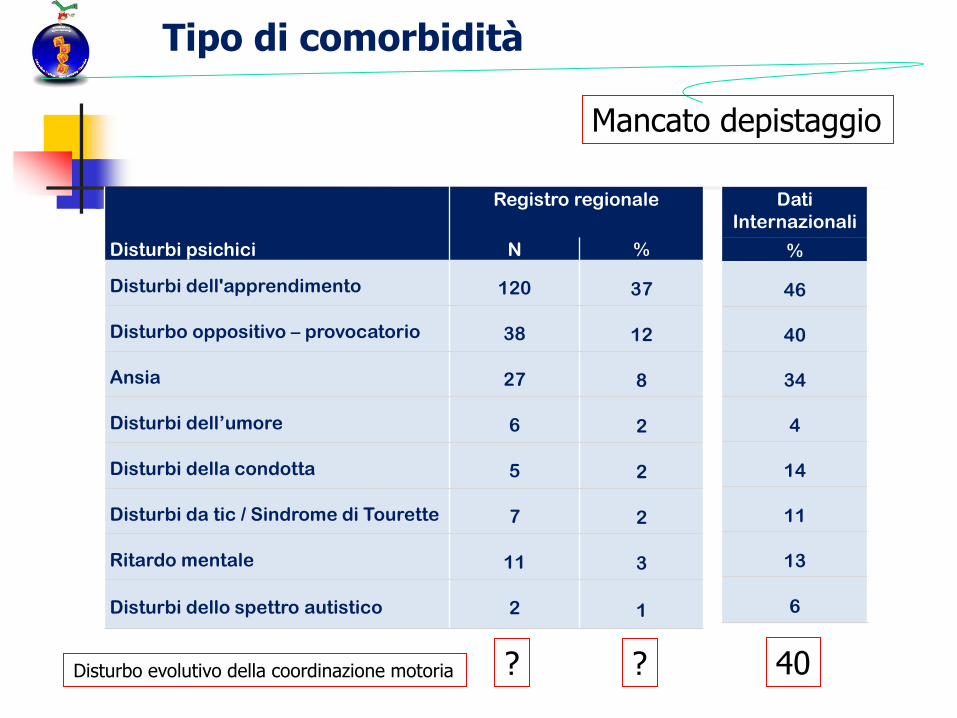
Registro regionale
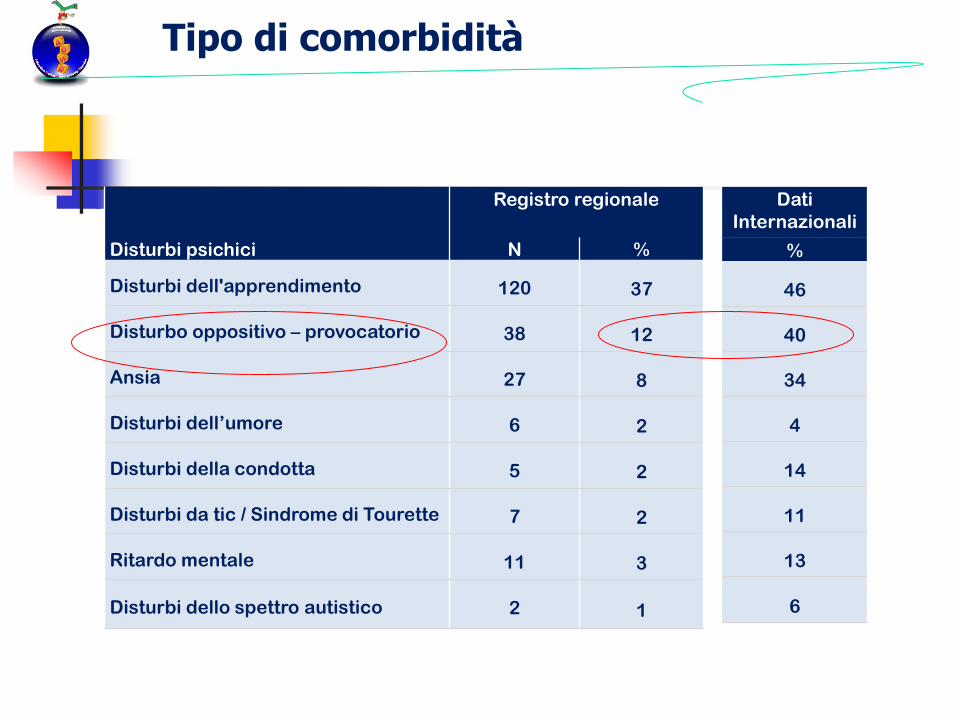
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità

DSM- I -> DSM-5


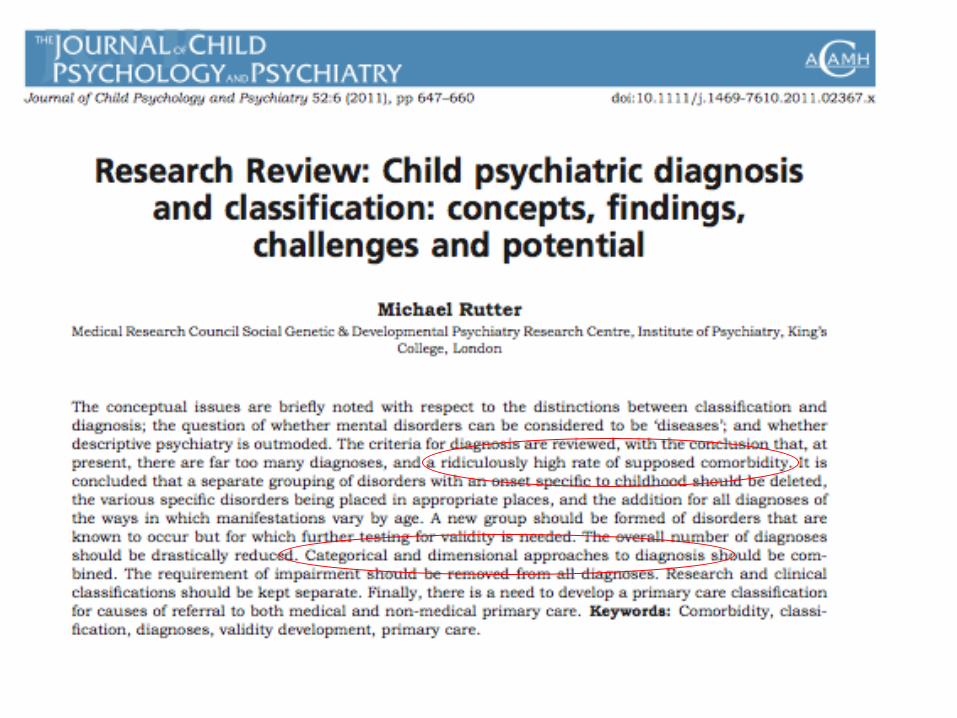

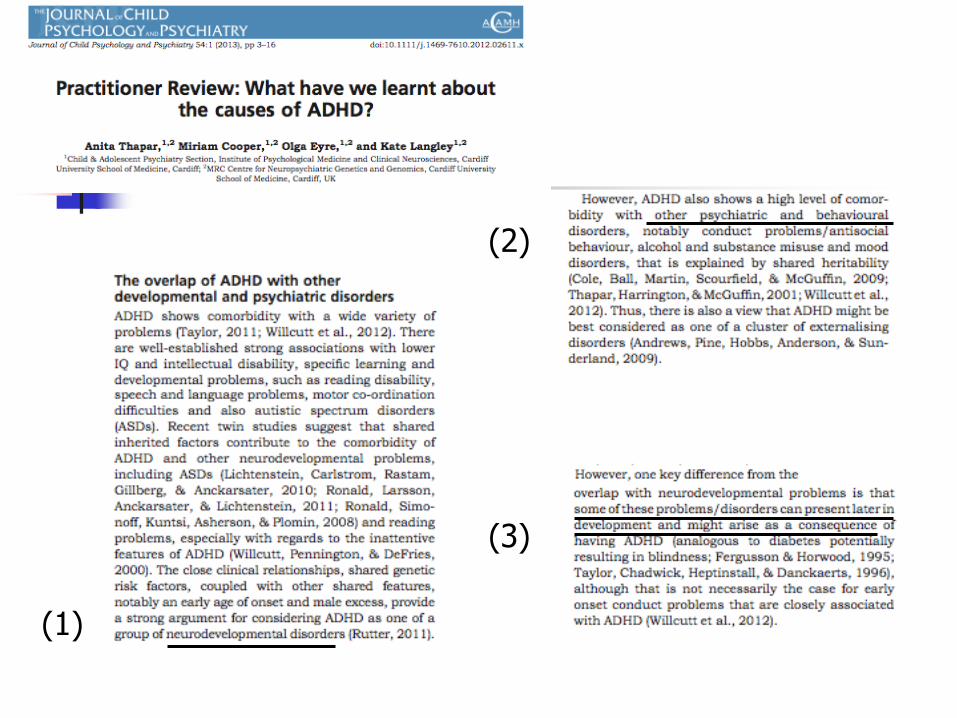
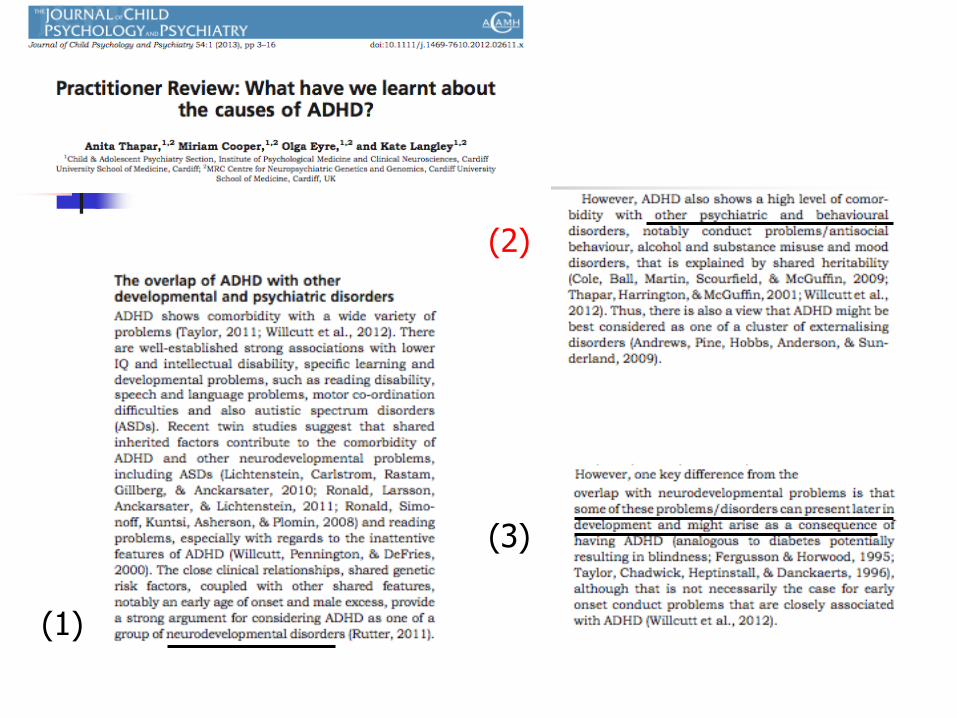
(1)
(2)
(3)

(1)
(2)
(3)

Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità
Depistaggio sistematico

15

Italia USA
3.6% 7.3%
Lindgren, De Renzi and Richman (1985)
Cross-national comparisons of developmental dyslexia in Italy and the United States.
Child Dev. 1985; 56:1404–1417.
Prevalenza della dislessia


Possible Locations of Genes That Influence
RD, ADHD, or both RD and ADHD
RD
R+A
R+A
RD
RD
RD RD
RD
R+A
RD
AD R+A
AD
AD
AD
R+A R+A
AD
R+A
R+A
RD
RD RD R+A
AD

ADHD / DSA
Eziopatogenesi comune Modello eziologico probabilistico e
multifattoriale (Pennington 2006)


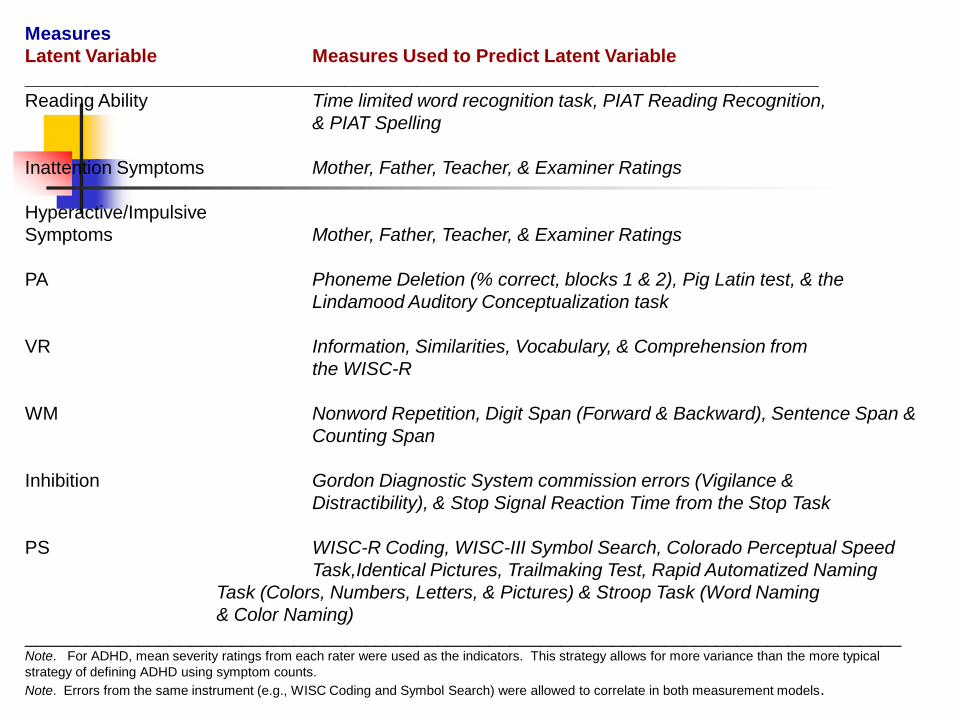
Measures
Latent Variable Measures Used to Predict Latent Variable
_____________________________________________________________________________
Reading Ability Time limited word recognition task, PIAT Reading Recognition,
& PIAT Spelling
Inattention Symptoms Mother, Father, Teacher, & Examiner Ratings
Hyperactive/Impulsive
Symptoms Mother, Father, Teacher, & Examiner Ratings
PA Phoneme Deletion (% correct, blocks 1 & 2), Pig Latin test, & the
Lindamood Auditory Conceptualization task
VR Information, Similarities, Vocabulary, & Comprehension from
the WISC-R
WM Nonword Repetition, Digit Span (Forward & Backward), Sentence Span &
Counting Span
Inhibition Gordon Diagnostic System commission errors (Vigilance &
Distractibility), & Stop Signal Reaction Time from the Stop Task
PS WISC-R Coding, WISC-III Symbol Search, Colorado Perceptual Speed
Task,Identical Pictures, Trailmaking Test, Rapid Automatized Naming
Task (Colors, Numbers, Letters, & Pictures) & Stroop Task (Word Naming
& Color Naming)
_____________________________________________________________________________________ Note. For ADHD, mean severity ratings from each rater were used as the indicators. This strategy allows for more variance than the more typical
strategy of defining ADHD using symptom counts.
Note. Errors from the same instrument (e.g., WISC Coding and Symbol Search) were allowed to correlate in both measurement models.
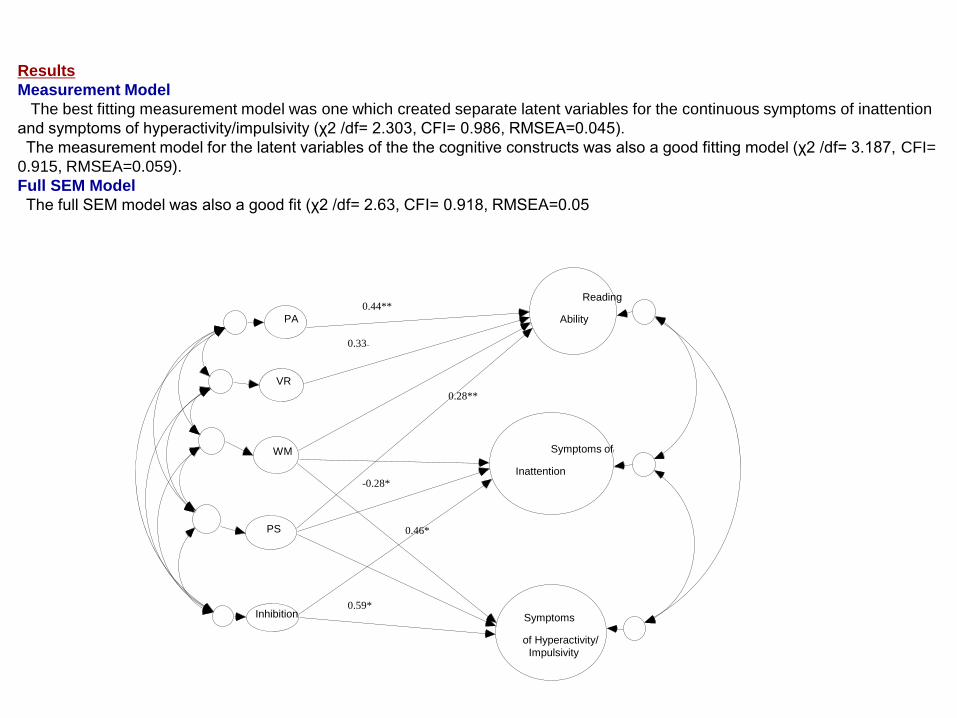
Results
Measurement Model
The best fitting measurement model was one which created separate latent variables for the continuous symptoms of inattention
and symptoms of hyperactivity/impulsivity (χ2 /df= 2.303, CFI= 0.986, RMSEA=0.045).
The measurement model for the latent variables of the the cognitive constructs was also a good fitting model (χ2 /df= 3.187, CFI=
0.915, RMSEA=0.059).
Full SEM Model
The full SEM model was also a good fit (χ2 /df= 2.63, CFI= 0.918, RMSEA=0.05
PA
VR
WM
PS
Inhibition
Reading
Ability
Symptoms off
Inattention
Symptoms
of Hyperactivity/
Impulsivity
0.33**
0.28**
0.59*
-0.28*
0.46*
0.44**
Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità
Mancato depistaggio
Disturbo evolutivo della coordinazione motoria ? ? 40

J Child Psychol Psychiatry. 2001 May;42(4):487-92. The comorbidity of ADHD in the general population of Swedish school-age children. Kadesjö B, Gillberg C. Source Göteborg University, Sweden. Abstract This study examined patterns of comorbid/associated diagnoses and associated problems in a population sample of children with and without DSM-III-R attention-deficit hyperactivity disorder (ADHD). Half (N = 409) of a mainstream school population of Swedish 7-year-olds were clinically examined, and parents and teachers were interviewed and completed questionnaires. The children were followed up 2-4 years later. Eighty-seven per cent of children meeting full criteria for ADHD (N = 15) had one or more and 67% at least two--comorbid diagnoses. The most common comorbidities were oppositional defiant disorder and developmental coordination disorder. Children with subthreshold ADHD (N = 42) also had very high rates of comorbid diagnoses (71% and 36%), whereas those without ADHD (N = 352) had much lower rates (17% and 3%). The rate of associated school adjustment, learning, and behaviour problems at follow-up was very high in the ADHD groups. We concluded that pure ADHD is rare even in a general population sample. Thus, studies reporting on ADHD cases without comorbidity probably refer to highly atypical samples. By and large, such studies cannot inform rational clinical decisions.
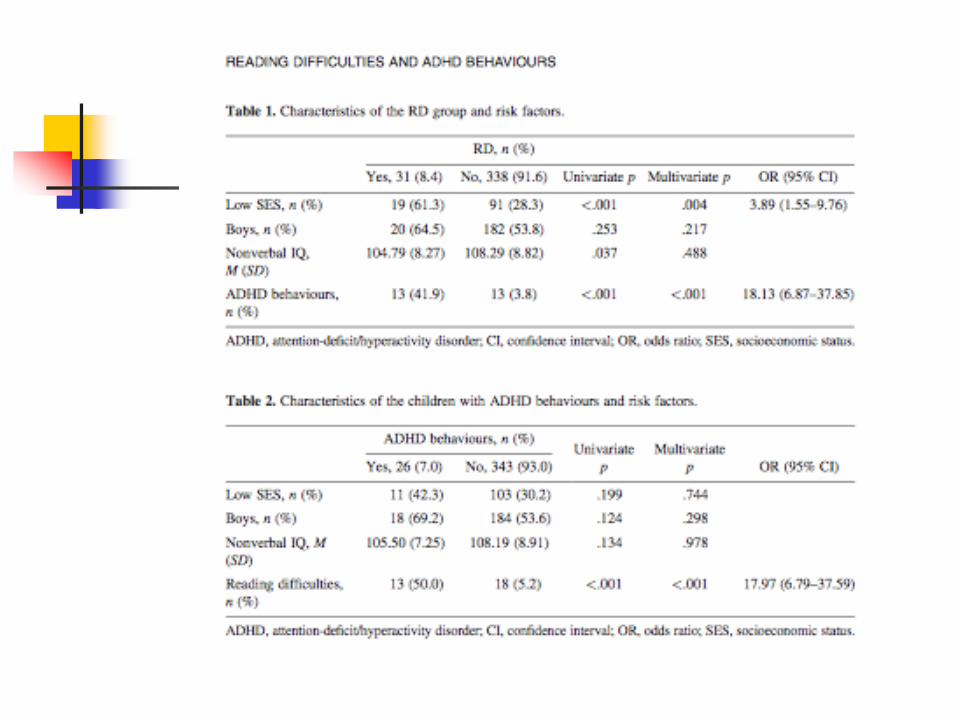
ADHD and developmental coordination disorder (DCD) are two developmental conditions that may cause motor, academic and social
dysfunctions (APA, 1994). Their coexistence was documented in several studies, and as many as 35–47%
of the children with ADHD were diagnosed as having comorbid DCD.
(1)
(2)
(3)
Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità

Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità

ADHD
326
CON KSADS
259
SENZA KSADS
67
Sintomi Sottosoglia Patologici Disturbo oppositivo-provocatorio 19 18
Ansia 9 4
Disturbi depressivi 8 5
Disturbo della condotta 7 1
Disturbo di ansia da separazione 6 2
Enuresi 2 1
Episodio maniacale 1 1
Disturbo da tic 1 3
Fobie 0 4
Disturbo psicotico 0 0
Disturbo di panico 0 0
Disturbo di fobia sociale 0 0
Disturbo ossessivo-compulsivo 0 0
Encopresi 0 0
Anoressia nervosa 0 0
Bulimia nervosa 0 0
Abuso di alcol 0 0
Abuso di sostanze 0 0
Disturbo post-traumatico da stress 0 0
Comorbidità KSADS
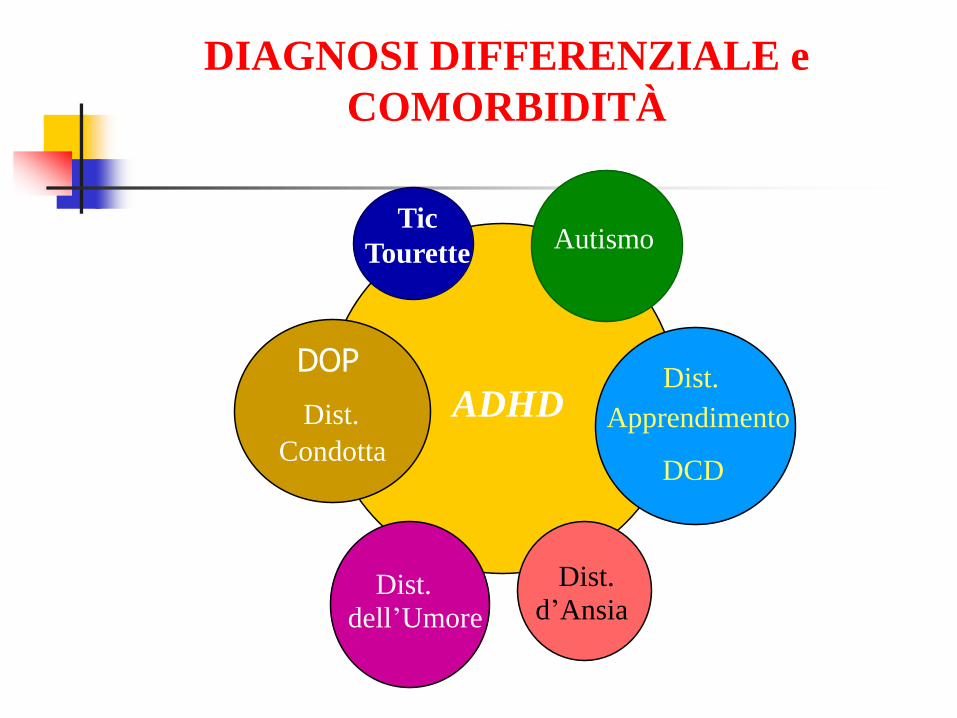
Dist.
Condotta
Tic
Tourette Autismo
Dist.
Apprendimento
Dist.
dell’Umore
ADHD
Dist.
d’Ansia
DIAGNOSI DIFFERENZIALE e
COMORBIDITÀ
DOP
DCD



Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità

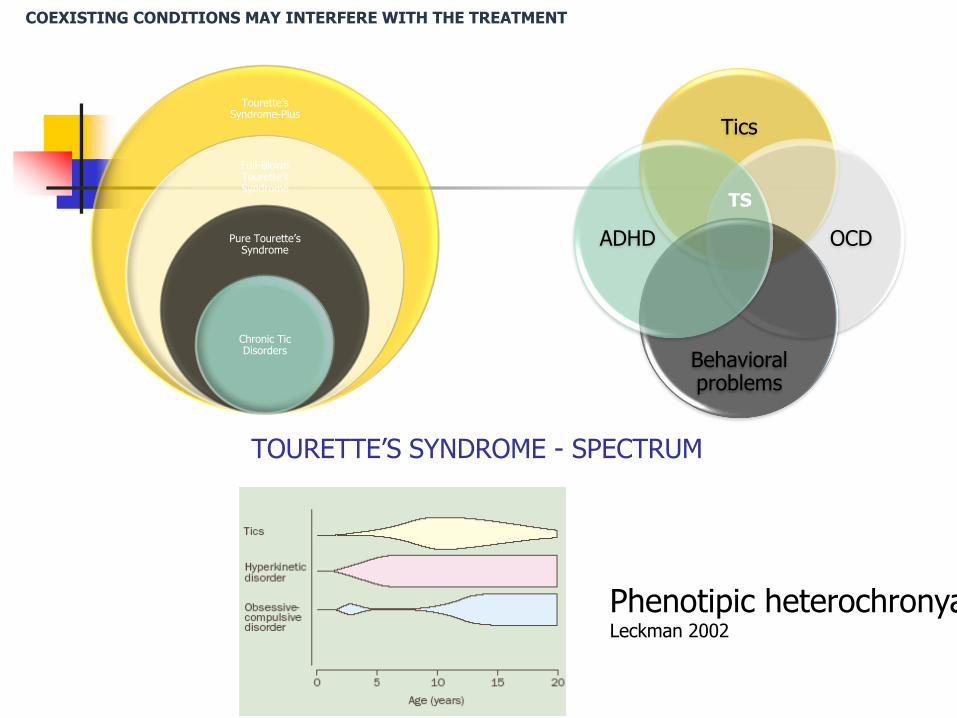
TOURETTE’S SYNDROME - SPECTRUM
Tics
OCD
Behavioral problems
ADHD
TS
Tourette’s Syndrome-Plus
Full-Blown Tourette’s Syndrome
Pure Tourette’s Syndrome
Chronic Tic Disorders
Phenotipic heterochronya Leckman 2002
COEXISTING CONDITIONS MAY INTERFERE WITH THE TREATMENT
ESSTS Annual Meeting 2013 COST International Conference for Tourette
Syndrome
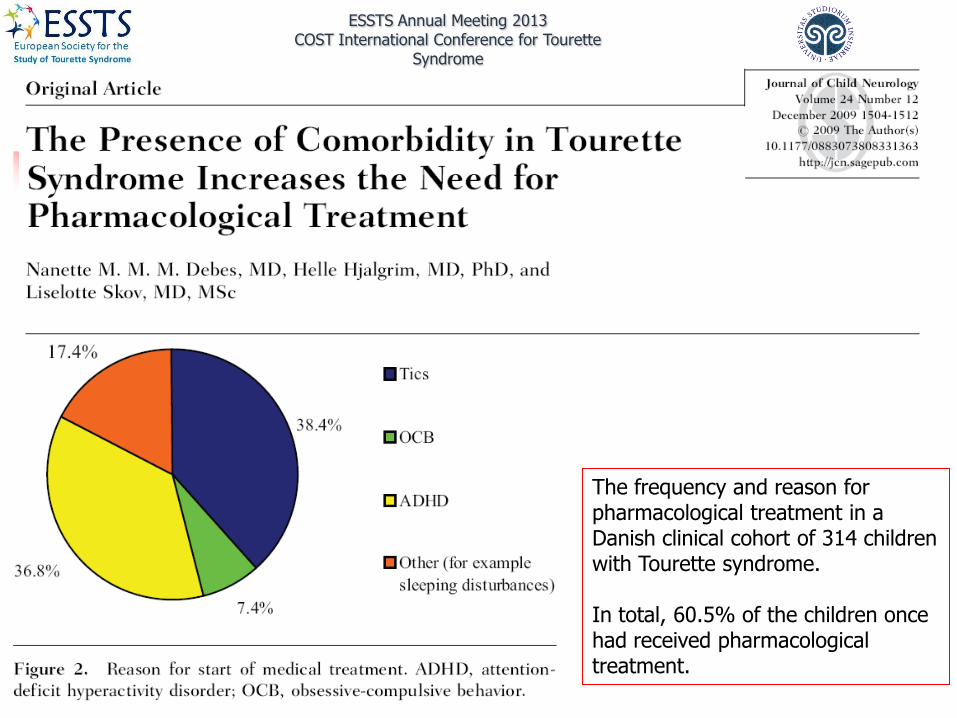
The frequency and reason for pharmacological treatment in a Danish clinical cohort of 314 children with Tourette syndrome. In total, 60.5% of the children once had received pharmacological treatment.

ESSTS Annual Meeting 2013 COST International Conference for Tourette
Syndrome
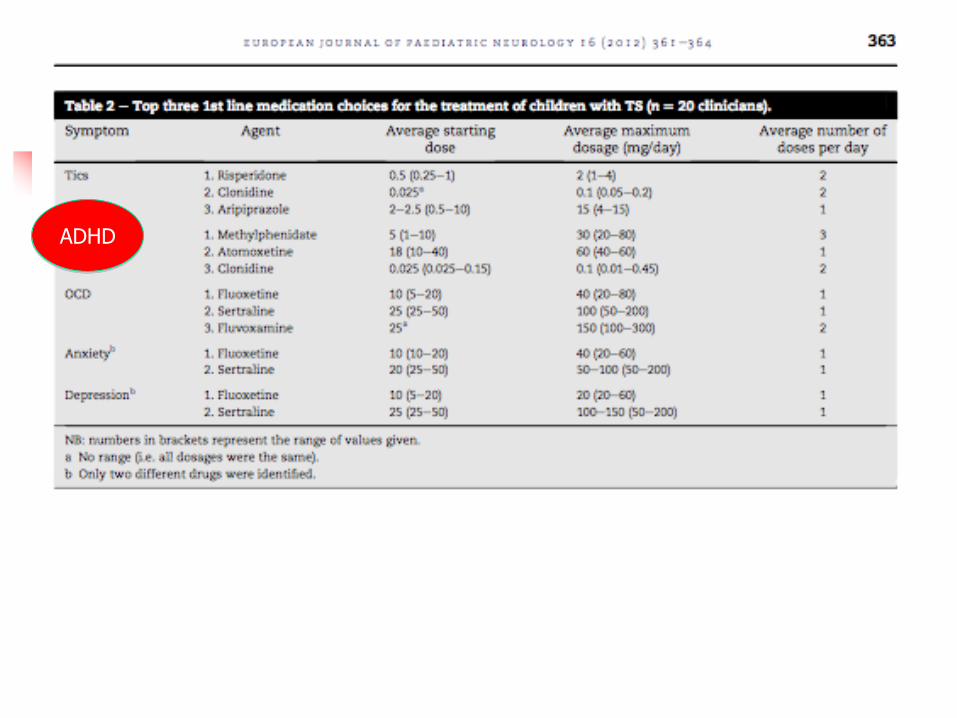
ADHD

ESSTS Annual Meeting 2013 COST International Conference for Tourette
Syndrome
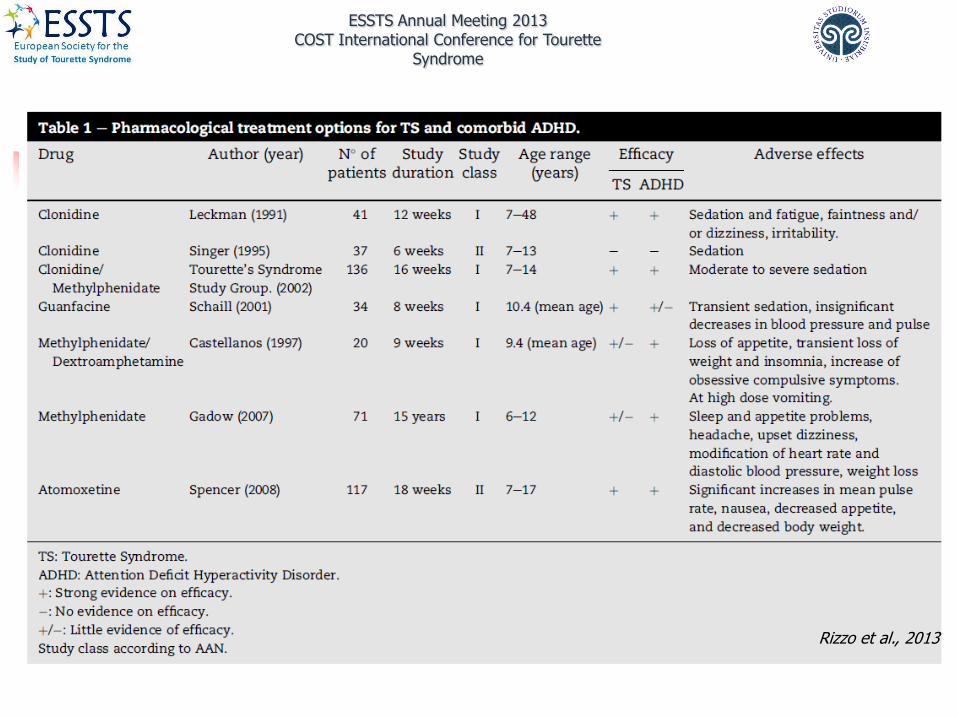
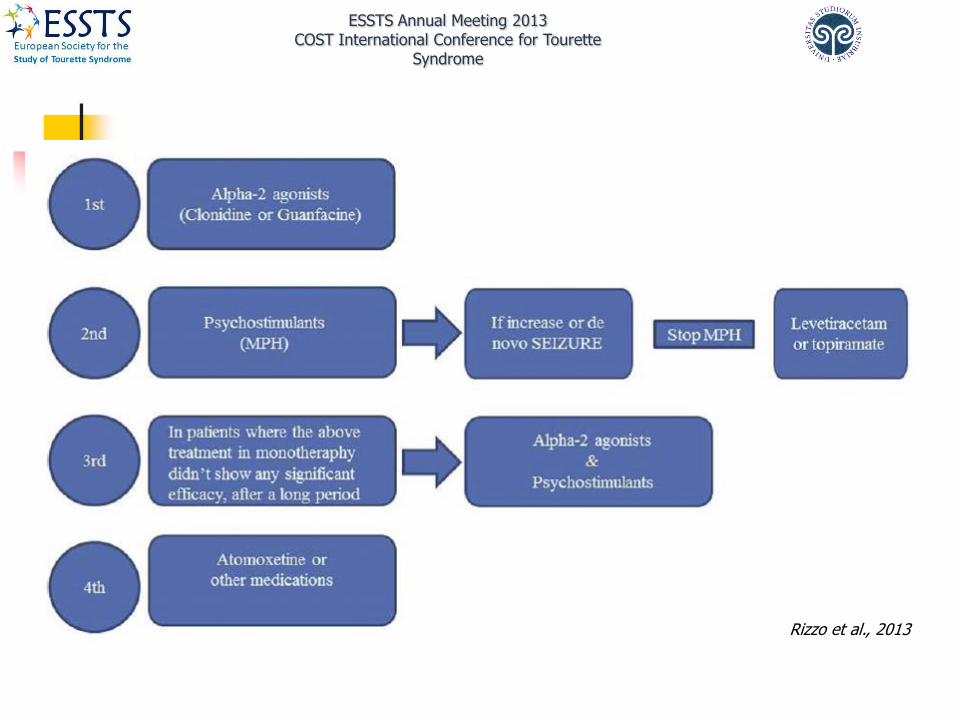
Treatment of comorbidities: ADHD
ESSTS Annual Meeting 2013 COST International Conference for Tourette
Syndrome
Rizzo et al., 2013
ESSTS Annual Meeting 2013 COST International Conference for Tourette
Syndrome
Rizzo et al., 2013

(1)
(2)
(3)

Registro regionale
Disturbi psichici N %
Disturbi dell'apprendimento 120 37
Disturbo oppositivo – provocatorio 38 12
Ansia 27 8
Disturbi dell’umore 6 2
Disturbi della condotta 5 2
Disturbi da tic / Sindrome di Tourette 7 2
Ritardo mentale 11 3
Disturbi dello spettro autistico 2 1
Dati
Internazionali
%
46
40
34
4
14
11
13
6
Tipo di comorbidità

COMORBIDITY:
the coexistence of two conditions
within a single individual (Feinstein, 1970)
- Current (at the time of study)
- Lifetime (over the course of an individual’s life)
Phenotypical heterochronia
varying expression of comorbidity over time (Nappi et al. 2000)



52
53