L’INCONTINENZA URINARIA E L’ATROFIA VAGINALE - medipro.it · In particolare l’incontinenza...
27
L’INCONTINENZA URINARIA E L’ATROFIA VAGINALE TRATTAMENTO FARMACOLOGICO E TRATTAMENTO LASER Bologna Sabato 30 Gennaio 2016 Strategie terapeutiche delle alterazioni della statica pelvica ed impatto sul costo sanitario Valerio M. Jasonni
Transcript of L’INCONTINENZA URINARIA E L’ATROFIA VAGINALE - medipro.it · In particolare l’incontinenza...

LrsquoINCONTINENZA URINARIA ELrsquoATROFIA VAGINALE
TRATTAMENTO FARMACOLOGICOE TRATTAMENTO LASER
Bologna Sabato 30 Gennaio 2016
Strategie terapeutiche delle alterazioni della statica pelvica ed impatto sul costo sanitario
Valerio M Jasonni
0
5
10
15
20
25
30
35
40
45
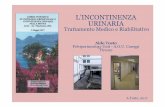
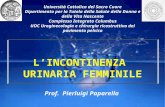
2000 2030
Italia donne con incontinenza proiezioni15-3 milioni donne con IU (ISTAT)
ISTAT 2006
bull Il 39 della popolazione femminile italiana ha piugrave di 50 anni
bull La spesa sanitaria per incontinenza urinaria egrave di 160 milioni di euro
bull 3 milioni di euro per traverse
bull 23 milioni per cateteri vescicali
Costi sanitari per anno
per incontinenza nelle donne
In Italia per donne gt 40 a3518 bilioni lire x anno
Considerando solo i farmaci e assorbenti
Pharmacoeconimics 2002
In USA $76 bilionianno se gt 65 a$36 bilionianno se lt 65 a
Brown et al Obstet Gynec 2001
USA ndash spesa annuale per IU donne 16 bilioni $ superiore alla spesa annuale
per Ca Mammella-Ovaio-Cervice uterina-Endmetrio complessivi
Leslee L et al 2006 Obstet Gynecol
USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
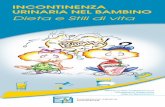
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

0
5
10
15
20
25
30
35
40
45
2000 2030
Italia donne con incontinenza proiezioni15-3 milioni donne con IU (ISTAT)
ISTAT 2006
bull Il 39 della popolazione femminile italiana ha piugrave di 50 anni
bull La spesa sanitaria per incontinenza urinaria egrave di 160 milioni di euro
bull 3 milioni di euro per traverse
bull 23 milioni per cateteri vescicali
Costi sanitari per anno
per incontinenza nelle donne
In Italia per donne gt 40 a3518 bilioni lire x anno
Considerando solo i farmaci e assorbenti
Pharmacoeconimics 2002
In USA $76 bilionianno se gt 65 a$36 bilionianno se lt 65 a
Brown et al Obstet Gynec 2001
USA ndash spesa annuale per IU donne 16 bilioni $ superiore alla spesa annuale
per Ca Mammella-Ovaio-Cervice uterina-Endmetrio complessivi
Leslee L et al 2006 Obstet Gynecol
USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

ISTAT 2006
bull Il 39 della popolazione femminile italiana ha piugrave di 50 anni
bull La spesa sanitaria per incontinenza urinaria egrave di 160 milioni di euro
bull 3 milioni di euro per traverse
bull 23 milioni per cateteri vescicali
Costi sanitari per anno
per incontinenza nelle donne
In Italia per donne gt 40 a3518 bilioni lire x anno
Considerando solo i farmaci e assorbenti
Pharmacoeconimics 2002
In USA $76 bilionianno se gt 65 a$36 bilionianno se lt 65 a
Brown et al Obstet Gynec 2001
USA ndash spesa annuale per IU donne 16 bilioni $ superiore alla spesa annuale
per Ca Mammella-Ovaio-Cervice uterina-Endmetrio complessivi
Leslee L et al 2006 Obstet Gynecol
USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Costi sanitari per anno
per incontinenza nelle donne
In Italia per donne gt 40 a3518 bilioni lire x anno
Considerando solo i farmaci e assorbenti
Pharmacoeconimics 2002
In USA $76 bilionianno se gt 65 a$36 bilionianno se lt 65 a
Brown et al Obstet Gynec 2001
USA ndash spesa annuale per IU donne 16 bilioni $ superiore alla spesa annuale
per Ca Mammella-Ovaio-Cervice uterina-Endmetrio complessivi
Leslee L et al 2006 Obstet Gynecol
USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

USA ndash spesa annuale per IU donne 16 bilioni $ superiore alla spesa annuale
per Ca Mammella-Ovaio-Cervice uterina-Endmetrio complessivi
Leslee L et al 2006 Obstet Gynecol
USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

USA Spesa annuale per incontinenza urinaria
=
Spesa per protesi cardiache + emodialisi
Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Classificazione clinica dellrsquoincontinenza urinaria
bullIncontinenza da sforzo (stress incontinence - IUS)
bullIncontinenza da urgenza (urge incontinence)
bullIncontinenza mista (stress - urge incontinence)
bullIncontinenza da rigurgito (overflow incontinence)
bullIncontinenza continua goccia a goccia (dribbling incontinence)
bullEnuresi notturna
bullIncontinenza funzionale
PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

PREVENZIONE PRIMARIARIVOLTA A TUTTE LE DONNE
INFORMAZIONI COMPORTAMENTALI
CONTROLLO CONSAPEVOLE DEI MUSCOLI PERINEALI
5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

5 milioni di donne sono portatrici di prolasso genitale con o senza
incontinenza urinaria
68 20-29dega18 30-50dega30 50-70dega
20-25 si rivolge allo specialista
Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Cost-Effectiveness of including a Nurse Specialist in the treatment
of Urinary Incontinence in Primary Care in the Netherlands
Holtzer-Goor et al PLoS One 2015
laquohellipsaving 402 euro x patientyear over 3 year period from a societal perspective
and reducing incontinencehellipraquo
Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Weight loss a novel and effective treatmentfor urinary incontinenceSubak et al J Urol 2005
laquoStress and urge incontinence decreased 60 after8 months weight loss in 40 obese overweight
patientsraquo
Decrease in urinary incontinence management costs in women enrolled in a clinical trial of weightloss to treat urinary incontinenceSubak et al Obeste Gynecol 2012
laquoMean cost decreased by 54 at 6 monthsand 81 at 18 months (77$ per week before)raquo
French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

French College of Gynecologists and Obstetricians
Pelvic muscle training is the treatment of first intention
Fauconnier et al Eur J Obst Reprod Bio 2010
LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

LrsquoAmerican Urologic Association raccomanda gli
esercizi e le tecniche di riabilitazione prima di ogni
intervento chirurgico che riguardi la sfera genitale
femminile In particolare lrsquoincontinenza urinaria
prima di essere trattata chirurgicamente deve essere
preceduta da tutti i presidi terapeutici non
chirurgici
Pelvic floor muscle training for urinary incontinence in womenHay-Smith EJ Boslash Berghmans LC Hendriks HJ de Bie RA van Waalwijk van Doorn ESDepartment of Womens and Childrens Health Dunedin School of Medicine University of Otago PO Box 913 Dunedin New Zealand
ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

ldquoThe review supports the widespreadRecommendation that
Pelvic Floor Muscle Training be includedas the first line treatment for women
With Stress-Urge or Mixed urinary incontinence
The treatment seemms greater in womenWith SUI alonerdquo
Cochrane database 2010Dumoulin amp Smith
The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

The Cochrane database of Systematic ReviewsSurgical management of pelvic organ prolapse
in womenMaher et al 2005
ldquonot enough evidence about the effects of differenttypes of surgery for pelvic organ prolapserdquo
ldquothe impact of pelvic organ prolapse surgery on bowelbladder and sexual function can be unpredicatablerdquo
2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

2 filosofie strategiche
Chirurgia del prolasso e della SUInello stesso tempo
Chirurgia del prolasso primaChirurgia specifica della SUI
in un secondo tempo(Mesh)
269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

269 operate per prolasso urogenitalefollow up 10 anni
Risultati oggettivi soddisfacenti 56-79
Risultati soggettivi soddisfacenti 46-73
Tegerstedt et al 2004
Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Difetto paravaginale
Difetto trasversale
Difetto centrale
Difetto del lig pubo-uretrale
Uretro-cistoceleRichardson
u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

u
pubo-urethral ligaments
Elevator Vagina
Arcus tendineus
LATERAL-CONNECTIVE
TISSUE
SLING
Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Outcomes after anterior vaginal wall repairwith mesh a randomized controlled trial
with 3 years follow upNieminen et al Am J Obstet Gynecol 2010
200 pazienti ricorrenza cistocele
Colporrafia = 40 su 97 (41)
Mesh = 14 su 105 (13)
Mesh erosioni = 19
FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

FDA Recommendations
Obtain specialized training for each mesh placement
Be vigilant for potential adverse eventsesp Erosion infection
Watch for complicationBladder-bowel-vessel perforations
Inform patients that may require additional surgerythat may or may not correct the complication
Inform patients about the potentialfor serious complications
A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

A decision-analytic model to compareThe cost-utility of anterior repair augmentedwith aynthetic mesh compared with non-mesh
repair in women with surgically treated prolapseJacklin P et al BJOG 2013
laquoat 5 years the incrementalcost-effectiveness ratio for mesh anteriorrepair was pound15 million including costs of
mesh and treating mesh erosionuse of mesh seems not cost-effectiveraquo
Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Anterior colporraphy vs transvaginal meshfor pelvic-organ prolpaseAltman et al N EnglJ Med 2011
STUDY ON 389 WOMENAs compared with anterior colporraphy use of a standardized trocar-guided mesh kit for cystocele repair resulted in highershort-term rates of successul treatment but
also in higher rates of surgicalcomplications and postoperative adverse events
Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Radiofrequency collagen denaturationin SUI attributable to hypermobility
as first approach or in case of suboptimalsurgical results
Apple amp Davila Curr MedRes Opin 2007
Transurethral radiofrequency energy collagenmicro-remodelling for female SUI
110 cases SUI moderate to severe74 well resolved
Appell et al Neurol Urodyn 2006
Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

Cost utility analysis of urethral bulking agents vs Midurethral sling in stress urinary incontinence
Kunkle CM et al Female pelvic Med Reconstr Surg 2015
SUI without urethral hypermobiltyBulking agents more cost effective
CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi

CONCLUSIONI
Lrsquoincontinenza urinaria egrave un problema negletto nonostante lrsquoenorme spesa sanitaria
La prevenzione parte da lontano
Adeguata ginnastica perineale in gravidanza e dopo Mantenere il peso corporeo nei limiti
Prevenire lrsquoatrofia vaginale Ricordare che molte pazienti non la riferiscono e quindi
accurata anamnesi