LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI TERAPEUTICI · LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI...
51
Gruppo di Ricerca Geriatrica Seminari del venerdì LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI TERAPEUTICI 17 maggio 2013 Luca Serchisu
Transcript of LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI TERAPEUTICI · LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI...

Gruppo di Ricerca Geriatrica Seminari del venerdì
LE DISLIPIDEMIE NELL’ANZIANO: ASPETTI TERAPEUTICI
17 maggio 2013 Luca Serchisu

The cholesterol controversy Lipid
hypothesis Virchow
Phl Thromb G
1856 1929
Macheboeuf MA. BullSocChimBiol
Lipoproteine Rabbits
cholesterol Ignatowski, A.
Virchows ArchPatholAnat
1909 1967
Fredrickson Classification
NEJM 1946
Framingham Study
Steinberg D. J Lipid Res 2004
1961
AHA Diet
Recommendations
- “Reduction of raised serum cholesterol is a card of uncertain quality in the primary prevention of [coronary heart disease]” - “Reduction of raised serum cholesterol could lead to adverse biological changes”
Oliver MF. Serum-cholesterol the knave of hearts and the joker. Lancet 1981
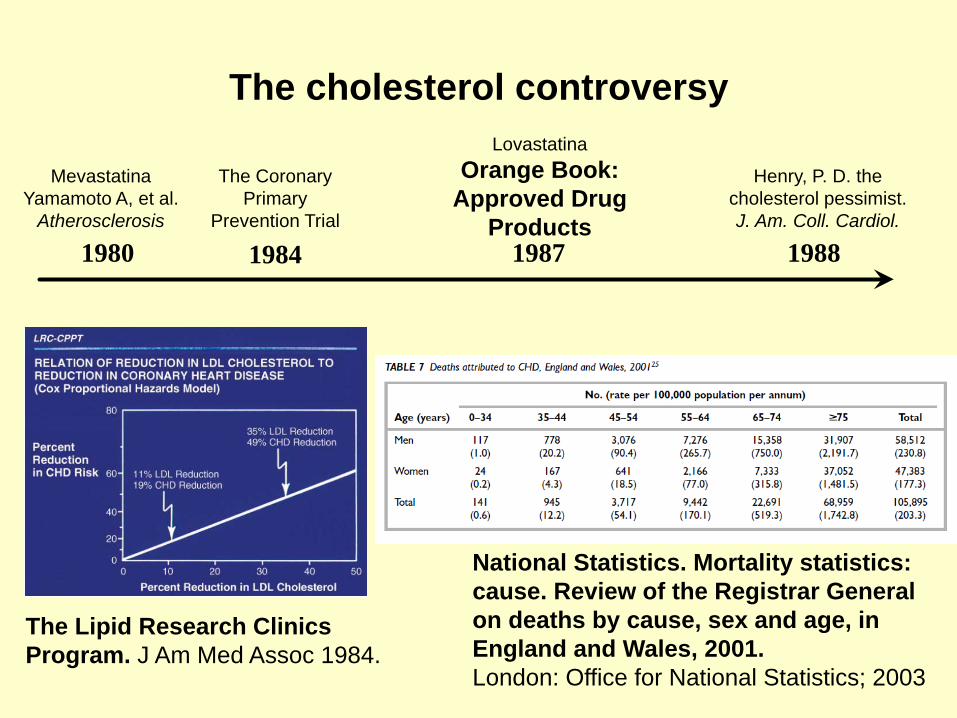
The cholesterol controversy
1984
Henry, P. D. the cholesterol pessimist. J. Am. Coll. Cardiol.
The Lipid Research Clinics Program. J Am Med Assoc 1984.
The Coronary Primary
Prevention Trial
Mevastatina Yamamoto A, et al.
Atherosclerosis
1980 1987
Lovastatina Orange Book:
Approved Drug Products
National Statistics. Mortality statistics: cause. Review of the Registrar General on deaths by cause, sex and age, in England and Wales, 2001. London: Office for National Statistics; 2003
1988
ESC/EAS Guidelines for the management of dyslipidaemias
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J 2011
“These guidelines deal with the management of dyslipidemias as an essential and integral part of CDV prevention”
Summary
•Significato del rischio CVD in età geriatrica
•Correlazione dislipidemie e CVD in età geriatrica
•Prevenzione CVD nel paziente anziano
•Dislipidemie nell’anziano nefropatico
•Dislipidemie nell’anziano demente
•Peculiarità della terapia farmacologica
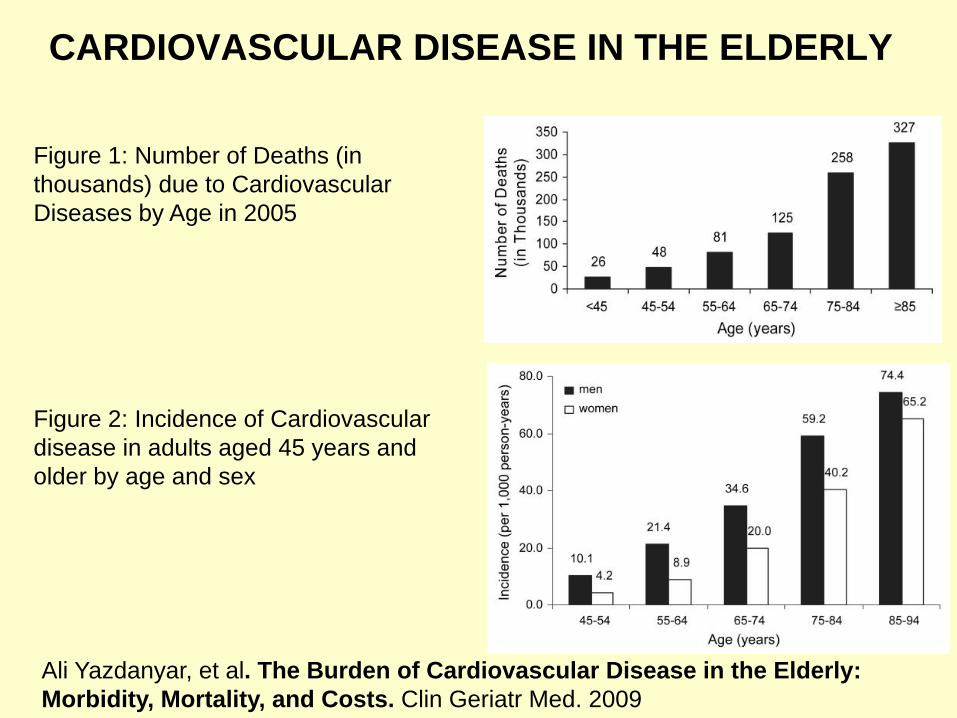
CARDIOVASCULAR DISEASE IN THE ELDERLY
Figure 1: Number of Deaths (in thousands) due to Cardiovascular Diseases by Age in 2005
Figure 2: Incidence of Cardiovascular disease in adults aged 45 years and older by age and sex
Ali Yazdanyar, et al. The Burden of Cardiovascular Disease in the Elderly: Morbidity, Mortality, and Costs. Clin Geriatr Med. 2009
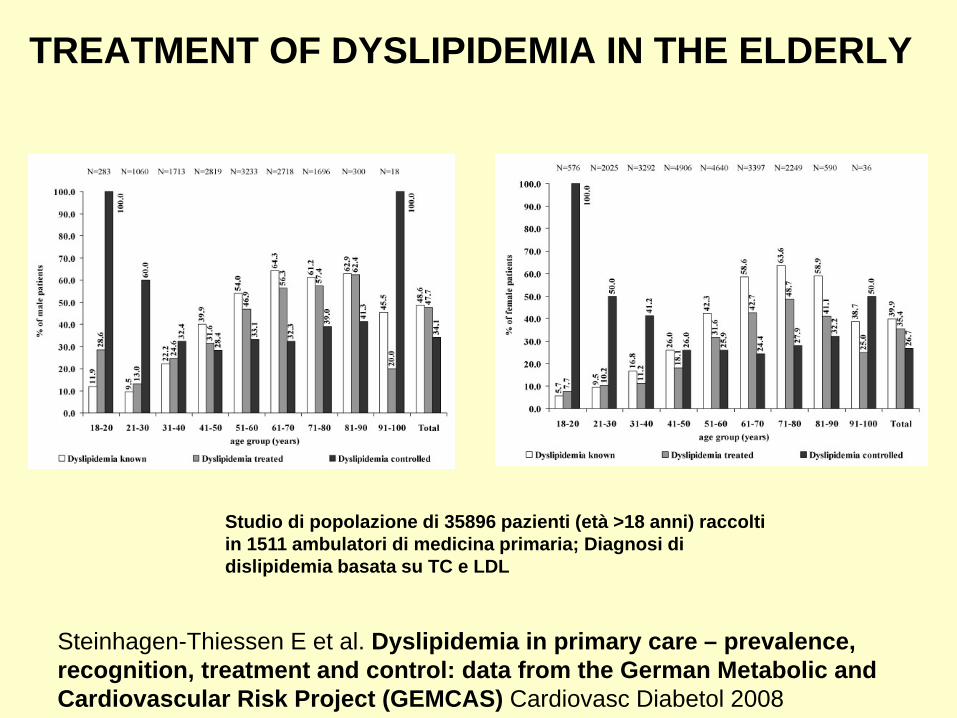
TREATMENT OF DYSLIPIDEMIA IN THE ELDERLY
Steinhagen-Thiessen E et al. Dyslipidemia in primary care – prevalence, recognition, treatment and control: data from the German Metabolic and Cardiovascular Risk Project (GEMCAS) Cardiovasc Diabetol 2008
Studio di popolazione di 35896 pazienti (età >18 anni) raccolti in 1511 ambulatori di medicina primaria; Diagnosi di dislipidemia basata su TC e LDL

Steinhagen-Thiessen E et al. Dyslipidemia in primary care – prevalence, recognition, treatment and control: data from the German Metabolic and Cardiovascular Risk Project (GEMCAS) Cardiovasc Diabetol 2008
Età Tot pz dislip
Pz Prev sec
Pz Prev sec %
18-20 559 2 0,4
21-30 3085 14 0,5
31-40 5005 62 1,2
41-50 7725 343 4,4
51-60 7873 970 12,3
61-70 6615 1509 22,8
71-80 3945 1514 38,4
81-90 890 414 46,5
91-100 54 23 42,6
Tot 35192 4849 13,8
TREATMENT OF DYSLIPIDEMIA IN THE ELDERLY

DYSLIPIDEMIA IN THE ELDERLY
Schatz IJ, Masaki K et al. Cholesterol and all-cause mortality in elderly people from the Honolulu Heart Program: a cohort study. Lancet 2001
Honolulu Heart Program •Studio di popolazione su in 3572 maschi americani e giapponesi (età 71-93 anni); Relazione tra livello di colesterolo e mortalità globale •Riduzione dei livelli plasmatici di colesterolo medi con l’aumentare dell’età (193 mg/dl nei soggetti di 71-74 anni; 178 mg/dl in quelli di > 84 anni) •Confrontando il livello di colesterolo misurato 20 anni prima con il livello attuale, il gruppo di soggetti con livelli bassi in tutte e due le occasioni aveva un rischio di mortalità significativamente maggiore rispetto ai soggetti con livelli intermedi o alti di colesterolo in entrambe le misurazioni.

Schatz IJ et al. Lancet 2001
DYSLIPIDEMIA IN THE ELDERLY
(150 mg/dl)
(180 mg/dl)
(200 mg/dl)
(230 mg/dl)
-Cuchel M, Rader DJ. Lancet. 2001 Dec 1; 358(9296):1903-4; author reply 1906.
-Tilvis RS, Strandberg TE, Miettinen TA. Lancet. 2001 Dec 1; 358(9296):1904-5; author reply 1906 -Law M, Wald NJ. Lancet. 2001 Dec 1; 358(9296):1904; author reply 1906.
-Terao T. Lancet. 2001 Dec 1; 358(9296):1905; author reply 1906.
-Weverling-Rijnsburger AW, Blauw GJ, Westendorp RG. Lancet. 2001 Dec 1; 358(9296):1905-6.
-Fernandez-Real JM, Ricart W. Lancet. 2001 Dec 1; 358(9296):1906-7.
-Ravnskov U. Lancet. 2001 Dec 1; 358(9296):1907.
Correspondence
DYSLIPIDEMIA IN THE ELDERLY
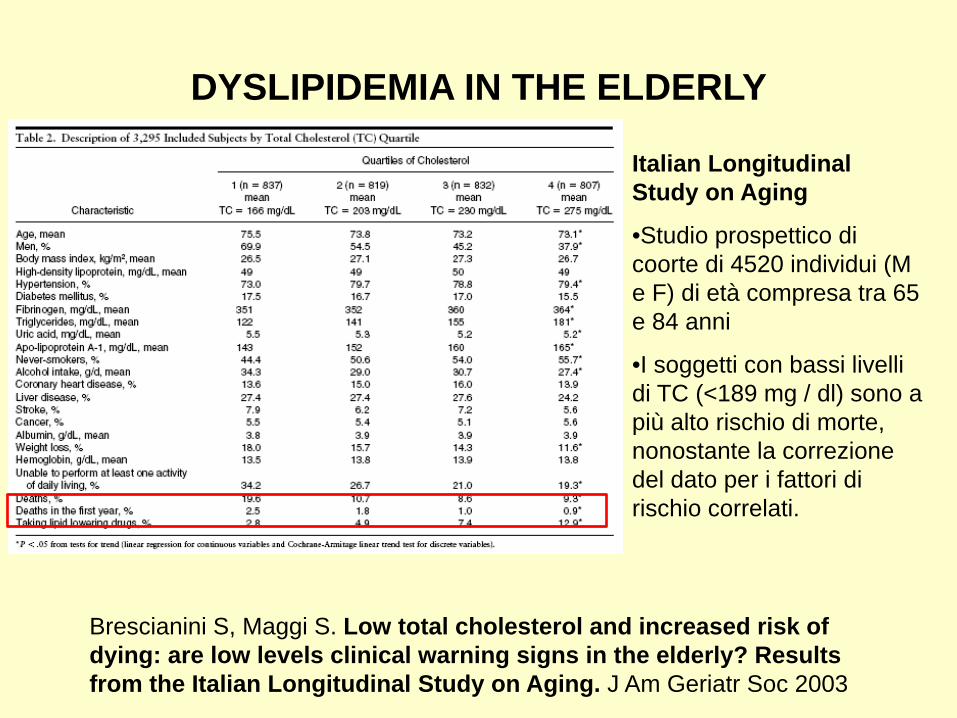
Brescianini S, Maggi S. Low total cholesterol and increased risk of dying: are low levels clinical warning signs in the elderly? Results from the Italian Longitudinal Study on Aging. J Am Geriatr Soc 2003
Italian Longitudinal Study on Aging
•Studio prospettico di coorte di 4520 individui (M e F) di età compresa tra 65 e 84 anni
•I soggetti con bassi livelli di TC (<189 mg / dl) sono a più alto rischio di morte, nonostante la correzione del dato per i fattori di rischio correlati.
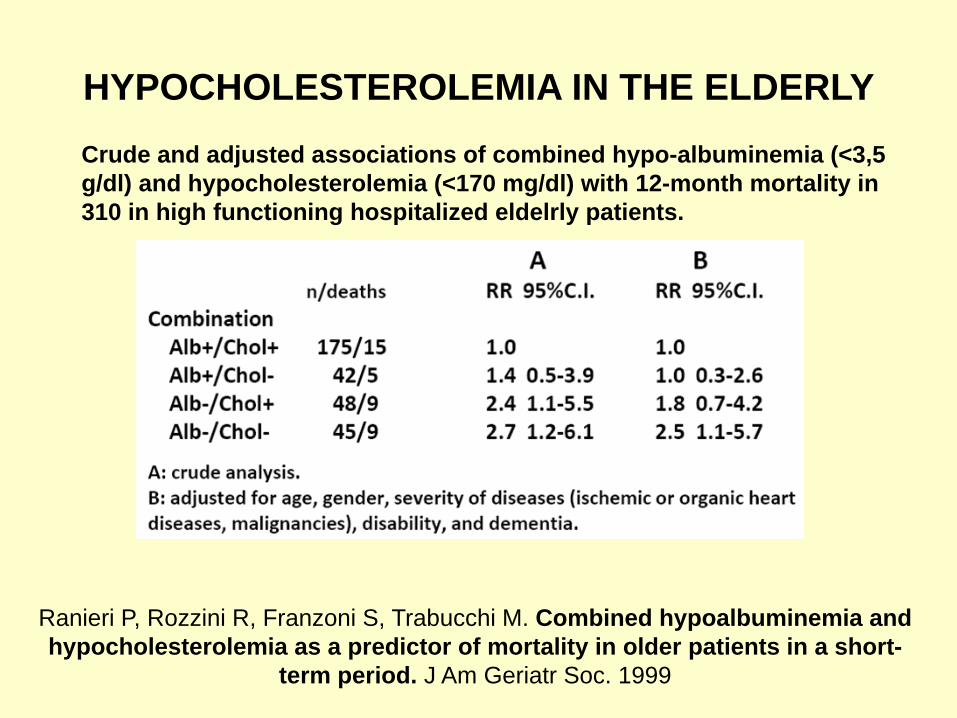
HYPOCHOLESTEROLEMIA IN THE ELDERLY
Ranieri P, Rozzini R, Franzoni S, Trabucchi M. Combined hypoalbuminemia and hypocholesterolemia as a predictor of mortality in older patients in a short-
term period. J Am Geriatr Soc. 1999
Crude and adjusted associations of combined hypo-albuminemia (<3,5 g/dl) and hypocholesterolemia (<170 mg/dl) with 12-month mortality in 310 in high functioning hospitalized eldelrly patients.
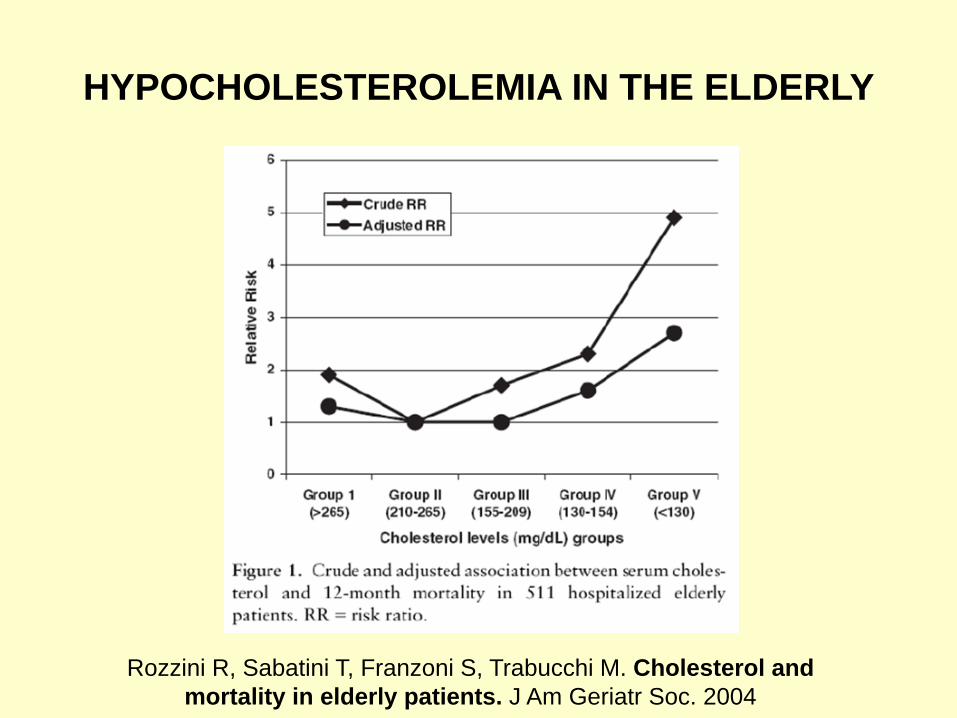
HYPOCHOLESTEROLEMIA IN THE ELDERLY
Rozzini R, Sabatini T, Franzoni S, Trabucchi M. Cholesterol and mortality in elderly patients. J Am Geriatr Soc. 2004
DYSLIPIDEMIA IN THE ELDERLY
People aged 80 or older are the fastest growing population in high-income countries. One of the most common causes of death among the elderly is the cardiovascular disease (CVD). Lipid-lowering treatment is common, e.g. one-third of 75-84-year-old Swedes are treated with statins. The assumption that hypercholesterolaemia is a risk factor at the highest ages seems to be based on extrapolation from younger adults. A review of observational studies shows a trend where all-cause mortality was highest when total cholesterol (TC) was lowest ('a reverse J-shaped' association between TC and all-cause mortality). Low TC (<5.5 mmol/l) is associated with the highest mortality rate in 80+-year olds. No clear optimal level of TC was identified. A review of the few randomised controlled trials including 80+-year olds did not provide evidence of an effect of lipid-lowering treatment on total mortality in 80+-year-old people. There is not sufficient data to recommend anything regarding initiation or continuation of lipid-lowering treatment for the population aged 80+, with known CVD, and it is even possible that statins may increase all-cause mortality in this group of elderly individuals without CVD.
Petersen LK, Christensen K, Kragstrup J. Lipid-lowering treatment to the end? A review of observational studies and RCTs on cholesterol and mortality in 80+-year olds. Age Ageing 2010
DYSLIPIDEMIA IN THE ELDERLY
Petursson H, Sigurdsson JA et al. Is the use of cholesterol in mortality risk algorithms in clinical guidelines valid? Ten years prospective data from the
Norwegian HUNT 2 study. J Eval Clin Pract 2012
• Bassi livelli di colesterolemia (<213 mg/dl) sono associati ad aumentata mortalità per tutte le cause nei soggetti ultraottantenni
• Nessun trial clinico randomizzato ha dimostrato che un trattamento ipolipemizzante riduce la mortalità per tutte le cause negli ultraottantenni
• E’ possibile che le statine aumentino la mortalità per tutte le cause negli anziani senza una patologia dell’apparato cardiovascolare in atto (Goldstein et al. J Am Geriatr Soc. 2008)
• Nella decade 70-80 anni tre trial su sei affermano che il trattamento con statine riduce la mortalità da malattia cardiovascolare
• Non è stato ancora individuato un valore target di colesterolemia nell’ultraottantene
• Non sufficienti evidenze per esprimere indicazioni sul trattamento ipolipemizzante nell’ultraottantenne
HUNT 2 Study: Studio di popolazione di 52087 Norvegesi (età 20-74 anni); Follow-up per mortalità da cause specifiche; durata 10 anni
DYSLIPIDEMIA IN THE ELDERLY
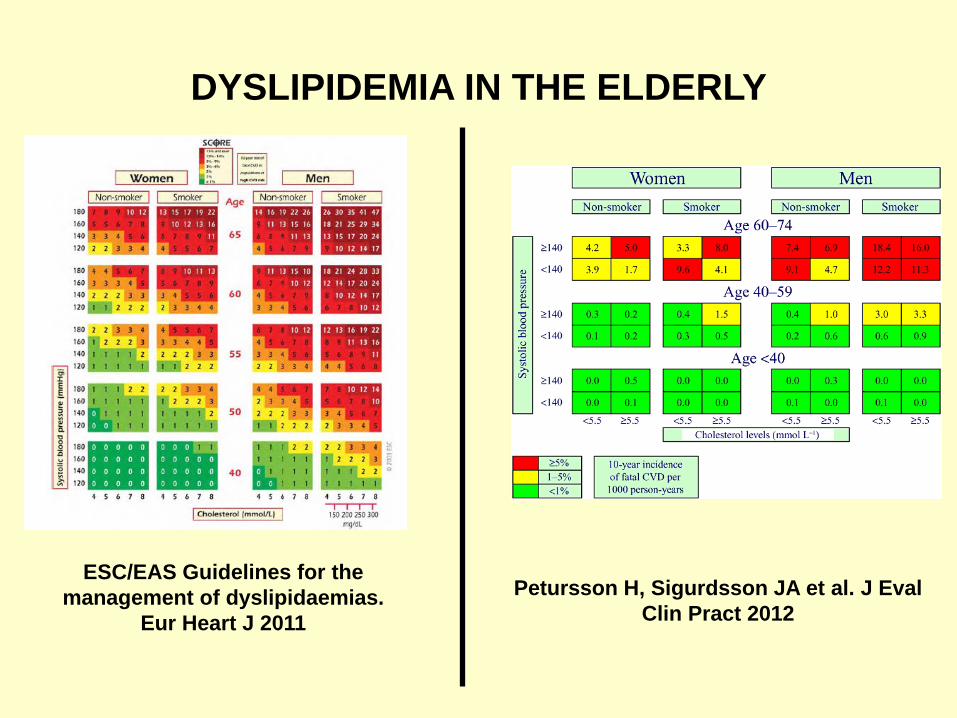
Petursson H, Sigurdsson JA et al. J Eval Clin Pract 2012
ESC/EAS Guidelines for the management of dyslipidaemias.
Eur Heart J 2011
DYSLIPIDEMIA IN THE ELDERLY
• Risk reduction in individuals older than 65 years is essential because two-thirds to three-quarters of them have either clinical CAD or subclinical atherosclerotic disease.
• Evidence for treatment above the age of 80–85 years is very limited, and clinical judgement should guide decisions in the very old.
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J 2011
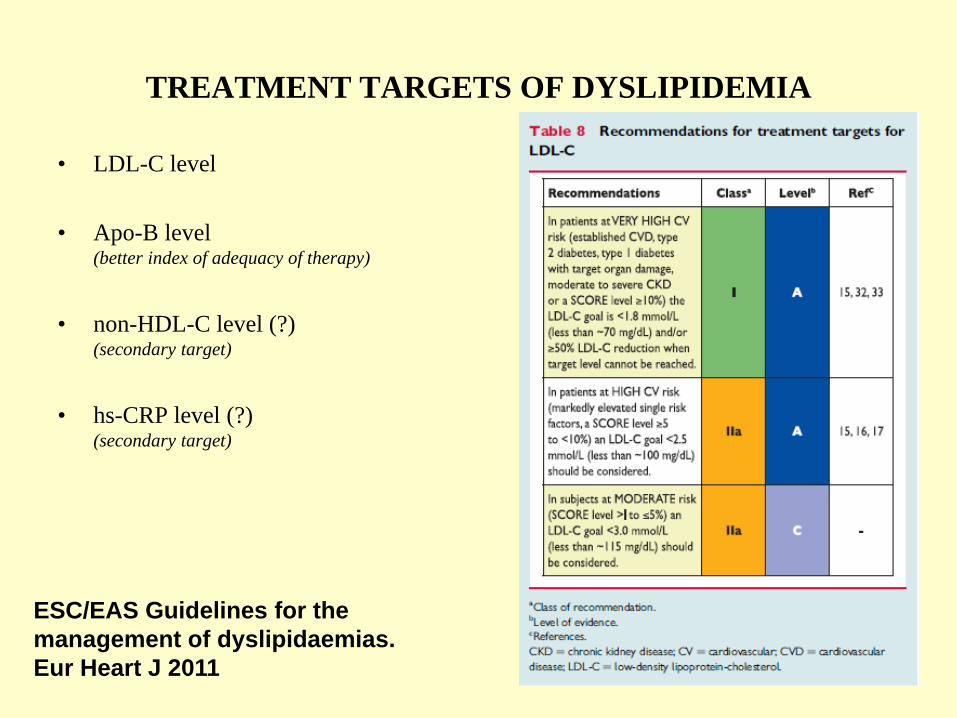
• LDL-C level
• Apo-B level (better index of adequacy of therapy)
• non-HDL-C level (?)
(secondary target)
• hs-CRP level (?)
(secondary target)
TREATMENT TARGETS OF DYSLIPIDEMIA
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J 2011
• Higher HDL-C levels have been associated with a lower risk of CVD
• HDL-C has been associated with increased longevity in some cohorts (>80 yo)
TREATMENT TARGETS OF DYSLIPIDEMIA
Rahilly-Tierney C, Sesso H et al. High-density lipoprotein and mortality before age 90 years in male physicians. Circ Cardiovasc Qual Outcomes 2012
• After adjusting for other factors previously associated with longevity, higher HDL-C levels were significantly associated with survival to age 90 in the PHS (Physicians’ Health Study )
• HDL-C likely increases survival to exceptionally old age by protecting against CVD death, the most prevalent cause of death
Rahilly-Tierney C, Sesso HD, Djoussé L, Gaziano JM. Lifestyle changes and 14-year change in high-density lipoprotein cholesterol in a cohort of male physicians. Am Heart J. 2011

WHAT TREATMENT TARGETS IN ELDERLY?
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J 2011
PRIMARY PREVENTION
Regole comportamentali • Smettere di fumare, dieta per dislipidemie, praticare
esercizio fisico, controllo peso corporeo
Studio PROSPER (PROspective Study of Pravastatin in the
Elderly at Risk) (5804 pazienti (M e F) con fattori di rischio per CVD (età 70-82 anni) in terapia con pravastatina confrontati con gruppo trattato con placebo)
• Nessuna riduzione della mortalità totale o riduzione del deterioramento cognitivo

SECONDARY PREVENTION
Studio 4 S (Scandinavian Simvastatin Survival Study) (4444 pazienti scandinavi (M e F) con angina pectoris o pregresso
IMA (età 35-70 anni), in regime dietetico ipolipidico, in terapia con simvastatina confrontati con gruppo trattato con placebo)
• Riduzione della mortalità totale (35%) e mortalità per cardiopatia ischemica (42%) nei pazienti trattati con pravastatina rispetto al placebo, dopo 5 anni, in individui ≥60 anni M e F
Studio CARE (Cholesterol and Recurrent Events) (4159 pazienti (M e F) con pregresso IMA e CT<240 mg/dl (età 21-
75 anni), in terapia con pravastitina 40 mg/die confrontati con gruppo trattato con placebo)
• Riduzione di sindromi coronariche acute (32%), decessi secondari a coronaropatia (45%) e stroke (40%)
DISLIPIDEMIE E RENE • The percentage reduction of TC with statins in CKD is less than the
general population • Statins were associated with reduced risk of incident or recurrent CV
events • Statins improve all-cause mortality in patients with or without
established CVD
Sheng X, Murphy MJ et al. Effectiveness of statins in chronic kidney disease. QJM. 2012
Choudhury D, Tuncel M et al. Disorders of Lipid Metabolism and Chronic Kidney Disease in the Elderly. Semin Nephrol. 2009
• Incremento esponenziale del rischio di CVD maggiore in pazienti anziani con Dislipidemia e Malattia Renale Cronica
• La dislipidemia potrebbe favorire la progressione della malattia renale cronica
• Nelle fasi precoci di malattia renale la terapia con statine sembra ridurre il rischio di CVD
• Nella malattia renale in fase terminale la terapia con statine non pare migliorare la mortalità

DISLIPIDEMIE E RENE
Levin A et al. Guidelines for the management of chronic kidney disease. CMAJ 2008
DISLIPIDEMIE E MEMORIA
• Influenza del genotipo APO-E e AD Genin E, Hannequin D, Wallon D et al. APOE and Alzheimer disease: a major gene with semi-dominant inheritance. Mol Psychiatry 2011; 16:903-7. Kuszczyk MA, Sanchez S et al. Blocking the Interaction between Apolipoprotein E and Aβ Reduces Intraneuronal Accumulation of Aβ and Inhibits Synaptic Degeneration. Am J Pathol. 2013
• Ruolo presunto delle statine nella prevenzione e terapia di AD (ridotta amiloidogenesi a seguito di ridotta neuroinfiammazione e blocco della funzione delle secretasi) Lloyd DG et al. Statins: the role in the treatment and prevention of Alzheimer's neurodegeneration. Pac-Soo C, J Alzheimers Dis. 2011.

DISLIPIDEMIE E MEMORIA
• The Rotterdam Study mostra evidenze su un ruolo protettivo delle statine nei confronti della Malattia di Alzheimer (riduzione del rischio di sviluppare AD nei pz trattati con statine (HR 0,57) rispetto ai pz non trattati o trattati con altri farmaci ipolipemizzanti (HR 1,05)) (Rotterdam Study: 6992 individui (M e F, età >45 anni). Valutazione delle nuove diagnosi di AD) Zamrini E, McGwin G, Roseman JM. Association between statin use and Alzheimer's disease. Neuroepidemiology. 2004
Haag MD, Hofman A. Statins are associated with a reduced risk of Alzheimer disease regardless of lipophilicity. The Rotterdam Study. J Neurol Neurosurg Psychiatry. 2009
• Gli studi PROSPER e HPS (Heart Protection Study) non mostrano evidenza che la terapia con statine può prevenire la demenza McGuinness B, Craig D, Bullock R, Passmore P. Statins for the prevention of dementia. Cochrane Database Syst Rev 2009
Sano M, Bell KL, Galasko D et al. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology 2011
Feldman HH, Doody RS, Kivipelto M et al. Randomized controlled trial of atorvastatin in mild to moderate Alzheimer disease: LEADe. Neurology 2010
DISLIPIDEMIE E MEMORIA
Zuliani G, Cavalieri M et al. Relationship Between Low Levels of High-Density Lipoprotein Cholesterol and Dementia in the Elderly. The InChianti Study. J Gerontol A Biol Sci Med Sci. 2010
Inchianti Study: Studio prospettico di 1260 individui (M e F) di età compresa tra 65 e 102 anni; Valutazione profilo lipidico e diagnosi di demenza effettuata attraverso i criteri DMS IV basale e a tre anni
•I pazienti affetti da demenza mostravano livelli significativamente inferiori di Colesterolemia Totale, non-HDL Colesterolo e HDL Colesterolo rispetto ai controlli non dementi.
•Non è stata riscontrata una differenza significativa tra i gruppi per la Trigliceridemia e i livelli di Lipoproteina (a).
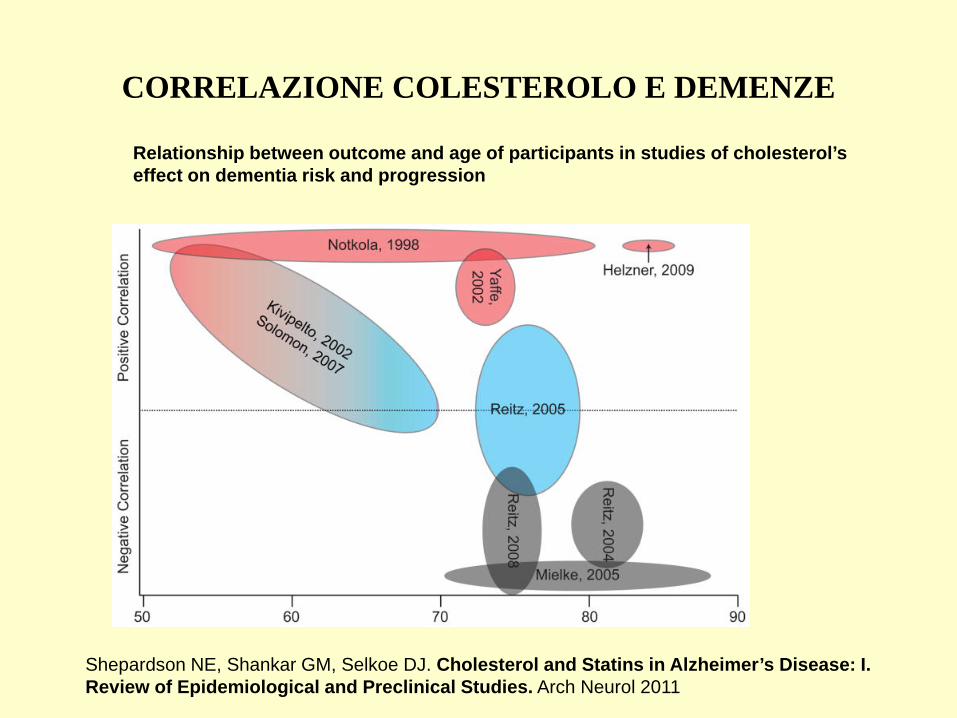
CORRELAZIONE COLESTEROLO E DEMENZE
Relationship between outcome and age of participants in studies of cholesterol’s effect on dementia risk and progression
Shepardson NE, Shankar GM, Selkoe DJ. Cholesterol and Statins in Alzheimer’s Disease: I. Review of Epidemiological and Preclinical Studies. Arch Neurol 2011
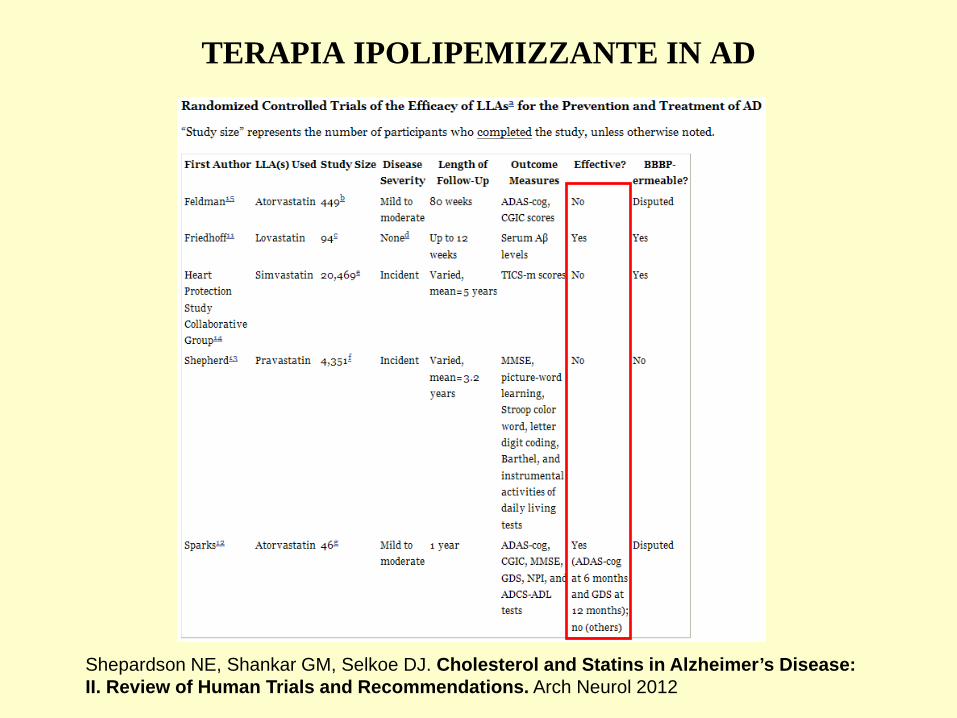
TERAPIA IPOLIPEMIZZANTE IN AD
Shepardson NE, Shankar GM, Selkoe DJ. Cholesterol and Statins in Alzheimer’s Disease: II. Review of Human Trials and Recommendations. Arch Neurol 2012

STATINE E PREVENZIONE DECADIMENTO COGNITIVO
Sánchez-Ferro A, Benito-León J et al. A review of the potential therapeutic role of statins in the treatment of Alzheimer’s disease: current research and opinion. Neuropsychiatr Dis Treat 2013
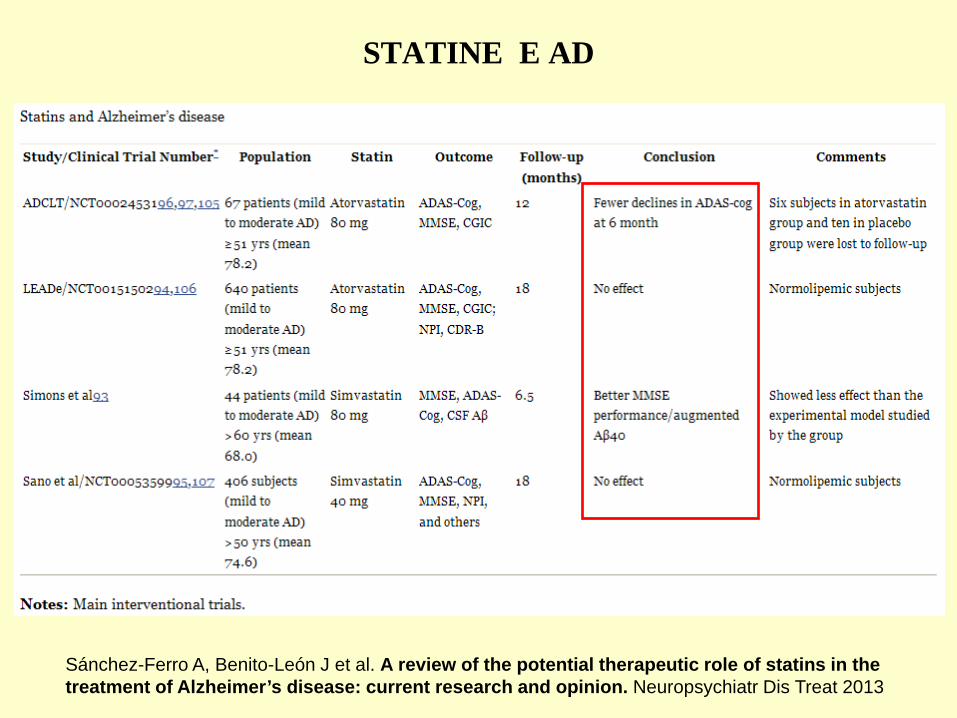
STATINE E AD
Sánchez-Ferro A, Benito-León J et al. A review of the potential therapeutic role of statins in the treatment of Alzheimer’s disease: current research and opinion. Neuropsychiatr Dis Treat 2013
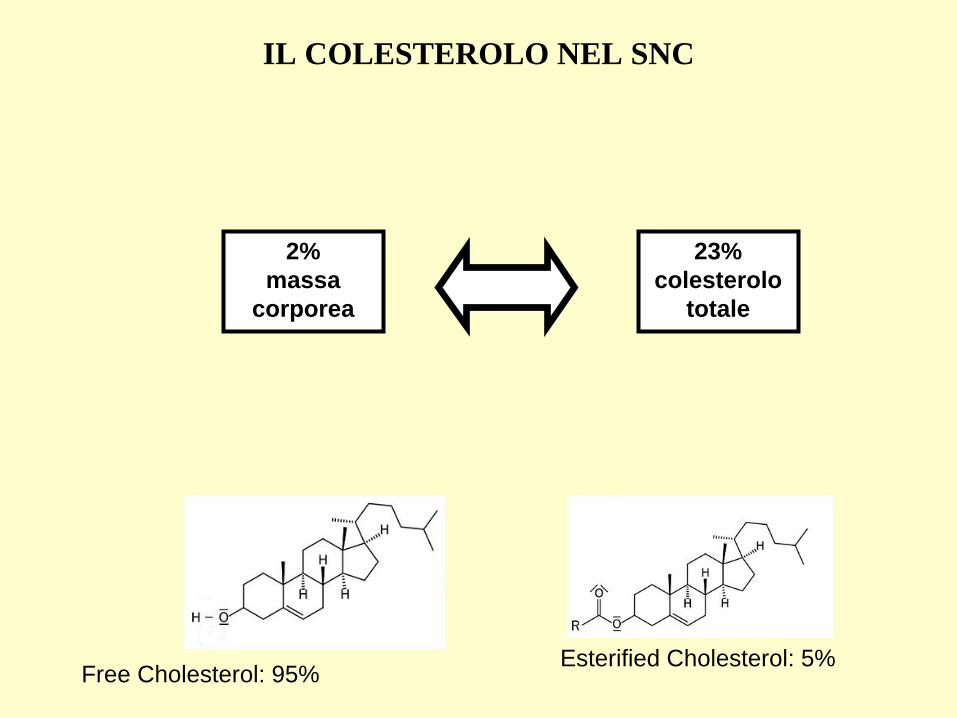
23% colesterolo
totale
2% massa
corporea
IL COLESTEROLO NEL SNC
Free Cholesterol: 95% Esterified Cholesterol: 5%
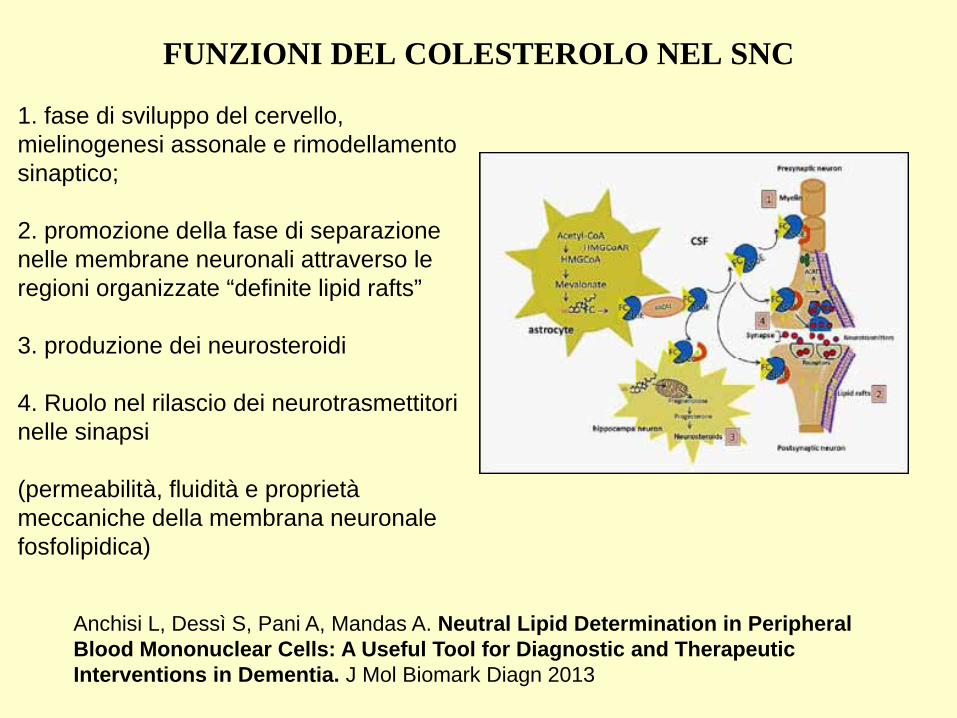
1. fase di sviluppo del cervello, mielinogenesi assonale e rimodellamento sinaptico; 2. promozione della fase di separazione nelle membrane neuronali attraverso le regioni organizzate “definite lipid rafts” 3. produzione dei neurosteroidi 4. Ruolo nel rilascio dei neurotrasmettitori nelle sinapsi (permeabilità, fluidità e proprietà meccaniche della membrana neuronale fosfolipidica)
FUNZIONI DEL COLESTEROLO NEL SNC
Anchisi L, Dessì S, Pani A, Mandas A. Neutral Lipid Determination in Peripheral Blood Mononuclear Cells: A Useful Tool for Diagnostic and Therapeutic Interventions in Dementia. J Mol Biomark Diagn 2013
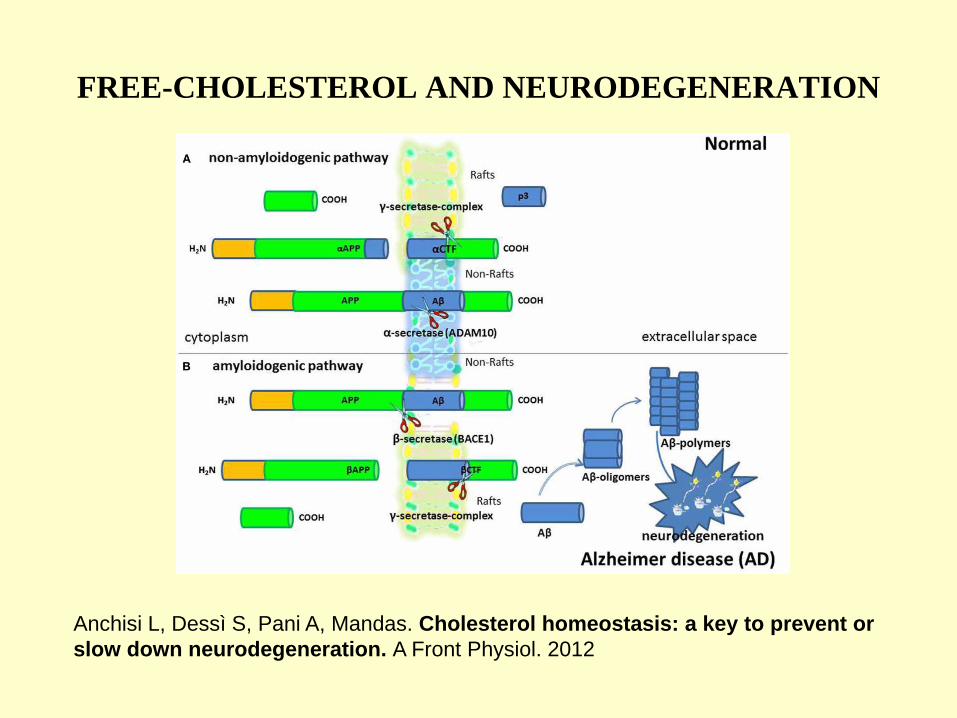
FREE-CHOLESTEROL AND NEURODEGENERATION
Anchisi L, Dessì S, Pani A, Mandas. Cholesterol homeostasis: a key to prevent or slow down neurodegeneration. A Front Physiol. 2012

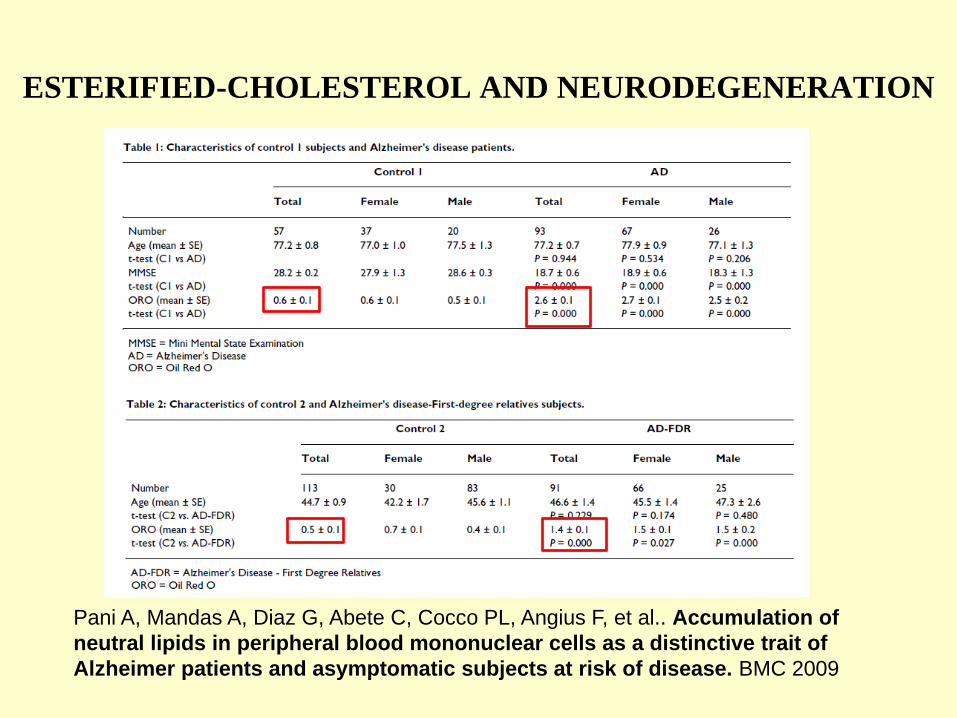
ESTERIFIED-CHOLESTEROL AND NEURODEGENERATION
Pani A, Norfo C, Abete C, Mulas C, Putzolu M, Laconi S et al. Antiprionactivity of cholesterol esterification modulators: a comparative study using ex vivo sheep fibroblasts and lymphocytes and mouse neuroblastoma cell lines. Antimicrob Agents Chemother 2007 Pani A, Norfo C, Abete C, Mulas C, Putzolu M, Laconi S et al. Accumulation of cholesterol esters in ex vivo lymphocytes from scrapie-susceptibles heep and inscrapie-infected mouse neuroblastoma cell lines. Am J Infec Dis 2007. Pani A, Abete C, Norfo C, Mulas C, Putzolu M, Laconi S et al. Cholesterol metabolism in brain and skin fibroblasts from Sarda breed sheep with scrapie-resistant and scrapie-susceptible genotypes. Am J Infec Dis 2008. Pani A, Dessì S, Diaz G, LaColla P, Abete C, Mulas C et al. Altered cholesterol ester cycle in skin fibroblasts from patients with Alzheimer’s disease. J Alzheimers Dis 2009.
ESTERIFIED-CHOLESTEROL AND NEURODEGENERATION
Pani A, Mandas A, Diaz G, Abete C, Cocco PL, Angius F, et al.. Accumulation of neutral lipids in peripheral blood mononuclear cells as a distinctive trait of Alzheimer patients and asymptomatic subjects at risk of disease. BMC 2009

ESTERIFIED-CHOLESTEROL AND AUTISTIC DISORDERS
Anchisi L, Dessì S, Pani A, Mandas A. Neutral Lipid Determination in Peripheral Blood Mononuclear Cells: A Useful Tool for Diagnostic and Therapeutic Interventions in Dementia. J Mol Biomark Diagn 2013

CHOLESTEROL LEVELS AND NEURODEGENERATION
Anchisi L, Dessì S, Pani A, Mandas. Cholesterol homeostasis: a key to prevent or slow down neurodegeneration. A Front Physiol. 2012
•Alcuni studi sostengono che bassi livelli di colesterolo avrebbero un ruolo protettivo nei confronti dell’amiloidogenesi in quanto allontanerebbero le APP dalle lipid raft.
•Tuttavia si tratta di studi limitati, eseguiti su colture di cellule di neuroblastoma e neuroni ippocampali esprimenti la mutazione amiloidogenica svedese per il gene APP
•E’ stato osservato che in molti disordini neurodegenerativi c’è un difetto nel metabolismo del colesterolo, così come nell’ippocampo dei pazienti AD è presente una moderata ma significativa riduzione del colesterolo di membrana (Abad Rodriguez 2004). •Topi modificati geneticamente incapaci di sintetizzare colesterolo hanno severi disturbi nella mielinogenesi, atassia e tremore. (Saher 2005)
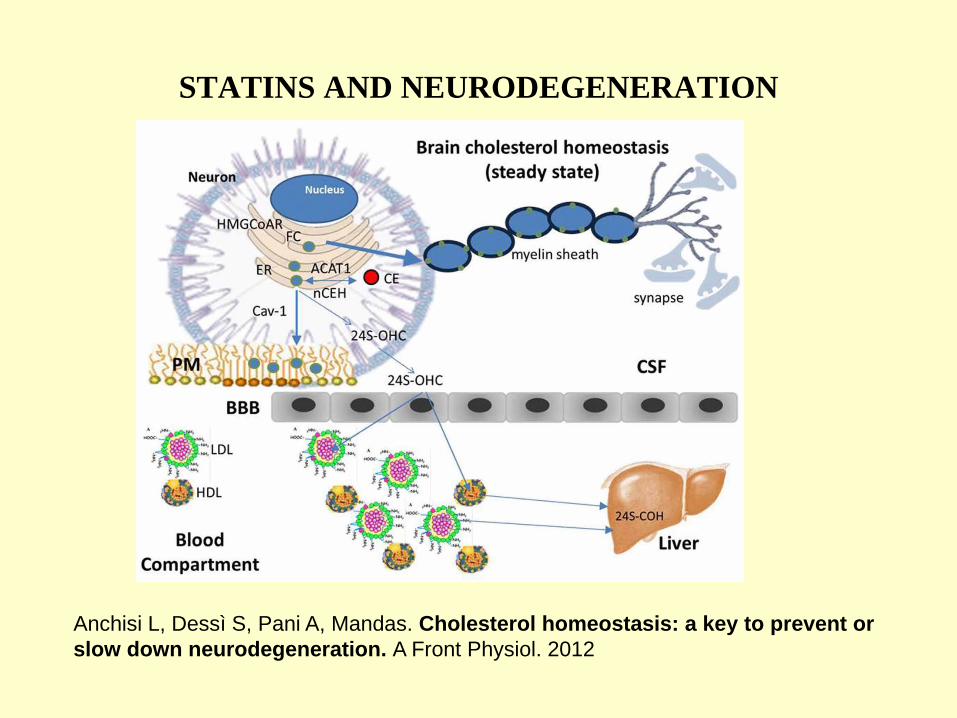
STATINS AND NEURODEGENERATION
Anchisi L, Dessì S, Pani A, Mandas. Cholesterol homeostasis: a key to prevent or slow down neurodegeneration. A Front Physiol. 2012
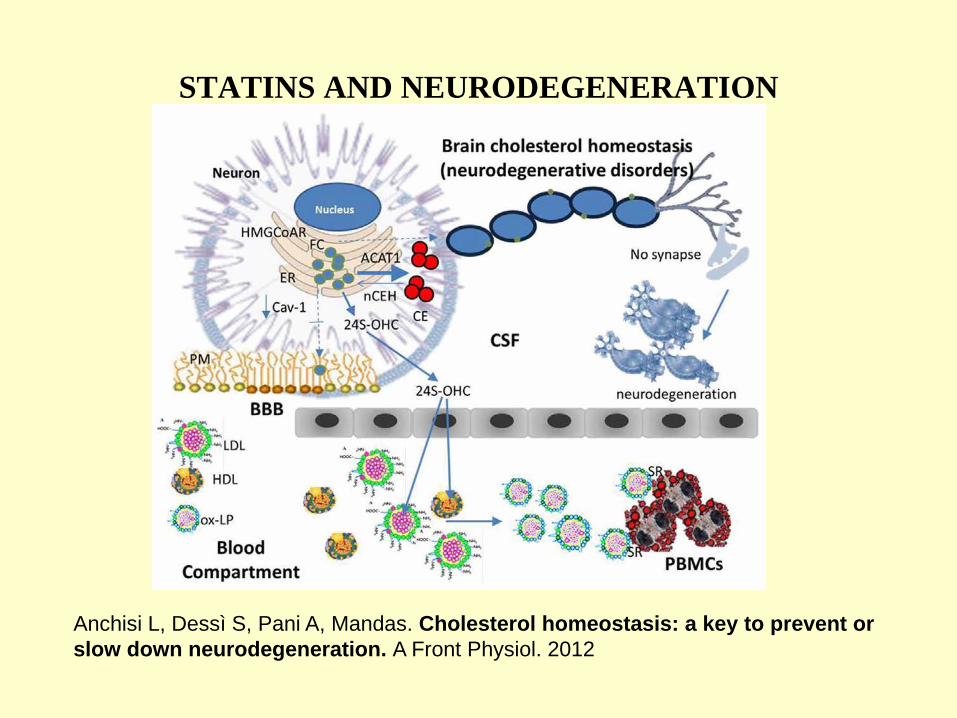
STATINS AND NEURODEGENERATION
Anchisi L, Dessì S, Pani A, Mandas. Cholesterol homeostasis: a key to prevent or slow down neurodegeneration. A Front Physiol. 2012
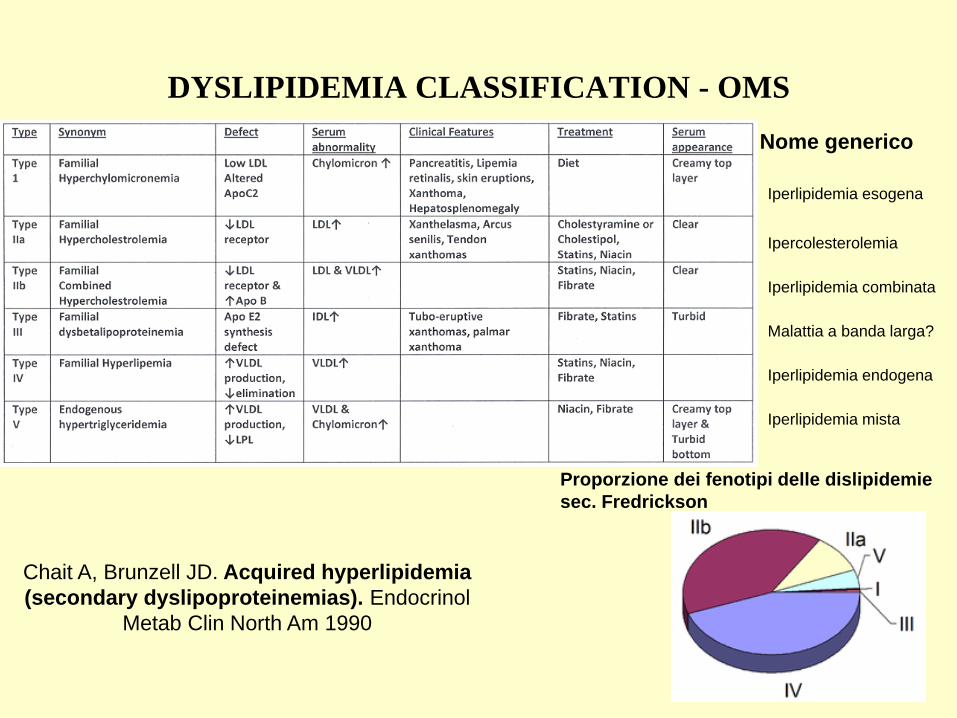
DYSLIPIDEMIA CLASSIFICATION - OMS
Ipercolesterolemia Iperlipidemia combinata Malattia a banda larga? Iperlipidemia endogena Iperlipidemia mista
Nome generico
Iperlipidemia esogena
Proporzione dei fenotipi delle dislipidemie sec. Fredrickson
Chait A, Brunzell JD. Acquired hyperlipidemia (secondary dyslipoproteinemias). Endocrinol
Metab Clin North Am 1990
DYSLIPIDEMIA CLASSIFICATION
• Forme primitive Ipercolesterlemia familiare (1:500), Apo-B 100 difettiva familiare (1:1000), Disbetalipoproteinemia
familiare (1:10000), altre forme (1:1000000)
• Forme secondarie Fattori dietetici Dieta ricca di ac grassi saturi e carboidrati, Esagerato consumo di alcool, Vita
sedentaria Alterazioni endocrinometaboliche Diabete mellito 1 e 2, Ipotiroidismo, S. Cushing, Acromegalia Malattie renali Sindrome nefrosica, Glomerulonefrite, IRC Malattie epatiche Epatite alcolica, Cirrosi biliare, Colestasi Farmaci Tiazidici, betabloccanti, immunosoppressori, corticosteroidi, estroprogestinici
Lifestyle modifications for the elderly •Esercizio fisico
•Eliminare il fumo di sigaretta
•Ridurre apporto di grassi saturi
•Limitare il consumo di carboidrati semplici
•Aumentare la proporzione di proteine assunte con la dieta
•Aumentare l’assunzione di Omega 3
•Assumere alimenti ricchi di fibre solubili
Hong Shao, Li-Quan Chen, Jun Xu Treatment of dyslipidemia in the elderly J Geriatr Cardiol. 2011

TERAPIA FARMACOLOGICA
IPERTRIGLICERIDEMIA • FIBRATI
Clofibrato Gemfibrozil Fenofibrato Bezafibrato
• AC. NICOTINICO niacina o vitamina B3
• OMEGA-3
IPERCOLESTEROLEMIA • STATINE
Atorvastatina Fluvastatina Lovastatina Pravastatina Simvastatina Rosuvastatina
• SEQUESTRANTI AC. BILIARI Colestiramina Colestipolo
• INIBITORI ASSORBIMENTO COLESTEROLO Ezetimibe
• AC. NICOTINICO
ESC/EAS Guidelines for the management of dyslipidaemias. Eur Heart J 2011

Pharmacologic approach: STATINS
Pleiotropic effects (endothelial function, vascular inflammation, oxidative stress, thrombosis - platelet aggregation, adhesion of platelets and white cells to the vascular endothelium)
Hong Shao, Li-Quan Chen, Jun Xu Treatment of dyslipidemia in the elderly J Geriatr Cardiol. 2011
Adverse effects: •Transaminase elevation •Myositis and rhabdomyolysis (increased risk with fibrate, cyclosporin, erythromycin, nicotinic acid, the protease inhibitors, nefazodone and macrolide antibiotics) •Insomnia, bad or vivid dreams, difficulty sleeping or concentrating
Actions: •lowering triglycerides •raising HDL cholesterol •lowering LDL cholesterol
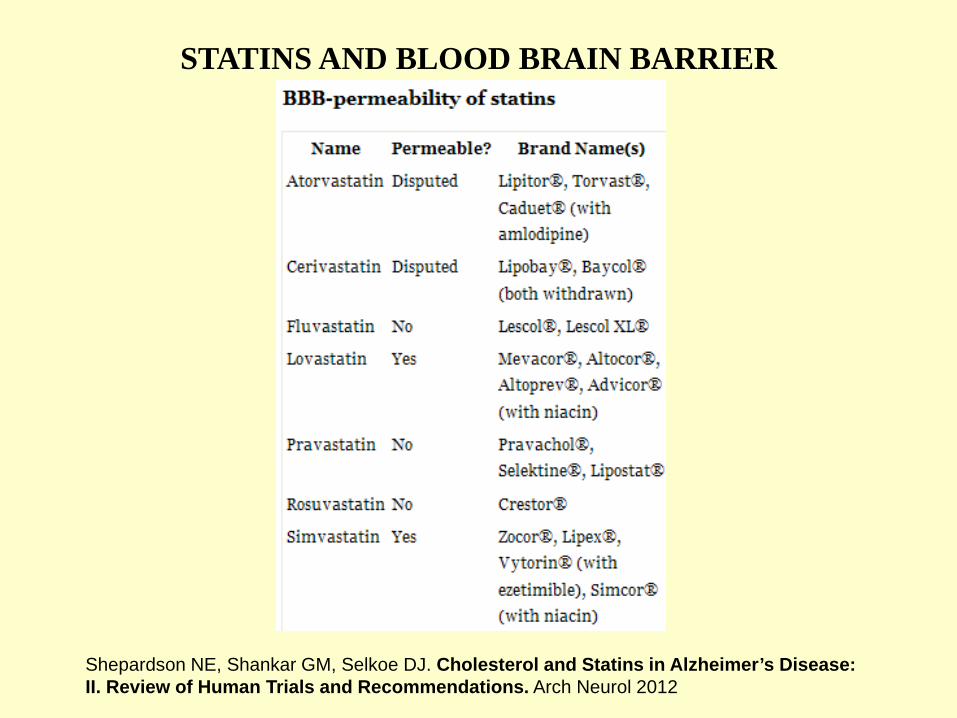
STATINS AND BLOOD BRAIN BARRIER
Shepardson NE, Shankar GM, Selkoe DJ. Cholesterol and Statins in Alzheimer’s Disease: II. Review of Human Trials and Recommendations. Arch Neurol 2012

Pharmacologic approach: FIBRATES
Renal excretion (fibrates accumulate in serum in patients with renal failure, which can lead to myositis)
Hong Shao, Li-Quan Chen, Jun Xu Treatment of dyslipidemia in the elderly J Geriatr Cardiol. 2011
Actions: •lowering triglycerides •raising HDL cholesterol •lowering LDL cholesterol

Pharmacologic approach: NICOTINIC ACID
Adverse effects: •Worsening glucose intolerance in patients with diabetes and metabolic syndrome •Hepatitis •Flushing of the skin •Conjunctivitis, nasal stuffiness, loose bowel movements or diarrhea, acanthosis nigricans and ichthyosis
Hong Shao, Li-Quan Chen, Jun Xu Treatment of dyslipidemia in the elderly J Geriatr Cardiol. 2011
Actions: •raising HDL cholesterol •lowering triglycerides •lowering LDL cholesterol •lowering Lipoprotein (a)
Pharmacologic approach: BILE ACID SEQUESTRANTS Adverse effects: •Increasing in triglyceride concentrations •Inhibiting the intestinal absorption of fat-soluble vitamins, including vitamin D, warfarin, digoxin, levothyroxin, thiazide diuretics, folic acid and statins •Abdominal fullness, gas and constipation
Action: •lowering LDL cholesterol

Pharmacologic approach: EZETIMIBE
Adverse effects: •Elevated liver enzyme levels
Hong Shao, Li-Quan Chen, Jun Xu Treatment of dyslipidemia in the elderly J Geriatr Cardiol. 2011
Actions: •raising HDL cholesterol •lowering LDL cholesterol
Peto R, Emberson J et al. Analyses of cancer data from three ezetimibe trials. N Engl J Med. 2008
EZETIMIBE AND CANCER RISK
1. Speranza di vita del paziente (se la speranza di vita è inferiore a due anni non è indicato il trattamento dei fattori di rischio, US NHANES III - Gravina CF et al. 2012)
2. Età biologica e capacità funzionale residua (considerare le comorbilità per iniziare la terapia e decidere il dosaggio)
3. Incidenza di CVD negli anziani (il 50-75% degli anziani è affetto da malattia vascolare ischemica o aterosclerosi subclinica)
4. Rischio complessivo per CVD nel singolo paziente
5. Reale efficacia della terapia nel trattamento dei fattori di rischio per CVD nell’anziano (La riduzione di 1 mmol/L (38 mg/dl) di TC comporta una riduzione del rischio di un evento CV maggiore pari a 25%, CTT - Gravina CF et al. 2012)
DYSLIPIDEMIA IN THE ELDERLY: treatment considerations
CHOLESTEROL
the Knave of Hearts or
the Joker?