Gli algoritmi terapeutici e le novità nella terapia di combinazione … algoritmi...
27
Gli algoritmi terapeutici e le novità nella terapia di combinazione per il diabete di tipo 2 Dipartimento di Medicina dei Sistemi Università di Roma, Tor Vergata Simona Frontoni
Transcript of Gli algoritmi terapeutici e le novità nella terapia di combinazione … algoritmi...

Gli algoritmi terapeutici e le novità
nella terapia di combinazione
per il diabete di tipo 2
Dipartimento di Medicina dei Sistemi Università di Roma, Tor Vergata
Simona Frontoni

Il sottoscritto Simona Frontoni
ai sensi dell’art. 76 comma 4 dell’Accordo Stato-Regioni del 2 febbraio 2017 e
in accordo con il Codice Etico della SIMI
dichiara
per l’evento in oggetto l’esistenza negli ultimi due anni di rapporti di natura
finanziaria e lavorativa con le seguenti imprese commerciali operanti in ambito
sanitario
Sanofi- Aventis, Novo Nordisk, Eli-Lilly, Takeda, Sigma-Tau, Astrazeneca,
Boheringer
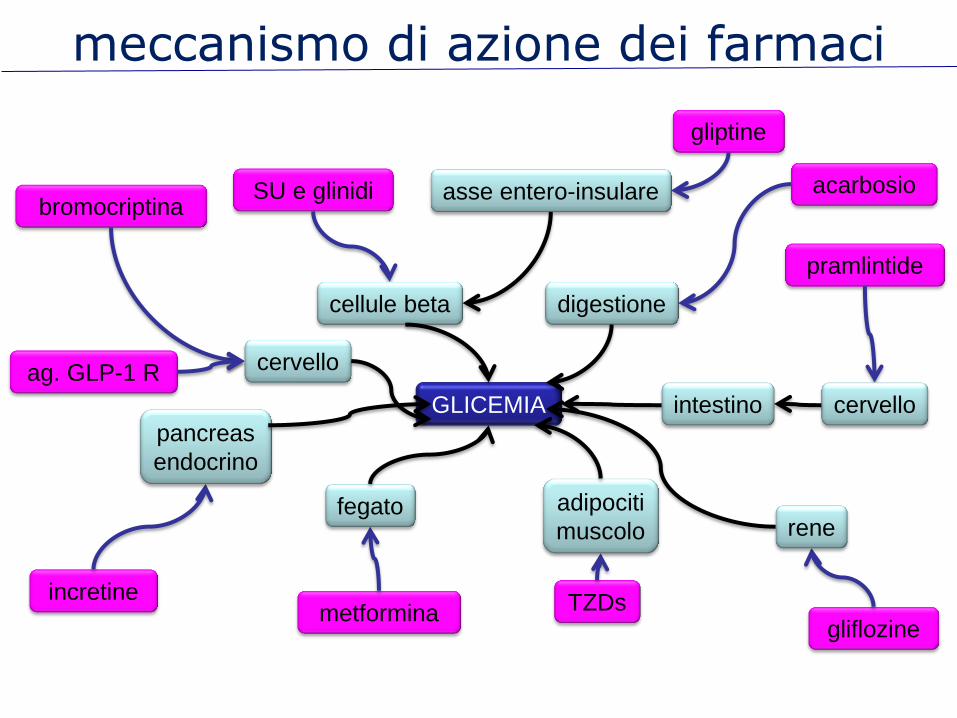
GLICEMIA
SU e glinidi acarbosio bromocriptina
gliptine
pramlintide
metformina TZDs incretine
gliflozine
ag. GLP-1 R cervello
rene
intestino
pancreas
endocrino
cervello
adipociti
muscolo fegato
digestione cellule beta
asse entero-insulare
meccanismo di azione dei farmaci


Network meta-analysis of pairwise comparisons of randomized controlled trials evaluating the use of anti-
hyperglycemic agents in addition to metformin vs. placebo
mean change from baseline in A1C
Liu S-C et al. Diabetes Obes and Metab 14: 810–820, 2012 Fujita Y et al. J Diabetes Investing 5: 265-275, 2014
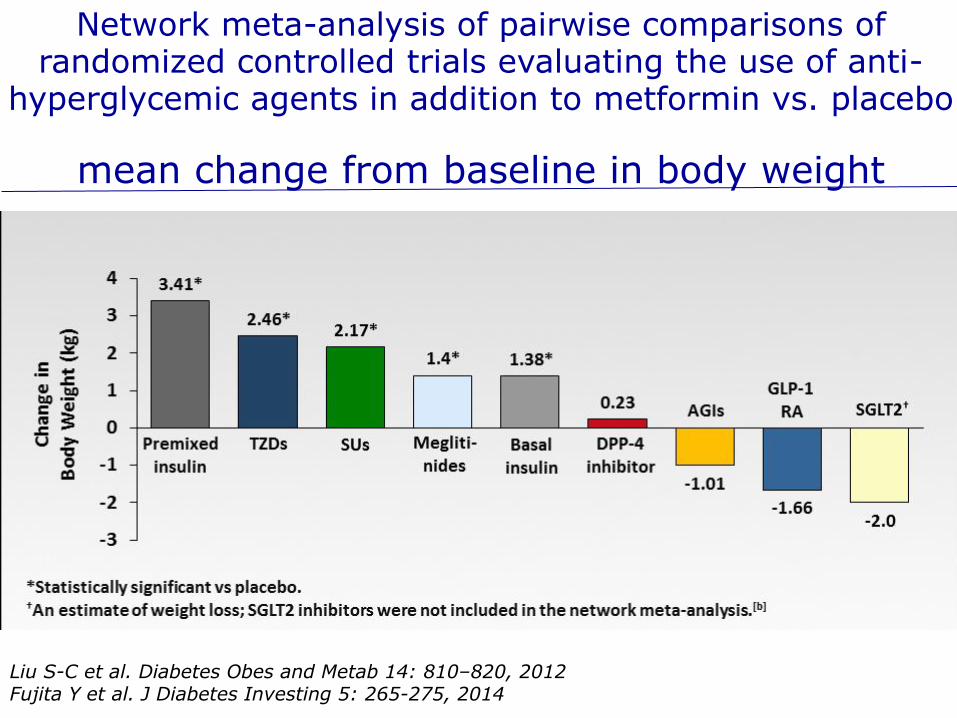
Network meta-analysis of pairwise comparisons of randomized controlled trials evaluating the use of anti-
hyperglycemic agents in addition to metformin vs. placebo
mean change from baseline in body weight
Liu S-C et al. Diabetes Obes and Metab 14: 810–820, 2012 Fujita Y et al. J Diabetes Investing 5: 265-275, 2014

Katout M al. Am J Hypertens 27: 130-139 , 2014
Meta-analysis of change in systolic blood pressure, in RCTs after at least 12 weeks of treatment
with GLP-1 RA

Baker WL et al. J Am Soc Hypertens 8: 262–275, 2014
Effects of sodium-glucose co-transporter 2 inhibitors on systolic blood pressure: Meta-analysis

Network meta-analysis of pairwise comparisons of randomized controlled trials evaluating the use of anti-
hyperglycemic agents in addition to metformin vs. placebo
At least one event of overall hypoglycemia
Liu S-C et al. Diabetes Obes and Metab 14: 810–820, 2012 Fujita Y et al. J Diabetes Investing 5: 265-275, 2014

Ongoing and recently completed cardiovascular outcomes trials within diabetes enrolling >130,000 patients
2013 2014 2015 2016 2017 2018 2019 2020
SGLT2i
GLP-1
DPP-4
Source: ClinicalTrials.gov (30 June 2015). ‘Completion date’ is the estimated completion date for the primary outcomes measure. *Also known as C-SCADE-8.
TECOS (Sitagliptin, DPP-4i)
n=14,671; follow-up ~3 yrs Q1 2015 - RESULTS
CARMELINA (Linagliptin, DPP-4i)
n= 8,300; duration ~4 yrs completion Q1 2018
CAROLINA (Linagliptin, DPP-4i vs SU) n= 6,000; duration ~8 yrs
completion Q3 2018
SAVOR TIMI-53 (Saxagliptin, DPP-4i)
n=16,492; follow-up ~2 yrs Q2 2013 - RESULTS
EXAMINE (Alogliptin, DPP-4i)
n=5,380; follow-up ~1.5 yrs Q3 2013 - RESULTS
ALECARDIO (Aleglitazar, PPAR-αγ)
n=7,226; follow-up 2.0 yrs Termin. Q3 2013 RESULTS
LEADER (Liraglutide, GLP-1)
n=9,340; duration 3.5-5 yrs completion Q4 2015
ELIXA (Lixisenatide, GLP-1)
n=6,068; follow-up ~2 yrs Q1 2015 –RESULTS
EMPA-REG OUTCOME* (Empagliflozin, SGLT2i)
n=7,097; duration up to 5yrs Q2 2015 –RESULTS
SUSTAIN 6 (Semaglutide, GLP-1)
n=3,297; duration ~2.8 yrs completion Q1 2016
EXSCEL (Exenatide QW, QW GLP-1)
n=14,000; duration ~7.5 yrs completion Q1 2018
OMNEON (Omarigliptin, QW DPP-4i) n=4,000; duration ~3 yrs
completion Q4 2017
CANVAS (Canagliflozin, SGLT2i)
n=4,407; duration 4+yrs completion Q2 2017
CANVAS-R (Canagliflozin, SGLT2i)
n=5,865; duration ~3 yrs completion Q1 2017
DEVOTE (Insulin degludec, basal insulin)
n=7,637; duration up to 5yrs completion H2 2016
FREEDOM-CVO (ITCA 650, GLP-1 in DUROS)
n=4,000; duration ~2 yrs completion Q3 2018
CREDENCE (cardio-renal) (Canagliflozin, SGLT2i)
n= 3,700; duration ~5.5 yrs completion Q1 2019
REWIND (Dulaglutide, QW GLP-1)
n=9,622; duration ~6.5yrs completion Q2 2019
DECLARE-TIMI-58 (Dapagliflozin, SGLT2i)
n=17,150; duration~6 yrs completion Q2 2019
NCT01986881 (Ertugliflozin, SGLT2i)
n=3,900; duration~6.3 yrs completion Q2 2021
HARMONY OUTCOMES (Albiglutide, GLP-1)
n=9,400; duration ~4yrs completion by Q2 2019
Completed with results Ongoing
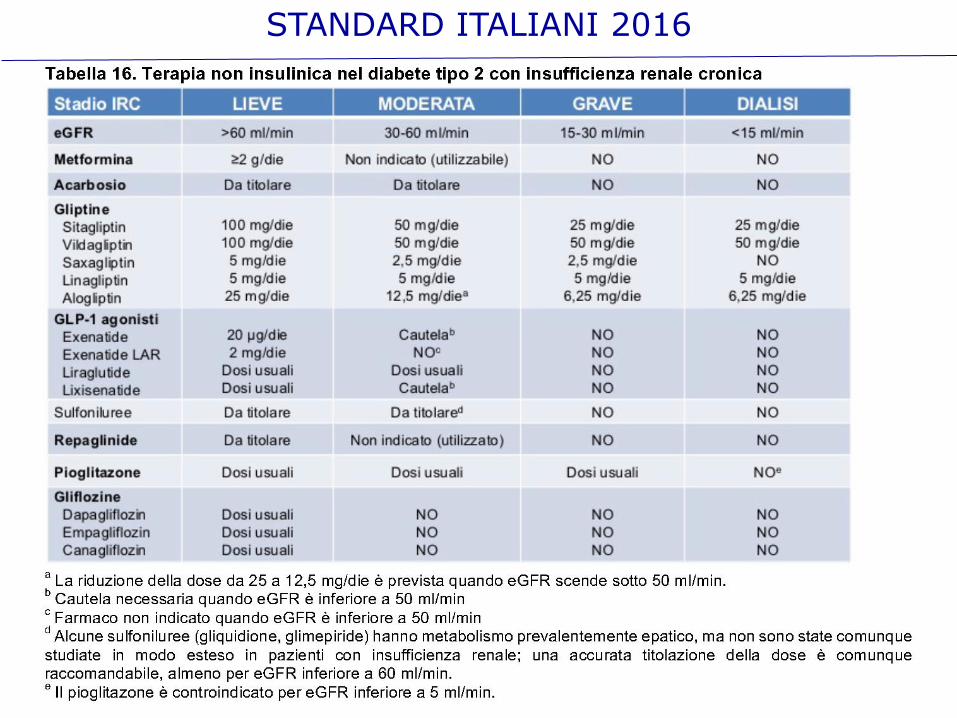
STANDARD ITALIANI 2016

Diabetes duration
Age/Life expectancy
Frailty
Occupation
Overweight/Obese
Dyslipidemia
Hypertension
Inflammation
LADA
MODY
CHD/CVD
Heart failure
NAFLD
CKD
Dementia
Osteoporosis
Psoriasis
Baseline HbA1c
Fasting hyperglycemia
Postprandial hyperglycemia
Glucose variability
Durability
Risk of hypoglycemia
Ramadan
Clinical features which may influence response to anti-hyperglycemic therapy in type 2 diabetes

triple therapy from diagnosis
time (months)
HbA1c (%)
Abdul-Ghani MA et al.: DOM 17:268, 2015
conventional:
1. titrated metformin
2. add-on and titrate glipizide
3. add-on and titrate glargine
triple:
since diagnosis
start metformin
+ pioglitazone
+ exenatide bid

gliflozin vs. gliptin as add on to metformin or combined
% of patients with HbA1c < 7.0% at W 24
0%
10%
20%
30%
40%
50%
saxagliptin dapagliflozin saxa + dapa
18%
22%
41%
Rosenstock J, et al. Diabetes Care 2015;38:376–383

gliflozins vs. gliptins pros
non insulin-mediated
no hypoglycemia
all settings
weight loss
reduce blood pressure
prevent heart failure
CV protection (one)
cons
genital infections
possible (rare) eDKA
stimulate glucagon
no with CKD (safe)
pros
stimulate insulin
no hypoglycemia
proved CV safety (some)
weight neutral
inhibit glucagon
efficacious in CKD
easy to handle
cons
non responders
No CV protection
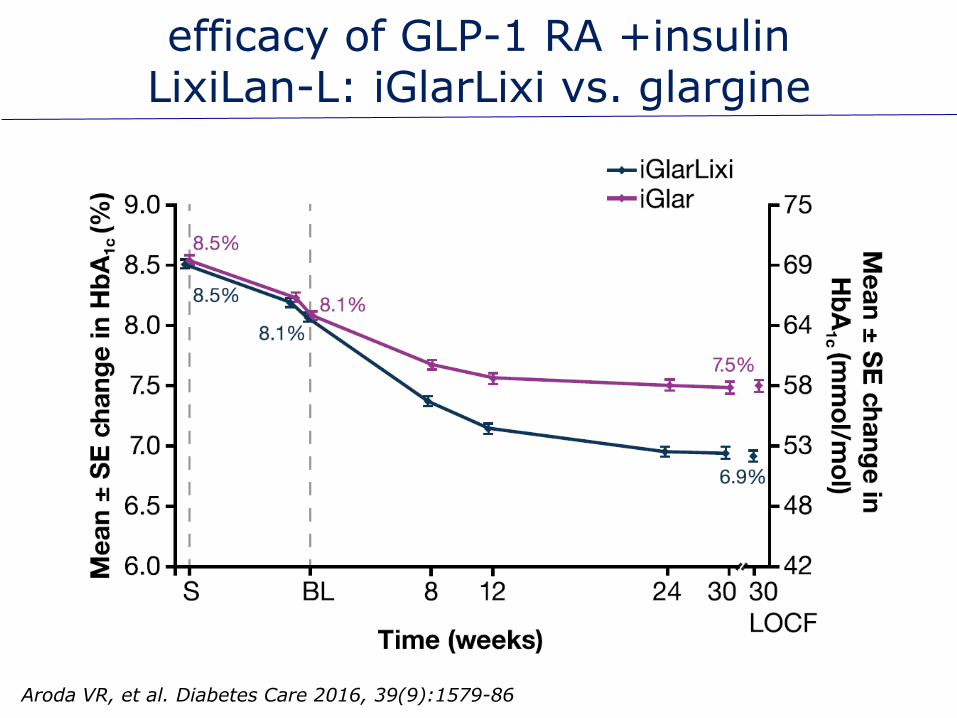
efficacy of GLP-1 RA +insulin LixiLan-L: iGlarLixi vs. glargine
Aroda VR, et al. Diabetes Care 2016, 39(9):1579-86

Gough SC, et al. DOM 17:965, 2015
efficacy of GLP-1 RA +insulin DUAL I: Ideg and/or Lira

efficacy of GLP-1 RA + SGLT-2i HbA1c
Frias JP, et al. Lancet D&E 4(12):1004-1016
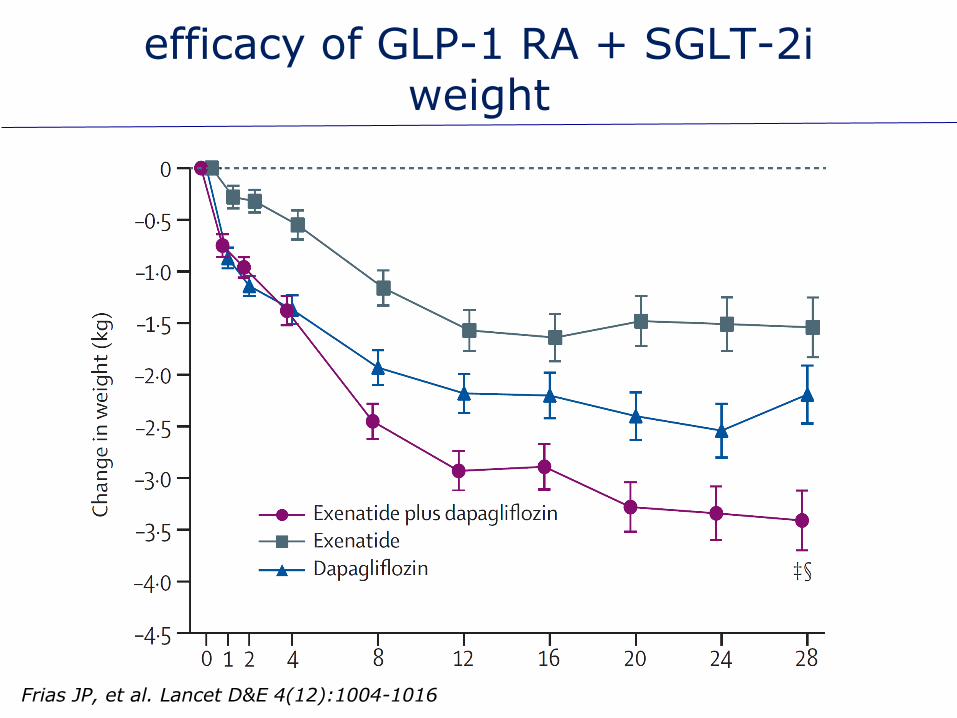
efficacy of GLP-1 RA + SGLT-2i weight
Frias JP, et al. Lancet D&E 4(12):1004-1016

how to choose the combination
age
BMI
gender
disease duration
occupation
driving
social/ center support
patient preference
ethnicity
renal function
blood pressure
CV disease
liver function
pancreatitis
osteoporosis
cognitive function
frailty
cancer
Patient characteristics Patient co-morbities
HealthCare System


Avogaro A et al. Cardiovasc Diabetol 15:111, 2016
1To be used with caution because of the risk of hypoglycemia;2consider dose reduction (except for linagliptin) and monitor eGFR frequently; 3preferred in the presence of marked insulin resistance; 4initiation of therapy currently not recommended. aUKPDS; bPROACTIVE trial; cSAVOR; dTECOS, eEXAMINE; fLEADER trial; gEMPA-REG Outcome trial; hORIGIN trial;kADVANCE; jELIXA; mDIGAMI 1
A treatment algorithm based on cardiac and renal co-morbidities and CVOTs

Diabetes duration
Age/Life expectancy
Frailty
Occupation
Overweight/Obese
Dyslipidemia
Hypertension
Inflammation
Clinical features which may influence response to anti-hyperglycemic therapy in type 2 diabetes

Baseline HbA1c
Fasting hyperglycemia
Postprandial hyperglycemia
Glucose variability
Durability
Risk of hypoglycemia
Ramadan
Clinical features which may influence response to anti-hyperglycemic therapy in type 2 diabetes

CHD/CVD
Heart failure
NAFLD
CKD
Dementia
Osteoporosis
Psoriasis
Clinical features which may influence response to anti-hyperglycemic therapy in type 2 diabetes

Cardiovascular Outcomes trials for diabetes
Proactive 16% secondary outcome (all-cause mortality, MI,
stroke)
HR 0.84 (0.72-0.98)
P= 0.027
Leader 13% primary outcome (CV death, non fatal MI,
non fatal stroke)
HR 0.87 (0.78-0.97)
P= 0.001 for
superiority
EMPA-REG 14% primary outcome (CV death, non fatal MI, non
fatal stroke)
HR 0.86 (0.74-0.99)
P= 0.0382 for
superiority
SUSTAIN 6 26% primary outcome (CV death, non fatal MI,
non fatal stroke)
HR 0.74 (0.58-0.95)
P<0.001 for
superiority

Pugliese G et at. Nutr Metab Cardiovasc Dis 24: 815-822, 2014
Prevalence of albuminuria and eGFR categoried and CKD stages (with stratification of subjects with Stages 3-5
CKD by albuminuria) in the RIACE cohort










![Algoritmi e Strutture Dati - Algoritmi Golosi (Greedy)computerscience.unicam.it/merelli/algoritmi06/[12]strategiaGolosa.pdf · Algoritmi e Strutture Dati Algoritmi Golosi (Greedy)](https://static.fdocumenti.com/doc/165x107/5c71c4f409d3f2cc4d8b53b1/algoritmi-e-strutture-dati-algoritmi-golosi-greedy-12strategiagolosapdf.jpg)