HIV, AIDS…… ……quasi 30 anni dopo - biblioteca.asmn.re.itbiblioteca.asmn.re.it/allegati/Corso...
205
HIV, AIDS…… ……quasi 30 anni dopo Clinica, terapia e comorbosità Stefania Cocchi Reggio Emilia, 06/04/2011 Università degli Studi di Modena e Reggio Emilia Clinica delle Malattie Infettive e Tropicali Direttore: Prof. Roberto Esposito
Transcript of HIV, AIDS…… ……quasi 30 anni dopo - biblioteca.asmn.re.itbiblioteca.asmn.re.it/allegati/Corso...

HIV, AIDS…… ……quasi 30 anni dopo
Clinica, terapia e comorbosità
Stefania Cocchi
Reggio Emilia, 06/04/2011
Università degli Studi di Modena e Reggio EmiliaClinica delle Malattie Infettive e Tropicali
Direttore: Prof. Roberto Esposito

HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis• Treatment & side effects of ARV drugs • Clinical manifestations

Mechanisms of HIV transmission
• Sexual: MSM, heterosexual
• Parenteral: transfusions, iv drug use
• Mother-to-child

A global view of HIV infection, 200932.8 million [30.9 million–34.7 million] living with HIV, 2009
Global report: UNAIDS report on the global AIDS epidemic 2010.
• In 33 countries, HIV incidence has fallen by more than 25% between 2001and 2009• The number of annual AIDS-related deaths worldwide is steadily decreasing from the peak of
2.1 million [1.9 million–2.3 million] in 2004 to an estimated 1.8 million [1.6 million–2.1 million] in 2009


Evoluzione epidemica
• L’epidemia assume i connotati di una infezione a trasmissione sessuale anche nel mondo industrializzato
• Pur diminuendo il numero dei nuovi casi di AIDS e dei decessi, non diminuisce in maniera significativa il numero delle nuove infezioni

HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis• Treatment & side effects of ARV drugs • Clinical manifestations

• Testing and counseling• Educazione sanitaria
Mass mediaScuolaNuove tecnologie di informazione (internet)Gruppi di pari / gruppi informali
• Controllo delle MST• Trattamenti antiretrovirali
Trasmissione materno-fetale
Interventi di prevenzione


Identificare i pazienti con comportamento di rischio
• A tutte le persone che hanno un comportamento di rischio è opportuno proporre un test HIV
• Le informazioni sulle preferenze sessuali o sull’uso di sostanze psico-attive sono parte integrante dell’anamnesi fisiologica

HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis• Treatment & side effects of ARV drugs • Clinical manifestations








HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis• Treatment & side effects of ARV drugs • Clinical manifestations

HIV



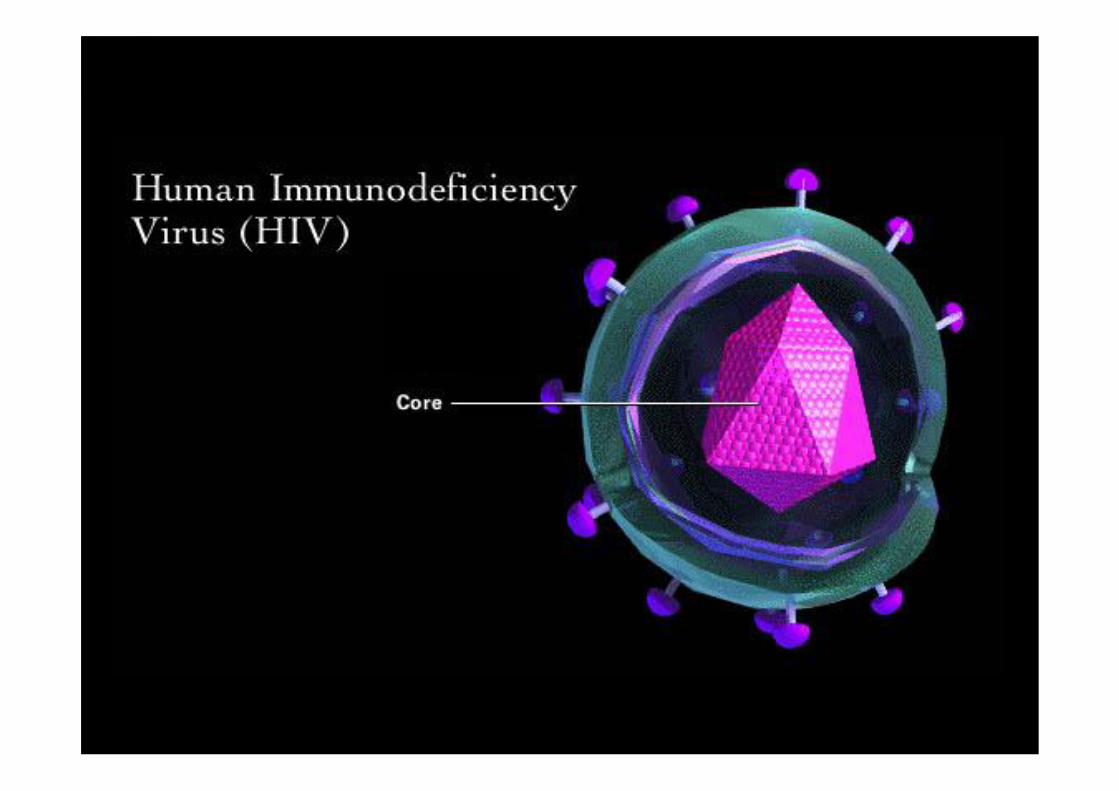


HIV structure
Adapted from Hoffman C & Rockstroh J. HIV Book 2009; p.46
lipid layer
p17 matrix antigen
gp120
gp41
integrase
host cell proteins
p24 core antigen
p7 gag
p9 gag
HIV-RNA
reverse transcriptase
lipid membrane
HLAClass II, DR
HLAClass I, DR
gp 120 docking glycoprotein gp 41 transmembrane
glycoprotein
gag
LTR pol
vif vpu env nef
vpr LTR



HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis • Treatment & side effects of ARV drugs • Clinical manifestations

HIV infection: disease progression
10
100
1, 000
10, 000
100, 000
1,000, 000
10, 000, 000
0
Acute Symptoms
Clinical Latency
AIDS, chronic HIV symptoms & death
Plasma RNA Viral Load
C4D Cell Count
Plas
ma
HIV
RN
A (
copi
es/m
L)
4-8 Weeks Up to 12 Years 2-3 Years
C4D Cell Count (cells/m
m3)
500
1, 000
200

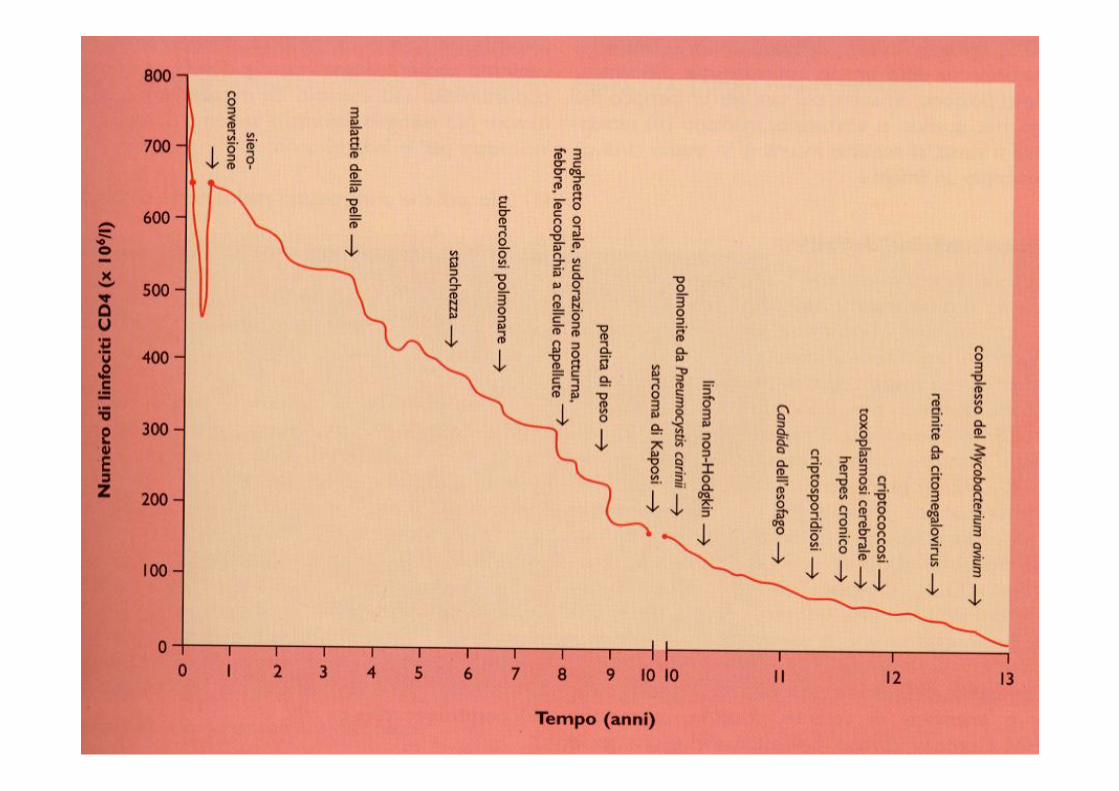
Storia naturale infezione da HIVStoria naturale infezione da HIV
settimane
CD4
T Ce
lls/m
m3
Viremia
plasmatica
0 3 6 2 111 109 12
100
200
300
400
500
600
700
800
900
1000
1100
1100
anni3 4 5 6 7 8 9
0
1:2
1:4
1:8
1:16
1:32
1:64
1:128
1:256
1:512
Infezione acuta
•Possibile sindrome infezione acuta•Ampia disseminazione del virus•Seeding organi linfoidi
Latenza clinica
Sintomi costituzionali
Malattieopportunistiche
morte

200
1000
years
High VL
Rapid progressor
Low VL
Slow progressor
HIV pathogenesisCD4
(cells/mm3)
Medium VL

Modificata da Coffin J 1996
Lo sviluppo dellLo sviluppo dell’’AIDSAIDSViral Load = Viral Load = VelocitVelocitàà del del trtrenoeno
CD4+ CD4+ = = DistanDistanzaza dal baratrodal baratro

HIV-1 replication cycle
Adapted from Weiss RA. EMBO Rep 2003; 4 S1: S10–S14
HIV particle
HIV binds to host cell
CCRSInfected cell
New viral particles
gp 120
CD4
HIV RNA
reversetranscription
integrase
DNA copy ofHIV RNA
DNA integrationinto host geonome
HIV proteins
Protease
HIV particlebudding from cell
RNA geonomes

Recettore
gp120
Fusione I

gp41
Co-recettore
Fusione II



Rilascio del core

RNA virale
Rilascio HIV-RNA ed enzimi virali

Trascrizione Inversa I
DNA-polimerasi RNA-dipendente virale

DNA virale
Trascrizione Inversa II

DNA virale
Cromosoma dell’ospite
Integrazione I

HIV integrasi
Integrazione II

Integrazione III

HIV provirus
RNA polimerasi
Trascrizione provirale I

Nuovo RNA virale
Trascrizione provirale II

ribosoma
Traduzione I

aminoacidi
Traduzione II
Proteina virale
Traduzione III
HIV proteasi
Attività della proteasi I

Enzimi viralie proteine del core
Attività della proteasiII

Assemblaggio I

Assemblaggio II

Assemblaggio III

Gp120/gp41core
Assemblaggio IV

Budding I

Budding II

Nuovo virus pronto ad infettare altre
cellule
Rilascio


L’utilizzo del corecettore influenza il tropismo e la patogenesi
R5, M-tropicTrasmissione
X4, T-tropicotardivoR5X4 virus
Tropismo doppio

Genetic variability & HIV variants
HIV-2
SIV
HIV-1 group N
HIV-1 group M
Subtype G
Subtype F
Subtype E
Subtype D
Subtype B
Subtype A
Subtype H
0.1
U46016
U52953
L41177
AF005496U51190
M62320
K03455U63632
M27323
M22639U54771
L03698L22085
AF005494U88825 U88826
HIV-1group O
Subtype C
Subtype J
AJ249239
Subtype K

HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis • Treatment & side effects of ARV drugs• Clinical manifestations

Terapia antiretrovirale
• Per prevenire l’emergenza di varianti virali resistenti ai farmaci, è necessario utilizzare associazioni di più farmaci che siano in grado di produrre una soppressione massimale della carica virale
• HAART (Highly Active Anti-Retroviral Therapy)

Classification of antiretroviral drugs

Recettore
gp120
Fusion Inhibitors
Enfuvirtide (ENF)

gp41
Co-recettore
CCR5sMaraviroc (MVC)

Trascrizione Inversa I NRTIs
Abacavir (ABC)Didanosine (ddI)
Emtricitabine (FTC)Lamivudine (3TC)Stavudine (d4T)Tenofovir (TDF)
Zidovudine (ZDV)

Trascrizione Inversa II NNRTIs
Efavirenz (EFV) Nevirapine (NVP)Etravirine (ETV)

HIV integrasi
Inibitori dell’integrasi
Integrase Inhibitor
MK-0518

Inibitori della proteasi PIs
Atazanavir (ATV)Darunavir (DRV)
Fosamprenavir (FPV)Indinavir (IDV)
Lopinavir/ritonavir (LPV/r)Nelfinavir (NFV)Ritonavir (RTV)
Saquinavir (SQV hgc)Tipranavir (TPV)

HIV-1 replication cycleHIV particle
HIV binds to host cell
CCRSInfected cell
New viral particles
gp 120
CD4
HIV RNA
reversetranscription
integrase
DNA copy ofHIV RNA
DNA integrationinto host geonome
HIV proteins
Protease
HIV particlebudding from cell
RNA geonomes
Protease Inhibitors
Entry Inhibitors
RT Inhibitors
IntegraseInhibitors
Adapted from Weiss RA. EMBO Rep 2003; 4 S1: S10–S14

1980 1985 1990 1995 2000 2005 2010
Zidovudine
Dual NRTItherapy
PI-containing cART
NNRTI-containing cART
HIV found to be cause
of AIDS
Antibody test
New drug
classes?
Entry inhibitors
RNA testShort Life expectancyPCP ~9 months
AIDS ~21 months
QoL poor
Good QoL
Natural life expectancy?Vaccines?
Rapidlylethal
ManageableLong-termIncremental therapeutic advances
From mortality to long-term manageability
Evolution of treatment for HIV infection
Kinchington D & Fitch N. Discovery and classification of HIV. In Human Immunodeficiency Virus, 2003; pp 1:1–1:10. Edited by Richman DD: International Medical Press, London.Moss AR, et al. J Natl Cancer Inst 1984; 73:1281–1284.FDA HIV/AIDS historical time line. Available at
http://www.fda.gov/ForConsumers/ByAudience/ForPatientAdvocates/HIVandAIDSActivities/ucm151079.htm (accessed November 2010).

Preferred
NNRTI-basedPI-basedINSTI-based
EFV + FTC + TDF [AI]ATV/RTV or DRV/RTV + FTC + TDF [AI]RAL + TDF + FTC [AI]
Alternative Regimens
NNRTI-based
PI-based
EFV + 3TC + (ABC or ZDV) [BI]NVP + ZDV + 3TC [BI]ATV/RTV + 3TC + (ABC or ZDV) [BI]FPV/RTV + (ABC + ZDV/3TC) or (TDF/FTC) [BI]LPV/RTV + (ABC + ZDV/3TC) or (TDF/FTC) [BI]SQV/RTV + TDF/FTC [BI]
Acceptable Regimens
NNRTI-basedPI-based
EFV + ddI + (3TC or FTC) [CI]ATV + 3TC + (ABC or ZDV) [CI]
DHHS USA GUIDELINES 2010Antiretroviral regimens recommended for naïve patients
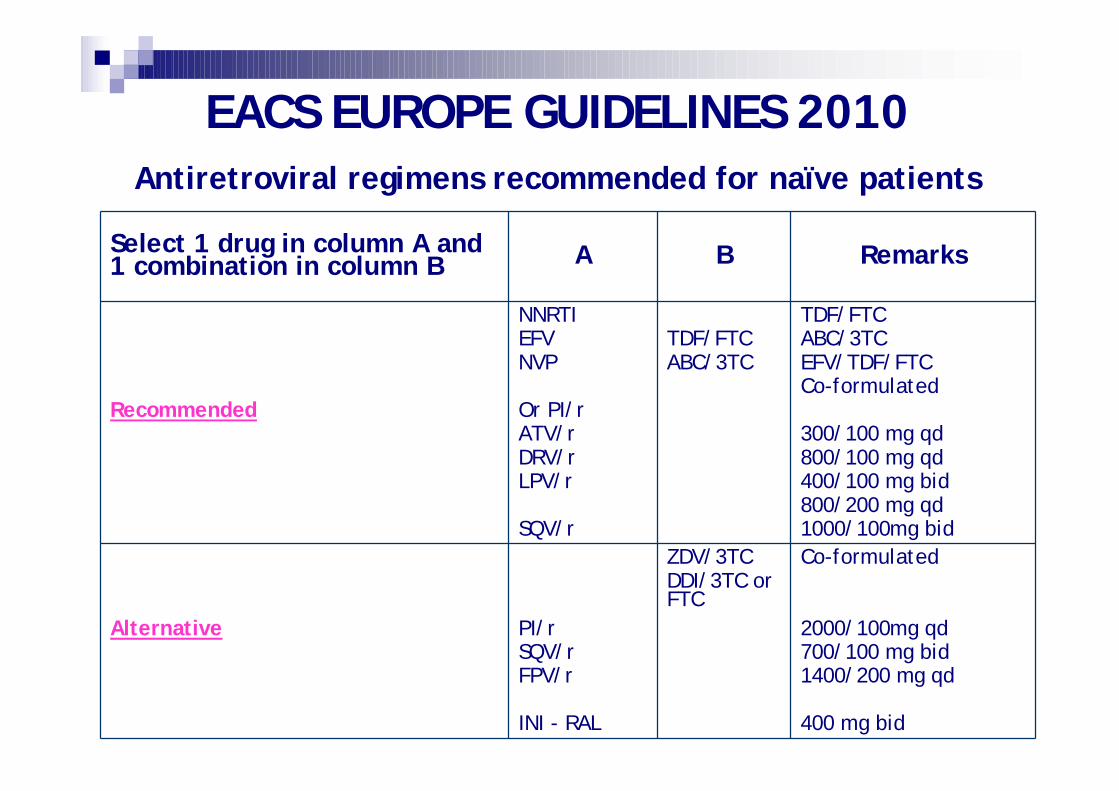
Select 1 drug in column A and 1 combination in column B A B Remarks
Recommended
NNRTIEFVNVP
Or PI/rATV/rDRV/rLPV/r
SQV/r
TDF/FTCABC/3TC
TDF/FTCABC/3TCEFV/TDF/FTCCo-formulated
300/100 mg qd800/100 mg qd400/100 mg bid800/200 mg qd1000/100mg bid
Alternative PI/rSQV/rFPV/r
INI - RAL
ZDV/3TCDDI/3TC or FTC
Co-formulated
2000/100mg qd700/100 mg bid1400/200 mg qd
400 mg bid
EACS EUROPE GUIDELINES 2010Antiretroviral regimens recommended for naïve patients

What to start ?
• Standard: 2 NRTIs + 1 NNRTI or 1 PI/r• Most common NRTIs (combos):
• Truvada (TDF/FTC), Kivexa (ABC/3TC)
• Most common NNRTIs• Sustiva, Viramune
• Most common PIs/r:• Kaletra, Reyataz/r, Prezista/r, Telzir/r
• Other: Isentress, Maraviroc, Intelence
Goal: undetectable viremia
CD4 recovery
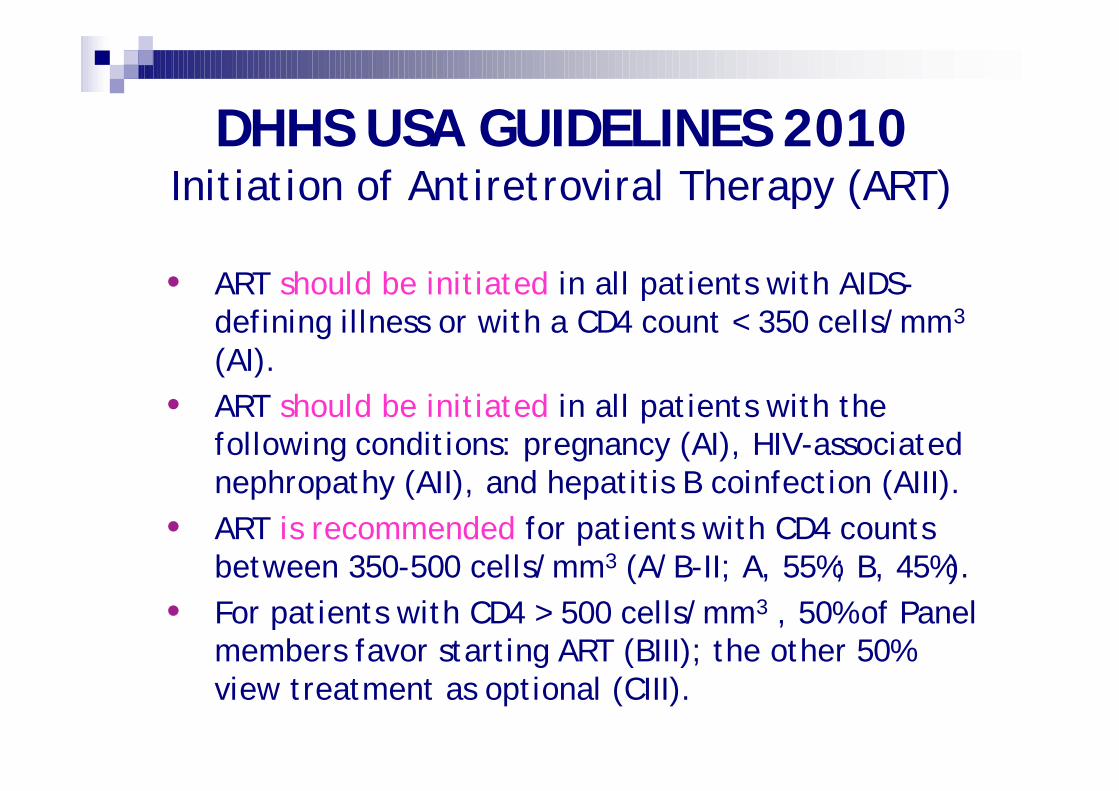
DHHS USA GUIDELINES 2010Initiation of Antiretroviral Therapy (ART)
• ART should be initiated in all patients with AIDS-defining illness or with a CD4 count < 350 cells/mm3
(AI). • ART should be initiated in all patients with the
following conditions: pregnancy (AI), HIV-associated nephropathy (AII), and hepatitis B coinfection (AIII).
• ART is recommended for patients with CD4 counts between 350-500 cells/mm3 (A/B-II; A, 55%; B, 45%).
• For patients with CD4 > 500 cells/mm3 , 50% of Panel members favor starting ART (BIII); the other 50% view treatment as optional (CIII).

SintomaticoStadiazione CDC B e C: Trattamento raccomandato
Se IO, iniziare più presto possibile
Asintomatico
CD4 <200: Trattamento raccomandato, senza indugioCD4 201-350: Trattamento raccomandatoCD4 350-500:
Trattamento raccomandato se co-infezione con epatite C, con epatite B cherichieda trattamento, nefropatia HIV associata o altre specificheinsufficienze d’organoIl trattamento dovrebbe essere preso in considerazione se CV >105 c/ml e/odeclino di CD4 >50-100/mm3/anno o età >50 o gravidanza, alto rischiocardiovascolare, neoplasia
CD4 >500:Il trattamento dovrebbe in generale essere rinviato, indipendentemente dallivello di HIV RNA plasmatico; follow-up ravvicinato di CD4 se CV >105 c/mlIl trattamento può essere offerto se presenza di 1 delle condizione di co-morbidità precedenti (CD4 350-500)
A qualsiasi livello di CD4 e HIV RNA plasmatico, il trattamento può essere offerto su base individuale, specialmente se il paziente lo richiede ed è pronto per la terapia ARV
Note aggiuntivePrima di iniziare il trattamento i CD4 dovrebbero essere ripetuti e confermati
Dovrebbe essere richiesto tempo per preparare il paziente, con lo scopo di ottimizzare “compliance” e aderenza
EACS EUROPE GUIDELINES 2010Initiation of Antiretroviral Therapy (ART)

When to start ?
• CD4 count < 350 cells/mm3
• Special situations:• Rapid CD4 decline (high viral load)• HIV-related conditions: nephropathy, thrombopenia,
CNS dysfunction,…• Pregnancy• Sexual partners• Chronic hepatitis B or C• Cardiovascular risk
Hammer SM et al. JAMA 2008;300:555-70.

How to monitor?
Routine • CD4 count• Viral load (HIV RNA)
Specific tests• Drug resistance testing• Tropism• HLA-B5701• Plasma drug levels (TDM)


ARV side effects• Rash: nevirapine, abacavir, darunavir, amprenavir,…• Hepatotoxicity: tipranavir, nevirapine• Kidney abnormalities: tenofovir• Anemia: zidovudine• Pancreatitis: didanosine• Lactic acidosis: stavudine• Insulin resistance and diabetes: zidovudine, stavudine,
didanosine• Hypertrigliceridemia: ritonavir, efavirenz, stavudine• Hypercholesterolemia: efavirenz• Lipodystrophy
• Lipoatrophy: zidovudine, stavudine, didanosine• Lipohypertrophy: PIs
The equation for ARV success
Success of ARV = Potency x Convenience
• pill burden
• toxicity profile
• inhibitory activity
HIV-RNA
• genetic barrier

I fallimenti terapeutici
Fallimento Virologico
Fallimento Clinico
Fallimento Immunologico

Goal of ARV therapy and risk of drug resistance
Viralload
1st regimen
2nd regimen
early
intermediate
late
Time
Increasing Resistance

HIV fundamentals
• Epidemiology• Prevention• Origin• Virology• Pathogenesis• Treatment & side effects of ARV drugs • Clinical manifestations



Generali• Febbre• Faringite• Linfoadenopatia• Artralgia• Mialgia• Malessere• Anoressia
Gastrointestinali• Candidosi orale/faringea• Nausea/vomito• Diarrea
Dermatologiche• Rash eritemato
maculopapulare• Ulcerazione mucocutanea• Orticaria diffusa• Desquamazione• Alopecia
Neuropatiche• Cefalea• Meningoencefaliti• Guillan-Barrè• Neuropatia periferica
Infezione primaria da HIV


Diagnosi differenziale dell’infezione primaria da HIV
• Mononucleosi da EBV
• Mononucleosi da CMV
• Toxoplasmosi
• Reazione da farmaci
• Epatite Virale

Condizioni cliniche inserite nella categoria B
• Candidosi orofaringea• Sintomi costituzionali (febbre ≥38,5°C e/o diarrea persistenti per più
di un mese)• Leucoplachia villosa orale• Herpes zoster multidermatomerico o ricorrente• Porpora trombocitopenica idiopatica• Angiomatosi bacillare• Listeriosi• Neuropatia periferica• Candidosi vulvovaginale (persistente, frequente o scarsamente
sensibile alla terapia)• Displasia cervicale (moderata o grave)/carcinoma in situ della cervice
uterina• Malattia infiammatoria pelvica (PID)



Clinical spectrum of HIV disease
HIV AIDSImmune deficiency
HIVPremature ageing(lipodystrophy and co-morbidities)
Immune activationand senescence
HIVNeuropsychologicaldisorders and AIDS dementia
HIV neurotropism
HIV clinical manifestations
• AIDS–opportunistic conditions:• Infections: PCP, CNS toxoplasmosis, TB,... • Neoplasms: NHL, KS,...
• AIDS-neurological diseases• AIDS dementia complex (ADC)• HIV-associated neurological disorders (HAND)
• Non-AIDS conditions: • HIV-directly associated: nephropathy • Non-HIV directly linked: acceleration of other medical
processes: chronic viral hepatitis, artherosclerosis

Le infezioni opportunistiche
Maggiori cause di mortalità dei pz con AIDS sono funzione di:
• numero dei CD4 • esposizione a potenziali patogeni
• virulenza dei patogeni
Per talune patologie è indicata la profilassi primaria, per tutte la profilassi secondaria
L’avvento della HAART ha modificato l’evoluzione e la capacità di recidiva di queste forme morbose
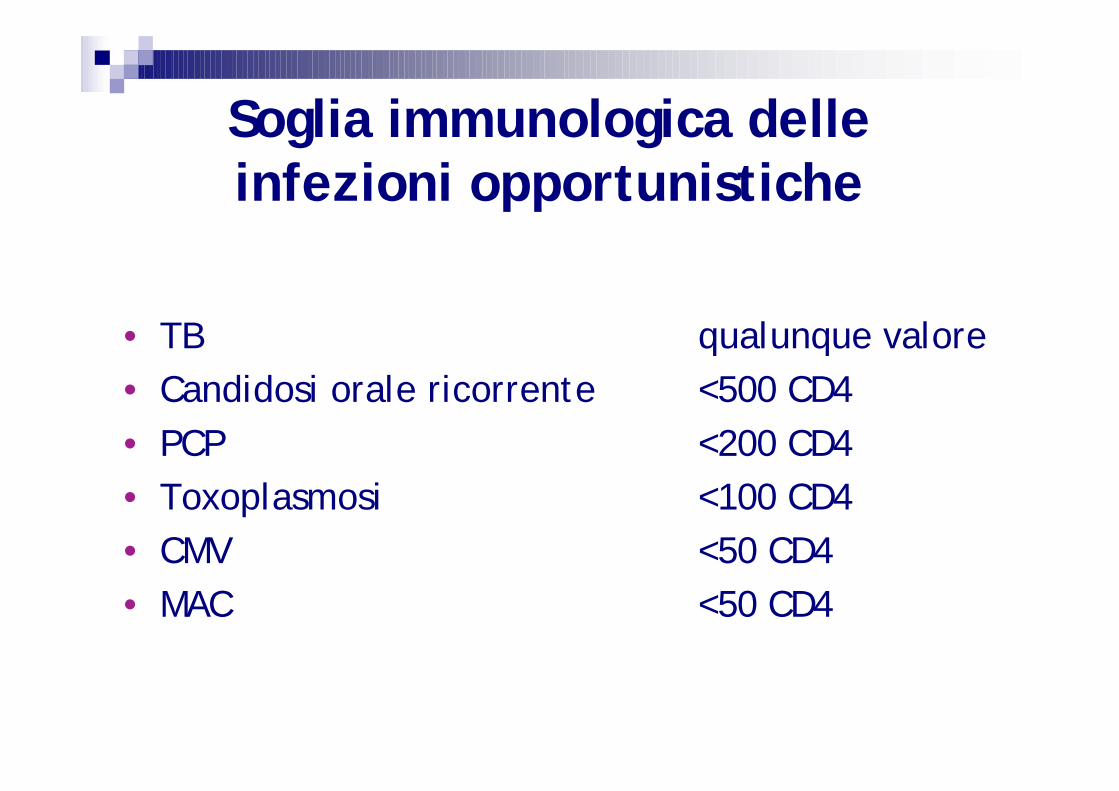
Soglia immunologica delle infezioni opportunistiche
• TB qualunque valore• Candidosi orale ricorrente <500 CD4• PCP <200 CD4• Toxoplasmosi <100 CD4• CMV <50 CD4• MAC <50 CD4
Apparato respiratorio
• PCP• TB• Polmoniti batteriche recidivanti• MOTT• Micosi profonde (Candida spp., Cryptococcus
neoformans)• Batteri intracellulari (Rhodococcus equi,
Nocardia asteroides)

PCP Pneumocystis jirovecii (fu carinii)
pneumonia
• P. carinii assimilabile ai funghi come omologia genomica
• Polmonite interstiziale febbrile, caratterizzata da severa dispnea
• Diagnosi microscopica da BAL• Indicata la profilassi primaria con
cotrimossazolo se CD4 <200
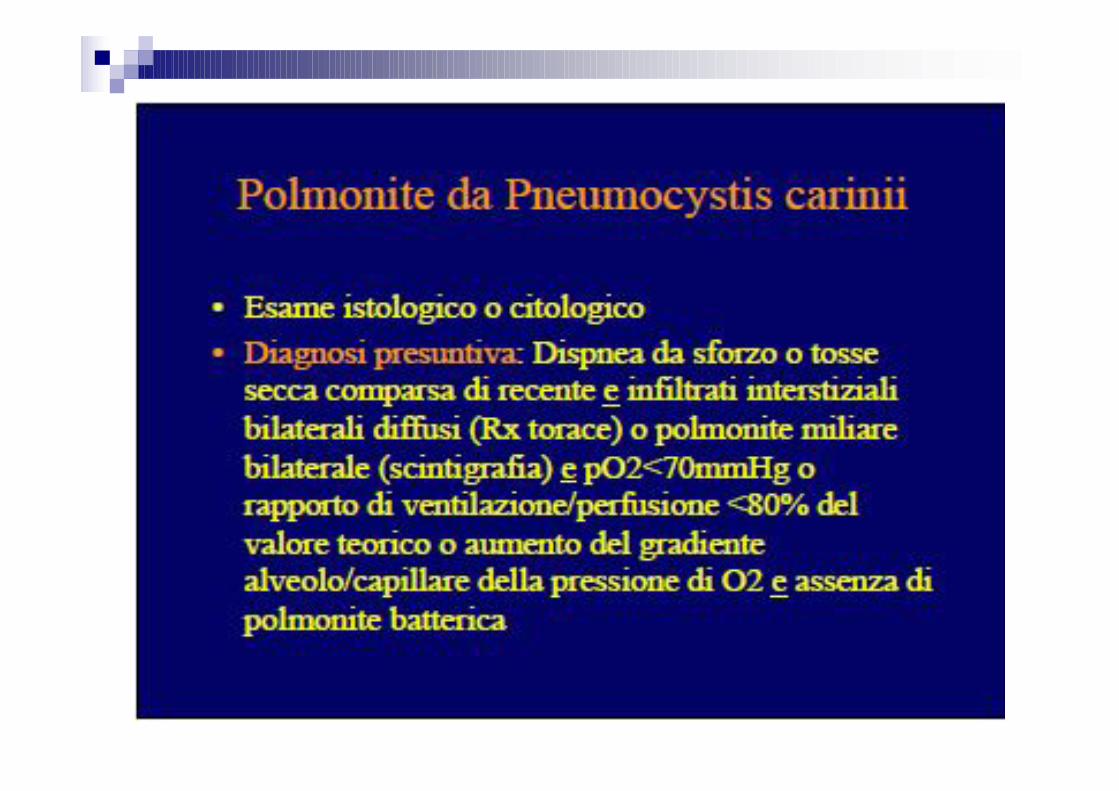

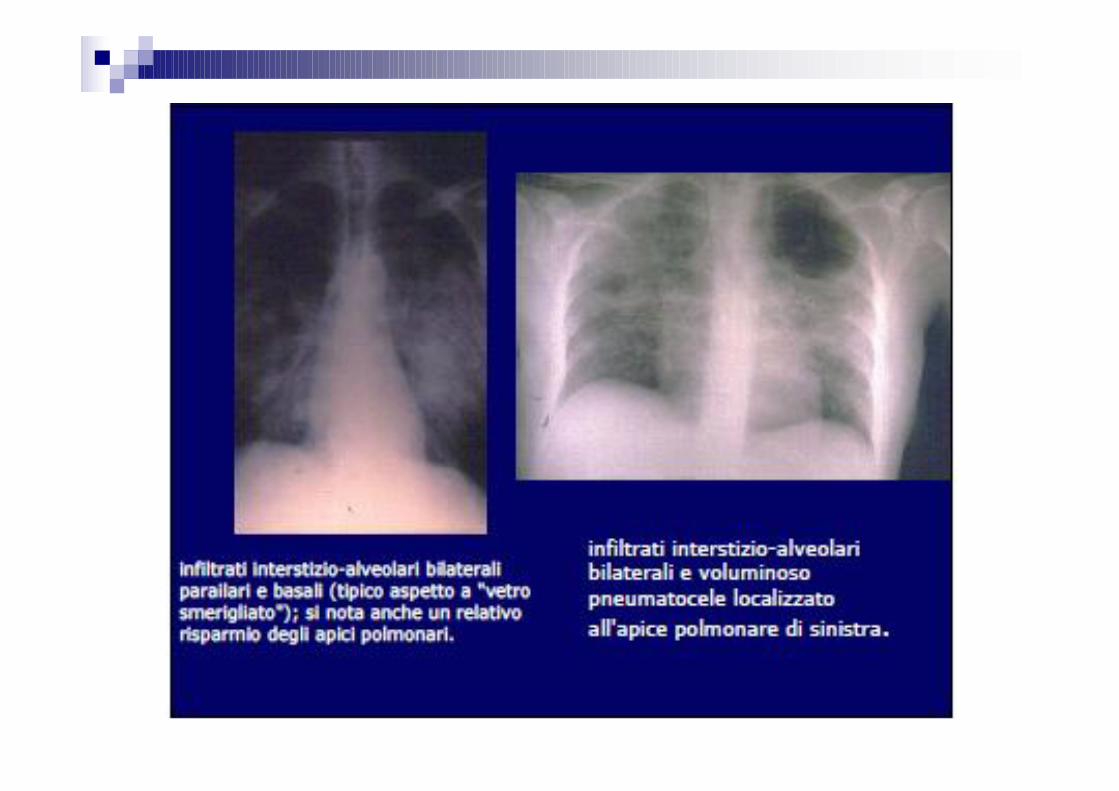
Polmonite da Pneumocystis carinii(PCP)




Profilassi PCP
Inizio con CD4+ = 200/mmc• Più precocemente se wasting/mughetto/infezioni
ricorrenti
Profilassi Primaria• TMP/SMZ• Dapsone o Atovoquone
Profilassi Secondaria• TMP/SMZ • Dapsone o Atovoquone o Pentamidina• Clindamicina/Primachina o TMP/Dapsone

Tubercolosi • Può essere osservata relativamente precocemente
durante la malattia da HIV quando i CD4+ sono circa 300/mmc. Generalmente la presentazione è quella classica
• E’ possibile osservare la tubercolosi anche nelle fasi tardive della malattia da HIV; in questo caso è piùfrequente l’interessamento di entrambi i polmoni e quello extra-polmonare. L’interessamento degli organi intraddominali è abbastanza comune.
• Le caratteristiche radiologiche della tubercolosi osservata durante le fasi avanzate della malattia da HIV sono generalmente atipiche (interessamento dei lobi inferiori, forme miliari)

Apparato digerente
• Candida• CMV• Microsporidi, Criptosporidi• Batteri comuni• HSV-1, HSV-2• Giardia, Ameba
Candidosi
• Forme superficiali (mughetto) • Forme invasive (esofagite, polmonite,
meningite)• Terapia: fluconazolo, itraconazolo,
anfotericina• Candida, talora resistente agli azolici

Candidosi orale






CMV
• Malattia virale sistemica• Corioretinite• Colite• Esofagite• Encefalite• Non è indicata una profilassi primaria• Terapia: ganciclovir, foscavir, cidofovir




Cute

Cute e mucose superficiali
• Candida• Leucoplachia villosa orale• Dermatite seborroica• HSV-1, HSV-2• VZV• Poxvirus • Papillomavirus

LeucoplachiaLeucoplachia oraleorale


Herpes simplex






Varicella in Varicella in HIV+HIV+



SNC
• Toxoplasmosi• Leucoencefalite multifocale progressiva (PML)• Encefalopatia da HIV
Toxoplasmosi cerebrale
Encefalite toxoplasmica:• Lesione occupante spazio• Frequenti lesioni multiple in sede di giunzione
tra sostanza bianca e grigia con “contrastenhancement” ed edema perilesionale
• Terapia di prima linea: sulfadiazina + pirimetamina



ToxoplasmosiToxoplasmosi

Profilassi toxoplasmosi
Da considerare quando CD4+ <100/mmc• TMP/SMZ
Altre opzioni• Dapsone + pirimetamina + acido folinico• Clindamicina + pirimetamina + acido folinico

Leucoencefalitemultifocaleprogressiva (PML)



Neoplasie in HIV
AIDS-Definenti Virus Sarcoma di Kaposi HHV8 Linfoma Non-Hodgkin EBV, HHV8, HIV? Carcinoma Cervice Invasivo HPV Linfoma cerebrale primitivo HIV?
AIDS-Associati Malattia di Hodgkin EBV Leiomiosarcoma (pediatrico) EBV Carcinoma Squamoso Congiuntivale HPV Carcinoma Squamoso Anale HPV










HIV clinical manifestations
• AIDS–opportunistic conditions:• Infections: PCP, CNS toxoplasmosis, TB,... • Neoplasms: NHL, KS,...
• AIDS-neurological diseases:• AIDS dementia complex (ADC)• HIV-associated neurological disorders (HAND)
• Non-AIDS conditions: • HIV-directly associated: nephropathy • Non-HIV directly linked: acceleration of other medical
processes: chronic viral hepatitis, artherosclerosis

AIDS Dementia Complex (ADC)
• HIV-1-associated dementia complex (HIV dementia) is one of the most frequent neurologic manifestations of HIV disease, developing in up to 10% of patients with AIDS


HIV-associated NeurocognitiveDisorders (HAND)

HIV clinical manifestations
• AIDS–opportunistic conditions:• Infections: PCP, CNS toxoplasmosis, TB,... • Neoplasms: NHL, KS,...
• AIDS-neurological diseases:• AIDS dementia complex (ADC)
• HIV-associated neurological disorders (HAND)
• Non-AIDS conditions: • HIV-directly associated: nephropathy • Non-HIV directly linked: acceleration of other medical
processes (chronic viral hepatitis)

Worldwide global prevalence of HIV–HBV-HCV co-infection
170 million HCV patients1
42 million HIV
patients2
12 million co-infected patients
1. World Health Organization. Hepatitis C Fact Sheet No. 164, October 2000 2. UNAIDS, AIDS Epidemic Update 2006
400 million HBV
patients2
4 million co-infected patients
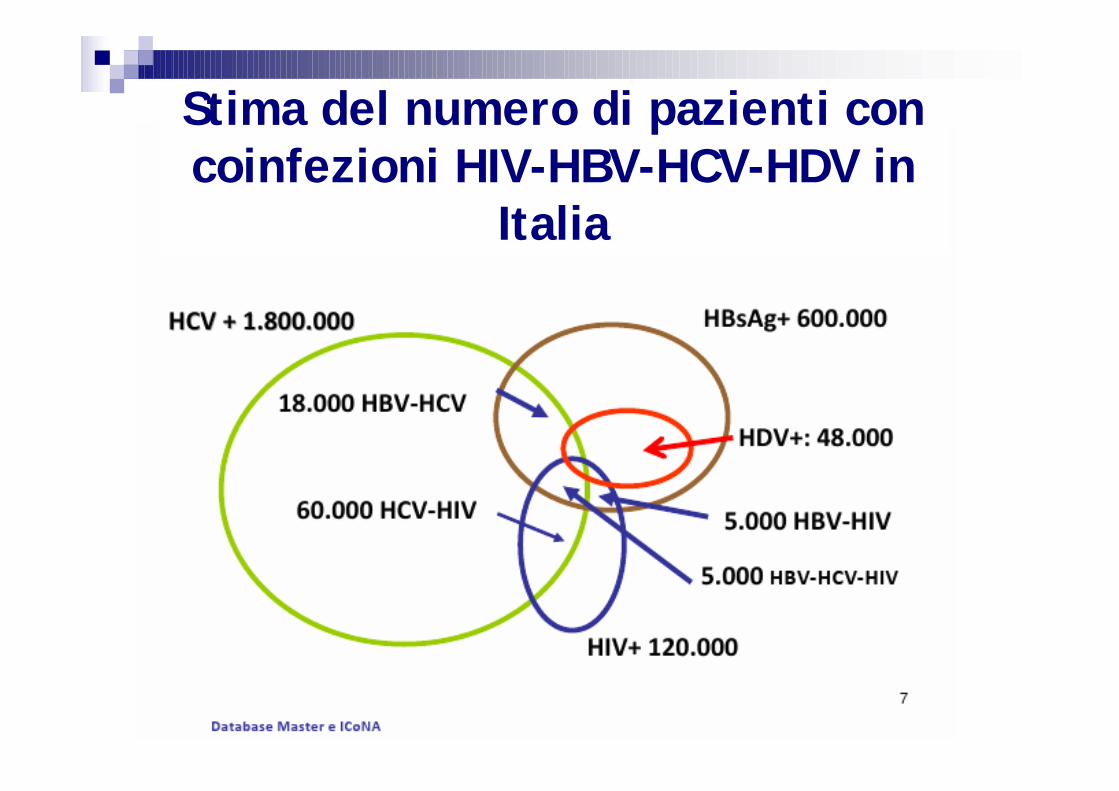
Stima del numero di pazienti con coinfezioni HIV-HBV-HCV-HDV in
Italia

Influence of HIV on viral hepatitis in co-infected patientsHIV accelerates the clinical course of HCV-HBV-related liver disease:• faster time to HCC• more patients develop cirrhosis within a given time-frame
Liver disease is now the leading cause of death among hospitalised AIDS patients
Drugs, alcohol and HAART have an additional aggravating effects
Soto et al. J Hepatol 1997; 26:1–5Mohsen. Gut 2003; 52:1035–1040Sulkowski et al. 12th CROI 2005, Abstract 121Giordano et al. 2nd IAS Conference on HIV Pathogenesis and Treatment 2003; Abstract 213Soriano et al. XIII International AIDS Conference 2000; Abstract ThOrB655

Poynard, T. et al. J Hepatol 2003;38:257-265
4,682 patients
180 HIV-HCV701 Alcohol812 HBV382 Hemochromatosis2,313 HCV93 Steatosis BMI>25200 PBC
1.00
0 20 40 60 80
Haz
ard
func
tion
Age in years
Progression to cirrhosis

Non-AIDS morbidity and mortality in Central Europe
Adapted from Weber R et al. Arch Intern Med 2006; 166: 1632-41

Liver toxicity is the most common severe adverse event
in the HAART era
0,0
1,0
2,0
3,0
4,0
Liver
Neutr
openia
Anem
ia
Cardi
ovascu
lar
Pancre
atitis
Psychi
atric
Kidney
Throm
bocyto
penia
Hemorr
hage
Coinfection with hepatitis B or C associated with 4.15(95% CI 2.26–7.60) hazard ratio of Grade 4 liver toxicity
Reisler RB, et al. J Acquir Immune Defic Syndr 2003;34:379–86
Inci
denc
e/
100
pers
ons
Liver Neutropenia Anemia Cardiovasc. Pancreatitis Psychiatric Kidney Thromboc. Haemorrhage

Proportion of causes of death(Modena 1993-2005)
0%
20%
40%
60%
80%
100%
1993 1995 1997 1999 2001 2003 20050
20
40
60
80
100
120
140
160
180
OtherAccidemtESLDAIDSAll
MODENAMODENA
HIVHIVCOHORTCOHORT
MODENAMODENA
HIVHIVCOHORTCOHORT

The “Palellogram”
Hepatic disease was the onlyreported cause of
death for which absolute ratesincreased over time

Nefropatia in HIVSi possono distinguere 4 gruppi di nefropatie da un punto di vista eziopatogenetico:
1) nefropatie correlate alla infezione da HIV come la nefropatia HIV correlata (NHC), la glomerulonefrite HIV-correlata, e la microangiopatia trombotica HIV-correlata;
2) patologie renali correlate alla immunodepressione e secondarie all’azione di virus , batteri, parassiti o processi linfoproliferativi;

Tx in HIV…why??
With the aging of the HIV infected patients the transplant community will need to address
the increasing need for transplantation as the result of
a higher rates of kidney and liver failure associated with the
co-morbidities of HIV

OLTx in HIV
Improvement in HIV-associated mortality make it difficult to deny transplantation
based on futility
Tzakis AG, Transplantation 1990;49:354–358Bouscarat F, Clin Infect Dis 1994;19:854–859
Ragni MV,J Infect Dis 2003;188:1412–1420
Short/Mid-term survival of OLTx in HIV-infected recipients is similar to that of non-HIV-infected patients

HIV-Infected Liver and Kidney transplant Recipients: 1- and 3-
Year OutcomesThe question is not if HIV patients do as well as age-matched
controlled, but rather if they do as well as their relatively poor prognosis groups that are considered appropriate
transplant candidates
Stock P, Am J Transplant. 2008 Feb;8(2):355-65
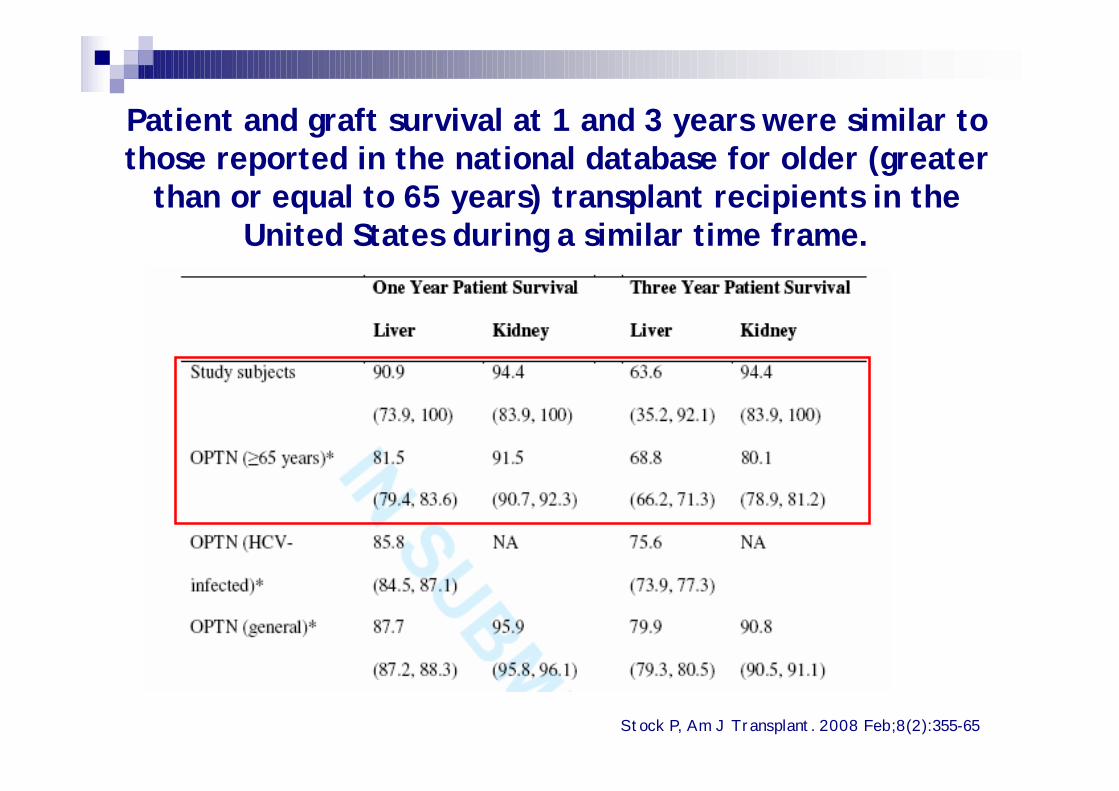
Patient and graft survival at 1 and 3 years were similar to those reported in the national database for older (greater
than or equal to 65 years) transplant recipients in the United States during a similar time frame.
Stock P, Am J Transplant. 2008 Feb;8(2):355-65

Attivitàtrapianto
al 30 marzo 2011
FONTE DATI: Dati CIR e CT
Protocollo nazionale trapianti in pazienti con
infezione da HIV

FONTE DATI: Dati CIR e CT
Trapianti di fegato – Anni 2002/2011**Dati aggiornati 30 marzo 2011
1
65
19
13
22 (2)
16
11 (1)
19 (1)
4
2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Fegato Fegato/Rene

Trapianti di fegato divisi per anno e per CTx**Dati aggiornati 30 marzo 2011
0123456789
Ancona Bologna Genova Modena Palermo Roma Udine
2002 2003 2004 2005 2006 20072008 2009 2010 2011

FONTE DATI: Dati CIR e CT
1100PALERMO
47(1*+3**)116 (4*+4**)4213 (+5 sosp)TOTALI
3601GENOVA
4 (1**)12 (1**)01ANCONA
1119203 (+3 sosp)BOLOGNA
7 (1*+1**)36 (1*+1**)02UDINE
12 (1**)29 (3*+2**)215 (+2 sosp)MODENA
91311ROMA
DECESSI POST-Tx
TRAPIANTI EFFETTUATI
PAZIENTI USCITI DA LISTA
PAZIENTI IN LISTA ATTESA (status attivo)
CENTRI TRAPIANTO
FEGATO (inclusi 4 tx combinati fegato/rene* e 4 ri-trapianti**)
Liste di attesa e report attivitàfegato al 30 marzo 2011

Trapianti di rene – Anni 2006/2011*
FONTE DATI: Dati CIR e CT
*Dati aggiornati 30 marzo 2011
1 1
10
1
2
10
2
9
1
4
1 1
2
2006 2007 2008 2009 2010 2011
Rene Rene/Pancreas Rene/Fegato
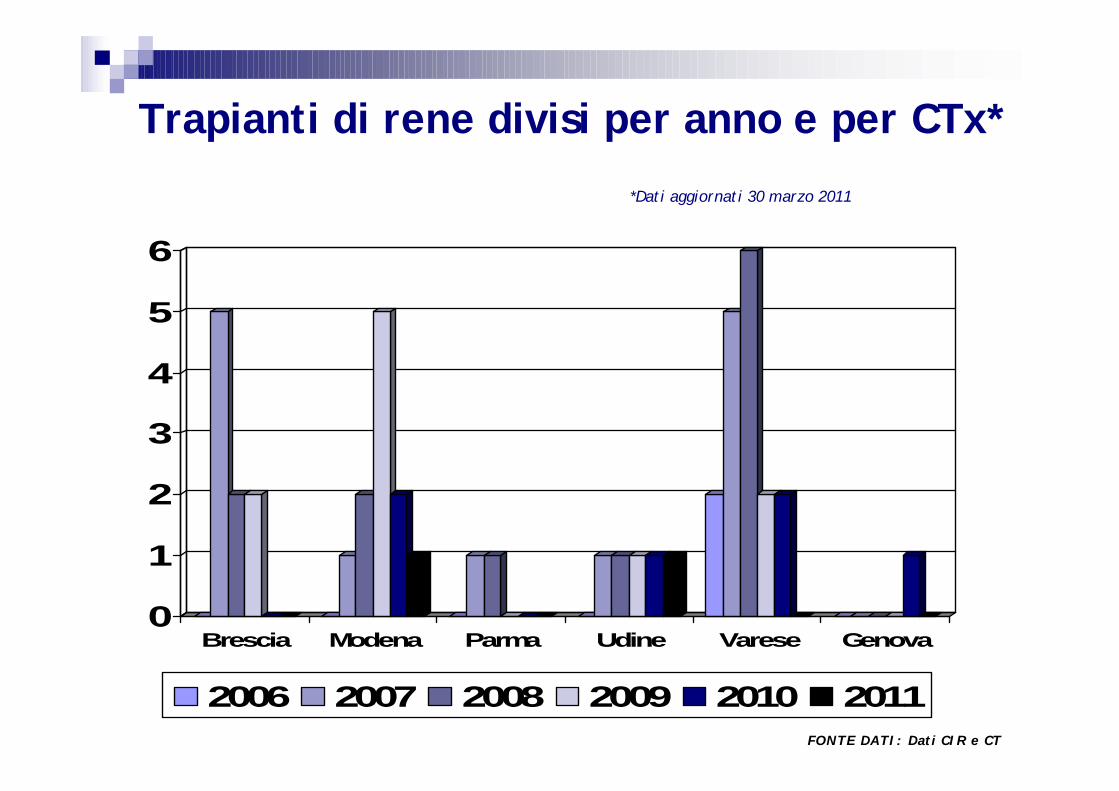
Trapianti di rene divisi per anno e per CTx*
*Dati aggiornati 30 marzo 2011
FONTE DATI: Dati CIR e CT
0
1
2
3
4
5
6
Brescia Modena Parma Udine Varese Genova
2006 2007 2008 2009 2010 2011

FONTE DATI: Dati CIR e CT
Liste di attesa e report attività rene al 30 marzo 2011
01 (1**)01GENOVA
1 (1*)44 (5**;4*)312 (1 sosp)TOTALI
0201PARMA
0914BRESCIA
1 (1*)5 (1*)00UDINE
011 (3*)21 (1 sosp)MODENA
017 (4**)04VARESE
DECESSI POST-Tx
TRAPIANTI EFFETTUATI
PAZIENTI USCITI DA
LISTA
PAZIENTI IN LISTA ATTESA (status attivo)
CENTRI TRAPIANTO
RENE (inclusi 4 tx combinati fegato/rene* e 5 tx combinati rene/pancreas**)

FONTE DATI: Dati CIR e CT
Report attività altri organi al 30 marzo 2011
0312TOTALI
0101NAPOLI
0211PALERMO
DECESSI POST-Tx
TRAPIANTI EFFETTUATIPOLMONICUORECENTRI TRAPIANTO
CUORE E POLMONI

Criteri di inclusione
• Infezione da HIV documentata
• Capacità di fornire/acquisire il Consenso informato
• Pazienti mai trattati con terapia antiretrovirale con conta di linfociti CD4+ circolanti, stabilmente > 100/mmc
• Pazienti in terapia antiretrovirale, senza precedenti infezioni opportunistiche “AIDS defining” con conta dei linfociti CD4+ >100/mmc, stabile da almeno 6 mesi. HIV-1- RNA undetectable al momento dell’inclusione in lista; è ammessa la presenza di attiva replicazione virale di HIV in pazienti con malattia epatica scompensata e, per tale motivo, intolleranti alla terapia antiretrovirale purchè presentino una documentata risposta alla terapia antiretrovirale nell’ultimo ciclo terapeutico
• Pazienti con storia di una o più patologie opportunistiche “AIDS defining” devono avere conta dei linfociti CD4 > 200/mmc, stabile da almeno 6 mesi e HIV-RNA undetectable, se in trattamento, o documentata risposta alla terapia antiretrovirale nell’ultimo ciclo terapeutico
• Compliance al trattamento immunosoppressivo e antiretrovirale ed alla profilassi delle infezioni opportunistiche, se indicata

I pazienti verranno monitorati per CD4 e HIV-RNA con cadenza trimestrale
La perdita di uno o più criteri di inclusione determina uscita temporanea dalla lista fino al recupero di validità di tutti i criteri di Inclusione.
Criteri di esclusione
• Mancanza dei criteri immunologici e virologici di inclusione
• Storia di patologie opportunistiche per le quali non esistono al momento attuale opzioni terapeutiche efficaci (Criptosporidiosi, LeucoencefalopatiaMultifocale Progressiva, Infezioni da Mycobacterium abscessus, etc.)
• Diagnosi di Sarcoma di Kaposi
• Storia di neoplasia (eccezion fatta per carcinoma baso-cellulare ed il carcinoma in situ della cervice con disease-free documentata superiore ai 5 anni; la guarigione dalla patologia neoplastica dovrà essere certificata da uno specialista oncologo)

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

Prevalence of late presentation in 2008
52%52%
64%64%
45%45%
54%54%
47%47%
41%41%
72%72%
41%41%
42%42%
42%42%
Late presentation: CD4 count <350 cells/µl
ATHENA Brussels St Pierre CohortBarcelona cohortUK CHICClinSurv HIVDHCSEuroSIDAFHDH ANRS CO4ICONASwedish CohortSHCS
Adapted from Lundgren J. EACS 2009

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

The infectious reservoir in Europe 200760% of HIV-infected persons are not currently
aware of their HIV status
Europe Population (13-64 yrs)250 million
HIV+ Population2.4 million
Known to be HIV+1.1 million(816,000)
HIV in Europe Steering Committee 2007

HIV – controlling the hidden and overt epidemic
• Aggressively ‘seek, test and treat’• Effective ART can lead to near-normal life expectancy
• Search for a cure• Sterilising cure (Vaccines – Thai trial)
• Functional cure – new therapies (integrase)
• Prevent new infections• PEP / PrEP / Microbicides
• Decrease transmission with lower viral loads
• Universal cART therapy
CROI 2010 last accessed 17 November 2010

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

Hostfactors
HIVHIV
treatment
Overlapping factors in the pathogenesis of non-AIDS comorbidities

DislipidemiaInsulin resistance & diabetesLipodystrophyCardiovascular risk
Decreased GFR and renal insufficiency
Osteopenia/osteoporosisOsteonecrosisSexual disfunctionsFatty liver…
HIV-associated comorbidities

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

The Metabolic Clinic model: a patient-centered approach in the management of HIV related non-infectious co-morbidities
Dyslipidaemia Abnormalities of body compositionDiabetes
The Metabolic Clinic model: a patient-centered approach in the management of HIV related non-infectious co-morbidities

Liver diseasesCVD Bone & Kidney disease
Moving from LIPODYSTROPHY to HIV related non-infectious Co-MORBIDITIES
HANDBody imagealterations
Dyslipidaemia Abnormalities of body compositionDiabetes
The Metabolic Clinic model: a patient-centered approach in the management of HIV related non-infectious co-morbidities

Many of the end-organ complications seen in the context of HIV, are the reflection of “normal” biological ageing in
the general population....
Many of the end-organ complications seen in the context of HIV, are the reflection of “normal” biological ageing in
the general population....
• Atherosclerosis• Diabetes mellitus• Changes in body fat distribution• Reduced renal function• Osteopenia• Cancer...
What then in the context of HIV infectionmay be accelerating biological ageing?
What then in the context of HIV infectionmay be accelerating biological ageing?
Antiretroviral treatment?HIV?Immunodeficiency or immune activation?

Challenges in HIV for 2011
• Patients not aware / late presentation of disease• Controlling hidden and overt epidemic• Non-AIDS morbidity / mortality • Continued immune activation despite therapy• Long-term toxicity of treatment• When to start?

When to start antiretroviral therapy?

When to start?
• Balance between benefit from cART versus risk from cART
• Recognition of benefits from cART at higher CD4+ T-cell counts
• CD4+ T-cell count ≤ 350 cells/mm3
• Recent guidelines suggest treating at higher CD4
• Less transmission
• Less immune activation
• Less morbidity / mortality
• Debate about need for further study
Hammer SM et al. JAMA 2008; 300: 555-70

Summary
• HIV disease has changed to a chronic disease• Treatment is lifelong• A cure remains elusive• Immune function does not return to normal• Long-term co-morbidities and toxicities are
challenging• Global strategies should be identified to arrest
the epidemic

Nuova cura per l'AIDS direttamente dalVaticano!!!!!