Eziopatogenesi Ipertensione Polmonare Arteriosa-PAH Etiopathogenesis
14
PAH: Meccanismi Etiopatogenetici Ipertensione Arteriosa Polmonare: meccanismi etiopatogenetici Dr. D.Libertucci Dr. P.Solidoro S.C. Pneumologia Dip. Cardiovascolare e Toracico Direttore Dr. S.Baldi A.O.U. Molinette Torino-Italy
-
Upload
pahupdate -
Category
Health & Medicine
-
view
830 -
download
0
description
Eziopatogenesi Ipertensione polmonare Arteriosa-PAH Etiopathogenesis
Transcript of Eziopatogenesi Ipertensione Polmonare Arteriosa-PAH Etiopathogenesis

PAH: Meccanismi Etiopatogenetici
Ipertensione Arteriosa Polmonare: meccanismi etiopatogenetici
Dr. D.Libertucci Dr. P.Solidoro
S.C. Pneumologia
Dip. Cardiovascolare e Toracico
Direttore Dr. S.Baldi
A.O.U. Molinette
Torino-Italy

PAH: Meccanismi Etiopatogenetici
Ipertensione Polmonare (PH): Definizione
Si definisce ipertensione polmonare (PH) il riscontro mediante cateterismo di un aumento della pressione media in arteria polmonare (mPAP) a riposo.
Ipertensione polmonare: PAPmedia 25 mmHg
The significance of a mean PAP between 21 and 24 mmHg is unclear. Patients presenting with PAP in this range need further evaluation in
epidemiological studies
Galiè et al., Eur Hearth J 2009; 30(20)2493-2537

PAH: Meccanismi Etiopatogenetici
CLASSIFICAZIONE 4th World Symposium 2008
1. Ipertensione Arteriosa Polmonare
Idiopatica
Ereditaria
Mutazione BMPR 2
Mutazione ALK1 Endoglina
Non nota
Farmaci ed agenti tossici
Associata a (APAH): Malattie del connettivo
Infezione HIV
Ipertensione portale
Malatie congenite cardiache
Schistosomiasi
Anemia emolitica cronica
Ipertensione persistente neonato
1’. Malattia polmonare veno occlusiva (PVOD) e angiomatosi capillare polmonare (PCH)
3. Ipertensione polmonare associata a pneumopatie/ipossiemia
BPCO
Interstiziopatie
Altre patologie polmonari miste restrittive ostruttive
Disturbi del respiro durante il sonno
Malattie con ipoventilazione alveolare
Esposizione cronica alle elevate altitudini
Alterazioni dello sviluppo
2. Ipertensione polmonare da patologie del cuore sinistro
Disfunzione sistolica
Disfunzione diastolica
Valvulopatie
4. Ipertensione polmonare cronica tromboembolica
5. Ipertensioni polmonari a genesi multifattoriale o non nota1: Patologie ematologiche, mieloproliferative, splenectomia.
2: Malattie sistemiche, sarcoidosi, istiocitosi, linfangiomatosi , neurofibromatosi. Vasculiti.
3: Malattie metaboliche, GD, malattie della tiroide.
4: Altro: Neoplasie occludenti, mediastiniti fibrosanti, dialisi

PAH: Meccanismi Etiopatogenetici
Introduzione: l’endotelio
L’endotelio vasale è un organo altamente specializzato e metabolicamente attivo
Infatti:
The endothelium provides a compatible interface to facilitate blood circulation, it inherently inhibits excessive platelet aggregation and leucocyte adhesion, and it produces a balance of vasoconstrictive and vasodilatory molecules that coordinate vascular tone and serve to inhibit extracellular matrix (ECM) deposition and prevent smooth muscle cell proliferation.Abraham et al., Arthritis Res Ther 2007, 9(Suppl 2):S2

PAH: Meccanismi Etiopatogenetici
Da notare come la disfunzione endoteliale è un’importante componente, costituisce il denominatore comune, di numerose patologie ivi comprese quelle a carattere infiammatorio e fibrotiche
La risposta dell’endotelio all’insulto patogeno di qualsivoglia natura può essere distinta in due fasi:
1. Rapida: modificazione quantitativa degli effettori vascolari quali endotelina ET-1, prostaglandine (PDG), ossido nitrico (NO), fattore Von Willenbrand e attivatore tissutale del plasminogeno (tPA)
2. Lenta: comporterà una progressiva modificazione della membrana basale, rilascio di molecole che intervengono nella cinetica cellulare delle cellule muscolari lisce, dei periciti e di altri elementi cellulari mesenchimali connessi con l’albero vasale; si incrementa, altresì, il deposito di matrice extracellulare.
Abraham et al., Arthritis Res Ther 2007, 9(Suppl 2):S2

PAH: Meccanismi Etiopatogenetici
PAH: meccanismi biochimici
Fattori genetici: mutazioni della linea germinale del gene che codifica per il recettore bone morphogenetic protein receptor type II BMPR-2 (appartenente alla superfamiglia del TGF-β di tipo 2) sono state riscontrate nel 50-70% delle forme ereditarie di PAH e nel 10-30% delle forme idiopatiche. Da segnalare, a latere, anche la mutazione activin-like kinase type 1 (ALK1) ed endoglina (alterazioni geniche normalmente presenti nella teleangiectasia emorragica ereditaria)
Laneet al., Nat Genet 2000; 26:81–84.Deng et al., Am J Hum Genet, 2000;. 67:737–744.Sztrymf Am J Respir Crit Care Med 2008; 177:1377– 83. Rabinovitch J Clin Invest 2008; 118(7):2372-2379Zhang et al., Am J Physiol Lung Cell Mol Physiol 2003; 285:L740–L754.Rosenzweig et al. J Heart Lung Transplant 2008;27:668 –74.
PAH has a multifactorial pathobiology that involves various biochemical pathways and cell types.
Galiè et al., Eur heart J 2009; 30(20):2493-2537

PAH: Meccanismi Etiopatogenetici
Canali ionici: ridotta espressione e funzione dei canali del potassio voltaggio dipendete e stata messa in relazione con il BMPR-2. In relazione a questo squilibrio vi sarà un influsso di ioni Ca++ che promuoverà proliferazione cellulare e vasocostrizione.
.
Recently, it has been suggested that patients with PAH associated with BMPR2 mutations may represent a subgroup of patients with more severe disease who are less likely to demonstrate vasoreactivity than those with IPAH without BMPR2 mutations
Loss of BMPRII causes proliferation of SMCs in response to TGF-β1 and BMP2, in contrast to inhibition of SMC proliferation and susceptibility to apoptosis normally observed with expression of these cytokines. BMP, in addition to being a negative regulator of PDGF signaling, is likely a negative regulator of other growth-promoting factors implicated in the pathobiology of PAH, such as EGF.
Laneet al., Nat Genet 2000; 26:81–84.Deng et al., Am J Hum Genet, 2000;. 67:737–744.Sztrymf Am J Respir Crit Care Med 2008; 177:1377– 83. Rabinovitch J Clin Invest 2008; 118(7):2372-2379Zhang et al., Am J Physiol Lung Cell Mol Physiol 2003; 285:L740–L754.Rosenzweig et al. J Heart Lung Transplant 2008;27:668 –74. Fantozzi et al., , Am. J. Physiol. Lung Cell Mol. Physiol. 2006; 291:L993–L1004

PAH: Meccanismi Etiopatogenetici
La via Rho/Rho kinasi: svolge un ruolo importante in diverse funzioni cellulari. Da notare come il segnale a cascata intracellulare coinvolge diverse sostanze vasoattive che sono implicate nella genesi di numerose malattie cardiovascolari
Role of Rho/Rho-kinase pathway in the pathogenesis of cardiovascular diseases. Rho/Rho-kinase–mediated pathway plays an important role in the signal transduction initiated by many agonists, including angiotensin II (Ang II), serotonin (5-HT), thrombin, endothelin-1 (ET-1), norepinephrine (NE), platelet-derived growth factor (PDGF), adenosine triphosphate (ATP)/adenosine diphosphate (ADP), and urotensin II (Uro II). Through the modulation of its target effectors, Rho-kinase is substantially involved in the vascular smooth muscle contraction (via inhibition of myosin phosphatase) and in the pathogenesis of arteriosclerosis (via activation of ERM, adducin, and other effectors).
Shimokawa J Cardiovasc Pharmacol. 2002; 39: 319–327 Morrell et al., J Am Coll Cardiol 2009; 54:S10-S19 Shimokawa Arterioscler Thromb Vasc Biol 2005;25:1767-1775.

PAH: Meccanismi Etiopatogenetici
Endothelial cell injury may be triggered by various mechanisms such as bacterial or viral infection, abnormal regulation of reactive oxygen species, hypoxia, turbulent blood flow and shear stress or environmental irritants. In autoimmune diseases, the presence of anti-endothelial cell antibodies may also contribute to endothelial cell injury and apoptosis. Abraham et al., Rheumatology 2008;47:v23–v24
Endothelial dysfunction leads to chronically impaired production of vasodilator and antiproliferative agents such as NO and prostacyclin, along with overexpression of vasoconstrictor and proliferative substances such as thromboxane A2 and endothelin-1. Many of these abnormalities both elevate vascular tone and promote vascular remodelling by proliferative changes that involve several cell types, including endothelial and smooth muscle cells as well as fibroblasts
Galiè et al., Eur Heart J 2009; 30(20):2493-2537

PAH: Meccanismi Etiopatogenetici
Vasocostrizione sia direttamente attraverso legame recettoriale ETB che indirettamente
Proliferazione cellulare azione mitogena su cellule endoteliali,cellule muscolari lisce e fibroblasti
Infiammazione Azione chemiotattica granulociti neutrofili, Amplificazione citochine infiammatorie (IL-6, IL-8, TNFα) recettore ETB Monociti, Aumentata
permeabilità vascolare (recettori ETA) promozione adesione cellulare
Fibrosi proliferazione dei fibroblasti, aumentata produzione proteine matrice extracellulare
Ipertrofia arterie distali polmonari (<500 μm diametro) alterazioni della parete vasale proliferazione intimale, ipertrofia della media ed ispessimento
avventiziale
L’Endotelina rappresenta il principale mediatore patogenetico
Clozel et al., Ann Med 2005;37:2–12. Deanfield et al., J Hyperten 2005; 23:7-17 Luscher et al., Circulation 2000; 102:2434-2440 Shi-Wen et al., J Invest Dermatol 2001; 116:417-425

PAH: Meccanismi Etiopatogenetici
Endothelin-1 plays a major role in the structural and functional abnormalities in the pulmonary vasculature and in the progression of PAH-CHD and ES.
Beghetti et al., J Am Coll Cardiol 2009;53:733–40

PAH: Meccanismi Etiopatogenetici
Imbalance degli effettori vascolari
squilibrio tra fattori vasocostrittori e vasodilatatori inibitori della crescita cellulare e fattori mitogeni
determinati antitrombotici e protromboticiAUMENTO RESISTENZE VASCOLARI – INCREMENTO
POSTCARICO Vdx – TENDENZA SCOMPENSO dx

PAH: Meccanismi Etiopatogenetici
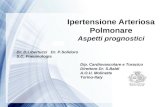
This ultimately results in vessel remodelling, withprofound changes in cellular architecture
Pathobiology of PH. Schema illustrating the different
vascular abnormalitiescompared with normal pulmonary circulation,
associated with PH. This schema depicts the abnormalities throughout the pulmonary circulation, including: (i) abnormal muscularization of distal precapillaryarteries, (ii) medial hypertrophy (thickening) of large pulmonary muscular arteries, (iii) loss of precapillary arteries, (iv) neointimal formation that is particularly occlusive in vessels 100–500 μM, (v) formation of plexiform lesions in these vessels.
Rabinovitch J Clin Invest 2008; 118(7):2372-2379