Dott.sa Marisa Pegoraro nefrologica senior. Svolgo attività clinica ... puntura della FAV... · LA...
29
Dott.sa Marisa Pegoraro, BCs, MS, infermiera nefrologica senior. Svolgo attività clinica, formativa e di sostegno alla ricerca clinica nell’ambito dell’associazione EDTNA/ERCA . Sono Presidente della Fil Italiana della stessa associazione. Non ho conflitti di interessi per l’argomento in oggetto. Sono promotore della metodica BH in Italia dal 2005, attraverso giornate di studio, workshop, pubblicazioni , traduzioni FILIALE ITALIANA
Transcript of Dott.sa Marisa Pegoraro nefrologica senior. Svolgo attività clinica ... puntura della FAV... · LA...

Dott.sa Marisa Pegoraro, BCs, MS, infermiera nefrologica senior. Svolgo attività clinica, formativa e di sostegno alla ricerca clinica nell’ambito dell’associazione EDTNA/ERCA . Sono Presidente della Fil Italiana della stessa associazione.Non ho conflitti di interessi per l’argomento in oggetto. Sono promotore della metodica BH in Italia dal 2005, attraverso giornate di studio, workshop, pubblicazioni , traduzioniFILIALE ITALIANA
LA PUNTURA DELLA FAVda momento di stress a
“occasione di cura infermieristica”
Dott.sa Marisa PegoraroInfermiera
Presidente FIL ITALIANA EDTNA/ERCA
La FAV……
• Connessione chirurgica tra un’arteria ed una vena (non è fisiologica)
• Vasi periferici, arti superiori, rari gli arti inferiori
• Ha permesso, alla fine degli anni ‘60, che la ED diventasse un trattamento cronico
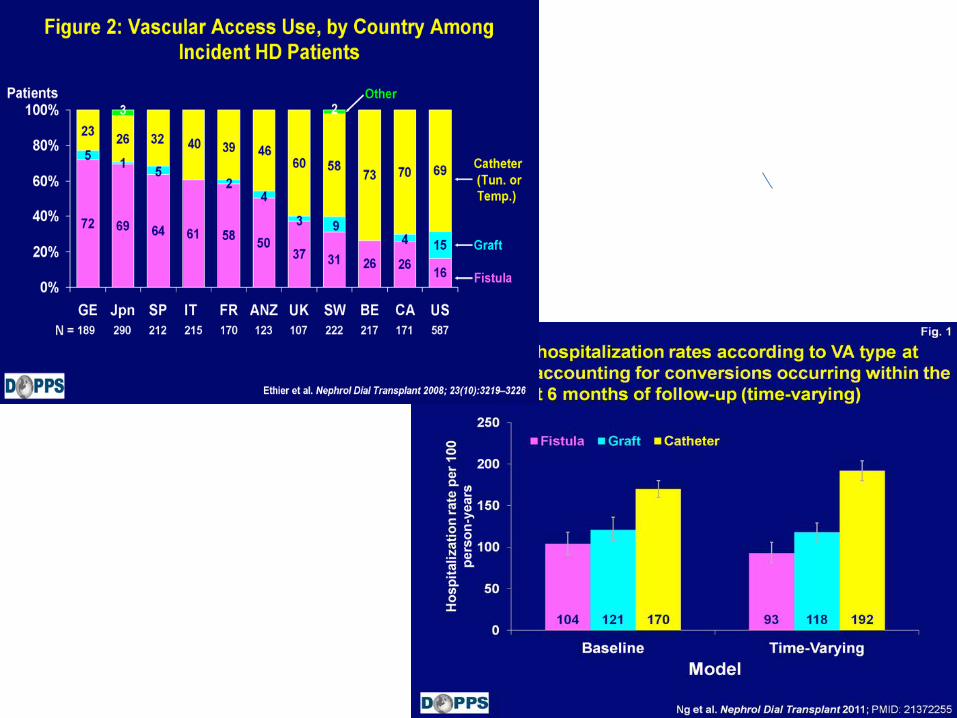
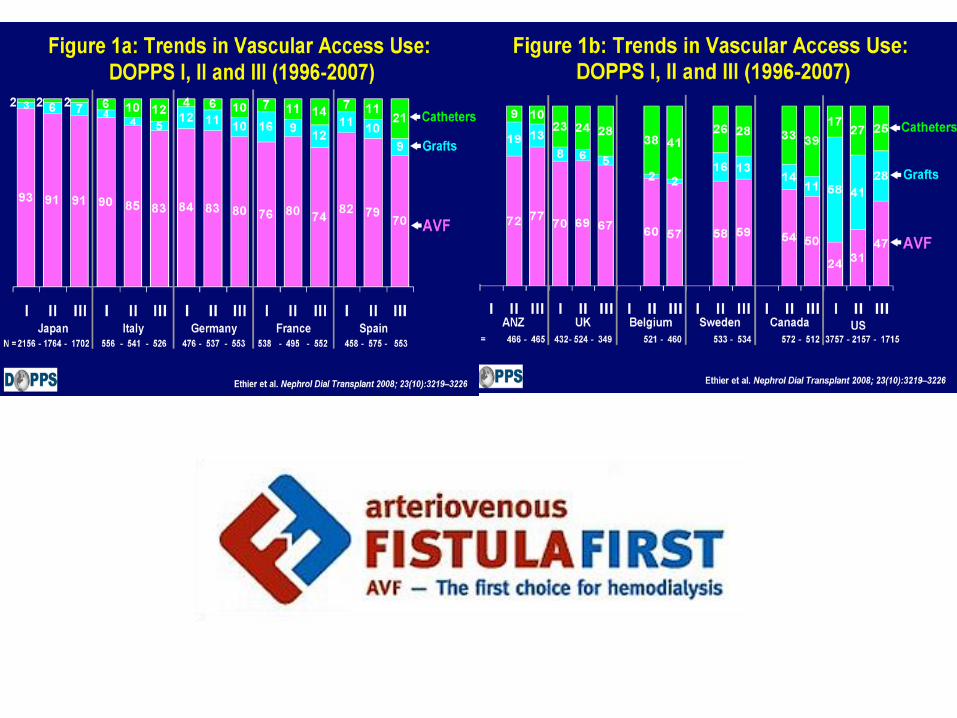
• Il miglior accesso per emodialisi (DOPPS, KDOQI, EBPGL): lunga durata, minori morbidità, migliore QdV.
0
0,2
0,4
0,6
0,8
1
0 100 200 300 400 500 600
Days
Fra
cti
on
wit
ho
ut
failu
re
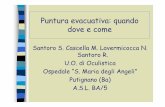
Fistula, Europe
Grafts , US
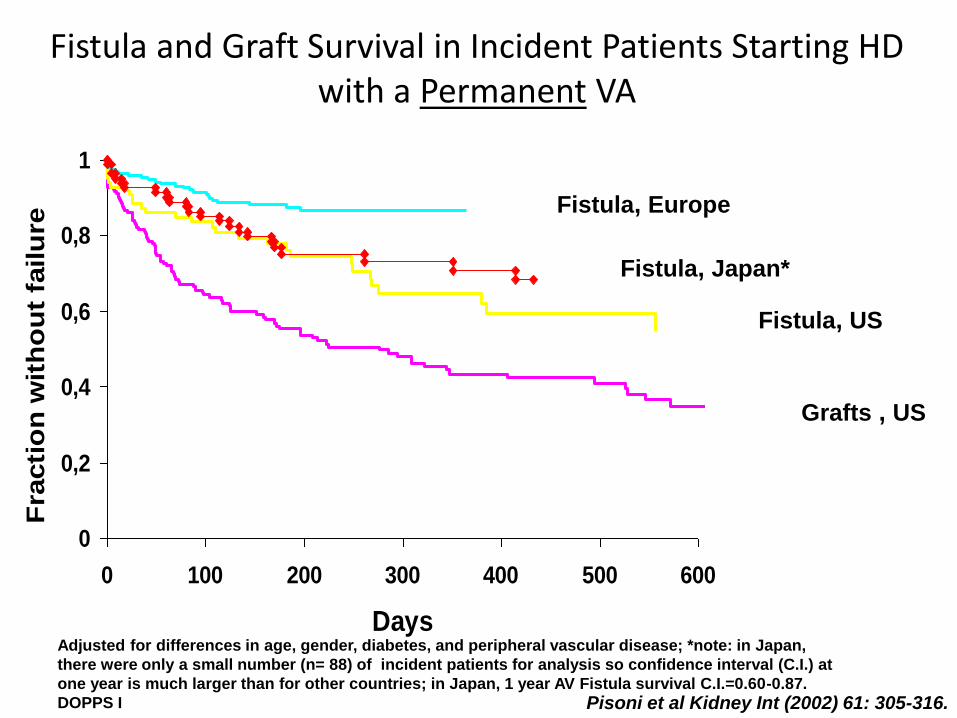
Adjusted for differences in age, gender, diabetes, and peripheral vascular disease; *note: in Japan,
there were only a small number (n= 88) of incident patients for analysis so confidence interval (C.I.) at
one year is much larger than for other countries; in Japan, 1 year AV Fistula survival C.I.=0.60-0.87.
DOPPS I
Fistula and Graft Survival in Incident Patients Starting HD with a Permanent VA
Fistula, US
Fistula, Japan*
Pisoni et al Kidney Int (2002) 61: 305-316.
0
0,2
0,4
0,6
0,8
1
0 200 400 600
Days
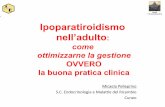
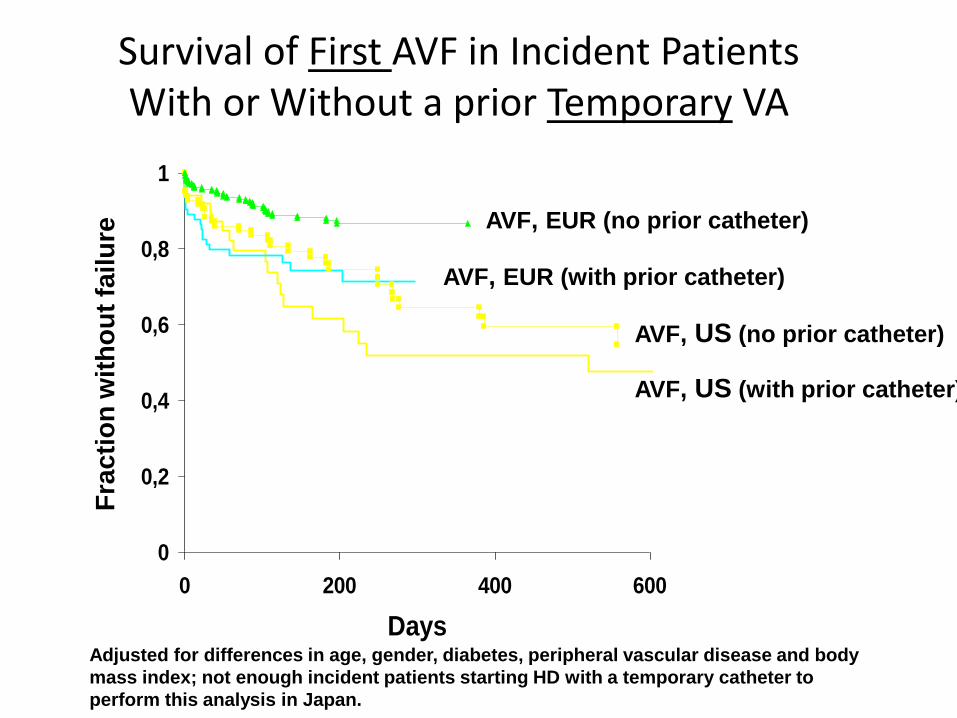
AVF, EUR (with prior catheter)
Survival of First AVF in Incident Patients With or Without a prior Temporary VA
Adjusted for differences in age, gender, diabetes, peripheral vascular disease and body
mass index; not enough incident patients starting HD with a temporary catheter to
perform this analysis in Japan.
Fra
cti
on
wit
ho
ut
failu
re
AVF, EUR (no prior catheter)
AVF, US (no prior catheter)
AVF, US (with prior catheter)
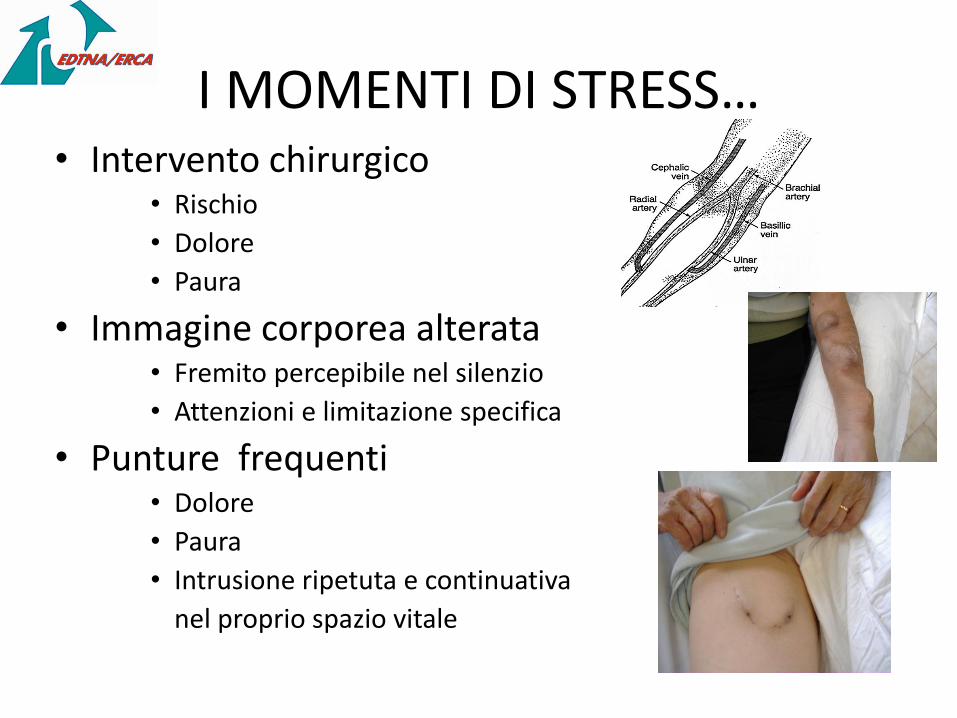
I MOMENTI DI STRESS…• Intervento chirurgico
• Rischio
• Dolore
• Paura
• Immagine corporea alterata• Fremito percepibile nel silenzio
• Attenzioni e limitazione specifica
• Punture frequenti • Dolore
• Paura
• Intrusione ripetuta e continuativa
nel proprio spazio vitale
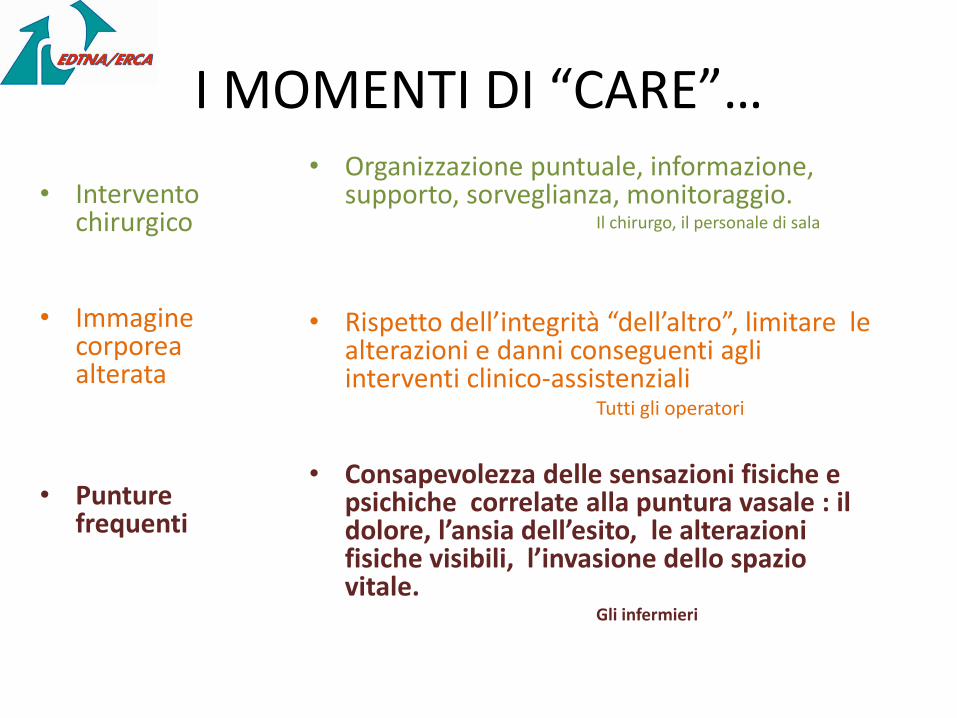
I MOMENTI DI “CARE”…
• Intervento chirurgico
• Immagine corporea alterata
• Punture frequenti
• Organizzazione puntuale, informazione, supporto, sorveglianza, monitoraggio.
Il chirurgo, il personale di sala
• Rispetto dell’integrità “dell’altro”, limitare le alterazioni e danni conseguenti agli interventi clinico-assistenziali
Tutti gli operatori
• Consapevolezza delle sensazioni fisiche e psichiche correlate alla puntura vasale : il dolore, l’ansia dell’esito, le alterazioni fisiche visibili, l’invasione dello spazio vitale.
Gli infermieri
LA PUNTURA DELLA FAV
COMPENTENZA INFERMIERISTICA SPECIALISTICANurses' impact on the choiches and longevity of Vascular Access.D, Maples. Nephrol Nurs J. 2005 Nov-Dec;32(6):670-4 PMID:16425812, NNJ, p. 670-674.
V A S – Vascular Access Nurse (VAC, VAM)
R A V – Referente Accessi Vascolari
Vascular access: a role for a renal nurse clinician. D, Waterhouse. EDTNA ERCA J. 2002 Apr-Jun;28(2):64-6, 69. - PMID:12216845.
Investing in the lifeline: the value of a vascular access coordinator. LC., Dinwiddie. NephrolNews Issues. 2003 May;17(6):49, 52-3 - PMID:12778617.
Effect of a vascular access nurse coordinator to reduce central venous catheter use in incident hemodialysis patients: a quality improvement report. Polkinghorne KR, Seneviratne M, Kerr PG. Am J Kidney Dis. 2009 Jan;53(1):99-106 - PMID:18805614.
• Chi punge…(le infermiere/i)……
• Chi l’ha fatta (sempre meno nefrologi)..
• Le linee guida … (conoscerle ed usarle)….
• L’evidenza scientifica.. (codificare le procedure
per verificare il migliore risultato)
Chi decide la tecnica puntura da usare?
Qual’è la tecnica migliore?Quella che :
• Dipende dall’accesso (fav, loop)
• Dipende dal sito (prox, dist, superf, prof.)
• Dipende dal paziente ()
• Dipende dai risultati………. (chi li raccoglie?)
• NON dipende dall’operatore (nessuno ama sbagliare)
• NON dipende dalle consuetudini (abbiamo sempre fatto così)
• NON dipende ….. da niente (ma da come lo si fa)
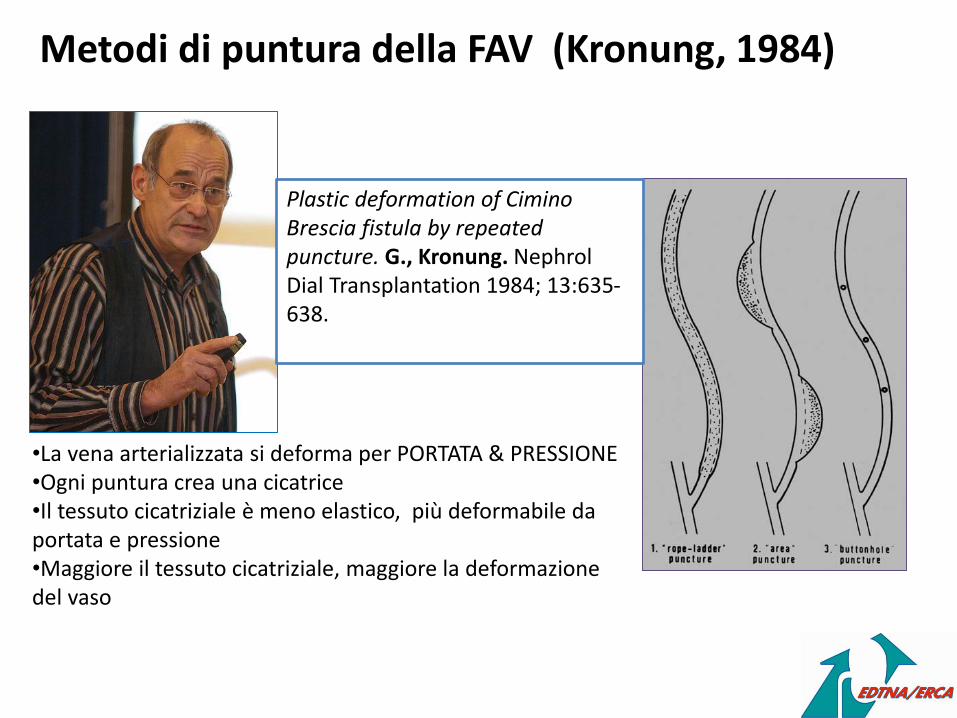
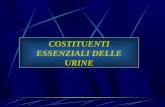
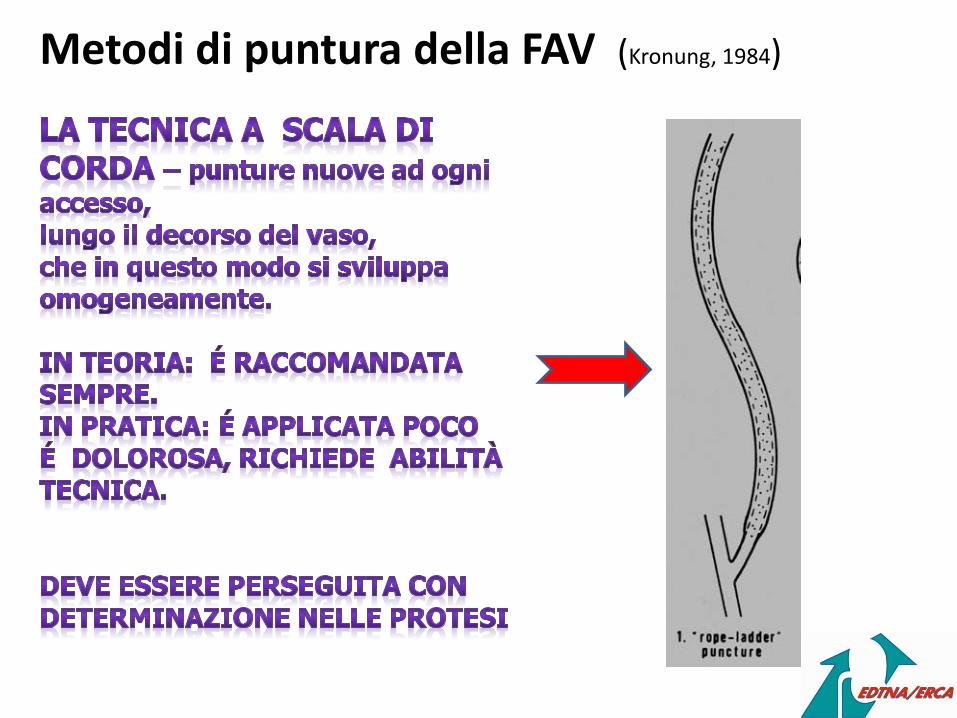
Metodi di puntura della FAV (Kronung, 1984)
Plastic deformation of CiminoBrescia fistula by repeated puncture. G., Kronung. NephrolDial Transplantation 1984; 13:635-638.
•La vena arterializzata si deforma per PORTATA & PRESSIONE•Ogni puntura crea una cicatrice•Il tessuto cicatriziale è meno elastico, più deformabile da portata e pressione•Maggiore il tessuto cicatriziale, maggiore la deformazione del vaso
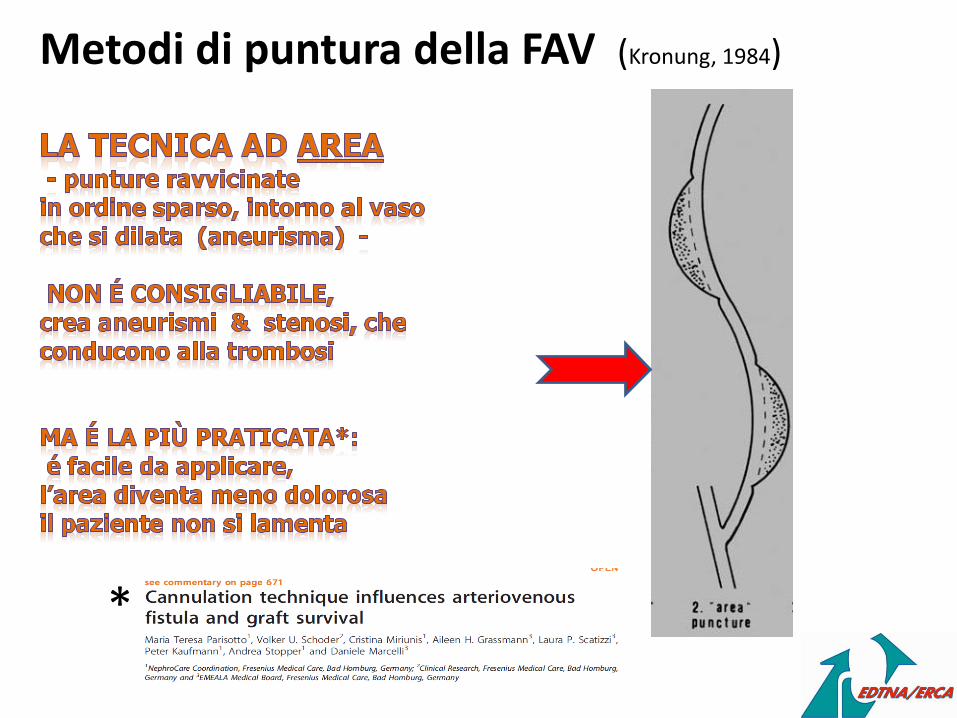
Metodi di puntura della FAV (Kronung, 1984)
Metodi di puntura della FAV (Kronung, 1984)
*
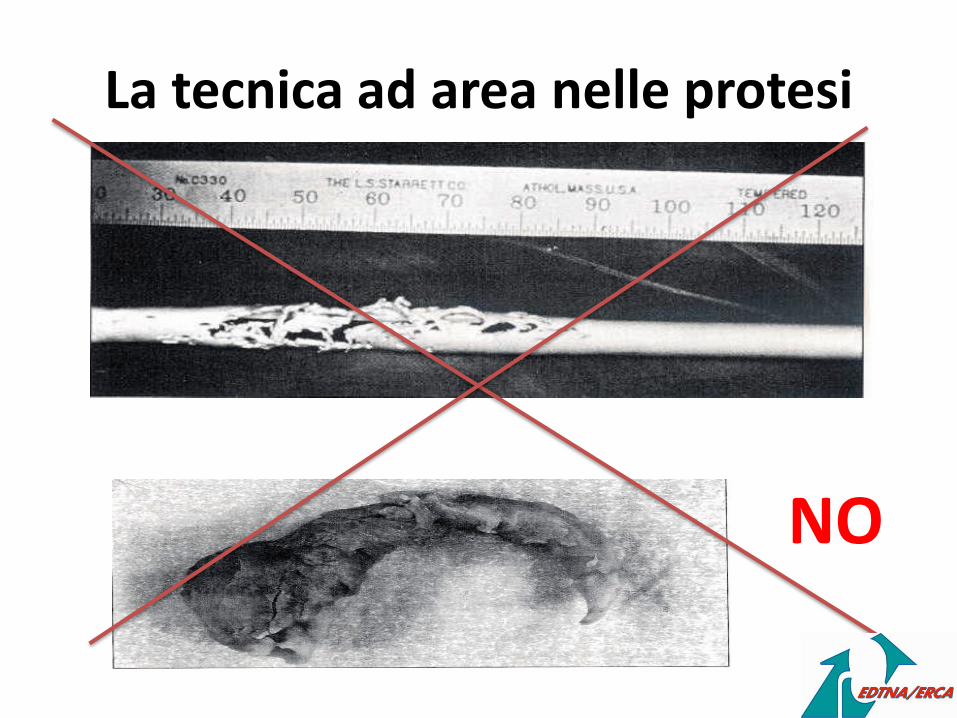
La tecnica ad area nelle protesi
NO
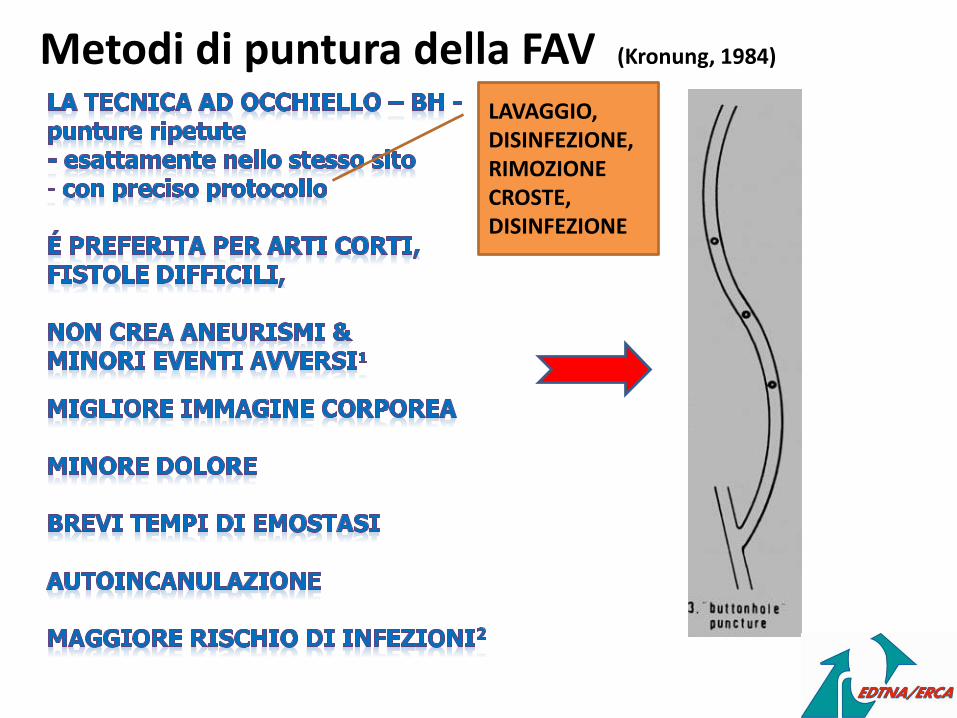
Metodi di puntura della FAV (Kronung, 1984)
LAVAGGIO, DISINFEZIONE, RIMOZIONE CROSTE, DISINFEZIONE
POTENZIALE MAGGIORE RISCHIO DI INFEZIONI :
VERO? FALSO ?
BUTTON HOLE
BUTTON HOLE
QUALI I DATI DI EVIDENZA?
NEI PRIMI 5 ANNI MOLTI DATI OSSERVAZIONALI (bassi livelli evidenza)molto entusiasmo e poca esperienza
NEGLI ULTIMI 5 ANNI alcuni studi RCT e revisioni sistematiche della letteraturamaggiore consapevolezza e molte critiche
QUALI DIFFERENZE?
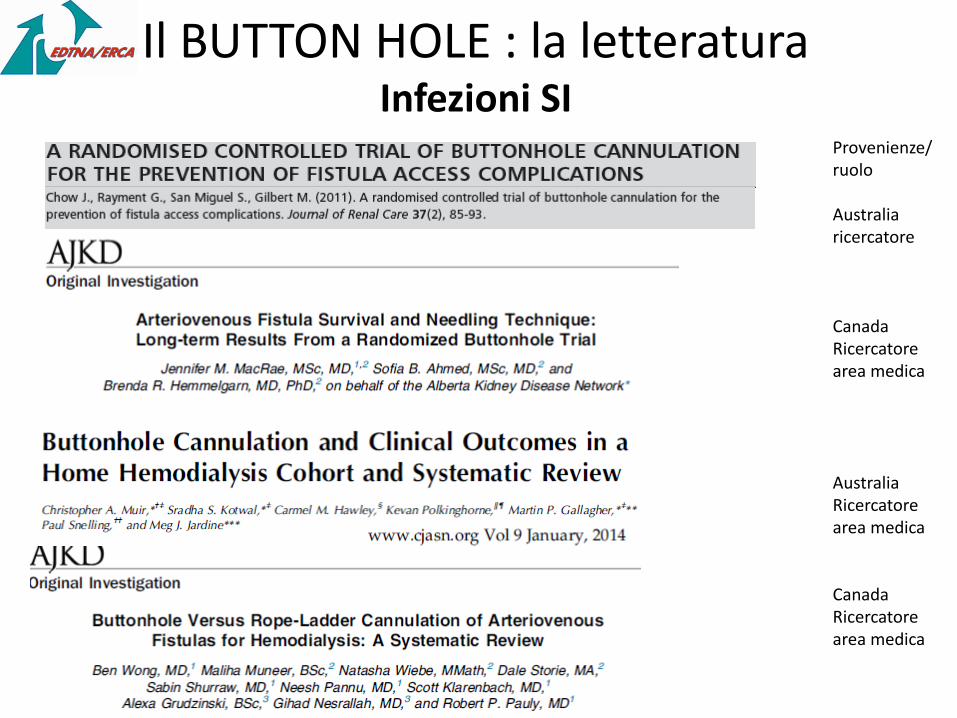
Il BUTTON HOLE : la letteraturaInfezioni SI
Provenienze/ruolo
Australiaricercatore
CanadaRicercatore area medica
Australia Ricercatore area medica
Canada Ricercatore area medica
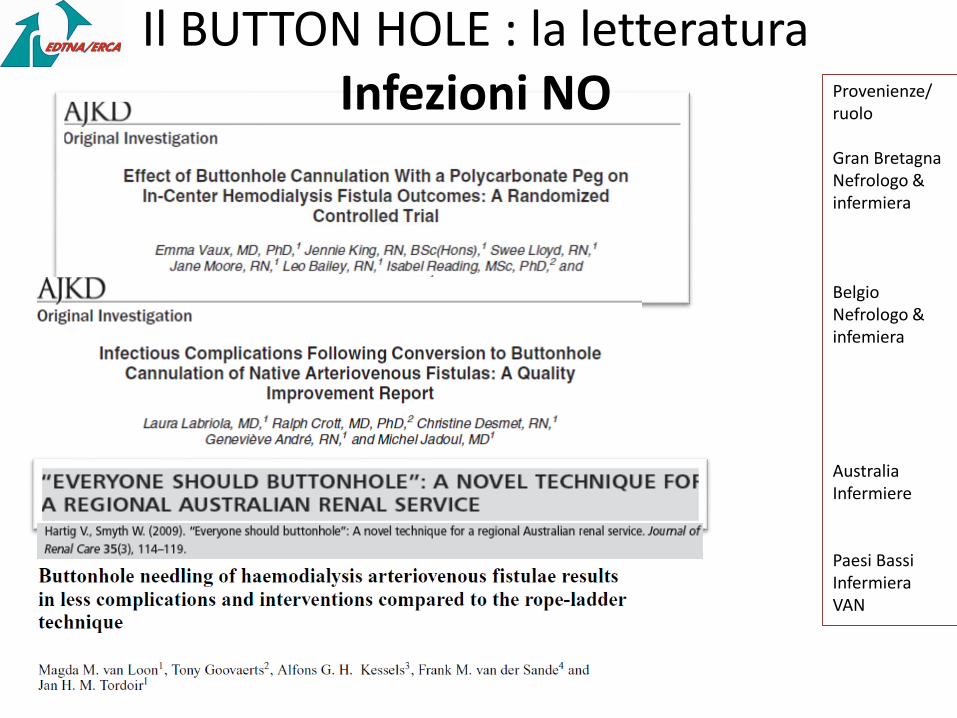
Il BUTTON HOLE : la letteraturaInfezioni NO Provenienze/
ruolo
Gran Bretagna Nefrologo & infermiera
Belgio Nefrologo & infemiera
Australia Infermiere
Paesi BassiInfermiera VAN
Altri contributi infermieristici
Managing the risks of buttonhole cannulation
Altri contributi infermieristici
DISCUSSION FORUM forRenal professionals
“...None of the contributors to RenalPro doubted that BH has led to very serious infections, many had seen them first-hand, but there was a feeling that the benefits of BH and the potential for improvements in practice had not been considered.”
There was concern that staff and patients used to cannulating established buttonholes would not have the skill and/or experience to switch to rope-ladder and would use area puncture, especially where only a short segment of the fistula is accessible.
Benefits of BH observed by advocates of the technique also included shorter post-dialysis bleeding time, fewer infiltrations and increased willingness for patients to self-cannulate
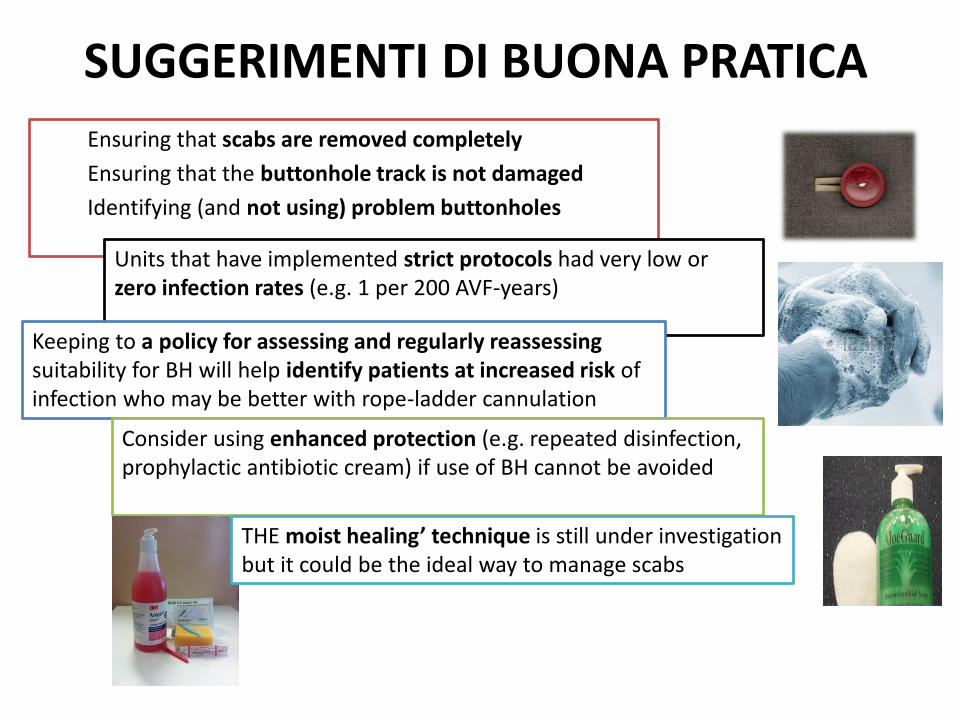
SUGGERIMENTI DI BUONA PRATICA
Ensuring that scabs are removed completely
Ensuring that the buttonhole track is not damaged
Identifying (and not using) problem buttonholes
Units that have implemented strict protocols had very low or zero infection rates (e.g. 1 per 200 AVF-years)
Keeping to a policy for assessing and regularly reassessing suitability for BH will help identify patients at increased risk of infection who may be better with rope-ladder cannulation
Consider using enhanced protection (e.g. repeated disinfection, prophylactic antibiotic cream) if use of BH cannot be avoided
THE moist healing’ technique is still under investigation but it could be the ideal way to manage scabs
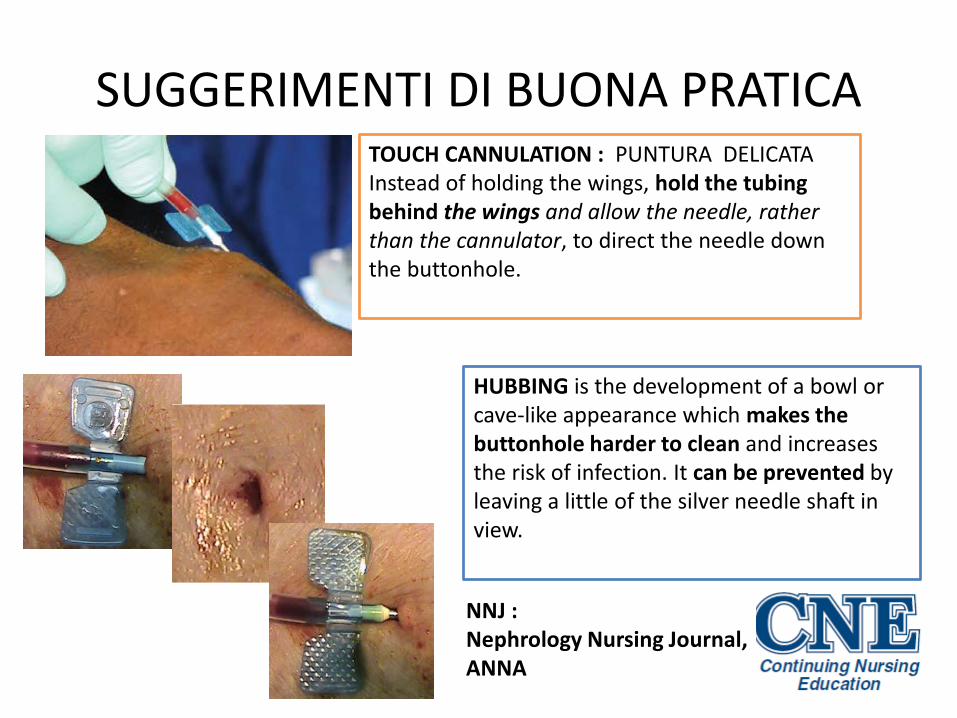
SUGGERIMENTI DI BUONA PRATICATOUCH CANNULATION : PUNTURA DELICATAInstead of holding the wings, hold the tubing behind the wings and allow the needle, rather than the cannulator, to direct the needle down the buttonhole.
HUBBING is the development of a bowl or cave-like appearance which makes the buttonhole harder to clean and increases the risk of infection. It can be prevented by leaving a little of the silver needle shaft in view.
NNJ : Nephrology Nursing Journal, ANNA
LINEE GUIDA PER UTILIZZO DEL BH
BH: CURA o STRESS?La tecnica BH si è rivelata essere
• Un detonatore di consapevolezza, • Un indicatore di qualità• Uno stimolo alla ricerca• Uno strumento di empatia e rispetto• Uno strumento di autonomia• Un argomento di riflessione • Una possibilità di scelta • Una scoperta di potenziali celati
………………………………………………………….
Se tutto ciò per voi è STRESS……..
NON PRATICATE IL BH…..
Avrete sicuramente dati negativi
Se tutto ciò per voi è CURA ALLA PERSONA,
……….PRATICATE il BH perché sarà
fonte di grandi soddisfazioni e ottimi
dati di evidenza.
BH: CURA o STRESS?
Grazie per l’attenzione
www.edtna-erca.itwww.edtnaerca.orgwww.anna.orgwww.brs.orgwww.vas.org