Depressione in gravidanza e nel puerperio - Medeacom s.r.l. - Settembre/28-09 Lundbeck... ·...
47
Depressione in gravidanza e nel puerperio Daniele La Barbera Dipartimento di Biomedicina sperimentale e Neuroscienze cliniche Sezione di Psichiatrica Università di Palermo Caltanissetta, 28 Settembre 2010
Transcript of Depressione in gravidanza e nel puerperio - Medeacom s.r.l. - Settembre/28-09 Lundbeck... ·...
Depressione in gravidanza e
nel puerperio
Daniele La Barbera
Dipartimento di Biomedicina sperimentale e
Neuroscienze cliniche Sezione di Psichiatrica
Università di Palermo
Caltanissetta, 28 Settembre 2010
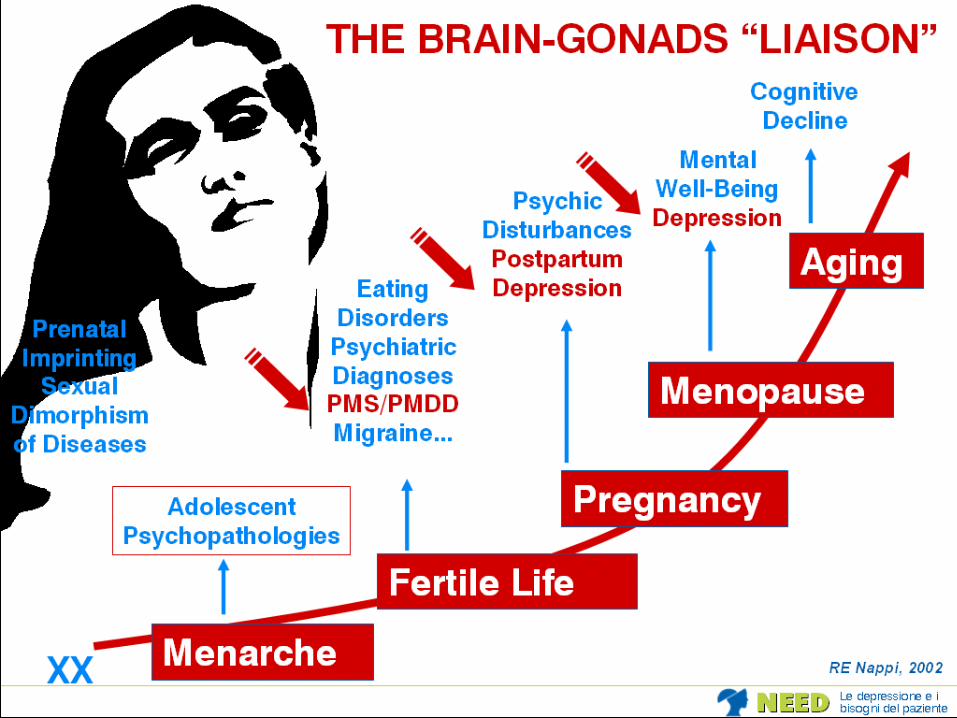
Il tempo
biologico e
psichico della
donna è un
tempo
ritmico.
Tutta la vita
psicobiologica
e sessuale
della donna è
inserita in una
dimensione
temporale
Aree cliniche di confine tra ginecologia
psicologia e psichiatria
• Sindrome premestruale
• Dismenorrea
• Pseudogravidanza psicogena
• Ipermenorrea, metrorragia
• Dolore pelvico
• Sterilità psicogena
• Aborto spontaneo
• Psicoprofilassi al parto
• Depressione in gravidanza
• Depressione puerperale
• Menopausa

Depressione Maggiore
• esordio: 3° decade di vita
• durata episodio: 20 settimane (mediana)
• frequenza episodi: 4 (mediana) nella vita
Depressione Maggiore
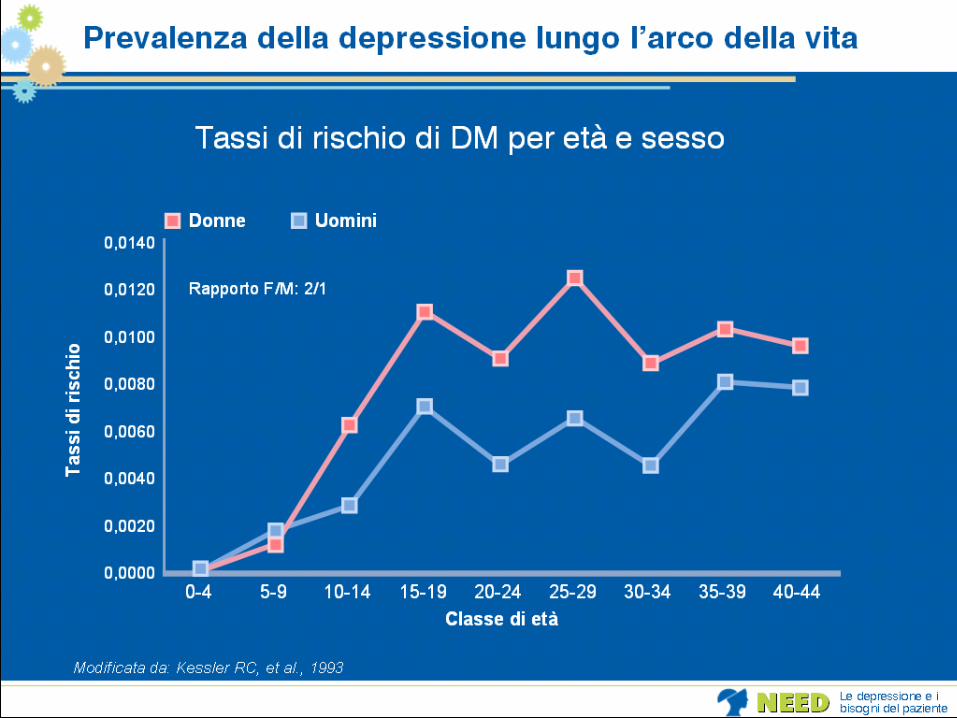
• 2 volte più frequente nelle donne:
15-54 anni donne 21%, uomini 12%
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15)
• prevalenza attuale o nel corso della vita
rapporto uomo: donna di 2:1
(Kuehner, Acta Psychiatr Scand 2003; 108: 163-174)
Perché la Depressione Maggiore è più frequente nelle donne ?
• fattori genetici: non vi sono dati univoci (?);
• eventi traumatici nell’infanzia: bambine più a rischio di abusi fisici e più
sensibili al loro effetto;
• fluttuazioni ormonali: le donne presentano episodi depressivi in risposta a
fluttuazioni degli ormoni sessuali e soffrono maggiormente di disfunzioni tiroidee;
• disturbi d’ansia: le donne ne soffrono maggiormente;
• stile cognitivo: donne più inclini alla ruminazione e all’autocommiserazione;
• ruolo sociale: nella donna sono più frequenti ruoli frustranti (casalinga),
conflittuali o eccessivamente onerosi (casa-lavoro, discriminazione..);
• eventi stressanti: le donne presentano più frequentemente un episodio
depressivo dopo un evento negativo rilevante.
(Piccinelli e Wilkinson, Br J Psychiatry 2000; 177:486-492)
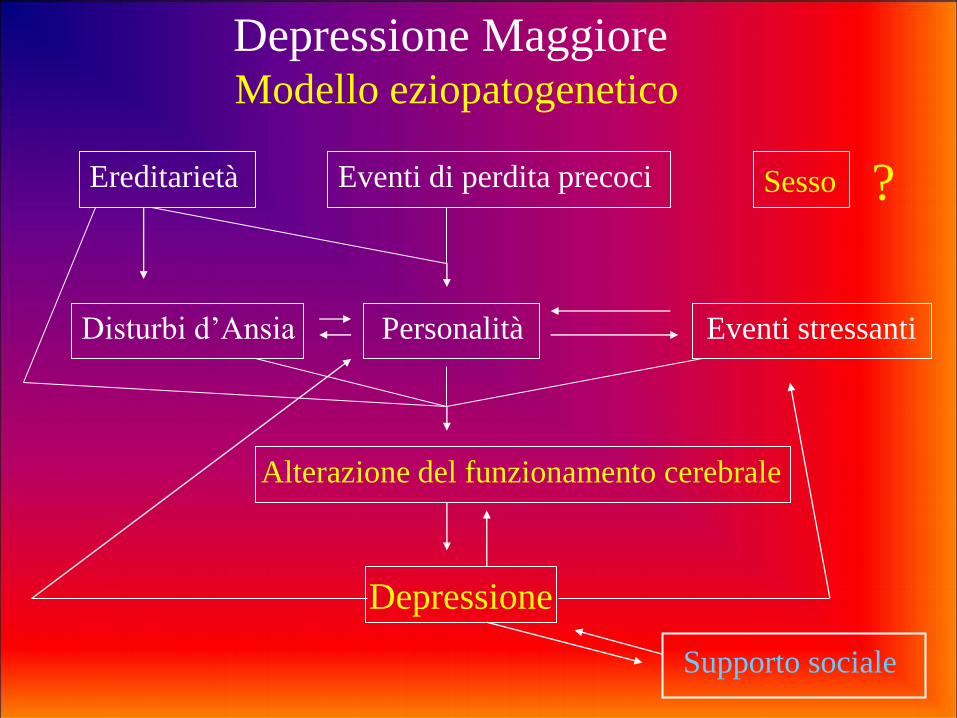
Depressione Maggiore Modello eziopatogenetico
Ereditarietà Eventi di perdita precoci Sesso
Personalità Eventi stressanti
Alterazione del funzionamento cerebrale
Depressione
Disturbi d’Ansia
Supporto sociale
?
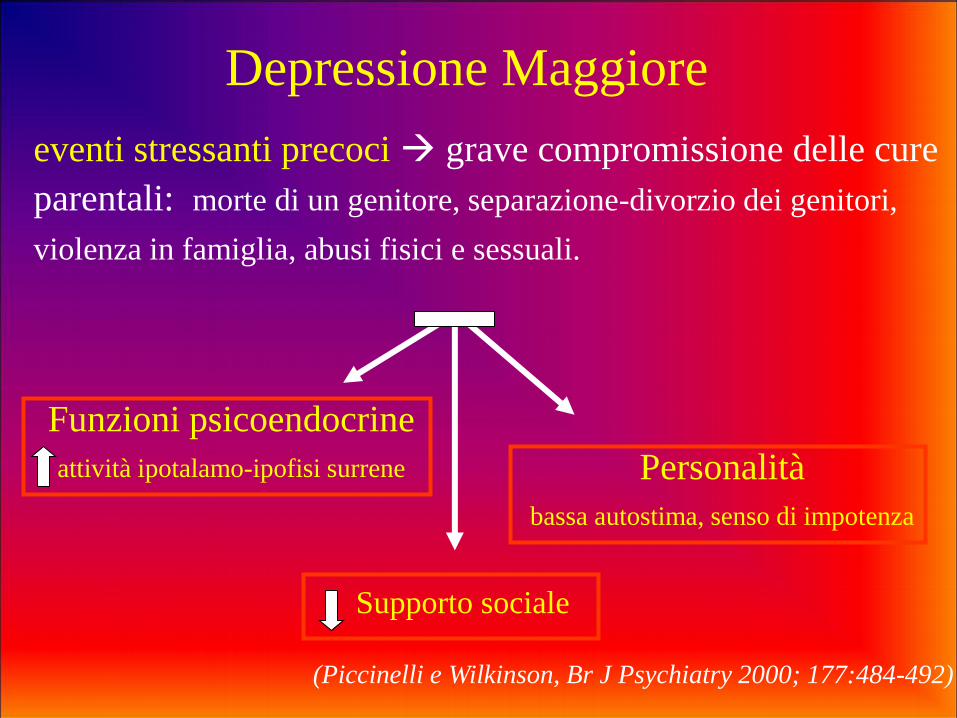
Depressione Maggiore
eventi stressanti precoci grave compromissione delle cure
parentali: morte di un genitore, separazione-divorzio dei genitori,
violenza in famiglia, abusi fisici e sessuali.
(Piccinelli e Wilkinson, Br J Psychiatry 2000; 177:484-492)
Funzioni psicoendocrine
attività ipotalamo-ipofisi surrene Personalità
bassa autostima, senso di impotenza
Supporto sociale
Sistema ipotalamo-ipofisi-surrene
L’elevazione dei livelli di glucocorticoidi è una caratteristica
della risposta allo stress nei mammiferi.
Stress cronico persiste l’aumento dei glucocorticoidi, mentre si
riducono i livelli di NA, 5HT, DA, GABA
CRF nell’animale induce comportamenti “depressivi”.
Il riscontro di elevati livelli di glucocorticoidi si ritrova nel 20-
40% dei pazienti depressi ambulatoriali e nel 40-60% di quelli
ricoverati (più frequenti nella depressione melancolica).
In genere l’ipercortisolemia si risolve in seguito al trattamento;
se persiste indica un rischio elevato di ricaduta.
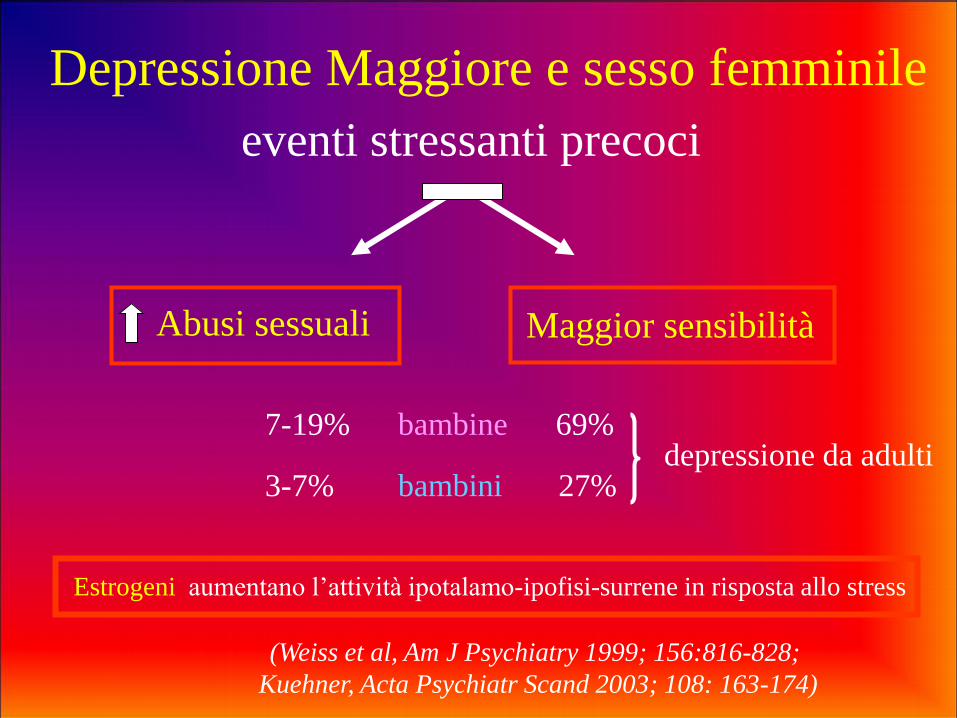
Depressione Maggiore e sesso femminile
eventi stressanti precoci
Abusi sessuali Maggior sensibilità
7-19% bambine 69% depressione da adulti 3-7% bambini 27%
Estrogeni aumentano l’attività ipotalamo-ipofisi-surrene in risposta allo stress
(Weiss et al, Am J Psychiatry 1999; 156:816-828;
Kuehner, Acta Psychiatr Scand 2003; 108: 163-174)
Nelle donne:
• maggior frequenza di scarsa autostima, insicurezza, senso di inadeguatezza, di impotenza e di disperazione; • maggior tendenza alla ruminazione, all’autocommiserazione, al pessimismo.
Disturbi depressivi e caratteristiche di personalità
(Piccinelli e Wilkinson, Br J Psychiatry 2000; 177:484-492
Kuehner, Acta Psychiatr Scand 2003; 108: 163-174)
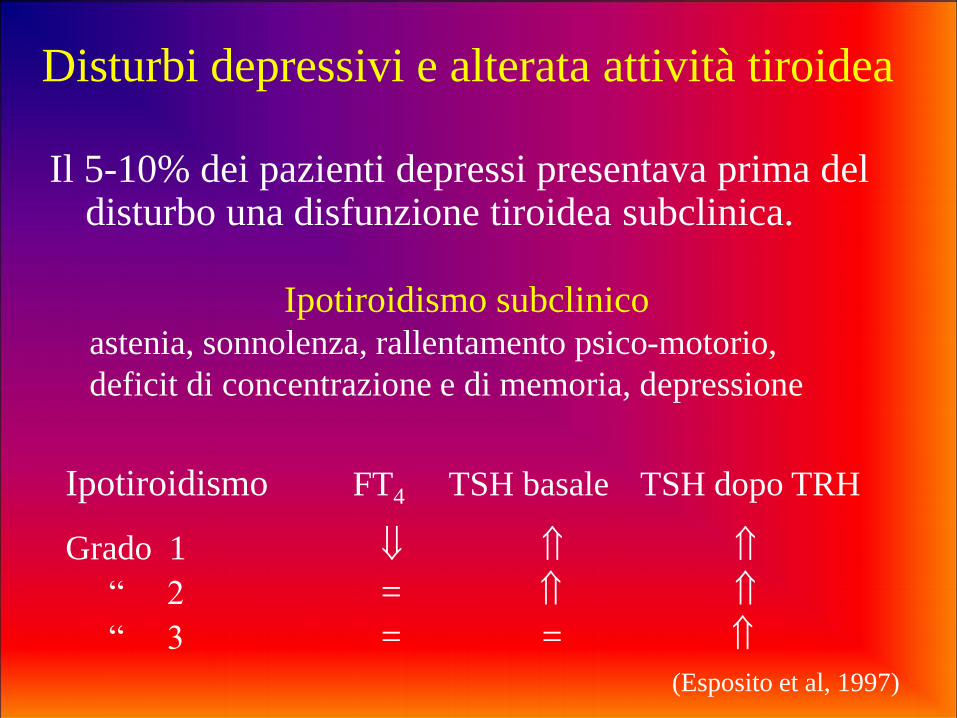
Disturbi depressivi e alterata attività tiroidea
Il 5-10% dei pazienti depressi presentava prima del disturbo una disfunzione tiroidea subclinica.
Ipotiroidismo subclinico astenia, sonnolenza, rallentamento psico-motorio,
deficit di concentrazione e di memoria, depressione
Ipotiroidismo FT4 TSH basale TSH dopo TRH
Grado 1
“ 2 =
“ 3 = =
(Esposito et al, 1997)
Depressione Maggiore
Caratteristiche cliniche
Nelle donne più frequente:
• la comparsa nel periodo novembre-febbraio
• un maggior numero di sintomi
• ipersonnia, iperfagia, reattività umore, ipersensibilità al rifiuto
• tentativi di suicidio (suicidio nell’uomo)
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15)
• pubertà
• fase premestruale
• puerperio
• peri-menopausa
• gravidanza e aborto
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15)
Nelle donne (predisposte) la depressione maggiore
si manifesta più frequentemente nei periodi di
intense fluttuazioni degli ormoni sessuali:

Disturbi Depressivi del Puerperio
• Maternity Blues (Postpartum Blues, Baby Blues)
• Depressione Maggiore ad esordio nel
postpartum
• Psicosi puerperale

Maternity Blues
• Prevalenza: 50-85% donne.
• Esordio: entro pochi giorni dal parto (48 ore).
• Sintomi: tristezza, tendenza al pianto, sentimenti di
insufficienza e di incapacità, irritabilità, ansia, difficoltà
di concentrazione e di memoria, disturbi del sonno e
dell’appetito, cefalea, astenia.
• Remissione: entro 2 settimane. Durata protratta:
comparsa di depressione postpartum.
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15
Steiner et al. J Affect Disord 2003;74:67-83)

Depressione Post-partum
- Esordio: primi tre mesi dal parto (primo mese).
- Prevalenza: 10-22%
- Sintomatologia : sovrapponibile alla Depressione Maggiore
- Effetti sullo sviluppo psichico del bambino: attaccamento insicuro e ambivalente, compromissione tono emozionale, sviluppo cognitivo e relazionale, manifestazioni psicopatologiche
- Prognosi: remissione entro 6-12 mesi
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15
Steiner et al. J Affect Disord 2003;74:67-83)
Psicosi Post-partum
• Prevalenza: 0.1-0.3 % di puerpere.
• Esordio: prima settimana dopo il parto (48-72 ore).
• Sintomi: intense e rapide oscillazioni dello stato di coscienza, allucinazioni visive o uditive a contenuto triste o terrifico, temi deliranti di tipo persecutorio o depressivo e incentrati sulla relazione madre-bambino, ansia, agitazione; rischio di suicidio e di infanticidio.
• Prognosi: favorevole con remissione in 6-12 mesi nell’ 80% casi; tendenza alla ricorrenza nel postpartum (75-90%). 70% Disturbo Bipolare o Depressione Maggiore con aspetti psicotici
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15
Steiner et al. J Affect Disord 2003;74:67-83)
• caduta ormoni placentari
• ipotiroidismo (in un sottogruppo)
• ambivalenza nei confronti del neonato
• stress connesso al ruolo materno
• esaurimento fisico; alterata attività asse ipotalamo-ipofisi-
surrene
•sonno insufficiente
• pregressi episodi di depressione o disturbo bipolare
• recenti eventi stressanti
• temperamento del neonato
• complicazioni perinatali
• scarso supporto familiare
Disturbi del puerperio
Eziologia
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15
Steiner et al. J Affect Disord 2003;74:67-83)
Depressione Maggiore in gravidanza
Rischi se la depressione non è trattata:
• scarsa igiene della gravidanza
• rischio suicida
• impulsività
• alterazioni neuro-endocrine (ipercortisolemia)
• stress materno prenatale -->minor peso e minore età gestazionale
Nell’animale lo stress materno --> aborto, basso peso, ipossia,
ipotensione, ritardo di crescita, difficoltà di apprendimento
(Wisner et al, 2000)
Prevalenza: 9% primo episodio in gravidanza
14% ricaduta
What are the signs of depression during pregnancy? Women with depression usually experience some of the following symptoms for 2 weeks or more:
•Persistent sadness
•Difficulty concentrating
•Sleeping too little or too much
•Loss of interest in activities that you usually enjoy
•Recurring thoughts of death, suicide, or hopelessness
•Anxiety
•Feelings of guilt or worthlessness
•Change in eating habits
What are possible triggers of depression during pregnancy? •Relationship problems
•Family or personal history of depression
•Infertility treatments
•Previous pregnancy loss
•Stressful life events
•Complications in pregnancy
What can happen if depression is not treated?
Untreated depression can hurt the mother and her baby. Some
women with depression have a hard time caring for themselves
during pregnancy. They may:
Eat poorly
Not gain enough weight
Have trouble sleeping
Miss prenatal visits
Not follow medical instructions
Use harmful substances, like tobacco, alcohol, or illegal drugs
Depression during pregnancy can raise the risk of:
Problems during pregnancy or delivery
Having a low-birth-weight baby
Premature birth
Aborto
Entro 6 mesi dall’aborto :
• Depressione Maggiore - 11% primo episodio
- 54% se episodi pregressi
- rischio 5 volte maggiore in assenza
di figli
• Gravidanza entro 1 anno: aumenta il rischio di depressione
dopo 1 anno: non aumenta il rischio di depressione
(Burt e Stein, J Clin Psychiatry 2002; 63 (suppl 7): 9-15)
Le classi di psicofarmaci con i più intensi effetti teratogeni
sono i Sali di litio e gli anticonvulsivanti
Gli SSRI sono i farmaci antidepressivi più comunemente
prescritti, per la loro efficacia e per il miglior profilo di tollerabilità
e sicurezza, rispetto ai più vecchi antidepressivi.
Tuttavia studi hanno dimostrato che l’esposizione ai farmaci SSRI
nella fase tardiva della gravidanza è associata a complicanze di
breve periodo nei neonati, tra cui il distress respiratorio lieve,
irritabilità, problemi di alimentazione, ittero e convulsioni.
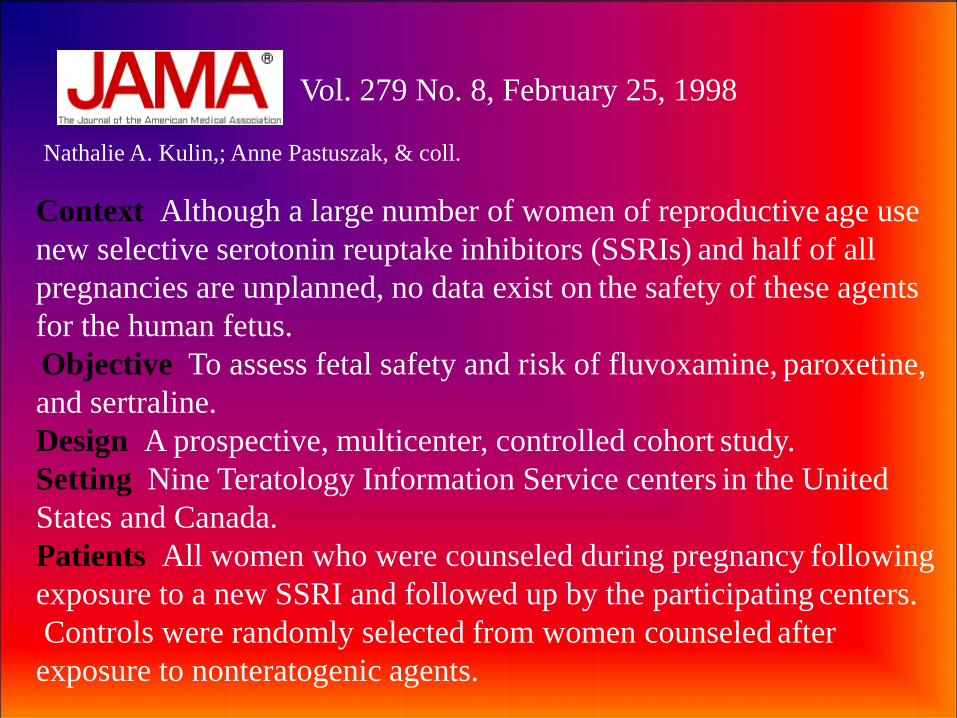
Vol. 279 No. 8, February 25, 1998
Nathalie A. Kulin,; Anne Pastuszak, & coll.
Context Although a large number of women of reproductive age use
new selective serotonin reuptake inhibitors (SSRIs) and half of all
pregnancies are unplanned, no data exist on the safety of these agents
for the human fetus. Objective To assess fetal safety and risk of fluvoxamine, paroxetine,
and sertraline.
Design A prospective, multicenter, controlled cohort study.
Setting Nine Teratology Information Service centers in the United
States and Canada.
Patients All women who were counseled during pregnancy following
exposure to a new SSRI and followed up by the participating centers.
Controls were randomly selected from women counseled after
exposure to nonteratogenic agents.
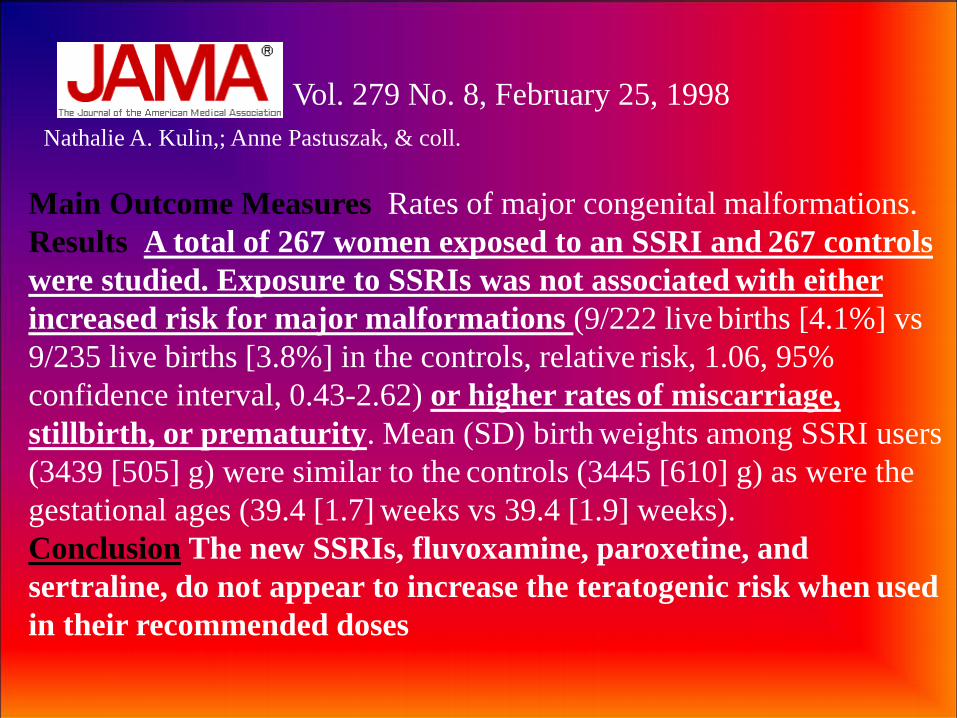
Vol. 279 No. 8, February 25, 1998
Nathalie A. Kulin,; Anne Pastuszak, & coll.
Main Outcome Measures Rates of major congenital malformations.
Results A total of 267 women exposed to an SSRI and 267 controls
were studied. Exposure to SSRIs was not associated with either
increased risk for major malformations (9/222 live births [4.1%] vs
9/235 live births [3.8%] in the controls, relative risk, 1.06, 95%
confidence interval, 0.43-2.62) or higher rates of miscarriage,
stillbirth, or prematurity. Mean (SD) birth weights among SSRI users
(3439 [505] g) were similar to the controls (3445 [610] g) as were the
gestational ages (39.4 [1.7] weeks vs 39.4 [1.9] weeks).
Conclusion The new SSRIs, fluvoxamine, paroxetine, and
sertraline, do not appear to increase the teratogenic risk when used
in their recommended doses
Volume 193, Issue 6, December 2005
Anna Sivojelezova
Citalopram use in pregnancy: Prospective comparative
evaluation of pregnancy and fetal outcome
Objective Citalopram is a selective serotonin reuptake inhibitor indicated for depression.
The safety of this medication in pregnancy has not been fully established. The purpose
of this study was to investigate whether citalopram is associated with an increased
incidence of adverse pregnancy outcomes.
Study design Pregnant women who contacted the Motherisk Program, a Teratogen Information
Center in Toronto, Ontario, with regard to the safety of citalopram in pregnancy were
enrolled in the study. The exposed women were matched to a disease-matched group
of women and a nonteratogenic group.
All women were matched for age (± 2 years) and gestational age at time of first call
to the Motherisk (± 2 weeks). A structured telephone follow-up interview was
conducted following the expected date of confinement.
Volume 193, Issue 6, December 2005
Results The total number of pregnant women enrolled in this study was 396 (132 women in
each group). A total of 125 women took citalopram at least in the first trimester.
Seventy-one (54%) women continued to take the drug throughout pregnancy.
One hundred fourteen women (86%) had live births, 14 (11%) had spontaneous
abortions, 2 (1.5%) had elective terminations, and 2 (1.5%) experienced stillbirths.
Fetal survival rates, mean birth weights, and duration of pregnancy were not
statistically different among the 3 groups. Of 108 live-born infants whose mothers
were exposed to citalopram in the first trimester, there was 1 (0.9%) male infant
born with a major malformation. There was a relative risk of 4.2 (95% confidence
interval 1.71-10.26) in neonates exposed to citalopram close to term to be admitted
to special-care nurseries as compared with the unexposed infants.
Conclusion Citalopram use during the period of embryogenesis in pregnancy is not associated
with an apparent major teratogenic risk. Late pregnancy use of citalopram is associated
with increased risk of poor neonatal adaptation syndrome, recently described with
other selective serotonin reuptake inhibitors.
Neonatal Adaptation Syndrome
In recent years there has been increasing recognition of a set of
neurobehavioral signs in infants born to mothers taking antidepressants.
This ‘syndrome’ has been given a number of names including Neonatal
Adaptation Syndrome, Neonatal Abstinence Syndrome, Neonatal
Withdrawal Syndrome and Neonatal Serotonergic Syndrome.
.
Newborn babies exposed to antidepressants in utero may manifest:
Insomnia or somnolence
Agitation , tremors, jitteriness, shivering and/ or altered tone
Restlessness, irritability &constant crying
Poor feeding, vomiting or diarrhoea
Poor temperature control, hypoglycaemia
Tachypnoea, respiratory distress, nasal congestion or cyanosis
Seizures
Reports of incidence suggest 30% of SSRI exposed full term
babies show poor neonatal adaptation – this compares with
approximately 10% of non exposed babies .
It is usually short lived with a median duration of 3 days, and
75 % complete resolution by 5 days. However there have been
reports of adaptation signs lasting up to 4 weeks.
Premature babies are more vulnerable to NAS, and are more
likely to develop signs, which may be more severe. One study
reported 100% of exposed babies born before 37 weeks
developed signs of NAS. Premature babies have been found to
require 4 times as long in NICU compared to an age controlled
non exposed group.
Symptoms can vary greatly in severity from mild transitory
symptoms to more severe symptoms including seizures and
dehydration.
Jul 2010
.
Use of antidepressants during pregnancy and the
risk of spontaneous abortion Hamid Reza Nakhai-Pour, MD PhD, Perrine Broy, BSc and Anick Bérard, PhD
Background: The risk of relapse of depression or the diagnosis of some other psychiatric disorders
during pregnancy necessitates the use of antidepressants despite possible adverse effects. Whether such
use increases the risk of spontaneous abortion is still being debated. We evaluated the risk of
spontaneous abortion in relation to the use of antidepressants during pregnancy.
Methods: Using a nested case–control study design, we obtained data from the
Quebec Pregnancy Registry for 5124 women who had a clinically detected
spontaneous abortion. For each case, we randomly selected 10 controls from the
remaining women in the registry who were matched by the case’s index date (date of
spontaneous abortion) and gestational age at the time of spontaneous abortion.
Use of antidepressants was defined by filled prescriptions and was compared with
nonuse. We also studied the classes, types and doses of antidepressants.
Results: A total of 284 (5.5%) of the women who had a spontaneous abortion
had at least one prescription for an antidepressant filled during the pregnancy, as
compared with 1401 (2.7%) of the matched controls (odds ratio [OR] 2.09, 95%
confidence interval [CI] 1.83–2.38).. When we looked at antidepressant use by
type versus no use, paroxetine use alone (OR 1.75, 95% CI 1.31–2.34) and
venlafaxine use alone (OR 2.11, 95% CI 1.34–3.30) were associated with an
increased risk of spontaneous abortion.
Interpretation: The use of antidepressants, especially paroxetine,
venlafaxine or the combined use of different classes of
antidepressants, during pregnancy was associated with an increased
risk of spontaneous abortion
• Fluoxetine promotes gliogenesis during neural differentiation
in mouse embryonic stem cells
Kusakawa S, Nakamura K, Miyamoto Y,
Sanbe A, Torii T, Yamauchi J, Tanoue A
Sept. 2010
Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed for treatment of mood
disorders and depression, even during pregnancy and lactation. SSRIs are thought to be much safer than
tricyclic antidepressants, with a low risk of embryonic toxicity. Several recent studies, however, have
reported that fetal exposure to SSRIs increases the risk of adverse effects during fetal and neonatal
development. This is consistent with our previous finding that fluoxetine, a prototypical SSRI,
profoundly affected the viability of cultured embryonic stem (ES) cells as well as their ability to
differentiate into cardiomyocytes. Furthermore, we found that fluoxetine induced fluctuations in
ectodermal marker gene expression during ES cell differentiation, which suggests that fluoxetine may
affect neural development. In the present study, we investigated the effects of fluoxetine on the process
of differentiation from ES cells into neural cells using the stromal cell-derived inducing activity (SDIA)
method. Fluoxetine treatment was found to enhance the expression of glial marker genes following
neural differentiation, as observed by immunocytochemical analysis or quantitative RT-PCR. The
promoter activity of glial marker genes was also significantly enhanced when cells were treated with
fluoxetine, as observed by luciferase reporter assay. The expression of neuronal markers during ES
cell differentiation into neural cells, on the other hand, was inhibited by fluoxetine treatment. In
addition, FACS analysis revealed an increased population of glial cells in the differentiating ES cells
treated with fluoxetine. These results suggest that fluoxetine could facilitate the differentiation of
mouse ES cells into glial cell lineage, which may affect fetal neural development

Citalopram Risks: Has been associated with a rare
but serious newborn lung problem (persistent
pulmonary hypertension of the newborn, or PPHN)
when taken during the last half of pregnancy; has been
associated with septal heart defects; has been
associated with a birth defect that affects the brain and
skull (anencephaly), a birth defect that affect sutures on
the head (craniosynostosis) and a birth defect that
affects the abdominal organs (omphalocele)
Recommendation: Consider as an option during
pregnancy
Fluoxetine Risks: Has been associated with PPHN
when taken during the last half of pregnancy
Recommendation: Consider as an option during
pregnancy
Paroxetine Risks: Has been associated with fetal
heart defects when takenduring the first three months
of pregnancy; has been associated with PPHN when
taken during the last half of pregnancy; has been
associated with anencephaly, craniosynostosis and
omphalocele
Recommendation: Avoid during pregnancy
Sertraline Risks: Has been associated with PPHN
when taken during the last half of pregnancy; has been
associated with septal heart defects; has been
associated with omphalocele
Recommendation: Consider as an option during
pregnancy
Amitriptyline Risks: Suggested risk of limb
malformation in early studies, but not confirmed by
newer studies
Recommendation: Consider as an option during
pregnancy
Nortriptilina Risks: Suggested risk of limb
malformation in early studies, but not confirmed by
newer studies
Recommendation: Consider as an option during
pregnancy
• Some studies associate the use of antidepressants
during pregnancy with preterm birth, but other studies
don't support this link.
• Use of more than one type of SSRI during the first
trimester of pregnancy has been associated with an
increased prevalence of septal heart defects.

Grazie per
l’attenzione