Corso teorico di Ecografia Generalista Villasimius 1-5 ...ecografia della spalla - anatomia...
76
Corso teorico di Ecografia Generalista Villasimius 1-5-ottobre 2012 Ecografia della spalla:quadri normali e metodologia di studio Piero Zaninetti Scuola di Ecografia Generalista SIEMG5 FIMMG martedì 16 ottobre 12
Transcript of Corso teorico di Ecografia Generalista Villasimius 1-5 ...ecografia della spalla - anatomia...
Corso teorico di Ecografia GeneralistaVillasimius 1-5-ottobre 2012
Ecografia della spalla:quadri normali e metodologia di studio
Piero&Zaninetti&Scuola'di'Ecografia'Generalista
SIEMG5'FIMMG
martedì 16 ottobre 12

Regioni della spalla!
• Anteriore!
• Superiore!
• Antero-laterale!
• Posteriore!
martedì 16 ottobre 12

Regione anteriore!
Collo anatomico
Piccola tuberosità
Grande tuberosità
Processo coracoideo
martedì 16 ottobre 12

Regione anteriore!
martedì 16 ottobre 12
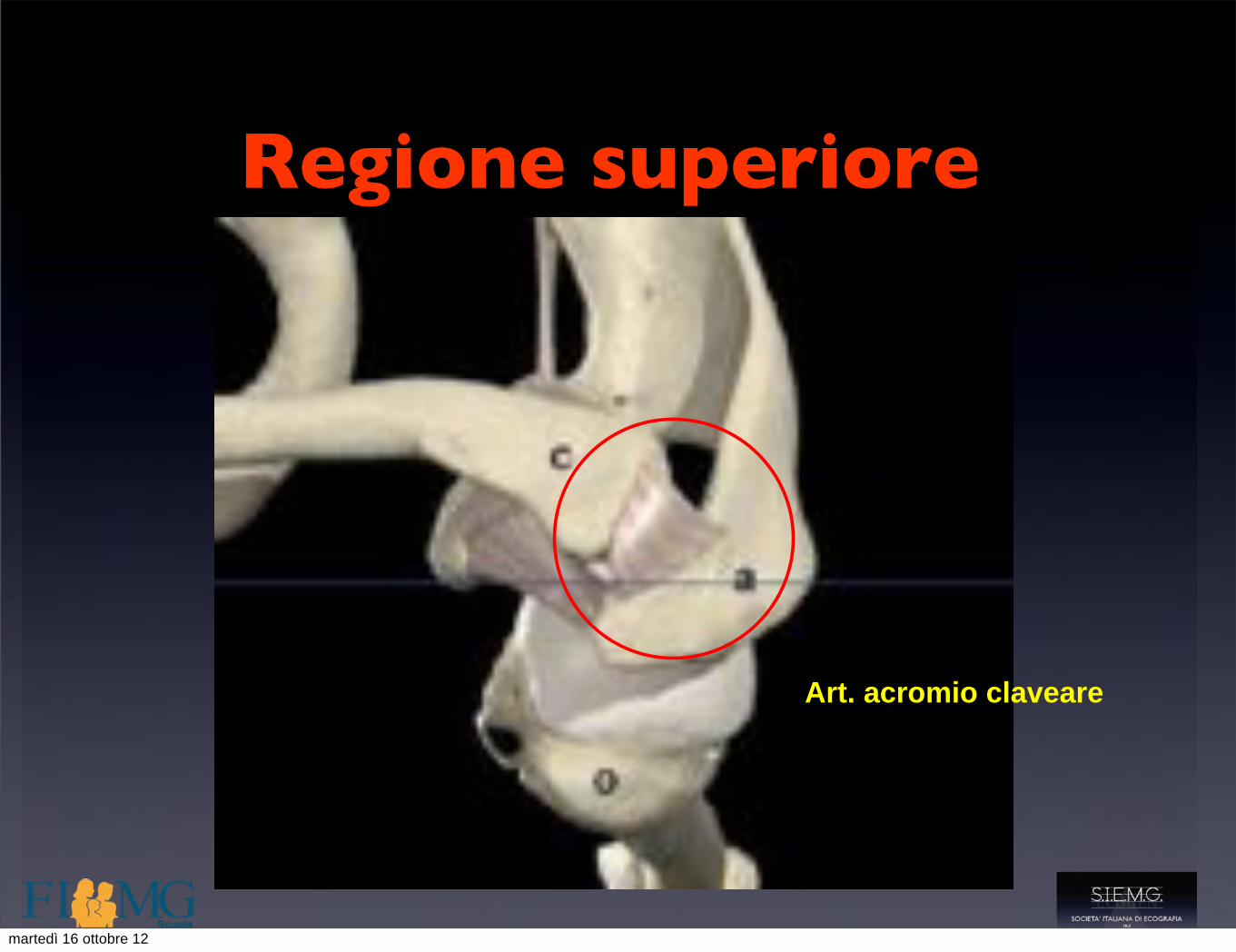
Regione superiore!
Art. acromio claveare
martedì 16 ottobre 12

Regione posteriore!Regione posteriore!
martedì 16 ottobre 12

Regione posteriore!Regione posteriore!
martedì 16 ottobre 12

Regione posteriore!Regione posteriore!
martedì 16 ottobre 12

Regione antero laterale!Regione antero laterale!
martedì 16 ottobre 12
martedì 16 ottobre 12

Muscolo deltoide!Muscolo deltoide!
martedì 16 ottobre 12

Regione antero laterale!
• L!
La borsa sottoacromio-deltoidea
Regione antero laterale!
• L!
La borsa sottoacromio-deltoidea
martedì 16 ottobre 12

martedì 16 ottobre 12

I legamenti!
martedì 16 ottobre 12
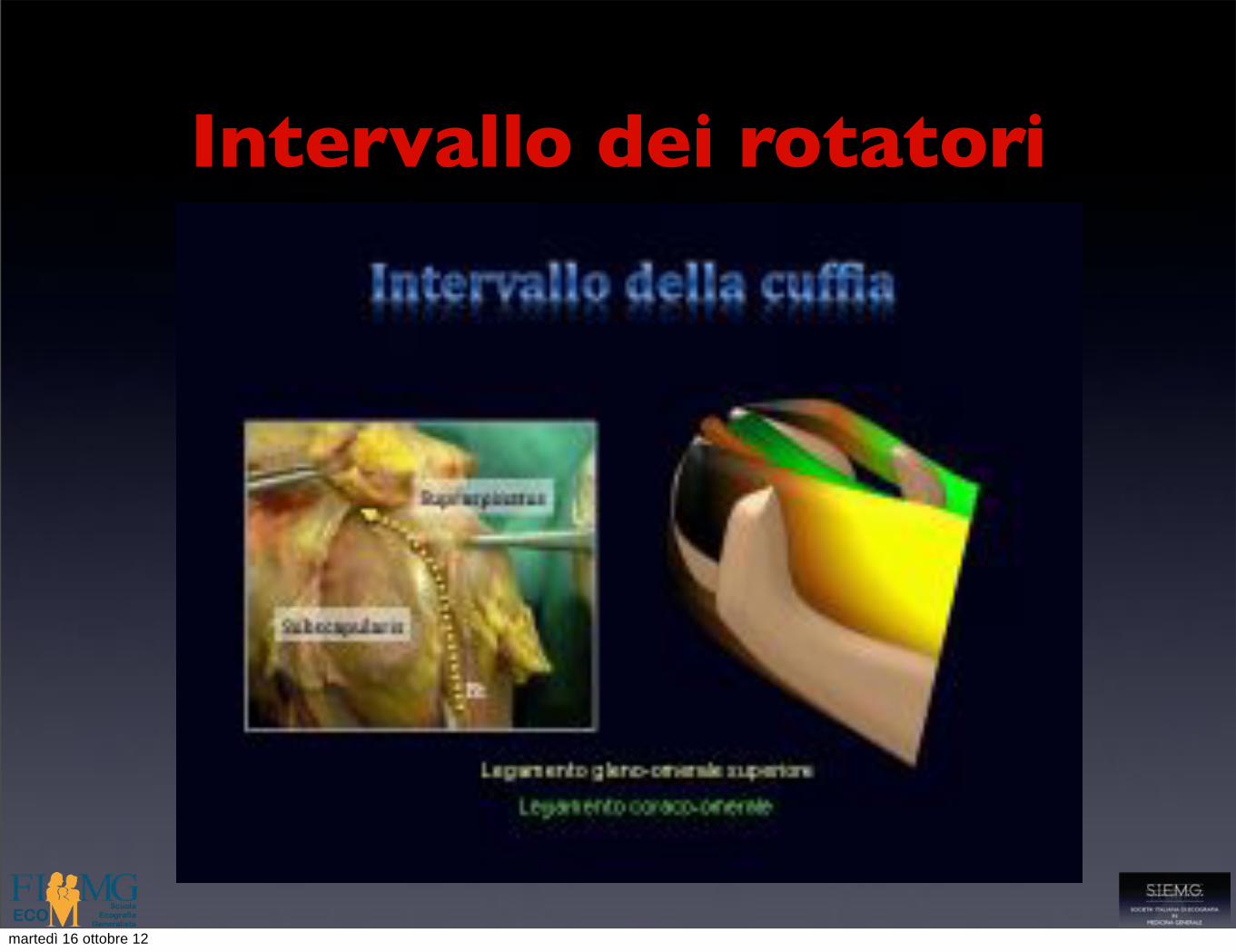
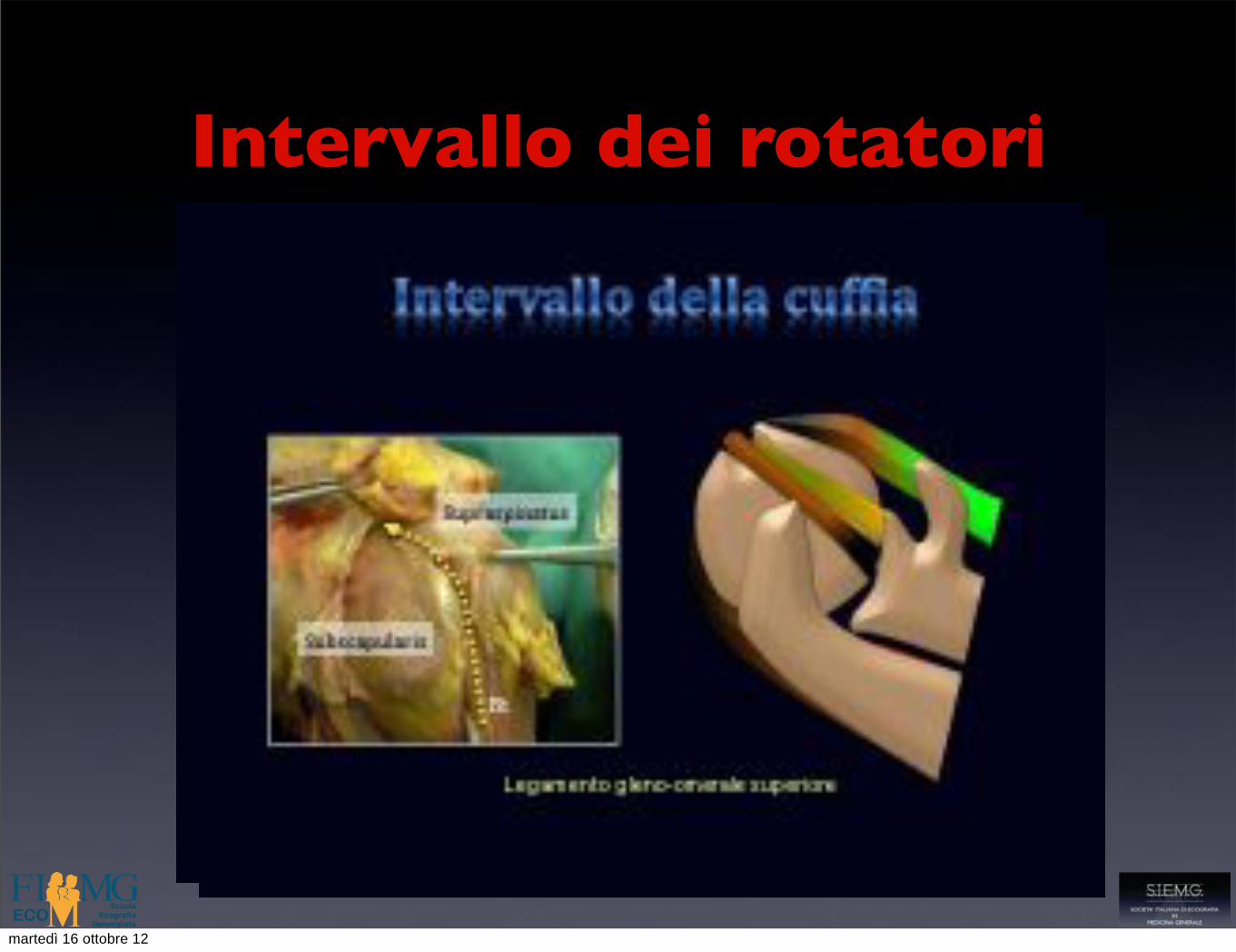
Intervallo dei rotatori
martedì 16 ottobre 12
Intervallo dei rotatori
martedì 16 ottobre 12

Intervallo dei rotatori
martedì 16 ottobre 12

Intervallo dei rotatori228 S. Bianchi and C. Martinoli
SubSSupraS *GTLT SubS
SGHL
CHL
SupraS *
GT
LT SubS
**GT
LT
SubS
SupraS
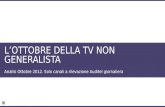
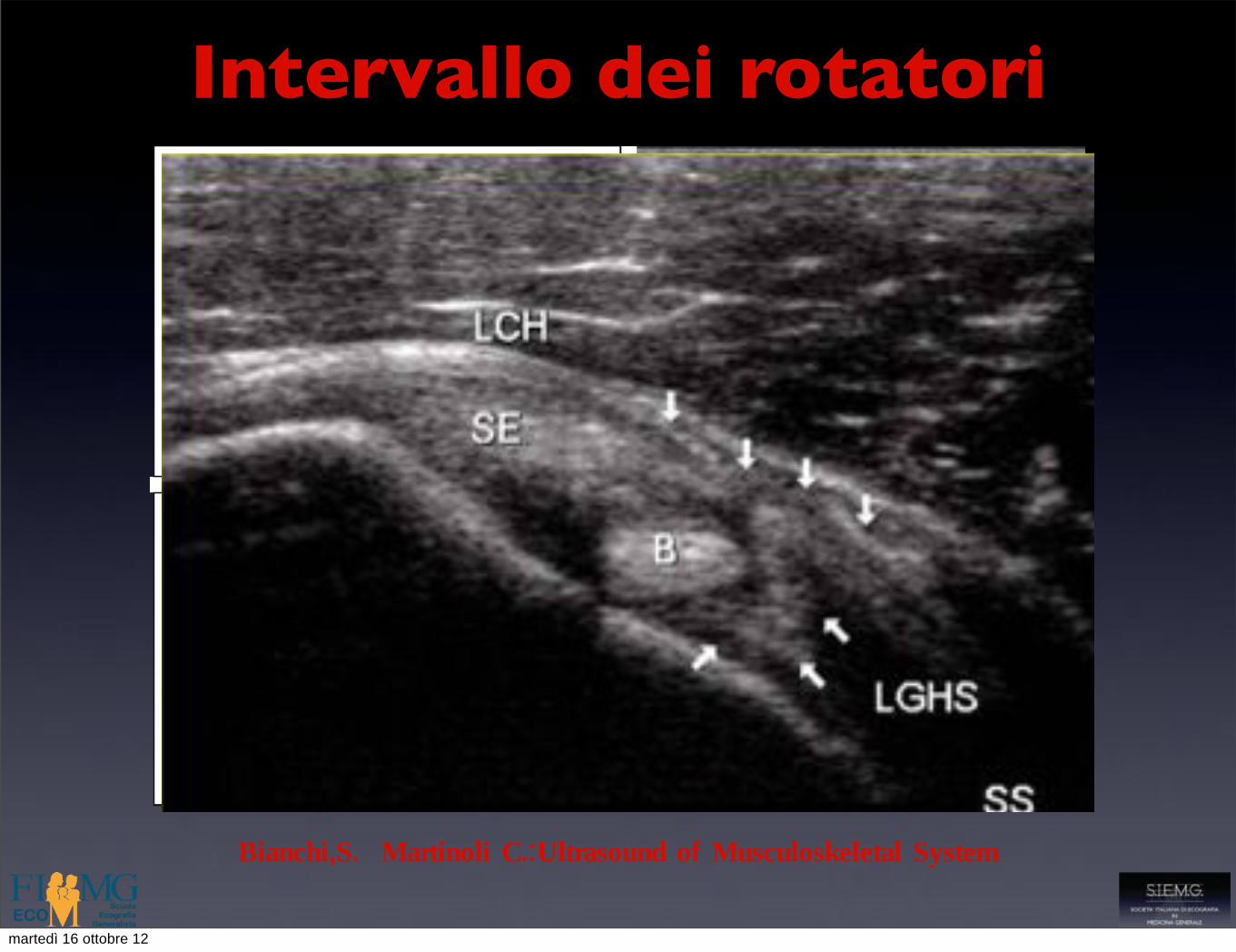
Fig. 6.44a–d. Rotator cuff interval: intermediate and distal levels. a Schematic drawing with b corresponding transverse 12–5 MHz US image of the intermediate level of the rotator cuff interval. The medial cord of the coracohumeral ligament (CHL) and the superior glenohumeral ligament (SGHL) form an anterior sling (arrowheads) around the biceps tendon (asterisk), the so-called refl ection pulley. In the US image, note that the biceps is elevated at this site relative to the bone and assumes an oblique orienta-tion due to the pulley which surrounds it with a crescentic shape. The deep fi bers of the pulley that infi ltrates the undersurface of the biceps tendon are part of the superior glenohumeral ligament. SubS, subscapularis; SupraS, supraspinatus. c Schematic drawing with d corresponding transverse 12–5 MHz US image of the distal level of the rotator cuff interval. In the proximity of the bicipital groove, the biceps tendon (asterisk) lies in contact with the lesser tuberosity (LT) and the subscapularis tendon (SubS) and is stabilized by fi brous bands arising from it. Arrowheads indicate the insertion of the supraspinatus tendon into the greater tuberosity (GT)
a
c
b
d
of movement of the arm. The large axillary recess arises, for instance, from a deep folding of the cap-sule that permits a complete elevation of the arm without stretching the inferior capsule. The same is true for the anterior and posterior recesses, which allow maximal external and internal rotation of the arm. In normal states, the small amount of synovial fluid contained in the joint space cannot be rec-ognized with US. On the other hand, US has high sensitivity for appreciating even a minimal amount of pathologic fluid inside the main synovial recesses (i.e., the dependent axillary pouch, the posterior and anterior recesses and the sheath of the long head of the biceps tendon).
Although a caudal approach through the axilla has been described to evaluate the axillary pouch, poste-rior transverse scans are usually preferred for better accessibility. Once the teres minor tendon is localized, the transducer is shifted more caudally to investigate the space intervening between the humeral metaph-ysis and the inferior neck of the scapula, where the
axillary pouch lies. If distended by considerable effu-sion, this pouch is visible as a fluid-filled area.
The posterior recess is best examined on trans-verse scans by placing the transducer over the infra-spinatus tendon (Fig. 6.45). An effusion filling the posterior recess appears as a hypoanechoic crescent surrounding the tip of the posterior labrum. In larger effusions, the infraspinatus tendon can be seen dis-placed posteriorly by the fluid contained in the recess. In doubtful cases, the examiner can induce changes in the shape of the recess by passively moving the patient’s arm externally and internally, which results in reduced/increased tension of the posterior capsule and the overlying infraspinatus. Due to the lack of intervening vessels and easy accessibility, procedures of needle aspiration or injection in the posterior recess can be safely performed under US guidance while the patient is seated or prone (Fessell et al. 2000; Zwar et al. 2004). This recess can be selected for a safe US-guided needle placement for shoulder arthrography (Cicak et al. 1992; Valls and Melloni 1997).
*
*
Bianchi,S. Martinoli C.:Ultrasound of Musculoskeletal System
martedì 16 ottobre 12
Intervallo dei rotatori228 S. Bianchi and C. Martinoli
SubSSupraS *GTLT SubS
SGHL
CHL
SupraS *
GT
LT SubS
**GT
LT
SubS
SupraS
Fig. 6.44a–d. Rotator cuff interval: intermediate and distal levels. a Schematic drawing with b corresponding transverse 12–5 MHz US image of the intermediate level of the rotator cuff interval. The medial cord of the coracohumeral ligament (CHL) and the superior glenohumeral ligament (SGHL) form an anterior sling (arrowheads) around the biceps tendon (asterisk), the so-called refl ection pulley. In the US image, note that the biceps is elevated at this site relative to the bone and assumes an oblique orienta-tion due to the pulley which surrounds it with a crescentic shape. The deep fi bers of the pulley that infi ltrates the undersurface of the biceps tendon are part of the superior glenohumeral ligament. SubS, subscapularis; SupraS, supraspinatus. c Schematic drawing with d corresponding transverse 12–5 MHz US image of the distal level of the rotator cuff interval. In the proximity of the bicipital groove, the biceps tendon (asterisk) lies in contact with the lesser tuberosity (LT) and the subscapularis tendon (SubS) and is stabilized by fi brous bands arising from it. Arrowheads indicate the insertion of the supraspinatus tendon into the greater tuberosity (GT)
a
c
b
d
of movement of the arm. The large axillary recess arises, for instance, from a deep folding of the cap-sule that permits a complete elevation of the arm without stretching the inferior capsule. The same is true for the anterior and posterior recesses, which allow maximal external and internal rotation of the arm. In normal states, the small amount of synovial fluid contained in the joint space cannot be rec-ognized with US. On the other hand, US has high sensitivity for appreciating even a minimal amount of pathologic fluid inside the main synovial recesses (i.e., the dependent axillary pouch, the posterior and anterior recesses and the sheath of the long head of the biceps tendon).
Although a caudal approach through the axilla has been described to evaluate the axillary pouch, poste-rior transverse scans are usually preferred for better accessibility. Once the teres minor tendon is localized, the transducer is shifted more caudally to investigate the space intervening between the humeral metaph-ysis and the inferior neck of the scapula, where the
axillary pouch lies. If distended by considerable effu-sion, this pouch is visible as a fluid-filled area.
The posterior recess is best examined on trans-verse scans by placing the transducer over the infra-spinatus tendon (Fig. 6.45). An effusion filling the posterior recess appears as a hypoanechoic crescent surrounding the tip of the posterior labrum. In larger effusions, the infraspinatus tendon can be seen dis-placed posteriorly by the fluid contained in the recess. In doubtful cases, the examiner can induce changes in the shape of the recess by passively moving the patient’s arm externally and internally, which results in reduced/increased tension of the posterior capsule and the overlying infraspinatus. Due to the lack of intervening vessels and easy accessibility, procedures of needle aspiration or injection in the posterior recess can be safely performed under US guidance while the patient is seated or prone (Fessell et al. 2000; Zwar et al. 2004). This recess can be selected for a safe US-guided needle placement for shoulder arthrography (Cicak et al. 1992; Valls and Melloni 1997).
*
*
Bianchi,S. Martinoli C.:Ultrasound of Musculoskeletal System
cartilage; this section must be comparative. Renoux [4]established that tendon thickness of >2.5 mm at thislevel should be considered pathological (Fig. 2).
This is an extremely important sign because bicepstendinopathy of this type is difficult to demonstrate withother techniques. Aside from the pain it produces, it canalso cause problems of entrapment. As demonstrated byBoileau [5], the thickened tendon is unable to slide into thebicipital groove when the arm is abducted.
The rotator interval
The long head then passes into the space that separates thesupraspinatus (posterolaterally) and subscapularis (ante-romedially) tendons; this canal is covered by the cor-acohumeral ligament, which merges with the superiorglenohumeral ligament to form a retention band thatprevents medial luxation of the tendon (Fig. 3).
Tendinopathies involving the long head can be observedat this level, especially when the anterior part of thesupraspinatus tendon is torn, which leads to retraction ofthe coracohumeral ligament. The tendon comes into directconflict with the inferior aspect of the acromion, and thisresults in microtrauma, which is the cause of the tendin-opathy [6]. The tendon appears thickened, hypoechoic,with relatively poorly defined margins (Fig. 4). Almostinvariably, this condition is associated with substantial painand inflammation, which make it difficult for the patient tosleep. It can lead to rupture of the tendon, which dimin-ishes the pain. However, it can also cause cranialdisplacement of the head with scapulohumeral dysmobility.
Disinsertion or rupture of the coracohumeral ligamentcan also lead to luxation of the long head of the biceps onthe anterior side of the subscapularis tendon (Fig. 5).
Traumatic ligament lesions and calcifications can alsoproduce pain in the area of the rotator interval, and it is
important to recall that thickening of the coracohumeralligament is a valuable indirect sign of capsulitis, asdemonstrated by Homsi [7].
Reflection to the upper part of the groove
At this level, the examination should focus mainly onexcluding subluxation of the tendon. This phenomenon isfacilitated by the angulation of the tendon, which leads toits medial displacement. As we have seen, the ligamentband of the rotator interval provides support at this level.Stabilizing effects at the upper part of the groove areprovided by the intact subscapularis muscle, which insertson the medial aspect [of the groove], and its superficial
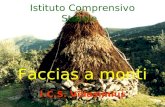
Figure 2 Comparative axial scan of the tendon of the long head of the biceps brachii at the level of the upper pole of the head ofthe humerus. The right tendon displays thickening (>2.5 mm), a finding indicative of tendinopathy.
Figure 3 Ligament band that keeps the tendon of the longhead within the interval; the superficial layer of the band isformed by the coracohumeral ligament and the deep layer ofthe superior glenohumeral ligament.
The biceps tendons 31
martedì 16 ottobre 12
Ricordare sempre !
martedì 16 ottobre 12

martedì 16 ottobre 12
martedì 16 ottobre 12
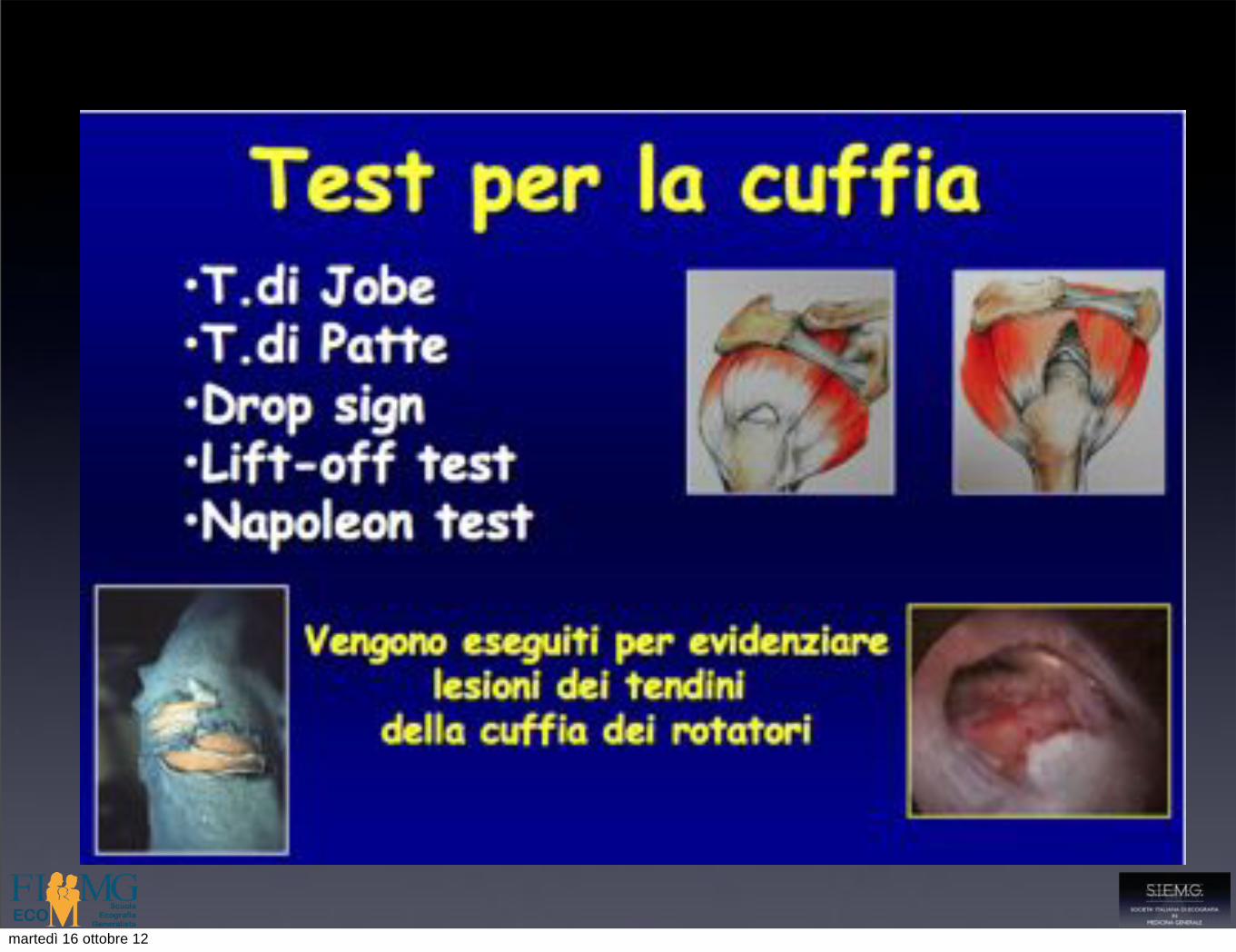
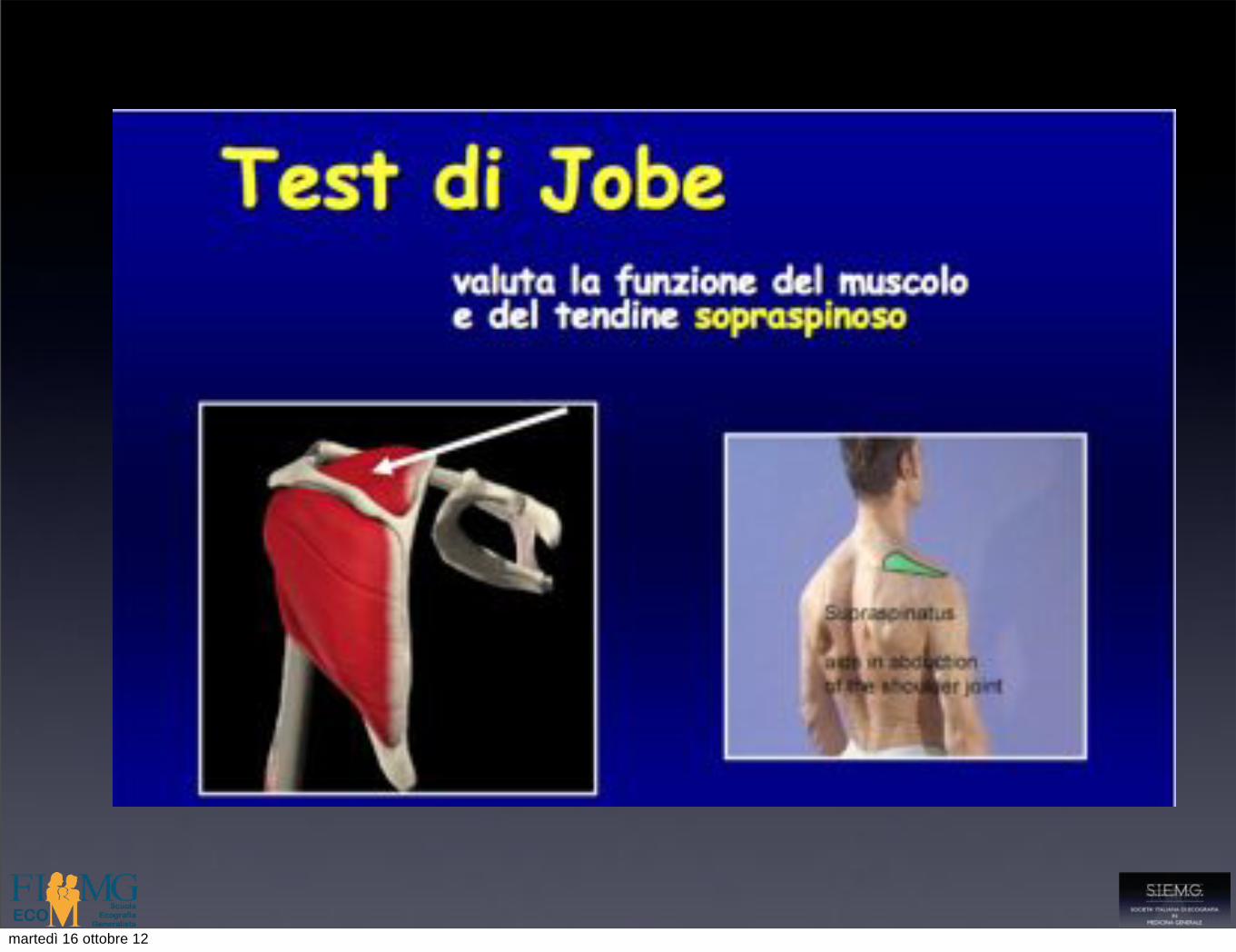
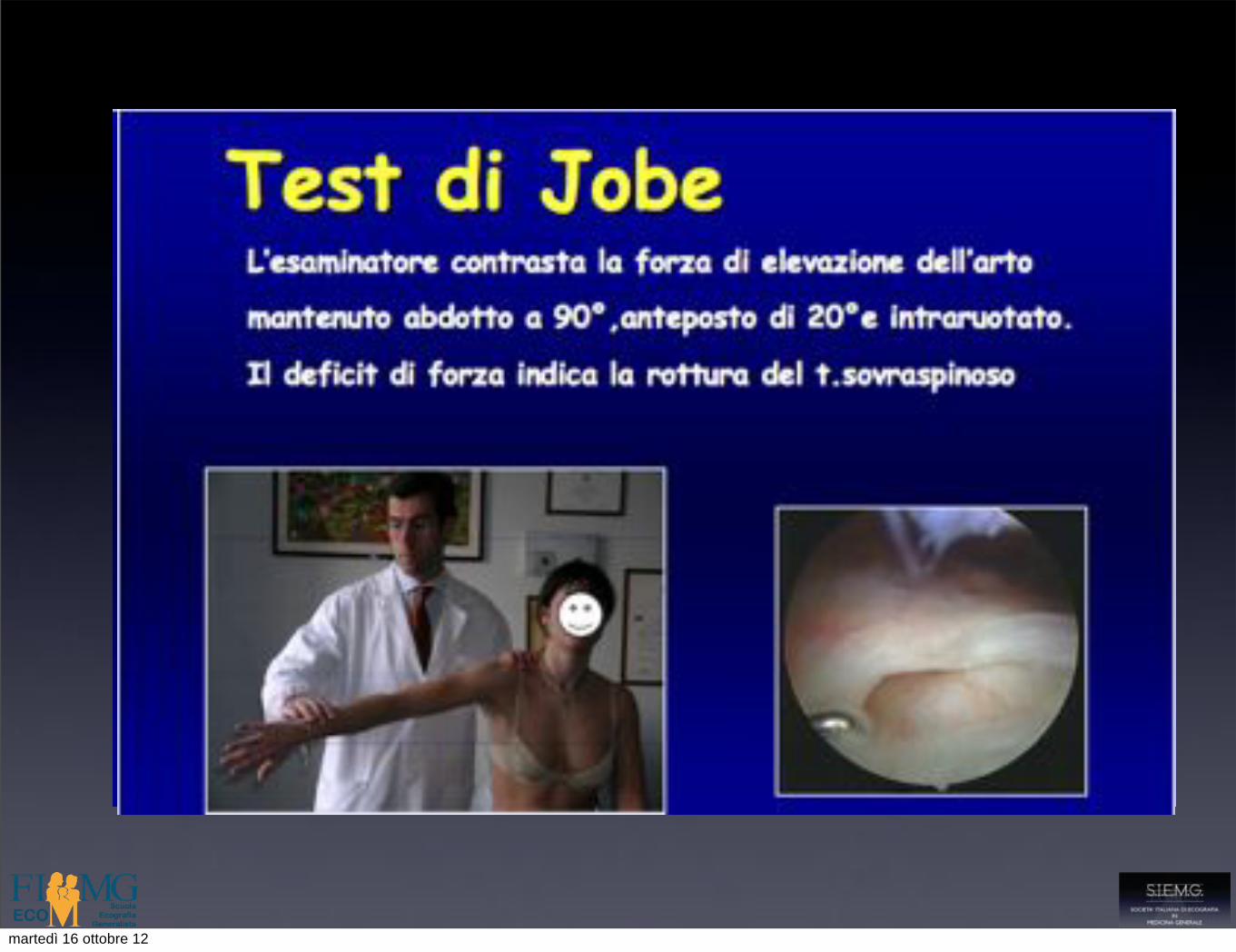
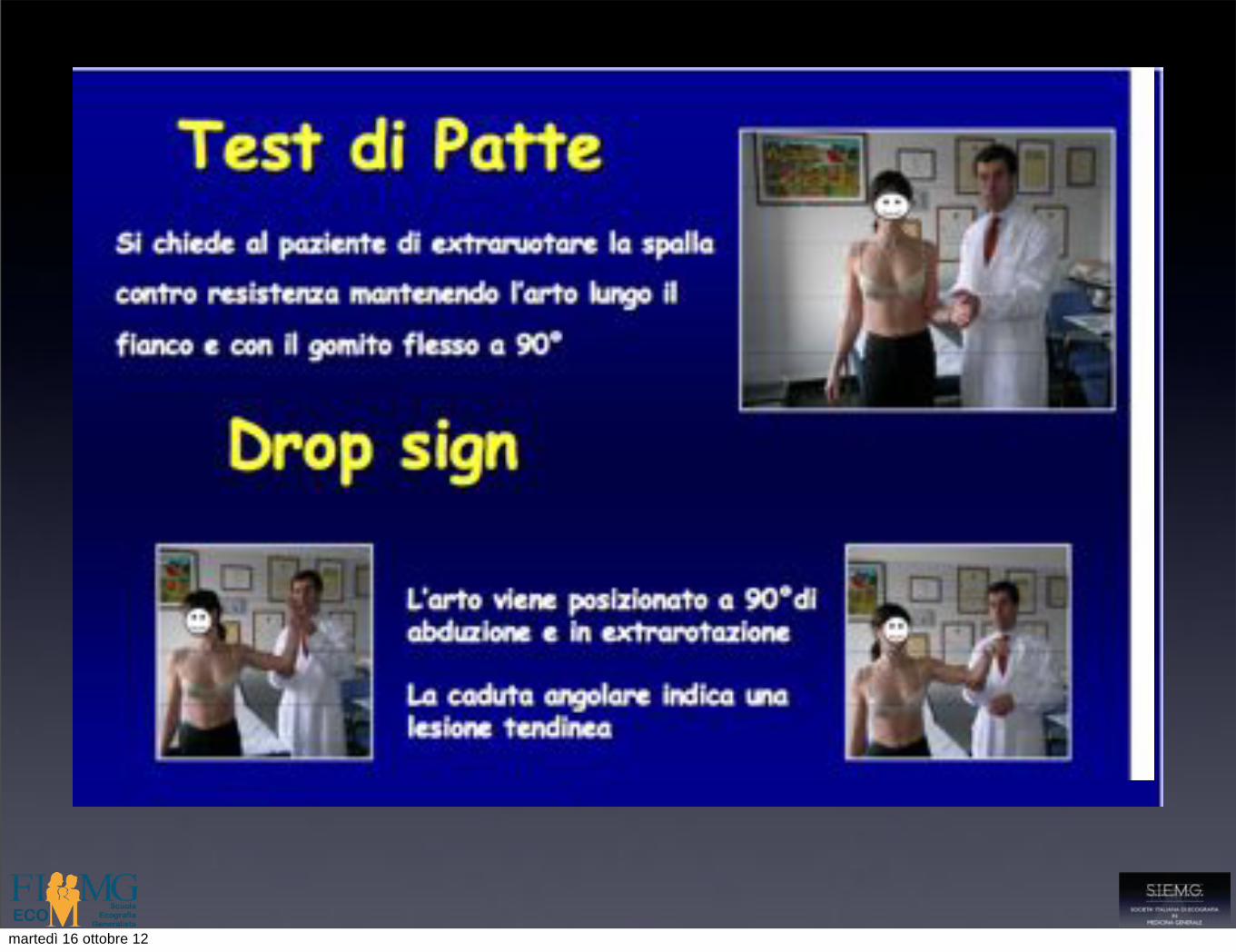
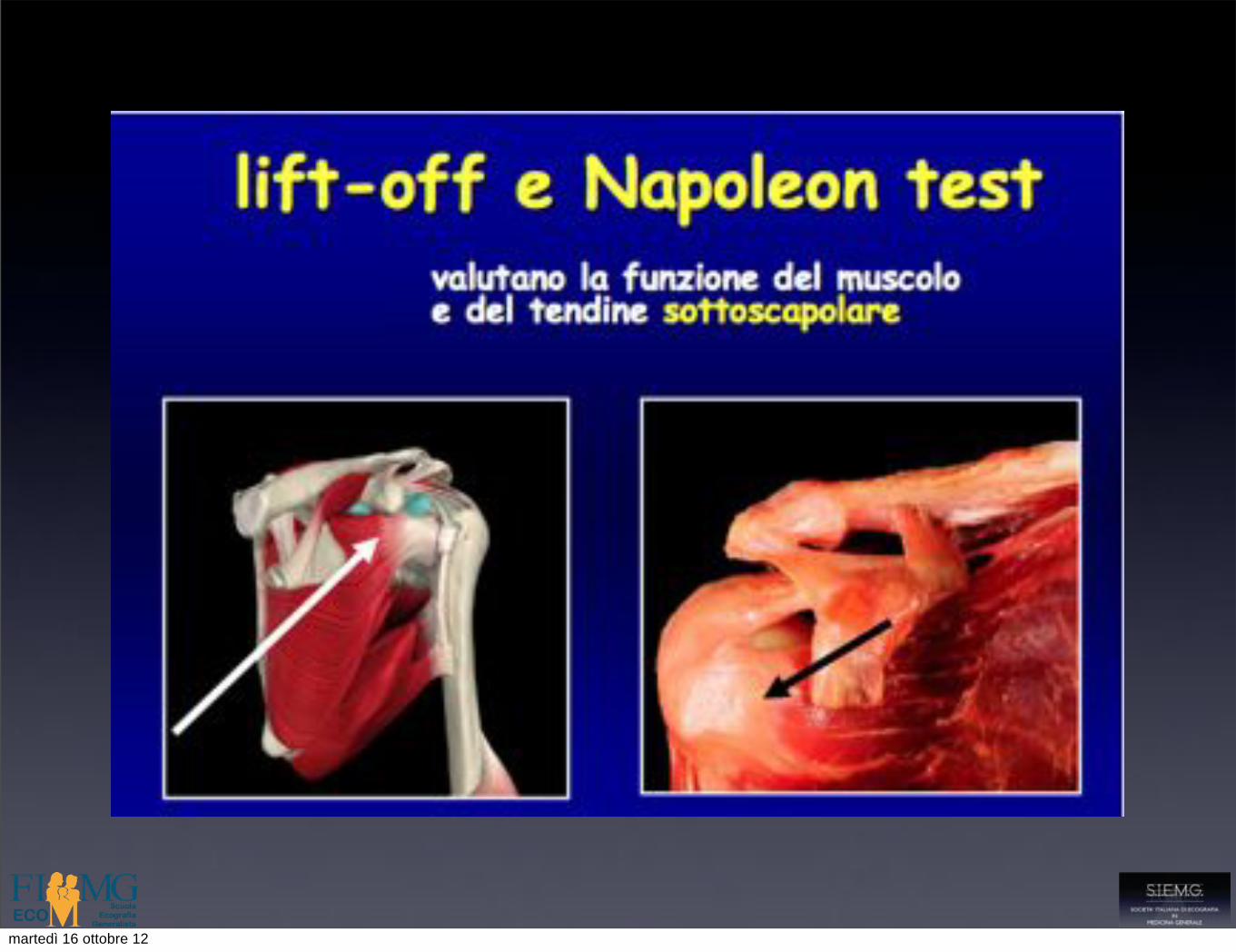
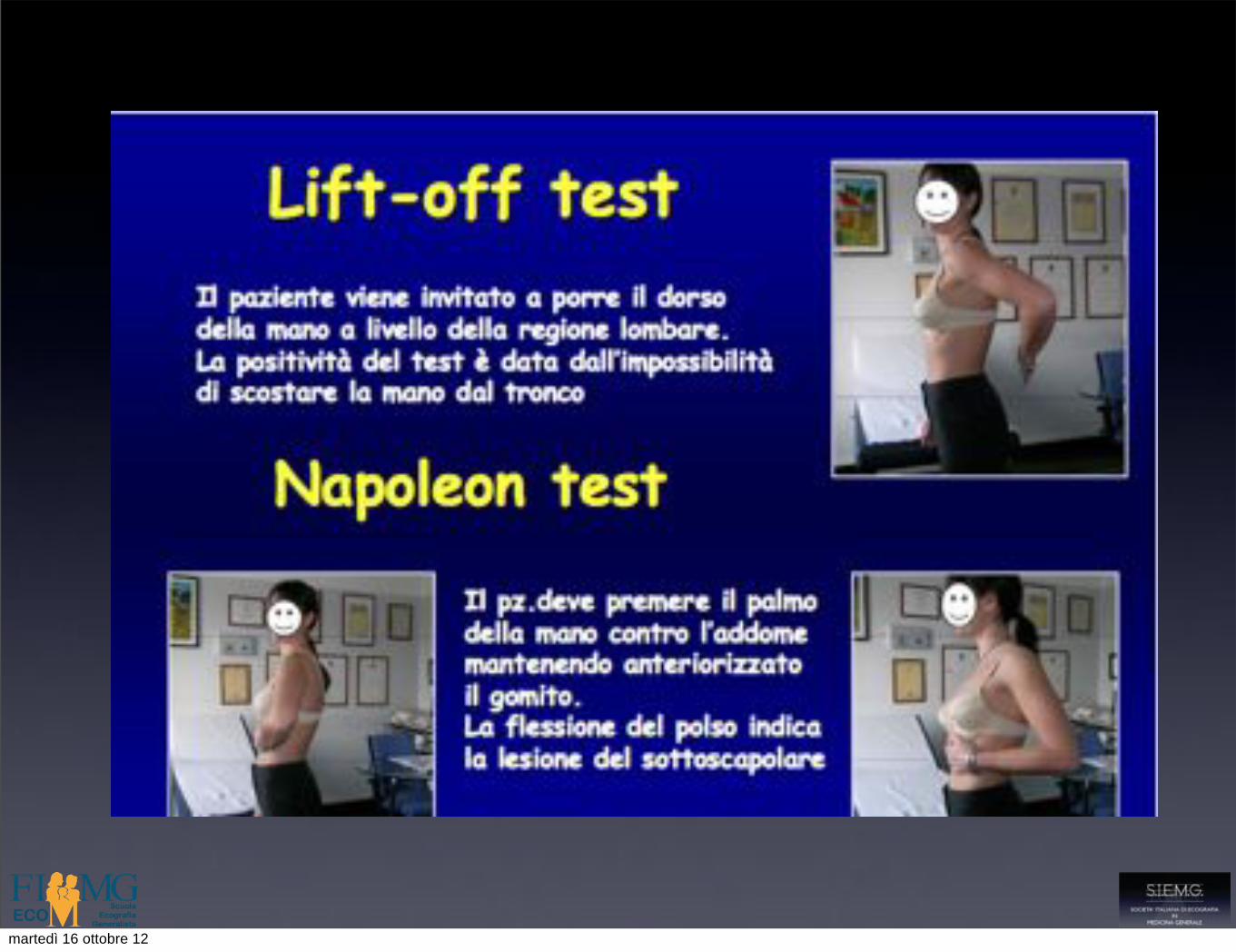
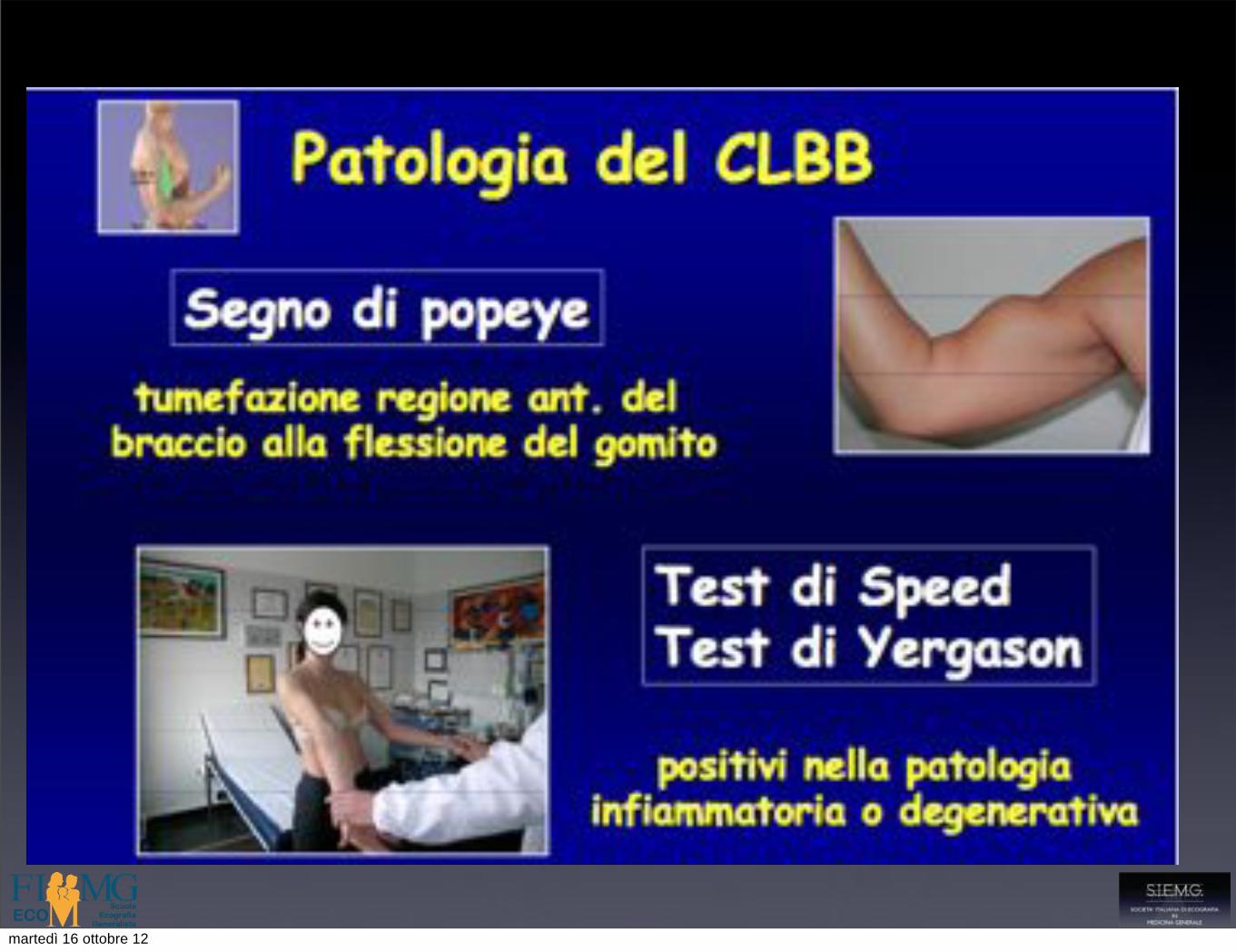
• Test di valutazione per
• Conflitto sub acromiale
• Patologia della cuffia dei rotatori
• Patologia del tendine del CLB
• Instabilità
Esame clinico della spalla
martedì 16 ottobre 12

martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12

martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12
martedì 16 ottobre 12

Esecuzione dell’esame !
martedì 16 ottobre 12

Esecuzione dell’esame
• Paziente seduto a gambe parallele,sulla destra e di fronte all’operatore
• L’esame è da effettuarsi sempre in comparativa
• La posizione del braccio del paziente varia in relazione alla struttura da esaminare
• Si utilizzano sonde lineari con frequenza 7,5 MHz o superiore in relazione alla tipologia del paziente e alla struttura anatomica da esaminare
martedì 16 ottobre 12
Esecuzione dell’esame: valutare ogni tendine
• in maniera sistematica
• nella corretta posizione ( massimo stiramento del tendine)
• nei due piani ortogonali ( longitudinale e assiale)
• dalla giunzione miotendinea alla inserzione ossea
martedì 16 ottobre 12

Non tutte le spalle sono uguali
martedì 16 ottobre 12
Tendine del CLB
• Scansioni longitudinali e trasversali
• Studio del tendine in sede intra ed extraarticolare
• Studio del legamento trasverso e della puleggia di riflessione
• Valutazione della guaina sinoviale
• Valutazione della giunzione miotendinea all’intersezione con il tendine del m. grande pettorale
martedì 16 ottobre 12

Tendine del CLB
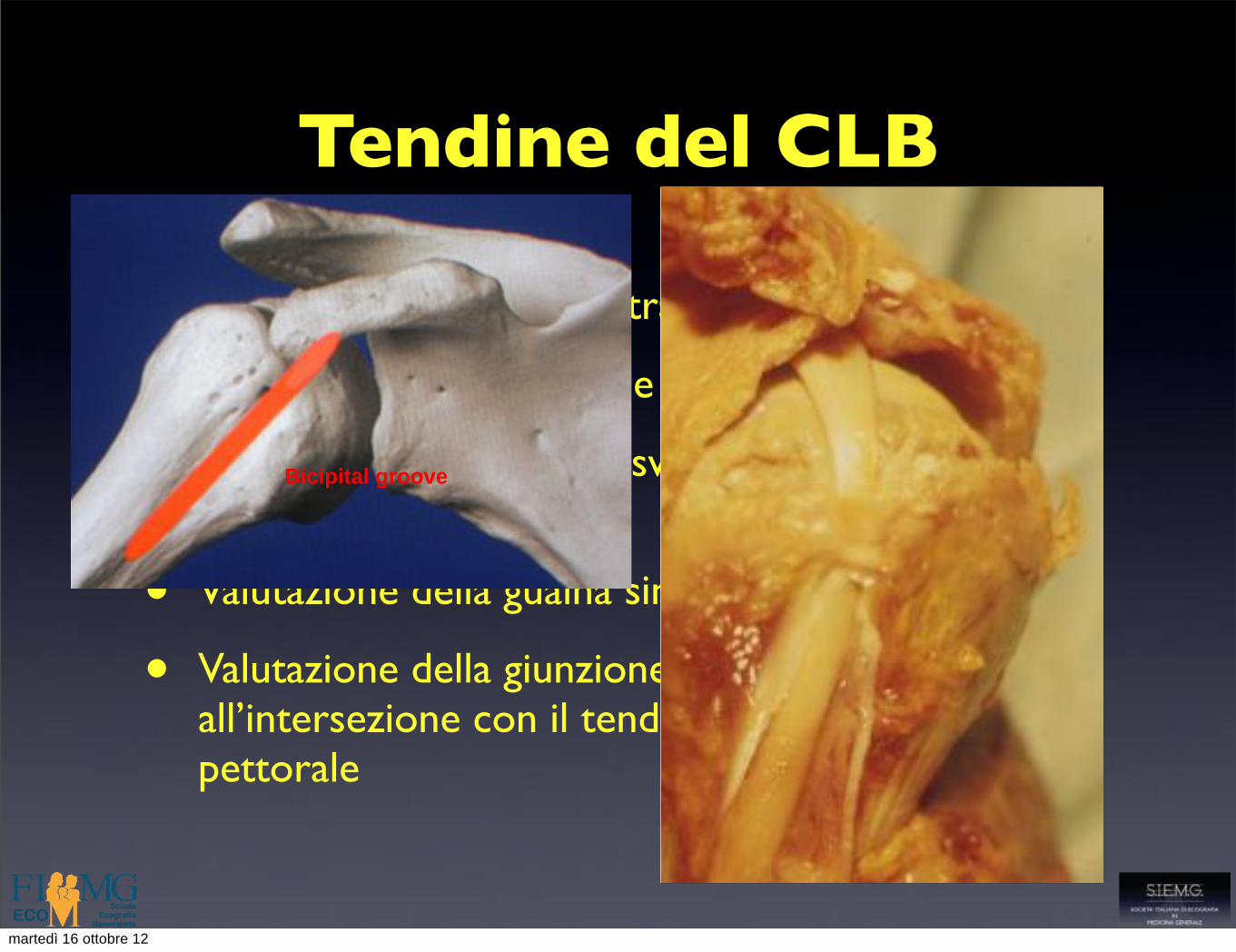
• Scansioni longitudinali e trasversali
• Studio del tendine in sede intra ed extraarticolare
• Studio del legamento trasverso e della puleggia di riflessione
• Valutazione della guaina sinoviale
• Valutazione della giunzione miotendinea all’intersezione con il tendine del m. grande pettorale
Bicipital groove
martedì 16 ottobre 12
Tendine del CLB
• Scansioni longitudinali e trasversali
• Studio del tendine in sede intra ed extraarticolare
• Studio del legamento trasverso e della puleggia di riflessione
• Valutazione della guaina sinoviale
• Valutazione della giunzione miotendinea all’intersezione con il tendine del m. grande pettorale
Bicipital groove
Sagittal antérieur5: Chef long du biceps
Sagittal antérieur5: Chef long du biceps
¾ANTERIEUR sagittal
¾SUPERIEUR
¾POSTERIEUR
martedì 16 ottobre 12

Tendine del CLB!
martedì 16 ottobre 12

Tendine del CLB!
martedì 16 ottobre 12

Tendine del CLB
martedì 16 ottobre 12
Tendine del sottoscapolare
• Studio della inserzione sulla piccola tuberosità omerale
• Valutazione della giunzione miotendinea ( muscolo multipennato con interdigitazione di fasci muscolari e tendinei)
• Esame dinamico con movimenti di intra ed extrarotazione ( scorrimento del tendine dietro il processo coracoideo della scapola)
martedì 16 ottobre 12

Tendine del sottoscapolare!
martedì 16 ottobre 12

Tendine del sottoscapolare!
Les conflits de la coiffeLes conflits de la coiffe
¾ CONFLIT ANTERO-SUPERIEUR
¾CONFLIT ANTERIEUR
¾ CONFLIT POSTERO-POSTERIEUR
C Courthaliac
martedì 16 ottobre 12

Tendine del sottoscapolare!
coracoide
Testa omerale trochine
martedì 16 ottobre 12

Tendine del sottoscapolare!
muscolo tendine
martedì 16 ottobre 12

Tendine del sottoscapolare
martedì 16 ottobre 12
Strutture antero-mediali!
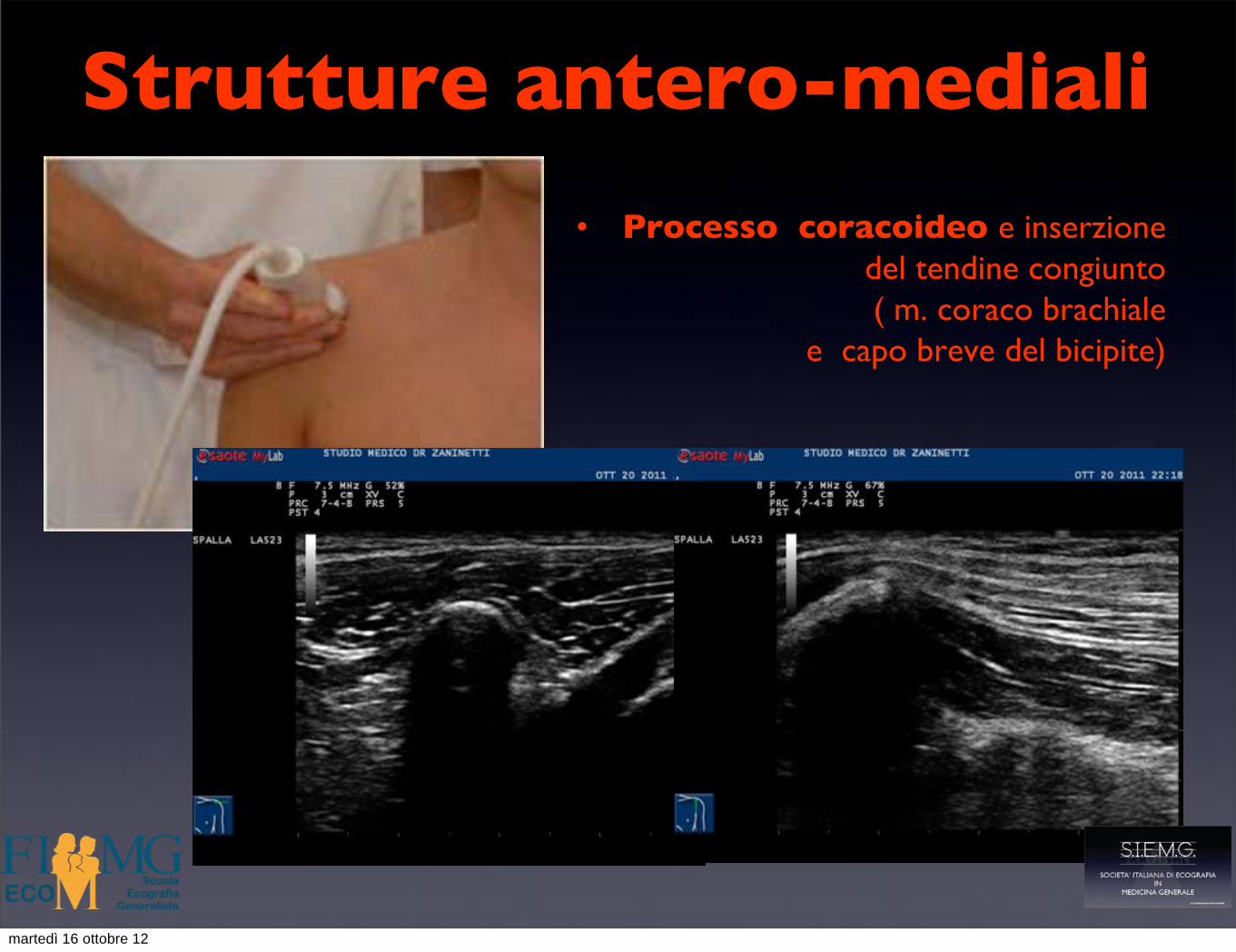
• Processo coracoideo e inserzione !del tendine congiunto !( m. coraco brachiale !
e capo breve del bicipite)!!!!
martedì 16 ottobre 12

Legamento coraco acromiale!
coracoide acromion
martedì 16 ottobre 12
Tendine del sopraspinato
• Studio della inserzione sulla grande tuberosità omerale
• Valutazione della struttura tendinea
• valutazione dello scorrimento nello spazio sub acromiale,sotto l’arcata formata dall’acromion e dal legamento coraco acromiale )
martedì 16 ottobre 12

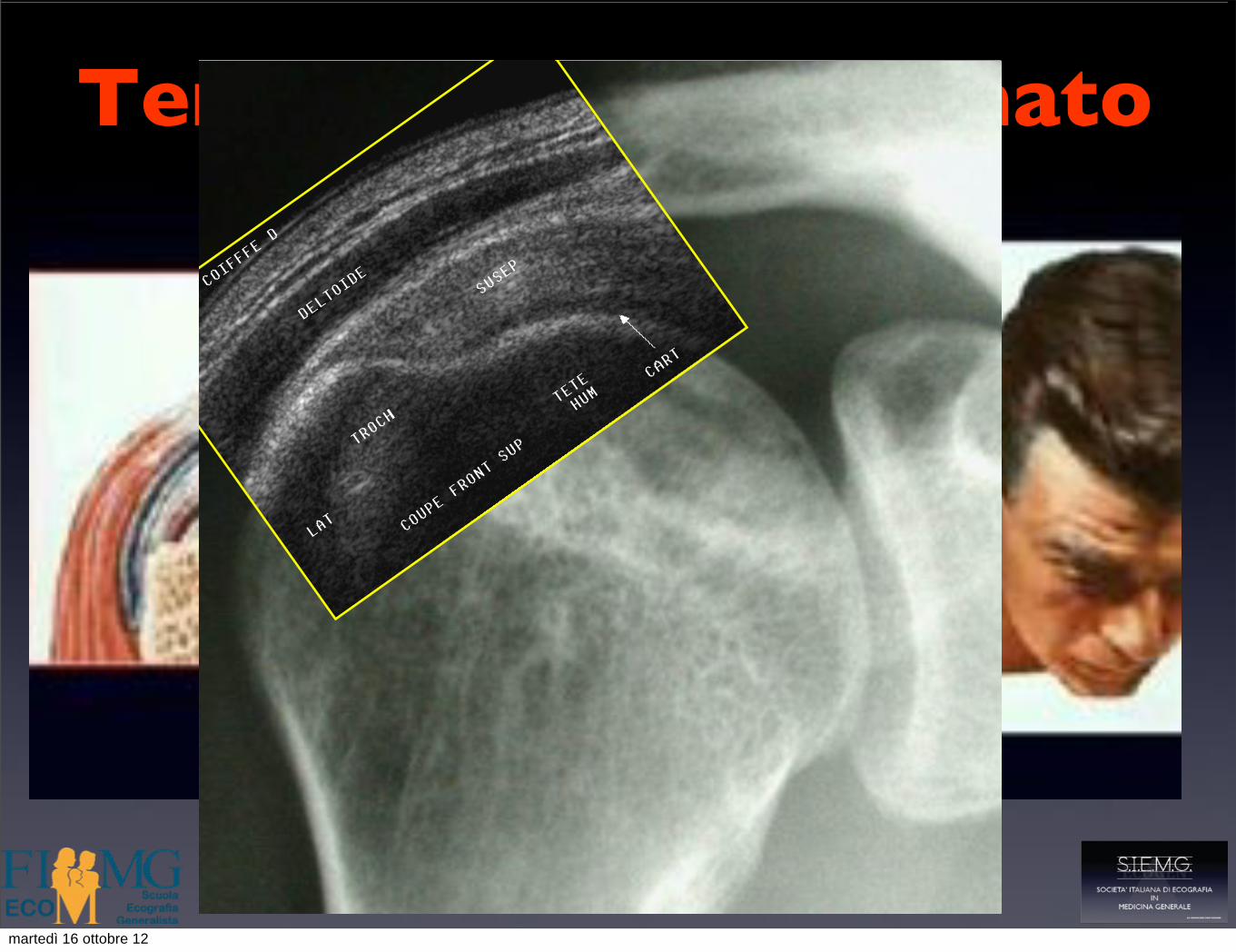
Tendine del sopraspinato!
martedì 16 ottobre 12

Tendine del sopraspinato!
martedì 16 ottobre 12
Tendine del sopraspinato!
Couple RX - EchographieCouple RX - Echographie
¾Peu onéreux¾Atraumatique
¾Complémentaire +++
?
martedì 16 ottobre 12
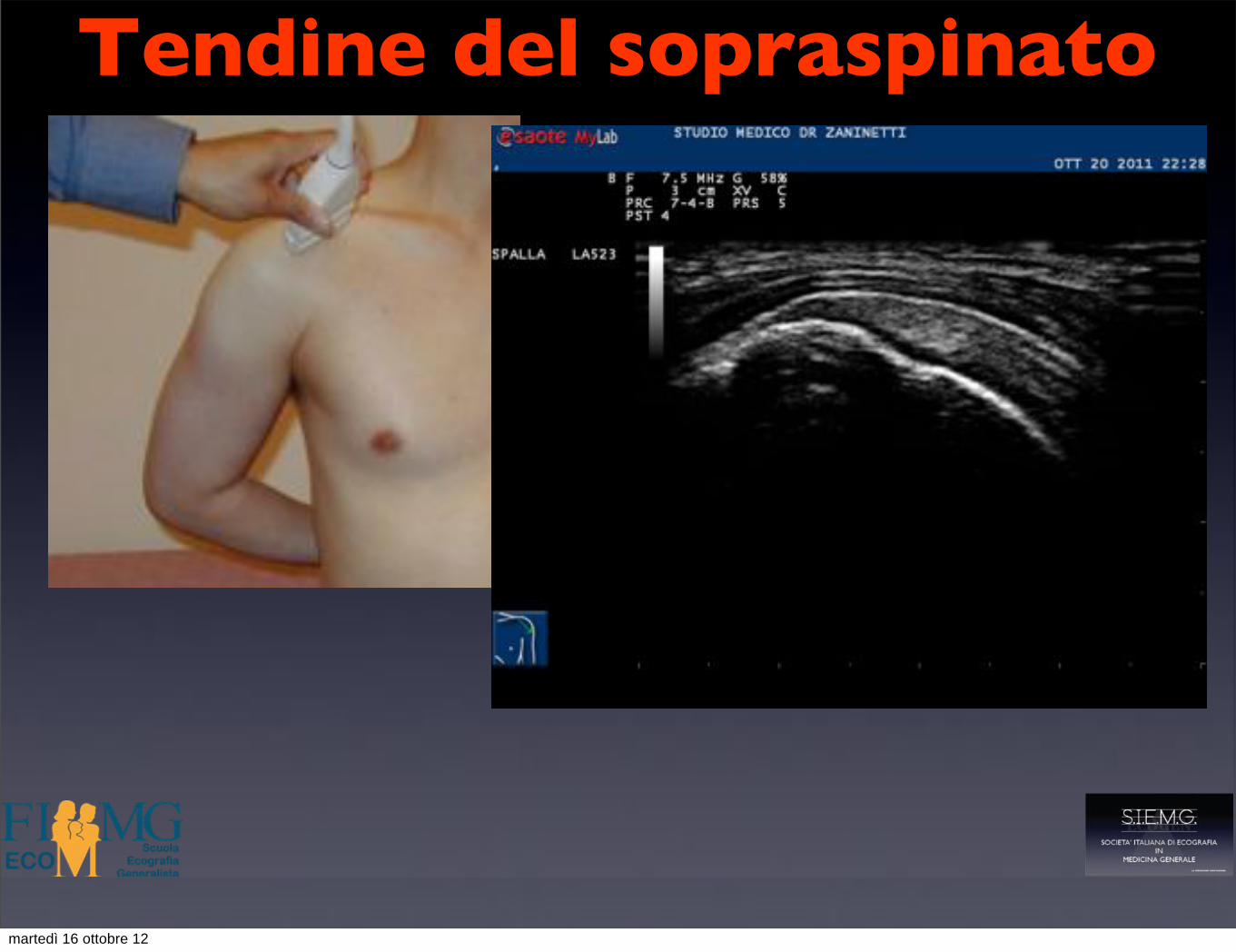
Tendine del sopraspinato!
martedì 16 ottobre 12

Tendine del sopraspinato!
the last few years. Armfield et al. (2003) publisheda detailed review about shoulder biomechanics and howimaging can detail shoulder function and dysfunction,including some brief notes about rotator cable. Kasket al. (2008) and Sheah et al. (2009) described themagnetic resonance (MR) arthrography appearance ofsuch structure either in cadavers (Kask et al. 2008) or in
injured shoulders (Sheah et al. 2009) while its ultrasound(US) appearance was described by Morag et al. in 2009.
US plays a central role in rotator cuff imaging(El-Dalati et al. 2009; Rutten et al. 2009; Teefey et al.2009; Vlychou et al. 2009; Seibold et al. 2009). Beingquick, noninvasive, and allowing a dynamic evaluation,US is ideal to focus on a structure as involved in theshoulder biomechanics as the rotator cable. On US scans,the morphology of the rotator cable could vary froma thick cable of fibers to thin flattened fibers traversingdeep to the rotator cuff (Morag et al. 2009). To our latestknowledge, no imaging studieswere performed to describethemodification of rotator cable consistencywith aging, aspostulated at surgery by Burkhart et al. (1993).
Thus, the purpose of our study was to characterizethe US appearance of the rotator cuff cable in asymptom-atic shoulders of volunteers of different ages, also esti-mating interobserver reproducibility.
MATERIALS AND METHODS
Institutional Review Board approval and volunteerinformed consent were obtained.
From September 2009 to August 2010, 84 asymp-tomatic volunteers were prospectively screened to beincluded in our study. Volunteers with shoulder pain,limited range of motion or history of symptomaticshoulder or trauma were previously excluded from thescreening. They were divided into two groups accordingto their age, matched for sex. Our screening group wascomposed by 42 ‘‘young’’ (21 males and 21 females,age range 21–35 years, mean age 26 6 7.1 years[mean 6 standard deviation]) and 42 ‘‘elderly’’ volun-teers (21 males and 21 females, age range 65–84 years,mean 74 6 5.2 years). Eighty-four shoulders werescreened for each group, 168 shoulders overall.
US evaluation of supraspinatus and infraspinatustendons was performed both on long and short axiswith ultrasound equipment (MyLab 70 XvG; Esaote,Genova, Italy) provided with a high-resolution 13–6MHz transducer, according to the guidelines issued bythe European Society of Musculoskeletal Radiology(Martinoli 2010). Evaluations were performed by twodifferent radiologists (E.S. and L.M.S.) with 20 and5 years of experience in musculoskeletal US, respec-tively. To assess interobserver reproducibility, all shoul-ders of elderly volunteers were evaluated separately byeach radiologist blinded to the other. Shoulders of youngvolunteers were assessed by the most experienced radiol-ogist only.
Shoulders where any partial- or full-thickness tearsof supraspinatus and/or infraspinatus tendon were foundwere excluded from our study (one shoulder in younggroup and 18 shoulders in elderly group). Thus, our study
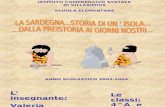
Fig. 1. Anatomy of the rotator cuff cable. (a) Coronal cross-sectional illustration of the shoulder showing the site of rotatorcable (white arrow), located approximately 1–1.5 cm mediallyto the crescent area (asterisks) of the supraspinatus tendon(SSPt). A 5 acromion; C 5 clavicula; D 5 deltoid muscle;H 5 humerus; SSPm 5 supraspinatus muscle belly. (b) Ultra-sound appearance of rotator cable (white arrows) and of thecrescent area (asterisks) in a volunteer of 72 years. D5 deltoid;
H 5 humerus.
36 Ultrasound in Medicine and Biology Volume 38, Number 1, 2012
martedì 16 ottobre 12

Tendine del sopraspinato!
the last few years. Armfield et al. (2003) publisheda detailed review about shoulder biomechanics and howimaging can detail shoulder function and dysfunction,including some brief notes about rotator cable. Kasket al. (2008) and Sheah et al. (2009) described themagnetic resonance (MR) arthrography appearance ofsuch structure either in cadavers (Kask et al. 2008) or in
injured shoulders (Sheah et al. 2009) while its ultrasound(US) appearance was described by Morag et al. in 2009.
US plays a central role in rotator cuff imaging(El-Dalati et al. 2009; Rutten et al. 2009; Teefey et al.2009; Vlychou et al. 2009; Seibold et al. 2009). Beingquick, noninvasive, and allowing a dynamic evaluation,US is ideal to focus on a structure as involved in theshoulder biomechanics as the rotator cable. On US scans,the morphology of the rotator cable could vary froma thick cable of fibers to thin flattened fibers traversingdeep to the rotator cuff (Morag et al. 2009). To our latestknowledge, no imaging studieswere performed to describethemodification of rotator cable consistencywith aging, aspostulated at surgery by Burkhart et al. (1993).
Thus, the purpose of our study was to characterizethe US appearance of the rotator cuff cable in asymptom-atic shoulders of volunteers of different ages, also esti-mating interobserver reproducibility.
MATERIALS AND METHODS
Institutional Review Board approval and volunteerinformed consent were obtained.
From September 2009 to August 2010, 84 asymp-tomatic volunteers were prospectively screened to beincluded in our study. Volunteers with shoulder pain,limited range of motion or history of symptomaticshoulder or trauma were previously excluded from thescreening. They were divided into two groups accordingto their age, matched for sex. Our screening group wascomposed by 42 ‘‘young’’ (21 males and 21 females,age range 21–35 years, mean age 26 6 7.1 years[mean 6 standard deviation]) and 42 ‘‘elderly’’ volun-teers (21 males and 21 females, age range 65–84 years,mean 74 6 5.2 years). Eighty-four shoulders werescreened for each group, 168 shoulders overall.
US evaluation of supraspinatus and infraspinatustendons was performed both on long and short axiswith ultrasound equipment (MyLab 70 XvG; Esaote,Genova, Italy) provided with a high-resolution 13–6MHz transducer, according to the guidelines issued bythe European Society of Musculoskeletal Radiology(Martinoli 2010). Evaluations were performed by twodifferent radiologists (E.S. and L.M.S.) with 20 and5 years of experience in musculoskeletal US, respec-tively. To assess interobserver reproducibility, all shoul-ders of elderly volunteers were evaluated separately byeach radiologist blinded to the other. Shoulders of youngvolunteers were assessed by the most experienced radiol-ogist only.
Shoulders where any partial- or full-thickness tearsof supraspinatus and/or infraspinatus tendon were foundwere excluded from our study (one shoulder in younggroup and 18 shoulders in elderly group). Thus, our study
Fig. 1. Anatomy of the rotator cuff cable. (a) Coronal cross-sectional illustration of the shoulder showing the site of rotatorcable (white arrow), located approximately 1–1.5 cm mediallyto the crescent area (asterisks) of the supraspinatus tendon(SSPt). A 5 acromion; C 5 clavicula; D 5 deltoid muscle;H 5 humerus; SSPm 5 supraspinatus muscle belly. (b) Ultra-sound appearance of rotator cable (white arrows) and of thecrescent area (asterisks) in a volunteer of 72 years. D5 deltoid;
H 5 humerus.
36 Ultrasound in Medicine and Biology Volume 38, Number 1, 2012
rotator cuff cable
martedì 16 ottobre 12

Tendine del sopraspinato!
martedì 16 ottobre 12

Tendine del sopraspinato!
martedì 16 ottobre 12

Tendine del sopraspinato
martedì 16 ottobre 12

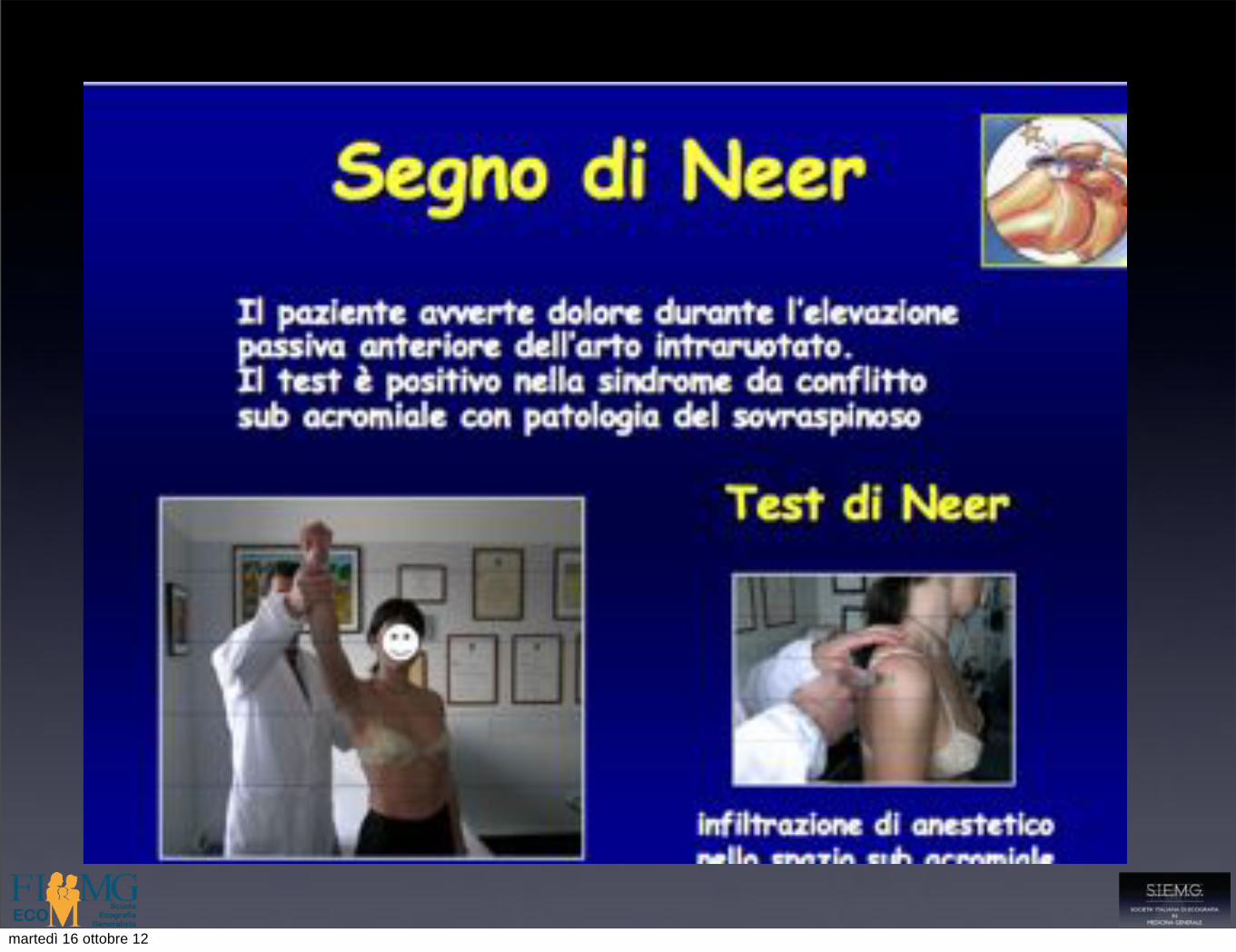
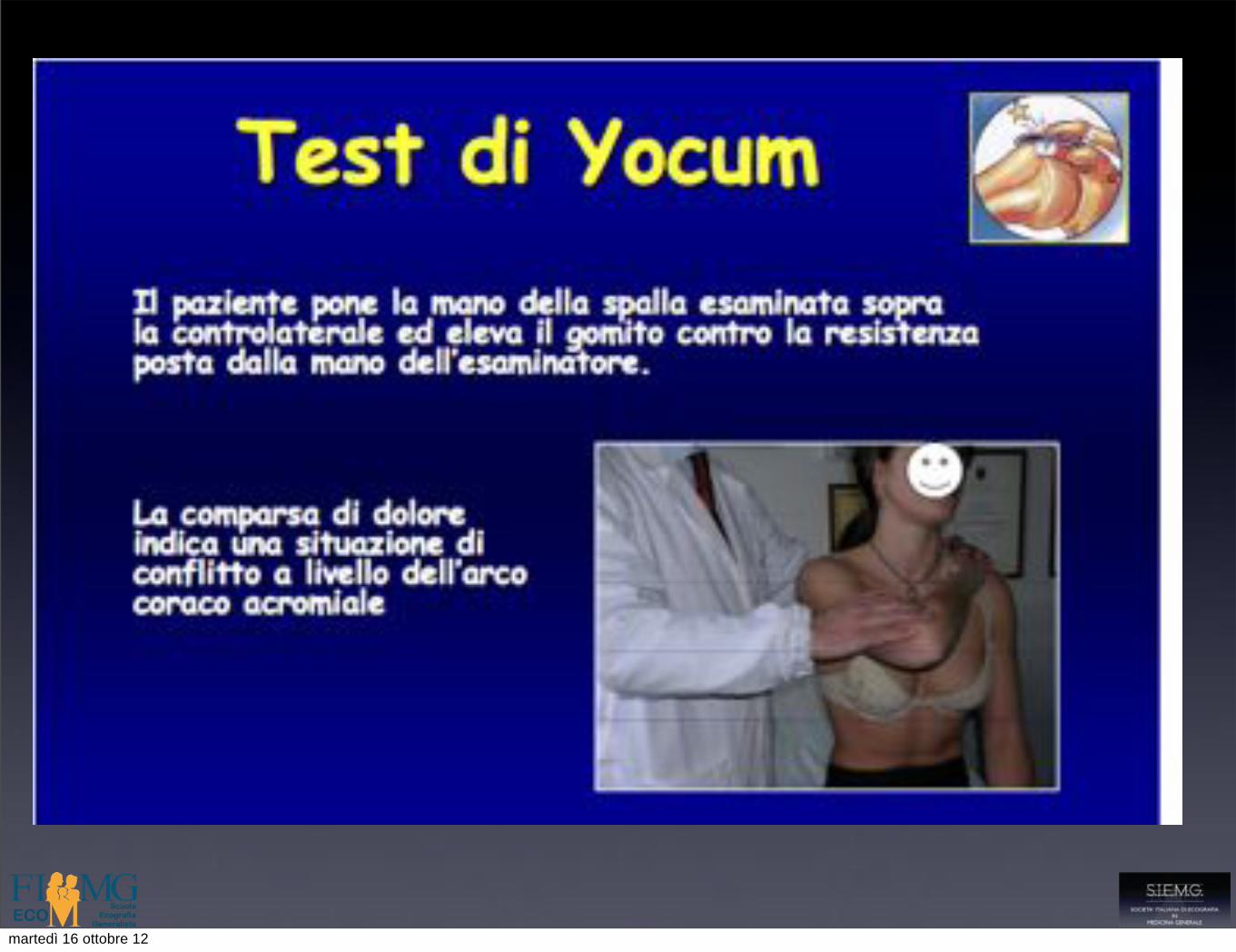
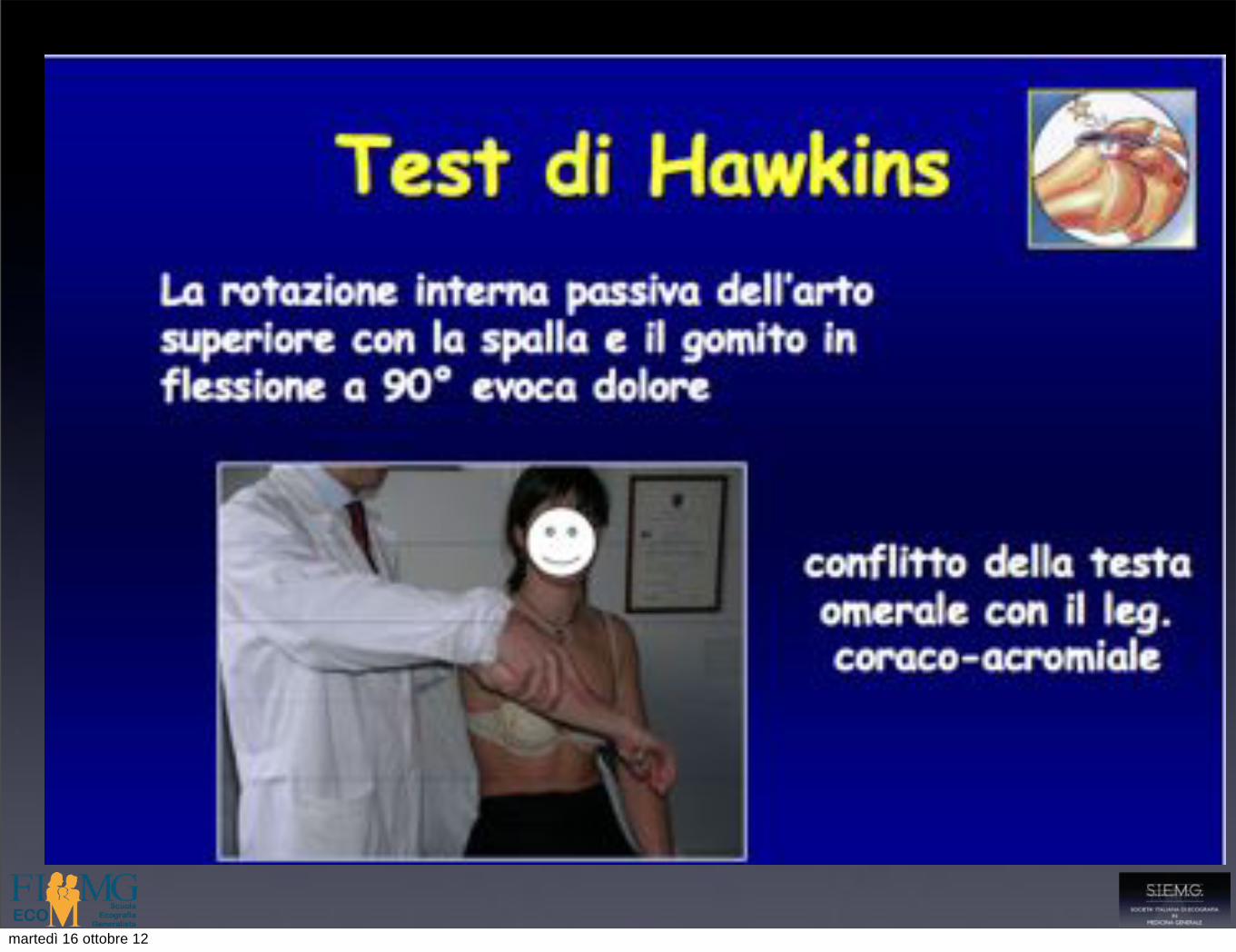
Test impingment subacromiale !( antero-superiore)"
martedì 16 ottobre 12
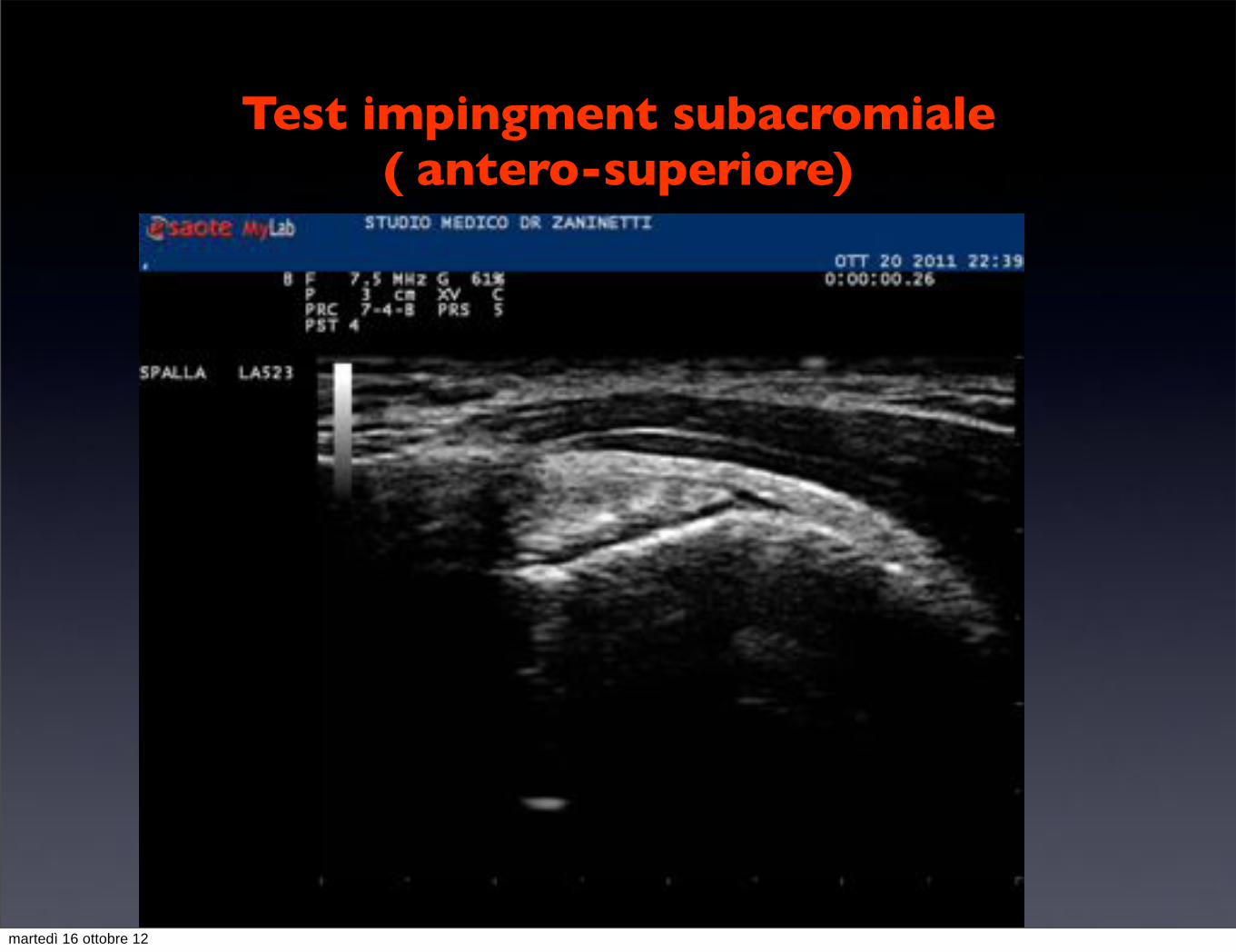
Test impingment subacromiale ( antero-superiore)
martedì 16 ottobre 12
Borsa sotto acromio deltoidea
• In condizioni normali è uno spazio virtuale fra il tendine del sopraspinato e il soprastante m. deltoide
• Ha l’aspetto di una linea anecogena dello spessore di circa 1-2 mm
• La linea iperecogena di analogo spessore che separa la borsa dal deltoide è costituita dalla parete della borsa e dalla fascia muscolare del deltoide a stretto contatto
martedì 16 ottobre 12

Borsa sotto acromio deltoidea
• In condizioni normali è uno spazio virtuale fra il tendine del sopraspinato e il soprastante m. deltoide
• Ha l’aspetto di una linea anecogena dello spessore di circa 1-2 mm
• La linea iperecogena di analogo spessore che separa la borsa dal deltoide è costituita dalla parete della borsa e dalla fascia muscolare del deltoide a stretto contatto
martedì 16 ottobre 12
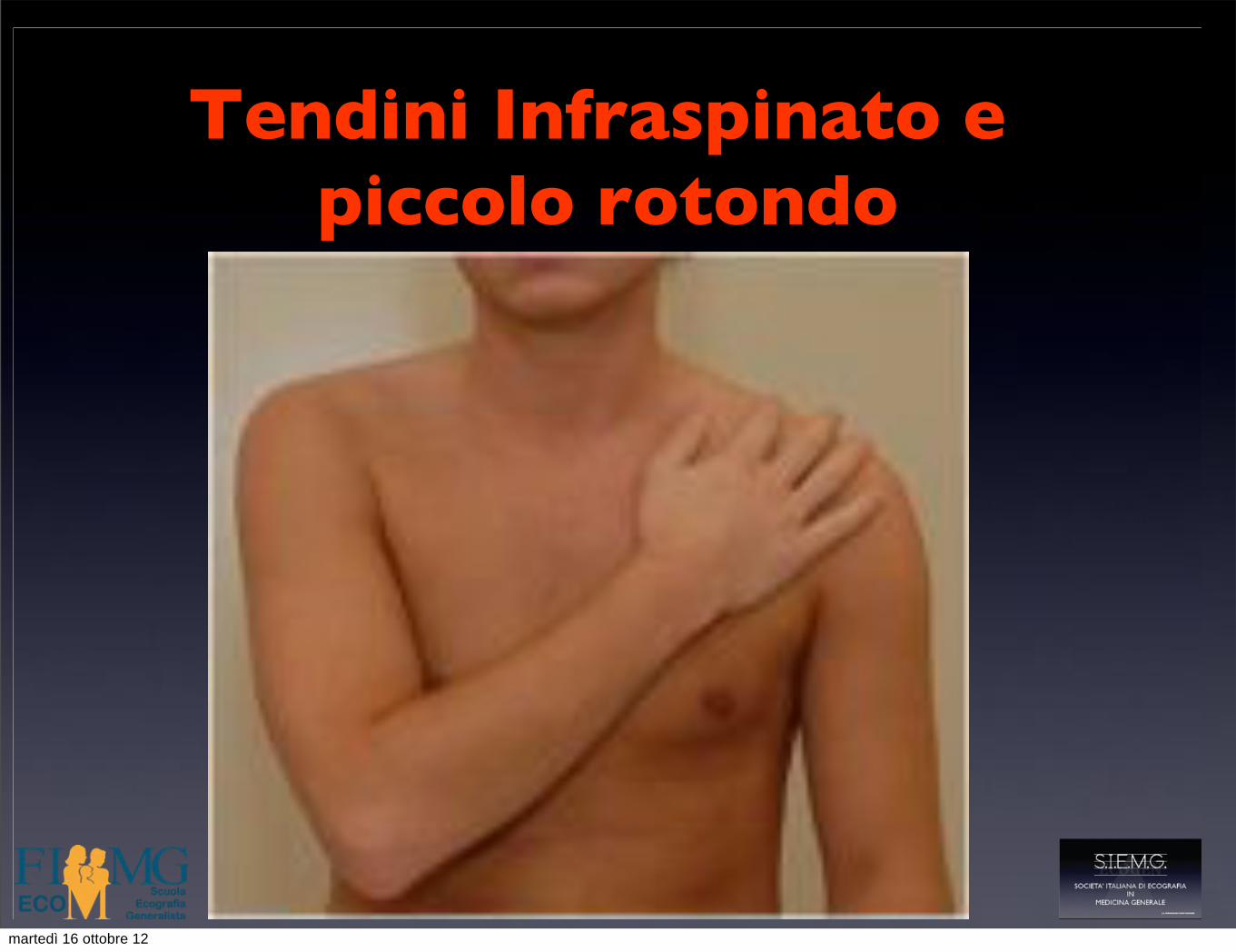
Tendini Infraspinato e piccolo rotondo!
martedì 16 ottobre 12

Tendini Infraspinato e piccolo rotondo!
martedì 16 ottobre 12

Tendini Infraspinato e piccolo rotondo!
infraspinato Picc rotondo
martedì 16 ottobre 12
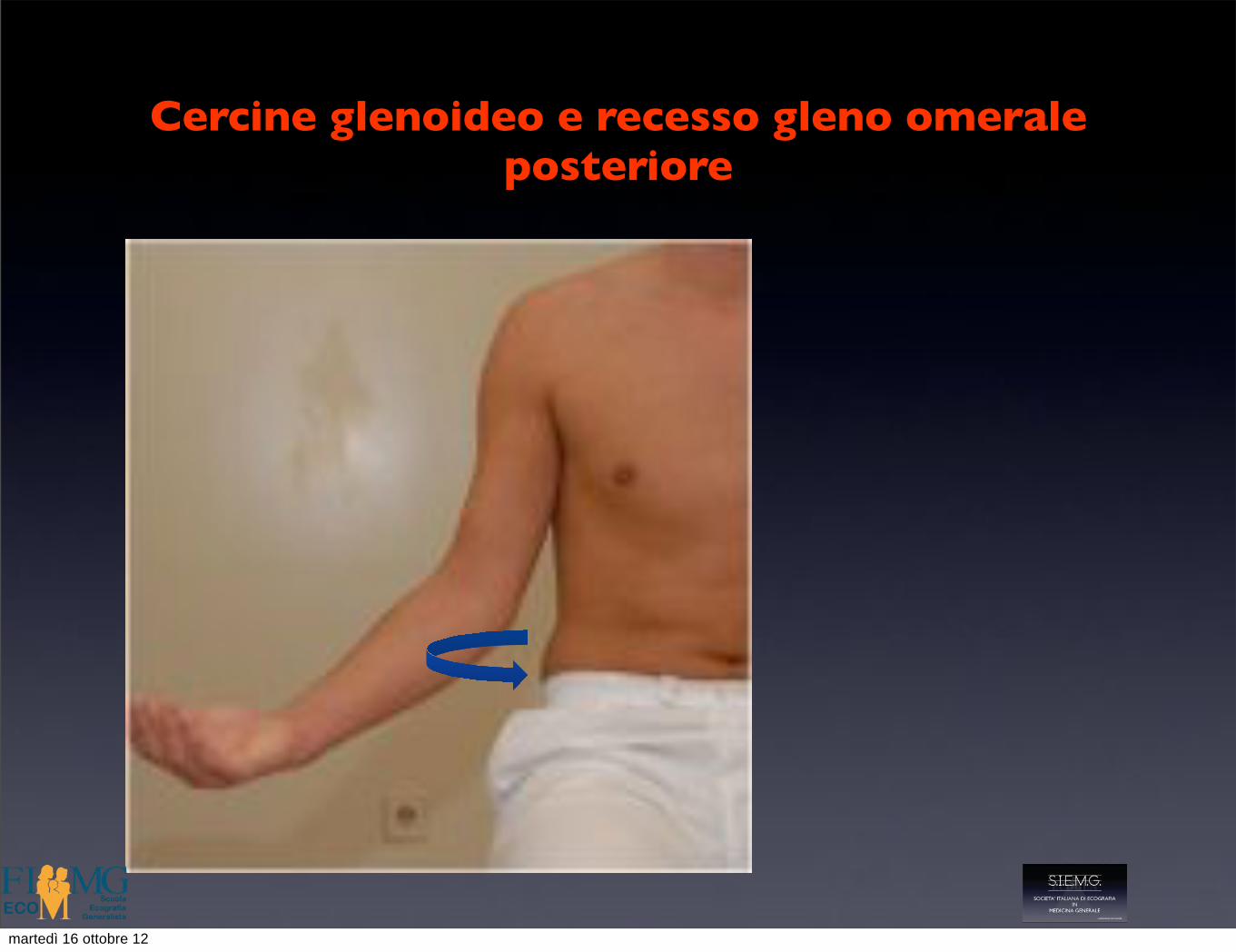
Cercine glenoideo e recesso gleno omerale posteriore
martedì 16 ottobre 12
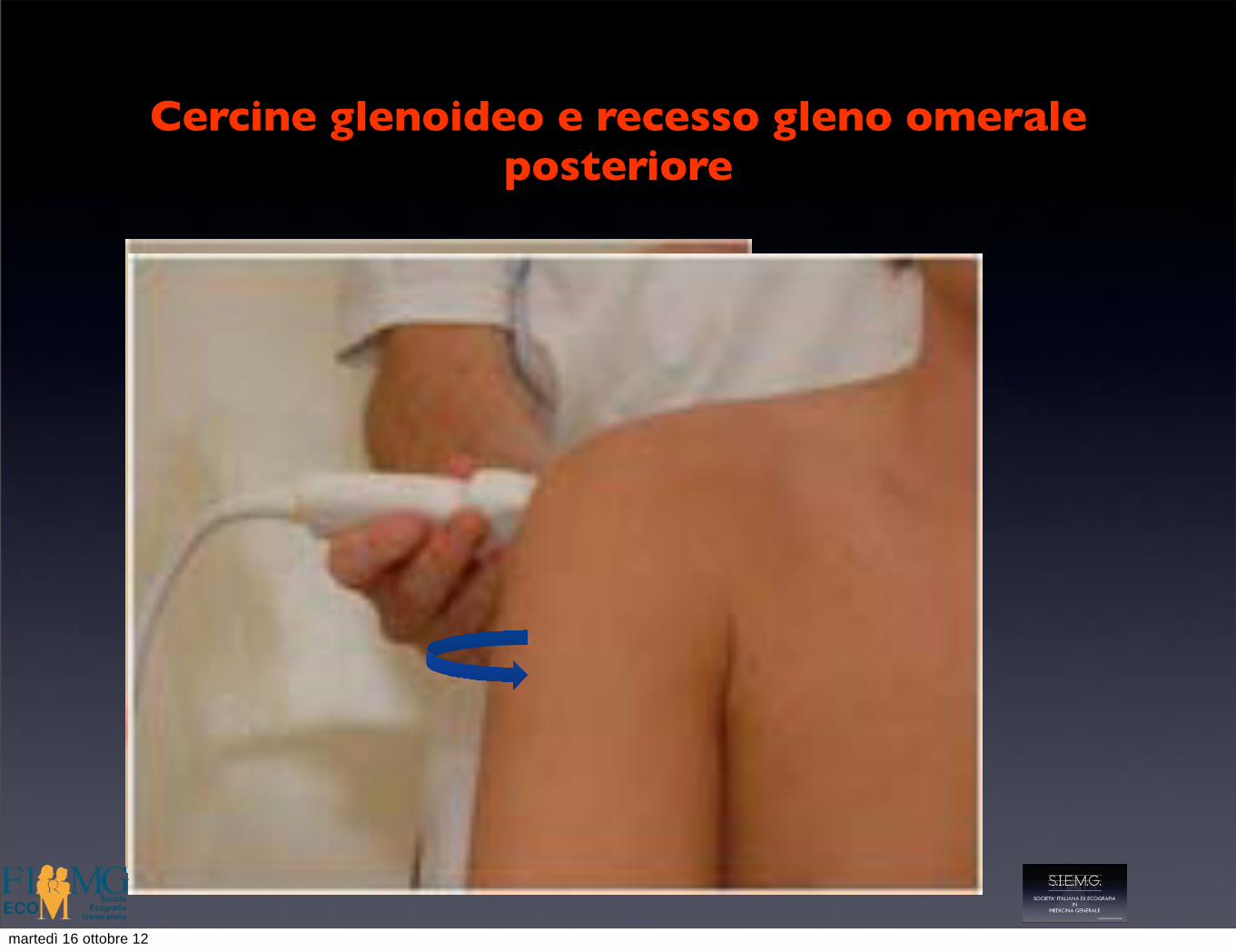
Cercine glenoideo e recesso gleno omerale posteriore
martedì 16 ottobre 12
Cercine glenoideo e recesso gleno omerale posteriore
Les conflits de la coiffeLes conflits de la coiffe
¾CONFLIT ANTERO-SUPERIEUR
¾CONFLIT ANTERIEUR
¾CONFLIT POSTERO-POSTERIEURmartedì 16 ottobre 12

Cercine glenoideo e recesso gleno omerale posteriore
Les conflits de la coiffeLes conflits de la coiffe
¾CONFLIT ANTERO-SUPERIEUR
¾CONFLIT ANTERIEUR
¾CONFLIT POSTERO-POSTERIEURmartedì 16 ottobre 12

Artic. Acromio-claveare!
martedì 16 ottobre 12
grazie per l’attenzione
martedì 16 ottobre 12