Nucleo Poro nucleare Involucro nucleare Nucleolo Sintesi rRNA.

Prof. Giovanni Paganelli
Dipartimento delle procedure e tecnologie avanzate, IRST-IRCCS – Meldola.
Universita degli Studi Ferrara
Contributo della medicina nucleare nei tumori mammari: dal linfonodo
sentinella alla IART
Months
0 60 120 180 240 300
0.0
0.2
0.4
0.6
0.8
1.0
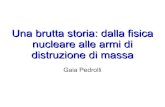
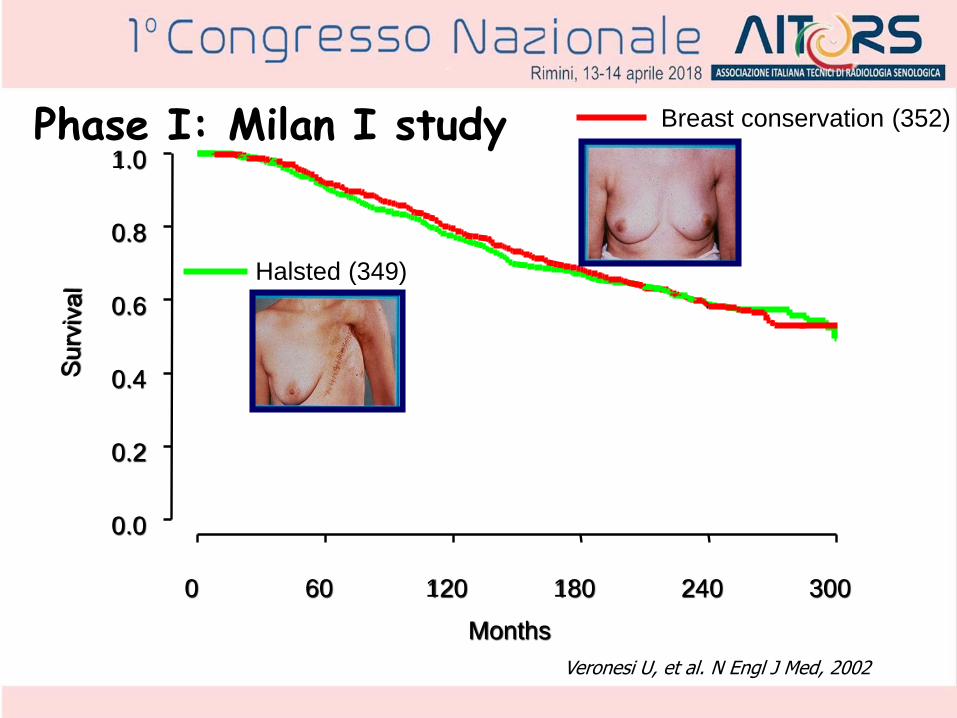
Halsted (349)
Breast conservation (352)Phase I: Milan I study
Veronesi U, et al. N Engl J Med, 2002

Twenty years ago the challenge was:
Can lymphoscintigraphy + radioguided SNB replace
axillary dissection?

Multiple SNs
lymphatic vessels to diaphragmatic and liver lymph nodes
lymphatic vessels to the controlateral breast
internal mammary chain (IMC)
subclavian axillary group
lymphatic vessels to
anterior mediastinal
lymph nodes
anterior
axillary
group
subscapular
axillary
group
lateral
axillary
group
central axillary group
interpettoral lymph nodes

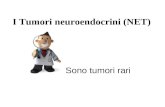
99mTc-labelled colloids (0.3 mCi/0.2ml)
< 50 nm < 80 nm 200-1000 nmSulphide Human albumin Human albumin
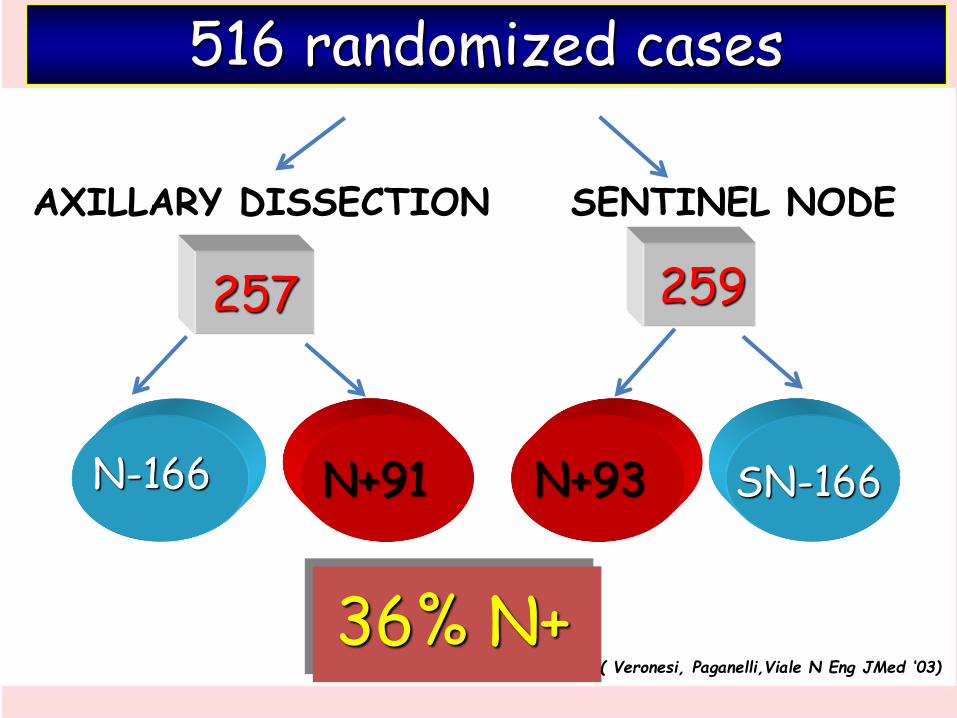
AXILLARY DISSECTION SENTINEL NODE
N-166 SN-166N+93N+91
516 randomized cases
257 259
36% N+( Veronesi, Paganelli,Viale N Eng JMed ‘03)
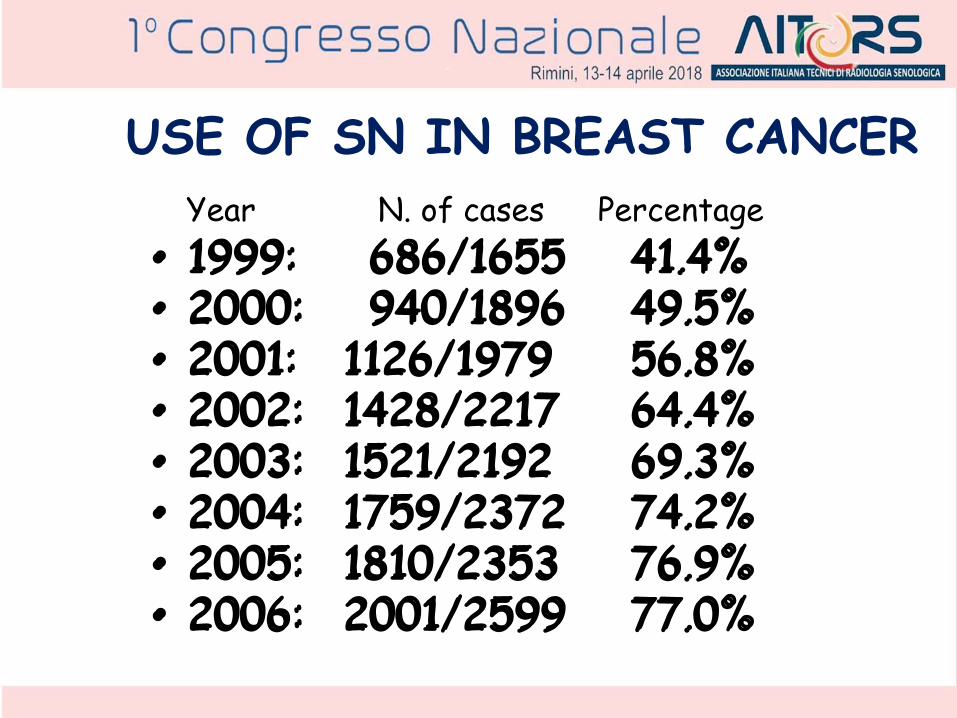
USE OF SN IN BREAST CANCER
• 1999: 686/1655 41.4%• 2000: 940/1896 49.5%• 2001: 1126/1979 56.8%• 2002: 1428/2217 64.4%• 2003: 1521/2192 69.3%• 2004: 1759/2372 74.2%• 2005: 1810/2353 76.9%• 2006: 2001/2599 77.0%
Year N. of cases Percentage

SNB after breast surgery YesSNB in multicentric cancer YesSNB after chemotherapy Yes SNB after SNB Yes SNB in pregnancy Yes SNB in male breast cancer YesSNB in DCIS OPTIONAL
Indications to SN
The 2nd Challenge was:
Can non palpable breastlesions be localized with
radioisotopes?

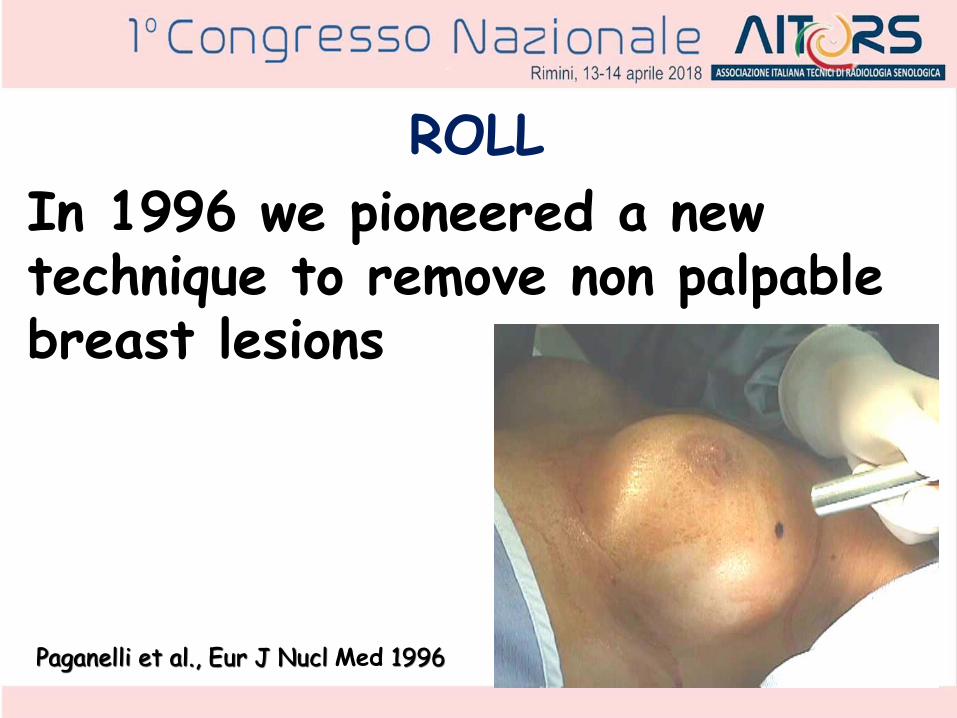
In 1996 we pioneered a new technique to remove non palpable breast lesions
ROLL
Paganelli et al., Eur J Nucl Med 1996

lateralanterior
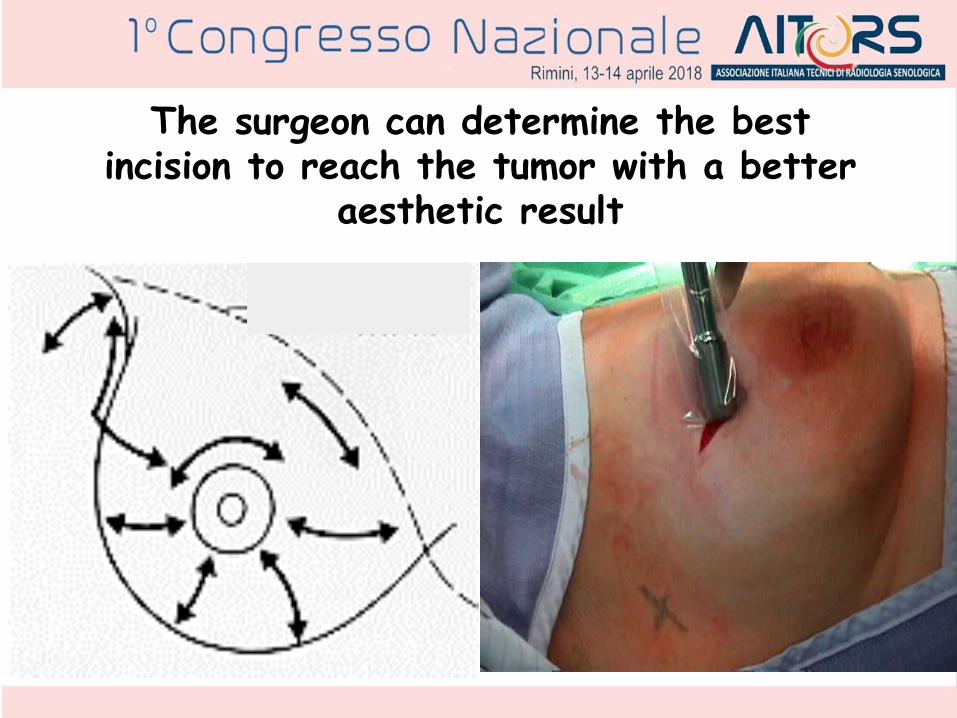
The surgeon can determine the best incision to reach the tumor with a better
aesthetic result

1 cm.
This results in high excision accuracy and centring of the lesion within specimen so that it is rarely necessary to radicalize the margins

THE FUTURE
From ROLL diagnosis to
IART® therapy

Quadrantectomy + SNB + EBRT
represent the standard therapy
in Early Breast Cancer

Open problems with EBRT• EBRT post-quadrantectomy requires 6 – 8
weeks to be completed
• EBRT may cause side effects and complications (lung – heart)
• The radiation centres are often not easy accessible

Acute skin toxicity during RT
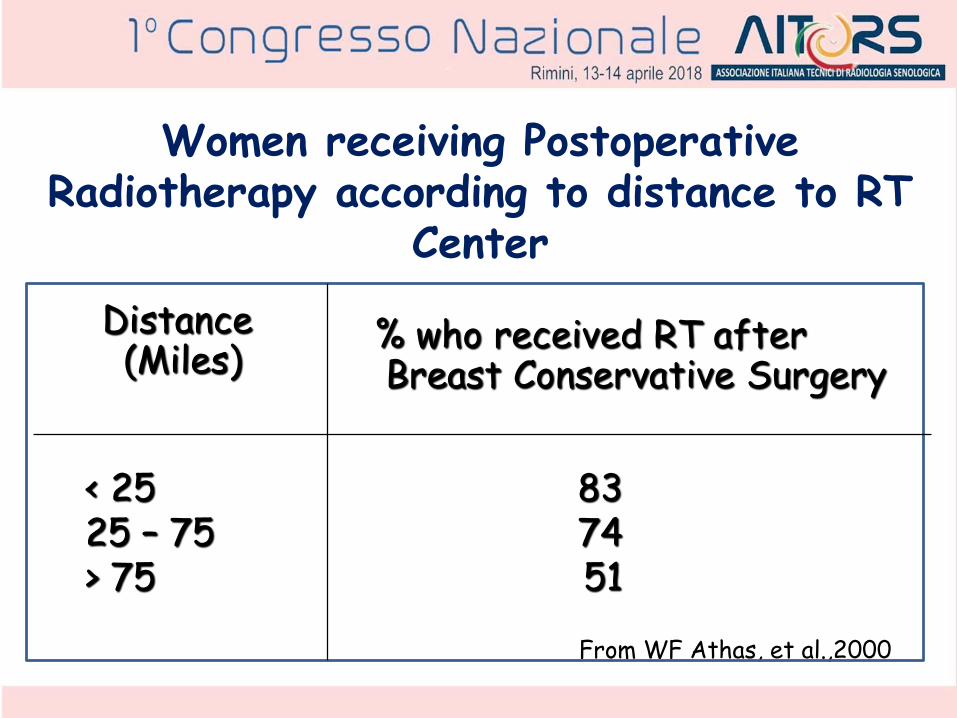
Women receiving Postoperative Radiotherapy according to distance to RT
Center
< 25 8325 – 75 74> 75 51
% who received RT afterBreast Conservative Surgery
Distance(Miles)
From WF Athas, et al.,2000

Can we modify EBRT in early breast cancer?

IntraoperativeRadiotherapyIORT / ELIOT
Partial breastIrradiationPBI

➢There are obvious advantages in terms of overall treatment time, patients comfort, cosmetic results, quality of life.
➢ELIOT represents a step to improve the quality of life of breast cancer patients.
Electrons IntraOperative Therapy
Veronesi et al., Ann Surg 2005

However ELIOT is affected by some limitations:
➢Costs
➢Limited targeted area
Electrons IntraOperative Therapy

Collimator
Skin separator
Target

anterior lateral+
+
+
Are there other methods to deliver
electrons in the operated breast?
ROLL: too large injections of 99mTc-MAA
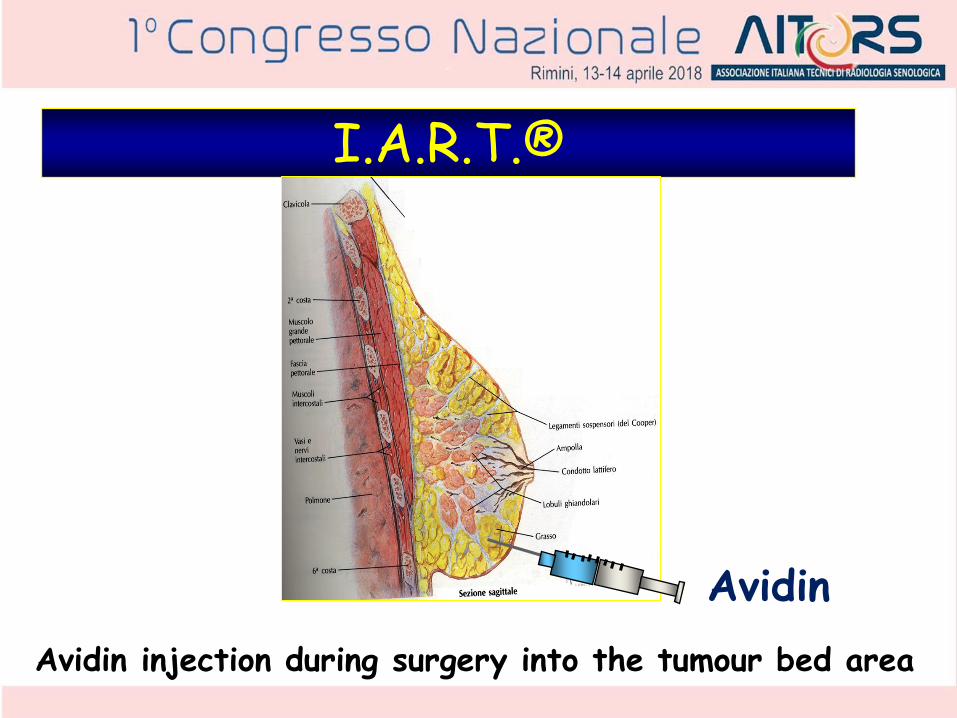
I.A.R.T.®
Avidin injection during surgery into the tumour bed area
Avidin

IART ®Intra-operative
Avidination for
Radionuclide
Theraphy

In the operative room…

Dedicated vial for90Y or 177Lu-biotin

16 to 48 hrs post-surgery 90Y-Biotin i.v. injection
…in the Nuclear Medicine Dept.

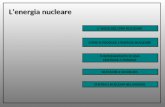
Total Body anterior view - pt no 25
1h 4h 24h 48h

Fig. 1a)
b)

IART Phase II study: summary on dosimetry
Tumour bed uptake: 8 % (4 %– 12%) of IA
Avidin injected 100 mg with dedicated syringe
Activity: 3.7 GBq of 90Y-biotin
Safe !
BED 23 Gy
Gy
20 (15 – 27)
3.7 (2.2 – 5.9)
5.2 (3.0 – 7.4)
Tumour quadrant:
Kidneys:
Ur. Bladder:
1
Pre surgery
2
Post surgery
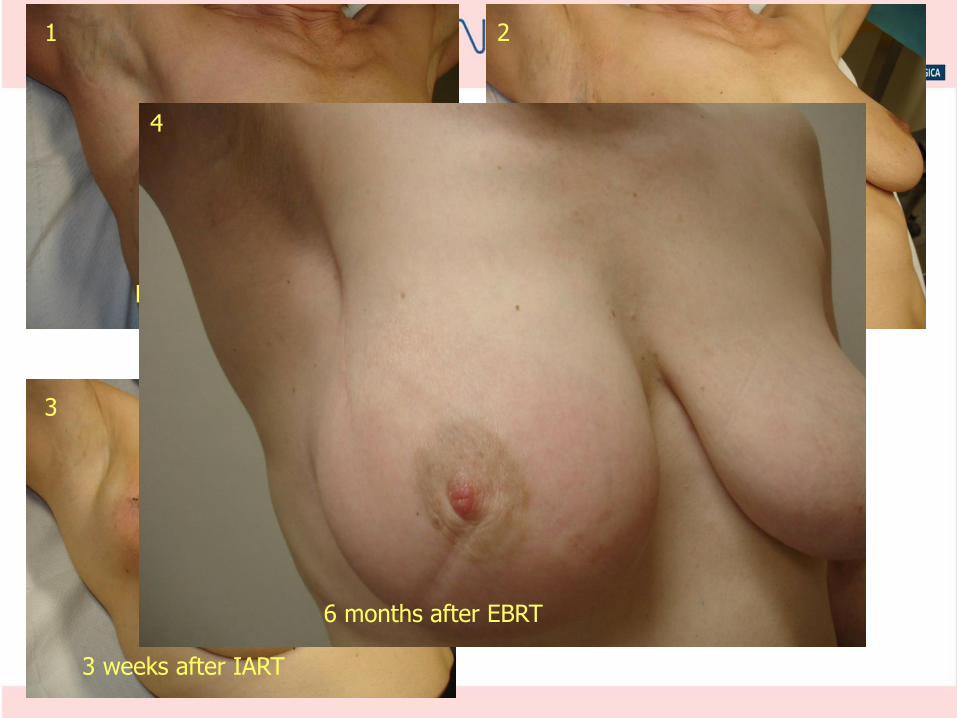
3
3 weeks after IART
6 months after EBRT
4
Conclusions
• IART® is safe and it can be applied to allBC conserving surgery in any hospital without dedicated acellerator
Dosimetry calculation ,based on our phaseII trial, supports its use in early breastcancer.
The S.A.R.A. StudyStandard -vs –Accelerated- Radio
metabolic Avidinated therapy
Phase III, multicenter, randomized, clinical trial to evaluate IART with 90Y-Biotin compared to Standard RT in patients with breast cancer candidate to RT after conservative surgery
Giovanni Paganelli IRST, Meldola